Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Relationship Between Psychological Contract Violation and Physicians’ Destructive and Constructive Behaviors in Tertiary Public Hospitals: An Empirical Evidence in Beijing
Authors Hu L, Chen C, Zhu J ![]() , Zhang Y, Chen Y, Jia Y
, Zhang Y, Chen Y, Jia Y
Received 15 November 2022
Accepted for publication 17 February 2023
Published 7 April 2023 Volume 2023:16 Pages 997—1010
DOI https://doi.org/10.2147/JMDH.S397501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Scott Fraser
Lujia Hu,1,2,* Chen Chen,1,* Junli Zhu,1 Yao Zhang,3 Yun Chen,4,5 Yufei Jia6
1School of Public Health, Capital Medical University & Research Center for Capital Health Management and Policy, Beijing, People’s Republic of China; 2Department of Basic Health Care, Tianjin Hedong District Health Commission, Tianjin, People’s Republic of China; 3Department of Human Resources, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 4The National Clinical Research Center for Mental Disorders & Beijing Key Laboratory of Mental Disorders, Beijing Anding Hospital, Capital Medical University, Beijing, People’s Republic of China; 5Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, People’s Republic of China; 6Department of Human Resources, Beijing Shijitan Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junli Zhu, School of Public Health, Capital Medical University & Research Center for Capital Health Management and Policy, No. 10, Xitoutiao, Youanmen Wai, Fengtai District, Beijing, 100069, People’s Republic of China, Tel +86 18701515093, Fax +86 01083911578, Email [email protected]
Background: In China, physicians have long faced long working hours, high stress levels, and tensions between physicians and patients, which can lead to negative behaviors. Understanding physicians’ expectations and requirements of the hospital and increasing satisfaction with their psychological contract can help improve physician motivation and stabilize the hospital team.
Aim: The study aims to analyze the relationship between physicians’ psychological contract violations and different behavioral choices, encourage hospitals to conclude a balanced psychological contract with physicians, and provide governance and intervention strategies for hospital human resource management.
Methods: Stratified cluster sampling was used to select 321 physicians from four public hospitals in Beijing for questionnaire surveys. Descriptive statistical analysis, t-test, ANOVA, correlation analysis, and regression models were performed using Stata 15.0 and SPSS 26.0 to analyze the relationship between psychological contract violations, physicians’ EVLN behaviors and organizational justice.
Results: Psychological contract violation had a positive effect on exit behavior and neglect behavior, and a negative effect on voice behavior and loyalty behavior. Organizational justice plays a mediating role between psychological contract violation and physicians’ exit, voice and loyalty behaviors.
Conclusion: Psychological contract violation can drive negative behavior among physicians, and organizational justice can play a mediating role in this. Public hospitals should establish a healthy psychological contract with physicians and place a premium on organizational justice to promote constructive behaviors and prevent destructive behaviors. This study constructs a more complete theoretical framework to explain physicians’ behavior, and further dynamic tracking investigations are necessary because the evolution of physicians’ behavior is a dynamic and long-term process.
Keywords: tertiary public hospitals, physicians, psychological contract violation, EVLN, China, mediation effect
Introduction
Physicians, as the main providers of medical services in hospitals, have decision-making authority for admitting and discharging patients, performing clinical operations, and prescribing medications. Yet Chinese medical staff have long faced long working hours, high levels of stress, under-valued labor, and strained physician-patient relationships, especially violence by patients against physicians.1,2 From July 2001 to July 2018, there were 47 medical injuries resulting in the death of medical personnel, which greatly affected physicians’ sense of security and work ethic.3 The “Physician Career Satisfaction” survey conducted by China Youth Daily and Chunyu Doctor revealed that 39.6% of physicians were dissatisfied with their jobs.4 The results of Chinese medical institutions’ physician turnover survey in 2015 showed that the proportion of physicians who had the intention to leave was 45.4%, 58.0% and 63.4% in primary, secondary and tertiary hospitals respectively.5 Public hospitals are the main body of China’s medical service system, accounting for almost 89% of hospital beds and 92% of hospital admissions.6 As the capital of China, Beijing has over 100 tertiary hospitals and many national medical centers, and the tertiary public hospitals lead the country in terms of workload.7 The high volume of outpatient and emergency care, the complexity of patient conditions, and the heavy teaching and research tasks often make physicians have a higher stress level, which in turn leads to anti-productivity behaviors such as hidden absenteeism.8 Healthcare staff are the important implementer of public hospital reform.9 For hospital managers, understanding physicians’ expectations and requirements of the hospital and enhancing the satisfaction of their psychological contract can help improve physicians’ motivation, activate physicians’ creativity and stabilize the team.
The psychological contract refers to individual beliefs, shaped by the organization, regarding terms of an exchange agreement between individual and organization.10 Schein (1980) pointed out that the “self-evident” contract that exists in people’s subconscious mind is an important factor that influences employees’ attitudes and behaviors toward the organization.11 Previous researchers conclude that psychological contract violation may occur when the organization violates on purpose or for unforeseen reasons, and it may also occur when employees’ understanding of organizational commitments is inconsistent with the organization.10,12,13 Argyris (1957) first developed the idea that psychological contracts can have an impact on employees’ attitudes and behaviors.14 Then some researchers used psychological contract theory to explore the hospital-physician relationship and found that the fulfillment of the psychological contract can result in positive attitudinal and behavioral responses of physicians, such as job satisfaction and organizational citizenship behavior.15,16 The violation of the psychological contract can lead to negative physician attitudes and behaviors, such as job dissatisfaction and thoughts of quitting.17,18 Collins et al (2020) found that psychological contract violation was negatively associated with physicians’ job satisfaction and well-being.19
Hirschman (1970) and Farrell (1983) summarized the employee behaviors that emerge in job dissatisfaction as EVLN behaviors, which are exit behavior, voice behavior, loyalty behavior, and neglect behavior.20,21 “Exit” is the tendency and behavior of employees to leave the organization through resignation, transfer, or finding a new job. “Voice” refers to the behavior of employees to improve their environment and conditions through active efforts such as discussing work difficulties with their supervisors or colleagues, taking actions to solve the difficulties, or seeking outside help. “Loyalty” refers to the behavior of employees to passively but optimistically wait for improvement of the environment and conditions by giving the organization support and acting as a well-behaved citizen. “Neglect” refers to the behavior of employees temporarily abandoning work by reducing effort, being late or absent for a long time, doing private tasks during working hours, and increasing the error rate. According to the destructive-constructive dimensions, “Exit” and “Neglect” are destructive behaviors, while “Voice” and “Loyalty” are constructive behavior.21
There have been studies exploring the effect of psychological contract violation on employee behavior based on EVLN theory.22,23 Yet studies applying psychological contract theory to physicians’ behavior are limited, especially in China. Unlike the international mainstream that the physicians are freelance practitioners, Chinese physicians are “unit persons” and are affiliated with medical institutions, which hinders the mobility of Chinese physicians. Cultural differences between China and the Western countries may also cause Chinese physicians to behave differently in the face of psychological contract violations. Zhang et al (2020) designed a psychological contract scale for pharmacists and argued that psychological contract theory could be used in hospital pharmacy.24 Accordingly, this study takes physicians in Beijing public hospitals as the subject to explore physicians’ behavioral choices in the face of psychological contract violations. EVLN theory provides a framework for employees’ responses to psychological contract violation. Physicians respond to psychological contract violation by increasing turnover and negligence, as well as reducing their voice and loyalty; psychological contract fulfillment increase physicians’ constructive behaviors because their needs are met.25,26 Therefore, we argue the following:
Hypothesis 1: Psychological contract violation is significantly related to physicians’ EVLN behaviors. Hypothesis 1a: Psychological contract violation is negatively related to physicians’ constructive behaviors in public hospitals, including “voice” and “loyalty” behaviors. Hypothesis 1b: Psychological contract violation is positively related to physicians’ destructive behaviors, including “exit” and “neglect” behaviors.
Also of interest is that previous research has found that organizational justice can strongly influence the relationship between psychological contract violations and employee responses. Organizational justice refers to the perceptions of fairness in organizational decision-making and resource allocation.27 Leineweber (2020) found that team turnover was negatively related with changes in interpersonal justice perceptions.28 Zhou, P.(2019) found that organizational justice was an important mediator of the negatively correlation between physicians’ psychological contract violation and their willingness to leave, and that physicians were likely to have the intention to leave if salary distribution and development opportunities were unfair.29 It has also been shown that when physicians perceive higher levels of psychological contract and organizational justice fulfillment, they have higher job satisfaction, lower intention to leave, and higher motivation to contribute to the organization.16,17,30 Thus we also tested the mediating role of organizational justice in the relationship between psychological contract violation and physician EVLN behavior. This leads to our hypothesis:
Hypothesis 2: Organizational justice plays an intermediary role between physicians’ psychological contract violation and EVLN behavior. Hypothesis 2a: Psychological contract violation is negatively related to organizational justice. Hypothesis 2b: Organizational justice is significantly related to physicians’ constructive behaviors in public hospitals, including “voice” and “loyalty” behaviors. Hypothesis 2c: Organizational justice is significantly related to physicians’ destructive behaviors, including “exit” and “neglect” behaviors.
Materials and Methods
Sample and Data
In this study, stratified cluster sampling was used to conduct a questionnaire survey of physicians in four public hospitals in Beijing. Beijing’s tertiary public hospitals are mainly concentrated in Dongcheng District, Xicheng District, Haidian District, Fengtai District, and Chaoyang District. First, we randomly selected three districts from the above five districts, namely Dongcheng District, Xicheng District and Haidian District. Secondly, we randomly selected one hospital in each of the three districts, and two general hospitals and one specialty hospital were selected. In order to ensure the representativeness of the hospitals, we added one more specialist hospital to the sample. Two general hospitals and two specialty hospitals were finally identified. Finally, the samples were selected from the formal clinicians of the four hospitals by using proportional sampling according to the hospital size. The specific sampling process as shown in Figure 1. The questionnaire was anonymous, and all respondents voluntarily participated and signed written informed consent. To ensure the quality of the investigation, the investigators were trained in questioning techniques and communication skills. This study passed the ethical review of the Medical Ethics Committee of Capital Medical University.
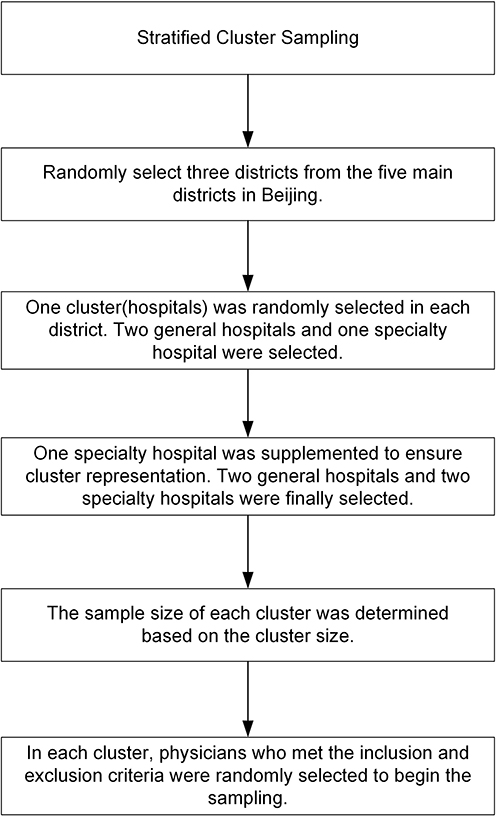 |
Figure 1 Flowchart of sampling. |
The inclusion criteria for survey subjects of this study were as follows: (1) voluntary participation in this study and (2) physicians without management positions and working for more than one year. The exclusion criteria were the physicians who are temporarily in the hospital for advanced studies, job-training, or internship. A total of 321 questionnaires were distributed, of which 292 were valid, with an effective rate of 91%. The sample sizes of the four selected hospitals were 42, 40, 120 and 90, respectively.
Instruments
The instrument in this study was adapted from the relevant literature, which showed sound levels of reliability and constructs validity. The scale for physician psychological contract violation was referenced from Russeau (1990) and Turnley & Feldman (1999).13,31 There are 12 items, such as “The hospital pays salaries and bonuses based on your performance”, “The hospital maintains a harmonious relationship between colleagues”, etc. The EVLN behavior scale was referenced from Rusbult (1988) and includes 18 items.32 Organizational justice was referenced from Colquitt’s (2001) organizational justice scale.33 The meta-analysis of Hauenstein, McGonigle, and Flinder (2001) suggested that a simpler view of justice is one that focuses on general perceptions of justice, rather than specific forms of justice.34 Therefore, this study explored the overall justice dimension, named perceptions of organizational justice (JUST). Further define the questionnaire items by following several steps:
First, we translated the English scale into Chinese. Second, two professors and three hospital HR managers assisted in reviewing the Chinese questionnaire for appropriateness. Third, a pilot study was executed for modifying the questionnaire. The pilot study was conducted by recruiting medical students because the demographic characteristics of medical students are highly homogeneous and the influence of demographic characteristics factors can be avoided, followed by the fact that medical students mostly have internship experience and their behavioral choices are close to physicians, which can be used as the study subjects for the pilot study. Finally, a total of 211 medical students participated in the questionnaire. A 5-point Likert scale was used, with scores from 1 to 5 representing “strongly disagree” to “strongly agree”. Exploratory factor analysis (EFA) was used to extract behavioral dimensions. The items with loads less than 0.5 on their own factor or greater than 0.3 on other factors were removed from the analysis.35 The results of pilot study showed that the scale had acceptable reliability and validity and could be adopted.
Analysis
The relationship between the variables was: (1)  (2)
(2)  (3)
(3)  Where EVLN represents the exit, voice, loyalty, and neglect behavior; PCV represents the psychological contract violation; βi1 represents the standardized regression coefficients for psychological contract violation in equation i; β32 represents the standardized regression coefficients for organizational justice on EVLN; βi0 represents the constant of equation i. The significant mediating effect must satisfy: 1. The independent variable in Equations 1 and 2 can predict the dependent variable and the intermediate variable, β11, and β21 are significant; 2. The intermediate variable in Equation 3 can predict the dependent variable, and β32 is significant; 3. After the intermediate variable is introduced in Equation 3, the influence of the independent variable on the dependent variable must be weakened or eliminated, β31 < β11 (partial mediation) or β31 is not significant (complete mediation).
Where EVLN represents the exit, voice, loyalty, and neglect behavior; PCV represents the psychological contract violation; βi1 represents the standardized regression coefficients for psychological contract violation in equation i; β32 represents the standardized regression coefficients for organizational justice on EVLN; βi0 represents the constant of equation i. The significant mediating effect must satisfy: 1. The independent variable in Equations 1 and 2 can predict the dependent variable and the intermediate variable, β11, and β21 are significant; 2. The intermediate variable in Equation 3 can predict the dependent variable, and β32 is significant; 3. After the intermediate variable is introduced in Equation 3, the influence of the independent variable on the dependent variable must be weakened or eliminated, β31 < β11 (partial mediation) or β31 is not significant (complete mediation).
This study used Stata 15.0 and SPSS 26.0 for descriptive statistics analysis, exploratory factor analysis, and regression modeling. The differences between participant characteristics and EVLN behaviors was explored using the independent t-test and one-way ANOVA. The correlations between variables were assessed via Pearson’s correlation coefficients. The hierarchical regression analysis was used to test the mediating effects of organizational justice on the relationship between psychological contract violation and EVLN behavior. The Sobel test was used to explore the mediating effect of organizational justice between psychological contract violation and EVLN behavior.36 Cronbach’s alphas and coefficients were used to assess the reliability and validity of the scales.
Results
Reliability and Validity of the Scale
Psychological Contract Violation Scale
The KMO value was 0.95 and the Bartlett’s sphericity test was significant, which demonstrated that the data were suitable for factor analysis. Principal component analysis was used to extract factors with eigenvalues greater than to 1. There was 1 main factor extracted, and the cumulative variance explained was 66.19%, indicating that the scale is a single dimensional structure. Internal consistency measured through Cronbachs’ α was 0.95, indicating a good stability of the scale.
EVLN Scale
Three items (two neglected behavior items and one voice behavior item) were deleted to ensure the validity of the scale, and 15 items were retained at the end. The KMO value was 0.87 and the Bartlett’s sphericity test was significant, allowing the EFA to be conducted. The EFA showed a four-factor solution as shown in Table 1, with a cumulative contribution of 70.24%. The factor composition was the same as the questionnaire dimensions, named exit behavior, neglect behavior, voice behavior, and loyalty behavior, respectively. The Cronbach’s α value for the overall scale was 0.75, and the Cronbach’s α values for the exit, voice, loyalty, and neglect behavior dimensions were 0.87, 0.89, 0.80, and 0.84, respectively, indicating a good stability of the scale.
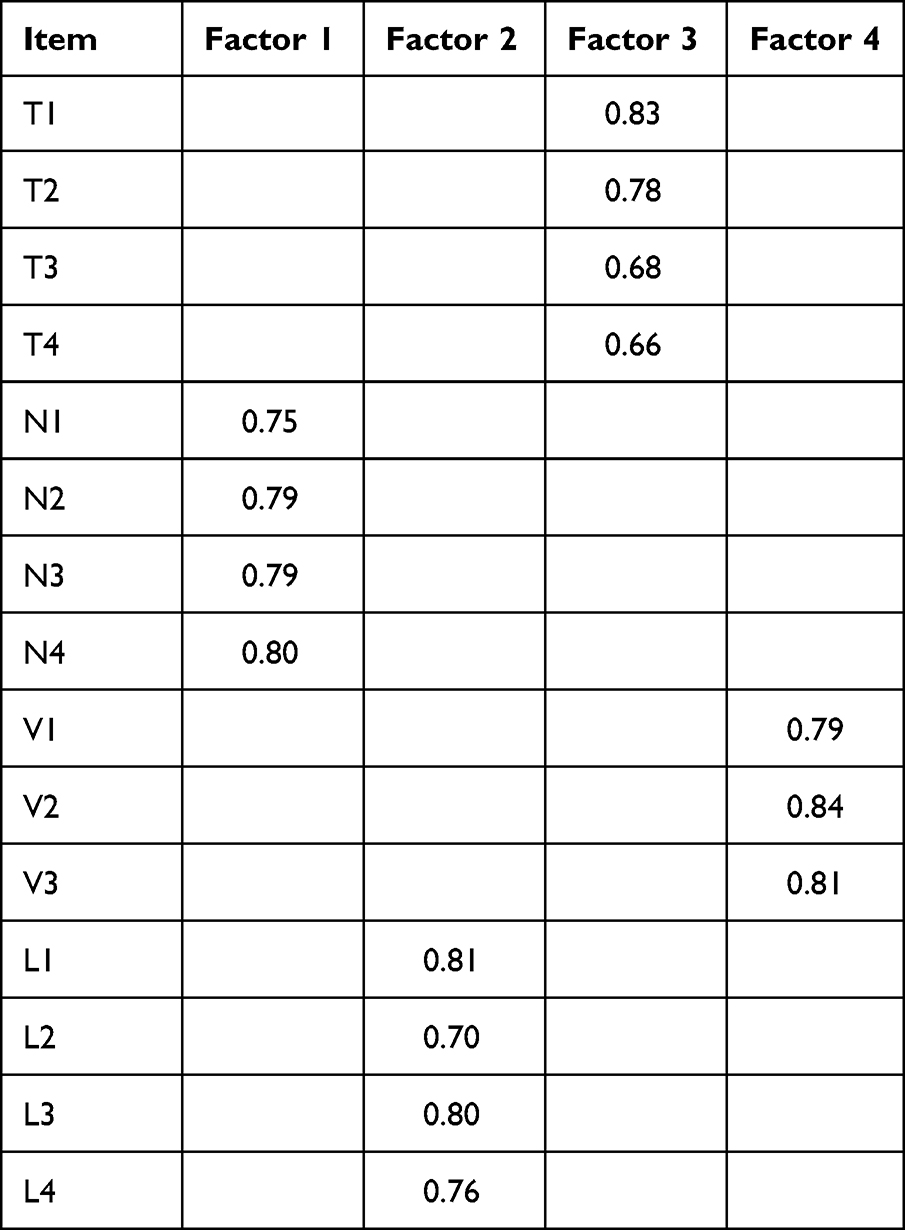 |
Table 1 Factor Load Matrix After Rotation |
Organizational Justice Scale
The KMO value was 0.94 and the Bartlett’s sphericity test was significant, which demonstrated that the data were suitable for factor analysis. Principal component analysis was used to extract factors with eigenvalues greater than to 1. There was 1 main factor extracted, and the cumulative variance explained was 70.50%, indicating that the scale is a single dimensional structure. Internal consistency measured through Cronbachs’ α was 0.96, indicating a good stability of the scale.
The Respondents’ Characteristics
The characteristics of the respondents are shown in Table 2. It can be seen that the 292 respondents in this study included 71.92% from general hospitals and 28.08% from specialized hospitals. Among the respondents, 185 (63.36%) were female and 230 (78.77%) were married. 3.77% of respondents were aged less than or equal to 25, 40.41% were 26–35 years, 38.70% were 36–45 years and 17.12% were 46–55 years. Most respondents (84.25%) had gotten master’s degree or above. Physicians of key disciplines comprised 51.03%, while physicians of non-key disciplines comprised 48.97%. As for working years, 29.11% had worked for over 15 years, followed by those for 11–15 years and those for 6–10 years and less than or equal to 5 years accounted for 14.73%, 25.68%, and 30.48% respectively. Respondents who were chief physicians accounted for 7.29%, associate chief physicians were 27.74%, 33.90% were attending physicians, and physicians or below comprised 31.07%.
 |
Table 2 The Basic Information of Respondents (n=292) |
The Differences in Demographic Characteristics of EVLN Behavior
Table 2 shows that there were statistically significant differences in EVLN behaviors among different participants’ characteristics. There were significant differences in exit behaviors among physicians in different section category (t=−2.845, p<0.01); there were significant differences in neglect behavior among physicians in different hospital category (t=−2.876, p<0.01), gender (t=1.921, p<0.1) and section category (t=−2.887, p<0.01); there were significant differences in voice behavior among physicians in different hospital category (t=3.569, p<0.01), age (F=1.971, p<0.1) and section category (t=1.876, p<0.1); and there were significant differences in loyalty behavior among physicians in different hospital category (t=3.631, p<0.01), gender (t=−3.428, p<0.01) and section category (t=3.487, p<0.01).
Relationship Between the Variables
Table 3 shows the mean level of the physician’s EVLN behavior choices, perceptions of organizational justice and psychological contract violations, and the correlations between them. The mean scores for exit, neglect, voice, and loyalty behaviors were 2.360, 1.894, 3.182, and 3.403, respectively, indicating higher scores for constructive behaviors than destructive behaviors. The results also showed that psychological contract violation was significantly related to physicians’ EVLN behaviors. Psychological contract violation was positively correlated with exit behavior (r=0.295, P<0.05) and neglect behavior (r=0.127, P<0.1), and negatively correlated with voice behavior (r=−0.246, P<0.05) and loyalty behavior (r=−0.466, P<0.05), which means physicians who experience higher levels of psychological contract violation were more likely to be burned out or even leave the organization and to be less enthusiastic and attached to their work environment.
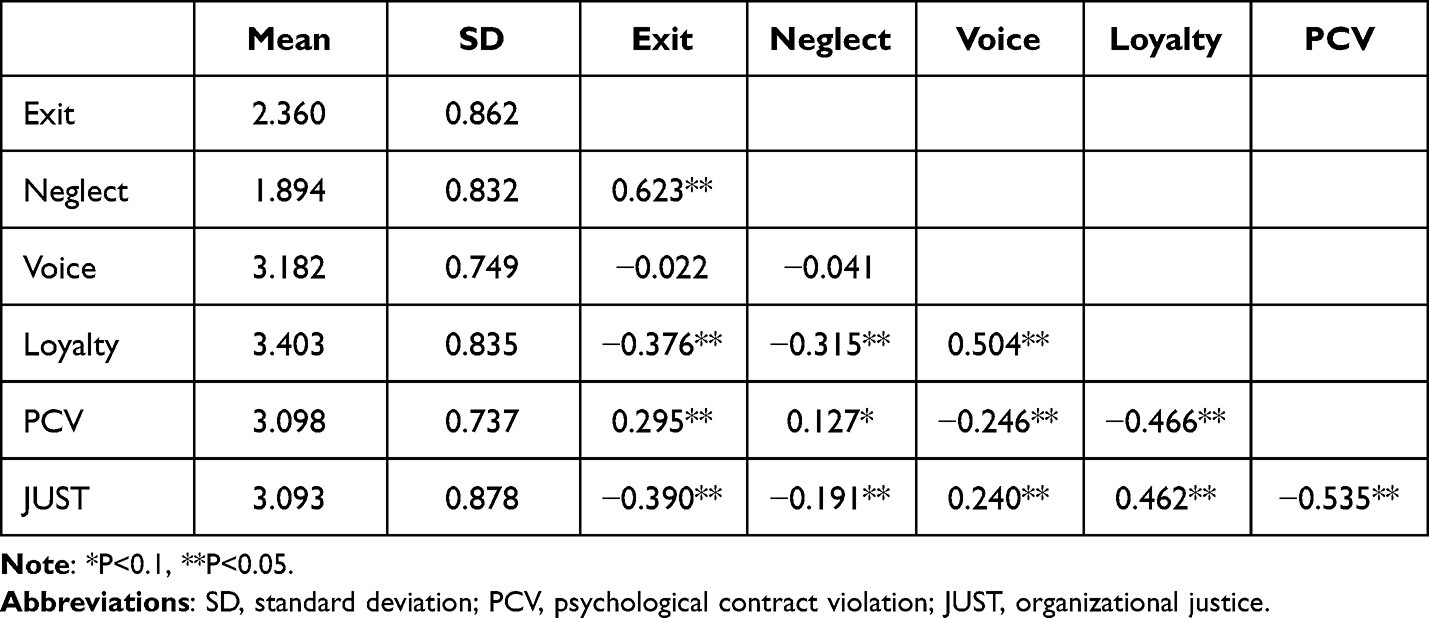 |
Table 3 Correlation Analysis of Variables (n=292) |
Regression Analysis Results
The variance inflation factor for each variable was not greater than 5, so the multi-collinearity was within the acceptable level. In Table 4, the results of model (1) showed that psychological contract violation positively affects physician exit behaviors (P<0.01) and negatively affects physician voice and loyalty behaviors, which indicates that hypotheses H1a and H1b were accurate. Model (2) showed that psychological contract violation negatively affects organizational justice, which indicates that hypotheses H2a was accurate. Model (3) introduced organizational justice based on model (1), and the effect of psychological contract violation on EVLN behavior changed at this point. Organizational justice positively affects constructive behavior and negatively affects destructive behavior, indicating that hypothesis H2b and H2c is supported. The results showed that the regression coefficient of psychological contract violation on exit behavior decreased (P<0.1), indicating that organizational justice partially mediated the effect between psychological contract violation and exit behavior. Figure 2 illustrated the mediation regression equations in a path diagram. The absolute value of the regression coefficients of psychological contract violations on voice and loyalty behaviors decreased (P<0.05), indicating that organizational justice played a part in the mediating role. Hypothesis H2 was supported. Besides, model (1) showed that the regression coefficient of gender was significant in neglect and loyalty behavior (β=−0.185, p<0.1; β=0.335, p<0.01). Model (2) showed that the regression coefficient of gender in organizational justice was significant (β=0.232, P<0.05); model (3) showed that the regression coefficient of gender was no longer significant in neglect behavior (β=−0.149, P>0.1) and decreased in loyalty behavior (β=0.277, P<0.05), indicating that organizational justice played a mediating role between gender and neglect and loyalty behavior. Table 4 also showed that the mediating role of organizational justice accounts for more than 33% of the total effect and even up to 56.6% of exit behavior. This suggests that when psychological contract violations occur, physician behavior is affected primarily through physicians’ perceptions of organizational justice.
 |
Table 4 The Correlation Between Psychological Contract Violation and EVLN and the Mediating Role of Justice |
 |
Figure 2 Mediating effect of organizational justice between psychological contract violation and EVLN behavior. (Notes: on the connecting line pointing to constructive and destructive behaviors, bolded are the regression coefficients of PCV or Justice when voice and exit behaviors are the dependent variables, and unbolded are the regression coefficients of PCV or Justice when loyalty and neglect behaviors are the dependent variables; *P<0.1, **P<0.05, ***P<0.01). |
Discussion
Under the background of the new round of medical and health system reform, hospital structures and strategies have been adjusted: the previous departmental, hierarchical, and colleague relationships have changed, which may break physicians’ previous psychological contracts. Psychological contract violation is inevitable in organizations. The violation and imbalance of the psychological contract can lead to an increase in physician dissatisfaction and trigger different behaviors. Physicians play a vital role in hospitals. Pay attention to guiding physician behaviors and creating a better physician-hospital relationship is of great significance to the challenges of current society.
The study found that Chinese physicians showed more constructive than destructive behaviors in the organization. Construction behaviors scored higher, “loyalty” behaviors scored highest, while destructive behaviors scored lower and “neglect” behaviors scored lowest. This may be related to the special status of physicians in public hospitals in China. Public hospitals are public institutions in China, and physicians in public hospitals are similar to civil servants, with stable jobs and high social status that are very attractive to young physicians. In recent years, the Chinese government has begun to implement reforms in the personnel system of public hospitals, including the removal of institution staff member, making it even more precious to have this status. At the same time, this study also found that the perceived psychological contract violation of Chinese public hospital physicians are both at an upper-middle level, which is higher than the perception of Flemish physicians (2.86) in the study conducted by Trybou (2016) based on data from 130 physicians in six hospitals.30
This study also found that when physicians perceive that the psychological contract is violated, physicians’ building behaviors decrease and disruptive behaviors increase, and these results support previous research findings.13,15–17,30 Psychological contract violation was positively associated with physicians’ intention to leave, and high fulfillment of their psychological contract provided more motivation to contribute to the hospital. These results are consistent with social exchange theory and control theory.37–39 When physicians feel that there is a discrepancy between reality and what the hospital promises, from the perspective of the physician, this difference reflects an imbalance in the social exchange relationship between them and the organization. Physicians have the motivation to eliminate or reduce this imbalance, including both constructive and destructive behaviors. Therefore, it is important to focus on the breach of the physician’s psychological contract when the physician’s behavior changes. In the psychological contract established between hospitals and physicians, hospital responsibilities include providing promotions, offering reasonable remuneration, providing educational and training opportunities, and providing career development opportunities.31 The fulfillment of the hospital’s promised obligations will enable physicians to perform their duties, promote positive behavior and deter negative behavior.
The mediating effects of organizational justice are different for different gender. Before introducing organizational justice as the mediating variable, male’s neglect behavior is less and loyalty behavior is more than female’s, which seems to be “more positive” than female in work. After introducing organizational justice as mediating variable, there is no gender difference in neglect behavior, and the gender difference in loyalty behavior is also reduced, which reminds us that organizational justice is a factor that female attach great importance to. Studies have shown that female may face more potential gender bias in work, which leads to female’s low enthusiasm and pessimism about the organizational environment, with the highest number of female physicians changing their area of practice.40 So, the organization must offer equal rights for male and female, increasing female representation and encouraging equal opportunities through female empowerment. The research also shows that people with professional titles above physicians and in general hospitals have more neglect behavior. It could be partly explained that the working objects and contents of this group are more complex, working intensity is higher, but lack advancement because of the limited job opportunities. So it is easy for physicians to job burnout and even neglective behavior, such as attending to fewer patients or spending less time at the bedside.41 Chênevert (2021) also suggested that stress is a strong precursor of emotional exhaustion as well as a ‘loss spiral’ ultimately culminating in burnout and health problems.42 Therefore, hospitals need to design multiple career development channels for physicians, such as clinical type, teaching type, and scientific research type to make physicians have confidence in their professional development. Meanwhile, hospitals are advised to pay more attention to the health status of physicians with more stress and more complex work tasks, not only helping physicians relieve tension, but also encouraging healthy lifestyles and working patterns.
In addition, this study found that organizational justice mediated the relationship between physician psychological contract violation and EVLN behavior. A high level of organizational justice has a negative buffering effect on psychological contract violations and physicians’ exit behaviors, and a positive buffering effect between psychological contract violations and physicians’ voice and loyalty behaviors. The results suggests that hospitals should pay attention to organizational justice in the development process of hospitals and build a scientific distribution system and evaluation system. In addition to justice in allocation outcomes, attention should be paid to justice in the allocation process. Siun (2019) argued that care for employees and commitment to equitable treatment are the basis of any allocation process.43 Physicians should be allowed to participate in the development of the allocation system as much as possible, and the appraisal system should be combined with physicians’ self needs, self-worth, and sense of honor to ensure that the wishes of the majority of employees are met.
Besides, the study also found that the mediating role of organizational justice was particularly significant for exit behavior (the mediating role of organizational justice accounted for 56.6% of the total effect). Trybon (2016) also showed that in Belgium the organizational justice negatively affected physicians’ intention to leave.30 Pan Y. (2016) believes that organizational justice plays a mediating role between nurses’ psychological contract fulfillment and EVLN behavior in China;44 Zhou P. (2019) took Chinese public hospital physicians as subjects and found that justice was an important mediator of hospital responsibility fulfillment and physician resignation.29 Hu (2013) found that organizational justice is essential to the stability of professional employees.45 These results suggest that as a positive factor, organizational justice has a greater power on destructive behavior because people who are prone to destructive behavior are more sensitive to justice. When people feel that the decision-making process is fair, people are less likely to behave negatively.46–48 Therefore, hospitals should establish a scientific and effective monitoring system to ensure fairness. Only when physicians’ sense of unfairness is reduced, negative behaviors such as resignation will be fundamentally reduced and risks in human resource integration will be decreased.
This study is an extension of the research into the behavioral choices of physicians in organizations. The study has three theoretical contributions. Firstly, most previous studies have discussed only one behavior, in particular exit behavior. Whereas other behavior may have emerged or are emerging prior to the exit behavior, such as decreasing loyalty and increasing neglect. This study provides a more comprehensive and systematic of physicians’ behavior choices based on EVLN theory. Second, EVLN theory is generally used to examine the behavior of corporate employees, and this study applies it to physicians, which is an enrichment of EVLN behavior theory. Third, this study introduces the organizational justice as a mediating variable, which constructs a more complete theoretical framework to explain physicians’ behaviors. The study has two practical contributions. First, physicians in tertiary hospitals are more stressed and more prone to burnout due to society’s high expectations. Focusing on tertiary hospitals, this study explores the root causes of physician behavior change from a psychological contract perspective and explores new ideas for physician motivation. Second, psychological contract violations do lead to negative physician behaviors. Therefore, monitoring the level of psychological contract violation among medical staff is an important part of human resource management.
This study is not without its limitations. First, this study is only conducted on Beijing’s tertiary public hospitals. Further research on factors such as different grades and geographic areas can be considered in the future, while including more hospitals and physicians in order to draw more general conclusions. Second, the evolution of physicians’ behaviors is a dynamic and long-term process. This article only conducted a cross-sectional survey and did not conduct dynamic tracking studies. It would be more meaningful to analyze the changes in physicians’ behaviors before and after reforms to evaluate reform policies. Third, considering that it is difficult to obtain evaluation information from physicians by multiple parties, the effect indicators of this study mainly rely on individual self-evaluation. In the future, information may be collected through multiple channels and methods to ensure comprehensiveness and objectivity. What’s more, quality interview study could be considered in the future to supplement and reinforce the results of the questionnaire.
Conclusion
This study shows that psychological contract violations can have a negative effect on physicians’ constructive behaviors and a positive effect on destructive behaviors. The research also shows that organizational justice has a mediating effect between physicians’ psychological contract violation and EVLN behavior, with the most significant mediating effect on exit behavior. Therefore, it is important to pay attention to physicians’ psychological contract violations and build a good psychological contract relationship between hospitals and physicians to promote their constructive behaviors and prevent the destructive behaviors.
Ethics Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Capital Medical University (protocol code Z2020SY131, date 2020-11-16).
Acknowledgments
The authors thank the editor and the anonymous reviewers for their helpful and constructive comments, which greatly improved the paper.
Funding
The research is supported by the National Natural Science Foundation of China (no.71974133, 71573182).
Disclosure
The authors declare no conflict of interest.
References
1. Tang L, Guan M. Rise of health consumerism in China and its effects on physicians’ professional identity and the physician–patient relationship and communication. Health Commun. 2018;33(5):636–642. doi:10.1080/10410236.2017.1290015
2. Bareeqa SB, Ahmed SI, Samar SS, et al. Prevalence of depression, anxiety and stress in China during COVID-19 pandemic: a systematic review with meta-analysis. Int J Psychiatry Med. 2021;56(4):210–227. doi:10.1177/0091217420978005
3. Wen X. What can we do about the high incidence of violence against physicians? Beijing News; 2020. Available from: https://baijiahao.baidu.com/s?id=1667541621258060511&wfr=spider&for=pc.
4. Wang C, Cheng J, Qi Y. Practicing medicine in the cracks: 68.1% of the interviewed doctors bluntly said that the doctor’s practice environment is poor. China Youth Daily; 2021. Available from: http://politics.people.com.cn/n/2015/0420/c70731-26869588.html.
5. Xu Q. Over 60% of physicians in tertiary hospitals want to resign, hospitals should hurry to find a solution. Health Community; 2016. Available from: https://www.cn-healthcare.com/article/20160628/content-483834.html?from=timeline&isappinstalled=0.
6. Barber SL, Borowitz M, Bekedam H, Ma J. The hospital of the future in China: china’s reform of public hospitals and trends from industrialized countries. Health Policy Plan. 2013;29(3):367–378. doi:10.1093/heapol/czt023
7. Liu J. Research on the Impact of Job Stressors on Occupational Burnout for Clinicians of Level a Tertiary Hospitals in Beijing. University of International Business and Economics; 2020.
8. Zhu J, Zhang M, Zeng J, Liu Y. Current situation and its influencing factors of perceived stress among doctors in Beijing. Occup Health. 2016;32(14):1888–1893. doi:10.13329/j.cnki.zyyjk.2016.0546
9. Li C, Song X. Study on implementation strategy of knowledge employee’s psychological contract management in public hospital. Chin Health Serv Manag. 2012;29(1):64–66+79.
10. Rousseau DM. Psychological contracts in organizations: understanding written and unwritten agreements. Adm Sci Q. 1995;43(1):184–186. doi:10.2307/2393595
11. Schein E. Organizational Psychology. New Jersey: Prentice-Hall; 1980.
12. Morrison EW, Robinson SL. When employees feel betrayed: a model of how psychological contract violation develops. Acad Manag Rev. 1997;22(1):226–256. doi:10.5465/AMR.1997.9707180265
13. Turnley WH, Feldman DC, Discrepancy A. Model of psychological contract violations. Hum Resour Manag Rev. 1999;9(3):367–386. doi:10.1016/S1053-4822(99)
14. Argyris C. The individual and the organization: some problems of mutual adjustment. Adm Sci Q. 1957;2(1):1–24. doi:10.2307/2390587
15. Bellou V. Matching individuals and organizations: evidence from the Greek public sector. Empl Relat. 2009;31(5):455–470. doi:10.1108/01425450910979220
16. Trybou J, Gemmel P, Desmidt S, Annemans L. Fulfillment of administrative and professional obligations of hospitals and mission motivation of physicians. BMC Health Serv Res. 2017;17(28):1–10. doi:10.1186/s12913-017-1990-0
17. Bunderson JS. How work ideologies shape the psychological contracts of professional employees: doctors’ responses to perceived breach. J Organ Behav. 2001;22(7):717–741. doi:10.1002/JOB.112
18. Jeroen TMB, Canfyn S, Lieven A, Paul G. Physiciaé hospital exchanges and extra-role behaviour of physicians: the moderating role of the chief medical officer. Int J Healthc Manag. 2016;9(4):225–235. doi:10.1179/2047971915Y.0000000022
19. Collins A, Beauregard AT. The effect of breaches of the psychological contract on the job satisfaction and wellbeing of doctors in Ireland: a quantitative study. Hum Resour Health. 2020;18(89):1–8. doi:10.1186/s12960-020-00534-3
20. Hanson RA. Exit, voice, and loyalty: response to decline in firms, organizations, and states. By Albert O. Hirschman, (Cambridge: Harvard University Press, 1970. Pp. 162. $6.95.). Am Polit Sci Rev. 1970;64(4):1274–1276. doi:10.1017/S0003055400133611
21. Farrell D. Exit, voice, loyalty, and neglect as responses to job dissatisfaction: a multidimensional scaling study. Acad Manag J. 1983;26(4):596–607. doi:10.2307/255909
22. Turnley WH, Feldman DC. The impact of psychological contract violations on exit, voice, loyalty, and neglect. Hum Relat. 1999;52(7):895–922. doi:10.1177/001872679905200703
23. Si SX, Wei F, Li Y. The effect of organizational psychological contract violation on managers’ exit, voice, loyalty and neglect in the Chinese context. Int J Hum Resour Manag. 2008;19(5):932–944. doi:10.1080/09585190801995849
24. Zhang T, Yin C, Geng Y, Zhou YMJ, Sun S, Tang F. Development and validation of psychological contract scale for hospital pharmacists. J Multidiscip Healthc. 2020;13:1433–1442. doi:10.2147/JMDH.S270030
25. Chatman JA. Improving interactional organizational research: a model of person-organization fit. Acad Manag Rev. 1989;14(3):333–349. doi:10.5465/AMR.1989.4279063
26. Griffeth RW, Hom PW, Gaertner S. A Meta-analysis of antecedents and correlates of employee turnover: update, moderator tests, and research implications for the next millennium. J Manage. 2000;26(3):463–488. doi:10.1177/014920630002600305
27. Greenberg J. A taxonomy of organizational justice theories. Acad Manag Rev. 1987;12(1):9–22. doi:10.5465/AMR.1987.4306437
28. Leineweber C, Peristera P, Bernhard-Oettel C, Eib C. Is interpersonal justice related to group and organizational turnover? Results from a Swedish panel study. Soc Sci Med. 2020;265:113526. doi:10.1016/j.socscimed.2020.113526
29. Zhou P, Shi J, Zhou H. Research on the association mechanism and moderating variables between physician’s perceived hospital accountability status and turnover willingness. China Health Res. 2019;22(6):465–471. doi:10.13688/j.cnki.chr.2019.19032
30. Trybou J, Gemmel P, Annemans L. The impact of economic and noneconomic exchange on physicianì organizational attitudes: the moderating effects of the chief medical officer. Health Care Manage Rev. 2016;41(1):75–85. doi:10.1097/HMR.0000000000000047
31. Rousseau DM. New hire perceptions of their own and their employer’s obligations: a study of psychological contracts. J Organ Behav. 1990;11(5):389–400. doi:10.1002/JOB.4030110506
32. Rusbult C, Farrell D, Rogers G, Mainous AG. Impact of exchange variables on exit, voice, loyalty, and neglect: an integrative model of responses to declining job satisfaction. Acad Manag J. 1988;31(3):599–627. doi:10.2307/256461
33. Colquitt JA, Conlon DE, Wesson MJ, Porter C, Ng KY. Justice at the millennium: a meta-analytic review of 25 years of organizational justice research. J Appl Psychol. 2001;86(3):425–445. doi:10.1037/0021-9010.86.3.425
34. Hauenstein NMA, McGonigle TP, Flinder SW. A meta-analysis of the relationship between procedural justice and distributive justice: implications for justice research. Empl Responsib Rights J. 2001;13(1):39–56. doi:10.1023/A:1014482124497
35. Hair JF. Multivariate Data Analysis: A Global Perspective. Upper Saddle River, NJ: Pearson; 2010.
36. Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol Methodol. 1982;13:290.
37. Adams JS. Toward an understanding of inequity. J Abnorm Psychol. 1963;67(5):422–436. doi:10.1037/h0040968
38. Blau PM. Exchange and Power in Social Life. Routledge; 1964.
39. Carver CS, Scheier MF. Control theory: a useful conceptual framework for personality-social, clinical, and health psychology. Psychol Bull. 1982;92(1):111–135.
40. Lim WH, Wong C, Jain SR, et al. The unspoken reality of gender bias in surgery: a qualitative systematic review. PLoS One. 2021;16(2):e0246420. doi:10.1371/journal.pone.0246420
41. Leung S, Panda M, McIntosh G, et al. Relationship between physician burnout and patient’s perception of bedside time spent by physicians. J Patient Cent Res Rev. 2021;8(1):58–63. doi:10.17294/2330-0698.1764
42. Chênevert D, Kilroy S, Johnson K, Fournier PL. The determinants of burnout and professional turnover intentions among Canadian physicians: application of the job demands-resources model. BMC Health Serv Res. 2021;21(1):993. doi:10.1186/s12913-021-06981-5
43. Gallagher S, Little M. Procedural justice and the individual participant in priority setting: doctors’ experiences. Soc Sci Med. 2019;228:75–84. doi:10.1016/j.socscimed.2019.03.012
44. Yan P. An Empirical Study on the Relationship Between Nurses’ Psychological Contract and Their EVLN Behavior. Zhejiang University of Traditional Chinese Medicine; 2016.
45. Hu G. Research on the Relationship Between Organizational Justice and Turnover Intention of Knowledge-Based Employees in B Company. Shanghai: East China University of Science and Technology; 2013.
46. Brockner J, Wiesenfeld BM. An integrative framework for explaining reactions to decisions: interactive effects of outcomes and procedures. Psychol Bull. 1996;120(2):189–208. doi:10.1037/0033-2909.120.2.189
47. Moorman RH. Relationship between organizational justice and organizational citizenship behaviors: do fairness perceptions influence employee citizenship? J Appl Psychol. 1991;76(6):845–855. doi:10.1037/0021-9010.76.6.845
48. Skarlicki DP, Folger R. Retaliation in the workplace: the roles of distributive, procedural, and interactional justice. J Appl Psychol. 1997;82(3):434–443. doi:10.1037/0021-9010.82.3.434
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.