Back to Journals » Nature and Science of Sleep » Volume 13
Relationships Between a Range of Inflammatory Biomarkers and Subjective Sleep Quality in Chronic Insomnia Patients: A Clinical Study
Authors Xia L, Zhang P ![]() , Niu JW, Ge W, Chen JT
, Niu JW, Ge W, Chen JT ![]() , Yang S
, Yang S ![]() , Su AX
, Su AX ![]() , Feng YZ
, Feng YZ ![]() , Wang F, Chen G
, Wang F, Chen G ![]() , Chen GH
, Chen GH ![]()
Received 12 March 2021
Accepted for publication 6 July 2021
Published 12 August 2021 Volume 2021:13 Pages 1419—1428
DOI https://doi.org/10.2147/NSS.S310698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Lan Xia,1,* Ping Zhang,2,* Jing-Wen Niu,2 Wei Ge,2 Jun-Tao Chen,2 Shuai Yang,2 Ai-Xi Su,2 Yi-Zhou Feng,2 Fang Wang,3 Gong Chen,4 Gui-Hai Chen2
1Department of Neurology, The Second Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2Department of Neurology (Sleep Disorders), The Affiliated Chaohu Hospital of Anhui Medical University, Hefei (Chaohu), People’s Republic of China; 3Department of Neurology, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 4Hefei Technology College, Hefei (Chaohu), People’s Republic of China
*These authors contributed equally to this work
Correspondence: Gui-Hai Chen
Department of Neurology (Sleep Disorders), The Affiliated Chaohu Hospital of Anhui Medical University, Hefei (Chaohu), People’s Republic of China
Tel/Fax +86-551-82321571
Email [email protected]
Gong Chen
Hefei Technology College, Hefei (Chaohu), People’s Republic of China
Tel +86-551-82367072
Fax +86-551-82351650
Email [email protected]
Purpose: To examine whether associations exist between chronic insomnia disorder (CID) and overlooked inflammatory factors (Serum amyloid protein A [SAA]), tumor necrosis factor [TNF]-α, granulocyte-macrophage colony-stimulating factor [GM-CSF], and regulated on activation and normal T cell expressed and presumably secreted [RANTES]).
Patients and Methods: A total of 65 CID patients and 39 sex- and age-matched good sleeper (GS) controls participated in this study. They completed a baseline survey to collect data on demographics, and were elevated sleep and mood by Pittsburgh Sleep Quality Index (PSQI), Athens Insomnia Scale (AIS), 17-item Hamilton Depression Rating Scale (HAMD-17) and 14-item Hamilton Anxiety Rating Scale (HAMA-14), respectively. The blood samples were collected and tested the serum levels of SAA, TNF-α, GM-CSF and RANTES.
Results: The CID group had higher serum levels of SAA, TNF-α, and GM-CSF and a lower level of RANTES than the GS group. In the Spearman correlation analysis, SAA and GM-CSF positively correlated with the PSQI and AIS scores. After controlling for sex, HAMD-17 score, and HAMA-14 score, the partial correlation analysis showed that GM-CSF was positively correlated with PSQI score. Further stepwise linear regression analyses showed that GM-CSF was positively associated with the PSQI and AIS scores, while RANTES was negatively associated with them, and SAA was positively associated with just the AIS score.
Conclusion: The serum levels of inflammatory mediators (SAA, TNF-α, and GM-CSF) were significantly elevated and the level of RANTES was significantly decreased in CID patients and, to some extent, the changes are related to the severity of insomnia. These findings may help us to improve interventions to prevent the biological consequences of CID by inhibiting inflammation, thereby promoting health.
Keywords: chronic insomnia disorder, serum amyloid protein A; tumor necrosis factor (TNF)-α, granulocyte-macrophage colony-stimulating factor, regulated on activation and normal T cell expressed and presumably secreted
Introduction
In the general population, about a third of individuals have sleep complaints, and nearly 10% fulfill the diagnostic criteria for chronic insomnia disorder (CID).1 CID has a strong impact on quality of life and is a risk factor for the development of other disorders, including psychological disease,2,3 cardiovascular disease,4 diabetes,5 certain cancers,6 obesity,7 and functional decline. This has substantial public health implications. In recent years, sleep research has increasingly focused on the biological mechanisms underlying these associations between insomnia and somatic diseases,8–10 with substantial attention on the effect of chronic sleep loss on inflammation.
Compelling evidence has demonstrated that sleep disturbance (defined as difficulty initiating or maintaining sleep) and shorter sleep duration are associated with elevated inflammatory biomarkers, which may be linked to increased risk of chronic diseases.11–13 A systematic review and meta-analysis of 72 studies (n > 50,000) examined associations between insomnia and the proinflammatory markers interleukin (IL)-6 and the acute-phase protein C-reactive protein (CRP).14 The results showed that insomnia assessed based on self-reported symptoms was associated with higher levels of IL-6 but not CRP, while insomnia assessed by questionnaire was associated with higher levels of both IL-6 and CRP.14 However, other studies found that insomnia symptoms were associated with elevated CRP but not IL-6 in young adults.15,16 Other inflammatory factors that have frequently been explored in insomnia are tumor necrosis factor (TNF)-α and IL-1β, with associations between elevated levels and poor sleep quality.17–20 However, several other studies have shown no associations of insomnia with TNF-α and IL-1β.21,22 In brief, previous studies on insomnia and inflammation have predominantly focused on CRP, IL-6, TNF-α, and IL-1β, with slightly varying findings. These varying findings may be a result of inconsistent assessment of insomnia symptoms and different age group compositions. Importantly, the changes in other kinds of inflammatory factors remain unclear. To fill this knowledge gap, examining insomnia–inflammation associations based on a range of inflammatory biomarkers is warranted.
Inflammatory factors include ILs, colony-stimulating factors, TNFs, and chemokines.23 Granulocyte-macrophage colony-stimulating factor (GM-CSF) is best viewed as a major regulator governing the functions of granulocyte and macrophage lineage populations at all stages of maturation, playing a key role in inflammation.24 There is a mutual dependence between GM-CSF activity and monocyte or macrophage-derived proinflammatory cytokine activity, such as IL-1 and TNF-α activity.25 Regulated on activation and normal T cell expressed and presumably secreted (RANTES; also known as C-C motif chemokine ligand 5 [CCL5]) is a chemokine.26 IL-1β has been shown to upregulate RANTES and GM-CSF mRNA in all fibroblast lines.27 TNF-α and IL-1β were found to be altered in insomnia patients.17–20 However, there is no research on the changes in GM-CSF and RANTES in insomnia patients. In addition, acute-phase proteins are blood proteins that can be used to assess inflammation. These proteins undergo changes in their serum concentrations by >25% in response to proinflammatory cytokine release during disease processes.28 Serum amyloid protein A (SAA) and CRP are the most prominent members of the acute-phase response. SAA gene transcription is mainly induced by lipopolysaccharide and cytokines, including IL-6, IL-1, and TNF-α; the most prominent proinflammatory activities of SAA include the induction of the synthesis of pro-IL-1β.29 SAA has been implicated in several chronic inflammatory diseases, such as rheumatoid arthritis and cardiovascular disease,30 and a study reported elevated SAA in the plasma of patients with clinical depression relative to healthy controls.31 The changes in SAA in patients with CID have not been explored.
In this study, we sought to examine whether associations exist between insomnia and the overlooked inflammatory factors (SAA, TNF-α, GM-CSF, and RANTES), to further understand the changes in inflammatory factors in CID patients.
Patients and Methods
Sample and Ethics Approval
Sixty-five patients (27 males and 38 females) with CID were recruited over a 6-month period from the Clinic of Sleep Disorder at the Affiliated Chaohu Hospital of Anhui Medical University. The CID patients had a mean age of 41.4±12.1 years (range, 18 to 60). The inclusion criteria were as follows: 1) complaints of sleep difficulty with enough time and proper environment for sleep accompanied by impairment of daytime functions; and 2) diagnosed based on the International Classification of Sleep Disorders (Third Edition) criteria,32 all the participants met criterion as listed in the ICSD-3 insomnia definition. The exclusion criteria were as follows: 1) taking antidepressants, antipsychotics, hypnotics and antibiotics within 2 weeks; 2) noncooperation or unable to complete the questionnaires due to vision and hearing impairment; 3) chronic inflammatory diseases, organic brain diseases, drug abuse, or other serious medical conditions; 4) comorbid with other mental disorders; and 5) pregnant or lactating. Thirty-nine good sleeper (GS) controls with no sleep or mood complaints and similar medical history were recruited from the Center of Health Examination in the same hospital during the corresponding period in order to reduce the differences in regions and study period. Good sleepers (19 males and 20 females) had a mean age of 42.2±14.3 years, with Pittsburgh Sleep Quality Index (PSQI) score < 7, Athens Insomnia Scale (AIS) score < 4, 17-item Hamilton Depression Rating Scale (HAMD-17) score < 7, and 14-item Hamilton Anxiety Rating Scale (HAMA-14) score < 7. The study was conducted in accordance with the Declaration of Helsinki, and it was approved by the Ethics Committee of the Affiliated Chaohu Hospital of Anhui Medical University. All subjects provided signed informed consent before study commencement.
Data Collection
Baseline Data Collection
We chose the appropriate assessment scales from our preliminary experiments. Before the beginning of the study, all the researchers were well trained to be familiar with the whole process of the survey and the instruction of the scale, and the standard of evaluation was unified, in order to ensure the consistency of methods of data collection and scales assessment. Demographic data, including sex, age, illness duration, and education level, were collected. HAMD-17 and HAMA-14 were used to evaluate depression and anxiety, respectively, as they are the most frequently used scales for this purpose. Sleep quality was assessed by PSQI and AIS. PSQI is a standard scale assessing sleep quality based on recalling sleep behaviors in the past month, consisting of subjective sleep quality, sleep latency, sleep duration, sleep efficiency, somnipathy, use of hypnotic drugs, and diurnal dysfunction.33 The total score ranges from 0 to 21 and, in China, a score ≥ 7 has high diagnostic sensitivity and specificity for distinguishing patients with poor sleep from normal subjects.34 AIS was modified in 2000 according to the International Classification of Diseases (ICD)-10 system.35 It is used to assess sleep quality in the prior month, and is suitable for evaluating sleep quality and monitoring treatment effects in patients with sleep disorders and mental disorders. There are eight items on the scale: sleep onset, night and early-morning waking, sleep time, sleep quality, frequency and duration of complaints, distress caused by the experience of insomnia, and interference with daily functioning. Each item is rated from 0 to 3, and the total score ranges from 0 to 24, and the score ≥ 6 being classified as insomnia. The higher the score, the worse the sleep.34
Serum Levels of TNF-α, RANTES, SAA, and GM-CSF
Elbow intravenous blood was collected between 7:00 and 9:00 a.m., with fasting and avoidance of strenuous activity and mental stimulation. The samples were separated immediately by centrifugation and the serum was frozen at –80°C. The serum levels of TNF-α, RANTES, SAA, and GM-CSF were assessed using a RayBiotech Chip Detection Test (Peachtree Corners, GA, USA) according to the manufacturer’s instructions by the simultaneous processing at last. All the samples were tested twice and got the average when the results were similar; otherwise, they would be retested and calculated again in order to reduce the test error.
Statistical Analysis
We checked and reviewed the data carefully and chose the correct statistical analysis methods. Statistical analyses were performed using IBM SPSS Statistics version 22.0 software (SPSS, Chicago, IL). Extreme values were deleted if they were higher than “mean + 3 SD” or lower than “mean – 3 SD”. The data were then assessed using normality plots. Normally distributed data are expressed as mean ± standard deviation, and differences between groups were assessed using t-tests. Non-normally distributed data are expressed as P50 (P25, P75), differences between groups were assessed using Mann–Whitney U-tests and the chi-square test was used to compare sex differences between groups. In order to discriminate between confounding factors and their influence, Spearman correlation analysis, partial correlation analysis, and stepwise linear regression were used to explore the associations between the serum levels of inflammatory factors and the sleep quality. In addition, receiver operating characteristics (ROC) analysis was performed to compare the diagnostic information provided by different inflammatory factors, according to the calculated area under the curve (AUC), optimal cut-off points, sensitivity, and specificity. The AUCs at 0.9 indicated that these inflammatory factors had high diagnostic value. Two-tailed P<0.05 was considered to be statistically significant.
Results
Baseline Characteristics
There were no significant differences in age (t = 0.299, P = 0.766), sex (χ2 = 0.509, P = 0.475), or education level (Z = 0.306, P = 0.760) between the CID and GS groups. The PSQI, AIS, HAMD-17, and HAMA-14 scores were significantly higher in the CID group than the GS group (P < 0.001) (Table 1).
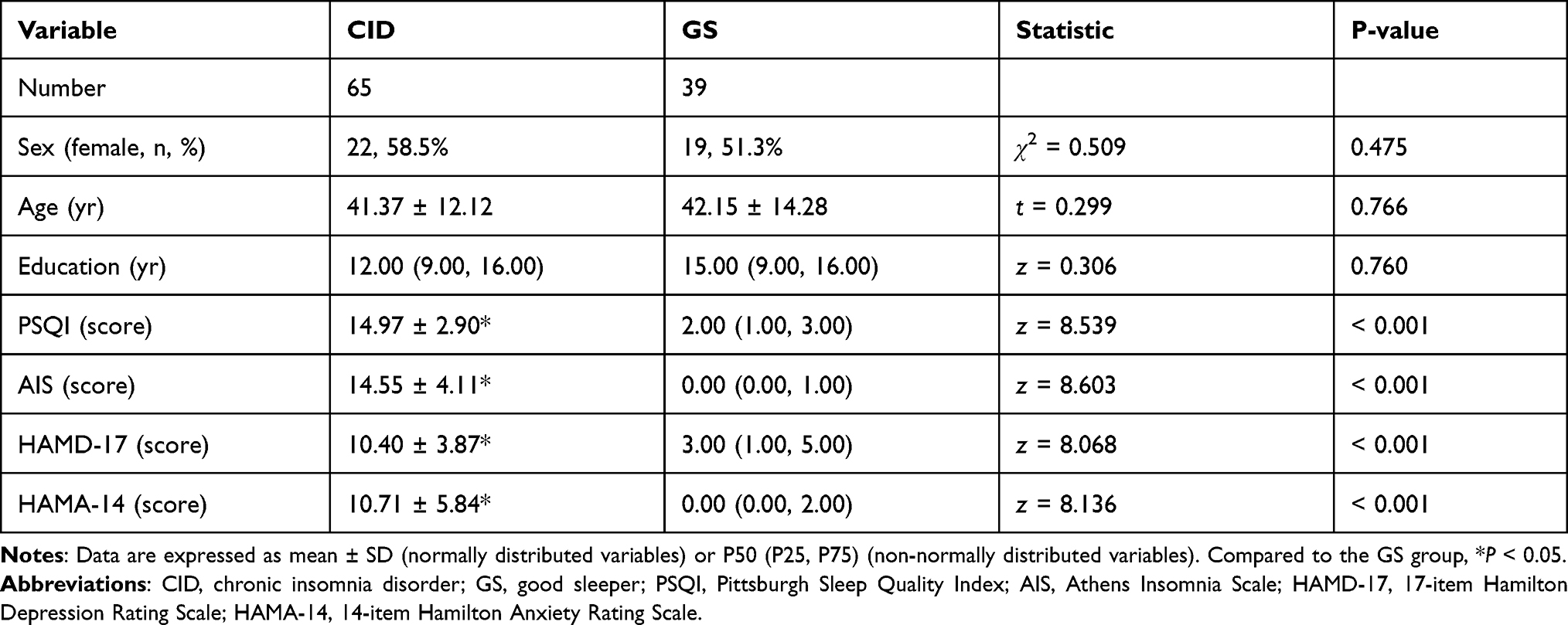 |
Table 1 Demographic and Clinical Characteristics of Participants |
TNF-α, RANTES, SAA, and GM-CSF Levels
Compared to the GS group, the serum levels of TNF-α, SAA, and GM-CSF were significantly higher in the CID group, while the RANTES level was lower (P < 0.05, Table 2).
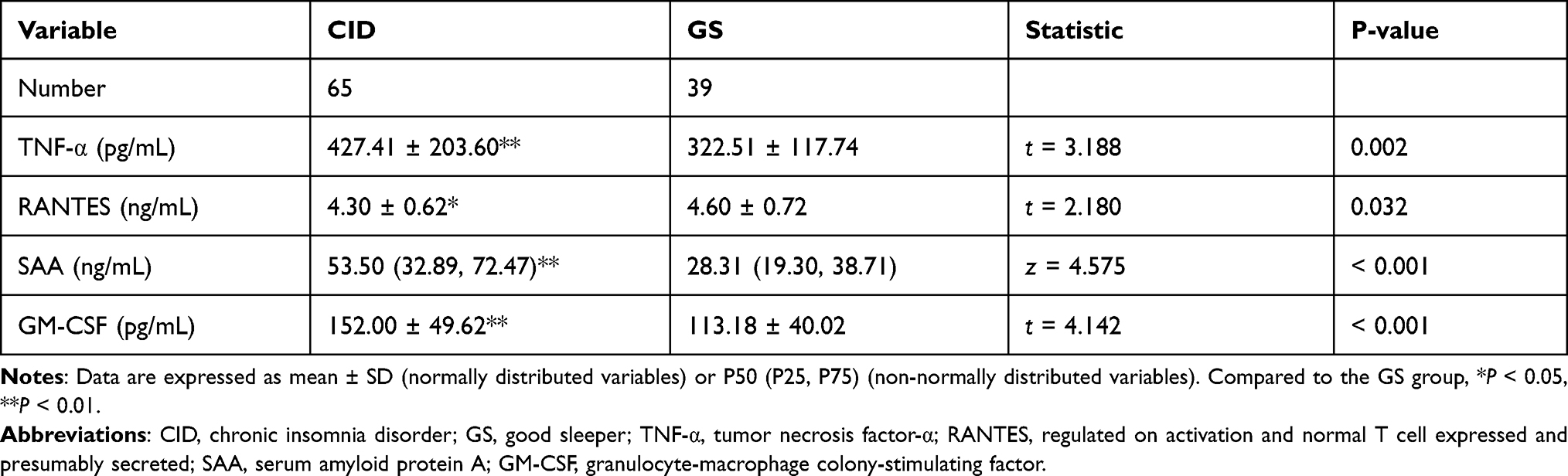 |
Table 2 TNF-α, RANTES, SAA and GM-CSF Levels in Participants |
Correlations of RANTES, SAA, GM-CSF, and TNF-α with Mood
In the Spearman correlation analyses, sex, the PSQI score, the AIS score and the serum levels of SAA and GM-CSF were positively correlated with the HAMD-17 and HAMA-14 scores (P < 0.05), and the TNF-α serum level was also positively correlated with the HAMD-17 score (P < 0.05). After controlling for sex, PSQI, and AIS scores, the partial correlation analyses showed that there was no relationship between the serum levels of inflammatory factors (SAA, TNF-α, GM-CSF, and RANTES) and the HAMD-17 and HAMA-14 scores (P > 0.05). Furthermore, the linear regression method by stepwise showed that HAMD-17 and HAMA-14 scores were positively associated with the AIS score (P < 0.05). HAMD-17 score was also positively associated with PSQI score (P < 0.05, see Table 3).
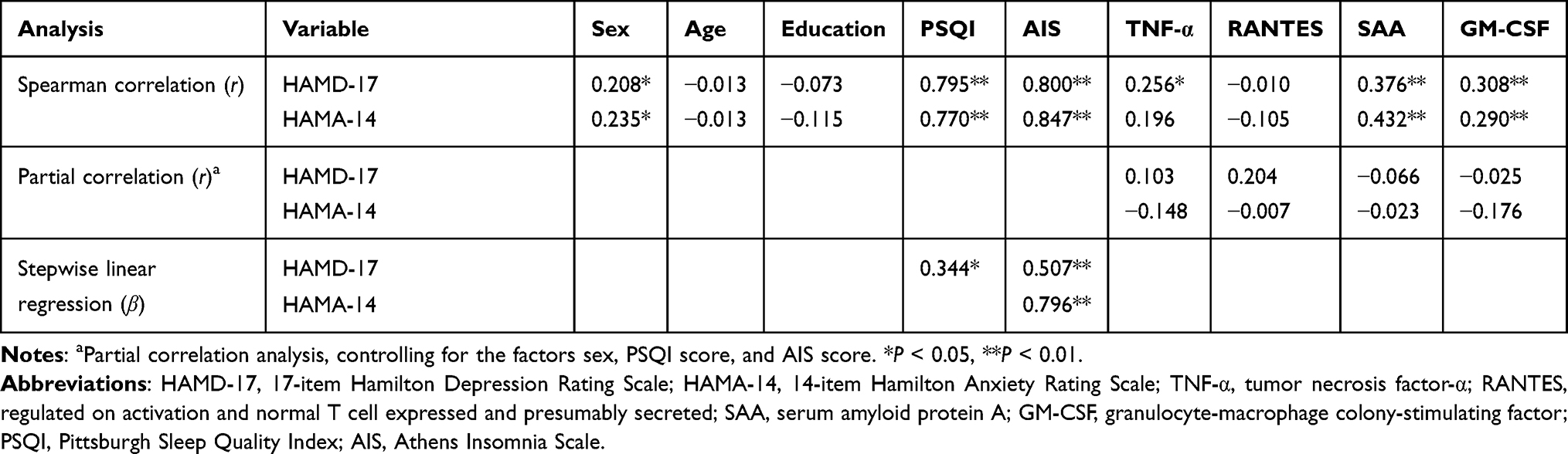 |
Table 3 Correlations of RANTES, SAA, GM-CSF, and TNF-α with Mood |
Correlations of RANTES, SAA, GM-CSF, and TNF-α with Sleep Quality/Insomnia Severity
In the Spearman correlation analyses, sex, HAMD-17 score, HAMA-14 score, and the serum levels of SAA and GM-CSF were positively correlated with the PSQI and AIS scores (P < 0.05). After controlling for sex, HAMD-17, and HAMA-14 scores, the partial correlation analyses showed that the serum level of GM-CSF was positively correlated with the PSQI score (P < 0.05). Furthermore, stepwise linear regression showed that PSQI and AIS scores were positively associated with HAMD-17 and HAMA-14 scores and GM-CSF and negatively associated with RANTES (P < 0.05). AIS score was also positively associated with SAA (P < 0.05, see Table 4).
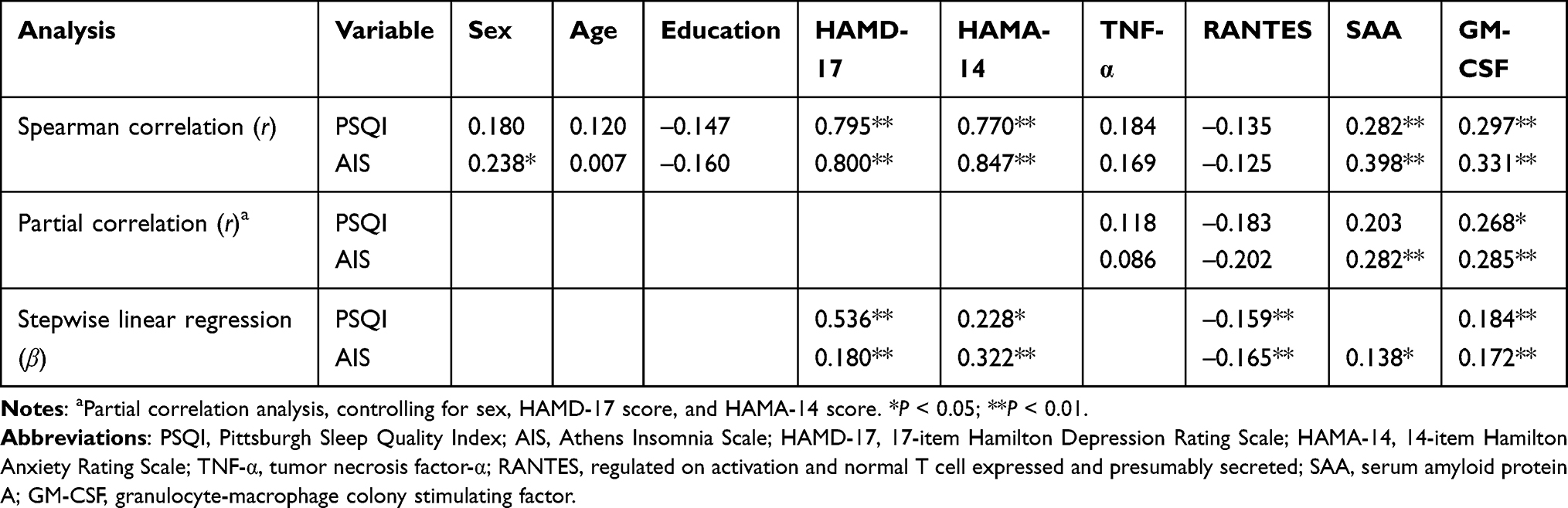 |
Table 4 Correlations of RANTES, SAA, GM-CSF, and TNF-α with Insomnia |
Potential Blood Biomarkers of CID Based on Receiver Operating Characteristic (ROC) Curve Analyses
Regarding the ROC curve analyses, the sensitivity, specificity, and area under the curve (AUC) values are shown in Table 5. The AUCs of TNF-α, RANTES, SAA, and GM-CSF for differentiating between CID and GS were all > 0.60. The optimal cut-off values were 367.12 pg/mL, 3.81 ng/mL, 52.09 g/mL, and 133.46 pg/mL, respectively.
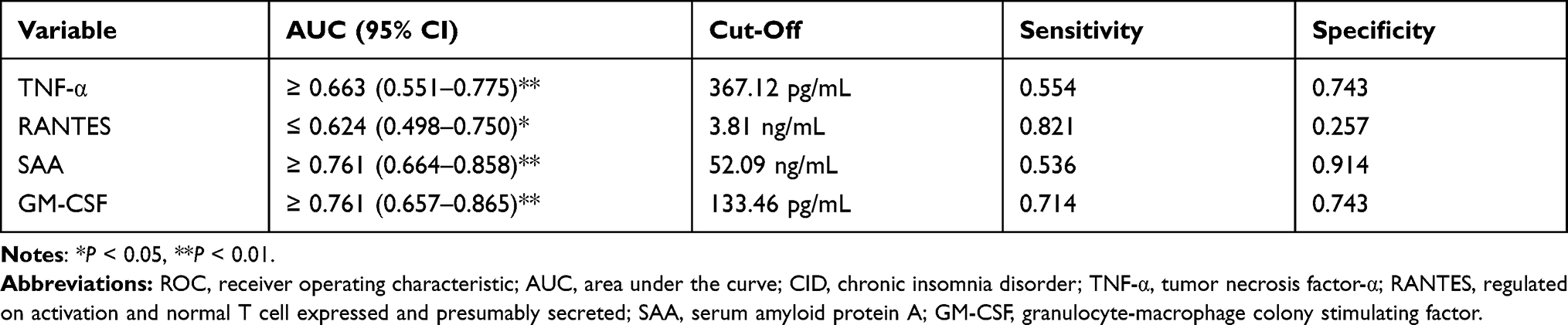 |
Table 5 ROC Curve Analysis Results Regarding Potential Blood Biomarkers of CID |
Discussion
These Inflammatory Factors Were Altered in Patients with CID
This study examined the associations between insomnia and a range of inflammatory biomarkers in a cohort of 65 CID patients and 39 GS controls. We found that the levels of inflammatory mediators (SAA, TNF-α, and GM-CSF) in the CID patients were significantly elevated, while RANTES was significantly lower than in GS controls. Higher serum SAA and GM-CSF levels were significantly associated with higher total scores on the PSQI and AIS.
Previous studies have shown there was a strong relationship between inflammatory cytokines and depression and anxiety. For example, there was an increase in serum levels of TNF-α, IL-6, IL-13, IL-18, IL-12, IL-1RA, sTNFR2, CCL2 (MCP-1), CXCL4, and CXCL7, and a decrease in IFN-γ and CCL4 in people suffering from depression.36 It has been well established that a significant proportion of patients with anxiety-related disorders exhibit evidence of elevated inflammatory markers, including increases in cerebrospinal fluid and blood concentrations of inflammatory cytokines and acute-phase reactants, such as IL-1, IL-6, TNFs and their soluble receptors, and C-reactive protein.37 In the current study, we found that the CID patients had not only higher levels of SAA, TNF-α and GM-CSF, and lower levels of RANTES (Table 2) but also higher levels if depression and anxiety (Table 1). Moreover, the Spearman correlation showed that the serum levels were positively correlated with both depressive and anxious scores in SAA and GM-CSF, and with depressive scores in TNF-α (Table 3). These findings appeared to suggest that the changed levels of detected inflammatory cytokines are the results from changed emotional states, at least partially. However, our data from Partial correlation and Stepwise linear regression indicated that the internal connection with SAA, GM-CSF, RANTES only occurred in insomnia but not in emotion (Tables 3 and 4). The cause might be that the severity of depression and anxiety was too mild to result in alteration of immune states.
Why did SAA exhibit robust associations with insomnia severity in our study? SAA is a powerful proinflammatory regulator, reciprocally interacting with multiple aspects of the inflammatory cascade.38,39 It binds to and activates multiple structurally diverse receptors that mediate inflammation, including Toll-like receptors 2 and 4 (TLR2/TLR4), formyl peptide receptor-like 1 (FPRL1), and receptor for advanced glycation end products (RAGE).30 Through activation of these receptors, SAA has been shown to induce the secretion of the proinflammatory cytokines TNF-α, IL-6, IL-8, IL-23, and IL-18 and of the anti-inflammatory cytokine IL-10 in monocytes, macrophages, neutrophils, and fibroblasts. In addition, SAA is able to induce the secretion of mature IL-1β by providing the two signals needed for its production: binding to TLR2/TLR4 and activation of the NLR family pyrin domain-containing 3 (NLRP3) inflammasome in macrophages, dendritic cells, neutrophils, and mast cells. It is important to highlight that a growing body of the literature has evaluated the associations between elevated levels of IL-6, IL-1β, and TNF-α in people with insomnia symptoms, with slightly varying findings.17–20 Other reports found that two nights of total sleep deprivation increased SAA, which may be related to the onset of subclinical inflammation, weight gain, and insulin resistance in both mice and humans.38,40 This increase may be due to increased SAA production or reduced SAA clearance. In short, most of the previous studies involved artificial sleep restriction under experimental conditions or people with insomnia symptoms but without a diagnosis of CID. Our study, for the first time, found an elevated serum level of SAA in CID patients in a natural state. SAA has been suggested to play a role in obesity and insulin resistance.39 In addition, an elevated serum level of SAA is an independent and strong predictor of coronary artery disease and adverse cardiovascular outcomes.38 Our findings may improve the understanding of the signaling linking CID to its associated comorbidities, such as obesity, type 2 diabetes, and cardiovascular disease.
It is currently not known whether the SAA in the peripheral circulation can cross the blood–brain barrier (BBB) and enter the central nervous system. Peripheral inflammation can increase BBB permeability, so it is possible that peripherally produced SAA may influence the development of insomnia symptoms either by crossing the BBB itself or by inducing other inflammatory factors that then may cross the BBB. To investigate the role of SAA in the brain, Yu et al examined the effects of recombinant human SAA on primary cultures of microglia and astrocytes.41 They found that SAA was able to stimulate the production of IL-6, TNF-α, and other cytokines in microglia and astrocytes. SAA reduced the viability of astrocytes by inducing G1 cell cycle arrest. In addition, our previous study showed that CID patients had significantly increased serum levels of astrocyte biomarkers and we speculated that CID patients may have pathological changes in their astrocytes.42,43 It is therefore possible that SAA, produced in the central or peripheral nervous system, could influence the development of insomnia symptoms by activating microglial cells and inducing proinflammatory cytokine production. It is important to note that this study only cross-sectionally investigated the levels of potential biomarkers in CID patients. It is therefore not possible to draw any conclusions based on this study as to whether SAA is causally involved in the pathogenesis of CID.
This study demonstrated that the level of TNF-α, which is a proinflammatory cytokine, increased in CID patients. The enhanced TNF-α in the CID patients at least partially stems from increased SAA, as SAA can upregulate several proinflammatory cytokines, including IL-1β, IL-6, IL-8, and TNF-α.44 TNF plays a role in sleep regulation and its sleep-related effectors and actions. Substantial evidence from young healthy animals indicates that acute enhancement or inhibition of endogenous brain TNF promotes or inhibits sleep, respectively.45–47 Research has shown that TNF-α can improve non-rapid eye movement sleep,48 while the inhibition of TNF-α reduces spontaneous sleep. In addition, TNF-α is considered part of a larger biochemical cascade involved in sleep regulation; other somnogenic substances in this cascade include growth hormone-releasing hormone and nitric oxide.49 Notably, in most human studies on TNF and sleep, pathological conditions have been found to be associated with chronic elevations of systemic TNF and disrupted sleep. The chronic sleep disruption and shortening of sleep duration that occur in insomnia patients suggest that the chronicity of sleep loss across weeks or even years is an important factor in altering circulating TNF-α levels.50 Further research is needed to determine the changes in TNF levels in patients with different degrees and subtypes of insomnia.
GM-CSF is a hematopoietic cytokine that may affect various functions of the central nervous system, as the molecule and its receptors are expressed in the brain.51 We assessed the GM-CSF levels in CID patients for the first time, and we found that insomnia patients had significantly higher GM-CSF than GS controls, and GM-CSF positively correlated with the severity of insomnia. GM-CSF is not a proinflammatory cytokine produced immediately after the onset of infection or inflammation. Rather, it is induced as a result of the proinflammatory cytokine activation cascade, involving somnogenic IL-152 and TNF-α.53 SAA can also upregulate GM-CSF.44 The human body is a complex physiological entity, with various inflammatory factors influencing each other. The chronic process of insomnia is an important factor leading to changes in the levels of many circulating cytokines.
RANTES is classified as a chemokine and is a chemoattractant of T cells, eosinophils, and basophils, recruiting leukocytes into inflammatory sites.54 Apart from its widely known role in human immunodeficiency virus infection, RANTES plays a role in inflammation in patients with obstructive sleep apnea,55,56 which manifests as a positive association between RANTES and Apnea–Hypopnea Index (AHI) in adults. A recent study found that sleep deprivation was associated with a potential decrease in the RANTES/CXCL9 ratio, which is related to changes in the Th1-related chemokine balance.57 Our study, for the first time, detected the serum level of RANTES in CID patients and found that it was negatively correlated with the severity of insomnia.
The Possible Diagnostic and Prognostic Value of These Inflammatory Biomarkers
ROC analysis was used to calculate the cut-off values of different inflammatory biomarkers to discriminate between true and false CID diagnosis as established by the ICSD-3 criteria. The results showed that the AUCs of all four inflammatory biomarkers were over 0.6 between patients with CID and GS. The optimal cut-off values for TNF-α, SAA and GM-CSF indicated that subjects should be considered to have CID if their inflammatory biomarkers levels were above the corresponding cut-off values. The optimal cut-off values for RANTES indicated that subjects should be considered to have CID if their inflammatory biomarkers levels were lower than the corresponding cut-off values. These results might provide strong cues for considering CID relative to healthy sleep, implying the possibility that these serum indexes act as objective diagnostic markers for CID. Combining these four indicators may provide a more specific and sensitive method to better manage and offer more accurate prognosis of patients with CID.
Limitations
There are several limitations in this study. The inflammatory factors were only measured at initial presentation rather than being tracked during the treatment of insomnia. Additionally, this study is an exploratory analysis based on a relatively small sample. The limited statistical power due to the sample size means that we cannot accurately determine the different contributions of each inflammatory factor to insomnia. In future research, a larger sample size is needed to increase the statistical power. Finally, our analysis was limited to the serum levels of the inflammatory factors, and we were unable to assess the association between the inflammatory factors and complications caused by insomnia. The study findings should motivate further investigations into the inflammatory mechanisms underlying the effects of CID, which will have implications for cardiovascular and other chronic inflammatory disorders in insomnia patients.
Conclusions
In summary, our data showed that the levels of inflammatory mediators (SAA, TNF-α, and GM-CSF) were significantly elevated, while the level of RANTES decreased in CID patients and, to some extent, these changes are related to the severity of insomnia. In the future, we can verify the roles of these inflammatory mediators (SAA, TNF-α, GM-CSF, and RANTES) in the mechanism of insomnia by animal experiments, and find the interventions of preventing the biological consequences of CID by inhibiting inflammation. As a result, the health of insomnia will be improved.
Acknowledgments
We would like to thank the Neurology (Sleep Disorders), the Affiliated Chaohu Hospital of Anhui Medical University for their support during data collection. Gong Chen and Gui-Hai Chen are co-correspondence authors for this study.
Funding
This work was financially supported by the National Natural Science Foundation of China (81671316), and the Natural Science Foundation of Anhui Medical University (2018xkj066).
Disclosure
The authors have indicated no conflicts of interest.
References
1. Chung KF, Yeung WF, Ho FY, Yung KP, Yu YM, Kwok CW. Cross-cultural and comparative epidemiology of insomnia: the diagnostic and statistical manual (DSM), international classification of diseases (ICD) and international classification of sleep disorders (ICSD). Sleep Med. 2015;16(4):477–482. doi:10.1016/j.sleep.2014.10.018
2. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135(1–3):10–19. doi:10.1016/j.jad.2011.01.011
3. Riemann D, Voderholzer U. Primary insomnia: a risk factor to develop depression? J Affect Disord. 2003;76(1–3):255–259. doi:10.1016/s0165-0327(02)00072-1
4. Palagini L, Bruno RM, Gemignani A, Baglioni C, Ghiadoni L, Riemann D. Sleep loss and hypertension: a systematic review. Curr Pharm Des. 2013;19(13):2409–2419. doi:10.2174/1381612811319130009
5. Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO. Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev. 2013;17(4):241–254. doi:10.1016/j.smrv.2012.09.005
6. Shi T, Min M, Sun C, Zhang Y, Liang M, Sun Y. Does insomnia predict a high risk of cancer? A systematic review and meta-analysis of cohort studies. J Sleep Res. 2020;29(1):e12876. doi:10.1111/jsr.12876
7. Nixon JP, Mavanji V, Butterick TA, Billington CJ, Kotz CM, Teske JA. Sleep disorders, obesity, and aging: the role of orexin. Ageing Res Rev. 2015;20:63–73. doi:10.1016/j.arr.2014.11.001
8. Johansson M, Jansson-Fröjmark M, Norell-Clarke A, Linton SJ. The role of psychiatric and somatic conditions in incidence and persistence of insomnia: a longitudinal, community study. Sleep Health. 2016;2(3):229–238. doi:10.1016/j.sleh.2016.05.004
9. Hsieh CG, Martin JL. Short sleep, insomnia, and cardiovascular disease. Curr Sleep Med Rep. 2019;5(4):234–242. doi:10.1007/s40675-019-00157-8
10. Thomas SJ, Calhoun D. Sleep, insomnia, and hypertension: current findings and future directions. J Am Soc Hypertens. 2017;11(2):122–129. doi:10.1016/j.jash.2016.11.008
11. Patel SR, Zhu X, Storfer-Isser A, et al. Sleep duration and biomarkers of inflammation. Sleep. 2009;32(2):200–204. doi:10.1093/sleep/32.2.200
12. Matthews KA, Zheng H, Kravitz HM, et al. Are inflammatory and coagulation biomarkers related to sleep characteristics in mid-life women? Study of women’s health across the Nation Sleep Study. Sleep. 2010;33(12):1649–1655. doi:10.1093/sleep/33.12.1649
13. Hale L, Parente V, Dowd JB, et al. Fibrinogen may mediate the association between long sleep duration and coronary heart disease. J Sleep Res. 2013;22(3):305–314. doi:10.1111/jsr.12020
14. Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. 2016;80(1):40–52. doi:10.1016/j.biopsych.2015.05.014
15. Slavish DC, Graham-Engeland JE, Engeland CG, Taylor DJ, Buxton OM. Insomnia symptoms are associated with elevated C-reactive protein in young adults. Psychol Health. 2018;33(11):1396–1415. doi:10.1080/08870446.2018.1500577
16. Fernandez-Mendoza J, Baker JH, Vgontzas AN, Gaines J, Liao D, Bixler EO. Insomnia symptoms with objective short sleep duration are associated with systemic inflammation in adolescents. Brain Behav Immun. 2017;61:110–116. doi:10.1016/j.bbi.2016.12.026
17. Satyanarayanan SK, Chien YC, Chang JP, et al. Melatonergic agonist regulates circadian clock genes and peripheral inflammatory and neuroplasticity markers in patients with depression and anxiety. Brain Behav Immun. 2020;85:142–151. doi:10.1016/j.bbi.2019.03.003
18. Lu Y, Wang X, Yang G, Liu X, Xu M. Effects of chronic intractable insomnia on inflammatory cytokines, blood pressure characteristics, and antihypertensive efficacy in hypertensive patients. Med Sci Monit. 2018;24:9259–9264. doi:10.12659/MSM.911997
19. Rethorst CD, Greer TL, Toups MS, Bernstein I, Carmody TJ, Trivedi MH. IL-1β and BDNF are associated with improvement in hypersomnia but not insomnia following exercise in major depressive disorder. Transl Psychiatry. 2015;5(8):e611. doi:10.1038/tp.2015.104
20. Li H, Chen Y, Wu H, et al. Relationship between serum IL-1β and insomnia and liver depression in patients with perimenopausal non-organic sleep disorder. Exp Ther Med. 2019;17(1):759–763. doi:10.3892/etm.2018.6990
21. Bower JE, Ganz PA, Irwin MR, Kwan L, Breen EC, Cole SW. Inflammation and behavioral symptoms after breast cancer treatment: do fatigue, depression, and sleep disturbance share a common underlying mechanism? J Clin Oncol. 2011;29(26):3517–3522. doi:10.1200/JCO.2011.36.1154
22. Walker JL, Slavish DC, Dolan M, et al. Age-dependent associations among insomnia, depression, and inflammation in nurses. Psychol Health. 2020:1–18. doi:10.1080/08870446.2020.1805450
23. Shrihari TG. Dual role of inflammatory mediators in cancer. Ecancermedicalscience. 2017;11:721. doi:10.3332/ecancer.2017.721
24. Hamilton JA. GM-CSF in inflammation. J Exp Med. 2020;217(1):e20190945. doi:10.1084/jem.20190945
25. Lee KMC, Achuthan AA, Hamilton JA. GM-CSF: a promising target in inflammation and autoimmunity. Immunotargets Ther. 2020;9:225–240. doi:10.2147/ITT.S262566
26. Akoum A, Lemay A, Maheux R. Estradiol and interleukin-1beta exert a synergistic stimulatory effect on the expression of the chemokine regulated upon activation, normal T cell expressed, and secreted in endometriotic cells. J Clin Endocrinol Metab. 2002;87(12):5785–5792. doi:10.1210/jc.2002-020106
27. Nonaka M, Pawankar R, Saji F, Yagi T. Distinct expression of RANTES and GM-CSF by lipopolysaccharide in human nasal fibroblasts but not in other airway fibroblasts. Int Arch Allergy Immunol. 1999;119(4):314–321. doi:10.1159/000024209
28. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999;340(6):448–454. doi:10.1056/NEJM199902113400607
29. Migita K, Koga T, Satomura K, et al. Serum amyloid A triggers the mosodium urate -mediated mature interleukin-1β production from human synovial fibroblasts. Arthritis Res Ther. 2012;14(3):R119. doi:10.1186/ar3849
30. Eklund KK, Niemi K, Kovanen PT. Immune functions of serum amyloid A. Crit Rev Immunol. 2012;32(4):335–348. doi:10.1615/CritRevImmunol.v32.i4.40
31. Wang Q, Su X, Jiang X, et al. iTRAQ technology-based identification of human peripheral serum proteins associated with depression. Neuroscience. 2016;330:291–325. doi:10.1016/j.neuroscience.2016.05.055
32. Morin CM, Drake CL, Harvey AG, et al. Insomnia disorder. Nat Rev Dis Primers. 2015;1(1):15026. doi:10.1038/nrdp.2015.26
33. Buysse DJ, Reynolds CF
34. Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:52–73. doi:10.1016/j.smrv.2015.01.009
35. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens insomnia scale: validation of an instrument based on ICD-10 criteria. J Psychosom Res. 2000;48(6):555–560. doi:10.1016/s0022-3999(00)00095-7
36. Lee CH, Giuliani F. The role of inflammation in depression and fatigue. Front Immunol. 2019;10:1696. eCollection 2019. doi:10.3389/fimmu.2019.01696
37. Jennifer CF. Imaging the role of inflammation in mood and anxiety-related disorders. Curr Neuropharmacol. 2018;16(5):533–558. doi:10.2174/1570159X15666171123201142
38. Sack GH
39. Zhang Y, Zhang J, Sheng H, Li H, Wang R. Acute phase reactant serum amyloid A in inflammation and other diseases. Adv Clin Chem. 2019;90:25–80.
40. de Oliveira EM, Visniauskas B, Tufik S, Andersen ML, Chagas JR, Campa A. Serum amyloid A production is triggered by sleep deprivation in mice and humans: is that the link between sleep loss and associated comorbidities? Nutrients. 2017;9(3):311. doi:10.3390/nu9030311
41. Yu Y, Liu J, Li SQ, Peng L, Ye RD. Serum amyloid a differentially activates microglia and astrocytes via the PI3K pathway. J Alzheimers Dis. 2014;38:133–144. doi:10.3233/JAD-130818
42. Zhang P, Tan CW, Chen GH, et al. Patients with chronic insomnia disorder have increased serum levels of neurofilaments, neuron-specific enolase and S100B: does organic brain damage exist? Sleep Med. 2018;48:163–171. doi:10.1016/j.sleep.2017.12.012
43. Zhang P, Li YX, Zhang ZZ, et al. Astroglial mechanisms underlying chronic insomnia disorder: a Clinical Study. Nat Sci Sleep. 2020;12:693–704. doi:10.2147/NSS.S263528
44. Song C, Hsu K, Yamen E, et al. Serum amyloid A induction of cytokines in monocytes/macrophages and lymphocytes. Atherosclerosis. 2009;207(2):374–383. doi:10.1016/j.atherosclerosis.2009.05.007
45. Churchill L, Rector DM, Yasuda K, et al. Tumor necrosis factor alpha: activity dependent expression and promotion of cortical column sleep in rats. Front Immunol. 2019;10:1696.
46. Jewett KA, Taishi P, Sengupta P, Roy S, Davis CJ, Krueger JM. Tumor necrosis factor enhances the sleep-like state and electrical stimulation induces a wake-like state in co-cultures of neurons and glia. Eur J Neurosci. 2015;42(4):2078–2090. doi:10.1111/ejn.12968
47. Karrer M, Lopez MA, Meier D, et al. Cytokine-induced sleep: neurons respond to TNF with production of chemokines and increased expression of Homer1a in vitro. Brain Behav Immun. 2015;47:186–192. doi:10.1016/j.bbi.2014.11.008
48. Shoham S, Davenne D, Cady AB, Dinarello CA, Krueger JM. Recombinant tumor necrosis factor and interleukin 1 enhance slow-wave sleep. Am J Physiol. 1987;253(1 Pt 2):R142–R149. doi:10.1152/ajpregu.1987.253.1.R142
49. Krueger JM, Fang J, Taishi P, Chen Z, Kushikata T, Gardi J. Sleep. A physiologic role for IL-1 beta and TNF-alpha. Ann N Y Acad Sci. 1998;856:148–159. doi:10.1111/j.1749-6632.1998.tb08323.x
50. Haack M, Pollmächer T, Mullington JM. Diurnal and sleep-wake dependent variations of soluble TNF- and IL-2 receptors in healthy volunteers. Brain Behav Immun. 2004;18(4):361–367. doi:10.1016/j.bbi.2003.12.009
51. Kimura M, Kodama T, Aguila MC, Zhang SQ, Inoue S. Granulocyte-macrophage colony-stimulating factor modulates rapid eye movement (REM) sleep and non-REM sleep in rats. J Neurosci. 2000;20(14):5544–5551. doi:10.1523/JNEUROSCI.20-14-05544.2000
52. Henricson BE, Neta R, Vogel SN. An interleukin-1 receptor antagonist blocks lipopolysaccharide-induced colony-stimulating factor production and early endotoxin tolerance. Infect Immun. 1991;59(3):1188–1191. doi:10.1128/iai.59.3.1188-1191.1991
53. Duru F, Ertem U, Taçyildiz N, Kirazli S. Production of granulocyte colony stimulating factor, granulocyte macrophage colony stimulating factor, and tumor necrosis factor alpha during remission and infections in patients with acute leukemia. J Med. 1995;26(5–6):241–252.
54. Arnaud C, Beguin PC, Lantuejoul S, et al. The inflammatory preatherosclerotic remodeling induced by intermittent hypoxia is attenuated by RANTES/CCL5 inhibition. Am J Respir Crit Care Med. 2011;184(6):724–731. doi:10.1164/rccm.201012-2033OC
55. Chuang HH, Huang CG, Chuang LP, et al. Relationships among and predictive values of obesity, inflammation markers, and disease severity in pediatric patients with obstructive sleep apnea before and after adenotonsillectomy. J Clin Med. 2020;9(2):579. doi:10.3390/jcm9020579
56. Testelmans D, Tamisier R, Barone-Rochette G, et al. Profile of circulating cytokines: impact of OSA, obesity and acute cardiovascular events. Cytokine. 2013;62(2):210–216. doi:10.1016/j.cyto.2013.02.021
57. Said EA, Al-Abri MA, Al-Saidi I, et al. Sleep deprivation alters neutrophil functions and levels of Th1-related chemokines and CD4+ T cells in the blood. Sleep Breath. 2019;23(4):1331–1339. doi:10.1007/s11325-019-018511
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.