Back to Journals » Cancer Management and Research » Volume 18

Relationship Between Netrin-1 Staining and Neoadjuvant Treatment Response in HER2-Positive Locally Advanced Breast Cancer
Authors Gülbağcı B ![]() , Çakırsoy Çakar G, Küçükarda A, Çavdar E, Hacıbekiroğlu I
, Çakırsoy Çakar G, Küçükarda A, Çavdar E, Hacıbekiroğlu I
Received 8 October 2025
Accepted for publication 27 January 2026
Published 11 February 2026 Volume 2026:18 551516
DOI https://doi.org/10.2147/CMAR.S551516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Harikrishna Nakshatri
Burcu Gülbağcı,1 Gözde Çakırsoy Çakar,2 Ahmet Küçükarda,1 Eyyüp Çavdar,1 Ilhan Hacıbekiroğlu3
1Tekirdağ Dr Ismail Fehmi Cumalıoğlu State Hospital, Tekirdağ, Department of Medical Oncology, Tekirdağ, Turkey; 2Sakarya University Training and Research Hospital, Department of Medical Pathology, Sakarya, Turkey; 3Sakarya University Training and Research Hospital, Department of Medical Oncology, Sakarya, Turkey
Correspondence: Burcu Gülbağcı, Tekirdağ Dr Ismail Fehmi Cumalıoğlu State Hospital, Department of Medical Oncology, 59100- Süleymanpaşa-Tekirdağ, Tekirdağ, Turkey, Tel +90 545 878 33 66, Email [email protected]
Background: Netrin-1 is a laminin-related glycoprotein involved in embryonic development and cancer progression. In breast cancer, increased Netrin-1 expression has been associated with lymph node positivity, metastatic disease, and treatment resistance. Given its potential role in tumor aggressiveness and response to therapy, we aimed to investigate the relationship between Netrin-1 expression and neoadjuvant treatment response in HER2-positive breast cancer.
Methods: A total of 90 patients were included in the study. Netrin-1 expression was evaluated immunohistochemically in formalin-fixed, paraffin-embedded tumor tissues retrieved from pathology archives. Netrin-1 expression was assessed using two scoring parameters: staining proportion and staining intensity. Patients were divided into two groups according to the netrin-1 staining intensity and strength. Clinicopathological features were compared statistically between groups.
Results: Pathological responses after neoadjuvant treatment were compared according to Netrin-1 staining proportion and intensity, and no statistically significant differences were observed. Miller–Payne Grades 4– 5 were more frequent in the high staining proportion and intensity groups; however, these differences were not statistically significant (p = 0.69 and p = 0.38, respectively). Univariate logistic regression identified Ki-67, hormone receptor status, and tumor dimension as factors associated with pathological complete response. These variables remained independently associated with pCR in multivariate binary logistic regression analysis.
Conclusion: Netrin-1 expression was not associated with neoadjuvant treatment response in HER2-positive breast cancer. Nevertheless, considering its biological role and therapeutic relevance in multiple malignancies, further studies are warranted to clarify the predictive and therapeutic potential of Netrin-1.
Keywords: breast cancer, HER-2 positive, netrin-1
Corrigendum for this paper has been published.
Introduction
Netrin-1 is a laminin-related glycoprotein that plays a crucial role in embryonic development and is aberrantly expressed in a wide range of malignancies. Within cancer cells and the tumor microenvironment, Netrin-1 has been shown to regulate key processes such as epithelial–mesenchymal transition (EMT) and angiogenesis. Initially described in the early 1990s as a secreted chemotropic guidance molecule, increased Netrin-1 expression has since been reported in several cancer types; including breast, lung, colorectal, melanoma, lymphoma, and glioblastoma.1,2
The two principal receptors of Netrin-1, Deleted in Colorectal Carcinoma (DCC) and UNC5 homologs (UNC5H), induce apoptosis in the absence of ligand. Accordingly, loss of receptor expression or upregulation of Netrin-1 has been associated with tumor progression and aggressiveness. In breast cancer, higher Netrin-1 expression has been observed in lymph node–positive compared with lymph node–negative disease, as well as in metastatic compared with non-metastatic tumors.2,3
Human epidermal growth factor receptor 2 (HER2) positivity accounts for approximately 20% of all breast cancers and is associated with aggressive tumor biology, early recurrence, and inferior survival outcomes.4 Response to neoadjuvant therapy varies according to intrinsic molecular subtypes within HER2-positive breast cancer, with the highest pathological response rates observed in HER2-enriched and HER2 basal-like tumors. Importantly, achieving a pathological complete response (pCR) in these subtypes has been linked to improved event-free survival.5
The EMT-like phenotype is more frequently encountered in HER2-positive breast cancer and has been implicated in resistance to anti-HER2 therapies. In this context, overexpression of Netrin-1 has been shown to facilitate EMT, while preclinical studies have demonstrated that both de novo and acquired resistance to trastuzumab occur more commonly in tumors exhibiting EMT-like features.6,7
With the success of anti-HER2 therapies in early-stage disease, neoadjuvant treatment has become the standard of care. pCR achieved after neoadjuvant therapy is strongly associated with favorable survival outcomes, with pCR rates reaching 57–66% following dual HER2 blockade with trastuzumab and pertuzumab.8,9 Ongoing research has therefore focused on identifying radiological biomarkers, such as functional tumor volume (FTV), and pathological biomarkers, including tumor-infiltrating lymphocytes (TILs) and hormone receptor status, to better characterize tumor biology and optimize treatment strategies.5,10 In line with this rationale, we aimed to investigate the relationship between Netrin-1 expression and neoadjuvant treatment response in HER2-positive breast cancer.
Material and Methods
Study Population
A total of 106 patients diagnosed with locally advanced/oligometastatic HER2-positive breast cancer and treated with neoadjuvant chemotherapy combined with anti-HER2 monoclonal antibody between March 1, 2015, and September 30, 2022, Sakarya University were included in the study. Archived tumor tissues from breast biopsies performed at the time of diagnosis were used. Sixteen patients with formalin-fixed and paraffin-embedded (FFPE) tissues that did not contain sufficient tumor cells for Netrin-1 staining were excluded. Data from a total of 90 patients were analyzed.
Patients were over 18 years of age, hormone receptor-positive/negative and HER2-positive, radiologically early stage or oligometastatic (one metastatic site and <3 metastases, no solid metastases), and receiving neoadjuvant treatment. HER2 positivity was defined as an immunohistochemical (IHC) score of 3 or 2 and being positive by fluorescence in situ hybridization (FISH). Hormone receptor positivity was defined estrogen and/or progesterone receptor ≥ 1%. There were 5 oligometastatic patients (3 patients had 1 bone metastasis, 1 patient had mediastinal lymph node metastasis, and 1 patient had 2 bone metastases). Oligometastatic patients were operated on according to their radiological response to neoadjuvant treatment. Pathological response in the primary tumor was evaluated using the Miller–Payne grading system: grade 5 in two patients, grade 4 in two patients, and grade 3 in one patient.
This study was planned as an exploratory study to determine the predictive value of the Netrin-1 molecule on neoadjuvant therapy response. Since there were no similar studies in the literature, IHC staining cut-off values were used. Netrin-1 was evaluated by IHC in FFPE tissues from the pathology archives of the patients. Netrin-1 positivity was determined by two scoring methods: cytoplasmic staining proportion and intensity. The staining proportion was scored as 0 (<10%), 1 (10–25%), 2 (25–50%), 3 (50–75%), and 4 (75–100%), and the staining intensity was scored as 0 (absent), 1 (weak), 2 (moderate), and 3 (strong). For analysis, the ≥75% cut-off for staining proportion and the 0–1 vs 2–3 grouping for staining intensity were selected a priori to facilitate comparative analysis in a limited sample size and should be interpreted as exploratory rather than definitive thresholds. BIOSS BS-1858R Netrin-1 polyclonal concentrated 0.1 mL (1:400) and DAKO GV82311-2 Env FLEX Mini KIT were used. Formalin-fixed paraffin-embedded sections were processed using standard immunohistochemical procedures according to the manufacturer’s protocol, with appropriate positive and negative controls included in each run. All evaluations were performed under standardized conditions, and the pathologist was blinded to clinical outcomes. Netrin-1 immunohistochemical staining results were evaluated by a single pathologist.
The Miller Payne grading system was used to evaluate neoadjuvant treatment response in the postoperative pathology report. Grade 1 defines no change in individual malignant cells; Grade 5 defines no malignant cells identifiable at the tumor site. Additionally, no malignant cells at the tumor site was considered pathological complete response (pCR).
Patient data (demographics, clinicopathological, outcome data, pathological response evaluation, and laboratory parameters) were collected from medical oncology outpatient clinic records, medical records and computer records.
Statistical Analysis
All analyses were performed using SPSS Version 23 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was applied to test the normal distribution of all data. Data are presented as mean ± standard deviation or median (1st quartile −3rd quartile) for continuous variables and as frequency (percentage) for categorical variables based on normality of distribution. An analysis of continuous variables between groups was performed using the independent samples t-test or Mann–Whitney U-test, depending on the normality of distribution. To compare categorical variables, the chi-square test was used, and when the chi-square test was not appropriate, Fisher’s exact test was applied. Univariate and multivariate logistic regression analysis was used to determine the factors predicting pCR. The mean was employed to determine cut-off values for age. Odds Ratio (OR) was reported with corresponding 95% confidence intervals (95% CI) and p<0.05 was considered statistically significant.
Ethical Approval
This study was conducted retrospectively. The study protocol was approved by the Ethics Committee of Sakarya University Faculty of Medicine (02.02.2022–71,522,473-050.01.04–102,086-07). Informed consent was waived due to the retrospective design of the study and the use of anonymized patient data. All patient data were fully anonymized prior to analysis, and patient confidentiality was strictly maintained in accordance with the Declaration of Helsinki.
Results
A total of 90 patients were included in the study. The median age of the patients was 48.5 (40–57.25) years. All patients received trastuzumab in neoadjuvant treatment, 46 (51.1%) patients received trastuzumab+ pertuzumab with chemotherapy. After neoadjuvant therapy, pCR was observed in 33 (36.7%) patients. The clinical and pathological characteristics of the patients are summarized in Table 1.
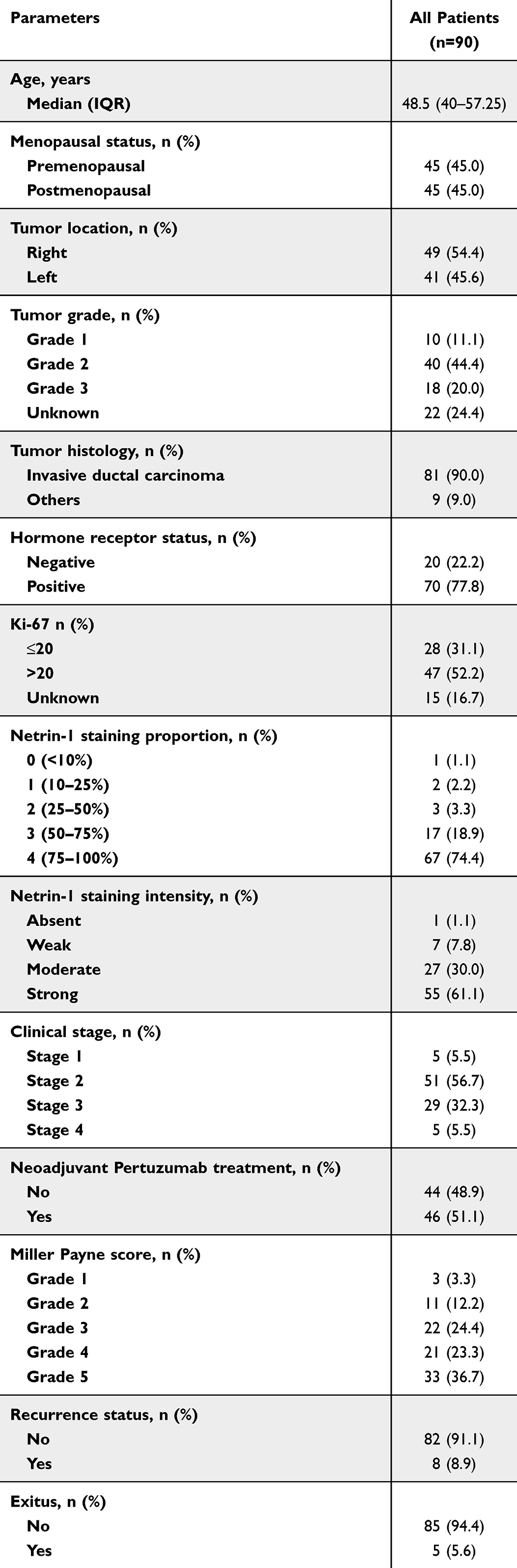 |
Table 1 Demographic and Clinical Characteristics of the Study Population |
Patients were divided into two groups according to netrin-1 staining proportion. Twenty-three patients had low staining proportion (<75%), and 67 patients had high staining proportion (≥75%). Patient characteristics were similar between the two groups. Patients were also divided into two groups according to netrin-1 staining intensity. Thirty-five patients had absent-weak staining intensity (0–1), and 55 patients had moderate-high (2–3) staining intensity. Hormone receptor–positive tumors were significantly more frequent in the moderate-to-strong Netrin-1 staining intensity group compared with the absent–weak group (p = 0.028) (Figure 1).
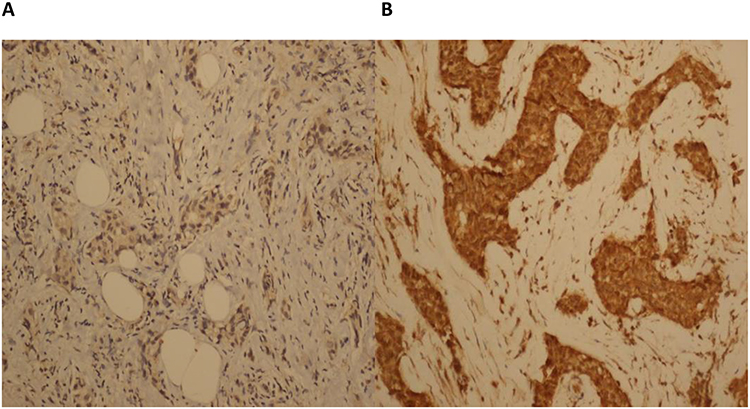 |
Figure 1 Netrin-1 staining intensity weak (A) and strong (B) in breast cancer cells. |
Among the five oligometastatic patients, Netrin-1 staining proportion was low (<75%) in two patients and high (≥75%) in three patients. Regarding staining intensity, three patients showed absent–weak, while two patients exhibited moderate–strong staining.
Pathological responses after neoadjuvant treatment were compared within the groups for netrin-1 staining proportion and intensity, and no statistically significant difference was found. Miller Payne Grades 4–5 were more common in the higher proportion and intensity groups, but this difference was not statistically significant (p= 0.69, p=0.38, respectively). (Table 2 and Table 3).
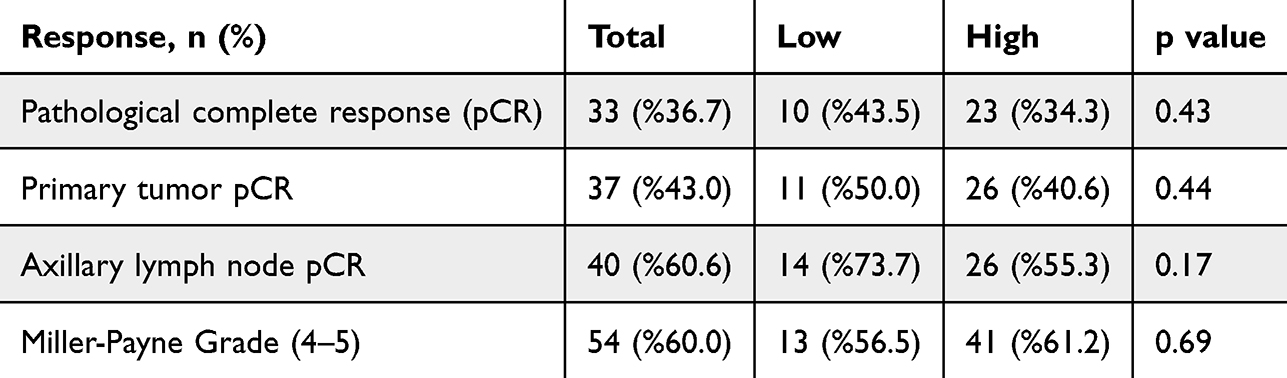 |
Table 2 Response Evaluation Between Netrin-1 Staining Proportion Groups and the Population |
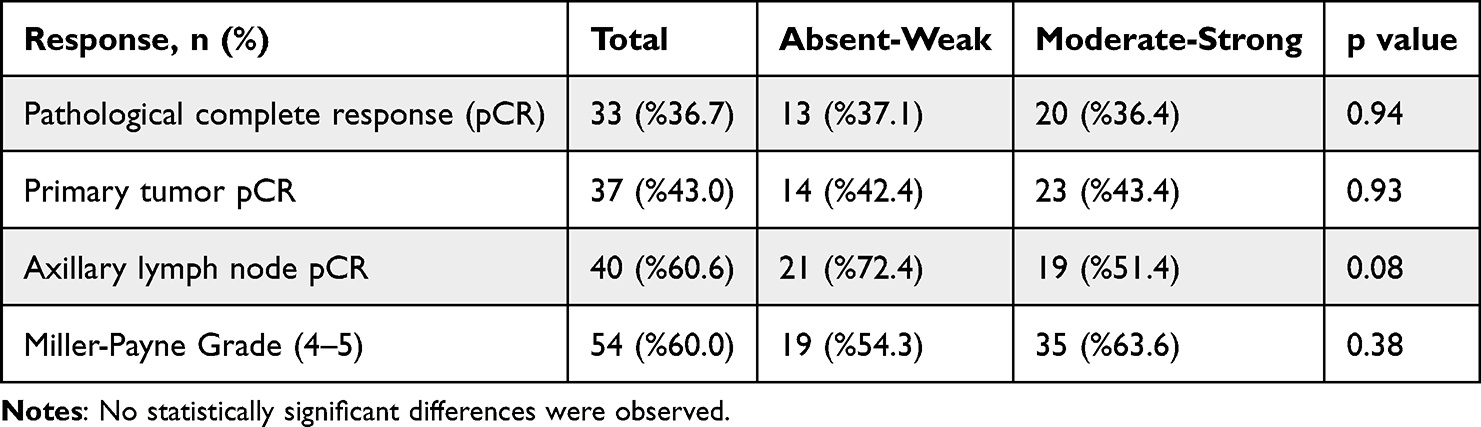 |
Table 3 Response Evaluation Between Netrin-1 Staining Intensity Groups and the Population |
Factors predicting pCR were evaluated univariate logistic regression analysis (Table 4). In the established model, Ki-67 (OR: 4.41, 95% CI 1.43–13,56, p:0.010), hormone receptor status (OR: 0.29, 95% CI 0.10–0.80, p:0.017) and tumor dimension (OR: 0.91, 95% CI 0.32–2.58, p:0.079) were found to be predictive factors. Variables with p <0.10 in the univariate analysis were subsequently included in the multivariate binary logistic regression model. In multivariate binary logistic regression analysis, Ki-67, hormone receptor status, and tumor dimension remained independent predictors of pathological complete response. Higher Ki-67 expression was associated with an increased likelihood of pCR, whereas hormone receptor positivity and smaller tumor size were also independently associated with pCR (Table 5).
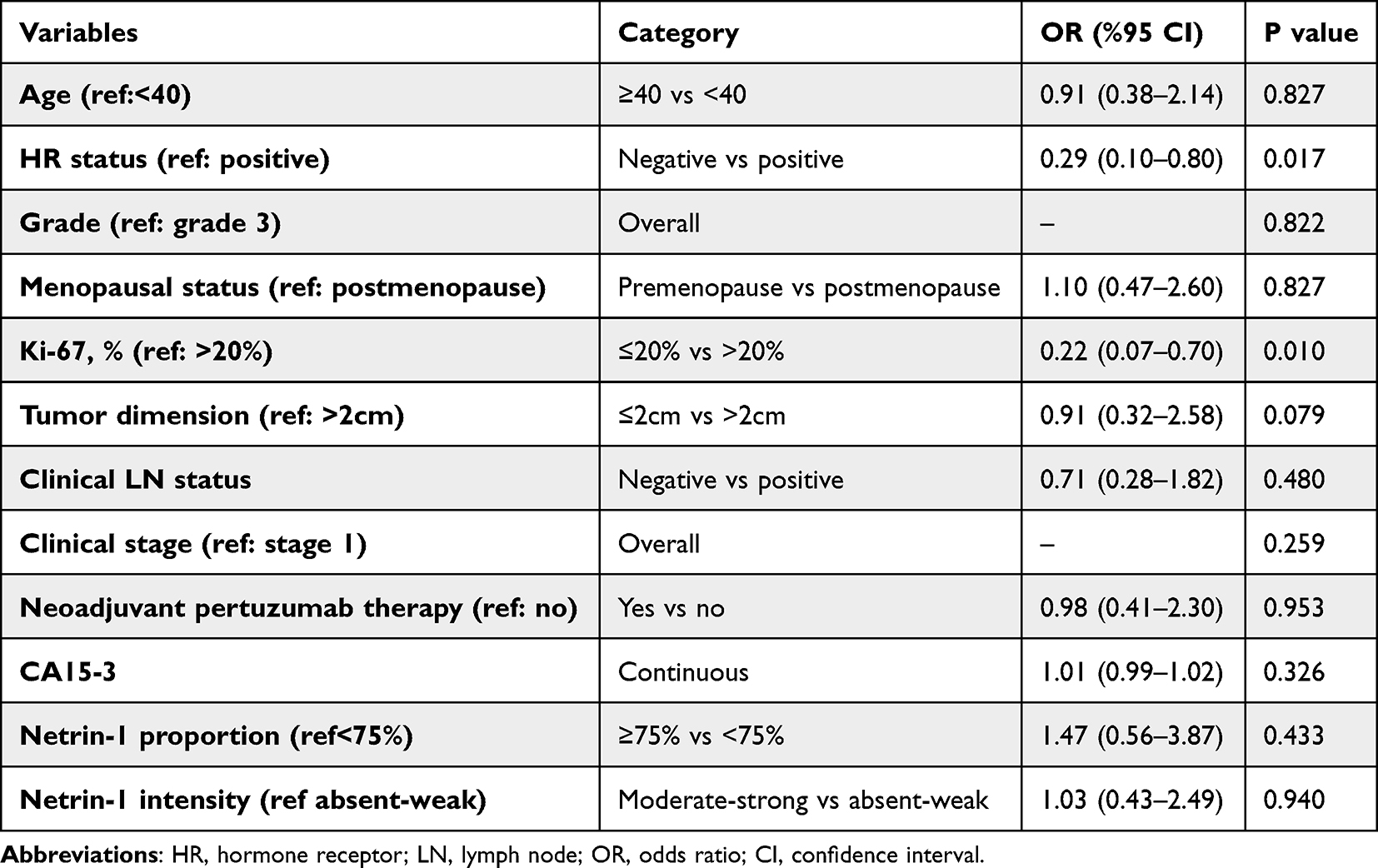 |
Table 4 Factors That Predict Pathological Complete Response |
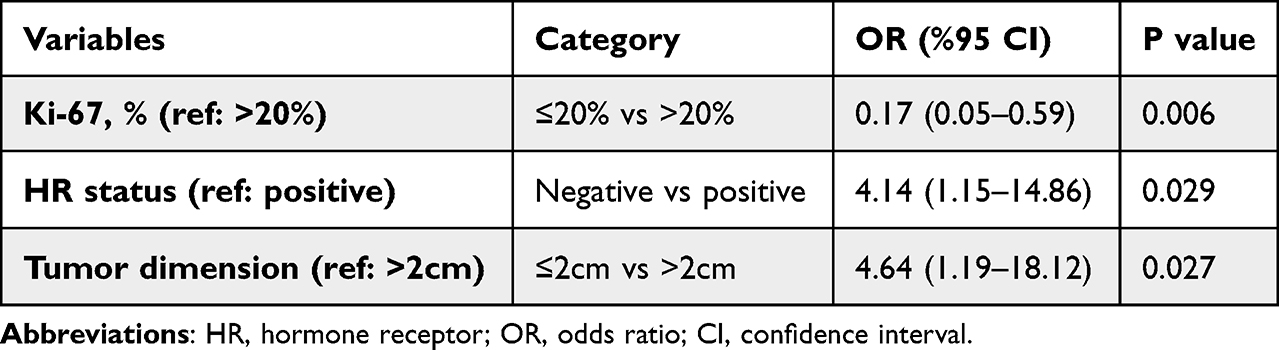 |
Table 5 Multivariate Analysis of Predictors of Pathological Complete Response |
Discussion
It is known that the expression level of netrin-1 varies in many cancer types. Our study is the first in the literature to evaluate the relationship between netrin-1 expression and treatment. In our study, we examined the relationship between netrin-1 expression level and pathological response after neoadjuvant treatment in HER2-positive locally advanced/oligometastatic breast cancer patients. Consistent with the literature, the pathological complete response after neoadjuvant treatment was correlated with Ki-67 (p=0.010), however no correlation was found with the staining proportion and netrin-1 intensity (p=0.940; p=0.433, respectively).
Blocking netrin-1 as a therapeutic target with an anti-Netrin-1 antibody (NP137), alone or in combination with different agents, is under investigation for various tumors. Reducing the risk of metastasis and progression through EMT inhibition by NP137 may be a promising therapeutic target for HER2-positive breast cancer.11–13
Netrin-1 expression was evaluated immunohistochemically and interpreted as two parameters: staining proportion and intensity. We did not evaluate the netrin-1 receptor expression in our study. The relative increase in Netrin-1 levels due to decreased receptor expression may affect tumor aggressiveness and treatment response.
Fitamant et al evaluated the netrin-1 level by quantitative polymerase chain reaction (Q-PCR) and found that it was expressed more in node-positive patients than in node-negative patients.3 The detection of netrin-1 by PCR or the measurement of receptor expression may be more helpful as regards treatment response. Chen et al evaluated Netrin-1 expression IHC in archived breast cancer tissues and classified cytoplasmic staining intensity using a 0–3+ scoring system.14 In their cohort of 106 patients, Netrin-1 expression was not associated with estrogen receptor positivity, lymph node involvement, or tumor size. In contrast, our study focused on a biologically and clinically distinct population of patients with HER2-positive breast cancer treated with neoadjuvant therapy and demonstrated a significant association between higher Netrin-1 staining intensity and hormone receptor positivity. These discrepant findings may be explained by differences in patient selection, treatment context, and study objectives. Importantly, as no standardized or outcome-based cut-off values for Netrin-1 expression have been established in the literature, the cut-off values applied in the present study were selected to enable meaningful group comparisons within a limited sample size and should be regarded as exploratory rather than definitive clinical thresholds. Accordingly, our results should be interpreted as hypothesis-generating and warrant validation in larger, prospective cohorts.
In our study, hormone receptor–positive tumors were significantly more frequent in the moderate-to-strong Netrin-1 staining intensity group compared with the absent–weak group (p = 0.028). Previous studies have demonstrated that high expression of Netrin-1 receptors, particularly Down syndrome cell adhesion molecule (DSCAM) and UNC5B, is associated with increased sensitivity to fulvestrant, a selective estrogen receptor degrader (SERD).15,16 Taken together, these findings suggest that Netrin-1 and its receptors may play a role in the mechanisms underlying endocrine sensitivity and resistance in hormone receptor–positive tumors. Although direct causal relationships cannot be established in the present study, the association between Netrin-1 signaling and hormone receptor status raises the possibility that this pathway could be involved in modulating endocrine response and resistance.
Hormone receptor and HER2 discordance may be seen in primary tumors and synchronous lymph node metastases, and this affects survival.17 The existence of a similar discordance of netrin-1 is unknown. In our study, netrin-1 levels in breast biopsy tissues collected for diagnosis were examined; lymph node netrin-1 status was not evaluated. In our study, no correlation was observed between primary tumor and axillary complete response rates, and Netrin-1 levels (p=0.44, p=0.17 for staining proportion; p=0.93, p=0.08 for staining intensity, respectively).
The main limitations were the use of archival tissues due to the retrospective design, the detection of netrin-1 levels by IHC, and the unknown expression level in the concomitant lymph node. Immunohistochemical evaluation was performed by a single experienced pathologist to ensure scoring consistency; however, the absence of interobserver agreement analysis represents a limitation of the study. Due to the limited sample size, survival endpoints such as progression-free survival associated with pathological complete response could not be reliably evaluated. In addition, survival analyses were not performed because of the retrospective design and the limited follow-up duration of the study cohort.
Conclusion
In our study, we investigated netrin-1 as a marker predicting response to standard neoadjuvant treatment in HER2-positive breast cancer and found no correlation. However, netrin-1 is an essential marker in many cancers as a therapeutic target. As the importance of netrin-1 as a therapeutic target increases, it will be practical to determine netrin-1 expression through easily accessible methods such as IHC.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is none received.
Disclosure
None of the authors received any support that could be considered a potential conflict of interest regarding the paper.
References
1. Serafini T, Kennedy TE, Galko MJ, et al. The netrins define a family of axon outgrowth‐promoting proteins homologous to C. Elegans UNC-6 Cell. 1994;78:
2. Kefeli U, Kefeli AU, Cabuk D, et al. Netrin-1 in cancer: potential biomarker and therapeutic target? Tumour Biol. 2017;39(4):1010428317698388.
3. Fitamant J, Guenebeaud C, Coissieux MM, et al. Netrin-1 expression confers a selective advantage for tumor cell survival in metastatic breast cancer. Proc Natl Acad Sci. 2008;105(12):4850–8. doi:10.1073/pnas.0709810105
4. Wolff AC, Hammond MEH, Hicks DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American pathologists clinical practice guideline update. J Clin Oncol. 2013;31(31):3997–4013. doi:10.1200/JCO.2013.50.9984
5. Fernandez-Martinez A, Rediti M, Tang G, et al. Tumor intrinsic subtypes and gene expression signatures in early-stage ERBB2/HER2-Positive breast cancer: a pooled analysis of CALGB 40601, NeoALTTO, and NSABP B-41 trials. JAMA Oncol. 2024;10(5):603–611. doi:10.1001/jamaoncol.2023.7304
6. Lengrand J, Pastushenko L, Vanuytven S, et al. Pharmacological targeting netrin-1 inhibits EMT in cancer. Nature. 2023;620(7973):402–408. doi:10.1038/s41586-023-06372-2
7. Nami B, Ghanaeian A, Black C, Wang Z. Epigenetic silencing of HER2 expression during epithelial-mesenchymal transition leads to trastuzumab resistance in breast cancer. Life. 2021;11(9):868. doi:10.3390/life11090868
8. Gianni L, Pienkowski T, Im YH, et al. 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): a multicentre, open-label, Phase 2 randomised trial. Lancet Oncol. 2016;17(6):791–800. doi:10.1016/S1470-2045(16)00163-7
9. Schneeweiss A, Chia S, Hickish T, et al. Long-term efficacy analysis of the randomised, Phase II TRYPHAENA cardiac safety study: evaluating pertuzumab and trastuzumab plus standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer. Eur J Cancer. 2018;89:27–35. doi:10.1016/j.ejca.2017.10.021
10. Onishi N, Gibbs JE, Li W, et al. Functional tumor volume at 3 and 6-week MRI as an indicator of patients with inferior outcome after neoadjuvant chemotherapy. Cancer Res. 2022;82.
11. Ray-Coquard I, Cassier P, Chabaud S, et al. GYNET study- Safety and efficacy of anti-netrin 1 (NP137) in combination with chemotherapy and/or pembrolizumab in patients (pts) with pretreated locally advanced/metastatic endometrial carcinoma or cervix carcinoma: an adaptive multi-arms randomized phase I/II trial. Ann Onc. 2021;32. doi:10.1016/j.annonc.2021.08.1259.
12. Xia X, Yin K, Wang S. Targeting of netrin-1 by monoclonal antibody NP137 inhibits the EMT in cancer. J Immunother Cancer. 2024;12(4). doi:10.1136/jitc-2024-008937
13. Breusa S, Thomas E, Baldinotti N, et al. Anti-Netrin-1 decorated nanoparticles combined with chemotherapy for the treatment of triple-negative breast cancer. Biomater Adv. 2024;161:213881. doi:10.1016/j.bioadv.2024.213881
14. Sheen-Chen SM, Ching-Hua T, Yueh-Wei L, Chao-Cheng H. Netrin-1 expression in breast cancer. J Cancer Res Pract. 6(3):124–127. doi:10.4103/JCRP.JCRP_8_19
15. Gao Y, Hu Y, Zhu Y, et al. Pan-cancer analysis reveals netrin-1 receptors as potential tumor biomarkers and immune-related therapeutic targets. Sci Rep. 2025;15(1):44015. doi:10.1038/s41598-025-28437-0
16. Robertson JFR, Jiang Z, Di Leo A, et al. A meta-analysis of clinical benefit rates for fulvestrant 500 mg vs. alternative endocrine therapies for hormone receptor-positive advanced breast cancer. Breast Cancer. 2019;26(6):703–711. doi:10.1007/s12282-019-00973-4
17. Ieni A, Barresi V, Caltabiano R, et al. Discordance rate of HER2 status in primary breast carcinomas versus synchronous axillary lymph node metastases: a multicenter retrospective investigation. Onco Targets Ther. 2014;7:1267–1272. doi:10.2147/OTT.S65294
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.