Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Remodeling Interprofessional Collaboration Through a Nurse-for-a-Day Shadowing Program for Medical Residents
Authors Low S, Gray E, Ewing A, Hain P, Kim L
Received 3 June 2021
Accepted for publication 29 July 2021
Published 27 August 2021 Volume 2021:14 Pages 2345—2349
DOI https://doi.org/10.2147/JMDH.S319728
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sarah Low,1 Emily Gray,1,2 Amanda Ewing,1– 3 Patricia Hain,1– 4 Linda Kim1– 5
1Patient Family Support Program, Cedars-Sinai Medical Center, Los Angeles, CA, USA; 2Medical Nursing Services, Cedars-Sinai Medical Center, Los Angeles, CA, USA; 3Internal Medicine Residency Training Program, Cedars-Sinai Medical Center, Los Angeles, CA, USA; 4Surgical Nursing Services, Cedars-Sinai Medical Center, Los Angeles, CA, USA; 5Nursing Research Department, Cedars-Sinai Medical Center, Los Angeles, CA, USA
Correspondence: Sarah Low Email [email protected]
Background: Evidence reflects that effective collaboration leads to improved care quality, patient satisfaction, nurse and physician retention, as well as decreased length of stay, readmissions, and costs. While interprofessional collaboration is widely accepted as the gold standard for health care, room for improvement exists within the nurse–physician relationship.
Purpose: To evaluate the impact of a shadowing experience on nursing and resident perceptions of communication and collaboration through a shared clinical experience in providing direct patient care.
Methods: From 2016 to 2020, the Internal Medicine Residency Training Program and Medical-Surgical Nursing Department collaborated to pair all internal medicine residents with a nurse preceptor for a 12-hour shift, where participants worked side-by-side in providing patient care. A total of 148 residents and 75 nurse preceptors participated in the study and were provided with a checklist of nursing activities as a guideline. Both residents and nurses completed a questionnaire regarding the shadowing experience utilizing a 5-point Likert scale, with questions focusing on collaboration and communication, program value, and impact on practice.
Results: The study found increases in resident communication with nurses from pre-intervention to post-intervention, as well as enjoyment of collaboration with nurses and understanding of the nurse’s role. Residents believed that the program should be included for all residents at the beginning of their training; similarly, nurses advocated for the program, believing that the program would improve physician–nurse communication and collaboration.
Conclusion: Interprofessional training through a Nurse-for-a-Day Program may strengthen nurse–resident relations by cultivating understanding essential for effective collaboration through mutual role understanding.
Keywords: communication, interdisciplinary, nurse–physician, nurse–resident, teamwork
Introduction
While interprofessional collaboration has been widely accepted as the gold standard in healthcare, much room for improvement exists within the nurse–physician relationship.1–5 Evidence reflects that effective collaboration leads to improved care quality, patient satisfaction, nurse and physician retention, as well as decreased length of stay, readmissions, and costs.6–17 Researchers theorized that dedicated time for collaboration and knowledge sharing between interprofessional team members, as well as a reversal of the traditional physician-to-nurse hierarchy, would serve as an integral part of new physician training, leading to lasting and improved nurse–physician collaboration.
Findings from recent studies showed promise for improving interprofessional communication and collaboration between nurses and physicians. Benike and Clark18 paired residents with a nurse preceptor for a 4-hour window, where they observed direct bedside care provided by nurses, and found that residents and nurses lacked an understanding of the work of each discipline.18 Two studies examined the pairing of physicians and nurses for a 4-hour shadowing experience; Benike and Clark19 paired experienced physicians with nurses, and Johnson et al20 paired 17 first-year residents with nurses in which the nurses acted as preceptors and physicians as preceptees. Both found that such programs could improve perceptions of physician–nurse collaboration and knowledge of nursing workflows.19,20
The purpose of this study was to evaluate the effect of the Nurse-for-a-Day (NFAD) program on interprofessional communication and collaboration through the creation of a shared clinical and patient care experience, with the ultimate goal of improving the interprofessional experience for both disciplines. This study builds upon existing literature by extending the length of the shadowing experience to cover the full 12-hour shift from beginning to end, utilizing the resources and educational culture of an academic teaching hospital in a unique way at the bedside, providing residents with structured clinical and hands-on skills opportunities, and facilitating the opportunity at the beginning of residency.
Materials and Methods
This study was conducted on medical units at Cedars-Sinai Medical Center in Los Angeles, CA. First-year medical residents received an orientation that described the clinical aspects of the NFAD rotation, which was part of the required residency curriculum. They were also invited to participate in the research study by volunteering to fill out a survey if they wished. Out of a pool of roughly 175 medical nurses available in the participating units, nurse preceptors were nominated by their leadership to participate in the program due to their communication ability, clinical skills, and desire to educate and share nursing knowledge. The number of nurse preceptors recruited for the program equaled the number of residents.
Intervention
The Internal Medicine Residency Training Program (IMRTP) and nursing departments collaborated to pair all medical residents with a nurse preceptor for a 12-hour shift on a medical unit within the first ten weeks of residency. Residents and nurse preceptors were provided with a checklist of nursing activities (Appendix A), which provided the practice guidelines. All medical residents participated in the 12-hour training as a part of their medical education and were invited to participate in the study by completing an anonymous online survey if they wished. Similarly, nurse preceptors were invited to participate in an anonymous online survey. A link to the information sheet and online survey was provided to all participants with a statement saying that completion and submission of the online survey serves as the participant’s consent. This study was approved by the Cedars-Sinai Medical Center’s Institutional Review Board (IRB; #Pro00044746).
Data Collection and Analysis
This study included data collected from 2016 to 2020 including a total of five cohorts of internal medicine residents who completed the residency during this timeframe. Data were collected using the NFAD Questionnaire for Residents (Appendix B) that was completed before and after the program, and the NFAD Questionnaire for Nurses (Appendix C) that was completed post-intervention. The pre-survey could be completed at any point from the start of orientation to the morning of the NFAD shift and the post-survey could be completed immediately after the shift completion till three months after the completion of the entire program. Analysis of variance analysis (ANOVA) was performed to examine participant responses between the five cohorts. No statistically significant differences were found; therefore, to increase statistical power, responses from the five cohorts were combined. Both questionnaires were developed by the authors who are all clinical educators, and no further testing was conducted. Although the questionnaires used in this study were not validated, several questions were modeled after the collaboration scale developed by Vazirani et al.6 For the purposes of this paper, only the closed-ended items are discussed; closed-ended questions utilized a 5-point Likert scale (1=Strongly Disagree, 5= Strongly Agree). Data analysis included descriptive statistics as well as chi-square, t-tests, and ANOVA to evaluate changes in pre/post perceptions. All analyses were conducted using STATA v 13.0 (Stata Corp LP, College Station, TX).
Results
Of 163 residents, 148 (90.8%) completed the pre-survey, 142 (87.1%) the post-survey; and of 75 nurses, 55 nurses (73.3%) completed the post survey. Mean age for residents was 28 years (SD=2.6) with the largest percentage identifying as Asian (n=90, 55.2%) and White (n=52, 31.9%) (Table 1). Nurse preceptors’ mean age was 35 years (SD=8.0), with the largest percentage identifying as White (n=28, 40.6%) and Asian (n=20, 29%).
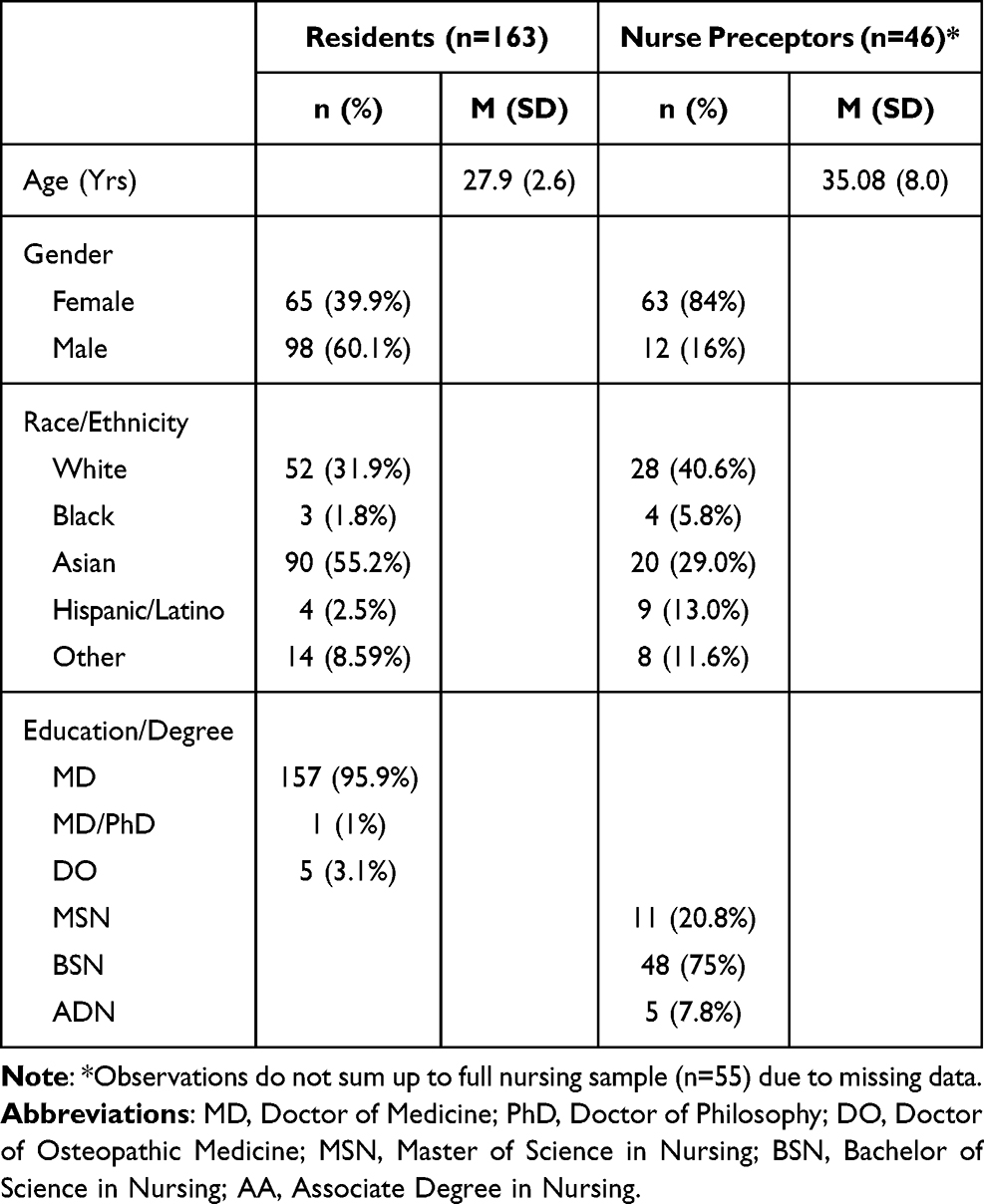 |
Table 1 Physician Residents and Nurse Preceptor Characteristics |
Statistically significant increases in physician perception of communication with nurses, enjoyment of collaborating with nurses, and understanding of the nurse’s role were evident (Table 2). Physician perception of communication with nurses improved from pre-intervention (M=3.94, SD=0.71) to post-intervention (M=4.40, SD=0.64); t(70)=−6.01, p < 0.001. Enjoyment of collaborating with nurses increased from baseline (M=4.22, SD=0.67) to post-intervention (M=4.60, SD=0.55); t(71)=−5.43, p<0.001. Residents reported their understanding of the nurse’s role deepened, with scores increasing from baseline (M=4.11, SD=0.61) to after the program (M=4.68, SD=0.50); t(71)=−8.882, p<0.001.
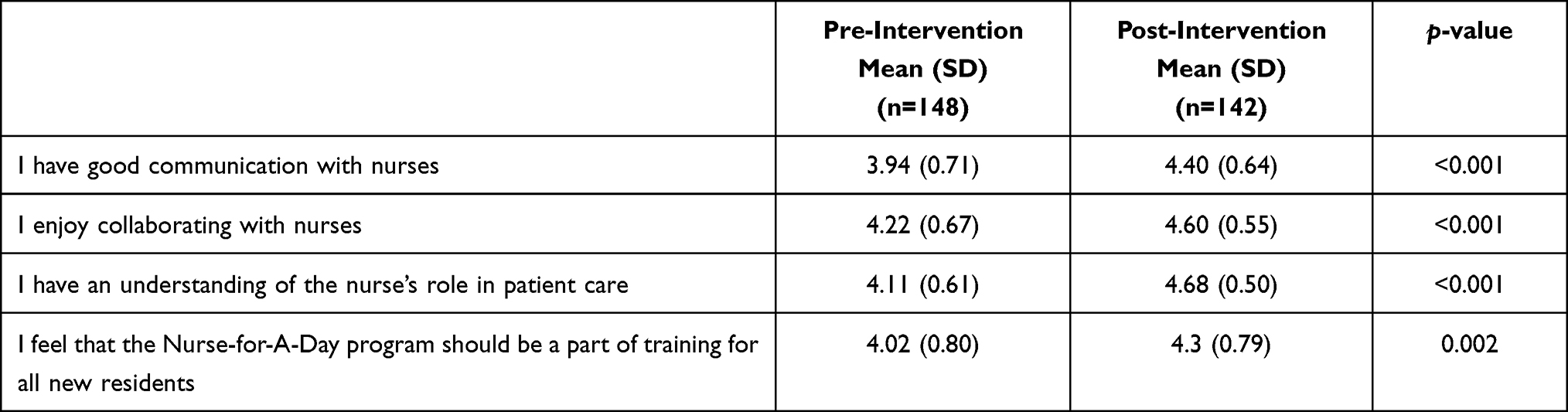 |
Table 2 Physician Residents’ Perception of Interprofessional Communication, Collaboration, Nurses’ Roles, and NFAD Program |
The study found that both disciplines deeply desired interprofessional training. Residents believed that the NFAD program should be included for all medical residents at baseline (M=4.02, SD=0.80) and more so after the program (M=4.3, SD=0.79); t(71)=−3.16, p=0.002 (Table 2). Similarly, nurses strongly advocated for the program (M=4.8, SD=0.45) (Table 3). Additionally, nurses strongly believed that the nurse for a day program would improve physician–nurse communication (M=4.76, SD=0.47) as well as physician–nurse collaboration (M=4.75, SD=0.48) (Table 2).
 |
Table 3 Nurse Perception of Interprofessional Communication, Collaboration, and NFAD Program |
Discussion
Findings from this study suggest that incorporating interprofessional training through a NFAD program may strengthen nurse–physician communication and collaboration. Both nurses and residents perceived such interprofessional training as valuable, with nurses placing higher value on this type of training. Traditional hierarchical physician and nurse relationships still exist and remain a barrier to effective interdisciplinary collaboration in a clinical setting.21 This program may also serve to invert traditional hierarchical physician and nurse relationships, and thereby promote equal decision-making, open two-way communication, and active listening that nurses reported desiring with physician counterparts.1
As training and educational curriculums presently exist in teaching institutions, there may be opportunities to create effective partnerships between disciplines with a high rate of return and lasting effects on the collaborative approach that physicians and nurses bring to their bedside throughout their careers.
Limitations to this study include the lack of a control group and the singular site nature of this study, which limits the generalizability of findings to other types of units and/or organizations. As nurse preceptors are nominated by the nursing leaders, a risk of bias is also possible. Nonetheless, the nominated preceptors also had the option of declining participation as a preceptor and in the study. Other healthcare organizations interested in implementing the NFAD or similar intervention should consider other recruitment strategies, including randomization of nurse preceptors from the available pool of nursing staff. Additionally, the resident and nurse questionnaires do not mirror each other as the original study intention was focused only on residents, and then expanded to include nurse preceptors. Since then, the questionnaires have been revised to mirror each other. Future studies applying more rigorous research methods across multiple units and/or organizations and a validated questionnaire are necessary to further support these findings. Further research should be done to evaluate the long-term impact of such programs as it relates to safety and clinical outcomes, as well as the patient experience.
Conclusion
Although future longitudinal studies are needed to validate the sustainability of improvements over time, the findings from our study highlight the importance of interprofessional training for residents early in their careers to facilitate interprofessional communication and collaboration. Interprofessional training programs, such as the NFAD program, may be used as an effective strategy to improve the work-life of healthcare providers, which, in turn, may enhance the patient experience, improve population health, and lower costs to achieve the ultimate goal of the Quadruple Aim.22
Acknowledgments
We would like to acknowledge nursing units 4NW, 4SE, 4SW, 5SE, 5SW, 7SE, and 7SW, as well as the nurse preceptors and residents who participated in this program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. House S, Havens D. Nurses’ and physicians’ perceptions of nurse-physician collaboration: a systematic review. J Nurs Adm. 2017;47(3):165–171. doi:10.1097/NNA.0000000000000460
2. Kimes A, Davis L, Medlock A, Bishop M. ‘I’m not calling him!’: disruptive physician behavior in the acute care setting. Medsurg Nurs. 2015;24(4):223–227.
3. Lancaster G, Kolakowsky-Hayner S, Kovacich J, Greer-Williams N. Interdisciplinary communication and collaboration among physicians, nurses, and unlicensed assistive personnel. J Nurs Scholarsh. 2015;47(3):275–284. doi:10.1111/jnu.12130
4. Matziou V, Vlahioti E, Perdikaris P, Matziou T, Megapanou E, Petsios K. Physician and nursing perceptions concerning interprofessional communication and collaboration. J Interprof Care. 2014;28(6):526–533. doi:10.3109/13561820.2014.934338
5. Tang CJ, Chan SW, Zhou WT, Liaw SY. Collaboration between hospital physicians and nurses: an integrated literature review. Int Nurs Rev. 2013;60(3):291–302. doi:10.1111/inr.12034
6. Vazirani S, Hays RD, Shapiro MF, Cowan M. Effect of a multidisciplinary intervention on communication and collaboration among physicians and nurses. Am J Crit Care. 2005;14(1):71–77. doi:10.4037/ajcc2005.14.1.71
7. Mast LJ, Rahman A, Bridges D, Horsley N. Exploring the impact of an interprofessional protocol on the patient experience and outcomes for seniors with diabetes. Patient Exp J. 2014;1(2):117–123. doi:10.35680/2372-0247.1034
8. Stimpfel AW, Rosen JE, McHugh MD. Understanding the role of the professional practice environment on quality of care in magnet® and non-magnet hospitals. J Nurs Adm. 2014;44(1):10–16. doi:10.1097/NNA.0000000000000015
9. Ansryan LZ, Aronow HU, Borenstein JE, et al. Systems addressing frail elder care: description of a successful model. J Nurs Adm. 2018;48(1):11–17. doi:10.1097/NNA.0000000000000564
10. Evans JR, Benore E, Banez GA. The cost-effectiveness of intensive interdisciplinary pediatric chronic pain rehabilitation. J Pediatr Psychol. 2016;41(8):849–856. doi:10.1093/jpepsy/jsv100
11. Kim LY, Rose DE, Soban LM, et al. Primary care tasks associated with provider burnout: findings from a veterans health administration survey. J Gen Intern Med. 2018;33(1):50–56. doi:10.1007/s11606-017-4188-6
12. Kim LY, Rose DE, Ganz DA, et al. Elements of the healthy work environment associated with lower primary care nurse burnout. Nurs Outlook. 2020;68(1):14–25. doi:10.1016/j.outlook.2019.06.018
13. Pakpour V, Ghafourifard M, Salimi S. Iranian nurses’ attitudes toward nurse-physician collaboration and its relationship with job satisfaction. J Caring Sci. 2019;8(2):111–116. doi:10.15171/jcs.2019.016
14. Ma C, Shang J, Bott MJ. Linking unit collaboration and nursing leadership to nurse outcomes and quality of care. J Nurs Adm. 2015;45(9):435–442. doi:10.1097/NNA.0000000000000229
15. Nelson J, Venhaus R. Improving retention through nurse/physician communication. Nurse Lead. 2005;3(1):54–56. doi:10.1016/j.mnl.2004.11.003
16. Smith CD, Balatbat C, Corbridge S, et al. Implementing optimal team-based care to reduce clinician burnout. NAM Perspectives. Discussion Paper. Washington, DC: National Academy of Medicine; 2018. Available from: https://nam.edu/implementing-optimal-team-based-care-to-reduce-clinician-burnout.
17. Welp A, Manser T. Integrating teamwork, clinician occupational well-being and patient safety - development of a conceptual framework based on a systematic review. BMC Health Serv Res. 2016;16:281. doi:10.1186/s12913-016-1535-y
18. Benike LA, Clark JE. Bridging the professional divide between nurses and medical residensts. Harvard Business Review; September 30, 2013. Available from: https://hbr.org/2013/09/bridging-the-professional-divide-between-nurses-and-medical-residents.
19. Benike LA, Clark JE. Enhancing nurse-resident physician partnerships. Creat Nurs. 2015;21(3):150–155. doi:10.1891/1078-4535.21.3.150
20. Johnson CM, Khan A, Stark S, Samee M. A nurse shadowing program for physicians: bridging the gap in understanding nursing roles. J Nurs Adm. 2020;50(6):310–313. doi:10.1097/NNA.0000000000000890
21. Filizli G, Onler E. Nurse-physician collaboration in surgical units: a questionnaire study. J Interprof Educ Pract. 2020;21:100386. doi:10.1016/j.xjep.2020.100386
22. Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573–576. doi:10.1370/afm.1713
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.