Back to Journals » Journal of Asthma and Allergy » Volume 16
Relationship Between the Response to Antibody Therapy and Symptoms of Depression and Anxiety Disorders in Patients with Severe Asthma
Authors Plank PM, Hinze CA, Campbell V, Konwert S, Welte T ![]() , Drick N, Kayser MZ
, Drick N, Kayser MZ ![]() , Suhling H, Fuge J
, Suhling H, Fuge J ![]()
Received 1 January 2023
Accepted for publication 27 March 2023
Published 18 April 2023 Volume 2023:16 Pages 421—431
DOI https://doi.org/10.2147/JAA.S403296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Pia Maria Plank,1,* Christopher Alexander Hinze,2,* Victoria Campbell,3 Stefanie Konwert,4 Tobias Welte,1,4 Nora Drick,1 Moritz Z Kayser,1 Hendrik Suhling,1,4,* Jan Fuge1,4,*
1Department of Cardiology and Angiology, Hannover Medical School, Hannover, Germany; 2Department of Respiratory Medicine and Infectious Disease, Hannover Medical School, Hannover, Germany; 3Department of Paediatric Pulmonology, Allergology and Neonatology, Hannover Medical School, Hannover, Germany; 4Biomedical Research in Endstage and Obstructive Lung Disease Hannover (BREATH), German Center for Lung Research (DZL), Hannover, Germany
*These authors contributed equally to this work
Correspondence: Christopher Alexander Hinze, Department of Respiratory Medicine and Infectious Disease, Hannover Medical School, Carl-Neuberg-Str. 1, Hannover, 30625, Germany, Tel +49 511-5323531, Email [email protected]
Purpose: Asthma is associated with a high prevalence of psychopathological disorders, especially depressive disorders or anxiety. In patients with uncontrolled severe asthma, monoclonal antibody (mAb)-therapy positively influenced control of mental disorders. Therefore, we evaluated the impact of antibody therapy on the burden of these mental diseases depending on responder status.
Patients and Methods: Data were collected retrospectively in patients with uncontrolled severe asthma (n = 82) prior to mAb-therapy (“baseline”) (omalizumab, dupilumab, benralizumab or mepolizumab). Symptoms of Major Depressive Disorder (MDD) or General Anxiety Disorder (GAD) were detected at baseline using the Hospital Anxiety and Depression Scale (HADS), as well as general sociodemographic data and lung function parameters. At 6-month (± 3 month) follow-up, the burden of psychopathological symptoms under mAb-therapy was assessed using the Patient Health Questionnaire-2 (PHQ-2) and Generalized Anxiety Disorder Scale-2 (GAD-2). Response status was classified using the Biologics Asthma Response Score (BARS), assessing exacerbations, oral corticosteroid usage and asthma control test (ACT) score. Predictors for non-response to mAb-therapy were identified using linear regression analysis.
Results: Patients with severe asthma suffered from symptoms of MDD/GAD more often compared to the general population, with a higher prevalence among mAb therapy non-responders. mAb-responders exhibited a declining burden of MDD, better quality of life (QoL), less exacerbations, better lung function and better disease control compared to non-responders. A history of symptoms of depression was identified as a predictor for non-response to mAb-therapy.
Conclusion: Asthma symptoms and psychological problems are linked and more prevalent in our cohort of severe asthma patients than in the general population. Patients with signs of MDD/GAD before mAb-therapy show less mAb therapy response suggesting a negative impact of prior psychological problems on treatment response. In some patients, the score on MDD/GAD was caused by severe asthma – here symptoms decreased after effective treatment.
Keywords: severe asthma, monoclonal antibody therapy, depression, anxiety, therapy response
Introduction
Asthma is a chronic airway inflammation characterized by varying respiratory symptoms and variable expiratory airflow limitation. In particular, patients with severe asthma suffer from exacerbations and variable impairment in exercise capacity.1 Moreover, mental disorders like Major Depressive Disorder (MDD) and Generalized Anxiety Disorder (GAD) are more common in severe asthma patients than in the general population.2–6 MDD is characterized by a state of depressed mood, loss of interest and enjoyment, and reduced energy leading to increased fatiguability and diminished activity. GAD is characterized by persistent or recurring symptoms of apprehension, motor tension and autonomic dysregulation.7–9
In patients with severe asthma insufficiently controlled by maximized conventional inhalator therapy and/or oral corticosteroids, monoclonal antibodies (mAb) like Omalizumab (anti-IgE), Benralizumab (anti-IL5 receptor alpha), Mepolizumab (anti-IL5) and Dupilumab (anti-IL4 receptor alpha), targeting underlying immunological pathways, have been established as additional treatment options.10–12 Previous research showed that disease management, perceived stress, anxiety and depressive symptoms improved significantly under mAb-therapy, independent of which mAb was used.13,14 While the reported responder rates vary, it is universally acknowledged that a significant subset of severe asthma patients do not respond to mAb therapy.15–17
In this study, we aim to determine a possible relation between mAb-therapy response and mental health conditions, as well as to identify predictors for mAb-nonresponse or decline in mental status.
Methods
Study Aim, Design and Setting
In this single-centre, retrospective analysis, all patients beginning mAb-therapy in our centre between March 2020 and March 2022 were investigated using GAD and MDD questionnaires. All data were collected during routine appointments at our severe asthma outpatient clinic at Hannover Medical School, Hannover, Germany. The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the local ethic committee of the Hannover Medical School (10539_BO_K_2022). All patients provided written informed consent allowing the use of their data for scientific research.
Patient Selection and Treatment
All patients included in this study had already been diagnosed with severe asthma, according to American Thoracic Society (ATS)/European Respiratory Society (ERS) guidelines with an eosinophilic, allergic or combined phenotype.18 All patients received treatment following the step scheme for asthma with medium to high-dose inhaled glucocorticoids and a long-acting β2-agonist and could receive a second or third controller and/or additional oral corticosteroid (OCS) therapy. Thus, all patients fulfilled preconditions for monoclonal antibody therapy in accordance with the Food and Drug Administration (FDA) and European Medicines Agency (EMA) and add-on therapy with either mepolizumab, benralizumab, dupilumab or omalizumab was initiated. The choice of antibody was made by the treating physician.
Data Collection at Baseline and Routine Follow-Up
Prior to initiation of mAb-therapy, patients’ characteristics including age, sex, BMI, smoking status with calculation of pack years, alcohol consumption/abuse evaluated by Audit-C-Score19 (>4 (male) or >3 (female) were classified as “alcohol abuse”), pollutant exposure, allergies, education level, subdivided in academic education, vocational education and no completed education, family status and comorbidities were assessed. Additionally, Hospital Anxiety and Depression Scale (HADS-A, HADS-D), Patient Health Questionnaire-2 (PHQ-2) and Generalized Anxiety Disorder Scale-2 (GAD-2)20,21 were assessed at baseline prior to initiation of mAb-therapy. Both HADS subscales for anxiety (HADS-A) as well as depression (HADS-D) consist of 7 questions with a maximum score of 21 points. HADS scores were used as a screening test, all patients with a suspect (>10 points) or probable score (8–10 points) in HADS-A and HADS-D were classified as patients with signs of MDD and/or GAD.22 A positive AUDIT-C-Score and a suspect or probable HADS-A and HADS-D were considered to be a “current mental disorder”. GAD-2 as well as PHQ-2 were developed as a valid ultra-short screening tool for anxiety (GAD-2) and depression (PHQ-2) and consist of two questions with a maximum score of 6 points. A higher score implies a higher probability for depression/anxiety with scores ≥3 indicating relevant symptoms of MDD and GAD.20 Six months (±3 month) after baseline, a routine follow-up appointment was conducted. Mental health under mAb-therapy was re-assessed using PHQ-2 and GAD-2 scores. Routine follow-up also included spirometry or body plethysmography standardised to ERS/ATS guidelines, capillary blood gas analysis, measurement of exhaled nitric oxide (eNO), and laboratory testing (differential blood count). Structured questionnaires assessing pulmonary symptoms and asthma control (Asthma Control Test – ACT)23 and changes in medication were assessed both at baseline and follow-up appointment. Exacerbations were defined as worsening of asthma symptoms requiring OCS for at least three days or an increase in the OCS dose. EQ5D questionnaire was used to evaluate quality of life (QoL) at both timepoints on a visual analogue scale (VAS) ranging from 0 points (worst imaginable health state) to 10 points (best imaginable health state).24 Educational status was defined as low (no education), moderate (non-academic education) and high (academic education). Exacerbation rate was assessed for the last 12 months at baseline appointment and annualised for follow-up. It was defined as phases of progressive increase in asthma symptoms and/or decrease in lung function that exceed the patient’s usual level of variability and that require modification or intensification of therapy over several days and the usage of oral corticosteroids over more than three days.
All pulmonary function tests (PFT) were performed under continued stable inhaled therapy. Responder status was assessed using Biologics Asthma Response Score (BARS) recently published by Milger et al.25 Patients classified “responder” or “partial responder” were grouped in the “responder group”.
Statistical Analysis
For data analysis, IBM SPSS Statistics 28.0 (IBM Corp, Armonk, NY, USA) and R environment for statistical computing version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) were used. Categorical variables are stated as numbers (n) and percentages (%). Depending on distribution, continuous variables are shown as median with interquartile ranges (IQR) or as mean ± standard deviation (SD) unless indicated otherwise. Delta-values between the two time points were calculated for continuous variables in order to compare the slope. For group comparisons, Fisher’s exact test, Chi-squared test, two-sided t-test or Mann–Whitney-U-test were used, as appropriate. For intergroup comparisons between time points paired t-test or Wilcoxon-signed-rank test were used as appropriate. Prevalence rates of GAD or MDD in patients with severe asthma and a representative German population (DEGS1-MH study)26 were compared using χ2 test. Point estimates with 95% confidence intervals (CI) and differences between the two populations were calculated. Simple- and multivariate logistic regression analysis was conducted to assess the impact on patients not responding to mAb-therapy. All reported p-values are two-sided. P-values <0.05 were considered statistically significant.
Results
Patients Characteristics
Data from 82 patients diagnosed with severe asthma undergoing mAb-therapy were included, of which 38 patients (46%) showed a suspect or probable MDD and/or GAD. Overall, 61 (74%) were classified as responders and 21 (26%) as non-responders (Figure 1). Notably, 24/61 (39%) responders showed probable or suspect MDD/GAD, in contrast to 14/21 non-responder (67%) (p = 0.030). Further baseline characteristics are displayed in Table 1.
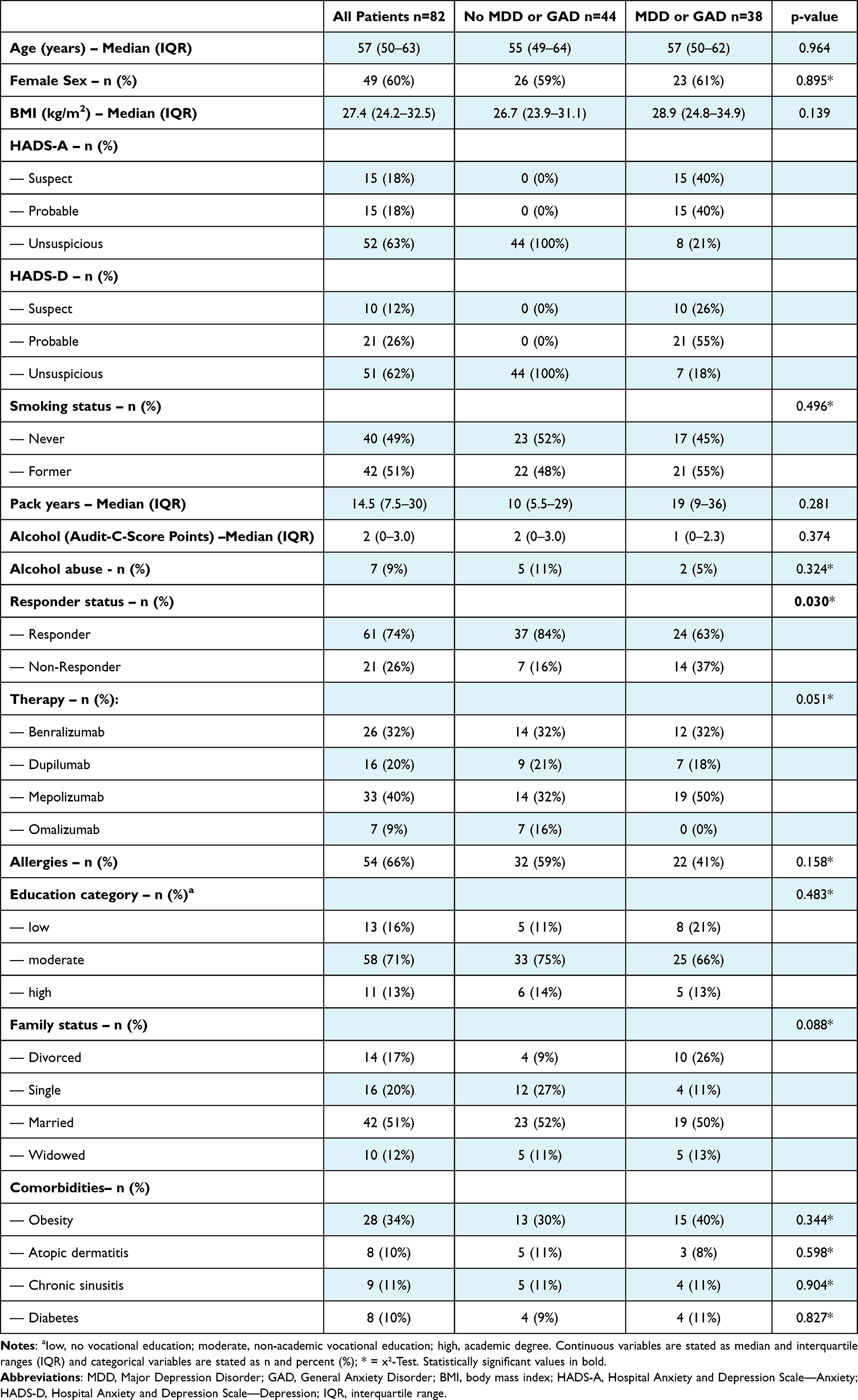 |
Table 1 Characteristics of the Patients at Baseline |
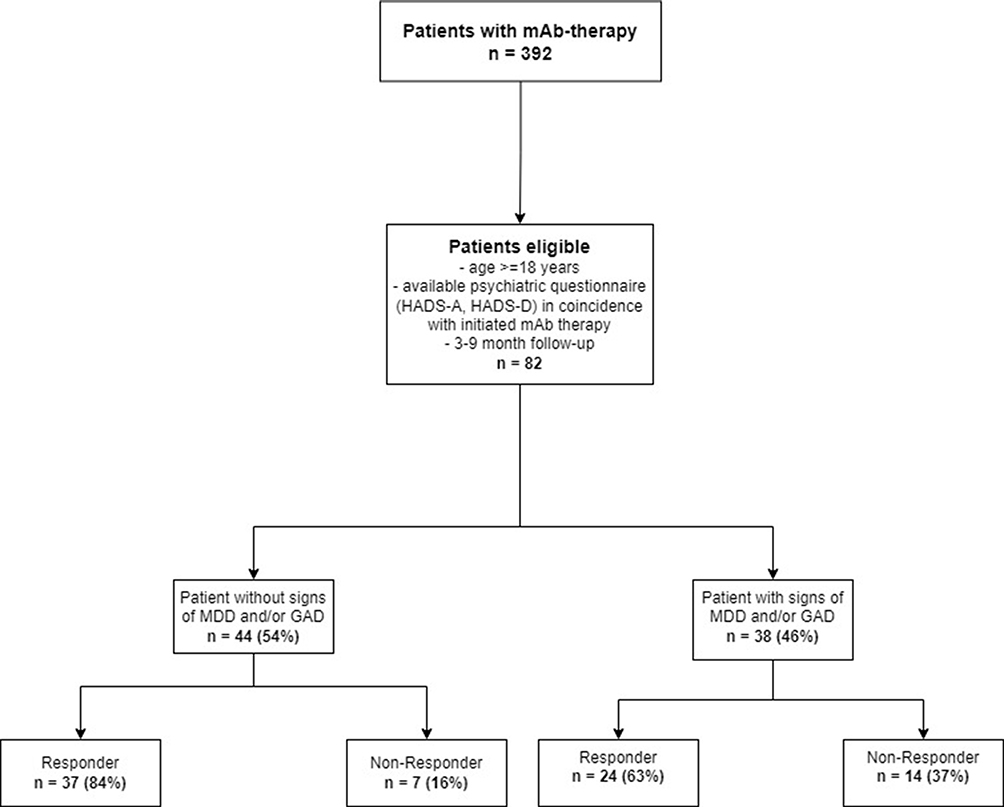 |
Figure 1 Flowchart of patient inclusion with consecutive subdivision in patients with and without signs of MDD/GAD and their respective responder-status. |
Treatment parameters at baseline and follow-up stratified by eventual treatment response are displayed in Figure 2. Responders showed significant improvements in FEV1 (p = 0.001), QoL and ACT (p < 0.001) and exacerbation rate (p < 0.001), while non-responders did not.
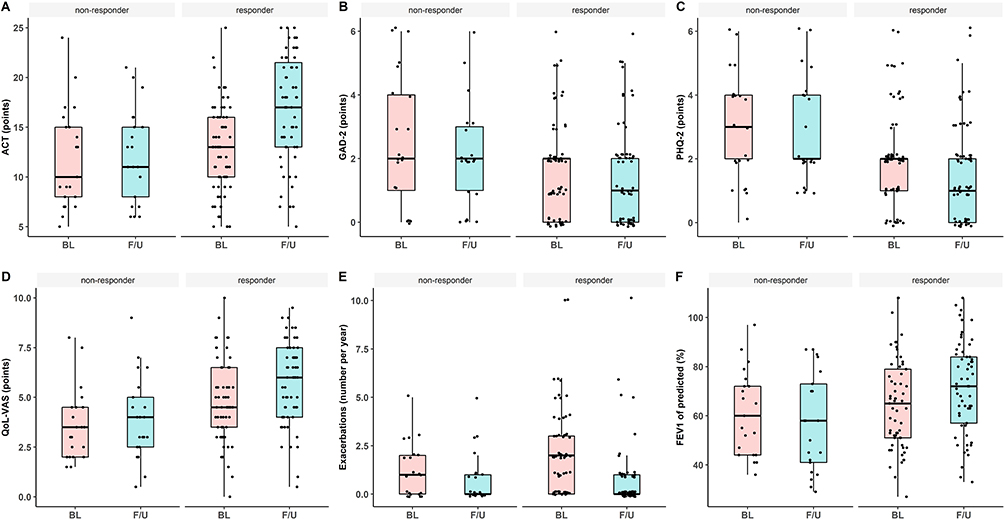 |
Figure 2 Comparison between baseline (BL) and follow-up (F/U) for (A) Asthma-Control Test (ACT), (B) Generalized Anxiety Disorder (GAD)-2 score, (C) Patients Health Questionnaire (PHQ)-2 score, (D) Quality of Life on Visual Analogue Scale (QoL-VAS), (E) Exacerbation counts and (F) Forced expiratory volume in one second (FEV1) subdivided in Responder and Non-Responder. Data are presented as boxplots. The bars show the median value, the lower and upper ends correspond to the first and third quantiles (25th and 75th percentiles). The upper whisker extends from the upper edge of the boxplot to the highest value, the lower whisker extends from the lower edge of the boxplot to the smallest value. |
Prevalence of Mental Disorders in Severe Asthma
53% of patients in our study cohort suffered from psychological problems at the time of mAb initiation, 38% from probable MDD, 37% from probable GAD as well as 9% from alcohol abuse. Compared to the German general population, this represents a drastically elevated prevalence among our severe asthma patient cohort (p < 0.001).26 Of note, we observed 16- and 5-fold higher risks for signs of GAD and MDD, respectively, in patients with severe asthma in our cohort compared to the general population (Table 2).
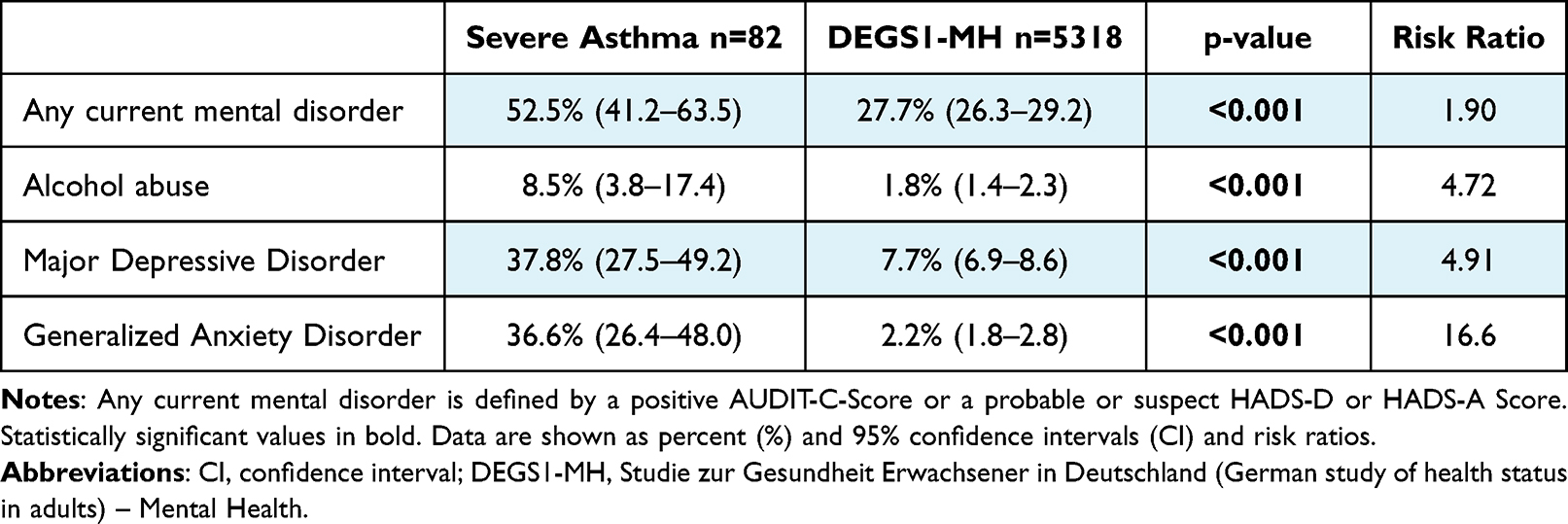 |
Table 2 Psychological Disorder Prevalence Rates in Patient with Severe Asthma Compared to German Population |
Differences in Mental Disorders Dependant on mAb Responder Status
Monoclonal antibody responders showed a significantly declining PHQ-2-score (BL: 2 (IQR: 1–2), FU: 1 (IQR: 0–2), p = 0.026) and tended towards a decrease in GAD-2-score (BL: 2 (IQR: 0–2), FU: 1 (IQR: 0–2), p = 0.051), while mAb non-responders showed no significant reduction in these scores Table 3 and Figure 2). Comparison between responder and non-responder revealed a significantly lower PHQ-2-score (p = 0.028) and GAD-2-score (p = 0.045) for baseline and significantly lower PHQ-2-score for follow-up (p = 0.003). Responders exhibit significant lower scores in HADS-D (p = 0.002) with no significant differences in HADS-A (p = 0.068) as well as in further analysed characteristics (Table 3).
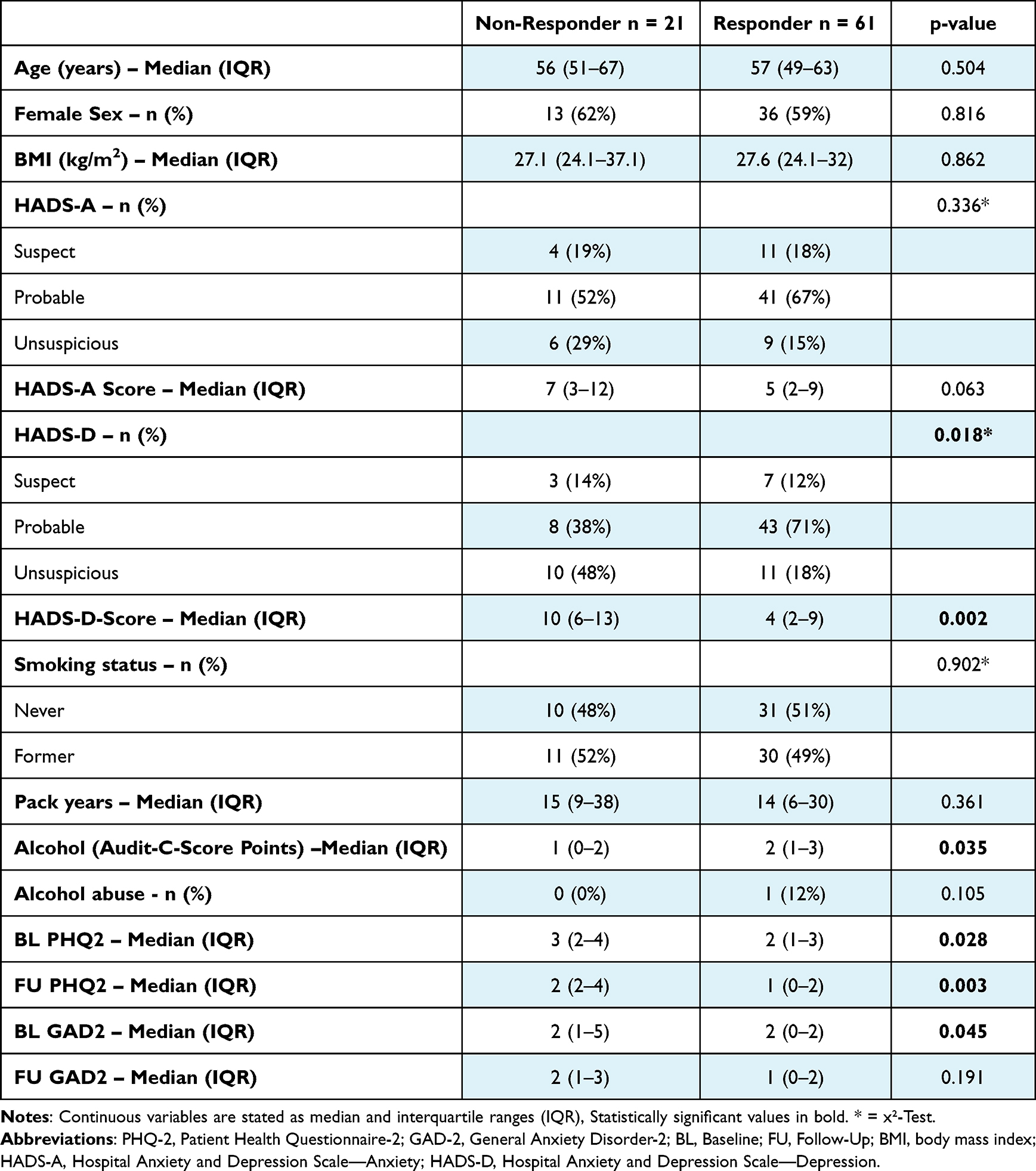 |
Table 3 Comparison Between Responders and Non-Responders |
In logistic regression analysis, non-responding to mAb-therapy was associated with an OR of 1.23 (CI: 1.07–1.42), p = 0.004 per HADS-D point increase. Analysis for HADS-A revealed no significant impact (p = 0.068) in univariate analysis. Furthermore, an influence of alcohol (Audit C Score) on mAb non-response was detected with an OR of 0.65 (0.43–0.99) in multivariate analysis (p = 0.043). All further analysed variables did not show significant impact of psychological problems on mAb-therapy response (Table 4).
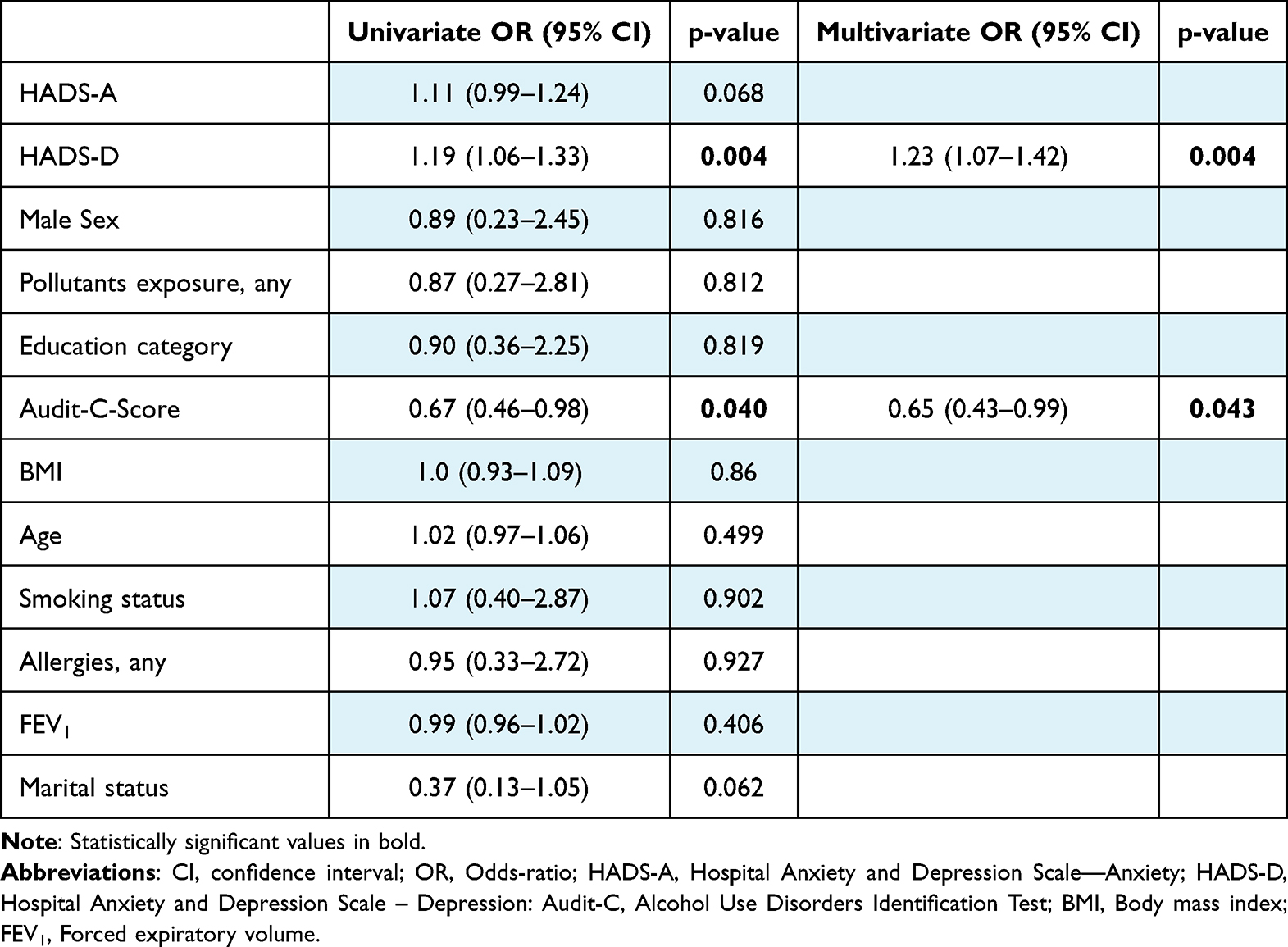 |
Table 4 Multivariate Analysis of Impact on Non-Responding to mAb-Therapy |
Discussion
To our knowledge, this is the first study to investigate changes in the burden and severity of psychological problems in patients with severe asthma receiving mAb-therapy and the impact on the patients’ mAb responder status.
Patients that respond to mAb-therapy exhibit lower levels of MDD- or GAD-related symptoms and prevalence of probable MDD and GAD decreased significantly after initiation of mAb-therapy. Logistic regression analysis revealed pre-existing symptoms of depression as a major predictor for non-response to mAb-therapy.
An increased prevalence of mental disorders, particularly MDD and GAD, in asthma patients as well as in other respiratory diseases is well documented in the literature: Previous studies about adolescents with asthma found a cumulative prevalence of 16.3% for anxiety and depressive disorder in an American population as well as a prevalence of 6.3% for depression disorder in a Taiwanese cohort.6,27 Fong et al identified a prevalence of 42.8% for depression and 38% for anxiety disorder in patients with severe asthma comparable to 37.8% for depression and 36.6% for anxiety in our cohort.14 Notably, another study found that 23% of patients suffering from idiopathic pulmonary hypertension exhibited depression disorder, whereas in patients with chronic thromboembolic pulmonary hypertension the prevalence of depression and anxiety resembled that of the general population, but panic disorders were more common.28,29 Concerning patients with chronic obstructive pulmonary disease (COPD), meta-analysis showed a prevalence of 24.6% for depression30 and 40% for anxiety.31 Both the cause for the general elevation in prevalence of mental disorders and the cause for the wide spread of prevalence among patients suffering from respiratory diseases remain unclear. The aforementioned studies analysed cohorts differing greatly in age, origin and stage of illness, so the weighting of mental illness is certainly related to this and thus an individualized approach must be taken to identify affected patients. Either way, the connection between psychological problems and asthma therapy remains to be elucidated.
A positive effect of mAb-therapy on anxiety and depression disorders in patients with severe asthma has been reported previously, without differentiation between mAb-therapy responders and non-responders.13 Comparable to our approach, one part of the above-mentioned WATCH study by Fong et al examined the relation between the response to Omalizumab/Mepolizumab and MDD/GAD evaluated by HADS-A/D. Non-responders suffered from mental disorders more frequently. Furthermore, depression was identified as a potential influence factor for mAb-therapy nonresponse,14 matching our own findings. Additionally, our study includes patients with omalizumab and mepolizumab as well as those with dupilumab and benralizumab. In fact, effects of mAb-therapy response on mental health have not only been described for severe asthma but also for other chronic diseases, particularly rheumatoid arthritis.32–34 While an association between GAD/MDD and mAb-therapy non-response is well-established, the underlying mechanisms remain unclear: One possible explanation is the well-described decreased therapy adherence in patients with psychiatric comorbidities.35,36 To date, there are no specific data on the adherence of patients with severe asthma and mAb-therapy, so we can only draw on empirical values from our daily work. For example, a regular application of the therapy can be indirectly deduced from falling values of IgE and/or eosinophils. Moreover, cytokine disbalances were identified in psychiatric patients, possibly affecting the efficacy of immunomodulation.37 For example, elevated production of disease-related Th2 and Th17 cytokines has been detected in asthmatic patients suffering from MDD,38 whereas the influence of these elevated cytokines on the success of mAb-therapy remains unclear. Thus, this issue needs further investigation.
Conversely, chronic diseases such as severe asthma may also cause or aggravate affective mood disorders and anxiety in affected patients, who consequentially avoid enjoyable activities and social contacts.39,40 In chronic respiratory diseases, repetitive breathlessness as well as frequent exacerbations can cause a loss of self-control and engulfment of daily routine. Thus, these factors favour mental distress with consecutive depression and anxiety disorder.40,41 The improvement of depression in PHQ2 test in mAb-responders shows the direct influence of pulmonary improvement on psychological status.
The cited literature in the preceding sections matches our results with regard to a negative impact of pre-existing depression on mAb-response but also with a positive effect of disease control on symptoms of depression. However, it has to be mentioned that our and the cited results just base on statistical observation without proof of a causal relationship. It remains unclear whether severe asthma and MDD/GAD are at all related in our patients. Consideration of risk factors and reasons of these mental disorders42,43 reveals a complexity that is not restricted to severe asthma. In patient cohorts suffering from asthma and other chronic diseases, risk factors for psychiatric morbidities (eg, history of depression, older age) are more prevalent.27,44 Given the complex and incompletely understood pathogenesis of asthma and the multitude of factors influencing its course and severity,45 further research concerning its interplay with mental illness is necessary.
The main advantage of our study is the classification of our treated patients in responder and non-responder according to the novel BARS Score that as universally applicable to classify mAb-therapy response.25
Limitations: The generalizability of our study is limited by its monocentric and retrospective design as well as the relatively small sample size. Further, using HADS in combination with PHQ-2 and GAD-2 scores to estimate the follow-up to classify patients with probable MDD and/or GAD does not allow diagnosis of mental disorders. Additionally, there are no values for the minimum clinically important difference (MCID) for these questionnaires, making a clinical appraisal of changes more difficult. Nevertheless, they prove useful as a reliable screening tool with the benefit of being able to discriminate between severity of symptoms.20,46 Our study also focuses on two of the most prevalent mental disorders, but does not consider the wide range of all mental illnesses.
Conclusion
This is the first study evaluating the impact of anxiety or depression on mAb-therapy response in severe asthma patients. Patients responding to mAb-therapy showed less signs of MDD/GAD. Conversely, a history of depression, but not anxiety, was a negative predictor for mAb-therapy success. Taken together, our findings highlight the need for a subsequent psychiatric evaluation in patients suffering most probably from mental disorders and severe asthma as well as for further research regarding possible causal connections between asthma and mental diseases.
Abbreviations
mAb, monoclonal antibody; MDD, Major Depression Disorder; GAD, General Anxiety Disorder; HADS, Hospital Anxiety and Depression Scale; PHQ-2, Patient Health Questionnaire-2; GAD-2, General Anxiety Disorder-2; CTEPH, Chronic thromboembolic pulmonary hypertension; QoL, Quality of Life; ACT, Asthma Control Test; ERS, European respiratory society; ATS, American thoracic society; FDA, Food and Drug agency; EMA, European Medicines agency; COPD, Chronic obstructive pulmonary disease; OCS, Oral corticosteroids; Audit-C-Score, Alcohol Use Disorders Identification Test; CI, Confidence interval; OR, Odds ratio; BMI, Body Mass Index; FEV1, Forced expiratory volume; IgE, Immunoglobulin E; MCID, minimum clinically important difference; BL, Baseline; FU, Follow-Up; IQR, Interquartile range.
Data Sharing Statement
Data used in this study are available on reasonable request by the corresponding author.
Ethics Approval and Consent to Participate
Approval of the local ethic committee of the Hannover Medical School (10539_BO_K_2022) was given and all patients provided written informed consent allowing the use of their data for scientific research.
Acknowledgments
We wish to thank all patients who participated in this project. We would also like to thank the clinical staff caring about the patients and the questionnaires and last but not least the families of the authors who have given up a lot of time with their loved ones to make this research possible.
Funding
There is no funding to report.
Disclosure
Tobias Welte and/or his institution received grants advisory/lecture/clinical trial fees and non-financial support by DFG (German Research Council), BMBF (German Ministry of Research and Education), BMG (German Ministry of Health), EU, WHO, AstraZeneca, Basilea, Biotest, Bayer, Boehringer, Berlin Chemie, GSK, Infectopharm, MSD, Novartis, Pfizer, Roche, AstraZeneca, Basilea, Biotest, Bayer, Boehringer, Gilead, GSK, Janssen, Novartis, Pfizer, Roche, German Center of Lung Research all outside the submitted work. Hendrik Suhling reports personal fees/speaker honoraria from AstraZeneca, GSK, Novartis, Sanofi, outside the submitted work. Jan Fuge reports personal fees/speaker honoraria from AstraZeneca outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Reddel HK, Boulet L-P, Bateman ED. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17–35. doi:10.1164/rccm.202109-2205PP
2. Alonso J, de Jonge P, Lim CCW, et al. Association between mental disorders and subsequent adult onset asthma. J Psychiatr Res. 2014;59:179–188. doi:10.1016/j.jpsychires.2014.09.007
3. Baumeister H, Balke K, Härter M. Psychiatric and somatic comorbidities are negatively associated with quality of life in physically ill patients. J Clin Epidemiol. 2005;58(11):1090–1100. doi:10.1016/j.jclinepi.2005.03.011
4. Calam R, Gregg L, Simpson B, et al. Childhood asthma, behavior problems, and family functioning. J Allergy Clin Immunol. 2003;112(3):499–504. doi:10.1016/S0091-6749(03)01606-3
5. Goodwin RD, Jacobi F, Thefeld W. Mental disorders and asthma in the community. Arch Gen Psychiatry. 2003;60(11):1125–1130. doi:10.1001/archpsyc.60.11.1125
6. Katon W, Lozano P, Russo J, et al. The prevalence of DSM-IV anxiety and depressive disorders in youth with asthma compared with controls. J Adolesc Health. 2007;41(5):455–463. doi:10.1016/j.jadohealth.2007.05.023
7. Cassano P, Fava M. Depression and public health: an overview. J Psychosom Res. 2002;53(4):849–857. doi:10.1016/S0022-3999(02)00304-5
8. DGPPN B, KBV A, Akdä B, et al. S3-Leitlinie/Nationale versorgungsleitlinie unipolare depression. Auflage. 2015;5:2015.
9. Gautam S, Jain A, Gautam M, et al. Clinical Practice Guidelines for the Management of Generalised Anxiety Disorder (GAD) and Panic Disorder (PD). Indian J Psychiatry. 2017;59(Suppl 1):S67–s73. doi:10.4103/0019-5545.196975
10. Agache I, Rocha C, Beltran J, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab and omalizumab) for severe allergic asthma: a systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020;75(5):1043–1057. doi:10.1111/all.14235
11. Gallo S, Castelnuovo P, Spirito L, et al. Mepolizumab improves outcomes of chronic rhinosinusitis with nasal polyps in severe asthmatic patients: a multicentric real-life study. J Pers Med. 2022;12:8.
12. Haldar P, Brightling CE, Hargadon B, et al. Mepolizumab and exacerbations of refractory eosinophilic asthma. N Engl J Med. 2009;360(10):973–984. doi:10.1056/NEJMoa0808991
13. Patella V, Pelaia C, Zunno R, et al. Biologicals decrease psychological distress, anxiety and depression in severe asthma, despite Covid-19 pandemic. Respir Med. 2022;200:106916. doi:10.1016/j.rmed.2022.106916
14. Fong WCG, Azim A, Knight D, et al. Real-world Omalizumab and Mepolizumab treated difficult asthma phenotypes and their clinical outcomes. Clin Exp Allergy. 2021;51(8):1019–1032. doi:10.1111/cea.13882
15. Drick N, Milger K, Seeliger B, et al. Switch from IL-5 to IL-5-Receptor α Antibody Treatment in Severe Eosinophilic Asthma. J Asthma Allergy. 2020;13:605–614. doi:10.2147/JAA.S270298
16. Drick N, Seeliger B, Welte T, et al. Anti-IL-5 therapy in patients with severe eosinophilic asthma - clinical efficacy and possible criteria for treatment response. BMC Pulm Med. 2018;18(1):119. doi:10.1186/s12890-018-0689-2
17. Kayser MZ, Drick N, Milger K, et al. Real-world multicenter experience with mepolizumab and benralizumab in the treatment of uncontrolled severe eosinophilic asthma over 12 months. J Asthma Allergy. 2021;14:863–871. doi:10.2147/JAA.S319572
18. Holguin F, Cardet JC, Chung KF, et al. Management of severe asthma: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2020;55(1):1900588. doi:10.1183/13993003.00588-2019
19. Gordon AJ, Maisto SA, McNeil M, et al. Three questions can detect hazardous drinkers. J Fam Pract. 2001;50(4):313–320.
20. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
21. Kroenke K, Spitzer RL, Williams JBW, et al. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. 2010;32(4):345–359. doi:10.1016/j.genhosppsych.2010.03.006
22. Snaith RP, Zigmond AS. The Hospital Anxiety and Depression Scale. Br Med J. 1986;292(6516):344. doi:10.1136/bmj.292.6516.344
23. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. doi:10.1016/j.jaci.2003.09.008
24. Spigel D, De Marinis F, Giaccone G, et al. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208. doi:10.1016/0168-8510(90)90421-9
25. Milger K, Korn S, Feder C, et al. Kriterien zur Evaluation des Ansprechens auf Biologika bei schwerem Asthma – der Biologics Asthma Response Score (BARS) [Criteria for evaluation of response to biologics in severe asthma - the Biologics Asthma Response Score (BARS)]. Pneumologie. 2023;2023:1. German.
26. Jacobi F, Höfler M, Strehle J, et al. Psychische Störungen in der Allgemeinbevölkerung. Studie zur Gesundheit Erwachsener in Deutschland und ihr Zusatzmodul „Psychische Gesundheit (DEGS1-MH) [Mental disorders in the general population: study on the health of adults in Germany and the additional module mental health (DEGS1-MH)]. Nervenarzt. 2014;85(1):77–87. German. doi:10.1007/s00115-013-3961-y
27. Chen MH, Su T-P, Chen Y-S, et al. Higher risk of developing major depression and bipolar disorder in later life among adolescents with asthma: a nationwide prospective study. J Psychiatr Res. 2014;49:25–30. doi:10.1016/j.jpsychires.2013.10.015
28. Dering MR, Lepsy N, Fuge J, et al. Prevalence of mental disorders in patients with chronic thromboembolic pulmonary hypertension. Front Psychiatry. 2022;13:821466. doi:10.3389/fpsyt.2022.821466
29. Olsson KM, Meltendorf T, Fuge J, et al. Prevalence of mental disorders and impact on quality of life in patients with pulmonary arterial hypertension. Front Psychiatry. 2021;12:667602. doi:10.3389/fpsyt.2021.667602
30. Zhang MW, Ho RCM, Cheung MWL, et al. Prevalence of depressive symptoms in patients with chronic obstructive pulmonary disease: a systematic review, meta-analysis and meta-regression. Gen Hosp Psychiatry. 2011;33(3):217–223. doi:10.1016/j.genhosppsych.2011.03.009
31. Willgoss TG, Yohannes AM. Anxiety disorders in patients with COPD: a systematic review. Respir Care. 2013;58(5):858–866. doi:10.4187/respcare.01862
32. Matcham F, Davies R, Hotopf M, et al. The relationship between depression and biologic treatment response in rheumatoid arthritis: an analysis of the British Society for Rheumatology Biologics Register. Rheumatology. 2018;57(5):835–843. doi:10.1093/rheumatology/kex528
33. Michelsen B, Kristianslund EK, Sexton J, et al. Do depression and anxiety reduce the likelihood of remission in rheumatoid arthritis and psoriatic arthritis? Data from the prospective multicentre NOR-DMARD study. Ann Rheum Dis. 2017;76(11):1906–1910. doi:10.1136/annrheumdis-2017-211284
34. Rathbun AM, Harrold LR, Reed GW. A prospective evaluation of the effects of prevalent depressive symptoms on disease activity in rheumatoid arthritis patients treated with biologic response modifiers. Clin Ther. 2016;38(7):1759–1772.e3. doi:10.1016/j.clinthera.2016.06.007
35. Ciechanowski PS, Katon WJ, Russo JE. Depression and diabetes: impact of depressive symptoms on adherence, function, and costs. Arch Intern Med. 2000;160(21):3278–3285. doi:10.1001/archinte.160.21.3278
36. Tarrants M, Oleen-Burkey M, Castelli-Haley J, et al. The impact of comorbid depression on adherence to therapy for multiple sclerosis. Mult Scler Int. 2011;2011:271321. doi:10.1155/2011/271321
37. Dowlati Y, Herrmann N, Swardfager W, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. 2010;67(5):446–457. doi:10.1016/j.biopsych.2009.09.033
38. Oyamada HAA, Cafasso MOSD, Vollmer CM, et al. Major depressive disorder enhances Th2 and Th17 cytokines in patients suffering from allergic Rhinitis and Asthma. Int Arch Allergy Immunol. 2021;182(12):1155–1168. doi:10.1159/000517478
39. Kharaba Z, Feghali E, El Husseini F, et al. An assessment of quality of life in patients with Asthma through physical, emotional, social, and occupational Aspects. A cross-sectional study. Front Public Health. 2022;10:883784. doi:10.3389/fpubh.2022.883784
40. Yohannes AM. Management of anxiety and depression in patients with COPD. Expert Rev Respir Med. 2008;2(3):337–347. doi:10.1586/17476348.2.3.337
41. Smoller JW, Pollack MH, Otto MW, et al. Panic anxiety, dyspnea, and respiratory disease. Theoretical and clinical considerations. Am J Respir Crit Care Med. 1996;154(1):6–17. doi:10.1164/ajrccm.154.1.8680700
42. McCarron RM, Shapiro B, Rawles J, et al. Depression. Ann Intern Med. 2021;174(5):Itc65–itc80. doi:10.7326/AITC202105180
43. DeMartini J, Patel G, Fancher TL. Generalized Anxiety Disorder. Ann Intern Med. 2019;170(7):Itc49–itc64. doi:10.7326/AITC201904020
44. Yohannes AM, Willgoss TG, Baldwin RC, et al. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: prevalence, relevance, clinical implications and management principles. Int J Geriatr Psychiatry. 2010;25(12):1209–1221. doi:10.1002/gps.2463
45. Russell RJ, Brightling C. Pathogenesis of asthma: implications for precision medicine. Clin Sci. 2017;131(14):1723–1735. doi:10.1042/CS20160253
46. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101–2107. doi:10.1001/archinte.160.14.2101
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Impact of Anxiety and Depression on the Level of Asthma Control Among Jordanian Adults with Asthma
Abu Al Karsaneh O, Al Anber A, Al Shboul S, Alrjoub M, Almashaqbeh OI, Alqaisi M, Abuatieh R, Ananzeh SM, Hamad AM, Almomani R, Tommalieh MM
Journal of Asthma and Allergy 2024, 17:463-476
Published Date: 19 May 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025
Montelukast Prescription Prevalence and Impact on Clinical Outcomes Among Patients with Asthma: A Cross-Sectional Study in Saudi Arabia
Alqarni AA, Aldhahir AM, Siraj RA, Alqahtani JS, Alghamdi RM, Baqais TA, Najrani NA, Albarqi AZ, Alasimi AH, Alwafi H
Journal of Asthma and Allergy 2026, 19:607631
Published Date: 30 June 2026