Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Relative Hypoglycemia is Associated with Delirium in Critically Ill Patients with Diabetes: A Cohort Study
Authors Zhao H, Ying HL, Zhang C, Zhang S
Received 8 April 2022
Accepted for publication 20 September 2022
Published 29 October 2022 Volume 2022:15 Pages 3339—3346
DOI https://doi.org/10.2147/DMSO.S369457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Hui Zhao, Hua-Liang Ying, Chao Zhang,* Shaohua Zhang*
Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Zhang; Shaohua Zhang, Intensive Care Unit (ICU), Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, No. 1 Tong-yang Road, Taizhou, People’s Republic of China, Tel +8613757602063 ; +8615268325868, Email [email protected]; [email protected]
Purpose: Critically ill patients with premorbid diabetes can suffer from relative hypoglycemia (RHG), falling below the normal blood glucose (BG) target. However, these events have not been well defined or studied. In the present study, we aimed to explore the incidence and clinical significance of RHG events in critically ill patients with diabetes.
Patients and methods: Patients with a history of diabetes who stayed in the intensive care unit (ICU) for more than three days with at least 12 BG recordings were retrospectively included in the study. A BG level > 30% below the estimated average according to patient hemoglobin A1c measured at admission was defined as a single RHG event. Outcomes were compared between patients with and those without RHG events.
Results: In total, 113 patients were included in the final analysis. RHG was detected in 73 patients (64.6%). Those who experienced RHG events had a significantly higher incidence of ICU delirium. They also had a higher risk of 28-day mortality, but this was not statistically significant. However, patients with a higher frequency of RHG events did have a significantly higher risk of overall mortality (57.1% for more than four events vs 15.4% for three to four events, P=0.006 and 15.1% for one to two events, P=0.003).
Conclusion: In conclusion, RHG is a common finding in critically ill patients with diabetes and is associated with mortality and the occurrence of delirium.
Keywords: relative hypoglycemia, delirium, diabetes, intensive care unit patients
Introduction
Delirium is a common neurological disease; it is characterized by a disturbance of consciousness and change in cognition,1,2 and it is frequently observed in patients in the intensive care unit (ICU). The prevalence of delirium in a medical ICU was recently reported as 28.6% in a Swiss university hospital.3 Numerous studies have demonstrated risk factors for the development of delirium in the ICU, such as age,4 type of coma,5 and length of ICU stay.6 To improve the prognosis of patients in the ICU, risk factors need to be further explored.
Frequent measurement of blood glucose (BG) levels has been the standard of care in the ICU, with the aim of avoiding persistent hyperglycemia and hypoglycemia. In a pioneering study conducted by van den Berghe et al, the maintenance of BG levels at or below 110 mg/dL was shown to benefit critically ill patients, as evidenced by a lower morbidity and mortality.7 However, subsequent studies, such as the Normoglycemia in Intensive Care Evaluation and Survival Using Glucose Algorithm Regulation (NICE-SUGAR) study, showed that intensive insulin therapy could lead to a significant increase in mortality, which could be attributed to the occurrence of severe hypoglycemic events following intensive glucose control.8 Moreover, Krinsley et al showed that even mild hypoglycemia, defined as BG < 70 mg/dL, was associated with a significantly increased risk of mortality in a cohort of critically ill patients.9
A controversy remains regarding the association between hypoglycemia and the occurrence of delirium among patients in ICU. Hypoglycemia has been shown to be positively associated with delirium in critically ill patients with diabetes;10 however, another study indicated that no direct relationship exists between hypoglycemia and the occurrence of delirium.11 Relative hypoglycemia (RHG) is defined as a 30% reduction in BG from the estimated average BG baseline, and this 30% reduction corresponds to the change from normoglycemia to hypoglycemia,12,13 which triggers a hypoglycemic stress response (increased glucagon and adrenaline secretion) in patients without diabetes.14 Given the involvement of hypoglycemia in the development of RHG, the aim of this study was to explore the incidence of RHG using a standard definition based on the glycated hemoglobin level (A1c) obtained at admission in a mixed ICU. Moreover, we investigated the correlation between RHG and the clinical outcomes of the study patients.
Methods
Patients
All adult patients who were admitted to the Department of Critical Care Medicine, Taizhou Hospital of Zhejiang Province from January 1, 2016 to December 31, 2018 were eligible for inclusion in this retrospective observational study. The study was approved by the ethics committee of the Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University. After a detailed description of the study, informed consent was obtained from patients or their relatives in cases where patients had difficulty writing owing to limb paralysis. This study was conducted in accordance with the Declaration of Helsinki.
Patients who had a history of diabetes, underwent glycated hemoglobin measurement at admission via the hemoglobin A1c test, were hospitalized in the ICU for at least three days, and had at least 12 BG values recorded during the first 72 h of their ICU stay were included in the study. We measured BG in whole blood by using a point-of-care blood gas analyzer; blood samples were obtained by means of arterial catheters used for arterial blood pressure monitoring. Glycated hemoglobin was measured by our central laboratory using a standard method and was used to estimate the premorbid baseline BG level. To avoid possible bias, patients admitted during the study period with a diagnosis of diabetic ketoacidosis or hyperosmolar non-ketotic coma were excluded from the final analysis.
Definition of RHG
A glucose level > 30% below the estimated average glucose level according to the hemoglobin A1c conversion table was defined as a single event of RHG,12,13,15,16 regardless of whether it reached the criteria of absolute hypoglycemia. We divided patients into three categories according to the number of RHG events they experienced during their ICU stay. Patients with one to two events were defined as category I, three to four events as category II, and more than four events as category III.
Insulin and BG Regulation Protocols
The goal of the insulin regulation protocol is to maintain glucose levels of < 180 mg/dL (10.0 mmol/L). Nurses intensively monitor glucose values at an interval of 2 h but less frequently if glucose values are consistent. The treating physician is responsible for the instigation, approval, and adjustment of insulin therapy for each patient, with an overall target BG level of < 10 mmol/L. Continuous intravenous insulin is used to treat the patient if the glucose value exceeds 200 mg/dL on two successive occasions. Insulin administration is reduced and then discontinued if the BG level drops below 144 mg/dL (8.0 mmol/L).8,17
Data Collection
In this cohort study, endpoints included 28-day mortality as well as clinical events, such as the incidence of hypoglycemia, delirium, and multiple organ dysfunction syndrome (MODS), during the patient’s time in the ICU. MODS is characterized by the development of progressive physiological dysfunction of at least two organs or organ systems, and is induced by various acute physiological damages, including trauma, burns, shock, and severe infection.
Demographic data, including age, sex, etiology, and APACHE II score, were recorded on admission. The definitions of organ failure, including respiratory, hepatic, cardiovascular coagulopathy, and renal, were based on a score of two or more on the Sequential Organ Failure Assessment scoring system.18 The number of RHG events was calculated and recorded for further analysis. Delirium was diagnosed using the positive confusion assessment method for the ICU.19,20 Data regarding clinical outcomes, such as mortality, use of mechanical ventilation, requirement of renal replacement therapy, and use of vasoactive agents, were also collected.
Statistical Analysis
Continuous variables were expressed as the median value (interquartile range), unless otherwise mentioned. Categorical variables were described as absolute numbers and percentages. Depending on the distribution of data, continuous variables were compared using the Mann–Whitney U-test or Kruskal–Wallis test, and categorical data were analyzed using the chi-squared test. All statistical tests were two-tailed, and the significance level was set at P<0.05. Univariate analysis and multiple logistic regression analysis were used to identify the factors related to ICU delirium. Data were analyzed using IBM SPSS Statistics for Windows version 21.0 (IBM Corp., Armonk, NY).
Results
Patient Population
A total of 113 patients (58 men and 55 women) were included in the analysis. Table 1 shows the demographic and clinical characteristics of patients at admission. Although the study site was a mixed ICU, medical patients were predominant in this study, accounting for nearly two-thirds of the study sample. No rigid glucose control protocol or other intervention was applied during the study period, and the treating physician was responsible for monitoring and adjusting patients’ glucose levels.
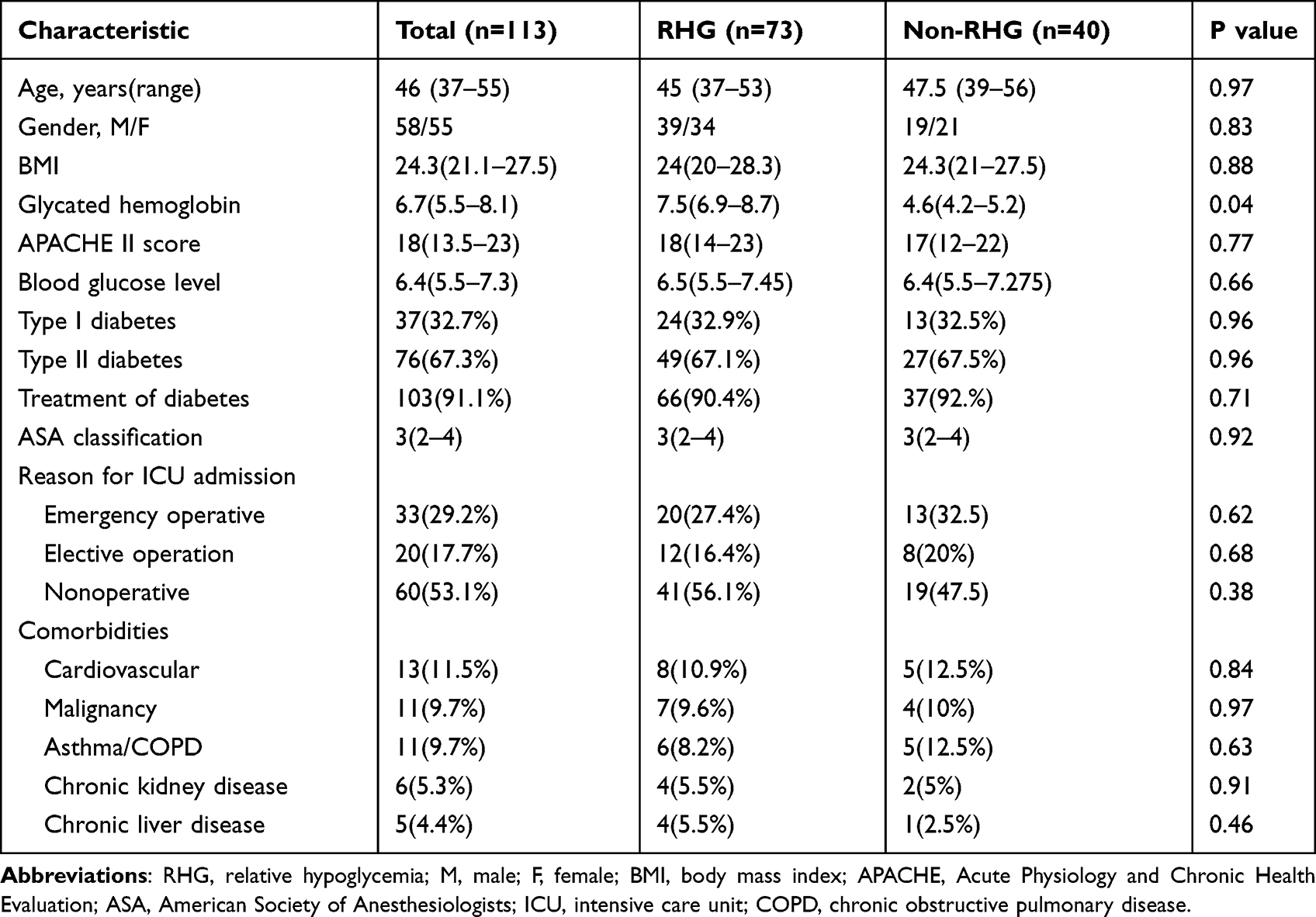 |
Table 1 Demographic and Baseline Clinical Characteristics of the Study Subjects |
Frequency of RHG Events
RHG was detected in 73/113 patients, an overall incidence of 64.6%. According to the number of RHG events during the first 72 h after ICU admission, 33 patients were assigned to category I, 26 to category II, and 14 to category III.
Patient Outcomes
Patients with RHG events had significantly higher rates of mortality, MODS (Table 2), and delirium (47.9% vs 27.5, P=0.04) than those without. Moreover, patients with a higher frequency of RHG events had a higher risk of mortality (57.1% in category III vs 15.4% in category II, P=0.006 and 15.1% in category I, P=0.003), but RHG event frequency was not significantly associated with delirium or MODS. Patients experiencing different number of RHG events, the outcome measures became even worse in a step-up fashion evidenced by increasing incidence of delirium (Figure 1).
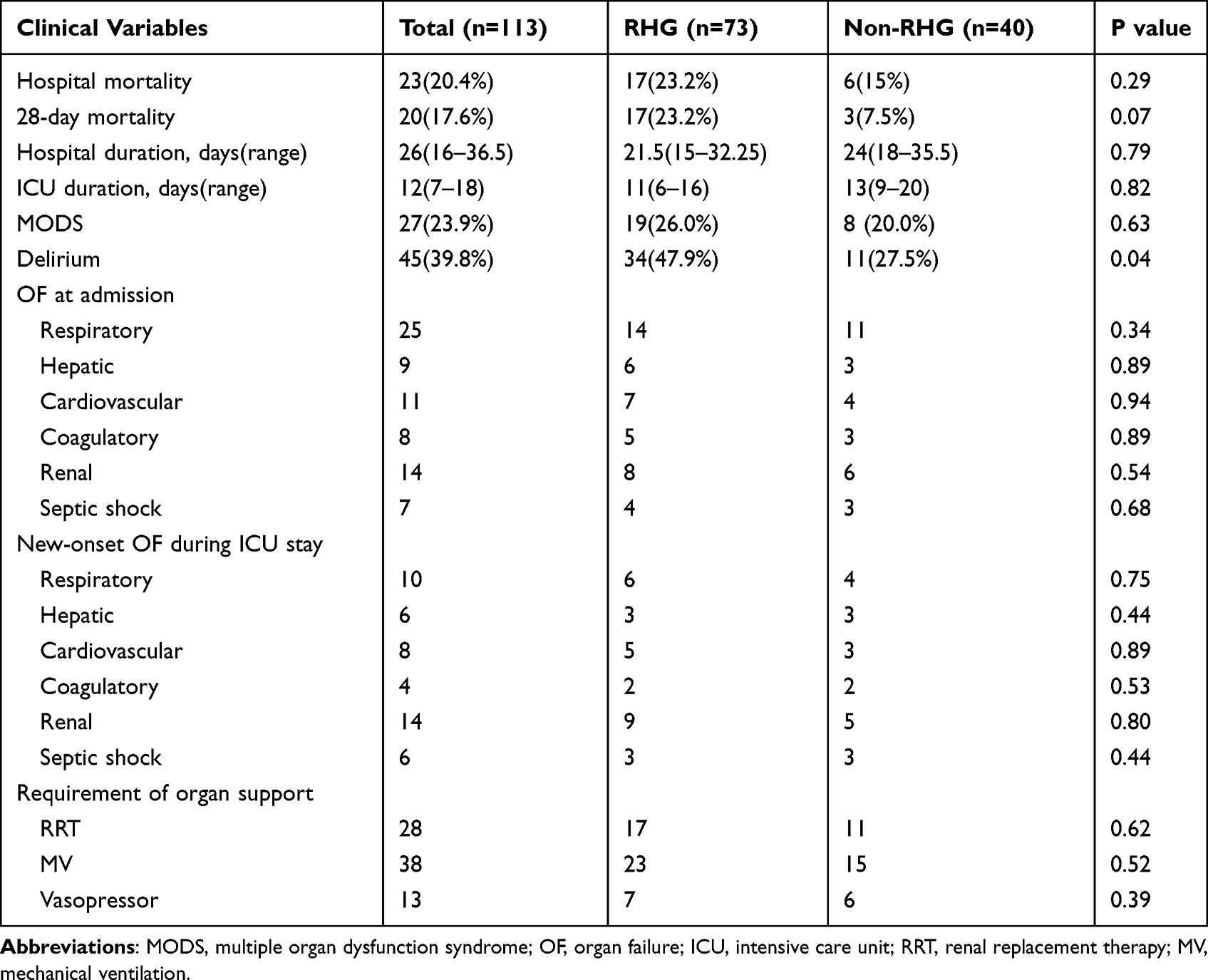 |
Table 2 Clinical Outcomes of the Study Subjects |
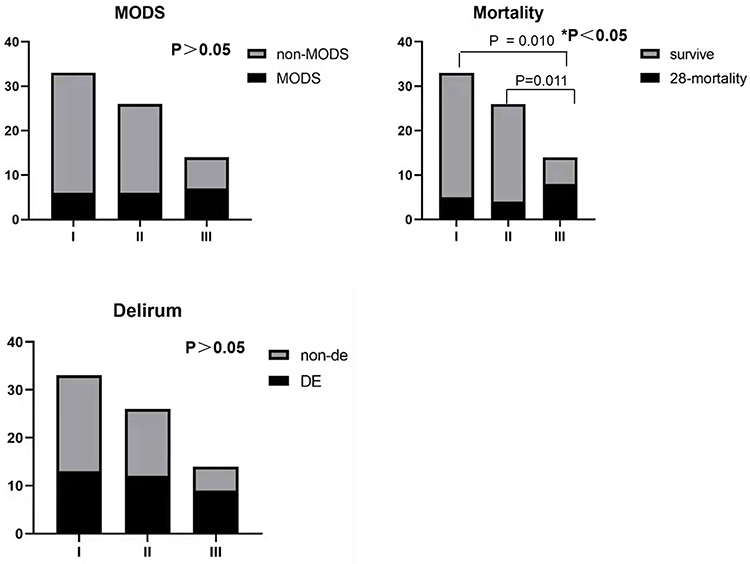 |
Figure 1 Clinical incidence of different RHG levels and their association with MODS, mortality, and delirium. *p<0.05 indicates statistical significance. Abbreviations: RHG, relative hypoglycemia; MODS, multiple organ dysfunction syndrome. |
Logistic Regression Analysis
Using the incidence of delirium as the dependent variable, logistic regression analysis (Table 3) showed a significant correlation between RHG and delirium (P=0.02, odds ratio [OR]: 3.409, 95% confidence interval [CI]: 1.186–9.801]). In addition, age was an independent risk factor for the development of ICU delirium (P=0.04, OR: 1.062, 95% CI: 1.013–1.113]).
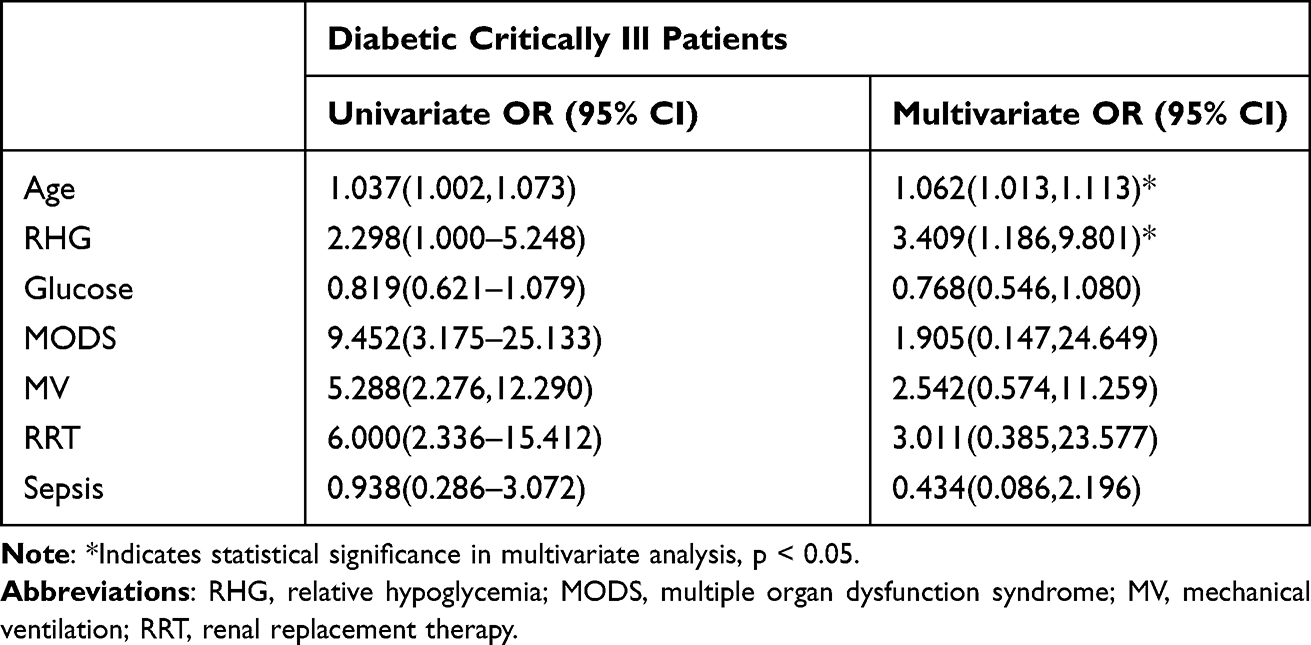 |
Table 3 Risk Factors for Development of ICU Delirium in the Study Subjects |
Discussion
Although dysglycemia has drawn growing attention in recent years, the concept of RHG based on estimated average BG levels is not widely used. In the present study, 73 RHG events occurred in 113 ICU patients (64.6%), and patients with RHG events had a higher incidence of delirium. Moreover, in logistic regression analyses, a strong correlation was observed between RHG and delirium (P=0.02, OR 3.409 [95% confidence interval, 1.186–9.801]). However, owing to the retrospective design of our study, causality could not be determined.
Some studies have focused on the association between RHG and the incidence of delirium in patients with diabetes. A previous study based on a prospective cohort showed that delirium was positively associated with hypoglycemia in patients with diabetes (adjusted OR: 2.78, 95% Cl: 1.71–6.32, P=0.005), but not in those without diabetes.10 Our results are in accordance with reports in which rigid glucose control was associated with higher rates of hypoglycemia and delirium.21,22 However, the mechanisms underlying these phenomena are poorly understood. In the present study, the association between RHG and ICU delirium may reflect mental impairment. Insulin-induced hypoglycemia affects brain function, and glucose metabolism has previously been suggested to contribute to the impairment of cognitive function, including delirium, in Alzheimer’s disease.23
Insulin therapy is a common ICU treatment owing to the variability in patient BG levels. Di Muzio et al demonstrated that adherence to a target BG level resulted in fewer episodes of hypoglycemia and a lower rate of insulin administration.12 Similar results were reported in another study, in that the prevalence of moderate-to-severe hypoglycemia was reduced with liberal glycemic control.24 Several pathological mechanisms may explain the effect of hypoglycemia on patients with diabetes in the ICU. Hypoglycemia can be detrimental and potentially lethal in critically ill patients.25,26 In both studies mentioned above, hypoglycemia was defined as a glycemic level below a standard designated level. A “relative” low glucose level must be defined to avoid underestimating the incidence of hypoglycemia, especially in patients with a clear history of diabetes, as RHG can be equally as harmful as absolute hypoglycemia. Physiologically, hypoglycemia can lead to the impairment of autonomic function, alteration of organ blood flow, change in the Q-T interval, white blood-cell activation, vasoconstriction, and release of cytokines,27–29 all of which may significantly impact the outcome of critically ill patients. In addition, hypoglycemia may contribute to increased platelet aggregation30 and prothrombotic factors.31 Hypoglycemia is also associated with neuronal damage.
In the ICU, patient BG levels should be monitored during delirium to avoid hypoglycemia. Hypoglycemia is assumed to be related to increased mortality independent of diabetic status.32 In a study by Mahmoodpoor et al, hypoglycemia, defined as a BG level < 50 mg/dL, was detected in 10% of patients in the ICU and was linked to increased mortality in critically ill patients.33 In the NICE-SUGAR study, severe hypoglycemia (defined as a BG level < 2.2 mmol/L) was detected in 206 of 3016 patients (6.8%) in the intensive-control group and 15 of 3014 (0.5%) in the conventional-control group, and was thus suggested to be an important contributor to the higher mortality observed in patients receiving intensive glucose control.8 Whether any causality exists between delirium and glucose variability warrants further exploration.
Our study has several limitations. First, it was a single-center, retrospective study with a relatively small sample and short observational window, which limits the generalizability of our results. Second, the concept of RHG is not globally accepted despite its solid theoretical underpinnings; thus, the clinical implications of this study need to be carefully interpreted. Third, the patients in our study were hospitalized in the ICU and had at least 12 BG values recorded during the first 72 h of their ICU stay. Intermittent random BG measurements cannot be used to detect episodes of hyperglycemia and hypoglycemia. Moreover, they are known to be fraught with inaccuracies and present a high workload for the nursing staff. Finally, our study was focused mainly on the relationship between RHG and delirium in patients in ICU with a history of diabetes, whereas other studies, such as the NICE-SUGAR trial, enrolled patients with other multiple organ failure conditions or etiologies (such as severe sepsis/trauma). However, we did include 28-day mortality, ICU duration, and MODS as clinical outcomes in our study, similar to the NICE-SUGAR trial.
Conclusions
In summary, our study shows a significant relationship between RHG and delirium in critically ill patients with diabetes, as well as an association with mortality. Based on our study findings, continuous glucose monitoring may be beneficial for glycemic control. Through this method, glucose fluctuations and hypoglycemic events can be observed. Providing insights into glucose trends. Further prospective studies are warranted to determine the benefits of reducing RHG events with a more liberal and individualized glucose target.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from corresponding authors on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the ethics committee of the the Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University. After a detailed description of the study, informed consent was obtained from patients or their relatives in cases where patients had difficulty writing owing to limb paralysis. This study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
The authors have all read and approve of this work for publication.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the Taizhou Municipal Sci-Tech Bureau Program (20ywa50 and 1701KY58).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Battle DE. Diagnostic and Statistical Manual of Mental Disorders (DSM). CoDAS. 2013;25(2):191–192. doi:10.1590/s2317-17822013000200017
2. Carrington SJ, Barrett SL, Sivagamasundari U, et al. Describing the profile of diagnostic features in autistic adults using an abbreviated version of the diagnostic interview for social and communication disorders (DISCO-Abbreviated). J Autism Dev Disord. 2019;49(12):5036–5046. doi:10.1007/s10803-019-04214-7
3. Schubert M, Schürch R, Boettger S, et al. A hospital-wide evaluation of delirium prevalence and outcomes in acute care patients - a cohort study. BMC Health Serv Res. 2018;18(1):550. doi:10.1186/s12913-018-3345-x
4. Aldemir M, Ozen S, Kara IH, Sir A, Baç B. Predisposing factors for delirium in the surgical intensive care unit. Crit Care. 2001;5(5):265–270. doi:10.1186/cc1044
5. Van Rompaey B, Schuurmans MJ, Shortridge-Baggett LM, Truijen S, Bossaert L. Risk factors for intensive care delirium: a systematic review. Intensive Crit Care Nurs. 2008;24(2):98–107. doi:10.1016/j.iccn.2007.08.005
6. Inouye SK. Predisposing and precipitating factors for delirium in hospitalized older patients. Dement Geriatr Cogn Disord. 1999;10(5):393–400. doi:10.1159/000017177
7. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19):1359–1367. doi:10.1056/NEJMoa011300
8. Finfer S, Chittock DR, Su SY, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283–1297. doi:10.1056/NEJMoa0810625
9. Krinsley JS, Schultz MJ, Spronk PE, et al. Mild hypoglycemia is independently associated with increased mortality in the critically ill. Crit Care. 2011;15(4):R173. doi:10.1186/cc10322
10. van Keulen K, Knol W, Belitser SV, et al. Glucose variability during delirium in diabetic and non-diabetic intensive care unit patients: a prospective cohort study. PLoS One. 2018;13(11):e0205637. doi:10.1371/journal.pone.0205637
11. van Keulen K, Knol W, Belitser SV, et al. Diabetes and glucose dysregulation and transition to delirium in ICU Patients. Crit Care Med. 2018;46(9):1444–1449. doi:10.1097/ccm.0000000000003285
12. Di Muzio F, Presello B, Glassford NJ, et al. Liberal versus conventional glucose targets in critically ill diabetic patients: an exploratory safety cohort assessment. Crit Care Med. 2016;44(9):1683–1691. doi:10.1097/ccm.0000000000001742
13. Kwan TN, Zwakman-Hessels L, Marhoon N, et al. Relative hypoglycemia in diabetic patients with critical illness. Crit Care Med. 2020;48(3):e233–e240. doi:10.1097/ccm.0000000000004213
14. Arbeláez AM, Rutlin JR, Hershey T, Powers WJ, Videen TO, Cryer PE. Thalamic activation during slightly subphysiological glycemia in humans. Diabetes Care. 2012;35(12):2570–2574. doi:10.2337/dc12-0297
15. Nathan DM, Kuenen J, Borg R, Zheng H, Schoenfeld D, Heine RJ. Translating the A1C assay into estimated average glucose values. Diabetes Care. 2008;31(8):1473–1478. doi:10.2337/dc08-0545
16. Rodríguez-Segade S, Rodríguez J, Paz JM, Camiña F. Translating the A1C assay into estimated average glucose values: response to Nathan et al. Diabetes Care. 2009;32(1):e10. doi:10.2337/dc08-1214
17. Jacobi J, Bircher N, Krinsley J, et al. Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit Care Med. 2012;40(12):3251–3276. doi:10.1097/CCM.0b013e3182653269
18. Jones AE, Trzeciak S, Kline JA. The sequential organ failure assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation. Crit Care Med. 2009;37(5):1649–1654. doi:10.1097/CCM.0b013e31819def97
19. Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286(21):2703–2710. doi:10.1001/jama.286.21.2703
20. Ely EW, Margolin R, Francis J, et al. Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Crit Care Med. 2001;29(7):1370–1379. doi:10.1097/00003246-200107000-00012
21. Saager L, Duncan AE, Yared JP, et al. Intraoperative tight glucose control using hyperinsulinemic normoglycemia increases delirium after cardiac surgery. Anesthesiology. 2015;122(6):1214–1223. doi:10.1097/aln.0000000000000669
22. Berger M, Browndyke J, Mathew JP. Intraoperative glycemic control to prevent delirium after cardiac surgery: steering a course between Scylla and Charybdis. Anesthesiology. 2015;122(6):1186–1188. doi:10.1097/aln.0000000000000670
23. Shinohara M, Sato N. Bidirectional interactions between diabetes and Alzheimer’s disease. Neurochem Int. 2017;108:296–302. doi:10.1016/j.neuint.2017.04.020
24. Kar P, Plummer MP, Bellomo R, et al. Liberal glycemic control in critically Ill patients with type 2 diabetes: an exploratory study. Crit Care Med. 2016;44(9):1695–1703. doi:10.1097/ccm.0000000000001815
25. Finfer S, Liu B, Chittock DR, et al. Hypoglycemia and risk of death in critically ill patients. N Engl J Med. 2012;367(12):1108–1118. doi:10.1056/NEJMoa1204942
26. Arabi YM, Tamim HM, Rishu AH. Hypoglycemia with intensive insulin therapy in critically ill patients: predisposing factors and association with mortality. Crit Care Med. 2009;37(9):2536–2544. doi:10.1097/CCM.0b013e3181a381ad
27. Adler GK, Bonyhay I, Failing H, Waring E, Dotson S, Freeman R. Antecedent hypoglycemia impairs autonomic cardiovascular function: implications for rigorous glycemic control. Diabetes. 2009;58(2):360–366. doi:10.2337/db08-1153
28. Wright RJ, Frier BM. Vascular disease and diabetes: is hypoglycaemia an aggravating factor? Diabetes Metab Res Rev. 2008;24(5):353–363. doi:10.1002/dmrr.865
29. Gill GV, Woodward A, Casson IF, Weston PJ. Cardiac arrhythmia and nocturnal hypoglycaemia in type 1 diabetes--the ‘dead in bed’ syndrome revisited. Diabetologia. 2009;52(1):42–45. doi:10.1007/s00125-008-1177-7
30. Hutton RA, Mikhailidis D, Dormandy KM, Ginsburg J. Platelet aggregation studies during transient hypoglycaemia: a potential method for evaluating platelet function. J Clin Pathol. 1979;32(5):434–438. doi:10.1136/jcp.32.5.434
31. Wieczorek I, Pell AC, McIver B, MacGregor IR, Ludlam CA, Frier BM. Coagulation and fibrinolytic systems in type I diabetes: effects of venous occlusion and insulin-induced hypoglycaemia. Clin Sci. 1993;84(1):79–86. doi:10.1042/cs0840079
32. Krinsley JS, Egi M, Kiss A, et al. Diabetic status and the relation of the three domains of glycemic control to mortality in critically ill patients: an international multicenter cohort study. Crit Care. 2013;17(2):R37. doi:10.1186/cc12547
33. Mahmoodpoor A, Hamishehkar H, Beigmohammadi M, et al. Predisposing factors for hypoglycemia and its relation with mortality in critically Ill patients undergoing insulin therapy in an intensive care unit. Anesth Pain Med. 2016;6(1):e33849. doi:10.5812/aapm.33849
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.