Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Relationship Between Muscle Cramps and Diabetic Retinopathy in Patients with Type 2 Diabetes
Authors Huiqing Hu, Wang C, Liang K ![]() , He Q, Song J, Guo X, Hou X
, He Q, Song J, Guo X, Hou X ![]() , Chen L
, Chen L ![]() , Yan F
, Yan F
Received 13 December 2021
Accepted for publication 24 February 2022
Published 15 March 2022 Volume 2022:15 Pages 827—837
DOI https://doi.org/10.2147/DMSO.S352735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Huiqing Hu,1 Chuan Wang,1– 4 Kai Liang,1– 4 Qin He,1 Jia Song,1 Xinghong Guo,1 Xinguo Hou,1– 4 Li Chen,1– 4 Fei Yan1– 4
1Department of Endocrinology, Qilu Hospital, Cheeloo College of Medicine, Shandong University, Jinan, 250012, People’s Republic of China; 2Institute of Endocrine and Metabolic Diseases of Shandong University, Jinan, 250012, People’s Republic of China; 3Key Laboratory of Endocrine and Metabolic Diseases, Shandong Province Medicine & Health, Jinan, People’s Republic of China; 4Jinan Clinical Research Center for Endocrine and Metabolic Diseases, Jinan, People’s Republic of China
Correspondence: Li Chen; Fei Yan, Department of Endocrinology, Qilu Hospital of Shandong University, No. 107 Wenhua Xi Road, Jinan, 250012, People’s Republic of China, Email [email protected]; [email protected]
Aim: Patients with type 2 diabetes (T2DM) often suffer from muscle cramps of varying severity. Studies have shown that muscle cramp is closely related to local microcirculation perfusion disorders. Diabetic retinopathy can not only reflect the microcirculation perfusion in the eye but also the systemic microcirculation in patients with diabetes. The aims of this study were to investigate the relationship between muscle cramps and diabetic retinopathy in patients with type 2 diabetes.
Methods: A total of 150 adult patients with type 2 diabetes were enrolled and administered a questionnaire on muscle cramping, along with a visual analogue scale for pain. Diabetic retinopathy (DR) was determined by using fundus photography and graded as non-proliferative DR (NPDR) and proliferative DR (PDR). To assess whether there was an association between the muscle cramps and diabetic retinopathy, we conducted binomial logistic regression analysis.
Results: Our study revealed that 48% of patients with T2DM experienced muscle cramps in the past three months. Patients self-reported suffering from muscle cramps exhibited a higher prevalence of DR (61% vs 38%, P < 0.05) and PDR (22% vs 4%, P < 0.05) compared with patients without muscle cramps. Serum 25-(OH) vitamin D, calcium, and magnesium levels were not significantly different between patients with and without muscle cramps. After adjusting for age, duration of diabetes, HbA1c, vitamin D, potassium, calcium, and magnesium, we demonstrated that diabetic retinopathy (OR, 2.18; 95% CI, 1.01– 4.69; P< 0.05) and albumin (OR, 0.90; 95% CI, 0.82– 1.00; P< 0.05) were highly associated with muscle cramps. Binomial logistic regression analysis also indicated that severity of DR is associated with muscle cramps. In addition, DR and PDR were found to be associated with muscle cramp frequency (P for trend < 0.05), duration (P for trend < 0.05), and pain severity (P for trend < 0.05).
Conclusion: Muscle cramps occur frequently in diabetes and are correlated with diabetic retinopathy and albumin. Patients with PDR exhibited a higher frequency, severity, and longer duration relative to those with NPDR or without DR. Our findings suggested that muscle cramps in individuals with T2DM might be a result of microvascular dysfunction. Modulation of microvascular perfusion might thus provide a therapeutic target for alleviating muscle cramps.
Keywords: muscle cramps, type 2 diabetes mellitus, diabetic retinopathy, proliferative diabetic retinopathy, vitamin D
Introduction
Muscle cramps are painful tonic contractions of the skeletal muscles that occur during sleep and rest. Certain physical activities and medical conditions such as exercise, polyneuropathy, hepatic and renal dysfunction, or metabolic disorders can induce muscle cramps.1,2 Some studies indicated that approximately 60% of patients with T2DM suffered from muscle cramps, and that the pain they experienced was more severe than that experienced by healthy people.3 Although muscle cramps are benign in nature, their occurrence is associated with a reduced quality of life and bodily pain T2DM.4
Common causes of muscle cramps include neurologic, muscular, and endocrine disorders; vitamin D insufficiency; or electrolyte imbalance.5–7 Several studies revealed that the pathophysiologic link to muscle cramps in patients may be the reduction in effective circulating volume.8,9 Since type 2 diabetes alters capillary hemodynamics, causes muscle capillary rarefaction, and decreased microvascular perfusion of muscle,10,11 we speculated that microvascular dysfunction may play a role in the pathogenesis of muscle cramps in type 2 diabetes. Investigators previously observed a significant correlation between diabetic peripheral neuropathy and muscle cramps, which was identified as the most important factor causing muscle cramps in patients with diabetes.3,12 However, a recent study of 120 diabetic patients reported that muscle cramps occur frequently in diabetes and are correlated clinically with both small and large nerve fiber measures in T1DM, but not in T2DM.13 The exact mechanism subserving the occurrence of muscle cramps in patients with T2DM remains elusive. However, despite the disparate pathogenesis of these two common forms of diabetes, they all share microvascular dysfunction.10,14 Three decades ago, the Framingham Heart and Eye Study indicated that diabetic retinopathy signs may reflect generalized micro-angiopathic processes that affect not only the eyes but also organs elsewhere in the body.15 However, the relationship between muscle cramps and diabetic retinopathy remains arcane. In this study, we evaluated the prevalence, characteristics, and predictors of muscle cramps in patients with type 2 diabetes, as well as the correlations between muscle cramp characteristics and diabetic retinopathy.
Materials and Methods
This cross-sectional study consisted of 150 patients with type 2 diabetes, recruited prospectively between July 2021 and September 2021 from Qilu Hospital of Shandong University. This study was approved by the Ethics Committee of Qilu Hospital of Shandong University. The written informed consent was obtained from each patient. Type 2 diabetes was diagnosed according to the 1999 World Health Organization criteria, which was defined as FPG greater than or equal to 7.0mmol/L, or blood glucose at random or 2 hours after an oral glucose tolerance test greater than or equal to 11.1mmol/L.16 Eligible patients also included pre-existing diabetes patients taking antidiabetic drugs, or physician-diagnosed type 2 diabetes. Inclusion criteria were an age of at least 18 years and the presence of T2DM. Exclusion criteria included the presence of diabetic ketoacidosis, a hyperglycemic hyperosmolar state, inflammatory or autoimmune disease, thyroid disease, parathyroid disease, malignancies, severe liver or kidney disease, cervical and lumbar vertebra disease, varicose veins of the lower extremities, and severe cerebral infarction. Diabetic ketoacidosis was defined as the presence of hyperglycemia (first plasma glucose≥13.9 mmol/l), acidosis (arterial or venous pH < 7.3 and and/or HCO3−≤15 mEq/L), and ketonuria in the absence of elevated effective plasma osmolality (≤320 mOsm/L). Hyperglycemic hyperosmolar state was defined as the presence of hyperglycemia (first glucose level >33.3 mmol/l) and elevated plasma effective osmolality (>320 mOsm/L).17 The National Institutes of Health Stroke Scale (NIHSS) was used to assess the severity of cerebral infarction. The NIHSS value was assessed and recorded by a neurologist. An NIHSS score of >5 was considered to severe cerebral infarction.18,19 For each eligible eye, two digital colour fundus photographs were captured and assessed by experienced physicians to minimize any possible bias. DR was considered present if any characteristic lesions as defined by Early Treatment Diabetic Retinopathy Study were present. Single-field photos of 45°, centred on the macula, were taken using non-mydriatic camera (pupils were not dilated) for both eyes in all study subjects (CanonCR-2; Canon). The minimum criterion for diagnoses of DR was presence of at least one definite micro aneurysm and/or retinal haemorrhage. DR severity was further categorized into non-proliferative DR (NPDR) and proliferative DR (PDR). DR was classified as NPDR based on the presence of one or more of the following features: micro aneurysms, haemorrhages, hard or soft exudates, venous beading and intraretinal microvascular abnormalities. DR was classified as PDR if there was neovascularization, pre-retinal haemorrhages, vitreous haemorrhage or panretinal laser photocoagulation scar.20
All subjects completed the questionnaire on cramping used in a previous study,21 details was in Figure 1. A medical doctor assisted the participants in understanding the characteristics of muscle cramps, and read the survey questions if/when patients needed assistance. The questions regarding the presence or absence of muscle cramps within the past three months, the frequency, duration, severity of pain using the VAS (visual analogue scale), duration, location of cramps, and time of day were translated from English into Chinese. Study variables, such as demographics (age, sex), physical findings [body mass index (BMI), mean arterial pressure (MBP)], lifestyle factor [tobacco smoking (yes or no), alcohol drinking (yes or no)], and serum indices (HbA1c, albumin, potassium, magnesium, creatinine, albumin, total calcium, and 25-OH-vitamin D3) within the last three months (closest to the enrollment day) were extracted from medical records. STROBE checklist was used as the guideline for this study.
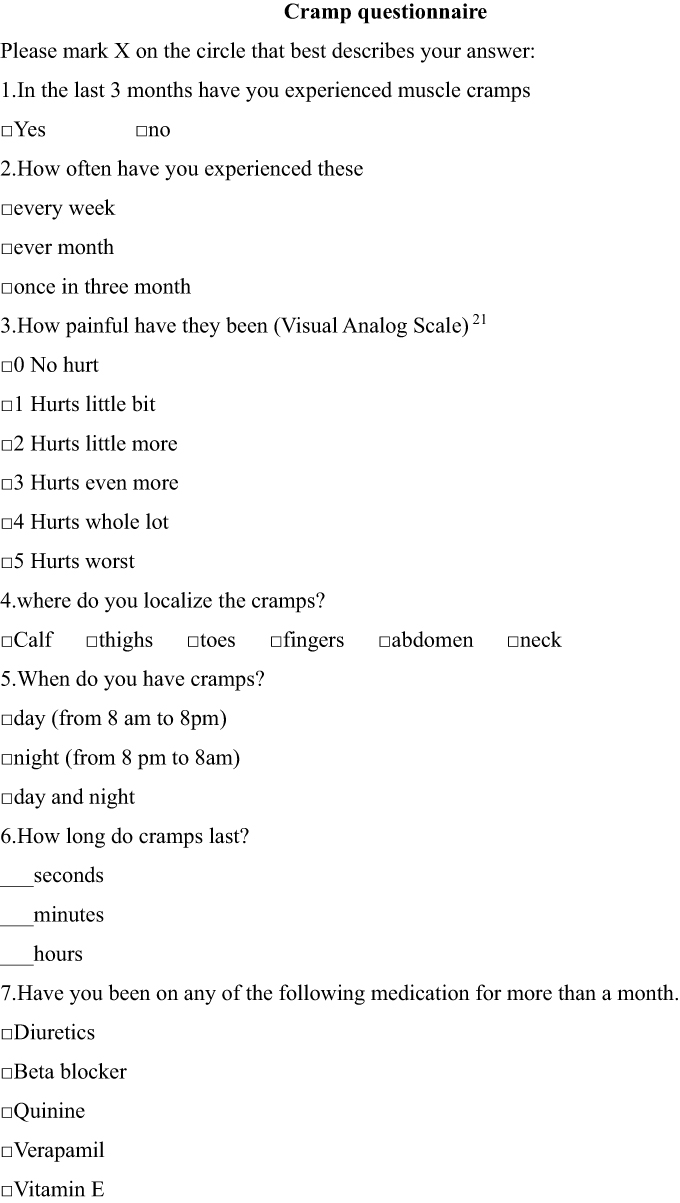 |
Figure 1 Muscle cramps questionnaire to capture description of muscle cramps (onset, frequency, duration, and localization) and severity of pain by visual analogue scale for pain (Wong-Baker FACES pain rating scale). |
Statistical Analysis
We performed statistical analysis using SPSS statistical software (version 23; SPSS, Chicago, IL). Categorical variables are presented as the number (percentage) of participants, and continuous variables are presented as the mean and SD; or, for those data with a skewed distribution, as the median (25th percentile, 75th percentile). Differences between groups were examined using an independent-sample t test. Continuous variables are presented as the median (interquartile range) for abnormally distributed data, and we employed the Mann–Whitney U-test to compare the differences between groups. Frequency differences were compared using χ2 test or Fisher’s exact test, where appropriate. Binomial logistic regression analyses were used to estimate the odds ratios (ORs) for potential risk factors associated with muscle cramps. Based on previous studies, we selected age alone for Model 1. Model 2 includes all variables in model 1 plus HbA1c and duration of diabetes (variables associated with diabetic retinopathy), Model 3 includes all variables in model 2 plus albumin, vitamin D, calcium, and magnesium (variables associated with muscle cramps).7,10,22,23 We presented the adjusted ORs for the muscle cramps with respect to diabetic retinopathy after adjustment for age, duration of diabetes, HbA1c, albumin, magnesium, albumin, total calcium, and 25-(OH) vitamin D3. A trend analysis was conducted by treating DR severity as an ordinal variable, assigning equally spaced numeric values to each category [ie, Patients without DR=0 (reference), Patients with NPDR=1, Patients with PDR=2]. This enabled the assessment of whether there was a linear pattern of increasing risk of muscle cramps with increasing DR severity. The linear trend for prevalence of muscle cramps with respect to diabetic retinopathy was examined using the χ2 test. The level of significance was set at P < 0.05.
Results
Comparisons Between Patients with and without Muscle Cramping
A total of 150 participants were prospectively enrolled in our study, and of these, 72 (48%) reported muscle cramps in the last three months. Although there were significant differences with regard to albumin and the presence of DR between individuals with and without cramps (P < 0.05, respectively), no significant differences were noted for BMI, age, SBP, smoking, drinking, HbA1c, albumin, potassium, magnesium, creatinine, albumin, total calcium, or 25-(OH) vitamin D3. Patients self-reported suffering from muscle cramps exhibited a higher prevalence of DR (61% vs 38%, P < 0.05) and PDR (22% vs 4%, P < 0.05) compared with patients without muscle cramps (Table 1).
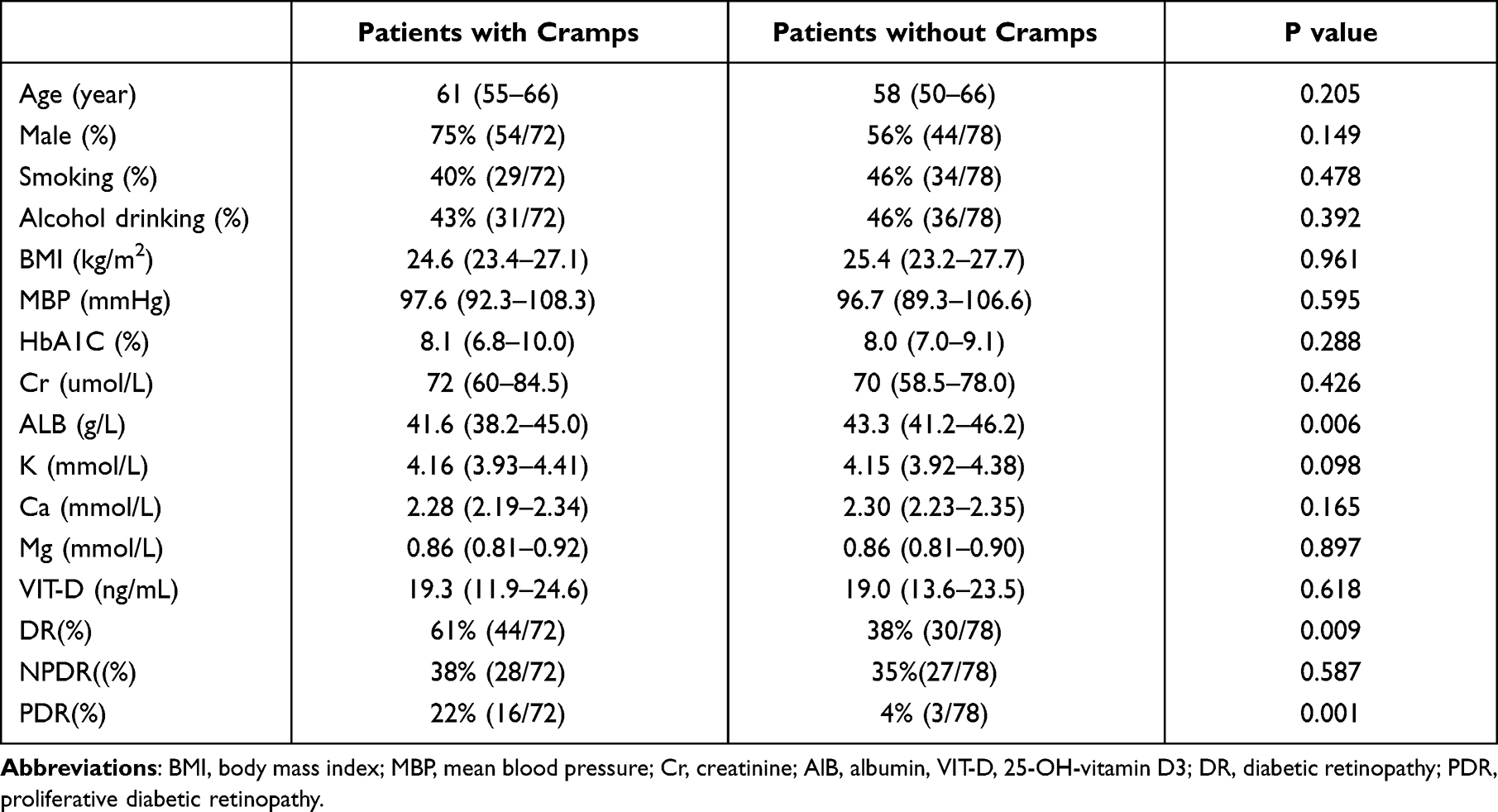 |
Table 1 Clinical Characteristics of All Patients (n=150) |
In the 72 diabetic patients self-reported suffering from cramps, we evaluated frequency, VAS, time of day, location, and duration of muscle cramps. Twenty-four (33.3%) patients experienced muscle cramping at least once a week, 31 (43.1%) at least once a month, and 17 (23.6%) experienced cramps once within the last three months. As for time of day, 49 (68.1%) experienced cramps at night and 8 (11.1%) during both the day and night. In addition, assessment of pain severity showed that 27 (37.5%) had a VAS of 4 or greater. 56 (77%) patients had muscle cramps lasting for minutes, whereas 16 (22.2%) reported them lasting for a few seconds (Figure 2).
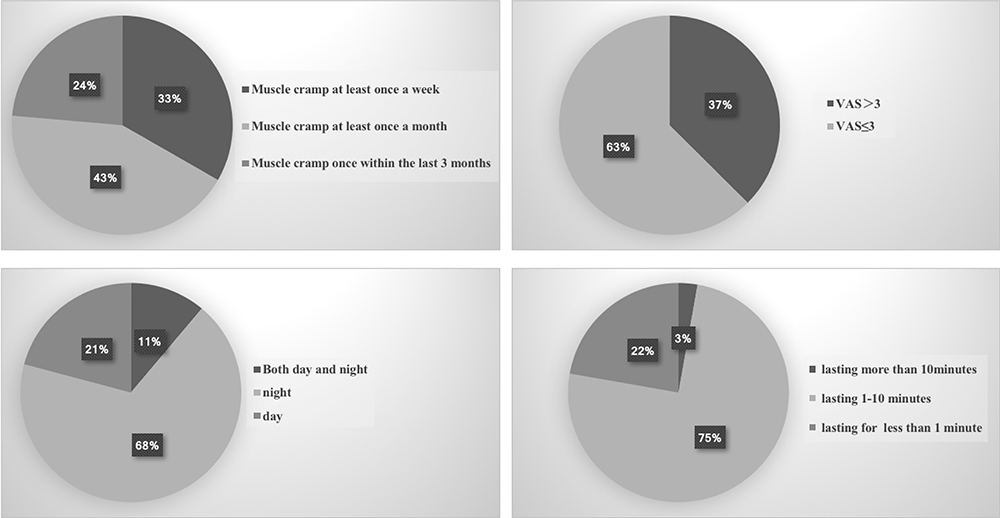 |
Figure 2 Frequency of muscle cramps, severity of pain, time of day of muscle cramps, duration of muscle cramps. Abbreviation: VAS, visual analogue scale. |
Relationship of Muscle Cramps to Diabetic Retinopathy and Severity of Diabetic Retinopathy in Patients with T2DM
In model 1, diabetic retinopathy (OR, 2.46; 95% CI, 1.27–4.76; P< 0.05) was highly associated with muscle cramps. Model 2 showed that diabetic retinopathy was the only significant determinant for muscle cramps (OR, 2.48; 95% CI, 1.24–4.95; P< 0.05) but not HbA1c and duration of diabetes. Model 3 showed that patients with diabetic retinopathy (OR, 2.18; 95% CI, 1.01–4.69; P< 0.05) and lower albumin levels (OR, 0.90; 95% CI, 0.82–1.00; P< 0.05) had higher odds of muscle cramps (Table 2).
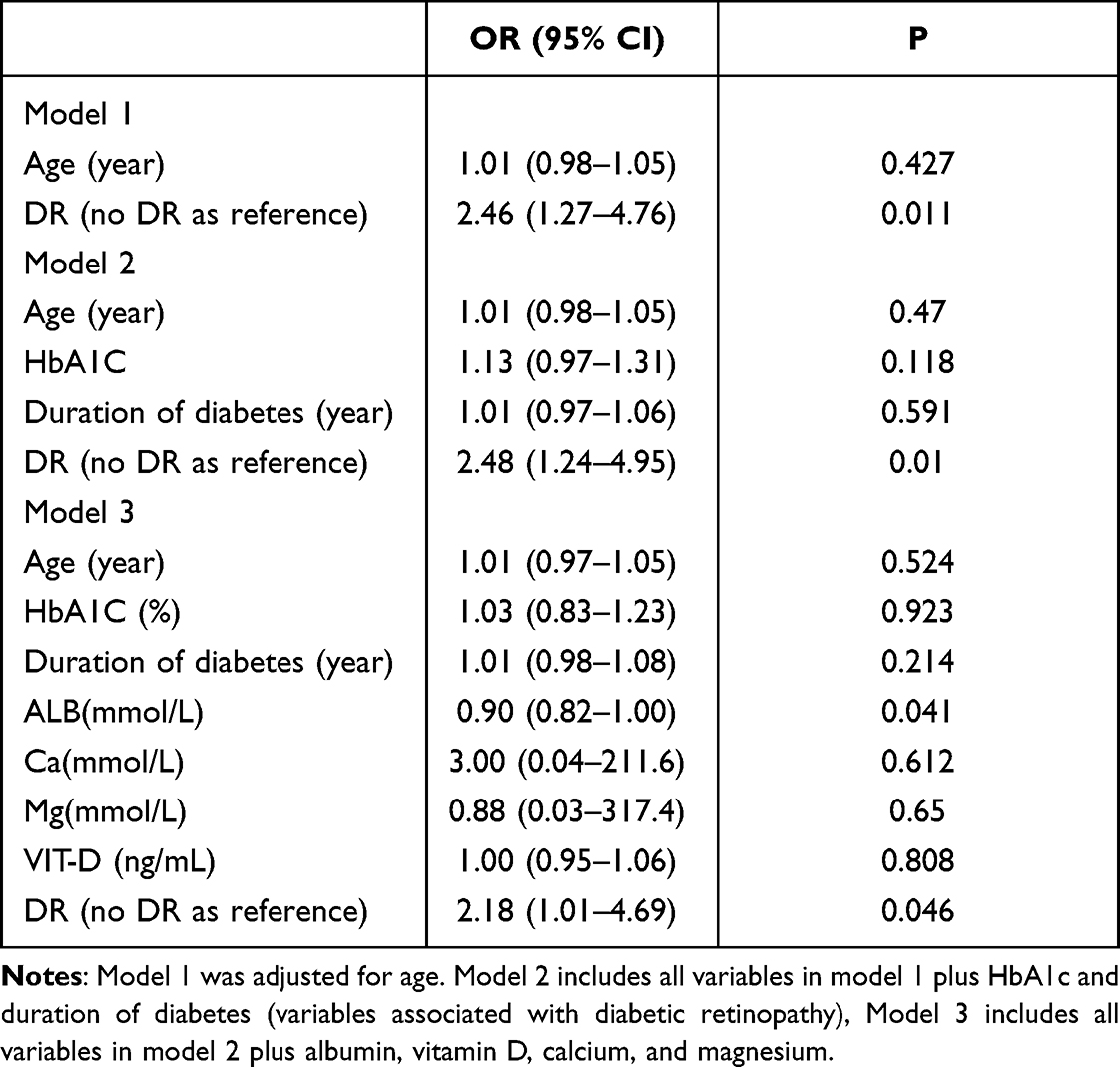 |
Table 2 Relationship Between Muscle Cramps and Diabetic Retinopathy a After Controlling for Confounding Factors |
After adjusting for age, duration of diabetes, HbA1c, vitamin D, potassium, calcium, and magnesium, among all DR severity levels, only patients with PDR (OR, 8.02; 95% CI, 1.41–45.4; P = 0.019) had higher odds of muscle cramps compared with patients without DR. Although no association was observed between NPDR and muscle cramps, a trend analysis showed a linear pattern of increasing risk of muscle cramps with increasing severity of DR (P for trend < 0.05) (Table 3).
 |
Table 3 Associations Between Severity of DR and Muscle Cramps in Type 2 Diabetes |
Relationship of Muscle Cramp Frequency, Duration, Pain Severity, Time of Day with Diabetic Retinopathy
PDR was significantly more prevalent (29%, P < 0.05) in patients with higher muscle cramping frequency (ie, several times per week). Patients with severe pain (>3 on a scale of 0–5) exhibited a higher prevalence of DR (74%, P < 0.05) and PDR (25%, P < 0.05) relative to patients with mild pain (>3 on a scale of 0–5) or patients without muscle cramps. Our data revealed that the prevalence of DR (65%, P < 0.05) and PDR (24%, P < 0.05) were higher in patients with a muscle-cramp duration lasting 1–10 minutes. In addition, DR and PDR were found to be associated with muscle cramp frequency (P for trend < 0.01), duration (P for trend < 0.01), and pain severity (P for trend < 0.01). Although the prevalence of DR and PDR was higher in patients with muscle cramps during the daytime, we observed no relationship between the time of the day and the prevalence of DR and PDR (Table 4).
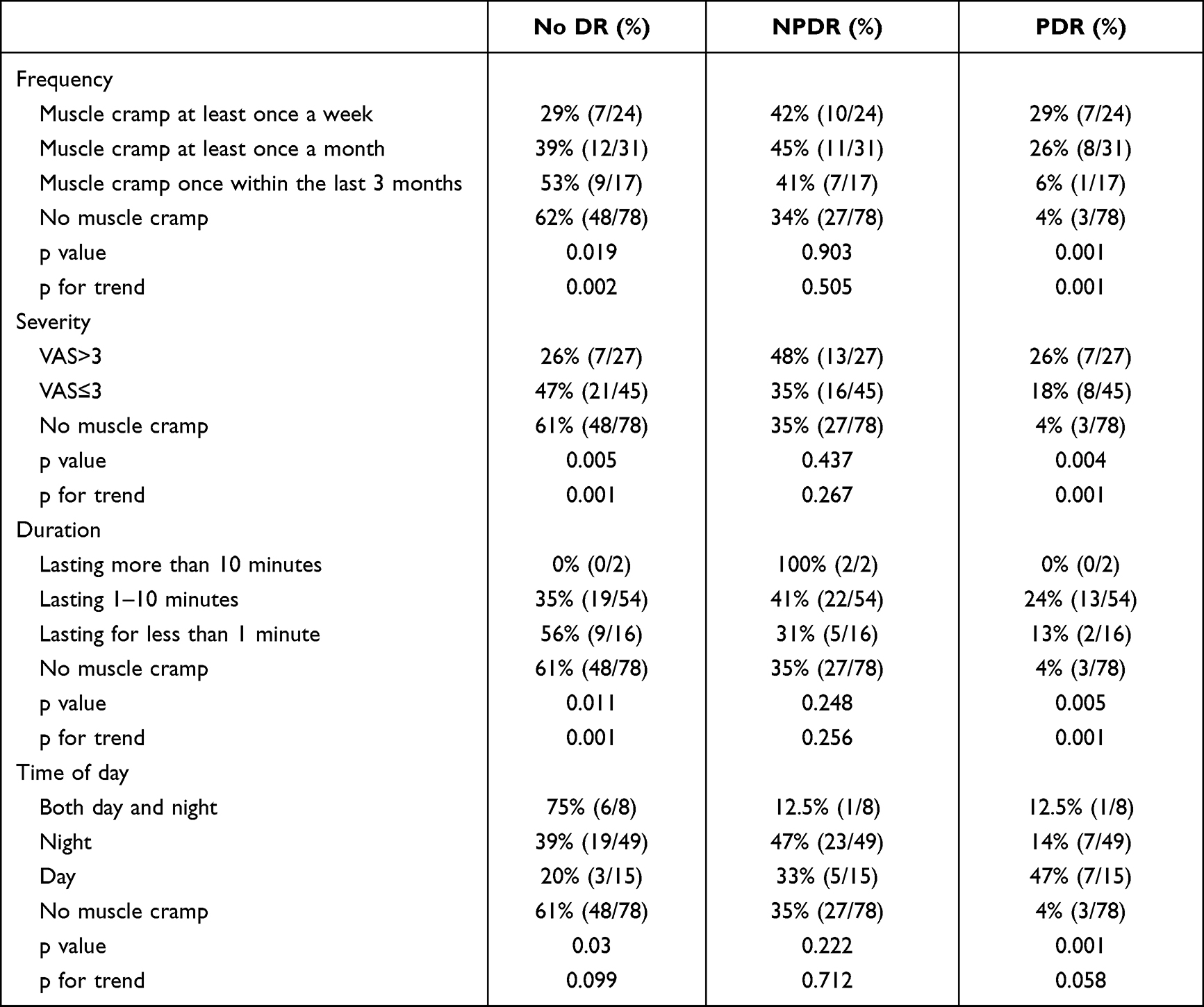 |
Table 4 Relationships Between Muscle Cramp Frequency, Duration Length, Pain Severity, Location of Muscle Cramps, Time of Day, and Diabetic Retinopathy |
Discussion
An association between muscle cramps and diabetes has been well documented. The prevalence of diabetic patients with muscle cramps is very high, and the prevalence varies—ranging from 65% to 75% depending upon the inclusion criteria used by the investigators.3,4,24 Due to the intermittent nature of muscle cramps, inability to measure an individual’s predisposition to muscle cramps by means of any diagnostic tool and lack of objective findings, the symptoms are often dismissed. The current study showed that muscle cramps were common in patients with T2DM in China, and were present in up to 48.7% of patients— which was lower than prior estimates (65–75%). This difference may be attributed to our patients being younger (58.3 vs 65.2) compared to a previous study.13 In addition, we herein reported various characteristics of muscle cramps in type 2 diabetes, including frequency (32.9% had cramps at least once a week), duration (lasting several minutes in up to 77.8% of cases), and severity of associated pain (56% were at >3 on a 0–5 scale). In our study, we found that 96% (70/73) of the patients reported cramping in the calf muscle with muscle cramps. Only 3 of the patients reported cramping in the upper limbs. Therefore, we did not analyzed the relationship of location of muscle cramps between diabetic retinopathy. Future studies with larger sample sizes may be feasible and necessary.
An additional finding in our study was the high prevalence of inadequate vitamin D levels. Approximately 94% of patients in our study exhibited vitamin D levels under 30 ng/mL. Investigators previously noted that patients with vitamin D insufficiency manifested severe symptoms of muscle cramps, fatigue, back pain, and weight gain.25,26 However, our study revealed that serum vitamin D and calcium levels were not different between patients with and without muscle cramps, and were not related to muscle cramps. Similarly, several groups have already reported that calcium and vitamin D levels were not predictive of the onset of muscle cramps in patients with cirrhosis or in pregnant women.21,27 More importantly, the calcium-vitamin D supplements did not improve the frequency or severity of the muscle cramps.22,28 Although other electrolyte imbalances (eg, hypomagnesemia and hypokalemia) were also reportedly associated with muscle cramps,23 we did not find relationship between muscle cramps and serum magnesium or potassium.
Based on previous studies, a reduction in the effective plasma volume may be involved in the pathophysiology of muscle cramps in cirrhosis. Infusion of human albumin decreased the frequency of muscle cramps by improving the effective circulating volume in 12 cirrhotic patients.8 In addition, muscular cramps occur frequently in patients with chronic arterial obstructive disorders of the lower limbs, which are associated with muscular ischemia.1,29 The potential mechanism of action underlying this association might be related to an alteration in neural cell membrane excitability as a consequence of decreased microvascular perfusion of the muscle.30 Therefore, we speculated that muscle capillary rarefaction and decreased microvascular perfusion to muscle may play a role in the pathogenesis of muscle cramps in T2DM. Previous studies suggested that the progression of diabetic retinopathy correlated with muscle-perfusion disturbances of the lower limbs.31–33 Consistent with these prior findings, our current data provided firsthand evidence that patients with muscle cramps showed a higher prevalence of DR and PDR, and that cramps were significantly associated with these two disorders. Intriguingly, we did not ascertain a relationship between NPDR and muscle cramps; the possible reason for this might be that the microvascular impairment of muscle in patients with NPDR was not as severe as in patients with PDR. We also found that DR severity was positively associated with muscle cramp frequency, duration, and pain severity. These findings signified that muscle cramps in individuals with type 2 diabetes might be a result of microvascular dysfunction. Modulation of microvascular perfusion might thus provide a therapeutic target for alleviating muscle cramps.
There were some limitations to this study. First, our study was retrospective in nature. Furthermore, objective evaluations of muscle cramps in this study were difficult because the findings were primarily based on an interview with each patient. Third, the sample size was small, and therefore studies with a larger sample size are needed to confirm our current findings. The last, we did not assess diabetic neuropathy in this study, despite the literature reporting that muscle cramps in T2DM do not appear to be associated with diabetic neuropathy,13 it’s one of the limitations of our study. In addition, both diabetic retinopathy and diabetic neuropathy are important microvascular complication of diabetes, the collinearity between those two variables may present in the model.34 Based on the present clinical results, effective strategies for interventions with respect to muscle cramps need to be established in the future.
Conclusions
Muscle cramps are frequent in diabetes and are correlated with diabetic retinopathy. Patients with muscle cramps exhibited a higher prevalence of DR and PDR, and cramps were significantly associated with the severity of DR. DR and PDR were positively associated with muscle cramp frequency, duration, and pain severity. However, additional research is needed to better understand the mechanism(s) underlying cramps, and to develop effective treatment modalities.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Statements
The research protocol was approved by the ethics committee of Qilu Hospital of Shandong University, and the ethics number is 20210701. All enrolled patients signed the informed consent form. Approval date of Registry is July 2, 2021. The study complied with the Declaration of Helsinki.
Acknowledgments
The authors thank all of the involved clinicians, nurses, and technicians for dedicating their time and skill to this study.
Author Contributions
Huiqing Hu collected and analyzed data. Fei Yan analyzed data and wrote the manuscript. Chuan Wang and Kai Liang, Qin He enrolled patients in the study. Xinghong Guo and Jia Song coordinated research. Xinguo Hou and Li Chen conceived the idea, designed the study. Fei Yan is the guarantor of this work and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the National Natural Science Foundation of China (grant no. 81100736), Shandong Province Key Research and Development Project (project no. 2019GSF108099) and China Diabetes Talents Research Project (grant no. 6010119049).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Parisi L, Pierelli F, Amabile G, et al. Muscular cramps: proposals for a new classification. Acta Neurol Scand. 2003;107(3):176–186. doi:10.1034/j.1600-0404.2003.01289.x
2. Sawada Y, Shiraki M, Iwasa M, et al. The effects of diuretic use and the presence of ascites on muscle cramps in patients with cirrhosis: a nationwide study. J Gastroenterol. 2020;55(9):868–876. doi:10.1007/s00535-020-01694-8
3. Katzberg H, Kokokyi S, Halpern E, et al. Prevalence of muscle cramps in patients with diabetes. Diabetes Care. 2014;37(1):e17–18. doi:10.2337/dc13-1163
4. Imbe A, Tanimoto K, Inaba Y, et al. Effects of L-carnitine supplementation on the quality of life in diabetic patients with muscle cramps. Endocr J. 2018;65(5):521–526. doi:10.1507/endocrj.EJ17-0431
5. Abrams GA, Concato J, Fallon MB. Muscle cramps in patients with cirrhosis. Am J Gastroenterol. 1996;91(7):1363–1366.
6. Salmanpour VA, Ibrahim HS, Salameh AG, Yahya AM, Debal BK. Vitamin D deficiency: knowledge and practices among the adult population in Sharjah, United Arab Emirates. Arch Osteoporos. 2016;11:15. doi:10.1007/s11657-016-0269-0
7. Marotta PJ, Graziadei IW, Ghent CN. Muscle cramps: a “complication” of cirrhosis. Can J Gastroenterol. 2000;14 Suppl D:21D–25D. doi:10.1155/2000/214916
8. Angeli P, Albino G, Carraro P, et al. Cirrhosis and muscle cramps: evidence of a causal relationship. Hepatology. 1996;23(2):264–273. doi:10.1002/hep.510230211
9. Vinciguerra G, Belcaro G, Cesarone MR, et al. Cramps and muscular pain: prevention with pycnogenol in normal subjects, venous patients, athletes, claudicants and in diabetic microangiopathy. Angiology. 2006;57(3):331–339. doi:10.1177/000331970605700309
10. Barrett EJ, Liu Z, Khamaisi M, et al. Diabetic microvascular disease: an endocrine society scientific statement. J Clin Endocrinol Metab. 2017;102(12):4343–4410. doi:10.1210/jc.2017-01922
11. Yan F, Yuan Z, Wang N, et al. Direct activation of angiotensin II Type 2 receptors enhances muscle microvascular perfusion, oxygenation, and insulin delivery in male rats. Endocrinology. 2018;159(2):685–695. doi:10.1210/en.2017-00585
12. Kastenbauer T, Irsigler P, Sauseng S, Grimm A, Prager R. The prevalence of symptoms of sensorimotor and autonomic neuropathy in Type 1 and Type 2 diabetic subjects. J Diabetes Complications. 2004;18(1):27–31. doi:10.1016/S1056-8727(03)00071-0
13. Abraham A, Barnett C, Lovblom LE, Perkins BA, Bril V, Katzberg HD. Cramps frequency and severity are correlated with small and large nerve fiber measures in type 1 diabetes. Clin Neurophysiol. 2018;129(1):122–126. doi:10.1016/j.clinph.2017.10.029
14. Zheng C, Liu Z. Vascular function, insulin action, and exercise: an intricate interplay. Trends Endocrinol Metab. 2015;26(6):297–304. doi:10.1016/j.tem.2015.02.002
15. Hiller R, Sperduto RD, Podgor MJ, Ferris FL
16. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
17. Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335–1343. doi:10.2337/dc09-9032
18. Heldner MR, Chaloulos-Iakovidis P, Panos L, et al. Outcome of patients with large vessel occlusion in the anterior circulation and low NIHSS score. J Neurol. 2020;267(6):1651–1662. doi:10.1007/s00415-020-09744-0
19. Da Ros V, Cortese J, Chassin O, et al. Thrombectomy or intravenous thrombolysis in patients with NIHSS of 5 or less? J Neuroradiol. 2019;46(4):225–230. doi:10.1016/j.neurad.2019.01.089
20. Wilkinson CP, Ferris FL
21. Chatrath H, Liangpunsakul S, Ghabril M, Otte J, Chalasani N, Vuppalanchi R. Prevalence and morbidity associated with muscle cramps in patients with cirrhosis. Am J Med. 2012;125(10):1019–1025. doi:10.1016/j.amjmed.2012.03.012
22. Mansouri A, Mirghafourvand M, Charandabi SMA, Najafi M. The effect of Vitamin D and calcium plus Vitamin D on leg cramps in pregnant women: a randomized controlled trial. J Res Med Sci. 2017;22:24. doi:10.4103/1735-1995.200271
23. Martinez-Navarro I, Montoya-Vieco A, Collado E, Hernando B, Panizo N, Hernando C. Muscle cramping in the marathon: dehydration and electrolyte depletion vs. muscle damage. J Strength Cond Res. 2020;Publish Ahead of Print. doi:10.1519/JSC.0000000000003713
24. Restivo DA, Casabona A, Frittitta L, et al. Efficacy of botulinum toxin A for treating cramps in diabetic neuropathy. Ann Neurol. 2018;84(5):674–682. doi:10.1002/ana.25340
25. Sadat-Ali M, Al Essa ON, Alani FM, Al Omar HK, Ebrahim WY. Correlation of symptoms to serum vitamin D levels? Clin Nutr ESPEN. 2018;24:31–34. doi:10.1016/j.clnesp.2018.02.004
26. Kinoshita Y, Masuoka K, Miyakoshi S, Taniguchi S, Takeuchi Y. Vitamin D insufficiency underlies unexpected hypocalcemia following high dose glucocorticoid therapy. Bone. 2008;42(1):226–228. doi:10.1016/j.bone.2007.09.042
27. Luo L, Zhou K, Zhang J, Xu L, Yin W. Interventions for leg cramps in pregnancy. Cochrane Database Syst Rev. 2020;12:CD010655. doi:10.1002/14651858.CD010655.pub3
28. Weiker MK, Nielsen B, Waclawik AJ, Staples AC, Hansen KE. Muscle cramps do not improve with correction of Vitamin D insufficiency. WMJ. 2017;116(5):200–204.
29. Yanase F, Kato M, Matsumoto R, Horaguchi T, Kinoshita H. Postoperative muscular cramp caused by lower limb ischemia related to the unilateral popliteal arteriovenous fistula. J Clin Anesth. 2016;34:143–144. doi:10.1016/j.jclinane.2016.03.051
30. Takeuchi M, Low PA. Dynamic peripheral nerve metabolic and vascular responses to exsanguination. Am J Physiol. 1987;253(4 Pt 1):E349–353. doi:10.1152/ajpendo.1987.253.4.E349
31. Tryniszewski W, Gadzicki M, Maziarz Z, et al. Progression of diabetic retinopathy correlated with muscle perfusion disturbances of the lower limbs, with clinically important diagnostic recommendations. Arch Med Sci. 2010;6(6):904–911. doi:10.5114/aoms.2010.19300
32. Klein RF, Feingold KR, Morgan C, Stern WH, Siperstein MD. Relationship of muscle capillary basement membrane thickness and diabetic retinopathy. Diabetes Care. 1987;10(2):195–199. doi:10.2337/diacare.10.2.195
33. Li J, Li Y, Ma W, et al. Association of time in range levels with lower extremity arterial disease in patients with type 2 diabetes. Diabetes Metab Syndr. 2020;14(6):2081–2085. doi:10.1016/j.dsx.2020.09.028
34. Faselis C, Katsimardou A, Imprialos K, Deligkaris P, Kallistratos M, Dimitriadis K. Microvascular complications of Type 2 diabetes mellitus. Curr Vasc Pharmacol. 2020;18(2):117–124. doi:10.2174/1570161117666190502103733
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.