Back to Journals » Research and Reports in Tropical Medicine » Volume 9
Relationships between the weaning period and the introduction of complementary foods in the transmission of gastrointestinal parasitic infections in children in Honduras
Authors Palmieri JR ![]() , Meacham SL
, Meacham SL ![]() , Warehime J, Stokes SA, Ogle J
, Warehime J, Stokes SA, Ogle J ![]() , Leto D, Bax M, Dauer AM, Lozovski JM
, Leto D, Bax M, Dauer AM, Lozovski JM
Received 20 December 2017
Accepted for publication 1 May 2018
Published 26 July 2018 Volume 2018:9 Pages 113—122
DOI https://doi.org/10.2147/RRTM.S160388
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Thomas Unnasch
James R Palmieri,1 Susan L Meacham,2 Jenna Warehime,1 Sarah A Stokes,1 Janie Ogle,1 Dezarae Leto,1 Maggie Bax,1 Anca M Dauer,1 Janie Milliron Lozovski1
1Department of Microbiology and Immunology, 2Department of Preventative Medicine and Public Health, Edward Via College of Osteopathic Medicine, Blacksburg, VA, USA
Purpose: This study was to investigate weaning practices used by mothers when transitioning infants from breast milk to complementary foods and to determine the role these foods have in the transmission of gastrointestinal parasites.
Participants and methods: On average, of the 175 mothers extensively interviewed, 93% said they had breast-fed their infants. Approximately 20.8% of mothers had added some other liquid to their infant’s diet at 3 months, while most mothers had added other liquids at 6 months (39.0%) and >6 months (32.1%). Some mothers expanded food offerings to infants before 3 months. The percentage of mothers who had added other liquids to their infants’ diet was reported by age of the infant: as early as 1 day (2.5%), <1 week (1.9%), first month (3.1%), 3 months (20.8%), 6 months (39.0%), and >6 months (32.1%). These foods included fruit, vegetables, meat, and grains. The maximum age a child was found to be still breastfeeding was 13 years.
Results: Forty percent of mothers involved in this survey reported that their children were diagnosed and/or treated for gastrointestinal parasitic infection. Routes of infection of protozoan and helminth parasites likely resulted from contaminated complementary foods and water given to infants while still breast-feeding or from contaminated foods after breast-feeding had been completed. Contaminated water is a likely source of protozoan parasites. Contaminated water was fed to infants, mixed with formula or complementary foods, or used to wash bottles for infant feeding. There was an absence of hand-washing by children and mothers before eating or while preparing foods.
Conclusion: The major source of soil-transmitted helminth infections was likely the result of unwashed or uncooked pureed fruit or vegetables used as complementary foods, unpasteurized animal milk, insanitary food storage, poor living conditions with exposed dirt floors, and exposure to roaming domestic animals.
Keywords: breast-feeding, complementary foods, gastrointestinal parasites, Honduras, transition foods, weaning period
Introduction
In a study published in 2015, Childers and Palmieri reported on the prevalence of gastrointestinal protozoan and helminth parasites from children who were recruited from the Clínica Rural de Verón, Punta Cana region, Dominican Republic during 2008–2011.1 Of the 128 fecal samples examined, 127 were positive for one or more gastrointestinal parasites. The age of the infected children was 2–15 years; 61 were males and 66 females. The only uninfected child was a 9-year-old female. Infection rates were 43.8% for Ascaris lumbricoides, 8.5% for Enterobius vermicularis, 21.1% for Entamoeba histolytica, and 22.7% for Giardia intestinalis. Of the children examined, 7.8% had double infections. Because of the 99.2% prevalence rate for parasite infection in these children, especially in the youngest, we tried to determine the critical factors contributing to the high rate of gastrointestinal parasitic infections. Our assumption was the high infection rate, especially in the youngest children examined, was due to complementary or weaning foods fed to children while still being breast-fed or due to contaminated solid and liquid foods and contaminated water fed to children who were no longer being breast-fed.1–4
In Honduras and other countries in Central America and the Caribbean, staggering health and economic burdens result from neglected tropical diseases, especially parasitic diseases. This is especially true with people at highest risk, who live in poverty on <US$2 per day.5,6 Indigenous populations, especially infants and children, are most vulnerable to neglected tropical diseases, resulting in chronic infections causing tissue damage, immunologic changes, chronic illnesses, malnutrition, anemia, cognitive changes, and growth stunting.7–10 Currently, >8 million Central American children require mass drug treatments annually, and often more frequently for gastrointestinal helminth infections.11–14 In Honduras, young infants and children are at greatest risk of acquiring gastrointestinal infections ranging from parasitic protozoa to helminths producing diseases mostly isolated to the intestinal tract. These diseases include balantidiasis, cryptosporidiosis, cyclosporiasis, giardiasis, isosporiasis (in HIV positive patients), enterobiasis, trichuriasis, and hymenolepiasis, while other gastrointestinal parasitic infections may become systemic, such as entamebiasis, toxoplasmosis, ascariasis, and hookworm.13–18
Honduras is located in Central America, bordering the Caribbean Sea between Guatemala and Nicaragua and bordering the Gulf of Fonseca between El Salvador and Nicaragua. Its climate is relatively constant throughout the year, being subtropical in lowlands and temperate in mountains.1 The population age structure as of 2017 is biased toward the young, with 32.95% 0–14 years, 21% 15–24 years, 36.63% 25–54 years, 5.13% 55–64 years, and 4.29% ≥65 years.6 The mean age at first birth is 20.4 years, and median age of first birth is 25–29 years.6 As of 2017, the total estimated fertility rate was 2.67 children per woman, with an average of three children per woman.4,6 As of 2014, the infant mortality rate (deaths/1,000 live births) was 18.72 and life expectancy at birth 70.91 years. The infant-mortality rate is 18.72. On average, children <5 years of age are average degree of underweight 8.6%.1 Approximately 90% of the population have access to improved water sources (piped water into dwelling, yard, or plot; public tap or standpipe; tube well or borehole; protected dug well; protected spring; or rainwater collection), while ~10% rely on unimproved sources of water (unprotected dug well; unprotected spring; cart with small tank or drum; tanker truck; surface water, which includes rivers, dams, lakes, ponds, streams, canals, or irrigation channels; or bottled water).1,2,6
In studies by Hotez et al, soil-transmitted helminth infections are endemic in Honduras, but their impact on children’s health is not well studied.7,8 Hotez et al reported the overall soil-transmitted helminth prevalence among 320 children studied was 72.5%, with almost half the infected children harboring multiple species of parasites. Polyparasitism is more likely to occur in children attending school, with absent or annual deworming schedules than in students attending schools where deworming takes place at least twice a year. Prevalence by species7,8 was 30%, 67%, and 16% for Ascaris, Trichuris, and hookworm, respectively. Infections of moderate–heavy intensity, as well as multiple parasite infections, are significant predictors of decreased weight-for-age scores in children aged 7–10 years.7–9
In this study, we set out to determine what the breast-feeding practices were in rural Honduras and how infants are weaned from breast-milk to complementary foods. We use the World Health Organization (WHO) definition of exclusive breast-feeding: when the infant takes only breast milk and no additional food, water, or other fluids, with the exception of medicine and vitamins or mineral drops. We also wanted to determine what other contributing factors, such as food preparation, water sources, and local environmental factors, were responsible for the high gastrointestinal parasite-infection rates in infants and children. In addition, we wanted to determine if there were treatment programs available to infants and children with parasitic infections.
Participants and methods
This study qualified for expedited review under the category of international research and was subsequently approved by the Virginia College of Osteopathic Medicine (VCOM) institutional review board (IRB) committee (2014/010). Development of this study, including design, procedures, instrumentation, data collection, and all aspects was a collaboration between James Moody Adams Clinic, Baxter Institute, Tegucigalpa, Honduras and the Edward Via VCOM personnel under the auspices of a signed agreement between the Honduran health ministry and VCOM. Approval in the USA complied with Honduran health-ministry agreements and involvement of medical personnel in Honduras.
The survey instrument was designed to obtain qualitative and quantitative information about the weaning process, transition to complementary foods, and steps that may introduce gastrointestinal parasitic vulnerabilities to infants and children in Honduras. The survey was written using lay terminology and made available in English; certified VCOM IRB translators provided versions in Spanish and French. This paper reports quantitative and qualitative findings from the study in Tegucigalpa, Honduras. VCOM osteopathic medical students administered surveys over a 2-year period at the James Moody Adams Baxter Clinic. In addition, observational information about breast-feeding, weaning practices, complementary foods utilized, and disease transmission was documented by seven on-site study personnel. Mothers awaiting treatment at the clinic were asked to complete the weaning foods survey voluntarily (Box 1). Participants were informed of the purpose of the study. Research personnel read and explained the consent form. Documentation of consent was waived by the VCOM IRB form F (2014). Individual participants either read and answered the survey questions or were provided assistance by research personnel to complete the survey. Qualitative questions were asked of participants during the survey (Box 2). Data from the survey were captured in Qualtrics, a commercially available quantitative statistical-analysis software program (Qualtrics, Provo, UT, USA). Pearson χ2, Fisher’s exact test and Student’s t-tests examined associations of interest regarding breastfeeding, weaning. or complementary foods and potential routes of parasite infections. Statistical analysis was performed using SPSS (version 22; IBM, Armonk, NY, USA) with significance set a priori at P=0.05. The WHO and United Nations Children’s Emergency Fund breast-feeding recommendations referenced key terminology and concepts in this report are defined in the Supplementary material.
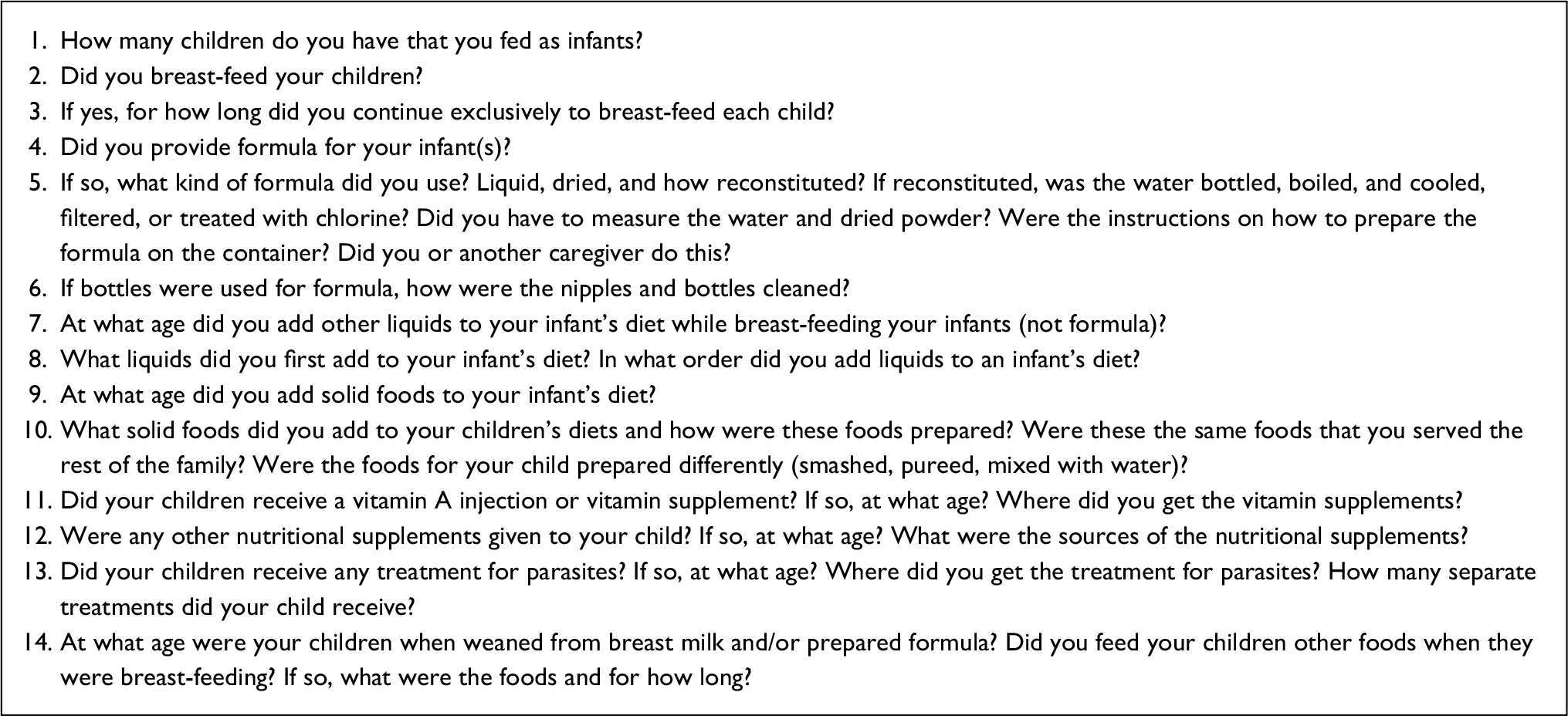 | Box 1 Quantitative survey questions (analyzed statistically) asked of mothers at the James Moody Adams Baxter Clinic, Tegucigalpa, Honduras |
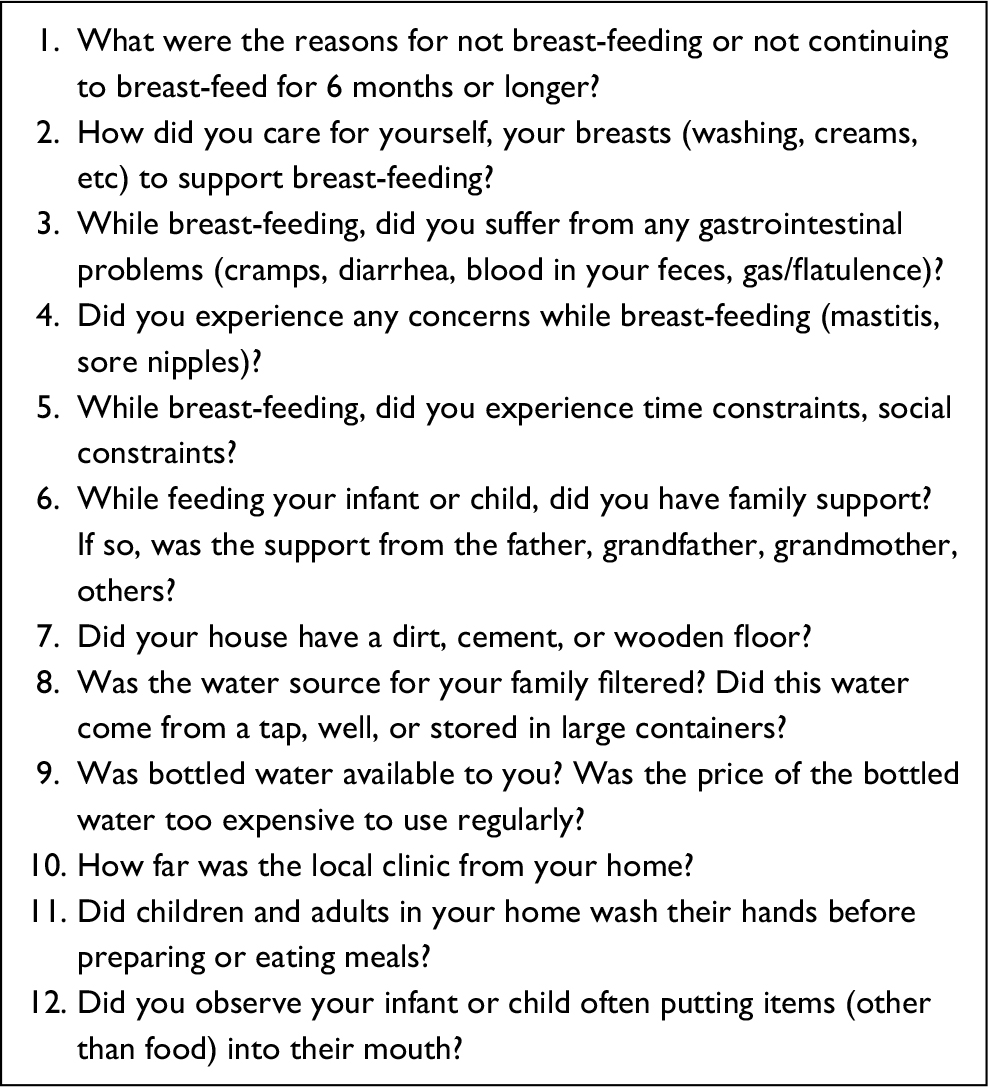 | Box 2 Qualitative questions asked of mothers at the James Moody Adams Baxter Clinic, Tegucigalpa, Honduras |
Results
The survey questions (Box 1) were voluntarily completed by participants attending the James Moody Adams Baxter Clinic in Tegucigalpa, Honduras between November 2014 and March 2015. Responses were received from 179 mothers who had had a total of 513 children. Most of the participants responded to the yes/no questions (66%–93%)and questions with categorical responses (73%–89%). Mothers were also asked other qualitative questions (Box 2) while responding to the survey questions.
At the time of the survey, the mothers who responded had had an average of 3.31 children, ranging from one to ten children per mother. When asked if they had ever breast-fed their children, 93% answered yes. The duration that mothers breast-fed their infants varied. A few mothers reported breastfeeding their children exclusively for only 1 day (4.1%), while 47.9% reported breastfeeding exclusively for >6 months. The average age at weaning from breast-feeding was 2.1 years, with a maximum age at weaning of 13 years.
The age at which other liquids were added to the diet of infants and children by their caregivers varied. Few mothers added other liquids at 1 day of age (2.5%). Approximately 20.8% of mothers had added some other liquid to their infant’s diet at 3 months, while most mothers had added other liquids at 6 months (39.0%) and >6 months (32.1%). The most frequently added liquids to an infant’s diet (other than milk) were boiled and cooled water (54.5%), followed by fruit juice (15.2%) and bottled water (10.1%). Carbonated flavored soda was the third or fourth liquid added to the infants’ diets. Approximately 51.2% of mothers introduced solid foods into their infant’s diet at 4–6 months, while 30.6% added solid foods at >6 months. Approximately 86.3% of infants and children had received some form of parasite treatment from 6 months and to 7 years of age, with an average age of treatment at 1.7±1.2 years.
There was no statistical significance regarding the relationship between whether a mother had ever breast-fed her child and the age that solid food was added to their child’s diet. This was also true even when reevaluated when food was added and recategorized into <3 months, 4–6 months, and >6 months of age. There was no statistical significance between being breast-fed and receiving parasite treatment (P>0.05) either. There was no association between the age when food was added to the infant’s diet and when they received parasite treatment (P=0.9). t-Tests indicated a significant relationship for those mothers who had breast-fed their children and the mean number of children (P=0.001). Those that had breast-fed had a higher mean number of children (P=0.001); t-test analysis also indicated that there was no difference between being breast-fed and maximum age when weaned from milk.
Discussion
This project was undertaken following a previous report by the primary author conducted in the Dominican Republic reporting that 127 of 128 children had gastrointestinal parasites based on stool examination.1 These children were at risk of sequelae, including physical and mental growth retardation, anemia, weight loss, and nutrient deficiencies.2 Because of this extremely high rate of infection in the infants and children, we questioned if the practice of weaning or the introduction of transitional foods may have been responsible. Likewise, in Honduras a great proportion of the population are affected by gastrointestinal parasites.2
Potential routes of parasitic infections
Forty percent of mothers involved in this survey reported that their children had been diagnosed and/or treated for gastrointestinal parasitic infection, a much higher prevalence than in other areas of the world. Research has shown that clinical diagnosis underestimates the actual prevalence of parasitic infections.19 In this study, on-site personnel recorded observations on potential routes of infection of protozoan and helminth gastrointestinal parasites from complementary foods and water given to infants while still breast-feeding or from contaminated foods given to infants after breastfeeding had been completed. Observations from the seven on-site study personnel uniformly confirmed that contaminated water was the most likely source of protozoan parasites. Sources of contamination included unfiltered or water that has not been boiled from wells, contaminated public water, and unfiltered water improperly stored in containers that were not cleaned or sanitized. Often throughout this study, we observed open and uncovered water sources within 15 m of latrine or outhouse facilities (Figures 1 and 2). Contaminated water was fed to infants directly, used to mix with formula or complementary foods, or used to wash bottles for infant feeding. Even when filtered or boiled water was used, often mothers or caregivers did not wash their hands prior to food preparation. The major source of soil-transmitted helminth infections was most likely the result of environmental contamination, such as unwashed or uncooked pureed fruit or vegetables used as complementary foods, unpasteurized animal milk, unsanitary food storage, poor living conditions with exposed dirt floors, and exposure to roaming domestic animals. Infants and young children often put unwashed items in their mouth.
 | Figure 1 Example of an open and uncovered water source that serves the water needs of a village. |
 | Figure 2 An open and uncovered water source within meters of the village latrine or outhouse facility. |
Although improvements in children’s health in Honduras have been comparatively moderate over the past 25 years, according to both a Honduras labor-market assessment (2017)20 and the WHO sustainable goals (2015), for which half the 19 established WHO goals to reduce mortality under age 5 years had been met.21 This progress is attributed to integrated interventions by the many health care services available to mothers, children, and infants in Honduras, which include improvements in nutrient deficiencies, breast-feeding and the weaning process, adequate energy intake, micronutrient optimization, and reduced pathogenic contamination.20,21 However, with inequities in underserved communities, there are still high rates of stunting due to malnutrition and high rates of gastrointestinal parasitic infections in Honduras, thereby preventing infants and children from growing or developing properly.22
Breast-feeding and nutrition
Malnutrition and infection often present concurrently in compromised infants and generally the underlying causes of diarrhea, are a major cause of infant and child morbidity and mortality. Both malnutrition and infection are responsive to intervention.23–25 According to the WHO (2017), references to infections in infants with diarrhea are often limited to just bacterial infection and address sources, organisms, and methods of reducing microbial load.26 Pathogenic infections, microbial and parasitic, are often transmitted by contaminated water and complementary foods introduced at weaning.27,28
Marino et al found that a history of breast-feeding was associated with a reduction in risk of various pathogenic illnesses, including aspecific gastroenteritis and severe lower respiratory tract infection.29 Education and promotion of breast-feeding practices have been prominent public-health initiatives for several decades, yet globally not as effective as expected.30,31
Cohen at al described one breast-feeding intervention study in Honduras. They addressed the timing of weaning in infants in relation to growth by recruited women with infants from two local hospitals in San Pedro Sula, Honduras.33 Mothers were given commercial complementary foods to introduce to their infants’ diets at various ages to determine differences in infant-weight gain by 6 months of age. The results indicated that infants self-regulated energy intake, and no difference in weight or length gained was noted compared to exclusively breast-fed infants to the age of 6 months.32 In vulnerable populations, contaminated complementary weaning foods, also of inferior nutritional value compared to breast milk, are considered a disadvantage. As such, there was no advantage for infant growth when introducing complementary foods before age 6 months.33,34
Promoting exclusive breast-feeding until six months of age has been a global goal.34 Breast milk is considered the best source of nutrition for infants, with numerous secondary benefits. In vulnerable populations, the additional benefits of breast-feeding were the availability and easy “access” of breast milk, cost savings, immunological advantages, and the advantage of reduced likelihood of introducing pathogens.35,36
Feeding practices, of vital importance to infants and children nutritionally, are also an important factor in the prevention of parasitic infections.37 The infant’s age at weaning and the types of complementary foods introduced at weaning are primary targets for parasite transmission and infection, and thus primary targets for parasite-infection interventions.3,4,38 The longer a child breast-feeds, the longer they will have reduced exposure to pathogens from a food source, given the mother’s personal hygiene practices are sanitary.39 Likewise, the longer a child breast-feeds, the longer they will avoid being given contaminated water and avoid complementary foods of lower nutritional content prepared with contaminated water.3,4 Each month, a well-nourished child’s strength, immunity, and resilience improve, reducing their vulnerability to pathogenic infections.40,41
Complementary food and water contamination and food and water recommendations
The WHO recommends breast-feeding exclusively for 6 months before beginning to supplement the infant’s diet with complementary foods.42 Complementary foods should be given in similar frequency, amount, and consistency on a daily basis, with incremental increases in quantity, introducing single foods one at a time to which the infant is accustomed, in order to ease the transition. It is recommended that caregivers supplement the infant’s diet with a variety of foods to ensure the nutritional needs of the child are being met.42,43 Caregivers can progress to supplementing more meals throughout the day as the child grows. All complementary foods should be prepared in a manner that minimizes the risk of contamination with pathogens.
As infants are weaned and potentially exposed to contaminated foods and water, they become increasingly susceptible to acquiring parasitic infections.1,3 Throughout the weaning process, breast milk may be supplemented with solid and liquid foods, helping infants to become accustomed to the change in diet while still contributing required nutrients from the breast milk.44 The content of supplementary foods and age at which supplementary or complementary foods are introduced into the child’s diet is highly varied, based on factors including local customs, national culture, and food availability.4,44 In areas of higher poverty, cow’s milk and other foods of animal origin are less likely to be introduced to the infant’s diet, due to cost. Traditional weaning foods in Honduras and other Central American countries include rice cereal, vegetables, and fruit, all of which are potential sources of infective pathogens.45,46 Proper food preparation and storage are essential in preventing the transmission of gastrointestinal protozoan and helminth parasites.2,3 Contaminated utensils used to prepare or dilute weaning foods and contaminated water used in preparation of food or infant formula are a common source of transmission of gastrointestinal parasites, especially Entamoeba and Giardia.47 Even if providers prepare foods carefully, proper cooking techniques do not ensure the elimination of parasites or other pathogens.3,48
Risk factors for infants and children developing gastrointestinal parasitic infections are numerous, and include improper handling of waste, improper hygiene practices, poverty, low parental education, contaminated water sources, and any animals that come in contact with caregivers while preparing food.3,49 Without proper hygiene, sanitation, and food-safety measures, an infant’s food and drinking water can easily become contaminated with microorganisms. Such precautions as caregiver education and proper weaning-food preparation can reduce contamination risks. Without preventive measures, there will continue to be an elevated prevalence of gastrointestinal parasitic infections in infants and children of Honduras.
Regardless of the pathogen, methods to prevent and reduce pathogenic infections are universally similar for all organisms, eg, hand washing, treating water, and preparing complementary foods properly. Key practices related to sanitation and hygiene are: dispose of feces safely (toilet/latrine/buried sufficiently to prevent resurfacing); wash hands thoroughly with soap (or ash) and water after contact with feces, before touching food, and before feeding children; wash the face with soap and water every day to help prevent eye infections; use water from a safe source or water that is purified and kept covered; wash or cook raw food, reheat cooked food thoroughly prior to eating, and do not delay consumption of food after its preparation; keep food, utensils, and food-preparation surfaces clean and store food in covered containers, keeping refrigerated when possible; safely dispose of all refuse to prevent illness.3,4,50–54
Recommendations
An estimated sixth of the world’s population is infected with one or more gastrointestinal parasites, and an increased proportion of these cases are children within developing countries, such as Honduras.3,4 Of the children whose mothers were surveyed in this study, a great number of them had contracted gastrointestinal parasitic infections during the weaning process. This suggests that contaminated food or liquids given to the infant during this time were the source of transmission of gastrointestinal parasites.3,4 The development of health-education programs encouraging breast-feeding and food-safety programs for caregivers and food handlers is imperative to decrease parasite acquisition among infants and children.
Before the weaning process is initiated, nutrition training should be offered to mothers and caretakers within the home. A step-by-step, easy-to-follow information packet, much like the WHO’s guide Weaning from Breast Milk to Family Food: A Guide for Health and Community Workers, would be a valuable resource.55 Health care professionals should be closely involved in educating caretakers on proper hygienic practices, appropriate water sources, and appropriate types of weaning foods. For example, it should be advised that caretakers boil drinking water for at least 3 minutes before using it in preparing weaning foods for the infant.56,57 Caretakers must also be aware of the signs and symptoms of parasitic infections in their child. If the child experiences nausea, vomiting, diarrhea, abdominal cramping, loss of appetite, or fever, caregivers should seek medical treatment immediately for their child.58 Education is key in reducing gastrointestinal parasitic infections in young children. It would be beneficial to have a multifaceted health-education team in local communities demonstrate preventive hygienic strategies and provide safe water-source education to reduce infections after weaning.3,4
Future studies should determine the environmental influences and water supplies available to communities and types of pathogens, microbial and parasitic, characteristically responsible for infection rates in infants and children in underdeveloped urban and rural communities where high rates of parasite infections are likely. Our findings support the United Nations Convention on the Rights of the Child supporting every country to ensure children’s right to the highest attainable standard of health by providing breast-feeding support, access to nutritious foods, appropriate health care, and clean drinking water to support health and prevent infection.
Acknowledgments
The authors thank the Edward Via College of Osteopathic Medicine for research facilities and Dr Dean Sutphin, PhD, Vice Provost for International and Appalachian Outreach Project for his support for the international research program in Honduras. We also thank the James Moody Adams Baxter Clinic in Tegucigalpa, Honduras and the Honduras Ministry of Health for collaboration on research and clinical facility use. Special appreciation is extended to Xiomara L Erazo, MD, Baxter Institute, attending VCOM physician at the James Moody Adams Clinic, who coordinates VCOM research and medical student responsibilities. This research was totally funded internally by the Edward Via College of Osteopathic Medicine.
Author contributions
All authors contributed to this study, under the leadership of JRP and SLM, which included project design, data acquisition, data interpretation, and data analysis. All authors were involved in the drafting and revision of this article and its intellectual content. All authors have approval the final version of this article and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. In addition, JW, SSK, DL, MB, ACD, JML, and JO spent time in Honduras interviewing mothers awaiting treatment at the James Moody Adams Baxter Clinic.
Disclosure
The authors report no conflicts of interest in this work.
References
Childers KA, Palmieri JR. Factors contributing to high prevalence of gastrointestinal parasites in children aged 2–15 years in the Punta Cana region of the Dominican Republic. Rep Parasitol. 2015;4:1–5. | ||
Childers KA, Palmieri JR, Sampson M, Brunet D. Prevalence of gastrointestinal parasites in children from Verón, a rural city of the Dominican Republic. Res Rep Trop Med. 2014;5:45–53. | ||
Childers KAG. A survey of the prevalence of gastrointestinal parasites and associated risk factors in children in a rural city of the Dominican Republic. Available from: https://vtechworks.lib.vt.edu/handle/ 10919/64807. Accessed June 15, 2018. | ||
Palmieri JR, Warehime J, Childers KA, Meacham S. Relationships between weaning food preparation and the transmission of parasitic infections among children in Honduras, El Salvador and the Dominican Republic. Austin J Microbiol. 2015;1(1):1003. | ||
Index Mundi. Haiti literacy. 2015. Available from: http://www.indexmundi.com/haiti/literacy.html. Accessed December 18, 2017. | ||
Central Intelligence Agency. The World Factbook. Washington: CIA; 2017. | ||
Hotez PJ, Woc-Colburn L, Bottazzi ME. Neglected tropical diseases in Central America and Panama: review of their prevalence, populations at risk and impact on regional development. Int J Parasitol. 2014;44(9):597–603. | ||
Hotez PJ. Holidays in the sun and the Caribbean’s forgotten burden of neglected tropical diseases. PLoS Neglected Tropical Diseases 2008;2(5):e239. | ||
Hotez PJ, Bottazzi ME, Franco-Paredes C, Steven KA, Periago MR. The neglected tropical diseases of Latin America and the Caribbean: a review of disease burden and distribution and a roadmap for control and elimination. PLoS Negl Trop Dis. 2008;2(5):e239. | ||
Muñoz-Antoli CA, Pavón A, Marcilla A, Toledo R, Esteban JG. Prevalence and risk factors related to intestinal parasites among children in Department of Rio San Juan, Nicaragua. Trans R Soc Trop Med Hyg. 2014;108(12):774–782. | ||
Baron S, Wakelin D. Helminths: pathogenesis and defenses. In: Baron S, editor. Medical Microbiology. 4th ed. Galveston (TX): University of Texas; 1996. | ||
Watkins WE, Pollitt E. Stupidity or worms: do intestinal worms impair mental performance? Psychol Bul. 1997;121(2):171–191. | ||
Kaminsky RG, Soto RJ, Campa A, Baum MK. Intestinal parasitic infections and eosinophilia in an human immunedeficiency [sic] virus positive population in Honduras. Mem Inst Oswaldo Cruz. 2004;99(7):773–778. | ||
de Kaminsky RG, Retes EH. Helmintiasis en niños en Amapala, Honduras. Hondur Pediátr. 2000;21(2):7–9. | ||
Sanchez AL, Gabrie JA, Rueda MM, Mejia RE, Bottazzi ME, Canales MA. Scoping review and prevalence analysis of soil-transmitted helminth infections in Honduras. PLoS Negl Trop Dis. 2014;8(1):e2653. | ||
Malavade SS. Assessment of Soil Transmitted Helminth Infection (STHI) in School Children, Risk Factors, Interactions and Environmental Control in El Salvador [PhD thesis]. Tampa: University of South Florida; 2015. | ||
Hofman P, Lucas S, Jouvion G, Tauziède-Espariat A, Chrétien F, Cathomas G. Pathology of infectious diseases: what does the future hold?. Virchows Arch. 2017;470(5):483–492. | ||
Kattula D, Sarkar R, Ajjampur SS, et al. Prevalence and risk factors for soil transmitted helminth infection among school children in south India. Indian J Med Res. 2014;139(1):76–82. | ||
Kwenti TE, Nkume FA, Tanjeko AT, Kwenti TD. The effect of intestinal parasitic infection on the clinical outcome of malaria in coinfected children in Cameroon. PLoS Negl Trop Dis. 2016;10(4):e0004673. | ||
United States Agency for International Development. Honduras labor market assessment. 2017. Available from: https://www.fhi360.org/sites/default/files/media/documents/resource-honduras-lma-report.pdf. Accessed December 18, 2017. | ||
United Nations. Sustainable development goals: 17 goals to transform our world. 2017. Available from: http://www.un.org/sustainabledevelopment. Accessed December 18, 2017. | ||
Pan American Health Organization. Country report: Honduras. 2016. Available from: http://www.paho.org/salud-en-las-americas-2017/?page_id=133. Accessed December 18, 2017. | ||
Sheth M, Dwivedi R. Complementary foods associated diarrhea. Indian J Pediatr. 2006;73(1):61–64. | ||
Muhimbula HS, Issa-Zacharia A. Persistent child malnutrition in Tanzania: risks associated with traditional complementary foods. Afr J Food Sci. 2010;4(11):679–692. | ||
Sanchez AL, Gabrie JA, Canales M, et al. Soil-transmitted helminths, poverty, and malnutrition in Honduran children living in remote rural communities. Hum Parasit Dis (Auckl). 2016;8:27–35. | ||
World Health Organization. Chagas disease (American trypanosomiasis). 2018. Available from: http://www.who.int/mediacentre/factsheets/fs340/en. Accessed December 18, 2017. | ||
World Health Organization. Female genital mutilation. 2018. Available from: http://www.who.int/mediacentre/factsheets/fs241/en. Accessed 24 May, 2018. | ||
Kutty PK. Breastfeeding and risk of parasitic infection: a review. Asian Pac J Trop Biomed. 2014;4(11):847–858. | ||
Marino DD. Water and food safety in the developing world: global implications for health and nutrition of infants and young children. J Am Diet Assoc. 2007;107(11):1930–1934. | ||
Chung M, Raman G, Chew P, Magula N, Trikalinos T, Lau J. Breastfeeding and maternal and infant health outcomes in developed countries. Evid Rep Technol Assess (Full Rep). 2007;(153):1–86. | ||
Kumar D, Goel NK, Mittal PC, Misra P. Influence of infant-feeding practices on nutritional status of under-five children. Indian J Pediatr. 2006;73(5):417–421. | ||
Bhandari N, Mazumder S, Bahl R, Martines J, Black RE, Bhan MK. An educational intervention to promote appropriate complementary feeding practices and physical growth in infants and young children in rural Haryana, India. J Nutr. 2004;134(9):2342–2348. | ||
Cohen RJ, Brown KH, Dewey KG, Canahuati J, Rivera LL. Effects of age of introduction of complementary foods on infant breast milk intake, total energy intake, and growth: a randomized intervention study in Honduras. Lancet. 1994;344(8918):288–293. | ||
Dewey KG, Roberta J, Cohen L, Rivera LL, Brown KH. Effects of age of introduction of complementary foods on iron status of breast-fed infants in Honduras. Am J Clin Nutr.1998;67(5):878–884. | ||
World Health Organization. Infant and young child feeding. 2017. Available from: http://www.who.int/mediacentre/factsheets/fs342/en. Accessed December 18, 2017. | ||
World Health Organization. Breastfeeding. 2017. Available from: http://www.who.int/nutrition/topics/exclusive_breastfeeding/en. Accessed December 18, 2017. | ||
US Department of Health and Human Services. The Surgeon General’s call to action to support breastfeeding. 2017. Available from: https://www.surgeongeneral.gov/library/calls/breastfeeding/factsheet.html. Accessed December 18, 2017. | ||
Khandelwal R, Gupta A, Singh G, Kapil U, Pandey RM, Upadhyay AD. Nutrient intake of adolescents in rural area of Himachal Pradesh. Indian J Community Health. 2017;29(2):194–197. | ||
Caulfield L, Richard S, Rivera J, Musgrove P, Black R. Stunting, wasting, and micronutrient deficiency disorders. In: Jamison D, Breman J, Measham A, et al, editors. Disease Control Priorities in Developing Countries. 2nd ed. Washington: Oxford University Press; 2006:551–567. | ||
Keusch GT, Fontaine O, Bhargava A, et al. Diarrheal diseases. In: Jamison DT, Breman JG, Measham AR, et al, editors. Disease Control Priorities in Developing Countries. 2nd ed. New York: Oxford University Press; 2006:371–387. | ||
US Agency for International Development. Multi-sectoral nutrition strategy: 2014–2025. 2014. Available from: https://www.usaid.gov/sites/default/files/documents/1867/USAID_Nutrition_Strategy_5-09_508.pdf. Accessed December 18, 2017. | ||
Tickell KD, Pavlinac PB, John-Stewart GC, et al. Impact of childhood nutritional status on pathogen prevalence and severity of acute diarrhea. Am J Trop Med Hyg. 2017;97(5):1337–1444. | ||
World Health Organization. Complementary feeding. 2017. Available from: http://www.who.int/nutrition/topics/complementary_feeding/en. Accessed December 18, 2017. | ||
Beral V, Bull D, Doll R, Peto R, Reeves G. Breast cancer and abortion: collaborative reanalysis of data from 53 epidemiological studies, including 83,000 women with breast cancer from 16 countries. Lancet. 2004;363(9414):1007–1016. | ||
Cohen RJ, Brown KH, Canahuati J, Rivera LL, Dewey KG. Determinants of growth from birth to 12 months among breast-fed Honduran infants in relation to age of introduction of complementary foods. Pediatrics. 1995;96(3):504–510. | ||
Motarjemi Y, Käferstein F, Moy G, Quevedo F. Contaminated weaning food: a major risk factor for diarrhoea and associated malnutrition. Bull World Health Organ. 1993;71(1):79–92. | ||
Walker AF. The contribution of weaning foods to protein–energy malnutrition. Nutr Res Rev. 1990;3(1):25–47. | ||
Wright J, Gundry S, Conroy R. Household drinking water in developing countries: a systematic review of microbiological contamination between source and point-of-use. Trop Med Int Health. 2004;9(1):106–117. | ||
Steketee RW. Pregnancy, nutrition and parasitic diseases. J Nutr. 2003;133(5):1661S–1667S. | ||
Baum R, Kayser G, Stauber C, Sobsey M. Assessing the microbial quality of improved drinking water sources: results from the Dominican Republic. Am J Trop Med Hyg. 2014;90(1):121–123. | ||
de Leon SY, Meacham SL, Claudio VS. Global Handbook on Food and Water Safety: For the Education of Food Industry Management, Food Handlers, and Consumers. Springfield (IL): Charles C Thomas; 2003. | ||
Ejemot-Nwadiaro RI, Ehiri JE, Arikpo D, Meremikwu MM, Critchley JA. Hand washing promotion for preventing diarrhoea. Cochrane Database Syst Rev. 2015;(9):CD004265. | ||
Arnold B, Arana B, Mäusezahl D, Hubbard A, Colford JM Jr. Evaluation of a pre-existing, 3-year household water treatment and handwashing intervention in rural Guatemala. Int J Epidemiol. 2009;38(6):1651–1661. | ||
Bowen A, Agboatwalla M, Luby S, Tobery T, Ayers T, Hoekstra RM. Association between intensive handwashing promotion and child development in Karachi, Pakistan: a cluster randomized controlled trial. Arch Pediatr Adolesc Med. 2012;166(11):1037–4444. | ||
Bowen A, Agboatwalla M, Ayers T, Tobery T, Tariq M, Luby SP. Sustained improvements in handwashing indicators >5 years after a cluster-randomised, community-based trial of handwashing promotion in Karachi, Pakistan. Trop Med Int Health. 2013;18(3):259–267. | ||
Pan American Health Organization. Health in the Americas 2012 Edition: Regional Outlook and Country Profiles. Washington: PAHO; 2012. | ||
Rosa G, Clasen T. Estimating the scope of household water treatment in low-and medium-income countries. Am J Trop Med Hyg. 2010;82(2):289–300. | ||
Food and Agriculture Organization. Feeding young children aged over six months. 2004. Available from: http://www.fao.org/docrep/007/y5740e/y5740e0a.htm. Accessed December 18, 2017. | ||
Miller SA, Rosario CL, Rojas E, Scorza JV. Intestinal parasitic infection and associated symptoms in children attending day care centres in Trujillo, Venezuela. Trop Med Int Health. 2003;8(4):342–347. |
Supplementary material
World Health Organization and United Nations Children’s Emergency Fund breast-feeding recommendations
- Early initiation of breast-feeding within 1 hour of birth
- Exclusive breast-feeding for the first 6 months of life
- Introduction of nutritionally adequate and safe complementary (solid) foods at 6 months together with continued breast-feeding up to 2 years of age or beyond
Definitions of key terminology and concepts
Adolescent: a person aged 10–19 years.
Child: a person of either sex between the time of birth and adolescence or puberty.
Complementary feeding: the process of starting when breast milk alone is no longer sufficient to meet the nutritional requirements of infants, and thus other foods and liquids are needed, along with breast milk.
Exclusive breastfeeding: the infant takes only breast milk and no additional food, water, or other fluids, with the exception of medicines and vitamin or mineral drops.
Infant: a child younger than 1 year of age.
Infant mortality rate: probability of dying between birth and exactly 1 year of age, expressed per 1,000 live births.
Moderate malnutrition: a weight-for-age height with –3 to –2 z-scores below the median for the World Health Organization child-growth standards due to wasting, stunting, or both.
Stunting: moderate malnutrition due to low height-for-age with –3 to –2 z-scores below the median for the World Health Organization child-growth standards.
Mortality under age 5 years: probability of dying between birth and exactly 5 years of age, expressed per 1,000 live births.
Wasting: moderate malnutrition due to low weight-for-height with –3 to –2 z-scores below the median for the World Health Organization child-growth standards.
Weaning: the process of switching an infant’s diet from breast milk or formula to other foods and fluids.
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.