Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Relationship of COPD Exacerbation Severity and Frequency on Risks for Future Events and Economic Burden in the Medicare Fee-For-Service Population
Authors Sethi S ![]() , Make BJ
, Make BJ ![]() , Robinson SB
, Robinson SB ![]() , Kumar S, Pollack M
, Kumar S, Pollack M ![]() , Moretz C, Dreyfus J, Xi A, Powell D
, Moretz C, Dreyfus J, Xi A, Powell D ![]() , Feigler N
, Feigler N
Received 19 November 2021
Accepted for publication 21 February 2022
Published 20 March 2022 Volume 2022:17 Pages 593—608
DOI https://doi.org/10.2147/COPD.S350248
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Sanjay Sethi,1 Barry J Make,2 Scott B Robinson,3 Shambhavi Kumar,3 Michael Pollack,4 Chad Moretz,5 Jill Dreyfus,5 Ann Xi,5 Dakota Powell,5 Norbert Feigler4
1University at Buffalo, Buffalo, NY, USA; 2National Jewish Health, Denver, CO, USA; 3Avalere, Health Economics and Advanced Analytics, Washington, DC, USA; 4AstraZeneca, Biopharmaceuticals Medical, Wilmington, DE, USA; 5Formerly Avalere, Washington, DC, USA
Correspondence: Michael Pollack, Health Economics and Payer Evidence-Global, 1800 Concord Pike, Wilmington, DE, 19850, USA, Tel +1 302-886-1253, Email [email protected]
Purpose: To quantify the effects of moderate and/or severe chronic obstructive pulmonary disease (COPD) exacerbations on future exacerbations and healthcare costs in Medicare Fee-For-Service beneficiaries.
Patients and Methods: A retrospective cohort study of patients ≥ 40 years of age, with continuous enrollment from 2015 to 2018, with an index COPD diagnosis defined as first hospitalization, emergency department visit, or first of two outpatient visits (≥ 30 days apart) in 2015 with a claim for chronic bronchitis, emphysema, or chronic airway obstruction. Patients were stratified by baseline exacerbation categories in year one (YR1) and subsequently evaluated in YR2 and YR3: (A) none; (B) 1 moderate; (C) ≥ 2 moderate; (D) 1 severe; and (E) ≥ 2, one being severe. Moderate exacerbations were defined as COPD-related outpatient/ED visits with a corticosteroid/antibiotic claim within ± 7 days of the visit and severe exacerbations as hospitalizations with a primary COPD diagnosis. Total all-cause costs for Categories B-E were compared to reference Category A using generalized linear models and inflation adjusted to 2019 dollars.
Results: A total of 1,492,108 patients met study criteria with a mean (±SD) age of 70.9± 10.9. In YR1, nearly 40% of patients experienced ≥ 1 moderate and/or severe exacerbations. Patients having multiple exacerbations, regardless of severity were 2– 4 times more likely to experience an exacerbation during YR2 and YR3. Adjusted costs ranged between $24,000 and $26,600 for all categories for YR2 and YR3. Adjusted YR2 costs for Category D and E were $1421 and $1548 higher than those without an exacerbation (Category A YR2 $25,084, YR3 $24,282; p< 0.0001). The respective YR3 adjusted costs were $2062 and $2117 higher than those without an exacerbation (Category A; p< 0.0001), representing an increase of 6– 8% and 8– 9% for YR2 and YR3.
Conclusion: Medicare patients with recent moderate or severe exacerbations, or at least two exacerbations per year are at significant risk for future exacerbations and incur higher all-cause costs.
Keywords: chronic obstructive pulmonary disease, exacerbations, medicare, maintenance therapy, costs
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity, mortality, and disability with a high economic burden.1–4 According to 2018 CDC estimates, the age adjusted COPD prevalence for the US population aged 45 years or older was 9.7%.5 The estimated number of diagnosed cases that were projected for the United States in 2020 was 16 million with patient-related costs of $49 billion.6 The clinical course of COPD is often complicated by exacerbations and episodes of worsening respiratory symptoms,7 which contribute to disease progression and are significant drivers for healthcare resource utilization (HRU) and treatment costs.2,8–10 Exacerbations, mostly triggered by bacterial or viral infections and possibly by other factors such as eosinophilic airway inflammation, environmental pollution, and nonadherence to maintenance medications, result in high HRU from frequent physician office visits, hospitalizations, chronic oxygen use, and medication needs.11,12 A single severe exacerbation can be associated with significant decline in lung function and increased risk for future hospitalizations.13,14 Moreover, a single moderate exacerbation increases the risk of future multiple exacerbation events leading to further disease progression and increased risk of death.15 Between 29–47% of patients with COPD experience at least one exacerbation annually.16 Chronic comorbidities, commonly reported in patients with COPD, can be worsened by an exacerbation event resulting in an additional driver for increased hospitalizations, deaths, and costs.17,18 This is particularly true for cardiovascular complications with more than 4 times the increased risk of a cardiovascular event 30 days after moderate/severe exacerbation and 10 times the increased risk of a cardiovascular event 30 days after exacerbation requiring hospitalization.19
Much of the published literature related to the burden of COPD exacerbations has primarily focused on combined categories of moderate and severe exacerbations, typically stratifying patients as experiencing frequent (two or more events per patient-year) versus infrequent (none or one) exacerbations or focused on populations of patients with COPD in specific settings such as administrative database and prospective observational cohort studies.2,8,14–16,18,20,21 Few studies have evaluated the impact of moderate events only, cumulative exacerbation events effect in causing further exacerbations, or focused on the incremental burden related to an increasing number of exacerbation events. Even fewer studies have assessed the burden of exacerbations and costs in the larger Medicare population, with findings mostly limited to the Medicare Advantage population or a nationally representative 5% of the Medicare Fee-For-Service (FFS) claims data.20
Availability of the 100% Medicare FFS claims data, representing 69% of Medicare beneficiaries in 2015,22 provides a unique opportunity to address this important knowledge gap in older patients within this population whose management is complicated by the presence of comorbidities, challenges of polypharmacy, and physical and cognitive disabilities.23 The overall goal of this study was to understand the real–world rates of COPD exacerbations among the 100% Medicare FFS population and associated economic burden. The specific objectives were to 1) quantify type and frequency of COPD exacerbations over three years by prior exacerbation history; 2) identify demographics and comorbidities of these patients; 3) assess prescribed treatments; and 4) report total all-cause health care utilization costs.
Methods
Study Design and Data Source
This retrospective cohort study utilized the 100% Medicare Fee-For-Service (FFS) claims data to identify patients with COPD, COPD exacerbations, treatments, and health care utilization. Access to the 100% Medicare FFS claims was permitted through a research-focused data use agreement with the Centers for Medicare & Medicaid Services (CMS) and did not require Institutional Review Board approval due to use of de-identified patient/member data. Inpatient and outpatient claims were derived from Medicare Parts A and B and prescription drug event data from Part D. Claims data included admission and discharge dates, dates of service for emergency department (ED), inpatient, outpatient or physician office visits, diagnoses and procedure codes, source of care, date of death, and demographic data.24
Patient Population
Patients included in the study were ≥40 years of age with at least one inpatient visit, or one ED visit, or two outpatient medical visits at least 30 days apart between January 1, 2015 and December 31, 2015 with a diagnosis code for COPD (chronic bronchitis, emphysema, or chronic airway obstruction) in any position on the claim. Diagnosis or procedure codes captured prior to October 1, 2015 used International Classification of Disease, 9th Revision (ICD-9): 490, 492.xx, 496; and on or after October 1, 2015 used International Classification of Disease, 10th Revision (ICD-10): J40.xx-J44.xx (xx indicates a wildcard designating any subcodes under the 3-digit code). Additionally, patients with a prior COPD diagnosis during a 12-month look-back period between January 1, 2014 and December 31, 2014 were flagged for use in adjusted analysis. Patients were required to have 36 months of continuous enrollment for medical (Parts A and B) and pharmacy benefits (Part D) from the index date to identify COPD-related exacerbations and study outcomes over the 36-month period; therefore, patients who died during the study period were excluded. Patients with a diagnosis of interstitial fibrosis and sarcoidosis in the first 12 months after the index date were excluded. Figure 1 summarizes patient attrition and study timeline between January 1, 2014 and December 31, 2018.
 |
Figure 1 Attrition Diagram and Study Timeline. The attrition diagram presents the inclusion and exclusion criteria used to select the study patient population with a COPD diagnosis date in 2015. The study timeline includes a 12-month look back period in 2014; baseline history of exacerbations in YR1; and post-index exacerbations in YR2 and YR3. |
Exacerbation Categories
The number and severity of exacerbations were assessed in baseline year one (YR1) after the index COPD diagnosis and subsequent post-index YR2 and YR3. Moderate exacerbations were defined as an outpatient or emergency department (ED) visit with a primary diagnosis of COPD and prescription claim for an antibiotic or systemic corticosteroid within 7 days of the visit. Severe exacerbations were defined as a hospitalization with a primary diagnosis of COPD. ED visits resulting in an inpatient stay were counted as a hospitalization. The end date of the exacerbation episode is defined as the last observed exacerbation event date or inpatient discharge date plus 14 days. Exacerbation events occurring within 14 days of each other were considered a single exacerbation episode and classified according to the highest severity contributing event. The first 12 months (baseline YR1) was used to classify patients into one of five exacerbation Categories (Cat A-Cat E): 0 exacerbations (Cat A); 1 moderate only (Cat B); ≥2 moderate only (Cat C); 1 severe only (Cat D); and ≥2 exacerbations, one being severe (Cat E). Months 13–24 (post-index YR2) and 25–36 (post-index YR3) were used to assess rates and risks of future exacerbations.
Study Variables and Covariates
The exposure variable was the severity and frequency of exacerbations during baseline YR1, as defined by the Categories A-E. Baseline demographics and comorbidities were identified during baseline YR1. Treatments were also identified during baseline YR1 and reported for overall study patients and by exacerbation categories. Demographics included age, gender, race, US census region, low-income subsidy, dual eligibility, and reason for Medicare entitlement (ie, age ≥65 or disability/end-stage renal disease). Low-income subsidy Medicare patients include those with a limited income and resources and receive state financial assistance to pay for Medicare premiums.25 Dual eligibility patients include those enrolled in Medicare and receive full Medicaid benefits.26 The Deyo-modified Charlson Comorbidity Index (CCI) score for overall health care status was calculated based on 17 comorbidities.27 The most frequent identified chronic conditions and exacerbation risk factors commonly reported in patients with COPD (tobacco dependence, other respiratory conditions, gastroesophageal reflux disease, metabolic and cardiovascular conditions, sleep apnea, cancer, and anxiety/depression) also were captured.17,18,28
Exacerbations
To determine if exacerbations in the baseline year predicted exacerbations in subsequent years, patients in Categories A-E in baseline YR1 were compared for differences in severity and number of exacerbations in post-index YR2 and YR3. A Sankey diagram was utilized to visualize transition between the five categories from YR1 to YR2 and YR3.29 Frequency of moderate and severe exacerbations were determined and rate per 100-patient-years reported for post-index YR2 and YR3. Percent of patients with single and multiple (≥2) exacerbations also were determined and similarly reported. Adjusted rate ratios for exacerbations in post-index YR2 and YR3 were calculated as described in the Statistical Analysis Section.
Pharmacological Treatments
To capture pharmacological treatments for COPD treatment, prescriptions of inhaled and systemic corticosteroids; bronchodilators (individual and combination products): long-acting muscarinic antagonists (LAMA) and long-acting beta2 agonists (LABA), short-acting muscarinic antagonists (SAMA) and short-acting beta2 agonists (SABA); antibiotics; and supplemental oxygen therapy were identified from National Drug Codes and Current Procedural Terminology/Healthcare Common Procedure Coding System. Patients may have received more than one class of medication and reported treatments are presented as percentage of patients having a prescription fill for that drug class. Baseline YR1 predated the availability of closed triple therapy.
Costs
Unadjusted and adjusted medical and pharmacy all-cause costs were determined for post-index years for each exacerbation category. Costs were inflation-adjusted to 2019 US dollars using the Consumer Price Index30 and represent the sum of Medicare payment amount and beneficiary out of pocket expenses. All-cause medical expenditures included inpatient; ED and outpatient visits, inclusive of primary care and pulmonologist office visits. All-cause pharmacy costs included any Part D medications filled and reimbursed by Medicare. COPD-related pharmacy expenditures included antibiotics, oral corticosteroids, short-acting bronchodilators, and long-acting maintenance therapy. Maintenance therapy included inhaled corticosteroids (ICS), LAMA, and LABA as individual components and combination therapy.
Statistical Analysis
Descriptive statistics were presented using means and standard deviation for continuous variables and frequencies and proportions for categorical variables. Patient characteristics, comorbidities, and treatments as well as cost outcomes for those with exacerbations (Cat B-E) were compared to those with no exacerbations during baseline YR1 (Cat A) using univariate statistical methods. Two sample t-test compared continuous variables, and chi-square test compared categorical variables. Unadjusted costs were reported using means and standard deviations. Adjusted analyses were performed on exacerbation and cost outcomes with Category A serving as the reference category. Generalized linear models (GLM) and models with log link and gamma distribution were used to adjust for patient, comorbidity, and treatment covariates (Tables 1 and 2) using backward selection (p<0.10) to determine final models.
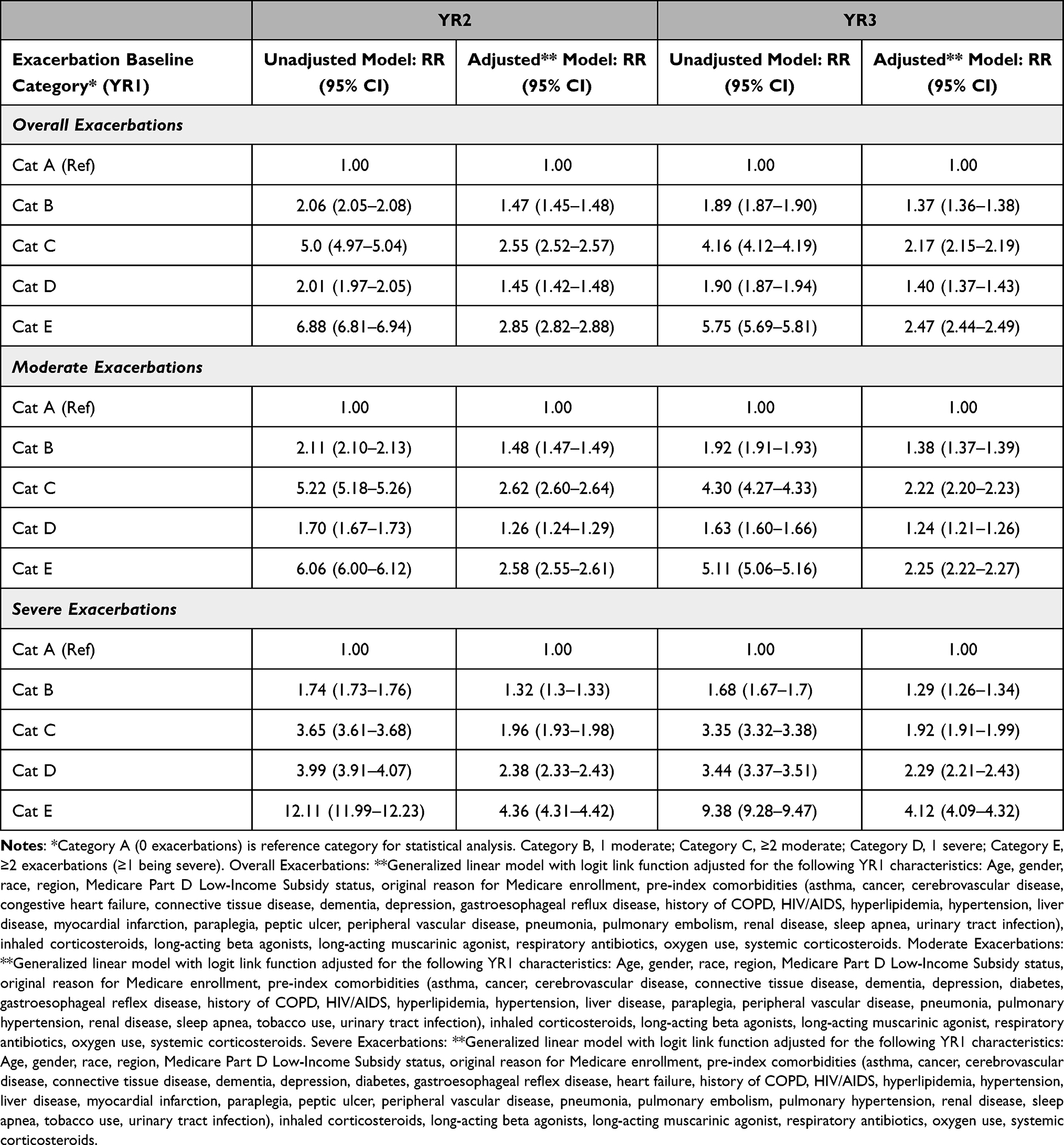 |
Table 1 Unadjusted and Adjusted Rate Ratios for Overall, Moderate and Severe Exacerbations in Post-Index YR2 and YR3 by Baseline YR1 Exacerbation Category |
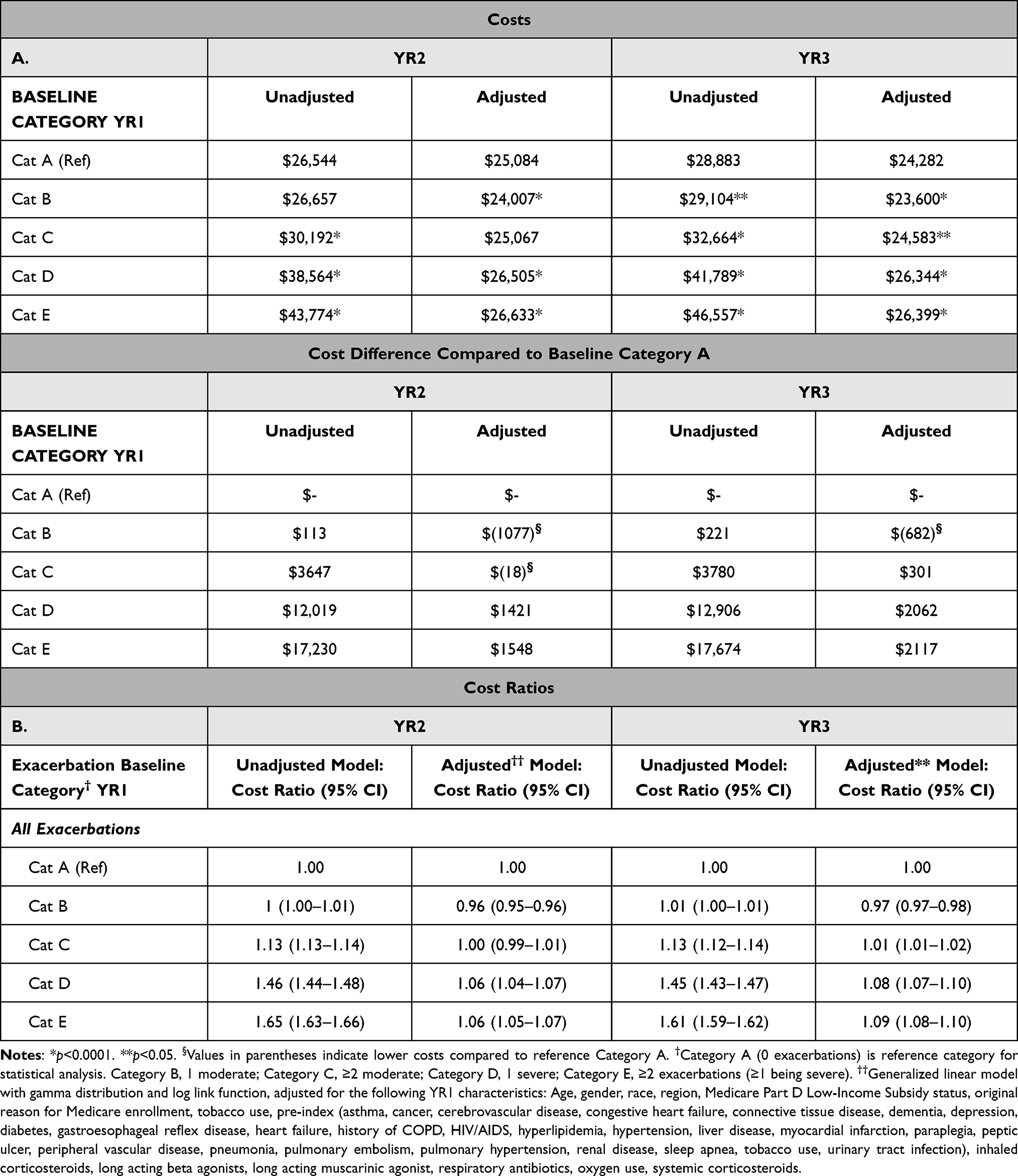 |
Table 2 Unadjusted and Adjusted All-Cause Costs (A) and Cost Ratios (B) for Exacerbation Categories B–E versus Category a in Post-Index YR2 and YR3 by Baseline YR1 Exacerbation Category |
All analyses performed using SAS Enterprise Guide 7.1 (SAS Institute; Cary, North Carolina) and SQL Aginity Workbench. The Sankey Diagram was created in RStudio version 1.1.456 (Boston, Massachusetts). Statistical significance was defined as p<0.05.
Results
Patient, Clinical, and Treatment Characteristics
A total of 3,738,000 patients had a COPD diagnosis during 2015, and 1,492,108 patients met full inclusion criteria (Figure 1). Statistically significant differences were observed for all patient and clinical characteristics of interest in Categories B through E, compared to reference Cat A (Table 3A and B; p<0.05). Overall mean (±SD) age was 70.9 (±10.9) years, with patients having one severe exacerbation being oldest (Cat D: 72.6 (±11.3)) years. Females comprised 58.6% of all COPD patients and more often had multiple exacerbations with at least one being severe (Cat E: 64.6%) (Table 3A). Black patients comprised 8.8% of patients overall but displayed higher percentages in categories that included at least one severe exacerbation (Cat D: 12.2%; Cat E: 9.8%). Severe exacerbation categories (D and E) also had the highest percentages of patients who were dual eligible and qualified for low-income subsidies (Table 3A). In addition, patients in those categories had the highest mean (±SD) CCI scores (Cat D: 5.0 (±3.0); Cat E: 4.6 (±2.9) and higher proportions of patients with individual comorbidities of interest, particularly asthma, cardiovascular, diabetes mellitus, pneumonia, and tobacco dependence (Table 3B).
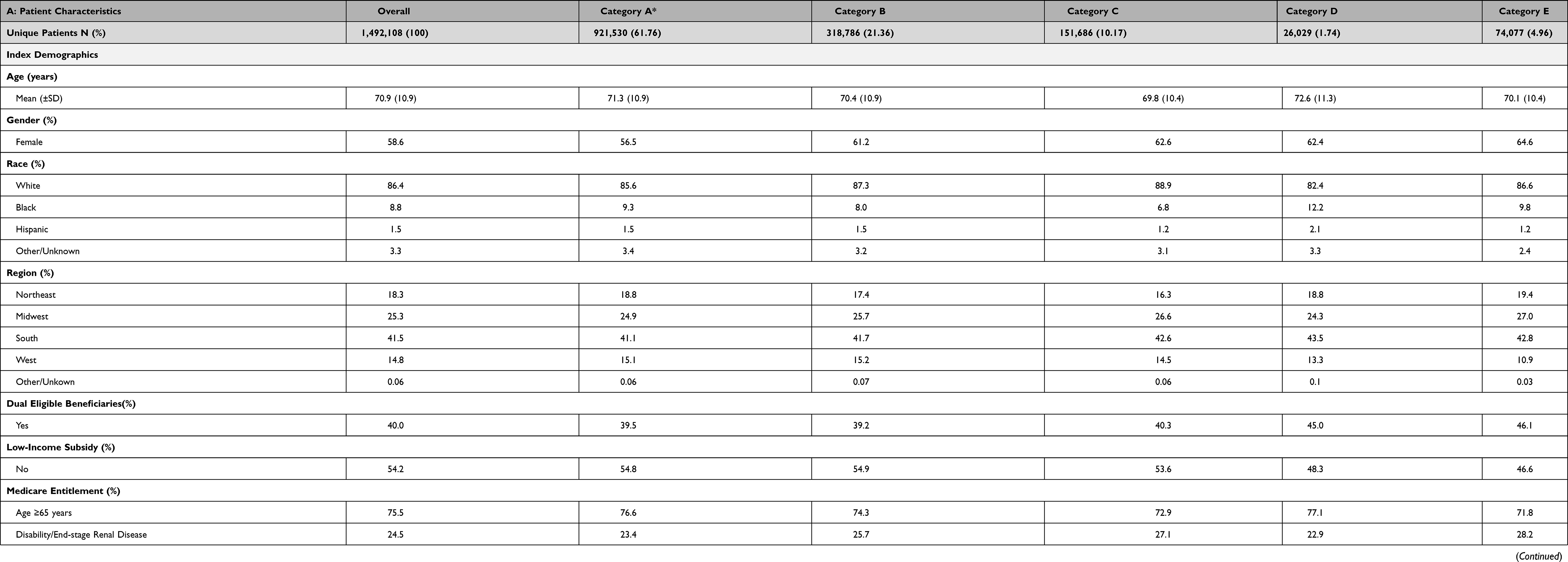 |
Table 3 Patient (A) and Clinical (B) Characteristics at Index Diagnosis Date at Baseline YR1 for Overall Chronic Obstructive Pulmonary Disease Cohort and for Exacerbation Categories A–E |
Overall Exacerbations by Categories
Overall, 61.8% of patients were found not to have an exacerbation (Cat A) in baseline YR1 with 31.5% having only moderate exacerbations (Cat B and Cat C) and 6.7% experiencing at least one severe exacerbation (Cat D and E) (Table 3A). Changes in exacerbation categories over time were observed. Among the patients without exacerbations (Cat A) in baseline YR1, 81.6% and 79.8% of patients continued to have no exacerbations in YR2 and YR3, respectively (Figure 2). Among those with 1 moderate (Cat. B) or 1 severe exacerbation (Cat D) in YR1, >30% continued to have 1 or more exacerbations in YR2 and YR3 (Figure 2). The majority (>58%) of patients with multiple exacerbations (Cat C and Cat E) in YR1 continued to have exacerbations over the following two years (Figure 2).
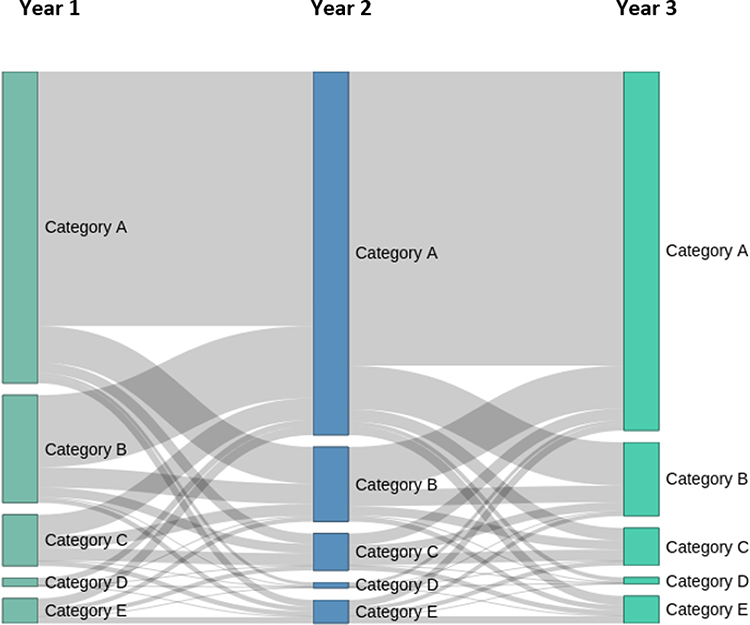 |
Figure 2 Changes in exacerbation Categories A-E for Baseline YR1 and Post-Index YR2 and YR3. Exacerbation rates are displayed in the Sankey diagram, which visualizes transition between the five exacerbation categories from YR1 to YR2 to YR3. The width at each time point is proportional to the number of patients in the category. Exacerbations were defined as 0 (Category A), 1 moderate (Category B); ≥2 moderate (Category C); 1 severe (Category D); ≥2 exacerbations, at least one being severe (Category E). |
Although 61.8% of patients (Cat A) did not have an exacerbation in YR1, this group accounted for 31.7% of all the exacerbation events in YR2, of which 13.4% were severe. Results for this group were found to be relatively consistent for YR3 as well, accounting for 37.6% of total exacerbation events, indicating that patients with no events in YR1 still contributed substantially to the burden of COPD exacerbations over the next two years. While 5% of the population was in Cat E in baseline, they accounted for just over 17% of all events in YR2 and YR3, and approximately 24% of these events were severe.
Exacerbations by Severity and Frequency
Figure 3 depicts exacerbation rates and severity of events in YR2 and YR3 by patient category. In YR2, there were a total of 779,750 exacerbation events equating to an overall rate of 52.3 per 100-patient-years, of which 85.9% were moderate and 14.1% were severe. In YR3, there were 836,494 events equating to an overall rate of 56.1 per 100-patient-years with 84% moderate and 15.8% severe. Figure 4 depicts exacerbation frequency by patient category. In YR2, overall, 28% of patients had at least one exacerbation, 16.0% of patients had a single exacerbation, and 12.0% had multiple exacerbations with YR3 showing similar results. The rate, severity type, and frequency of exacerbations was observed to be highest among patients with greater baseline YR1 events (Cat C and Cat E).
 |
Figure 3 Moderate and Severe Exacerbation Rates Per 100-Patient-Years. The bar graph depicts the moderate and severe exacerbation rates per 100-patient-years for the overall cohort and by baseline exacerbation Categories A–E for post-index YR2 and YR3. Exacerbations were defined as 0 (Category A), 1 moderate (Category B); ≥2 moderate (Category C); 1 severe (Category D); ≥2 exacerbations, at least one being severe (Category E). |
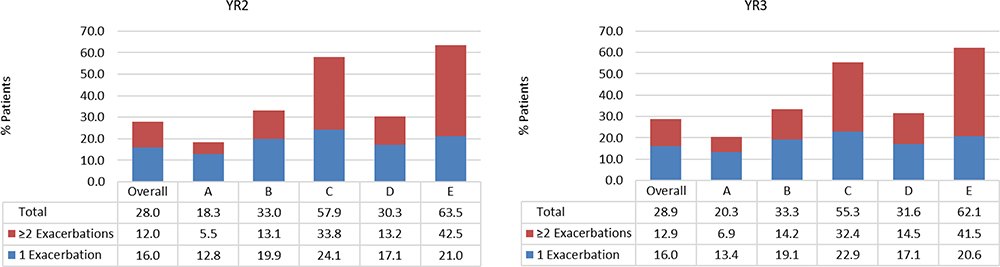 |
Figure 4 Percent of Patients with Single and Multiple Exacerbations. The bar graph depicts the percentage of patients with 1 and ≥2 exacerbations for the overall cohort and by baseline exacerbation Categories A-E for post-index YR2 and YR3. Exacerbations were defined as 0 (Category A), 1 moderate (Category B); ≥2 moderate (Category C); 1 severe (Category D); ≥2 exacerbations, at least one being severe (Category E). |
Adjusted Analysis of Exacerbations
After adjusting for baseline characteristics, individuals with exacerbations of any severity during baseline YR1 were significantly associated with greater rates of exacerbations in YR2 and YR3 (Table 1). Those with at least 1 moderate (Cat B) or severe (Cat D) exacerbation during baseline YR1 had similarly higher exacerbation rates of approximately 1.4 times relative to Cat A in YR2 and YR3 (Table 1). Those with multiple exacerbations in baseline YR1 (Cat C and Cat E) had over 2 times the rate of exacerbations in YR2 and YR3 relative to Cat A (Table 1). The increased risk for moderate exacerbations for Cat B-Cat E relative to Cat A followed a pattern similar to that for the overall exacerbations. However, the risk for severe exacerbations in YR2 and YR3 among those with a severe exacerbation in YR1 (Cat D and Cat E) were 2 to 4 times higher compared to those with no exacerbations (Cat A) in YR1 (Table 1).
Pharmacological Treatment Outcomes
Approximately 60% of patients with no exacerbations at baseline (Cat A) received no long-acting maintenance therapy over the 3-year period (Table 4). When considering use of short-acting and oral corticosteroids, 30% of patients did not receive these or long-acting treatments (Table 4). While greater use of any COPD treatment was observed as the number and severity of baseline exacerbations increased, a notable percentage of patients (between 21% and 55%) did not have any long-acting maintenance therapy over the three-year study period despite experiencing exacerbations in YR1 (Table 4). Among those with 1 exacerbation in YR1 (Cat B and D), approximately 50% (Cat B: 46% to 49%, Cat D: 48% to 55%) did not receive long-acting maintenance during each study year (Table 4). While use of long-acting maintenance was more common among those with multiple exacerbation events in YR1, a large percentage of both categories (Cat C: 30% to 35% and CatE: 21% to 28%) did not receive any long-acting maintenance therapy (Table 4). These findings highlight the undertreatment of patients with exacerbations, particularly those with severe exacerbations.
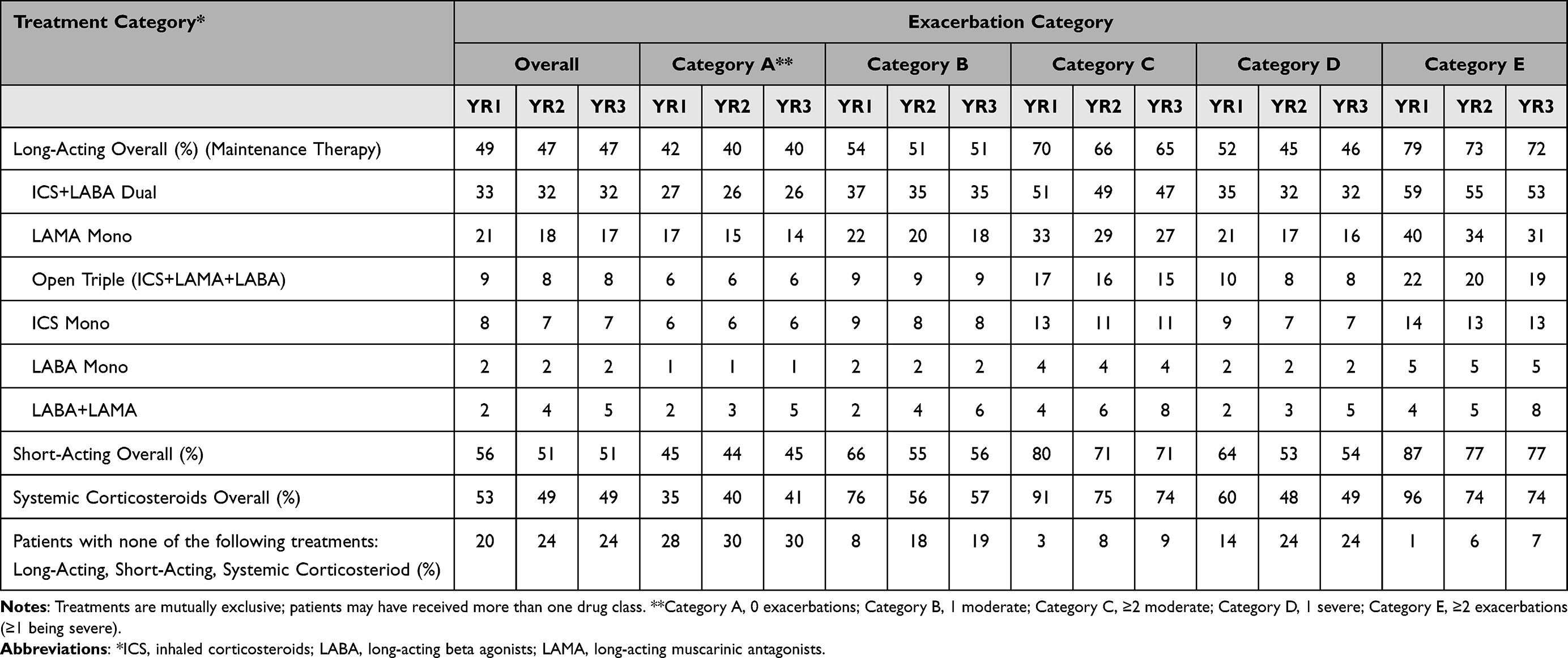 |
Table 4 Percentage of Patients with COPD Receiving Treatment for Overall Cohort and Exacerbation Categories A–E at Baseline YR1 and Post-Index YR2 and YR3 |
Cost Outcomes
Table 2A summarizes unadjusted and adjusted costs and cost differences for all exacerbation categories, and Table 2B shows unadjusted and adjusted cost ratios relative to Cat A. Unadjusted costs in YR2 and YR3 were observed to be similar for those with no exacerbation (Cat A: $26,544) and 1 moderate exacerbation (Cat B: $26,657) (Table 2). Mean unadjusted costs were highest for those with at least 1 severe exacerbation; Cat D: (YR2) $38,564 (p<0.0001) and (YR3) $41,789 (p<0.0001), Cat E: (YR2) $43,774 (p<0.0001) and (YR3) $46,557 (p<0.0001). After adjustment, mean YR2 total all-cause costs ranged between approximately $24,000–$26,600 for all categories and between approximately $23,600 and $26,400 for YR3. Incremental all-cause cost differences relative to Cat A were found to be highest among those patients in Cat D and E; these adjusted costs represented an increase of 6–8% and 8–9% for YR2 and YR3, respectively. Despite having greater risks for future exacerbations, these differences did not translate to noticeably greater total healthcare costs for those experiencing only moderate exacerbations (Cat B and Cat C).
Discussion
This retrospective observational study was conducted to understand the real-world rates, treatments, and costs of moderate and severe COPD exacerbations in 100% Medicare FFS beneficiaries between 2015 and 2018, the most currently available data from Medicare at the time of study design. In baseline YR1, nearly 40% of patients experienced one or more moderate and/or severe exacerbations. Patients with at least one severe exacerbation or those having multiple exacerbations, regardless of severity were more likely to experience an exacerbation during YR2 (12.0% to 24.2%) and YR3 (35.0% to 41.8%) compared to those without exacerbations. Moreover, those with greater exacerbation burdens (eg, higher frequency and severity) tended to have a larger number of comorbidities, particularly hypertension (Cat D and Cat E ≥90%), hyperlipidemia (Cat D and Cat E ≥63%), and tobacco dependence (Cat D and Cat E ≥70%). A relatively large percentage of patients in all exacerbation categories had no treatment or only short-acting treatment during baseline YR1, even though these patients were at risk for future exacerbation events. This treatment rate did not improve over the ensuing study period. Patients identified as having severe exacerbations consistently had higher costs compared to other patients.
Our real-world study of 100% Medicare FFS with COPD provided a unique opportunity to study exacerbation frequency and severity over a 3-year period in a large population of older patients. While the highest exacerbation rates were observed in frequent exacerbators, particularly those with a severe event, patients with no events or only moderate events in the baseline year still contributed greatly to the overall burden of COPD over the following two years, accounting for as much as a third of exacerbations in that time frame. When adjusted for baseline patient characteristics, patients with frequent exacerbations and/or a single severe exacerbation were approximately two to four times more likely to have an exacerbation in YR2 and YR3. Other observational studies have also shown exacerbations at baseline predict future events. The multicenter trial (2006–2010) Evaluation of COPD Longitudinally to identify Predictive Surrogate Endpoints (ECLIPSE) identified a major phenotype of frequent exacerbators across disease severities (Global Initiative for Chronic Obstructive Lung Disease [GOLD] grades II–IV) who are at risk for future exacerbations.16 In a real-world study of a managed care population using claims data from Truven Health MarketScan (2008–2010) Databases, Dalal et al similarly assessed COPD patients with one moderate or severe exacerbation (defined as infrequent), two or more exacerbations (defined as frequent) and those with no exacerbations within the index year.8 They found that infrequent exacerbators were three times more likely than non-exacerbators to experience two or more exacerbations yearly in follow-up and frequent exacerbators seven times more likely in follow-up. These findings were higher than that observed in our Medicare population, which may reflect combining moderate and severe exacerbations into a single category, data source and adjustment methods.
An important finding of our study is treatment underutilization in patients with COPD, despite both baseline events and observed risks over the next two years. Other real-world studies have observed similar results. Dalal found that 30% of patients with a history of exacerbations did not take COPD maintenance medications.8 In a study assessing medication management between 2010 and 2014 of the 100% Medicare FSS beneficiaries, Celli et al similarly reported inadequate use of maintenance medication.31 Lack of optimal maintenance treatment contrary to guidelines can lead to worse outcomes. A study of patients with COPD using the HealthCore Integrated Research Database with enrollees from 14 commercial and Medicare Advantage health plans showed that compliance with the 2017 GOLD Report32 were associated with less exacerbations and reduced COPD-related healthcare resource utilization and medical costs. This study also showed pharmacological treatment not being optimized despite occurrence of exacerbation events. Our study highlights a fundamental concern that lack of guideline treatment continues to be common in patients with COPD experiencing acute exacerbations, despite the added risk for future exacerbations. The importance of secondary prevention of exacerbations has not received the attention it deserves. Similar lack of guideline treatment in other therapeutic areas such as ischemic heart disease would not be acceptable. It is crucial that post-exacerbation management find parallels to address similar concerns to minimize recurring events.
Although results of pharmacological treatments in this study were based on prescription fills, patient nonadherence to medications contributes to treatment underutilization for COPD.33 It is estimated that 50% of all patients with COPD are not adherent to medications.34,35 Possible reasons for this may include complex treatment regimens, difficulties with inhaler devices, costs and medication side effects. Non-drug factors can also play a role such as age, underestimation of disease severity, patient education and disease knowledge, relationship with physician, and depression.32,35 These factors highlight the complexity of managing patients with frequent and severe COPD exacerbations.
Finally, our study showed that a single severe exacerbation and frequent exacerbations with at least one severe event resulted in the highest all-cause costs observed in YR2 and YR3. Other real-world studies have also demonstrated increased costs with exacerbation severity and frequency. Dhamane et al assessed COPD exacerbations in patients enrolled in a commercial plan or Medicare Advantage plan with prescription drug benefits in the Humana administrative claims database between 2007–2012.2 Exacerbation frequency categories included 0, 1, 2, ≥3, and severity categories were defined as ambulatory, requiring hospitalization, and leading to acute respiratory failure. Despite differences in exacerbation category definitions and costs reported by number of exacerbations, total all-cause costs were remarkably similar between the two studies. Dhamane reported unadjusted annual cost of $27,132 for no exacerbations; $36,173 for 1 exacerbation; and $43,414 for 2 exacerbations. We report similar cost differences and trends between exacerbation categories: $26,544 for no exacerbations; $38,564 for 1 severe exacerbation; and $43,774 for ≥2 exacerbations with at least one being severe.2 In another study of a large national healthcare plan with predominately Medicare population between 2007 and 2009, Pasquale et al also reported that patients with severe exacerbations and those with both severe and moderate exacerbations had the highest total all-cause costs consistent with our findings.10
It is important to note that among this Medicare FFS population that COPD-related hospitalizations and ED visits accounted for the majority of the medical costs. The Agency for Healthcare Resource and Quality reported that these types of visits resulted in $4 billion to Medicare in 2011 and responsible for 20% of 30-day all-cause readmissions.20,36 Consequently, Medicare has added acute exacerbations of COPD to a list of conditions monitored by the Medicare Hospital Readmission Program.20
This study has several limitations. Although exclusion of patients who died within the 36-month enrollment period is a study design limitation, it did allow for the overall longitudinal evaluation of the number and severity of exacerbation categories. Respective mortality of 4.6%, 24.4%, and 48.2% reported among individuals in the 30 days, 1 year, and 3 years subsequent to an acute care COPD encounter20 suggest that eliminating patients who die would potentially understate the occurrence of exacerbations. Pharmacological treatment during baseline YR1 and YR2 and YR3 are limited to identifying categories of medications. Dosing, adherence, or use of other respiratory medications such as Phosphodiesterase-4 inhibitors were not calculated or identified. Direct comparison of study findings was limited by lack of standardized definitions for exacerbations reported in the published literature.9 The study was limited to moderate and severe exacerbations based on administrative ICD codes, and Medicare hospitalization, outpatient, and pharmacy claims data. However, Medicare does not directly capture inpatient pharmacy claims data. Medication expenses paid out of pocket or by other insurance coverage are not available within these data. Since claims data are used for billing and reimbursement, there is a possibility of miscoding and unreported events. In addition, findings may not be generalizable to younger patients with COPD and to those who are uninsured or commercially insured.
Despite these limitations, use of the 100% Medicare FFS data source and study design did provide several advantages. The study included more than 11 million Medicare beneficiaries making results generalizable to traditional Medicare beneficiaries in the US. The study captured real-world prescribing practices to manage COPD and exacerbations highlighting under use of long-term maintenance therapy, even in patients experiencing frequent and/or severe exacerbations. Exacerbation category definitions were based on two current real-world studies, An observational Study on HEalthcare Resource utiLisation related to exacerbatiOns in patients with COPD (SHERLOCK, Scotland)37 and EXAcerbations of COPD and their OutcomeS (EXACOS) (U.S./International).38 Classifying frequency and severity of exacerbations during baseline YR1 allowed for assessment of further risk for those with an exacerbation during the two post-index years as well as for those without an exacerbation.
In conclusion, our observational study of the Medicare FFS COPD population confirms in a real-world setting that a history of exacerbations is a driver for future exacerbations. It also demonstrates that patients who were exacerbation free at baseline are also at risk for future moderate and severe exacerbations. Despite evidence-based GOLD recommended therapies, maintenance treatment of COPD is suboptimal and likely contributes to their risk for future exacerbations. Patients with one severe exacerbation and/or multiple exacerbations incur higher costs. Early evidence-based management should be a goal of patient care to reduce the medical and economic burden of COPD.
Acknowledgments
Carol Cohen, senior medical writer employed by Avalere Health, provided medical writing and editorial support. This work was presented in part at the Academy of Managed Care Pharmacy 2021 Virtual, April 12–April 16, 2021; American Thoracic Society 2021 Virtual, May 14–19, 2021.
Author Contributions
All Authors meet the following five criteria outlined by the International Journal of Chronic Obstructive Pulmonary Disease for Authorship:
- Made a significant contribution to the work reported herein, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
- Have drafted or written, or substantially revised or critically reviewed the article.
- Have agreed on the International Journal of Chronic Obstructive Pulmonary Disease to which the article is being submitted.
- Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
- Agree to take responsibility and be accountable for the contents of the article.
Funding
This study was supported by AstraZeneca. Employees of the sponsor were involved in various aspects of the conception and design of the studies, acquisition of data, analysis and interpretation of data, and input into manuscript development. The sponsor did not place any restrictions on the authors about the statements made in the final article.
Disclosure
Sanjay Sethi has received research funding (to institution) from Regeneron and Theravance. He has received advisory fees or honoraria from AstraZeneca, Boehringer Ingelheim, Chiesi, Nuvaira, Pulmonx, GlaxoSmithKline and Theravance. He has received royalties from Merck and Uptodate. Barry J Make has received consulting fees for development of this manuscript from AstraZeneca. Over the last three years, he has also received research grant funds, medical advisory board forms and consulting fees from AstraZeneca. Dr. Make reports research grant support from National Heart, Lung and Blood Institute, American Lung Association and Department of Defense; research grant support and medical advisory board fees from GlaxoSmithKline; medical advisory board fees from Novartis, Verona, Boehringer Ingelheim, Mylan and Phillips; DSMB fees from Spiration, Mt Sinai Medical Center, University of Wisconsin and Quintiles; honoraria for CME activities from American College of Chest Physicians, Mt. Sinai, Web MD, Projects in Knowledge, Integritas Communications, Medscape, Eastern Pulmonary Society; royalties from Wolters Kluwer (Up-To-Date), outside the submitted work. Michael Pollack and Norbert Feigler are employees of AstraZeneca, which provided the funding for this study. Scott B Robinson and Shambhavi Kumar are employees of Avalere Health, which received consulting fees from AstraZeneca for this manuscript. Chad Moretz, Jill Dreyfus, Ann Xi, and Dakota Powell were employees of Avalere Health at the time the study was completed. The authors report no other conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Division of Population Health. Chronic Disease Indicators (CDI) data. Available from: https://nccd.cdc.gov/cdi/rdPage.aspx?rdReport=DPH_CDI.ExploreByTopic&islTopic=COPD&islYear=9999&go=GO.
2. Dhamane AD, Moretz C, Zhou Y, et al. COPD exacerbation frequency and its association with health care resource utilization and costs. Int J Chron Obstruct Pulmon Dis. 2015;10:2609–2618. doi:10.2147/COPD.S90148
3. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of Chronic Obstructive Pulmonary Disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
4. López-Campos JL, Tan W, Soriano JB. Global burden of COPD. Respirology. 2016;21(1):14–23. doi:10.1111/resp.12660
5. Centers for Disease Control and Prevention. Mortality in the United States, 2019. NCHS data brief. No 395; 2020. Available from: https://www.cdc.gov/nchs/data/databriefs/db395-H.pdf.
6. COPD national action plan. Available from: https://www.nhlbi.nih.gov/health-topics/education-and-awareness/COPD-national-action-plan.
7. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2022 report. Available from: GOLD-REPORT-2022-v1.0-12Nov2021_WMV.pdf(goldcopd.org).
8. Dalal AA, Patel J, D’Souza A, Farrelly E, Nagar S, Shah M. Impact of COPD exacerbation frequency on costs for a managed care population. J Manag Care Spec Pharm. 2015;21(7):575–583. doi:10.18553/jmcp.2015.21.7.575
9. Toy EL, Gallagher KF, Stanley EL, Swensen AR, Duh MS. The economic impact of exacerbations of chronic obstructive pulmonary disease and exacerbation definition: a review. COPD. 2010;7(3):214–228. doi:10.3109/15412555.2010.481697
10. Pasquale MK, Sun SX, Song F, Hartnett HJ, Stemkowski SA. Impact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly Medicare population. Int J Chron Obstruct Pulmon Dis. 2012;7:757–764. doi:10.2147/COPD.S36997
11. Sethi S, Murphy TF. Evaluation for infection in exacerbations of chronic obstructive pulmonary disease; 2017. UpToDate. Available from: https://www.uptodate.com/contents/evaluation-for-infection-in-exacerbations-of-chronic-obstructive-pulmonary-disease.
12. Han MK, Dransfield MT, Martinez FJ. Chronic obstructive pulmonary disease definition, clinical manifestations, diagnosis, and staging. UpToDate. Available from: https://www.uptodate.com/contents/chronic-obstructive-pulmonary-disease-definition-clinical-manifestations-diagnosus-and-staging.
13. Halpin DMG, Decramer M, Celli BR, Mueller A, Metzdorf N, Tashkin DP. Effect of a single exacerbation on decline in lung function in COPD. Respir Med. 2017;128:85–91. doi:10.1016/j.rmed.2017.04.013
14. Dransfield MT, Kunisaki KM, Strand MJ, et al.; COPDGene Investigators. Acute exacerbations and lung function loss in smokers with and without chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(3):324–330. doi:10.1164/rccm.201605-1014OC
15. Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
16. Hurst JR, Vestbo J, Anzueto A, et al.; Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
17. Chatila WM, Thomashow BM, Minai OA, Criner GJ, Make BJ. Comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):549–555. doi:10.1513/pats.200709-148ET
18. Mannino DM, Higuchi K, Yu TC, et al. Economic burden of COPD in the presence of comorbidities. Chest. 2015;148(1):138–150. doi:10.1378/chest.14-2434
19. Kunisaki KM, Dransfield MT, Anderson JA, et al.; SUMMIT Investigators. Exacerbations of chronic obstructive pulmonary disease and cardiac events. A post hoc cohort analysis from the SUMMIT randomized clinical trial. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
20. Genao L, Durheim MT, Mi X, Todd JL, Whitson HE, Curtis LH. Early and long-term outcomes of older adults after acute care encounters for chronic obstructive pulmonary disease exacerbation. Ann Am Thorac Soc. 2015;12(12):1805–1812. doi:10.1513/AnnalsATS.201504-250OC
21. Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2898. doi:10.2147/COPD.S139470
22. Kaiser Family Foundation. A dozen facts about medicare advantage in 2020; 2021. Available from: https://www.kff.org/medicare/issue-brief/a-dozen-facts-about-medicare-advantage-in-2020/.
23. Hanania NA, Sharma G, Sharafkhaneh A. COPD in the elderly patient. Semin Respir Crit Care Med. 2010;31(5):596–606. doi:10.1055/s-0030-1265900
24. Mues KE, Liede A, Liu J, et al. Use of the medicare database in epidemiologic and health services research: a valuable source of real-world evidence on the older and disabled populations in the US. Clin Epidemiol. 2017;9:267–277. doi:10.2147/CLEP.S105613
25. Medicare savings program. Available from: https://www.medicare.gov/medicare-savings-programs.
26. Dually eligible beneficiaries under medicare and medicaid. Available from: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/Medicare_Beneficiaries_Dual_Eligibles_At_a_Glance.pdf.
27. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–709. doi:10.1016/0895-4356(92)90133-8
28. Donaldson GC, Hurst JR, Smith CJ, Hubbard RB, Wedzicha JA. Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest. 2010;137(5):1091–1097. doi:10.1378/chest.09-2029
29. Niegisch G, Gerullis H, Lin SW, et al. A real-world data study to evaluate treatment patterns, clinical characteristics and survival outcomes for first- and second-line treatment in locally advanced and metastatic urothelial cancer patients in Germany. J Cancer. 2018;9(8):1337–1348. doi:10.7150/jca.23162
30. Health Resources and Services Administration. Consumer Price Index (CPI) for medical care. Available from: https://www.hrsa.gov/sites/default/files/hrsa/get-health-care/affordable/hill-burton/cpitables.pdf.
31. Celli BR, Navaie M, Xu Z, Cho-Reyes S, Dembek C, Gilmer TP. Medication management patterns among Medicare beneficiaries with chronic obstructive pulmonary disease who initiate nebulized arformoterol treatment. Int J Chron Obstruct Pulmon Dis. 2019;14:1019–1031. doi:10.2147/COPD.S199251
32. Palli SR, Zhou S, Shaikh A, Willey VJ. Effect of compliance with GOLD treatment recommendations on COPD health care resource utilization, cost, and exacerbations among patients with COPD on maintenance therapy. J Manag Care Spec Pharm. 2021;27(5):625–637. doi:10.18553/jmcp.2021.20390
33. Mäkelä MJ, Backer V, Hedegaard M, Larsson K. Adherence to inhaled therapies, health outcomes and costs in patients with asthma and COPD. Respir Med. 2013;107(10):1481–1490. doi:10.1016/j.rmed.2013.04.005
34. Wedzicha JA, Brill SE, Allinson JP, Donaldson GC. Mechanisms and impact of the frequent exacerbator phenotype in chronic obstructive pulmonary disease. BMC Med. 2013;11:181. doi:10.1186/1741-7015-11-181
35. Bender BG. Nonadherence to COPD treatment: what have we learned and what do we do next? COPD. 2012;9(3):209–210. doi:10.3109/15412555.2012.679880
36. Torio CM, Andrews RM. National inpatient hospital costs: the most expensive conditions by payer 2011. Rockville, MD: Agency for Healthcare Research and Quality; 2013. HCUP Statistical Brief #160. Available from: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb160.jsp.
37. Haughney J, Lee AJ, Nath M, et al. The long-term clinical and economic impact of COPD exacerbations: an observational study (SHERLOCK). Eur Respir J. 2020;56(Suppl 64):4910.
38. Clinical Trials.gov. Exacerbations and their outcomes (EXACOS international). Available from: https://clinicaltrials.gov/ct2/show/record/NCT04928417.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.