")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Religious Practices and Spiritual Well-Being of Schizophrenia: Muslim Perspective
Authors Irawati K, Indarwati F, Haris F , Lu JY, Shih YH
Received 24 December 2022
Accepted for publication 1 March 2023
Published 12 March 2023 Volume 2023:16 Pages 739—748
DOI https://doi.org/10.2147/PRBM.S402582
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mei-Chun Cheung
Kellyana Irawati,1,2 Ferika Indarwati,2,3 Fahni Haris,1,2 Jing-Yi Lu,1 Yin-Hwa Shih1
1Department of Healthcare Administration, Asia University, Taichung, Taiwan, Republic of China; 2School of Nursing, Faculty of Medical and Health Sciences, Universitas Muhammadiyah Yogyakarta, Yogyakarta, Indonesia; 3School of Nursing, Faculty of Health, Queensland University of Technology, Brisbane, Australia
Correspondence: Yin-Hwa Shih; Jing-Yi Lu, Department of Healthcare Administration, Asia University, 500, Lioufeng Road, Wufeng, Taichung, 41354, Taiwan, Republic of China, Tel +886-4-23323456 #20040 ; +886-4-23323456 #1894, Fax +886-4-23316699, Email [email protected]; [email protected]
Purpose: To explore religious activities and its functions on the spiritual wellbeing of Muslim patients with schizophrenia.
Patients and Methods: Semi-structured in-depth interviews were conducted in six schizophrenia inpatients and two female nurses. Document analysis of the standard operating procedure related to patients’ spiritual needs fulfilment and patients’ medical records were also undertaken in order to triangulate data and to get insights about patient spiritual and religious activity. Thematic analysis was used to analyse data.
Results: Five themes and 12 sub themes were revealed from the study data. The five themes elicited from the study namely frequency, timing, barriers to perform religious activities, impact on health status and negative effects if not performing the religious activities. Religious activities such as salat and dhikr for schizophrenia inpatients are still performed five times a day and when they are not getting period. Feeling upset, restless, happy, grateful, and when they are missing their family was the common reason why patients perform the religious activities. The main barriers to performing salat and dhikr for example: insufficient prayer tools and Al-Qur’an, as well as patients’ physical conditions. Religious activities such as salat and dhikr positively impact patients’ physical and mental health status, mindfulness, and concentration. Negative impacts physical and emotional are released when patients did not perform salat and dhikr.
Conclusion: The findings show that salat and dhikr which perform on time and regularly have a positive impact on the physical and mental health of schizophrenia inpatients. The author might recommend the mental health hospital provide adequate worship or prayer equipment (gown and Al-Qur`an) for patients.
Keywords: salat, dhikr, Muslim, inpatient with schizophrenia, spiritual well-being
A Letter to the Editor has been published for this article.
Plain Language Summary
Aim of the Research
This study aims to describe Muslim religious activity in schizophrenia inpatients at Mental Health Hospital and to find out the religious activity function on their spiritual wellbeing. The benefit of this study for the patients are the patients understand more about the benefits of their religious activities to reduce signs and symptoms and increase their spiritual wellbeing.
Background to the Research
At present, there is a lot of opinion that religious activities for patients with mental disorder are not commonly carried out because they are included in the people with memory loss. Therefore, this research was conducted to provide evidence and reinforcement to the patients that religious activities provide benefits to improve their mental health and wellbeing.
Design and Methods Used
This research uses a descriptive qualitative study with semi-structured in-depth interview method conducted in six schizophrenia inpatients and two female nurses as the respondents.
Patients and Public Involvement
Patients involved in this research are patients who have good communication, able to cooperate, had attended rehabilitation, did not have a religious delusion, and are aged between 40 and 60 years. Not in the acute phase. In case the acute phase occurs, the respondent is not included and is taken to the Psychiatric Intensive Care Unit to be replaced with a new patient.
Introduction
The prevalence of people with schizophrenia and psychotic disorders worldwide, including in Indonesia, is quite high, around 24 million people, or 1 in 300 persons (0.32%), globally suffer with schizophrenia.1 In Indonesia, particularly in Yogyakarta, 7 out of 1000 (2.7%) people were diagnosed with schizophrenia in 2013. This number increases by 10% in 2018.2 According to data from Ghrasia mental health hospital in Yogyakarta Indonesia, the majority of the hospitalized patients are Muslim and 61 out of them (N = 66, 92.42%) are diagnosed with schizophrenia. Schizophrenia is a severe mental disorder characterized by disturbing thoughts and emotions, disorganized speech, poor self-esteem, hallucinations, and delusions.1 Due to the symptoms experienced, people with schizophrenia have a great deal of difficulty doing activity daily living (ADL) tasks.3 Moreover, compared to those without schizophrenia, schizophrenic patients engage in less physical activity and more sedentary behaviors including less participation in spiritual and religious activities.4 However, Das et al found that schizophrenia patients who practiced greater spirituality and religiosity were better at managing stress since they employed all adaptive methods as opposed to dysfunctional abilities.5 Religious activity and coping styles can help depressed persons with physical issues avoid depression by helping them cope with their afflictions.6
Several studies reported that religious activities such as sermons, commemoration of the activities of a god or gods, and meditation are associated with spiritual wellbeing. Yamada et al investigated perspectives of adults receiving public mental health services in California (USA) related to spirituality and mental health found that more than 80% of 2050 mental health participants agreed or strongly agreed that religious activities or practices, such as prayer (73%), meditation (47%), attending religious services (40%) and spending time in nature (41%), is beneficial to their mental health.7 Religious practices may improve patients spirituality (sense of peace and purpose) which may eventually help patients increase their energy levels, relax, and connect with themselves. Altogether, spirituality and religion also play important roles in the healing process, disease prevention, coping with stress, and rehabilitation.8 Individuals with better religious practices and spirituality levels have been found to have better mental health, improved adaptability to health problems, and greater quality of life.5,9 However, health-care facilities usually ignore patients’ spiritual fulfilment since these matters could be sensitive.10 Due to lack of knowledge, fear of exacerbating psychiatric symptoms,10 and the necessity to work with a chaplain, interacting with persons with schizophrenia and fulfilling patients’ spiritual needs are hard tasks to be undertaken.11,12
The primary data from Ghrasia Mental Hospital found that most Schizophrenia patients admitted in Indonesian hospitals are Muslim. Common cultural treatments in the spiritual and religion in Islam for mental illness include servanthood, invocation (duaa), recitation of the Quran (al-Ruqyah), remembrance of Allah (dhikr), Prophetic Medicine (Tibb-i Nabavi), charity (sadaqa), working with spiritual leaders, rituals, nightly prayers, joining spiritual conversation circles known as halaqas, focusing on diet, muraqaba, and prayer (Salat).13 Salat is a collection of five obligatory daily prayers and is a direct and intimate way for individuals to communicate with God (Allah), which helps them release their anxiety, fear, and pain stemming from the stress of daily life.14,15
In Islam, people with Schizophrenia were included in people with disability which is a mental disability, it makes these people not eligible to perform salat (prayer or worship) and dhikr because of lack self-awareness.16 On the other hand, schizophrenia patients believe that engaging in dhikr activities can calm the soul, and since dhikr therapy is in line with Islamic teachings, it is frequently used when receiving treatment.17 Schizophrenia patients gained peace, the ability to live with their mental illness, and hope for the future through religious activities such as meditation, yoga, prayer, and worship, as well as creating a quiet environment, hard physical work, creative work, and reading new age books.18
Dhikr means “remembrance of Allah” and is a meditative activity that can be performed alone or in a group and is done after a salat or when a Muslim has any wish.19 Dhikr has several effects including calmness and peace, gratitude, optimism, life satisfaction, and pleasant affect.20 Dhikr, praying, reading or listening to the Al-Qur’an, and mindfulness therapies with a spiritual approach are examples of spiritual therapies that can decrease psychotic symptoms by releasing endorphins, increasing the strength of alpha brain waves, and decreasing the expression of DRD2 mRNA.21 Furthermore, the spiritual therapies are also improving a person's interpersonal forgiveness which is one of the mechanisms linking Muslim religious commitment to health and spiritual well-being.22
The theory from Panzini et al states that fulfilment of spiritual well-being is part of holistic care and an important dimension of patients’ quality of life that could be met through the practice of a religious faith.23 Spiritual well-being has a strong correlation with treatment adherence in people with schizophrenia. Thus, implying the importance of spiritual well-being for patients’ recovery. Schizophrenic people with low spiritual well-being may be disadvantaged owing to long-term treatment, insufficient or excessive social support, patient stigmatization, and a lack of non-pharmaceutical options.24 Spiritual well-being was significantly as a predictor of the subjective recovery level of schizophrenia.25 Given the effects of religious activities in increasing spiritual well-being of people with schizophrenia, therefore this study aimed to explore religious activities and spiritual wellbeing of Muslim patients with schizophrenia in Indonesia to improve the quality of healthcare service for these patients.
Materials and Methods
Ethical Approval of the Study
The study was conducted according to the guideline of the Declaration of Helsinki and was approved by the Research Ethics Committee of the Grhasia Mental Health Hospital (number 24/EC-KEPKRSJG/XII/2019).
Study Design
This is a descriptive qualitative study with the participants chosen from schizophrenia inpatients at Mental Health Hospital. All invited schizophrenia inpatients (n = 6) are hospitalized in Mental Health hospital Yogyakarta agreed to join the study and recruited after screening from nurse ward. Semi-structured interview was also conducted with six patients. Interview was conducted in Mental Health Hospital Yogyakarta by a team from school of nursing student and Psychiatric Mental Health Nurse lecture by experienced qualitative research about mental health problem. Purposive sampling was used to select patients, which match the inclusion criteria. Sampling stopped once data saturation was reached, and no new themes were identified.
The COnsolidated criteria for REporting Qualitative research (COREQ)26 was used as a guideline for reporting in this study.
Subject
Participants in the current study were recruited using purposive sampling method. Ward nurses helped the researcher (Psychiatric Mental Health Nurse) to screen the patients and recruit the participants. The inclusion criteria of the study participants as follows: Muslims with schizophrenia, had willingness to cooperate and be a respondent, attended rehabilitation, not in the acute phase, did not have religious delusion, and aged between 40 and 60 years. Patients with schizophrenia who suddenly transitioned to the acute phase or refused to continue the interviews were excluded from the study. In total, six Muslim patients with schizophrenia hospitalized at Mental Health Hospital Yogyakarta Indonesia during the duration of the study being undertaken were involved in the current research. Two female nurses from the study field were interviewed, in addition, document analysis was also being undertaken of the standard operating procedure related to patients spiritual needs fulfilment and patients medical records in order to triangulate data and to get side insight about patient spiritual and religious activity.
The researcher created pseudonyms for the participants after they had completed the interviews to ensure confidentiality. The patient code represented the order, age, and sex of the participants. For example, the code P1-F-54 meant that the first participant to be interviewed was female and 54 years old. The participant demographic characteristics are listed in Table 1.
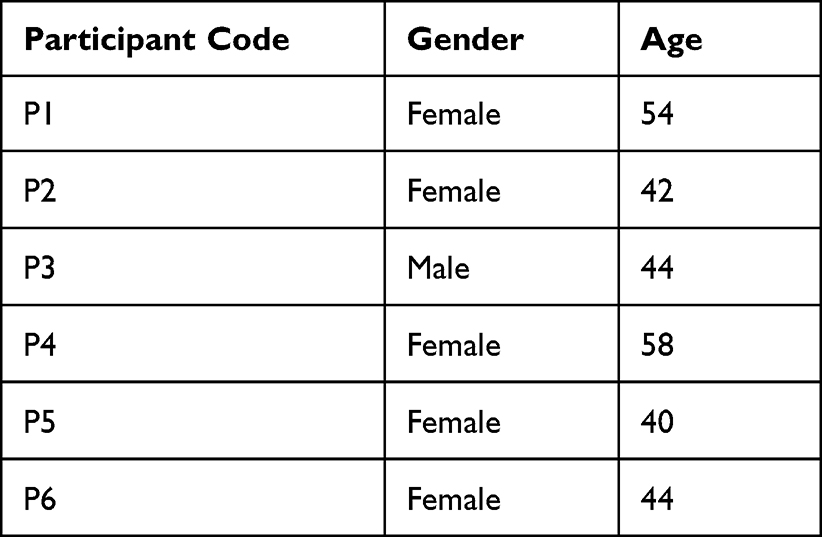 |
Table 1 Participants’ Characteristics |
Data Collection
In-depth, face-to-face interviews were utilised for data collection. Each participant was interviewed individually in a private room that was convenient for patients as well as for the researcher. Prior to the interview, participants were given information sheet and explanations related to the study. Written consent was sought from the participants if their mental capacity allows them to do so or from carers caregivers if participants are unable to consent themselves. Interview guide was used in the study, the interview questions included the following questions: 1) “What kind of religious activities do you do in this hospital?” 2) “In what kinds of situations do you perform dhikr?”; 2) “How do you perform your religious activities at a mental health hospital?”; 3) “How do you feel when you do these religious activities, can you explain?”; 4) “What is the impact of salat and dhikr on you?”; 4) “How do you feel when you do not perform the religious activities?”; 5) “What happens when you perform salat and dhikr?”; 6) “What do you think when you perform a salat?”; 7) “What do you think when you do not perform a salat?”; 8) “Do you think the hospital supports you to do the religious activities?”; 9) “Can you explain how the hospital support you?”; 10) “Do you have or experience difficulties to perform religious activities in this hospital?”; 11) “Can you explain what are the difficulties when you perform salat and dhikr?”; 12) “Do you have any complaints related to performing religious activities in this hospital?” In the interview, participants completed the information sheet with their initials, age, gender, and religion and then answered the main questions assisted by their nurse. Extended questions such as “You said that you feel calmer, can you describe what is calm do you mean?” “Can you give me an example of the calm that you feel?” were asked for clarification. Each interview lasted 45–60 minutes, depending on the participant’s status, and continued until sufficient data were obtained. The interview will be stopped if patients relapse into acute conditions, for example patients suddenly showing aggression or anger for no reason, experiencing hallucination attacks, or showing self-harm behaviours. The nurse will assist the patient to go to Psychiatric Intensive Care Unit if they are showing any negative behaviours or conditions.
The research was conducted after the patients and their families signed the informed consent forms. Responses were kept anonymous, and a non-disclosure agreement was reached, thereby giving the respondents the right to withdraw from the study at any time. The participants informed consent included publication of anonymized responses. The researcher also interviewed nurses and wrote field notes for data triangulation and to aid data analysis and interpretation. The interviews continued until no additional data could be obtained from the participants (saturation). The researcher recorded the interviews by audio-recorder and transcribed them on Microsoft Word.
Data Analysis
This study followed the steps proposed by Braun and Clarke for thematic analysis.27 The first step was familiarization with the data, which is the researcher (KI) and (FH) read and reread the data so that the researcher could become immersed in and intimately familiar with their substance. In the familiarization phase, psychiatric nurse (KI) and general nurse (FH) analysed the data that were associated with the topic. Second, the researcher (KI) and (FH) generate initial codes, which is the step in which succinct labels (codes) were created to highlight the significant characteristics of the data that could be useful in answering the research question. The third stage, the authors looked for fresh themes (ie, intriguing and noteworthy patterns in the data), choosing quotes that fit the main themes (inductive analysis). The literature and interview guides served as the basis for the creation of themes (deductive analysis). The fourth step was generating the initial themes, which included reviewing the codes and aggregated data to uncover significant broader patterns of meaning (potential themes). In this step, the researcher (KI, J-Y L, and Y-H S) compiled data pertinent to each prospective theme and assessed the potential of each candidate theme. The process of reviewing themes entails comparing the candidate themes to the dataset to ensure that they create a persuasive story about the data and answer the research question. This is the step in which themes are often refined, which may include splitting, combining, or discarding them. The fifth step was the process of defining and naming themes, which entailed conducting a thorough examination of each, determining the scope and focus of each, and determining the “story” of each. In addition, it entailed selecting an explanatory title for each theme. The sixth step was writing up, which entailed weaving together the analytic narrative and data extracts as well as contextualizing the analysis within the existing body of knowledge. This was carried out with Open Code Software version 4.0 (Informer Technologies, Inc, Los Angeles, United States) and using Microsoft Word (Microsoft, Redmond, Washington, USA).
Rigor
In terms of qualitative research, rigor is a means to build trust or confidence in the collection, processing, and interpretation of data. In this study, several steps were undertaken to ensure the rigor of the research. Before gathering the data, researcher develop the research protocol and interview guideline were created and adhered. Researchers also asked interviewees to confirm their responses (participants check), data analysis was peer reviewed by qualitative researchers, maintenance of an audit trail, and triangulation of data by the nurse in the study field and among research team members to ensure the rigor of the study.
Results
Five themes were explored in this study: the frequency of performing salat and dhikr during hospitalization, the timing of performing salat and dhikr, barriers to performing salat and dhikr, the impact of health status after performing salat and dhikr, the negative effect when the patients did not perform salat and dhikr. Table 2 presents the coding, subthemes, and themes.
 |
Table 2 Themes, Subthemes, and Codes for Data Analysis |
Theme 1. Frequency of Performing Salat and Dhikr During Hospitalization
Doing Salat Five Time a Day
Salat and dhikr are obligatory for Muslims, but not for people who lost their self-awareness including patients with mental disorders. Some of the participants stated that they performed salat and dhikr five times a day, as usual.
Yes, I do salat five times a day because salat is obligatory for Muslim. When I`m happy, sad, or in my difficult time… Whatever, I`ve done Salat five times a day… and also Sunnah prayer and dhikr. (P1-F-54)
I’m still doing salat five times a day. Yes, dhikr, I do dhikr after salat. (P6-F-44)
Doing Salat When They are Not Getting Period
The participants still perform salat and dhikr when they are hospitalized except when they have a period.
Thank God, I’m grateful because I can still do salat here, as long as I’m not menstruating. (P5-F-40)
I have been performing salat in here, even though I am not as intense at home. (P4-F-44)
Theme 2. The Timing of Performing Salat and Dhikr
The reasons for Muslim schizophrenic inpatients performing salat and dhikr are they felt upset and restless or wanted to be grateful to God or missed their families.
Feeling Upset and Restlessness
Muslim inpatients explained that they performed salat and dhikr to ease their feelings when they felt upset with their mental illness recovery or are disturbed by other patients in the ward.
I do salat and dhikr when I was offended by what my friend said and then I complained to God. Oh, Allah forgive me; my heart is offended by my feelings. O Allah, I hope I will recover, let my difficult feelings be relieved. I do salat to ask God, why my mental illness doesn’t recover. (P4-F-58)
Usually when the Adhan is heard, I go to Salat… If I’m sad, when I think about my child, I will do dhikr to ease my upset. (P6-F-44)
I do salat when I’m restless and hopeless, pray to God…and wishing I will get well soon. (P2-F-42)
Happy and Grateful
When they get a present or appreciation from their friends, nurse ward or their family about their recovery progress, they feel happy and blessed then they will do salat (Sunnah) and dhikr.
When I have got the gift or reward, I do salat as a gratitude to Allah… because I feel happy and bless. (P6-F-44)
I do salat when I`m happy, I`m cheerful. I feel blessed… I want to be closer with God. (P1-F-54)
Missing Their Family Members
The participants missed their family members which were reasons for continuing to perform salat and dhikr. If they have missed their homes, families, children, and daily activities at home, they would continue to perform salat and dhikr to relieve their concerns about their families.
I just think about wanting to go home, think about my children; their school must be good; I should cook for them every morning, should make breakfast before they go to school. (P2-F-42)
I think about my family; I want my family to feel peace and keep taking their medicine according to the rules. (P4-F-48)
If I’m sad and think about my children; I do dhikr… I miss my child; I am always thinking about my child. (P6-F-44)
Theme 3. Barriers to Performing Salat and Dhikr
Participants described impediments to praying and practicing religious activities at a mental health institution, such as a lack of Al-Qur’an, a personal prayer kit, and physical ailments that obstruct salat and dhikr.
Lack of Prayer Kit, and Al-Qur`an
There was only one gown, prayer rug, and Al-Quran in the ward, so patients had to take turns, which was uncomfortable
I do not have Al-Qur’an and there is no Al-Qur`an here, so I rarely recite the Al-Qur`an. (P1-F-54)
It is dependent on the prayer rug; we take turns with the prayer rug. Sometimes they are led, sometimes they are not, sometimes they fight to be priests, then they don’t even pray. (P3-M-44)
There is no Al-Qur’an or prayer rug. I must borrow the prayer kit and prayer rug that make me sluggish to do prayer. (P5-F-40)
The Physical Condition
The participants stated that their physical condition such as tiredness, sleepiness, and sluggishness impede the patients to do salat and dhikr in a hospital. This condition was due to the medicine that they should consume every day or exhausted with their activities in the Mental Health Hospital.
Sometimes I feel tired, I get bored, sleepy and sluggish…I don’t want to move to do salat and dhikr. (P1-F-54)
I’m tired, sleepy and sluggish, then I forget to pray. (P5-F-40)
Theme 4. Impact on Health Status After Performing Salat and Dhikr
Positive Impact on Physical Status
The participants stated that salat and dhikr had a positive impact on their physical status. They said that performing salat and dhikr made their bodies more comfortable, fit, relaxed, and flexible.
I am comfortable, calm, and pray diligently. I feel comfortable like healthy people, no angrier. (P2-F-42)
I feel fitter, not sick, calmer, happier and there is no problem with the mental illness; the body is not sick and feels calmer. (P3-M-44)
Positive Impact on Mental Status
The participants stated that after doing salat and dhikr had a positive impact, they feel more peaceful, calm, and closer to God, moreover, it can prevent the individual from getting angry and more patient.
I am more patient, like I don’t need to get angry with anyone, more calm… such we have got a reward and fortune from our God… feel happier, basically it is different if I do not pray. (P1-F-54)
I feel more relaxed, calmer. Calm down, there are no obstacles, no vengeance, no anger, and no hurt feelings. (P4-F-58)
Increased Mindfulness and Concentration
The participants stated that when they are doing salat and dhikr they experience increased concentration and mindfulness, without any interruption or other noises, and pray only to God.
If I do salat, I can be mindful. Mindfulness is full concentration, without any disturbance, focused on God, worship without any interference or other noises. (P1-F-54)
Focus, concentration while doing salat, praying when you are prostrate, not thinking anything, praying to God and surrendering. (P5-F-40)
More mindfulness when it is time to pray; I pray. I always remember God. I look at the prayer mat without anyone disturbing me. (P6-F-44)
Theme 5: The Negative Effects When the Patients Did Not Perform Salat and Dhikr
Negative Impact on Physical Status
When they did not pray, schizophrenic patients complained felt dizzy, restless, and suffered sleep disturbances. Salat and dhikr relieve fatigue and burden.
I am dizzy, restless, so I repent and do salat again. I am restless and cannot sleep. (P1-F-54)
Yes, when I do not do salat; I feel no calm; I feel more burdened. I should do dhikr even if I do not do salat. (P3-M-44)
Negative Impact on Emotion
Although mentally ill patients are exempt from salat and dhikr, they often need to worship to find calm. When they did not pray, the participants felt guilt and remorse.
I’m sorry that I used to pray often, but suddenly I did not pray. I am upset about reducing my reward from God and having more sin. (P1-F-54)
I feel regret, disappointment, and fidgety. I feel regret because of not doing salat and decreasing my reward from God. (P3-M-44)
Discussion
This qualitative study explored religious activities and its functions on spiritual wellbeing of Muslim patients with schizophrenia. The data revealed that many Muslim inpatients with schizophrenia performed salat and dhikr five times a day, as required. Because the second pillar of Islam is salat, which is required from Muslims to conduct five times daily and is the most fundamental and important act of devotion.28 They were aware of their responsibilities as Muslims and needed to satisfy their spirituality.
This study also pointed out that the participants did salat and dhikr more than five times a day or Salat Sunnah when they felt upset, restless and even more to express their happiness and gratitude. Because doing salat might affect the central nervous system and the autonomic nervous system which enhances relaxation and reduced anxiety.14,29 Even more, most of the participants performed salat and dhikr to assuage their anxiety for their family. When sorrowful and missing home, which may signify anxiety and worry, they did salat and dhikr. For them, prayer (salat) was a way to communicate with and increase trust in God during a challenging time.30 Islamic rituals supported a disciplined way of life and contributed to the development of self-control, which lowers daily stress and hopelessness31 so that salat and dhikr might reduce their worries and restlessness and increased the happiness.
However, the hospital did not provide a proper environment for them, including a lack of regular prayer times and suitable prayer rooms, and even more, inpatients did not have personal gowns and rugs which were the key points to impede their praying activities. Most mental illness sufferers stated prayer and reading the scripture helps them during difficult times and induces a willingness to obtain therapy through the Qur’an. In fact, this was related to Muslims’ belief and recognition of the Qur`an as a book of instruction and medicine.18,32 These findings emphasized that worship facilities, prayer kits, and the Al-Qur`an (the holy book) should be prepared by the mental health hospitals to support patients` prayer activity.
The study found that in performing salat and dhikr, their physical condition, such as drowsiness and exhaustion, might be due to their psychotic symptoms. Prior studies stated that patients with schizophrenia had poor physical activity due to the psychotic symptom related to increasing the activity of dopaminergic and serotonergic nerves in the brain.33–35 In addition to providing a proper environment and prayer tools, the authors suggest that hospitals arrange a proper praying time that aligns with inpatients’ specific sleep patterns.
Therefore, schizophrenia patients still need religious and spiritual activity to support their treatment, lower their psychiatric symptoms, and increase their quality of life. Because the patients found that they had positive effects on both their mental and physical conditions in a way that their bodies being more comfortable, fit, and relaxed after they did salat and dhikr. More importantly, the participants said that if they were doing salat and dhikr, it would make them be more concentrated and mindful. The relevant research proves individuals who offered a prayer on a regular and mindfulness level had better mental health than those who did not offer it on a regular and mindful basis.19 Salat movement can decrease psychiatric symptoms such as depression and anxiety,36 and activate the sympathetic nerves and parasympathetic nerves so that they can make the body relax, increase comfort and happiness, and improve their quality of life,23,29 as well as improve cognitive function. That is, individuals can obtain peace of mind through salat instead of taking medicine.
On the contrary, if the participants did not do salat and dhikr, they felt dizzy, restless, regretful, disappointed, and cannot sleep, which might have a negative effect on their emotions when they did not do salat and dhikr. The patients who have difficulty sleeping might be due to the stress of their hospitalization, so they can use meditation for stress management.37 Spirituality and religious activity have a role in mental health that might treat sleep disturbances and aid in the treatment of insomnia.38 Furthermore, people rely on their religion and beliefs to cope with stress and loss and increase their well-being and their levels of inner strength in people.39
Therefore, this study provides a better understanding of Muslim patients with schizophrenia regarding their feelings and unmet needs related to spiritual well-being during hospitalization. Salat and dhikr had positive effects on both their mental and physical conditions.
This study has some limitations. While it helped identify religious needs through one-on-one interviews with Muslim patients with schizophrenia, it was conducted at a single hospital; therefore, the results cannot be generalized. Furthermore, the discussion of barriers to spiritual activity focused solely on Muslims. This study did not reflect the prayer barriers of patients with other religious beliefs.
Conclusion
In this study, Muslim schizophrenia inpatients still pay attention to the time and frequency when performing salat and dhikr. Furthermore, the patients did salat more than five times a day related to timing and feeling. Although they have barriers to performing salat and dhikr, but they have a positive impact on their physical status and mental status and a negative impact when they do not perform it. The author suggests that medical facilities should implement practical policies and conduct ongoing staff education to remove barriers to spiritual activities to fulfil inpatients’ spiritual well-being and elevate the quality of care they receive. Therefore, the future study may describe and explore the prayer barriers of patients with other religious belief excluding Muslim.
Acknowledgments
The authors thank Dwi Cahya Ningrum, Peter Ardhianto, Ph.D. for the assistance, the Grhasia Mental Health Hospital, the nurses, and Universitas Muhammadiyah Yogyakarta for providing the research field.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Schizophrenia. WHO fact sheet schizophrenia web site; 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/schizophrenia.
2. Riskesdas T. National riskesdas report 2018. Lembaga penerbit badan penelitian dan pengembangan kesehatan. mental health web site; 2019. Available from: http://labdata.litbang.kemkes.go.id/images/download/laporan/RKD/2018/Laporan_Nasional_RKD2018_FINAL.pdf.
3. Ayres H, Panickacheril John A. The assessment of motor and process skills as a measure of ADL ability in schizophrenia. Scand J Occup Ther. 2015;22(6):470–477.
4. Scheewe TW, Jörg F, Takken T, et al. Low physical activity and cardiorespiratory fitness in people with schizophrenia: a comparison with matched healthy controls and associations with mental and physical health. Front Psychiatry. 2019;10:87.
5. Das S, Punnoose VP, Doval N, Nair VY. Spirituality, religiousness and coping in patients with schizophrenia: a cross sectional study in a tertiary care hospital. Psychiatry Res. 2018;265:238–243.
6. Koh KB. The role of religion and spirituality in health and illness. In: Koh KB, editor. Stress and Somatic Symptoms: Biopsychosociospiritual Perspectives. Cham: Springer International Publishing; 2018:305–313.
7. Yamada AM, Lukoff D, Lim SSF, Mancuso LL. Integrating spirituality and mental health: perspective of adults receiving public mental health services in California. Psycholog Relig Spiritual. 2020;12:276–287.
8. Wahyudi AW, Ah Y. The effectiveness of spiritual psychotherapy on patients with mental disorders: a systematic review. Poltekita. 2021;15(1):1–8.
9. Alshraifeen A, Alnuaimi K, Al-Rawashdeh S, Ashour A, Al-Ghabeesh S, Al-Smadi A. Spirituality, anxiety and depression among people receiving hemodialysis treatment in Jordan: a cross-sectional study. J Relig Health. 2020;59(5):2414–2429.
10. Neathery M, Taylor EJ, He Z. Perceived barriers to providing spiritual care among psychiatric mental health nurses. Arch Psychiatr Nurs. 2020;34(6):572–579. doi:10.1016/j.apnu.2020.10.004
11. Van Nieuw Amerongen-Meeuse JC, Schaap-Jonker H, Westerbroek G, Anbeek C, Braam AW. Conversations and beyond: religious/spiritual care needs among clinical mental health patients in the Netherlands. J Nerv Ment Dis. 2020;208(7):524–532. doi:10.1097/NMD.0000000000001150
12. Baumann K, Lee E, Reiser F. Spiritual needs in psychiatry and psychotherapy. In: Büssing A, editor. Spiritual Needs in Research and Practice: The Spiritual Needs Questionnaire as a Global Resource for Health and Social Care. Cham: Springer International Publishing; 2021.
13. Tanhan A, Young JS. Muslims and mental health services: a concept map and a theoretical framework. J Relig Health. 2022;61(1):23–63.
14. Doufesh H, Ibrahim F, Ismail NA, Wan Ahmad WA. Effect of Muslim prayer (Salat) on alpha electroencephalography and its relationship with autonomic nervous system activity. J Altern Complement Med. 2014;20(7):558–562.
15. Jannah S, Suttharangsaee W, Nukaew O. The effect of Islamic-Based Insight Enhancement Program (IBIEP) on medication adherence of persons with schizophrenia: a pilot study. Songklanagarind J Nurs. 2016;36:14.
16. Yaqin A. Capacity of persons with disabilities as legal subjects in Islamic law. Int J Humanit Soc Sci Religon. 2022;3(3):199–214.
17. Sulistyawati RA, Setiyarini S. Dhikr therapy for reducing anxiety in cancer patients. Asia Pac J Oncol Nurs. 2019;6(4):411–416.
18. Jones S, Sutton K, Isaacs A. Concepts, practices and advantages of spirituality among people with a chronic mental illness in Melbourne. J Relig Health. 2019;58(1):343–355.
19. Saniotis A. Understanding mind/body medicine from Muslim religious practices of Salat and Dhikr. J Relig Health. 2018;57(3):849–857.
20. Subandi MA, Chizanah L, Subhan S. Psychotheraputic dimensions of an Islamic-sufi-based rehabilitation center: a case study. Cult Med Psychiatry. 2022;46(2):582–601.
21. Krismiati Gani R, Sawitri B, Vilanova Syamsuri M. Cultural-based intervention for psychotic using spiritual therapy in Madura, Indonesia: a case report. Int J Sci Res Publ. 2022;97:1.
22. Abu-Raiya H, Ayten A. Religious involvement, interpersonal forgiveness and mental health and well-being among a multinational sample of Muslims. J Happiness Stud. 2020;21(8):3051–3067.
23. Panzini RG, Mosqueiro BP, Zimpel RR, Bandeira DR, Rocha NS, Fleck MP. Quality-of-life and spirituality. Int Rev Psychiatry. 2017;29(3):263–282.
24. Gültekin A, Kavak Budak F. Does spiritual well-being affect medication adherence in individuals diagnosed with mental illness in Turkey? J Relig Health. 2022;61(1):64–78.
25. Can ÖZY, Duran S. The effect of spirituality on the subjective recovery of psychiatric patients. J Relig Health. 2021;60(4):2438–2449.
26. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357.
27. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
28. Koubaa A, Ammar A, Benjdira B, et al. Activity monitoring if Islamic prayer (Salat) postures using deep learning.
29. Pasha MC, Pasha HC. A review of the literature on the health benefit of Salat (Islamic Prayer). Med J Malaysia. 2021;76:5.
30. Callender KA, Ong LZ, Othman EH. Prayers and mindfulness in relation to mental health among first-generation immigrant and refugee Muslim women in the USA: an exploratory study. J Relig Health. 2022;2022:1.
31. Najam KS, Khan RS, Waheed A, Hassan R. Impact of Islamic practices on the mental health of Muslims. J Int Dent Medical Res. 2019;5(1):1–6.
32. Saged AAG, Mohd Yusoff MYZ, Abdul Latif F, et al. Impact of Quran in treatment of the psychological disorder and spiritual illness. J Relig Health. 2020;59(4):1824–1837.
33. Arazi H, Seyedeh Shiva D, Suzuki K. Effects of exercise training on depression and anxiety with changing neurotransmitters in methamphetamine long term abusers: a narrative review. Biomed Hum Kinetics. 2022;14(1):117–126.
34. Stubbs B, Firth J, Berry A, et al. How much physical activity do people with schizophrenia engage in? A systematic review, comparative meta-analysis and meta-regression. Schizophr Res. 2016;176(2):431–440.
35. Ringen PA, Faerden A, Antonsen B, et al. Cardiometabolic risk factors, physical activity and psychiatric status in patients in long-term psychiatric inpatient departments. Nord J Psychiatry. 2018;72(4):296–302.
36. Serfaty DR, Cherniak AD, Strous RD. How are psychotic symptoms and treatment factors affected by religion? A cross-sectional study about religious coping among ultra-Orthodox Jews. Psychiatry Res. 2020;293:113349.
37. Sujeethasai K. The effect of meditation in insomnia due to stress: a case study. JDDT. 2020;10(3):1–3.
38. de Diego-Cordero R, Acevedo-Aguilera R, Vega-Escaño J, Lucchetti G. The use of spiritual and religious interventions for the treatment for insomnia: a scoping review. J Relig Health. 2022;61(1):507–523.
39. Koenig HG, Al Shohaib SS. Religiosity and mental health in Islam. In: Moffic HS, Hankir AZ, Peteet J, Awaad R, editors. Islamophobia and Psychiatry. Vol. 1. Switzerland: Springer Nature Switzerland AG; 2019:55–65.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.