Back to Journals » Psychology Research and Behavior Management » Volume 16
Reliability and Validity of Self-Concealment Scale in Chinese Older Adults
Authors Fan Z ![]() , Shi X
, Shi X ![]() , Hu C, Zhu L, Wang Z
, Hu C, Zhu L, Wang Z
Received 13 August 2023
Accepted for publication 11 October 2023
Published 25 October 2023 Volume 2023:16 Pages 4341—4352
DOI https://doi.org/10.2147/PRBM.S434491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Zhiguang Fan,1 Xiaoli Shi,2 Chunjie Hu,3 Liya Zhu,4 Zhe Wang5
1Department of Psychology, Shaoxing University, Zhejiang, 312000, People’s Republic of China; 2School of Education, Jilin International Studies University, Changchun, 130000, People’s Republic of China; 3The Affiliated Hospital of Changchun University of Chinese Medicine, Changchun, 130000, People’s Republic of China; 4School of Chinese Medicine, Changchun University of Chinese Medicine, Changchun, 130000, People’s Republic of China; 5School of Pharmacology, Changchun University of Chinese Medicine, Changchun, 130000, People’s Republic of China
Correspondence: Zhe Wang, Email [email protected]
Background: Individuals who initiate the concealment of their adverse or distressing thoughts from others can trigger off negative psychological experiences and social isolation, and lead to poorer health. Therefore, this study aimed to analyze the psychometric properties of the Self-Concealment Scale (SCS) in Chinese older adults.
Methods: A questionnaire was administered to 1085 elderly people using convenience sampling and snowball sampling. Scales used included the SCS, Distress Disclosure Index (DDI), Revised Cheek and Buss Shyness Scale (RCBS), Social Interaction Anxiety Scale (SIAS), Social Phobia Scale (SPS), UCLA Loneliness Scale (ULS-8), and Kessler Psychological Distress Scale (K10).
Results: The SCS consisted of 10 items with a one-dimensional structure, explaining 55.66% of the variance. The factor loading values for each item ranged from 0.68 to 0.75, and the covariance ranged from 0.46 to 0.57. Confirmatory factor analysis showed good model fit (χ 2/df=2.829, RMSEA=0.057, CFI=0.981, IFI=0.981, TLI=0.974, PNFI=0.712, PGFI=0.719). The criterion-related validity test found that the SCS was significantly and positively correlated with the RCBS, SIAS, SPS, ULS-8, K10, depression, and anxiety; and the SCS was significantly and negatively correlated with the DDI. The Cronbach’s α coefficient value for the scale was 0.923; the split-half reliability coefficient value was 0.923. In addition, the SCS had cross-gender consistency.
Conclusion: The SCS has good reliability and validity in older adults and can be used as a valid tool to assess self-concealment among older people.
Keywords: older adult, self-concealment, reliability, validity
Introduction
No one will ever completely disclose information about themselves to others, even to their loved ones and lovers.1 Not only is the subject and content of each person’s secret different, but there are also significant individual differences in the propensity to conceal or disclose information.2 Self-concealment refers to the active and conscious concealment of information about one’s thoughts, emotions, behaviors, or events.3 In terms of valence, information is usually highly intimate and negative. The content of the messages focuses on painful or traumatic experiences such as childhood abuse, grief, serious illness, painful psychological feelings or negative self-evaluation. People may make self-concealing decisions and behaviors for a variety of reasons. For example, individuals tend to hide their mistakes, shortcomings, pain, or negative feelings to maintain a positive image and to avoid damage to their reputation or relationships caused by secret disclosure.4
Self-concealment has attracted much attention due to its close association with poor health, interpersonal distress, and maladjustment.5,6 The empirical working model suggests that when self-concealment conflicts with the desire to obtain social support and to minimize distress through disclosure, it often leads to pathological consequences such as self-regulatory dysfunction, emotional distress, somatic symptoms, low willingness to seek help, and low social support.7 Previous studies have found that self-concealment is significantly and positively associated with psychological distress, unsatisfied interpersonal needs, and suicidal thoughts, and negatively associated with perceived social support.8,9 Moreover, self-concealment may also lead to the development of problematic behaviors such as internet addiction and eating regulatory disorders.10,11 In a study by Chinweuba et al it was found that an individual’s tendency to self-concealment increased the use of alcohol, tobacco, cannabis, cocaine, and tramadol, with a particularly pronounced effect on females.12
At present, population aging has become a common trend, affecting countries at different stages of development. Efforts to improve the quality of life and well-being of older persons are considered one of the fundamental responsibilities of Governments. Older people are more likely than younger people to experience health problems, major illnesses, stressful events such as living alone, death of a loved one or spouse, and loss of functioning, as well as experiencing distress and other negative emotions more frequently.13 Withholding distress or negative information in older adults can adversely affect their physical and psychological effects.14 Therefore, research and intervention on self-concealment of the elderly is one of the measures to achieve the goal of active aging.
Although, the phenomenon of self-concealment is prevalent among older people, relevant studies have been conducted mainly among college students and young adults. Several studies have discovered that self-concealment of older adults could lead to low quality of life, greater depressive symptoms and worse evaluation of the quality of the relationship with their spouse.15,16 Moreover, the effects of self-concealment on the older adults may exhibit different characteristics from those of younger adults. For instance, Friedlander et al revealed that self-concealment was significantly and positively associated with depressive symptoms in both young and older adults, whereas self-concealment was significantly and positively associated with suicidal behaviors only in the younger population.17 Furthermore, age concealment is an important element of research in the field of self-concealment in older adults. To minimize the negative effects of age discrimination and stigma, older adults tend to use antiaging products and beauty procedures to conceal their true age.18 Typically, older women are more likely to conceal.19
In view of the negative ramifications of self-concealment in seniors on their health and well-being, there is a need for a validated instrument to detect and intervene with the focus population. Currently, researchers have developed scales to measure this psychological construct. The Tilburg Secrecy Scale (TSS) consists of five dimensions: self-concealment, possession of a secret, cognitive preoccupation, apprehension about disclosure, and social distance.20 The TSS measures an individual’s tendency to hide information as well as concerns about secret disclosure. However, the TTS is not a specialized instrument for assessing self-concealment, and only some of the dimensions are represented. In addition, researchers have developed scales for specific populations or specific components of self-concealment. For instance, Wertheim et al developed the 13-item Couples Illness Self-Concealment (CISC) scale for assessing self-concealment behavior in the context of couples coping with chronic illness.21 The Information Concealment Scale for Caregivers was primarily used to assess how often caregivers withhold, falsify or modify information about the disease.22 Similarly, there are Body Concealment Scale for Scleroderma (BCSS),23 the Atheist Identity Concealment Scale (AICS),24 and Concealment of Epilepsy Scale.25 The above scales are only applicable to specific populations of patients, nurses, or atheists, and are not applicable to assessing the propensity for self-concealment in the general population.
At present, the most frequently used measurement tool in empirical studies related to the field of self-concealment is the Self-Concealment Scale (SCS).3 The SCS consists of 10 items with a one-dimensional structure and is 5-point scored. It is worth noting that the SCS was developed in a western cultural context and that the majority of the study subjects were female, with a low number of males, only 9.48% of the total. In addition, most of the study subjects were young and middle-aged (42±10.9), and only a small number of elderly people were covered. Although, there are some shortcomings, the SCS still shows good psychometric properties. In a review of 197 papers on self-concealment, it was noted that the SCS has good Cronbach’s α coefficients (mean 0.87), retest reliability, convergent validity, and discriminant validity, and that self-concealment differs empirically and conceptually from self-disclosure.7 The SCS has currently been widely used to assess self-concealment tendencies in different populations, such as adolescents,26 romantic partners,27 mental health outpatients,28 refugees,29 and prisoners.30
Researchers have tested the validity of the SCS in different cultural contexts and discovered that the scale possesses some cross-cultural applicability. Cramer and Barry validated the single-dimension structure of the SCS in a population of Canadian university students and found good Cronbach’s α coefficients and re-test reliabilities for the scale.31 Deniz and Çok translated the SCS into Turkish and tested its reliability with elementary and secondary school students between the ages of 14 and 18.32 The results of the study indicated that the Turkish version of the SCS could be used as a valid instrument to assess adolescents’ self-concealment. Salinas-Oñate et al based on university students found that the Chilean version of the SCS had good reliability and validity.33 Moreover, Wang revised the SCS in a population of Chinese middle school students.34 The Chinese version of the SCS also showed satisfactory psychometric properties.
It is evident from the analysis of the literature that previous relevant studies have examined the validity of the SCS primarily in the adolescent population. Although, there have been researchers who have used the SCS as an assessment tool in empirical studies of self-concealment in seniors, there are no studies that have specifically explored the applicability of the scale in this population. For this reason, the purpose of this study was to examine the reliability and validity of the Chinese version of the SCS in the elderly population. Also, it has been noted in previous studies that individuals with high self-concealment have lower levels of distress expression and perceived social support, as well as higher negative emotional experiences and poorer mental health.3,35 At the same time, self-concealment can also affect an individual’s social interactions and psychosocial adjustment. Higher levels of shyness and social anxiety have been detected in individuals with high self-concealment.36,37 Based on this, the Distress Disclosure Index (DDI), Revised Cheek and Buss Shyness Scale (RCBS), Social Interaction Anxiety Scale (SIAS), Social Phobia Scale (SPS), UCLA Loneliness scale (ULS-8), and Kessler Psychological Distress Scale (K10), were used as criterion instruments to further test the criterion validity of the SCS. It was hypothesized that the SCS would be significantly and positively correlated with the RCBS, SIAD, SPS, ULS-8, and K10, and that the SCS would be significantly and negatively correlated with the DDI.
Method
Procedure and Participants
The study was conducted in two phases of the questionnaire, in which the data from the first phase were used for item analysis and exploratory factor analysis; the data from the second phase were used for confirmatory factor analysis, criterion validity, reliability, and cross-sex consistency tests. Ten times the number of items was used as a criterion for calculating the minimum sample size.38 The inclusion criteria for the study subjects were (1) aged 65 years or older (in accordance with the National Bureau of Statistics of China’s age classification criteria for the elderly); (2) voluntary participation in this survey; (3) no cognitive impairment and able to understand the content of the questionnaire items; and (4) no communication barriers. The exclusion criteria for study participants were: (a) those with mental abnormalities; (b) Alzheimer’s disease and severe cognitive dysfunction; (c) Those who are unable to complete the investigation due to serious impairment of speech, eyesight and hearing. At the end of the survey, the researchers reviewed all the data and deleted those with exactly the same answers for positive and negative options as well as those whose response time was less than or more than 2 standard deviations.
Due to the limitation of research funds, in order to obtain a sufficient number of participants, the methods of convenience sampling and snowball sampling were adopted in this study. First, the researchers recruited 150 college students as investigators in 1 university. Upon completion of the survey, each college student would be given extra credit as a reward. Second, the researchers provided intensive training to all the investigators, detailing the process, precautions, methodology, confidentiality, and anonymity of this survey. Next, the survey was conducted by the investigators in their home communities or rural areas during their vacation time. At the end of the survey, respondents were asked to recommend potential respondents who met the inclusion criteria in order to keep expanding the sample. Before starting the survey, all respondents read and signed the informed consent form in detail. The study obtained informed consent from the subjects, followed the Declaration of Helsinki, and was also approved by the Ethics Committee of Jilin International Studies University (Approval No. JY202211003).
A total of 1162 older people were surveyed in the study, with 1085 (93.37%) valid data. In the first stage (Sample 1), there were 521 valid data, of which 247 (47.41%) were male and 274 (52.59%) were female; 339 (65.07%) in urban areas and 182 (34.93%) in rural areas; 477 (91.55%) Han Chinese and 44 (8.45%) ethnic minorities; 465 (89.25%) were married, 5 (0.96%) were divorced, and 51 (9.79%) were widowed; the education level was primary school and below 282 (54.13%), 144 (27.64%) in junior high school, 50 (9.60%) in high school or vocational high school, 21 (4.03%) in junior college, and 24 (4.61%) in bachelor’s degree and above. The age ranged from 65 to 89 years old, with an average age of 74.39±5.50.
In the second stage (Sample 2), there were 564 valid data, of which 279 (49.47%) were male and 285 (50.53%) were female; 331 (58.69%) in urban areas and 233 (41.31%) in rural areas; 511 (90.60%) Han Chinese and 53 (9.40%) ethnic minorities; 507 (89.89%) married, 4 (0.71%) divorced and 53 (9.40%) widowed; 305 (54.08%) educated in primary school and below, 136 (24.8%) in junior high school, 86 (24.1%) in high school or junior college, and 53 (9.40%) widowed. (0.71%), widowed 53 (9.40%); literacy level was 305 (54.08%) in elementary school and below, 136 (24.11%) in junior high school, 86 (15.25%) in high school or vocational high school, 17 (3.01%) in junior college, and 20 (3.55%) in bachelor’s degree and above. The age ranged from 65 to 89 years old, with an average age of 73.56±5.25.
Study Measures
Self-Concealment Scale (SCS)
The SCS is composed of 10 items in a single dimension structure (eg, “I have negative thoughts about myself that I never share with anyone”).3 The Chinese version of the scale was revised in a population of middle school students and showed good reliability.34 The SCS is scored on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). The sum of the scores of each item is the total score, and higher scores indicate that individuals tend to hide their negative or painful information.
Distress Disclosure Index (DDI)
The DDI consists of 12 items in a one-dimensional structure (eg, “When I feel depressed or sad, I tend to keep those feelings to myself”).39 The DDI is a 5-point scoring scale ranging from 1 (strongly disagree) to 5 (strongly agree). The sum of the scores of each item is the total score, and higher scores indicate that individuals are less likely to hide psychological distress and more inclined to disclose it proactively. The Cronbach’s α coefficient for the scale in this study was 0.86.
Revised Cheek and Buss Shyness Scale (RCBS)
The RCBS consists of 13 items structured in a single dimension (eg, “I am often uncomfortable at parties and other social functions”).40 The scale is scored on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). The sum of the item scores is the total score, and higher scores indicate that individuals are shyer and more sensitive to unfamiliar situations. The Cronbach’s α coefficient for the scale in this study was 0.82.
Social Interaction Anxiety Scale (SIAS) and Social Phobia Scale (SPS)
The Chinese versions of the SIAS and SPS scales were selected as survey instruments for the study.41 The total scale consists of 12 items, of which 6 items are used to measure an individual’s level of anxiety in social interactions (eg, “Tense up if meet acquaintance in street”), and the other 6 items are used to measure an individual’s level of fear of socialization (eg, “Self-conscious to eat in front of stranger”). Both the SIAS and the SPS adopt a 5-point scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The sum of the item scores is the total score, with higher scores indicating higher levels of social anxiety and social fear in individuals. The Cronbach’s α coefficients for the SIAS and SPS in this study were 0.89 and 0.92, respectively.
UCLA Loneliness Scale (ULS-8)
The ULS-8 consists of 8 items in a single-dimensional structure (eg, “I am unhappy being so withdrawn”).42 The scale is scored on a 4-point scale ranging from 1 (never) to 4 (always). The sum of the scores of each item is the total score, and the higher the score, the higher the level of loneliness experienced by the individual. The Cronbach’s α coefficient for the scale in this study was 0.80.
Kessler Psychological Distress Scale (K10)
The Chinese version of K10 consists of 10 items categorized into two dimensions: anxiety and depression (eg, “you feel tired out for no good reason”).43 The scale is scored on a 5-point scale ranging from 1 (all the time) to 5 (hardly ever). The sum of the scores for each item is the total score, with higher scores indicating that individuals are at higher risk of developing mental illness and poorer mental health. The Cronbach’s α coefficients for the total scale and the anxiety and depression dimensions in this study were 0.94, 0.86, and 0.90, respectively.
Statistical Analysis
The data from Sample 1 were subjected to item analysis and exploratory factor analysis using SPSS 20.0. In item analysis, the critical ratio value method, item-total correlation, and Cronbach’s α coefficient test were used to examine the differentiation and homogeneity of the items.44 Exploratory factor analysis was used to explore the factor structure of the SCS. Principal axis factor analysis was used for factor extraction. Also, oblique rotation was performed using the Promax method.45 The final number of factors was determined with eigenvalues greater than 1 and combined with the scree plot.46
The data from Sample 2 were subjected to confirmatory factor analysis, criterion-related validity, reliability and cross-group consistency tests using SPSS 20.0 and AMOS 24.0. The correlations between the SCS and each validity scale instrument were calculated using Pearson correlation analysis. The Cronbach’s α coefficient and split-half reliability of the scale were used as indicators to assess reliability. If the value of the reliability coefficient was greater than 0.70, the reliability was good.47 In addition, the study further conducted a cross-group consistency analysis to examine the equivalence of the SCS in different gender groups of older adults. The study constructed Configural Invariance Model (M1), Weak Invariance Model (M2), Strong Invariance Model (M3), and Strict Invariance Model (M4) respectively.48 A ∆CFI and ∆RMSEA of less than 0.01 were used as criteria for determining that the SCS had cross-gender invariance.49 On the basis of the gender equivalence test, the study took an independent samples t-test to analyze the data from the full sample to examine gender differences in self-concealment.
Results
Item Analysis
Table 1 shows the means and standard deviations of the individual items. The results of the independent samples t-test showed that the items differed significantly (p < 0.001) on the high and low subgroups. The results of the correlation analysis showed that the correlation coefficients between the items and the total score ranged from 0.71 to 0.78. In addition, the Cronbach’s α coefficient of the scale was 0.911. After deleting any of the items, the Cronbach’s α coefficient value of the scale decreased to varying degrees (0.900 to 0.904). Based on the criteria for item analysis, all items were retained at that stage.
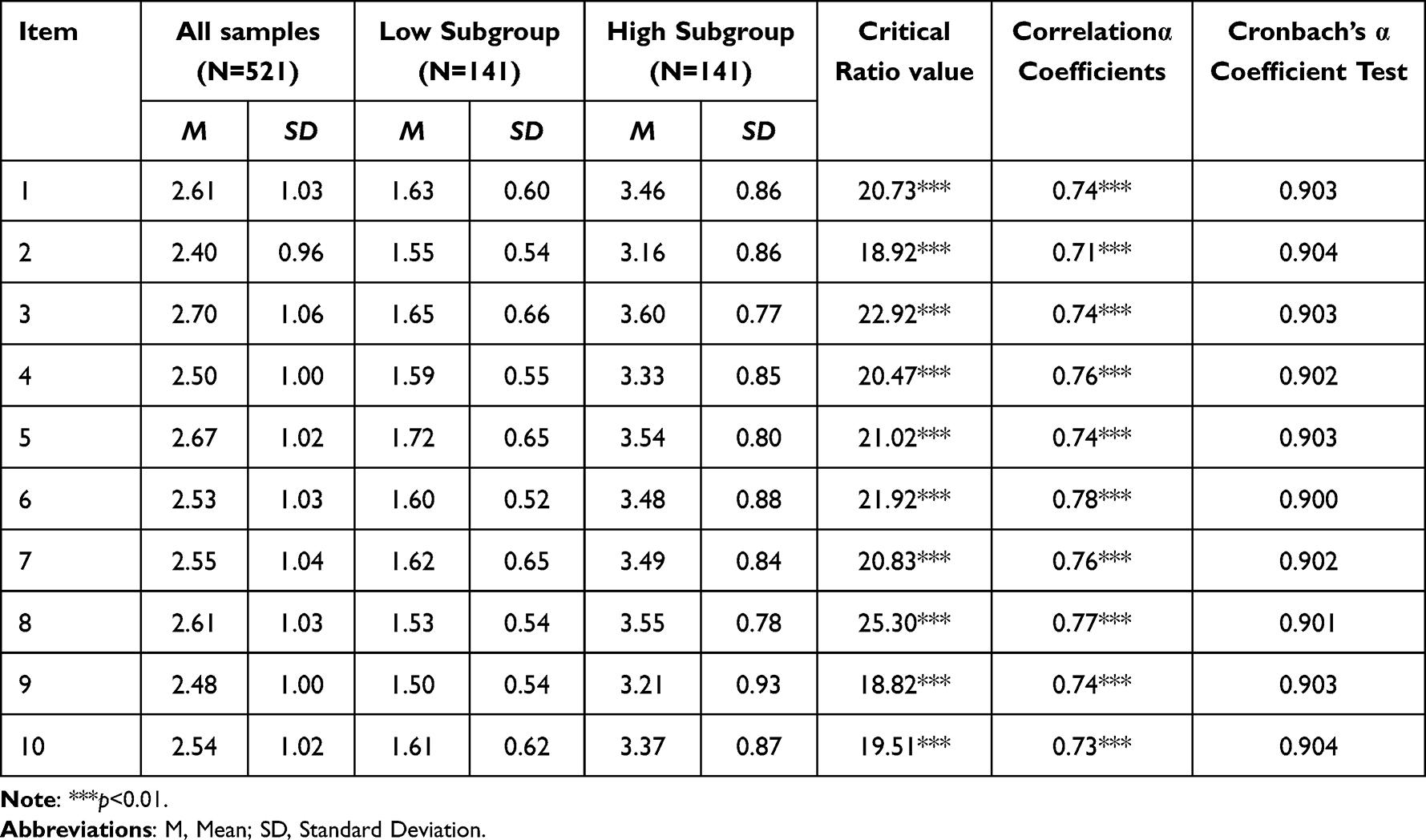 |
Table 1 The Result of the Item Analysis of SCS |
Exploratory Factor Analysis
Before exploratory factor analysis, the KMO value of the scale needed to be tested. The results showed that the KMO value of SCS was 0.931 and the Bartlett’s test of sphericity was 2616.14 (df=45, p<0.001). The results of exploratory factor analysis are shown in Table 2. A factor with an eigenvalue greater than 1 is extracted, with a variance explained of 55.66%. Combined with the scree plot, the extraction of 1 factor was reasonable. All the items met the retention criteria, in which the factor loading values of each item ranged from 0.68 to 0.75, and the communality ranged from 0.46 to 0.57.
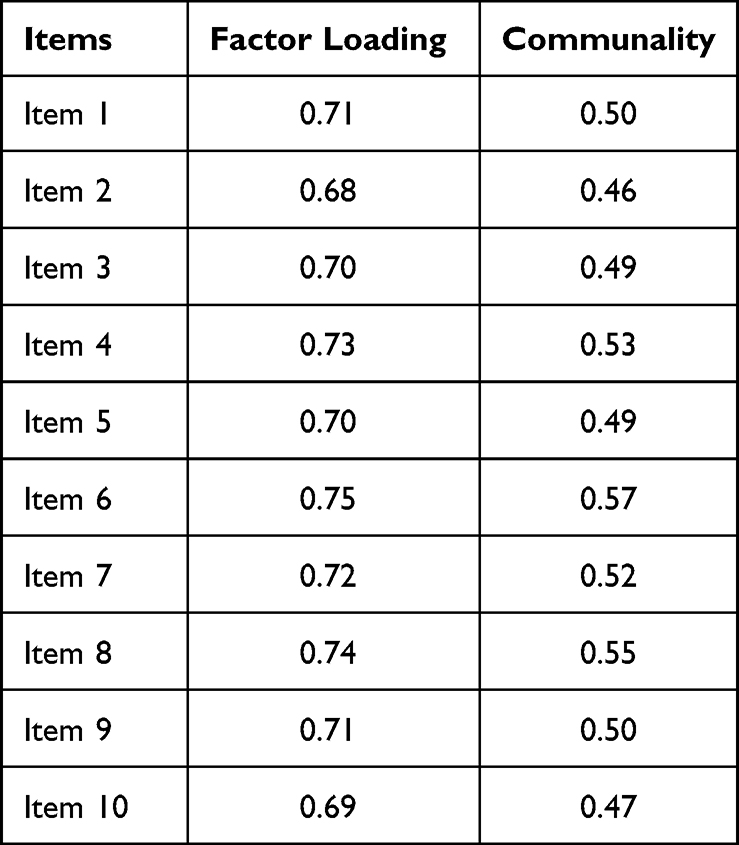 |
Table 2 The Result of the Exploratory Factor Analysis of SCS (N=521) |
Confirmatory Factor Analysis (CFA)
The results of the confirmatory factor analysis showed a good fit of the one-factor model with fit indices of χ2/df=2.829, RMSEA=0.057, CFI=0.981, IFI=0.981, TLI=0.974, PNFI=0.712, and PGFI=0.719.
Criterion Association Validity Test
The results of correlation analysis showed (see Table 3) that SCS was significantly and positively correlated with RCBS, SIAS, SPS, ULS-8, K10, depression, and anxiety (r=0.41 to 0.59); SCS was significantly and negatively correlated with DDI (r=−0.39).
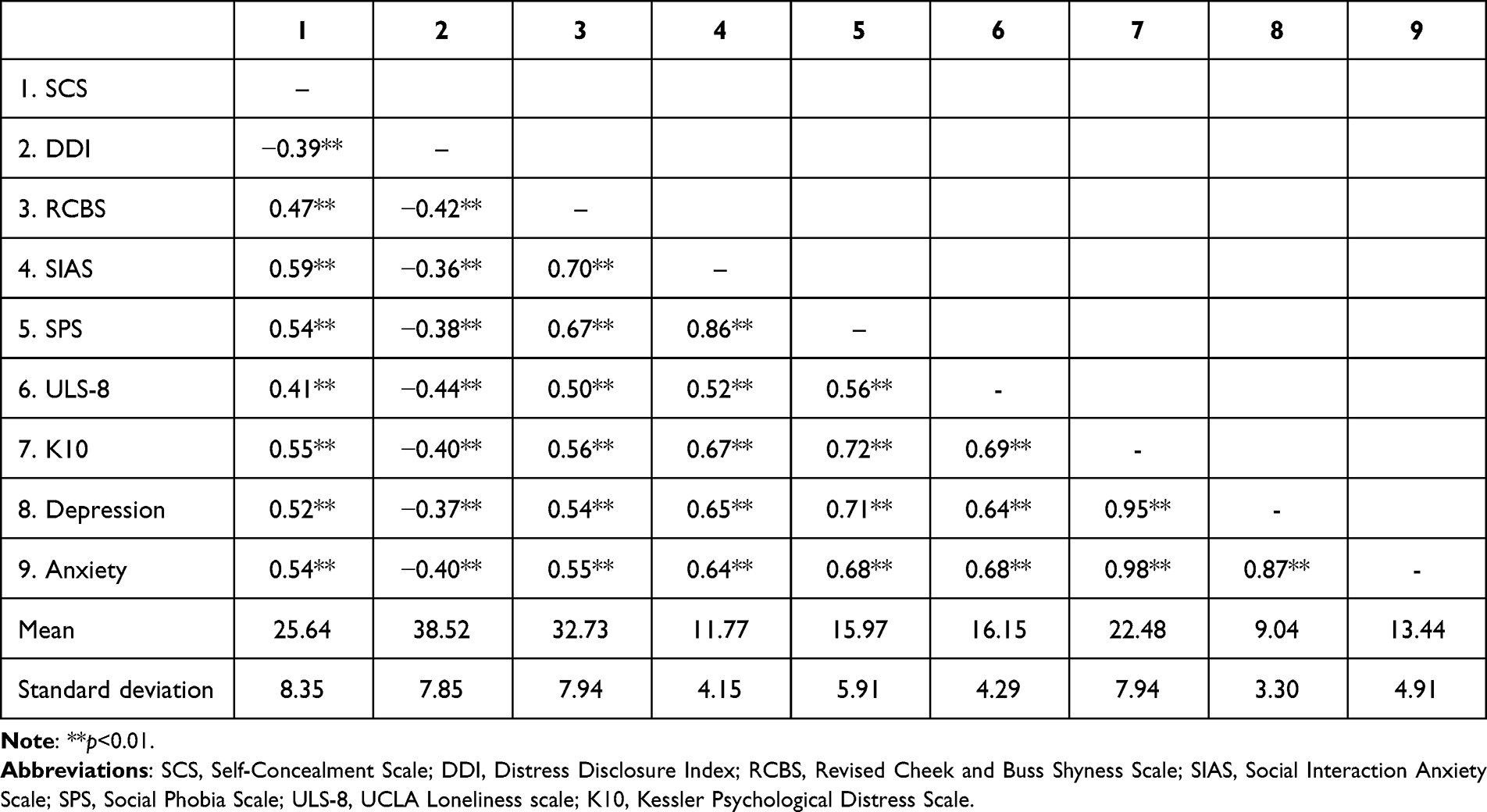 |
Table 3 The Result of the Criterion Association Validity Test of SCS (N=564) |
Reliability Test
The Cronbach’s α coefficient value for SCS was 0.923. The split-half reliability was calculated by adopting the odd-even split. The result revealed that the Spearman-Brown coefficient value was 0.923 both the Cronbach’s α coefficient value and the split-half reliability were above the criterion of 0.70.
Cross-Gender Consistency Test
The research constructed Configural Invariance Model (M1), Weak Invariance Model (M2), Strong Invariance Model (M3), and Strict Invariance Model (M4). Compared to M1, M2 set the factor loadings equal; compared to M2, M3 continued to set the intercepts equal; and compared to M3, M4 continued to set the residuals equal. The results show (see Table 4) that the four models have good fit indices and can be compared for cross-group consistency. In the comparison between M2 and M1, ∆CFI and ∆RMSEA are 0.001 and −0.004, respectively, indicating that the weak equivalence model holds; in the comparison between M3 and M2, ∆CFI and ∆RMSEA are −0.0008 and −0.003, respectively, indicating that the strong equivalence model holds; in the comparison between M4 and M3, ∆CFI and ∆RMSEA are −0.001 and −0.002, indicating that the strict equivalence model holds. The establishment of the above four models suggests that SCS is consistent across genders.
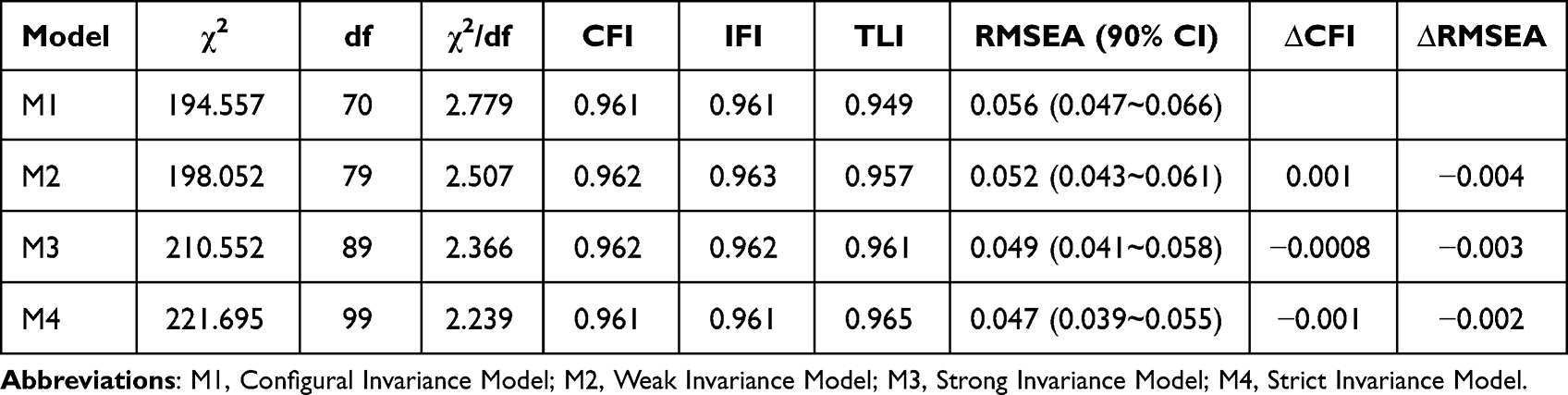 |
Table 4 The Result of the Cross-Gender Consistency Test of SCS (N=564) |
The study further examined gender variance in self-concealment. The results showed that the difference between males (25.63±7.78) and females (25.62±8.20) on the total self-concealment score was not significant (t=0.03, p=0.98)
Discussion
The objective of this study was to investigate the psychometric features of the Self-Concealment Scale (SCS) in Chinese older adults, to provide an effective tool for quantitative research and intervention practice of self-concealment among older people. The Self-Concealment Scale (SCS) was found to have good reliability and validity in the Chinese elderly population, and can be used as a valid tool to assess the tendency of older people to conceal negative or painful information.
Discussion of SCS Factor Structure
In the exploratory factor analysis, no items were removed and only one dimension was extracted. The results of the confirmatory factor analysis showed that the one-factor model was well fitted. The exploration of the dimensional structure of the SCS has always been a key concern of scholars. A total of two dimensions were explored in the study by Larson et al. However, considering that the SCS is essentially unidimensional and the first factor explains more than 65% of the total variance, so it is concluded that the scale should be single-dimensional.
In other related studies, consistent conclusions have been reached. Wismeijer et al adopted two approaches of principal components analysis (PCA) and Mokken scale analysis (MSA) to examine the factor structure of SCS.50 Both PCA and MSA explored a two-factor structure comprising of a two-factor structure consisting of strong factor and weak factor. However, PCA and MSA differed significantly in the number of items and attributions across dimensions, whereas both showed consistency in the one-factor structure. Therefore, Wismeijer et al concluded that SCS should be a one-dimensional structure.
This result is consistent with Larson et al and is also supported by some empirical evidence. For example, Cramer and Barry explored two dimensions in their study of Canadian university students, where the first dimension explained 44.3% of the total variance and the second dimension explained a low percentage of the total variance (11.0%). In a further confirmatory factor analysis, it was observed that the single dimensional structure was most comprehensive, efficient and parsimonious. The above study was conducted with an adolescent population, and the present study reached similar conclusions in older adults, ie, the SCS is a single dimensional structure. However, in contrast, the present study did not explore two dimensions, but only one.
The results of this study are also supported by some evidence. For instance, in an exploratory factor analysis of the Turkish version of the SCS, only one dimension was explored, explaining 43.76% of the total variance.32 In a revision of the Chinese version of the SCS in a population of secondary school students, only one factor was also extracted but explained only 33.37% of the total variance.34 In the present study, the explanation rate of the first factor was found to be 55.66%, which was slightly higher than the two studies mentioned above.
Of concern is that self-concealment is thought to be composed of three components, namely (1) the tendency to keep secrets to oneself, (2) having painful secrets or negative thoughts about oneself that are rarely or never shared with others, and (3) fear of privacy disclosure.3 Some scholars have pointed out that the single dimension structure does not reflect all the connotations of self-concealment and is inconsistent with the multidimensional structure of self-concealment, and that there is a necessity to revise and improve it.50 In addition, there are also studies which found that some of the scale’s items do not measure the individual’s self-concealing behaviors and feelings or are not private and secretive, and need to be removed.33 Therefore, whether the single dimension structure is an optimal solution for SCS still requires more research to validate this.
Discussion on SCS Criterion Validity and Reliability
The results of criterion validity analysis showed that the total SCS score was significantly positively correlated with the RCBS, SIAS, SPS, ULS-8, and K10 scores, and significantly negatively correlated with the DDI score. In other words, older adults with high SCS have higher shyness, social anxiety, social phobia, and loneliness experiences, are less likely to express their distress to others, as well as suffer from poorer mental health. This finding not only indicates that SCS has good validity, but also helps to better understand the effects of self-concealment on individuals, which is a stable personality trait that reflects the tendency of individuals to keep negative information about themselves from other people.
Self-Determination Theory Can Better Explain the Relationship Between SCS and Criterion Tools
Uysal et al, from the perspective of self-determination theory, argued that self-concealment can jeopardize an individual’s basic psychological needs such as sense of competence, autonomy, and relatedness, as well as one’s sense of happiness.51 The results of the present study support this view, finding that elderly people with high self-concealment need to constantly repress their thoughts, which undermines their connection with others, thus negatively affecting their psychological well-being. In addition, it was found that the Cronbach’s α coefficient and split-half reliability of the SCS exceeded 0.70, indicating that the scale has favorable internal consistency.
Discussion on Cross-Gender Consistency and Gender Differences of SCS
One very significant finding of this study is that SCS shows invariance among elderly people of different genders. The establishment of the four models, namely the morphological equivalence model, the weak equivalence model, the strong equivalence model, and the strict equivalence model, suggests that the SCS is equal in terms of the number of items and attributions, the factor loadings of the items, the intercepts, and the residuals among the elderly of different genders. Only if the SCS is consistent across genders, the between-group comparison is meaningful for measurement.52
On this basis, the study further conducted an analysis of variance, which showed that the differences in SCS scores among older people of different genders were not significant. In previous studies on gender differences in self-concealment, the results have been inconsistent. For instance, in Ritz and Dahme’s study of college students, it was found that there was no significant gender difference in self-concealment.53 In contrast, in a study by Wang et al, it was concluded that men had higher levels of self-concealment than women.34 In addition, in Cramer et al’s study 1, it was found that males had a higher level of self-concealment than females, whereas no significant gender difference was found in their study 2.31 The discrepancies in the results of different studies may be attributed to a number of reasons. For example, the characteristics of the individual and the person with whom he or she interacts, the degree of relationship between the two, and the type and level of social support perceived by the individual.7,54
This study’s results are in line with some of the previous studies. In Wang et al’s study, the reason for the higher level of self-concealment among male college students than females was attributed to the fact that males have higher independence and lower dependence. However, older adults show different characteristics in self-concealment than young adults. As individuals age, self-concealment declines.55 Regardless of gender, older adults have a high level of dependence on social support from family and other sources for care and assistance.56 Particularly for older adults with advanced age, poor health, and disabilities, the dependence on others is higher.57 Furthermore, most older adults also agree that maintaining positive interactions and communication with caregivers and expressing their feelings in a timely manner can help to obtain more emotional support and daily care.58,59 This may be a potential reason why gender differences in self-concealment among older adults are not significant.
The Theoretical Significance and Practical Value of the Research
The study has certain theoretical significance and practical value. Based on the analysis of existing literature, it is evident that this study represents the first time to test the psychometric properties of the SCS in an elderly population and found it to have good reliability and validity. The findings suggest that the SCS is a valid tool as an assessment of self-concealment tendencies in the elderly, which can provide instrumental support for the development of related research and can also be used for the identification, diagnosis, and intervention of self-concealment in older people. To ensure the achievement of the goal of active aging, it is necessary to carry out large-scale screening of self-concealment of older adults, identify key groups of concern, and take effective interventions.
An important contribution to this study examines the cross-gender invariance of SCS. The results of this study provide a tool to explore the gender gap of self-concealment. Furthermore, the study examined the impact of self-concealment on the psychology and behavior of the older people, which contributes to a better understanding of the negative impact of individual self-concealment on interpersonal interactions and mental health. Also, the findings validate the applicability of self-determination theory in explaining self-concealment, which enriches related theories.
Limitations and Future Research
There are some limitations of this study that should not be ignored. First, the study analyzed the reliability and validity of the SCS based only on cross-sectional questionnaire results and did not examine the retest reliability of the scale. In future studies, longitudinal studies need to be taken to examine the stability of the scale across time. Second, the study adopted convenience sampling and snowball sampling, resulting in an underrepresentative sample. Further evidence is needed on the applicability of the study findings to older adults in other regions. Moreover, traumas, insecure attachment orientations, and dispositional social-evaluative concerns were noted as antecedent variables of self-concealment in a study by Larson et al.7 This suggests that older adults with different upbringing and psychological characteristics may differ in the degree and content of self-concealment. Therefore, the validity of the scale needs to be examined in future studies in a population of older people with different characteristics.
Third, the study subjects were predominantly Han Chinese and included only a small number of participants from ethnic minorities. Previous research has found that cultural values can influence the development of individual self-concealment.60 Therefore, it is unclear whether the findings are applicable to the older adults in other ethnic or cultural contexts. Fourth, the development of Internet technology has expanded older adults’ social networks and increased interpersonal communication pathways. There is evidence that individuals do not have the same tendency to self-conceal in online social platforms and real interpersonal interactions.61 Therefore, the development of a social network self-concealment scale for older adults could be considered in future research. Fifth, self-concealment is a complex concept that may include different dimensions and structures. In future studies, qualitative research can be taken to analyze the internal structure of self-concealment in older adults to better define this concept.
Conclusion
Self-concealment in the older population has seen a negative impact on their physical health, mental health, interpersonal relationships, and quality of life. For this reason, it is imperative to examine the psychometric properties of the SCS among older adults so as to provide a valid tool for the development of relevant research and practice. The results of the study emphasize that the SCS is a reliable and valid tool for assessing self-concealment of older adults. Moreover, the scale has concise and easy-to-use properties that make it suitable for large-scale surveys and studies.
Ethics
Approved by the Jilin International Studies University (Approval No. JY202211003).
Funding
This study was under the Social Sciences Planning Project Supported by Jilin Province (No. 2022C86) and National College Students’ Innovation and Entrepreneurship Training Program (No. 202210199057).
Disclosure
The authors declare no conflicts of interest.
References
1. Davis CG, Brazeau H. Factors promoting greater preoccupation with a secret. Br J Soc Psychol. 2021;60(4):1419–1435. doi:10.1111/bjso.12462
2. Cruddas S, Gilbert P, Mcewan K. The relationship between self-concealment and disclosure, early experiences, attachment, and social comparison. Int J Cogn Ther. 2012;5(1):28–37. doi:10.1521/ijct.2012.5.1.28
3. Larson D, Chastain R. Self-concealment: conceptualization, measurement, and health implications. J Soc Clin Psychol. 1990;9(4):439–455. doi:10.1521/jscp.1990.9.4.439
4. Davis CG. Self-concealment, secrecy, and guilt. J Pers. 2023. doi:10.1111/jopy.12832
5. Edmonds J, Masuda A, Tully EC. Relations among self-concealment, mindfulness, and internalizing problems. Mindfulness. 2014;5(5):497–504. doi:10.1007/s12671-013-0204-z
6. Uysal A, Lin HL, Bush AL. The reciprocal cycle of self‐concealment and trust in romantic relationships. Eur J Soc Psychol. 2012;42(7):844–851. doi:10.1002/ejsp.1904
7. Larson DG, Chastain RL, Hoyt WT, Ayzenberg R. Self-concealment: integrative review and working model. J Soc Clin Psychol. 2015;34(8):705–774. doi:10.1521/jscp.2015.34.8.705
8. D’Agata MT, Holden RR. Self-concealment and perfectionistic self-presentation in concealment of psychache and suicide ideation. Pers Individ Dif. 2018;125:56–61. doi:10.1016/j.paid.2017.12.034
9. Hogge I, Blankenship P. Self‐concealment and suicidality: mediating roles of unmet interpersonal needs and attitudes toward help‐seeking. J Clin Psychol. 2020;76(10):1893–1903. doi:10.1002/jclp.22964
10. Zhou G, Wang E. Effects of self-concealment and self-esteem on Internet addiction in college students. Soc Behav Person. 2021;49(7):1–9. doi:10.2224/sbp.10370
11. Chung MC, Ye Z, Wang N, Thomas J. Linking posttraumatic stress disorder with eating disorders among Emirati university female students: the role of self-concealment. Current Psycholog. 2021. doi:10.1007/s12144-021-01391-6
12. Chinweuba DC, Ifeagwazi CM, Chinweuba AU, Chukwuorji JC. Does self-concealment and self-compassion differentially influence substance use for male versus female adolescents? J Subst Use. 2023;28(1):117–122. doi:10.1080/14659891.2021.2018726
13. Koszalinski RS, Olmos B. Communication challenges in social isolation, subjective cognitive decline, and mental health status in older adults: a scoping review (2019–2021). Perspect Psychiatr Care. 2022;58(4):2741–2755. doi:10.1111/ppc.13115
14. Sease TB, Perkins DR, Sandoz EK, Sudduth H. Automatic thoughts: understanding the precursors of self-concealment within the psychological flexibility framework. J Context Behav Sci. 2021;22:68–73. doi:10.1016/j.jcbs.2021.09.008
15. Maas J, Wismeijer AAJ, Van assen MALM. Associations between secret-keeping and quality of life in older adults. Int J Aging Hum Dev. 2019;88(3):250–265. doi:10.1177/0091415018758447
16. Lyons KS, Sadowski T, Lee CS. The role of concealment and relationship quality on patient hospitalizations, care strain and depressive symptoms in heart failure dyads. Eur J Cardiovasc Nurs. 2020;19(2):118–124. doi:10.1177/1474515119863791
17. Friedlander A, Nazem S, Fiske A, Nadorff MR, Smith MD. Self-concealment and suicidal behaviors. Suicide Life Threat Behav. 2012;42(3):332–340. doi:10.1111/j.1943-278X.2012.00094.x
18. Chasteen A, Bashir N, Gallucci C, Visekruna A. Age and antiaging technique influence reactions to age concealment. J Gerontol B Psychol Sci Soc Sci. 2011;66(6):719–724. doi:10.1093/geronb/gbr063
19. Cecil V, Pendry L, Ashbullby K, Salvatore J. Masquerading their way to authenticity: does age stigma concealment benefit older women? J Women Aging. 2022;1–18. doi:10.1080/08952841.2022.2128245
20. Maas J, Wismeijer AAJ, Van Assen MALM, Aquarius AEAM. Is it bad to have secrets? Cognitive preoccupation as a toxic element of secrecy. Int J Clin Health Psychol. 2012;12(1):23–37.
21. Wertheim R, Hasson-Ohayon I, Mashiach-Eizenberg M, Pizem N, Shacham-Shmueli E, Goldzweig G. Self-concealment among couples who cope with chronic illness: development and preliminary validation of the Couples Illness Self-Concealment (CISC) questionnaire. Support Care Cancer. 2016;24(12):4951–4959. doi:10.1007/s00520-016-3354-4
22. de la Piedra-Torres AJ, López-Martínez AE, Ramírez-Maestre C. Information concealment in palliative patients: development and pilot study of a new scale for caregivers. Health Soc Care Community. 2022;30(6):e4504–e4512. doi:10.1111/hsc.13854
23. Jewett LR, Malcarne VL, Kwakkenbos L, et al. Development and Validation of the Body Concealment Scale for Scleroderma (BCSS). Arthritis Care Res. 2016;68(8):1158–1165. doi:10.1002/acr.22819
24. Yeatts PE, Abbott DM, Mollen D. Development and evaluation of the atheist identity concealment scale (aics). J Relig Health. 2021;61(4):3525–3541. doi:10.1007/s10943-021-01465-6
25. Aydemir N, Kaya B, Yıldız G. Development of the perceived stigma scale and the concealment of epilepsy scale for the Turkish population. Epilepsy Behav. 2018;80:1–4. doi:10.1016/j.yebeh.2017.11.032
26. Geng Y, Zhan T, Zhang Y, Shi L, Yu J, Jin W. Why don’t you tell me? The mediating role of self-concealment in the relationship between Machiavellianism and break-up distress. Curr Psychol. 2023;42(20):17000–17007. doi:10.1007/s12144-022-02911-8
27. Sease TB, Perkins DR, Yang Y. The influence of emotion dysregulation on the relationship between emotional abuse and self-concealment among romantic partners. J Aggress Maltreat Trauma. 2021. doi:10.1080/10926771.2021.1921088
28. Kealy D, Rice SM. Dispositional connectedness and depressive symptoms among help-seeking outpatients: the mediating role of self-concealment. Eur J Psychiatry. 2020;34(4):219–222. doi:10.1016/j.ejpsy.2020.07.002
29. Nam B, Kim J, Ryu W, Kim DI, Frey JJ, DeVylder J. Perceived social stigma, self-concealment, and suicide risk among North Korean refugee women exposed to traumatic events. Suicide Life Threat Behav. 2021;51(6):1235–1246. doi:10.1111/sltb.12805
30. Chung MC, Chen ZS, Han BX. The impact of anger and self-concealment on post-traumatic stress and psychiatric comorbid symptoms in Chinese prisoners: a longitudinal study. Crim Behav Ment Health. 2022;32(5):320–336. doi:10.1002/cbm.2257
31. Cramer KM, Barry JE. Psychometric properties and confirmatory factor analysis of the Self-Concealment Scale. Pers Individ Dif. 1999;27(4):629–637. doi:10.1016/S0191-8869(98)00222-0
32. Deniz M, Cok F. Psychometric properties and adaptation of the Self-Concealment Scale to the Turkish Adolescents. Lköretim Online. 2010;9:424–432.
33. Salinas-Oñate N, Baeza-Rivera MJ, Salinas-Rehbein B, Escandón-Nagel N, Escobar-Alaniz B. Validation of the Adapted Version of the Larson & Chastain Self-Concealment Scale in Chilean University Students. Rev Iberoam Diagn Ev. 2022;62(1):51. doi:10.21865/RIDEP62.1.05
34. Wang CK. The factor structure of the Chinese adaptation of self-concealment scale in middle school students. Chin J Appl Psychol. 2002;8(2):15–17.
35. Luoma JB, Chwyl C. Interpersonal mechanisms for the maintenance of self-criticism: expressive suppression, emotion expression, and self-concealment. Curr Psychol. 2022;41(6):4027–4040. doi:10.1007/s12144-020-00920-z
36. Ichiyama MA, Colbert D, Laramore H, Heim M, Carone K, Schmidt J. Self-concealment and correlates of adjustment in college students. J College Stud Psychother. 1993;7(4):55–68. doi:10.1300/J035v07n04_05
37. Zhou S, King EJ, Gjorgiovska J, Mihajlov A, Stojanovski K. Self-concealment, discrimination, and mental health in Macedonia: disparities experienced by sexual and gender minorities. Glob Public Health. 2019;14(8):1075–1086. doi:10.1080/17441692.2018.1560484
38. Simms LJ. Classical and modern methods of psychological scale construction. Soc Personal Psychol Compass. 2008;2(1):414–433. doi:10.1111/j.1751-9004.2007.00044.x
39. Kahn JH, Hessling RM. Measuring the tendency to conceal versus disclose psychological distress. J Soc Clin Psychol. 2001;20(1):41–65. doi:10.1521/jscp.20.1.41.22254
40. Hopko DR, Stowell J, Jones WH, Armento MEA, Cheek JM. Psychometric properties of the revised cheek and Buss Shyness Scale. J Pers Assess. 2005;84(2):185–192. doi:10.1207/s15327752jpa8402_08
41. Fergus TA, Valentiner DP, McGrath PB, Gier-Lonsway SL, Kim HS. Short forms of the Social Interaction Anxiety Scale and the Social Phobia Scale. J Pers Assess. 2012;94(3):310–320. doi:10.1080/00223891.2012.660291
42. Hays RD, DiMatteo MR. A short-form measure of loneliness. J Pers Assess. 1987;51(1):69–81. doi:10.1207/s15327752jpa5101_6
43. Bougie E, Arim RG, Kohen DE, Findlay LC. Validation of the 10-item Kessler Psychological Distress Scale (K10) in the 2012 Aboriginal Peoples Survey. Health Rep. 2016;27(1):3–10.
44. Gehlbach H, Brinkworth ME. Measure twice, cut down error: a process for enhancing the validity of survey scales. Rev General Psychol. 2011;15(4):380–387. doi:10.1037/a0025704
45. Worthington RL, Whittaker TA. Scale development research: a content analysis and recommendations for best practices. Couns Psychol. 2006;34(6):806–838. doi:10.1177/0011000006288127
46. Fabrigar LR, Wegener DT, MacCallum RC, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. Psychol Methods. 1999;4(3):272–299. doi:10.1037/1082-989X.4.3.272
47. Viladrich C, Angulo-Brunet A, Doval E. A journey around alpha and omega to estimate internal consistency reliability. Anal de Psicologia. 2017;33(3):755–782. doi:10.6018/analesps.33.3.268401
48. Dimitrov DM. Testing for factorial invariance in the context of construct validation. Measure Eval Counsel Dev. 2010;43(2):121–149. doi:10.1177/0748175610373459
49. Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equat Model. 2002;9(2):233–255. doi:10.1207/S15328007SEM0902_5
50. Wismeijer AAJ, Sijtsma K, Van Assen MALM, Vingerhoets AJJM. A comparative study of the dimensionality of the self-concealment scale using principal components analysis and mokken scale analysis. J Pers Assess. 2008;90(4):323–334. doi:10.1080/00223890802107875
51. Uysal A, Lee Lin H, Raymond Knee C. The role of need satisfaction in self-concealment and well-being. Pers Soc Psychol Bull. 2010;36(2):187–199. doi:10.1177/0146167209354518
52. Schmitt N, Kuljanin G. Measurement invariance: review of practice and implications. Hum Resource Manag Rev. 2008;18(4):210–222. doi:10.1016/j.hrmr.2008.03.003
53. Ritz T, Dahme B. Repression, self-concealment and rationality/emotional defensiveness: the correspondence between three questionnaire measures of defensive coping. Pers Individ Dif. 1996;20(1):95–102. doi:10.1016/0191-8869(95)00142-S
54. Akdoğan R, Çimşir E. Linking inferiority feelings to subjective happiness: self-concealment and loneliness as serial mediators. Pers Individ Dif. 2019;149:14–20. doi:10.1016/j.paid.2019.05.028
55. Masuda A. Examining self-concealment within the framework of psychological inflexibility and mindfulness: (538602014-001); 2014. doi:10.1037/e538602014-001
56. Minayo MCDS, Mendonça JMB, Sousa GSD, Pereira TFDS, Mangas RMDN. Support policies for dependent older adults: Europe and Brazil. Ciênc saúde coletiva. 2021;26(1):137–146. doi:10.1590/1413-81232020261.30262020
57. Sunde OS, Alteren J, Ytrehus S. Caring for a home-dwelling older parent with mental health problems: a narrative analysis of family caregivers’ experiences. Int J Qual Stud Health Well-Being. 2023;18(1):2236373. doi:10.1080/17482631.2023.2236373
58. Hirschman KB, Rivera E, Sefcik JS, et al. Older adult and family caregiver perspectives on engagement in primary care. J Gerontol Nurs. 2022;48(11):7–13. doi:10.3928/00989134-20221003-02
59. Walker R, Newman L, Tsianikas M, Panagiotopoulos G, Hurley C. The perspectives of older Greek-Australians toward changes in the nature of family support: implications for family care policies. J Aging Soc Policy. 2013;25:320–334. doi:10.1080/08959420.2013.816194
60. Wallace BC, Constantine MG. Africentric cultural values, psychological help-seeking attitudes, and self-concealment in African American College Students. J Black Psychol. 2005;31(4):369–385. doi:10.1177/0095798405281025
61. Trub L. A portrait of the self in the digital age: attachment, splitting, and self-concealment in online and offline self-presentation. Psychoanalytic Psychol. 2017;34(1):78–86. doi:10.1037/pap0000123
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Validity and Reliability of the Thai Version of the 19-Item Compliance-Questionnaire-Rheumatology
Panichaporn S, Chanapai W, Srisomnuek A, Thaweeratthakul P, Katchamart W
Patient Preference and Adherence 2022, 16:2149-2158
Published Date: 17 August 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Development and Initial Validity of the Patients’ Literacy Scale Among Outpatients in Hangzhou City, China
Jiang D, Sang T, Xiao X, Wu Z, Wang H, Yang Q
Patient Preference and Adherence 2022, 16:2483-2496
Published Date: 7 September 2022
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023