Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Relationship Between Number of Cardiac Rehabilitation Exercise Training Sessions, Muscle Mass, and Cardiorespiratory Fitness in Rural Elderly Patients with Coronary Artery Disease
Received 7 September 2023
Accepted for publication 27 October 2023
Published 7 November 2023 Volume 2023:16 Pages 3309—3318
DOI https://doi.org/10.2147/JMDH.S434056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Seong Bok Choi, Ji Hee Kim
Department of Rehabilitation Medicine, Wonkwang University School of Medicine and Hospital, Iksan-si, Republic of Korea
Correspondence: Ji Hee Kim, Department of Rehabilitation Medicine, Wonkwang University School of Medicine and Hospital, 895 Muwang-ro, Iksan-si, 54538, Republic of Korea, Tel +82-63-859-1610, Fax +82-63-843-1385, Email [email protected]
Purpose: This study aimed to compare the effects of a cardiac rehabilitation (CR) exercise program on skeletal muscle index (SMI) and cardiorespiratory fitness (CRF) in patients aged ≥ 65 years.
Patients and Methods: From January 2012 to December 2021, patients living in rural regions aged ≥ 65 who underwent percutaneous coronary intervention for acute myocardial infarction (AMI) and at least one CR exercise session were enrolled. We retrospectively reviewed the medical records of the patients who underwent an exercise tolerance test (ETT) at initial and 3-month follow-ups. A total of 36 patients were enrolled who underwent a mean of 6.56 exercise sessions and were divided into groups based on the number of center-based CR (CBCR) sessions: 14 in Group A (≥ 7 sessions) and 22 in Group B (< 7 sessions). In CBCR session, we comprehensively counseled them about their nutrition, smoking cessation et al. Both groups underwent an ETT after 12 weeks. The outcomes were CRF parameters examined by a cardiorespiratory exercise test and the SMI examined by bioimpedance analysis (BIA).
Results: The number of exercise sessions was significantly correlated with the rate of SMI change. Group A showed significant increases in metabolic equivalent of task (MET), maximal oxygen uptake (VO2max), and SMI after 3 months. There were significant differences in the rates of change in MET, VO2max, and SMI between the two groups.
Conclusion: CRF significantly improved in Group A in a short period. Further studies are required to increase long-term CBCR adherence in elderly patients with AMI in rural regions.
Keywords: skeletal muscle index, dose-dependency, aging, adherence, center-base cardiac rehabilitation
A Letter to the Editor has been published for this article.
Introduction
Coronary heart disease (CHD), a type of cardiovascular disease (CVD), encompasses acute myocardial infarction (AMI) and acute coronary syndrome.1 CHD is the leading cause of death worldwide.2 Over 80% of patients dying from CHD were reported to be aged 65 years or older.3 In Korea, patients aged >60 years accounted for 32.9% of all patients with AMI between 2016 and 2020,4 and the mortality rate within three years of diagnosis was reported to be 19.7% in 2016.5
Patients with AMI experience increased functional impairment.6 When AMI occurs in elderly patients, heart complications such as cardiac failure and arrhythmia, fatality rates,7 and complications due to revascularization procedures increase, alongside an increase in the duration of hospitalization.8 Exercise-based cardiac rehabilitation (CR) is a crucial aspect of the comprehensive treatment of CVDs. CR has a positive impact on the health and well-being of elderly patients with CVD, including improvements in athletic performance, reduced risk of falls, increased muscle mass and significantly reduce mortality rates among patients with coronary artery disease (CAD).9–11 However, elderly patients, especially reside in rural regions, show low participation rate and poor adherence due to the poor accessibility to centers.12,13
The world is progressing into an aging demographic, and the decline in muscle mass and strength associated with aging is now recognized as sarcopenia.14 Skeletal muscle mass decreases with age, and cardiopulmonary function decreases proportionally to the degree of muscle mass reduction.15,16 Skeletal muscle mass after AMI was significantly positively correlated with peak oxygen uptake (VO2peak), and primary composite outcomes, including cardiovascular and all-cause deaths, in patients with ST-segment elevation myocardial infarction were reported to be significantly higher in patients with a low appendicular skeletal muscle mass index.17,18
However, after CR, studies have reported improved skeletal muscle index (SMI) in patients with CVD, as well as improved cardiopulmonary function and SMI in patients with coronary artery stenosis aged ≥65 years.19,20 Improvement in cardiopulmonary function with CR is proportional to the amount of exercise, and some studies have reported on the effects of CR in elderly patients with myocardial infarction.21,22 However, in elderly patients aged ≥65 years, few studies have investigated whether CR improves skeletal muscle mass or analyzed the effective number of treatments.
The purpose of this study was to analyze the short-term effects of center-based CR (CBCR) on cardiorespiratory fitness (CRF) and SMI in elderly patients with AMI and to explore the need for CR among elderly people in rural areas.
Materials and Methods
Participants
This single-center, cross-sectional study was a retrospective analysis of data from patients aged ≥65 years who were referred to a tertiary medical institution in a rural region between January 2012 and December 2021 for CR after percutaneous coronary intervention. Among these patients, those who underwent exercise stress tests at treatment initiation and after three months were included in the analysis. Participants in the exercise treatment group were defined as those who participated in at least one session of the CR program. Those who participated in seven or more sessions of the program were classified into the multi-exercise group (Group A), and those who participated in fewer than seven sessions were classified into the less-exercise group (Group B). Those who were unable to participate in CR, those who did not perform both the exercise tolerance test (ETT) and bioelectrical impedance analysis (BIA) in the first and third months due to pain, and those who did not perform sufficiently in the test to the extent of being unable to perform low-intensity exercise, with a respiratory exchange ratio (RER) of 0.8, were excluded.
Clinical data and variables were collected from the Wonkwang University Hospital electronic medical record system. Medical records included age, sex, CR type, number of CR treatments performed, type of AMI, body mass index (BMI), and other comorbidities (hypertension, diabetes, and dyslipidemia). The number of CR treatments was defined as the total number of times each patient underwent a hospital-based outpatient CR program.
Intervention
The CR exercise program consisted of 30–60 min/day of exercise with a frequency of 2–3 times per week, for 12 weeks. The program consisted of 5 min of warm-up stretching, 20 min of light cycling or walking, up to 30 min of exercise, and 5–10 min of cool-down. The exercise program prescribed for each patient included walking, treadmill exercise, power walking, cycling, and yoga after risk classification according to patient exercise capacity, analyzed through the exercise tolerance test, and medical conditions such as ejection fraction and comorbidities. The initial exercise intensity was gradually increased according to the target heart rate. The target heart rate was set at 60–85% reserve heart rate, relative to the heart rate calculated using the maximum heart rate and stable heart rate obtained from the ETT. CBCR provided comprehensive counseling, nutrition counseling feedback, smoking cessation counseling, diet counseling, and overall lifestyle improvements at every visit. Upon visiting the center, the CR program provided exercise booklets and checked the patients’ exercise diaries. CBCR was performed by visiting the hospital and monitoring vital signs, such as heart rate and blood pressure; if outpatient visits were not possible, an exercise program was performed at home. We prescribed home-based CR (HBCR) program as same as CBCR program for all patients to start strength training after 4–6 weeks of onset and were educated about their individualized target HR and Borg scale during exercise. In order to follow up on the short-term adherence to the exercise program, ETT was performed after three months.
Exercise Tolerance Test
All patients referred for CR after AMI participated in the ETT at the time of onset and three months later for an assessment of cardiopulmonary function. A treadmill (Q-stress TM55, Mortara Instrument Inc., WI Milwaukee, USA) was used for ETT, and respiratory gas analysis was conducted using a metabolic gas analyzer (TrueOne ® 2400, ParvoMedics, UT, USA). Blood pressure (BP) and heart rate (HR) were monitored (247BP, SunTech Medical, USA) throughout the testing process, and electrocardiogram (ECG) monitoring was conducted using a 12-lead ECG (Quinton Q-stress, Mortara Instrument Inc., USA) both before and after ETT. To assess CRF, all participants completed a symptom-limited exercise test using their physician’s modified version of the Bruce protocol based on the American Association of Cardiovascular Pulmonary Rehabilitation (AACVPR) guidelines.23 ETT was discontinued in participants who showed symptoms such as chest pain, severe leg pain, and severe dizziness, or those who wanted to discontinue the test due to symptoms.
The following indicators were measured: maximum heart rate (HRmax), maximum oxygen uptake (VO2max), peak minute ventilation (VEpeak), metabolic equivalent of task (MET), respiratory exchange ratio (RER), and ETT total exercise duration.
VO2max is an indicator of the maximum oxygen uptake and consumption by the body during exercise, whereas VEpeak is defined as the maximum volume of air inhaled and exhaled over one minute during exercise. MET is a unit of measurement of the ratio of the amount of energy the body expends during physical activity to the resting metabolism. These three parameters are the most important indices reflecting a patient’s CRF.
Bioelectrical Impedance Analysis
Body composition was analyzed using a BIA (InBody 370®; InBody, Seoul, Korea). This body composition analysis system uses current frequencies of 5, 50, and 250 kHz. Appendicular skeletal muscle mass (ASM; kg) and SMI (kg/m2) were analyzed. ASM was calculated as the sum of the muscle mass in both arms and legs. SMI was calculated as the ASM divided by height squared (m2).
Statistical Analysis
Student’s t-test was used to compare baseline data between groups A and B among the exercise treatment participants. The changes in cardiopulmonary function in each CR group measured using EET at the time of onset and at three months were compared using a paired t-test. The Pearson correlation test was used to analyze the correlation between the rate of change in SMI and the number of participants in CR and the rate of change in exercise capacity in the participants of exercise treatment. All statistical analyses were performed using SPSS version 27 software (SPSS Inc., Chicago, IL, USA). Statistical significance was set at p < 0.05.
Ethics
The study protocol received ethical approval from the Institutional Review Board of Wonkwang University Hospital, Korea (IRB approval number: 2022-12-008). As the data were collected retrospectively, patient consent was not required by the IRB of Wonkwang University Hospital, owing to the retrospective study design. Patient data were reserved confidential and used only for research purposes. This study was conducted according to the Declaration of Helsinki.
Results
Among the patients referred for CR after AMI, 102 patients aged ≥65 years completed ETTs at treatment initiation and at three months. Among these, nine did not undergo both ETT and BIA or could not be followed up after three months; seven discontinued the test due to severe leg and knee pain, dizziness, or chest pain; and three had exercise performance (RER < 0.8) insufficient to meet the low-intensity exercise standards for elderly patients aged ≥65 years and were excluded.24 Subsequently, 83 patients were evaluated, including 36 (43.4%) who participated in CR exercise programs and 47 (56.6%) who participated only in an educational program. The exercise treatment group participated in an average of 6.56 sessions; 14 participated in seven or more sessions of the exercise program (Group A), and 22 participated in less than seven sessions (Group B, Figure 1).
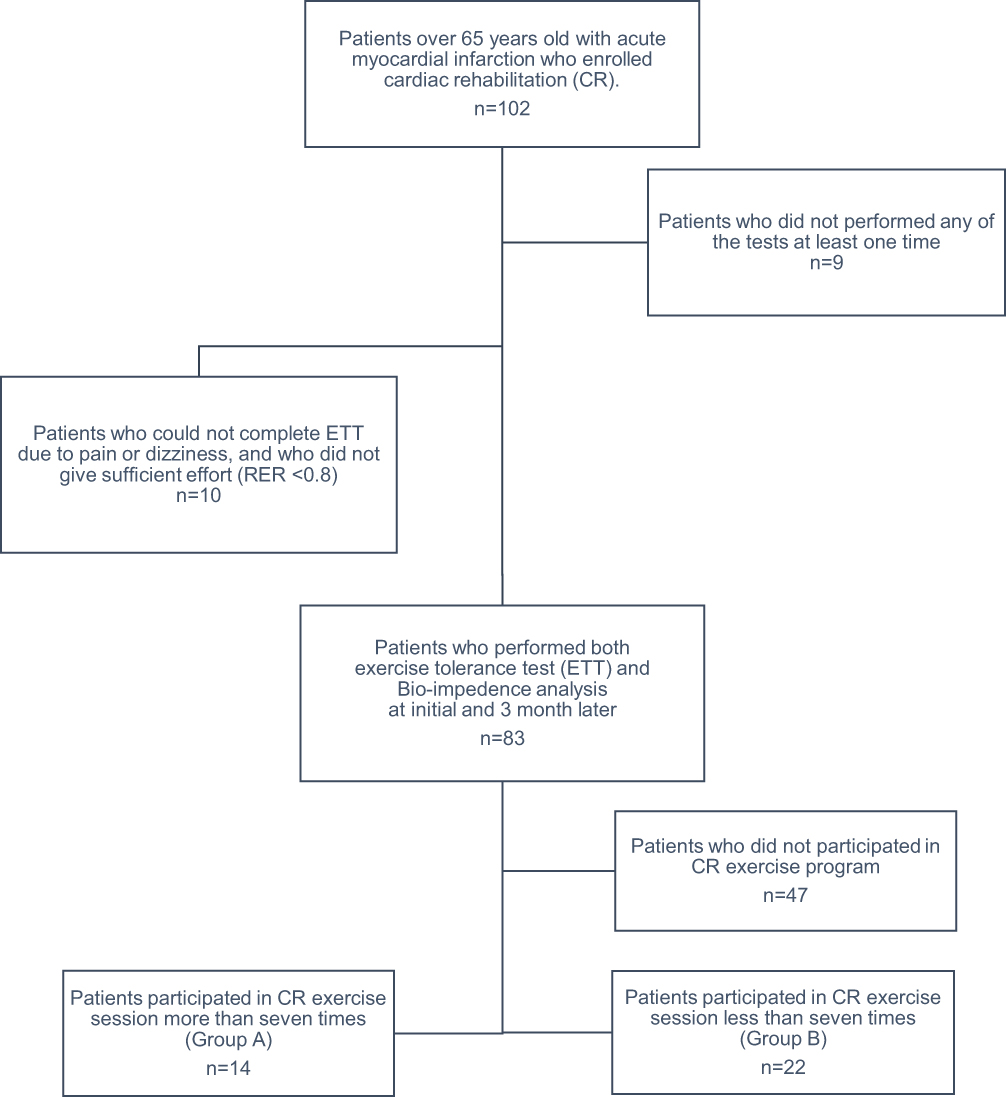 |
Figure 1 Data extraction process. |
There was no significant difference in the mean age before the initial ETT between Groups A and B (69.0 years and 69.5 years, respectively). Group A (seven men, 50%) and Group B (16 men, 72.7%) had no significant difference in sex distribution (p > 0.05). The left ventricular ejection fraction was 49.14% in Group A and 53.0% in Group B, with no significant difference between the two groups (p > 0.05). There were also no significant differences in other demographic characteristics, including BMI. However, there was a significant difference in the mean weight between the two groups, with a mean weight of 61.2 kg in Group A and 67.1 kg in Group B. All indices of exercise capacity, including VO2max, VEpeak, RER and MET, showed no significant difference between the two groups at the initial ETT (Table 1).
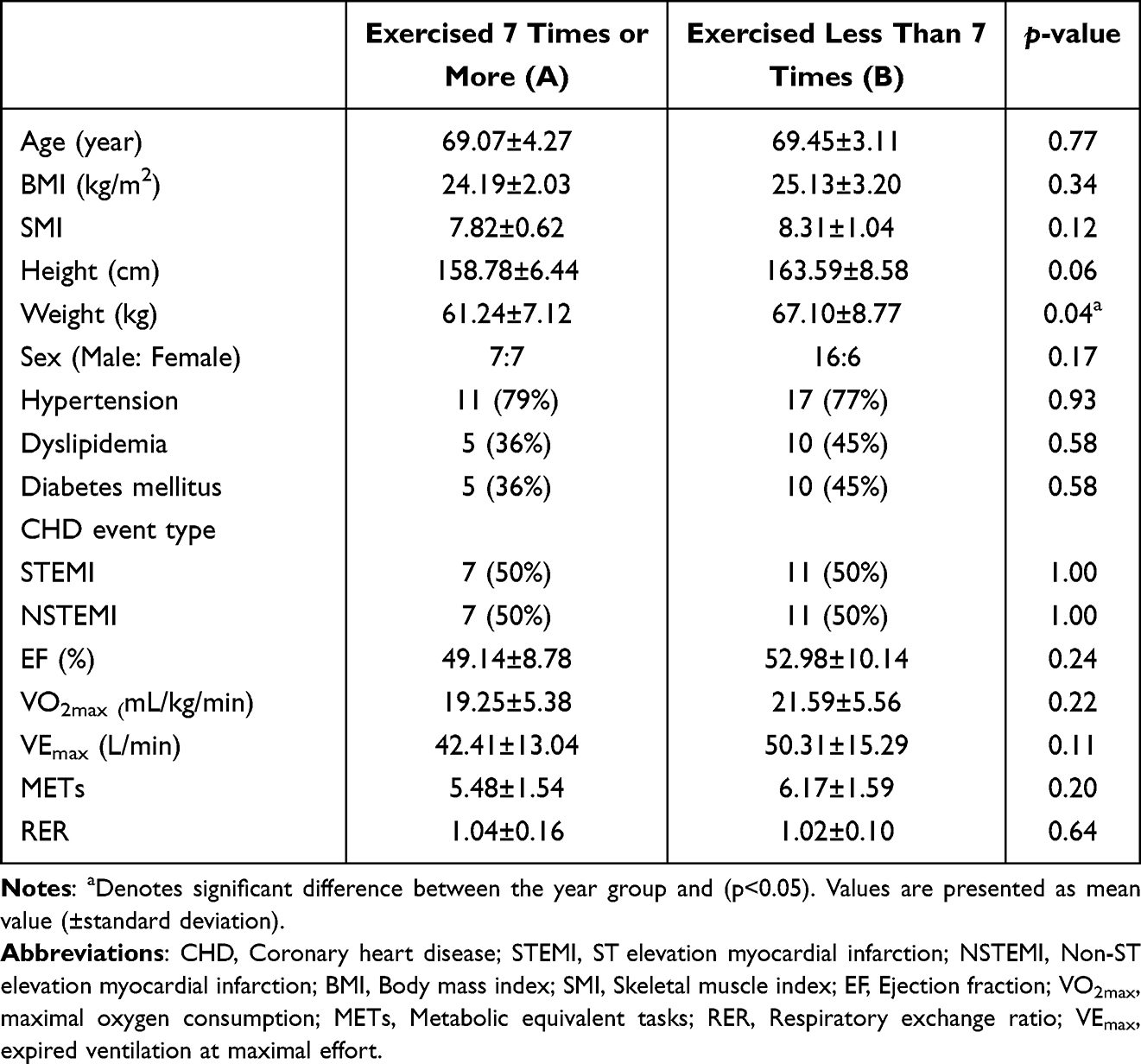 |
Table 1 Clinical Demographic Characteristics and Baseline CRF Characteristics of the Subjects |
Among the participants in the CR program, the number of participants who underwent one or more exercise sessions was correlated with the rate of change in SMI (R = 0.37, p < 0.05; Table 2). By contrast, the number of participants in the exercise sessions did not show a significant correlation with the rates of change in MET or VO2max.
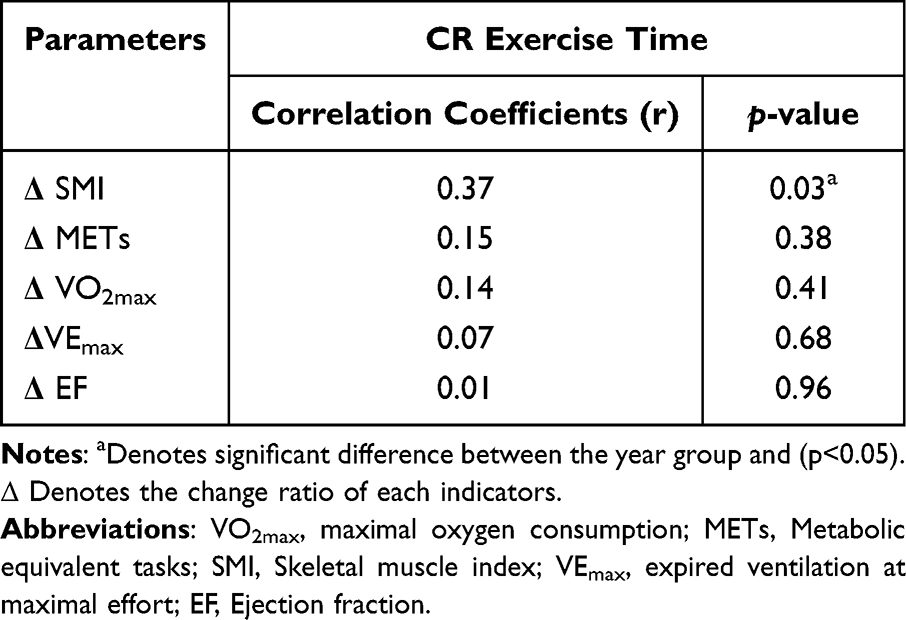 |
Table 2 Relationships Between the Exercise Time and the Change Ratio of Cardiorespiratory Parameters in Cardiac Rehabilitation Exercise Program Participants |
There was a significant increase in VO2max measured after three months in Group A (19.25 to 23.0 mL/kg/min; p < 0.01), but there was no significant change in Group B (21.6 to 21.7 mL/kg/min). MET increased significantly in Group A (5.48±1.54 to 6.58±1.44; p < 0.01), whereas Group B showed no significant change (6.17±1.59 to 6.18±1.72). Mean VEmax increased significantly in Group A after three months (42.41±13.04 to 50.41±14.57 L/min; p < 0.05). Contrarily, Group B showed no significant change in VEmax (50.31±15.29 to 49.57±16.38 L/min). Ejection fraction increased significantly in both Group A (49.14±8.78 to 56.31±9.28) and Group B (52.98±10.14 to 57.56±11.23) (Table 3).
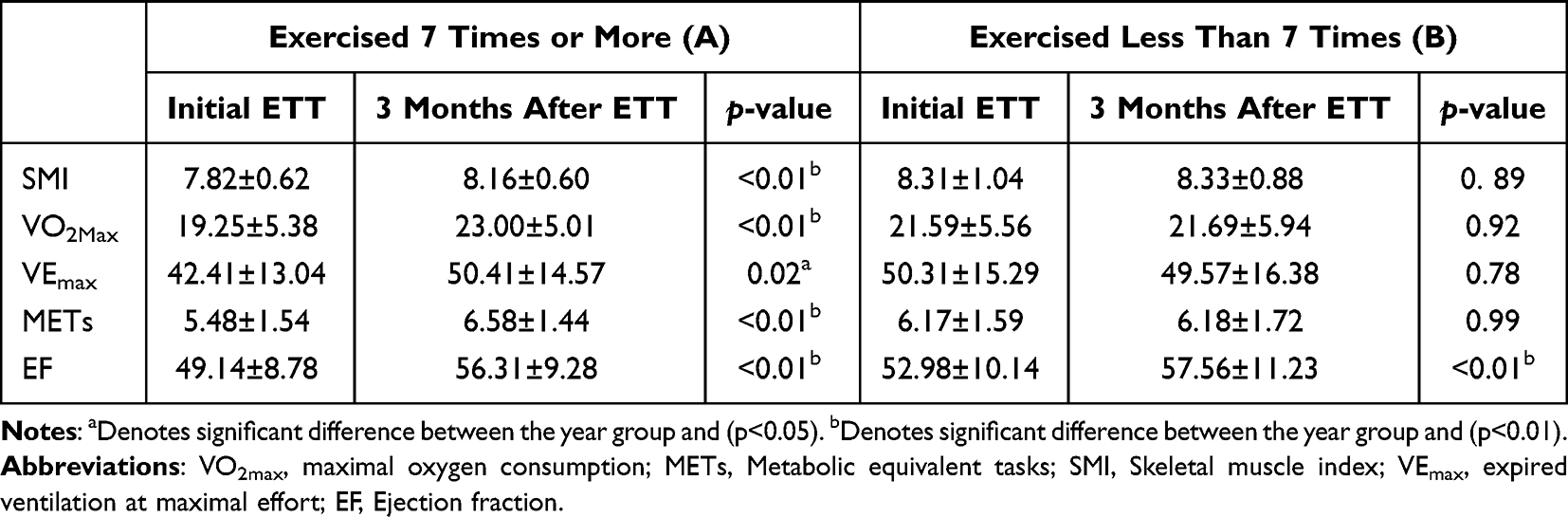 |
Table 3 Comparison of Exercise Capacity Between Onset and 3 month Follow Up Test in Cardiac Rehabilitation Exercise Program Participants Exercised 7 Times or More (Group A) and Less Than 7 Times (Group B) |
The rates of change in VO2max, MET, VEmax and SMI were significantly different between Groups A and B at three months (p < 0.05) (Table 4). Table 3 and Table 4 show significant increases in SMI, VO2max, and MET in Group A but not in Group B, and significantly higher rates of change in SMI, VO2max, MET, and VEmax in Group A than those in Group B.
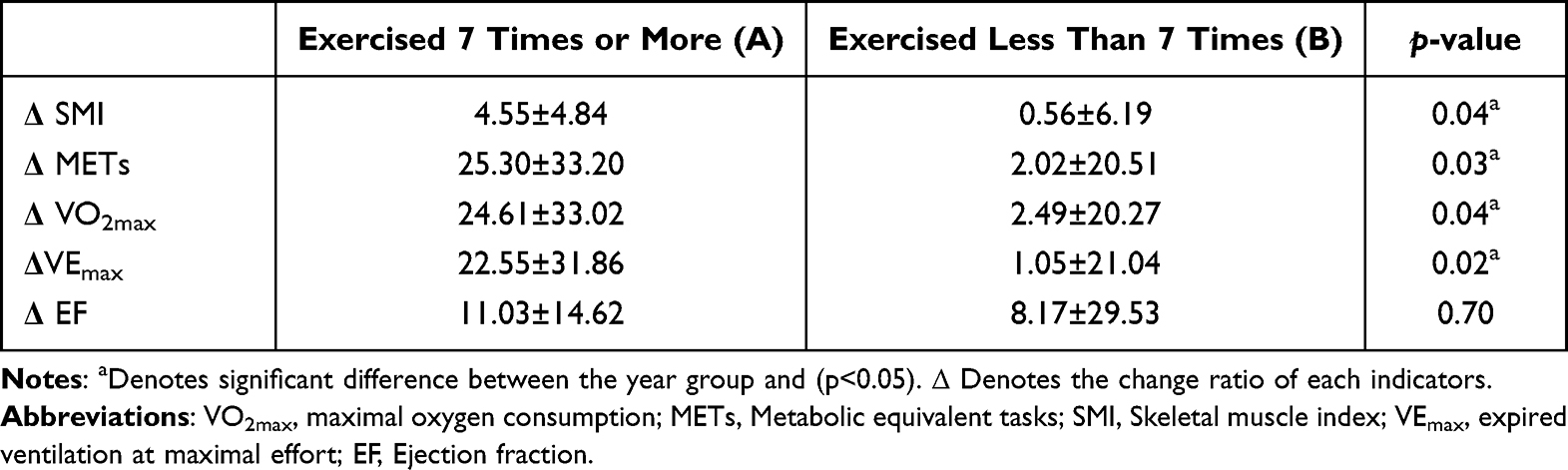 |
Table 4 Comparison of Change Ratios of SMI and Exercise Capacity Between Cardiac Rehabilitation Exercise Program Participants Exercised 7 Times or More (Group A) and Less Than 7 Times (Group B) |
Discussion
In this study, exercise ability and skeletal muscle mass were compared and analyzed by grouping patients aged ≥65 years based on their participation in at least seven sessions of a CR exercise program. The number of CR exercise program sessions attended showed a significant positive correlation with the rate of change in SMI. In addition, Group A showed significant improvements in SMI, VO2max, and MET after three months, and their rates of change in SMI, VO2max, and MET were significantly higher than those of Group B. However, there were no significant improvements in SMI, VO2max, or MET in the low-exercise group, and there was no significant correlation between the number of sessions attended and the rates of change in MET and VO2max. These results suggest that CR is essential for elderly patients with AMI and that the number of exercises also has a significant impact.
Society is aging worldwide, and exercise at an appropriate intensity is essential to restoring cardiac function in patients with increasing age.25 Accordingly, the CR exercise needs to be well monitored by experienced physicians, nurses or physiotherapists during the training period, and the intensity gradually increased according to established rules.26 Cardiopulmonary function and skeletal muscle mass decrease with age, with cardiopulmonary function decreasing in proportion to muscle mass.27 Muscle mass is associated with cardiac complications, mortality, and prognosis in older patients, and low muscle mass increases insulin resistance, causing disturbances in blood glucose control.7,8,17,18,28
Improving SMI is also necessary for medical prognosis and financial outcomes, because sarcopenia increases hospitalization costs.29 Even in frail elderly patients, exercise improves not only CRF, balance, and physical functions, but also psychological symptoms such as depression and anxiety, cognitive function decline, and the performance of daily activities, thereby enhancing the quality of life.30,31
Exercise is vital for improving prognosis. A 15% reduction in mortality rate was found for every 1 MET increase in CRF in healthy adults, and VO2max, which reflects CRF, is closely associated with survival.25 Among older patients with CHD, participation in CR exercise sessions reduced mortality dose-dependently, and even in the older patients aged ≥75 years with acute coronary syndrome showed improved physical performances after CR.21,30 Our result is similar to that of a previous study of patients with AMI aged ≥65 years, who showed dose-dependent improved physical performances.22
While most previous studies were limited to comprehensively discussing the effects of CR on CVD occurring at all ages, this study focused on patients with AMI aged ≥65 years and revealed a significant improvement in cardiopulmonary function and SMI depending on the number of CR treatments per patient and presented a specific number of exercise sessions that produced effective results. Despite the positive effects of CR, the rate of participation in CR exercise programs among patients aged ≥65 years is low, approximately 9.8–31.7% globally, and the participation rate is reported to decrease as age increases.32 However, even in such a limited situation, this study confirmed the minimum number of exercise to improve CRF and SMI in a short period of time in patients with AMI aged ≥65 years.
In this study, Phase 2 CR was performed in elderly patients aged ≥65 years, and CBCR and HBCR were combined. Whenever the patients visit the hospital for exercise session, nurse practitioners and medical staff educated the patients about the prescribed exercise and lifestyle modification and the importance of participating the exercise session. If they could not visit the hospital to perform center-based exercises performed the exercises at home. Considering that three months was a short period, in the group (<7) that focused on HBCR and performed CBCR, there was no significant change in aerobic capacity or SMI. However, in the group that focused more on CBCR (≥7), there was a significant improvement in aerobic capacity and SMI after three months. In the outpatient CR, comprehensive counseling and feedback for the patients’ exercise diaries were provided for every visit. People who participated more in CBCR showed better lifestyle improvements, suggesting that the effectiveness of CR was enhanced.
In this study, we found that performing more CBCRs, which include exercise session and comprehensive counseling about lifestyles, over shorter follow-up periods of less than three months further improved exercise capacity. In another study, approximately 29% of people who suffered their first heart attack developed anxiety or depression after three months, and approximately 20% were smokers.33 Thus, comprehensive CR, including lifestyle modifications such as psychosocial counseling and smoking cessation counseling, should be performed within three months, and this can be performed better in CBCR. Therefore, participation in CBCR in phase 2 is recommended.
In addition, studies on clinical outcomes depending on the approach of initial cardiological intervention are being discussed. One study has reported that the mortality rate increased depending on whether PCI was performed during daytime hours or nighttime hours.34 In our data, there was no difference in outcome according to the intervention time. Our hospital is a regional CVD center where specialists are on call 365 days at any time, hence there was no delayed PCI. Further studies about the mortality rate depending on initial intervention time are required in the future to improve the overall clinical outcome. For the femoral approach patients, we recommend to start ambulation as early as within 2~3 days, but it is thought that there would be some restrictions when performing some initial basic exercises such as lower limb stretching and range of motion exercises. In our data, radial approach was used in 13 patients and femoral approach was used in 23 patients. However, there was no difference in ejection fraction, CRFs and SMI between the two groups on initial and after 3 months. Although the impact of access site for intervention on rehabilitation has not been evaluated in this study, it seems that further research focusing on this topic is required.
However, there are some limitations of this study that this is a retrospective study and has data which were collected from a single hospital. In addition, the number of patients aged ≥65 years with AMI who participated in the CR program was small, and there were many patients whose CRF could not be measured because of the discontinuation of the ETT due to pain in the lower extremities. Furthermore, 47 of the 83 referred participants participated only in the educational program. Despite insurance coverage for CR since 2017, the CR participation rate of all patients in studies conducted in Korea was only 1.5%.35 This could be because adherence to CBCR is poor even after referral and participation in CR. At the center where this study performed, we run the cardiac rehabilitation critical pathway (CP) for patients with acute myocardial infarction. After the patients admitted and underwent cardiologic intervention, physician of rehabilitation visited each patient and educated the necessity, effects and content of cardiac rehabilitation. However, as in this study, the poor adherence has been observed worldwide. For instance, a study from United Kingdom reported the importance of the number of CBCR exercise sessions as low exercise session adherence would contribute to insufficient CRF improvement.36 In particular, adherence to cardiac rehabilitation is poor in elderly patients and those with poor accessibility to medical centers or who reside in rural regions.12,13
Another limitation of this study is that it was a short-term study with a follow-up of three months after the onset of the disease. According to a study, the therapeutic effect of phase 2 CR was lower than expected in elderly patients, even though the same number of exercise programs were performed during the same period of AMI cardiac rehabilitation. Thus, they recommended elderly patients to participate in phase 2 exercise programs for a longer period than the recommendation of WHO.37 Therefore, multicenter studies following the effect of CR in elderly patients for a longer period are necessary to expand the number of participants and provide evidence for the effectiveness of CR in the elderly population. In this study, many of the patients did not visit the hospital for follow-up for more than one year. This shows the one of the characteristics of elderly patients who reside in rural region with low compliance or adherence at CR. Therefore, further studies are required with long-term follow-up data.
Despite these limitations, this study is meaningful because there has been little information about minimal exercise volume to improve SMI and CRF. We report that CBCR should be performed at least seven times to be effective and could improve SMI in short term in elderly patients with myocardial infarction who reside in rural regions. It is notable that the participation in seven sessions presented in this study is the minimum number of CRs to be performed to achieve improvement in the short term.
Thus, further strategies should be developed to increase participation rates and adherence to CBCR by improving accessibility and awareness. For patients living in areas where accessibility or mobility is poor, tele-cardiac rehabilitation (Tele-CR), a new method of combining HBCR and CBCR, could be investigated, as it has been studied for people who had difficulty visiting hospitals.38,39 A study about HBCR with remote monitoring devices reported that this Tele-CR was as effective as the CBCR.40 However, as it is not easy to use advanced devices to monitor during exercise in the elderly and low socioeconomic level population, further researches are required to make them more user-friendly so that older patients can easily access them.
Conclusion
The CR program improved cardiopulmonary function and SMI. Increased SMI was significantly and positively correlated with the participated number of the CR exercise program, dose-dependently. Patients who participated in seven or more exercise sessions showed significant improvements in CRFs (MET and VO2max) and SMI after three months. Therefore, increasing the participation rate in CR exercise programs is recommended among patients aged ≥65 years with AMI. Further studies are needed to ensure the long-term effects of CR and to improve CR adherence in elderly patients.
Acknowledgments
This paper was supported by Wonkwang University in 2023.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sanchis-Gomar F, Perez-Quilis C, Leischik R, Lucia A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 2016;4(13):256. doi:10.21037/atm.2016.06.33
2. World Health Organization. The top 10 causes of death. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
3. Sidney S, Go AS, Jaffe MG, Solomon MD, Ambrosy AP, Rana JS. Association between aging of the US population and heart disease mortality from 2011 to 2017. JAMA Cardiol. 2019;4(12):1280–1286. doi:10.1001/jamacardio.2019.4187
4. Health Insurance Review & Assessment Service of Korea. September 29th, World Heart Day, Heart Diseases through Statistics; 2021. Available from: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020041000100&brdScnBltNo=4&brdBltNo=10428&pageIndex=1.
5. Kim RB, Kim HS, Kang DR, et al. The trend in incidence and case-fatality of hospitalized acute myocardial infarction patients in Korea, 2007 to 2016. J Korean Med Sci. 2019;34(50):e322. doi:10.3346/jkms.2019.34.e322
6. Dodson JA, Arnold SV, Reid KJ, et al. Physical function and Independence 1 year after myocardial infarction: patients’ Health status registry. Am Heart J. 2012;163(5):790–796. doi:10.1016/j.ahj.2012.02.024
7. Bhatia LC, Naik RH. Clinical profile of acute myocardial infarction in elderly patients. J Cardiovasc Dis Res. 2013;4(2):107–111. doi:10.1016/j.jcdr.2012.07.003
8. Shanmugam VB, Harper R, Meredith I, Malaiapanm Y, Psaltis PJ. An overview of PCI in the very elderly. J Geriatr Cardiol. 2015;12(2):174–184. doi:10.11909/j.issn.1671-5411.2015.02.012
9. O’Neill D, Forman DE. Never too old for cardiac rehabilitation. Clin Geriatr Med. 2019;35(4):407–421. doi:10.1016/j.cger.2019.07.001
10. Suaya JA, Stason WB, Ades PA, Normand S-LT, Shepard DS. Cardiac rehabilitation and survival in older coronary patients. J Am Coll Cardiol. 2009;54(1):25–33. doi:10.1016/j.jacc.2009.01.078
11. Kabboul NN, Tomlinson G, Francis T, et al. Comparative effectiveness of the core components of cardiac rehabilitation on mortality and morbidity: a systematic review and network meta-analysis. J Clin Med. 2018;7(12):514. doi:10.3390/jcm7120514
12. Daly J, Sindone AP, Thompson DR, Hancock K, Chang E, Davidson P. Barriers to participation in and adherence to cardiac rehabilitation programs: a critical literature review. Prog Cardiovasc Nurs. 2002;17(1):8–17. doi:10.1111/j.0889-7204.2002.00614.x
13. Ruano-Ravina A, Pena-Gil C, Abu-Assi E, et al. Participation and adherence to cardiac rehabilitation programs. A systematic review. Int J Cardiol. 2016;223:436–443. doi:10.1016/j.ijcard.2016.08.120
14. Malafarina V, Uriz-Otano F, Iniesta R, Gil-Guerrero L. Sarcopenia in the elderly: diagnosis, pathophysiology and treatment. Maturitas. 2012;71(2):109–114. doi:10.1016/j.maturitas.2011.11.012
15. Wilkinson DJ, Piasecki M, Atherton PJ. The age-related loss of skeletal muscle mass and function: measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res Rev. 2018;47:123–132. doi:10.1016/j.arr.2018.07.005
16. Boo SH, Joo MC, Lee JM, Kim SC, Yu YM, Kim MS. Association between skeletal muscle mass and cardiorespiratory fitness in community-dwelling elderly men. Aging Clin Exp Res. 2019;31(1):49–57. doi:10.1007/s40520-018-0987-9
17. Nichols S, O’Doherty AF, Taylor C, Clark AL, Carroll S, Ingle L. Low skeletal muscle mass is associated with low aerobic capacity and increased mortality risk in patients with coronary heart disease – a CARE CR study. Clin Physiol Funct Imaging. 2019;39(1):93–102.
18. Sato R, Akiyama E, Konishi M, et al. Decreased appendicular skeletal muscle mass is associated with poor outcomes after ST segment elevation myocardial infarction. J Atheroscler Thromb. 2020;27(12):1278–1287. doi:10.5551/jat.52282
19. Harada H, Kai H, Niiyama H, et al. Effectiveness of cardiac rehabilitation for prevention and treatment of sarcopenia in patients with cardiovascular disease – a retrospective cross-sectional analysis. J Nutr Health Aging. 2017;21(4):449–456. doi:10.1007/s12603-016-0743-9
20. He W, Peng N, Chen Q, Xiang T, Wang P, Pang J. The relationships among the skeletal muscle mass index, cardiorespiratory fitness and the prevalence of coronary artery disease in the elderly population. Arch Gerontol Geriatr. 2020;90:104107.
21. Hammill BG, Curtis LH, Schulman KA, Whellan DJ. Relationship between cardiac rehabilitation and long-term risks of mortality and myocardial infarction among Elderly Medicare Beneficiaries Bradley G. Circulation. 2010;121(1):63–70. doi:10.1161/CIRCULATIONAHA.109.876383
22. Doll JA, Hellkamp A, Thomas L, et al. Effectiveness of cardiac rehabilitation among older patients after acute myocardial infarction. J Am Heart J. 2015;170(5):855–864. doi:10.1016/j.ahj.2015.08.001
23. Williams MA, Roitman JL. Guidelines for Cardiac Rehabilitation Programs.
24. Kim C, Choi HE, Lee KH, Kim YJ, Lee SJ. Influence of low peak respiratory exchange ratio on cardiac rehabilitation in patients with coronary artery disease. Ann Rehabil Med. 2016;40(6):1114–1123. doi:10.5535/arm.2016.40.6.1114
25. Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024–2035. doi:10.1001/jama.2009.681
26. American College of Sports Medicine. ACSM’s Exercise Testing and Prescription. Philadelphia, PA, USA: Lippincott Williams & Wilkins; 2017.
27. Fleg JL, Lakatta EG. Role of muscle loss in the age-associated reduction in VO2max. J Appl Physiol. 1988;65(3):1147–1151. doi:10.1152/jappl.1988.65.3.1147
28. Fukuoka Y, Narita T, Fujita H, et al. Importance of physical evaluation using skeletal muscle mass index and body fat percentage to prevent sarcopenia in elderly Japanese diabetes patients. J Diabetes Investig. 2019;10(2):322–330. doi:10.1111/jdi.12908
29. Sousa AS, Guerra RS, Fonseca I, Pichel F, Ferreira S, Amaral TF. Financial impact of sarcopenia on hospitalization costs. Eur J Clin Nutr. 2016;70(9):1046–1051. doi:10.1038/ejcn.2016.73
30. Silva RB, Aldoradin-Cabeza H, Eslick GD, Phu S, Duque G. The effect of physical exercise on frail older persons: a systematic review. J Frailty Aging. 2017;6(2):91–96. doi:10.14283/jfa.2017.7
31. Baldassero S, Pratesi A, Francini S, et al. Cardiac rehabilitation in very old adults: effect of baseline functional capacity on treatment effectiveness. J Am Geriatr Soc. 2016;64(8):1640–1645. doi:10.1111/jgs.14239
32. Ritchey MD, Maresh S, McNeely J, et al. Tracking cardiac rehabilitation participation and completion among medicare beneficiaries to inform the efforts of a national initiative. Circ Cardiovasc Qual Outcomes. 2020;13(1):e005902. doi:10.1161/CIRCOUTCOMES.119.005902
33. Larsen KK, Vestergaard M, Søndergaard J, Christensen B. Rehabilitation status three months after first-time myocardial infarction. Scand J Prim Health Care. 2011;29(4):210–215. doi:10.3109/02813432.2011.629147
34. Tokarek T, Dziewierz A, Plens K, et al. Percutaneous coronary intervention during on- and off-hours in patients with ST-segment elevation myocardial infarction. Hellenic J Cardiol. 2021;62(3):212–218.
35. Kim SH, Ro JS, Kim Y, Leigh JH, Kim WS. Underutilization of hospital-based cardiac rehabilitation after acute myocardial infarction in Korea. J Korean Med Sci. 2020;35(30):e262. doi:10.3346/jkms.2020.35.e262
36. Gavin RHS, Cardoso F, Almodhy M, Pepera G. Cardiorespiratory fitness changes in patient receiving comprehensive outpatient cardiac rehabilitation in the United Kingdom: a multicentre study. Heart. 2013;99(11):785–790. doi:10.1136/heartjnl-2012-303055
37. Kim KH, Jang YC, Song MK, Park HK, Choi IS, Han JY. Changes in aerobic capacity over time in elderly patients with acute myocardial infarction during cardiac rehabilitation. Ann Rehabil Med. 2020;44(1):77–84. doi:10.5535/arm.2020.44.1.77
38. Thamman R, Janardhanan R. Cardiac rehabilitation using telemedicine: the need for tele cardiac rehabilitation. Rev Cardiovasc Med. 2020;21(4):497–500. doi:10.31083/j.rcm.2020.04.201
39. Sari DM, Wijaya LCG. Cardiac rehabilitation via telerehabilitation in COVID-19 pandemic situation. Egypt Heart J. 2021;73(1):31. doi:10.1186/s43044-021-00156-7
40. Antoniou V, Davos CH, Kapreli E, Batalik L, Panagiotakos DB, Pepera G. Effectiveness of home-based cardiac rehabilitation, using wearable sensors, as a multicomponent, cutting-edge intervention: a systematic review and meta-analysis. J Clin Med. 2022;11(13):3772. doi:10.3390/jcm11133772
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.