Back to Journals » Advances in Medical Education and Practice » Volume 14
Relationship Between Metacognitive Awareness of Undergraduate Students and Students’ Academic Performance at Vietnam Military Medical University
Authors Xuan Nguyen K ![]() , Viet Tran T, Duc Nghiem T, Ngoc Tran T, Ba Ta T, Van Nguyen B, Dinh Le T
, Viet Tran T, Duc Nghiem T, Ngoc Tran T, Ba Ta T, Van Nguyen B, Dinh Le T ![]() , Tien Nguyen S
, Tien Nguyen S ![]() , Nguyen KT
, Nguyen KT ![]() , Trung Dinh H
, Trung Dinh H ![]() , Pho DC
, Pho DC ![]() , Nguyen Duy T
, Nguyen Duy T ![]() , Toan PQ
, Toan PQ ![]()
Received 11 April 2023
Accepted for publication 7 July 2023
Published 17 July 2023 Volume 2023:14 Pages 791—801
DOI https://doi.org/10.2147/AMEP.S412912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Kien Xuan Nguyen,1,* Tien Viet Tran,2 Thuan Duc Nghiem,3 Tuan Ngoc Tran,1 Thang Ba Ta,4 Ba Van Nguyen,5 Tuan Dinh Le,6,* Son Tien Nguyen,6 Kien Trung Nguyen,7 Hoa Trung Dinh,8 Dinh Cong Pho,9 Toan Nguyen Duy,10,* Pham Quoc Toan11
1Department of Military Medical Command and Organization, Vietnam Military Medical University, Hanoi, 10000, Vietnam; 2Department of Infectious Diseases, Military Hospital 103, Vietnam Military Medical University, Hanoi, 10000, Vietnam; 3Department of Otolaryngology, Military Hospital 103, Vietnam Military Medical University, Hanoi, 10000, Vietnam; 4Respiratory Center, Military Hospital 103, Vietnam Military Medical University, Hanoi, 10000, Vietnam; 5Department of Oncology, Military Hospital 103, Vietnam Military Medical University, Hanoi, 10000, Vietnam; 6Department of Rheumatology and Endocrinology, Military Hospital 103, Vietnam Military Medical University, Hanoi, 10000, Vietnam; 7Center of Hematology and Blood Transfusion, Military Hospital 103, Vietnam Military Medical University, Hanoi, 10000, Vietnam; 8Department of Requested Treatment, National Hospital of Endocrinology, Hanoi, Vietnam; 9Department of Military Science, Vietnam Military Medical University, Hanoi, 10000, Vietnam; 10Cardiovascular Center, Military Hospital 103, Vietnam Medical Military University, Hanoi, 10000, Vietnam; 11Department of Nephrology, Military Hospital 103, Vietnam Military Medical University, Hanoi, 10000, Vietnam
*These authors contributed equally to this work
Correspondence: Pham Quoc Toan, Department of Nephrology, Military Hospital 103, Vietnam Military Medical University, 160 Phung Hung Street, Phuc La Ward, Ha Dong District, Hanoi, Vietnam, Email [email protected]
Introduction: Metacognition plays an essential role in competency-based medical education. Metacognitive skills consist of knowledge and regulation metacognition. This study was conducted to investigate the metacognition of undergraduate students and its correlation with students’ academic performance.
Methods: The metacognitive skills inventory comprised 52 binary-scale items administered to 202 Vietnam Military Medical University medical students. The entire semester and clinical results were used to measure their academic performance.
Results: Medical students’ total metacognitive awareness score was high (median 0.8). The median metacognitive knowledge score was significantly lower than the metacognitive regulation score (0.7 vs 0.8, respectively). The participants with a total metacognition score ≥ 0.8 had significantly higher academic results (full semester exam results of 7.4 and clinical exam of 7.5). The group of participants in the military, having sports habits and usually searching academic documents in English, had a higher proportion of total metacognitive awareness score ≥ 0.8 than the group without these above characteristics (with the percentages of 53.3%, 59%, and 64.3%, respectively; p < 0.05). The number of books read by participants with a total metacognitive awareness score ≥ 0.8 was significantly higher than those with a total metacognitive awareness score < 0.8 (3.5 compared to 2.4 books).
Conclusion: Metacognitive awareness of Vietnam Military Medical University medical students was likely to be high. A high score of metacognitive awareness could predict high academic performance. Being a military student, playing sports, reading books, and searching English documents were predictors of better metacognitive awareness.
Keywords: metacognition, medical student, metacognitive awareness, academic performance
Introduction
Competency-based medical education (CBME) is a common trend in the world and Vietnam in the early twenty-first century.1,2 Competency-based medical education approaches to teaching and learning methods emphasize that learners achieve the capacity to do medical jobs successfully and efficiently after medical education programs.3 The learners are centralized in medical education progression. They choose motivational learning methods and facilities to get outcomes related to patients, populations, and health professions education programs.3 The learners must get their knowledge and regulate the learning process called metacognition.4–6 Learners with metacognitive strategies can plan, control and regulate their cognition process.7,8
Brown was the first to call the term “metacognition”, which includes knowledge and the regulation of cognition.5,9 Knowledge about cognition has three components: declarative, procedural, and conditional knowledge.1,10,11 Regulation of cognition had five components: planning, information management strategies, comprehension monitoring, debugging strategies, and evaluation.1,4,11 There are many inventories have been created to assess metacognition.12–14 Some of them are more popular such as Metacognition awareness guidance (MCAG), metacognition awareness of reading strategy inventory (MARSI), Meta-cognition skills inventory (MSI), and MAI.14–17 The MAI was created by Schraw and Dennison (1994) that provided a more useful tool to assess baseline and follow-up levels of specific criteria of metacognition.1,18 These criteria include the development of metacognitive knowledge; planning and organizing; and selecting, implementing, monitoring, and evaluating learning strategies.1,5 Metacognition has been studied and published around the globe, showing the components of metacognition, including metacognitive knowledge and regulation, and showing more detailed compartments.7,19–21 Almost nations are affected by the Covid-19 pandemic. There are some papers researched on metacognition that have been published in the covid 19 pandemic era (2020–2022). The research on metacognition in Covid-19 pandemic era showed that MOOC was more effective in fostering the deep learning aspects of high metacognition skills and deep learning as a whole.22 Other study found that online flipped classrooms could improve self-directed learning and metacognitive awareness in nursing education.23 Iin Hindun observed work cognition and metacognitive awareness at different levels of local teachers in Indonesia.24 At Vietnam Military Medical University, medical assessments focus almost on clinical skills. We performed this study to investigate undergraduate students’ metacognitive awareness using the MAI questionnaire and the relation between MAI scores and students’ academic performance at Vietnam Military Medical University.
Methods
We performed a prospective, descriptive, cross-sectional study on 202 participants who were students in undergraduate general medical courses from the first year to the sixth year, including military and non-military students at the Vietnam Military Medical University from 2020 to 2021.
Data Collection: The questionnaire consisted of two main parts: background information and MAI score. The background information includes age, gender, year of academic education, military or non-military, place of living before, regional living before being a student, habit in sports, habit in reading, type of reading book, habit in learning, searching English documents, and academic results. The MAI score was assessed with MAI 52 binary-scale items that Schraw and Dennison created in 1994,1 the result of each question got 2 points on the binary scale, including a value of 1 if the participant answered “true” and a value of 0 if the participant answered “false”. Which includes knowledge and regulation of MAI with eight compartments: procedural knowledge, declarative knowledge, conditional knowledge, information management strategies, planning, comprehension monitoring, debugging strategies and evaluation12,18 (Table S1). MAI questionnaires were translated into Vietnamese by one expert in the English language who blinded to our research. Before starting the study, a trial survey was conducted on 32 Vietnamese students to ensure the feasibility and appropriateness of the MAI score for this population. The Vietnamese questionnaire version of MAI was administered online using a licensed Surveynuts tool. The link was sent to participants by Zalo, Messenger, and Email. The participants answered all of the questions through their online facilities during the Covid 19 pandemic (April 2021). All data was sent automatedly to the account of the researchers. Data from participants who had the same answers for all questions or did not complete all questions of the MAI score were excluded.
Ethical Statements
The participants were voluntary, and the research data was confidential and anonymized. The data sheets of respondents were kept locked up in a password-protected computer and were only used by the researchers. The study was approved by the Ethics Committee of the Vietnam Military Medical University (No 299/2014/VMMU-IRB). The study was also conducted using good clinical practice following the Declaration of Helsinki.
Statistical Analyzed
Data were analyzed using the licensed Stata 17. For each variable in varlist, sktest presents a test for normality based on skewness. The MAI score and base characteristics of participants were described as descriptive statistics. Chi-square and ANOVA tests were used to compare the participants with metacognitive awareness inventory scores ≥ 0.8 different from base characteristics, including average academic and clinical results of last semester. Multivariable logistic analysis was used to determine the variables that could significantly affect the metacognitive awareness total score ≥ 0.8.
Results
Table 1 shows the characteristics of 202 participants, in which males and females accounted for 72.8% and 27.2%, respectively. The proportion of military students was 75.2%, while 24.8% were non-military students. 76.2% came from suburban, while 23.8% were from urban (75.7% from the North and 24.3% from the South of Viet Nam) (Table 1).
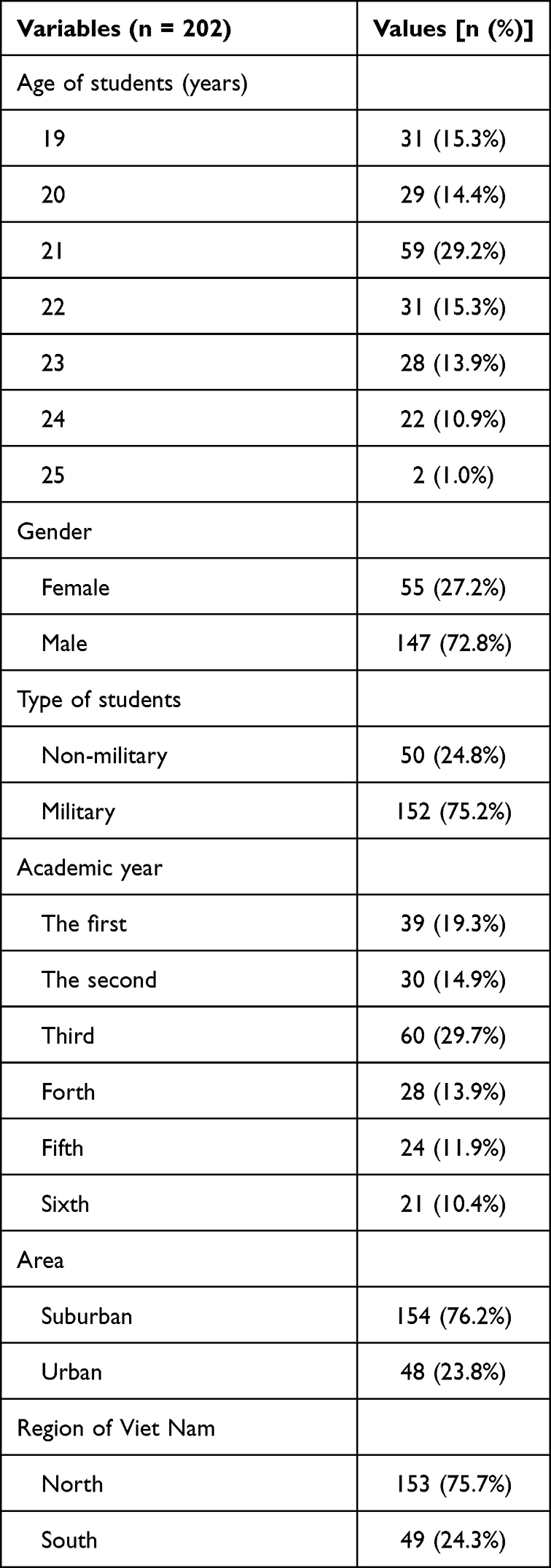 |
Table 1 Characteristics of the Participants |
The results in Table 2 showed the ratio of participants separated by favorites, habits in sports, studying, and academic performance in the last semester (Table 2).
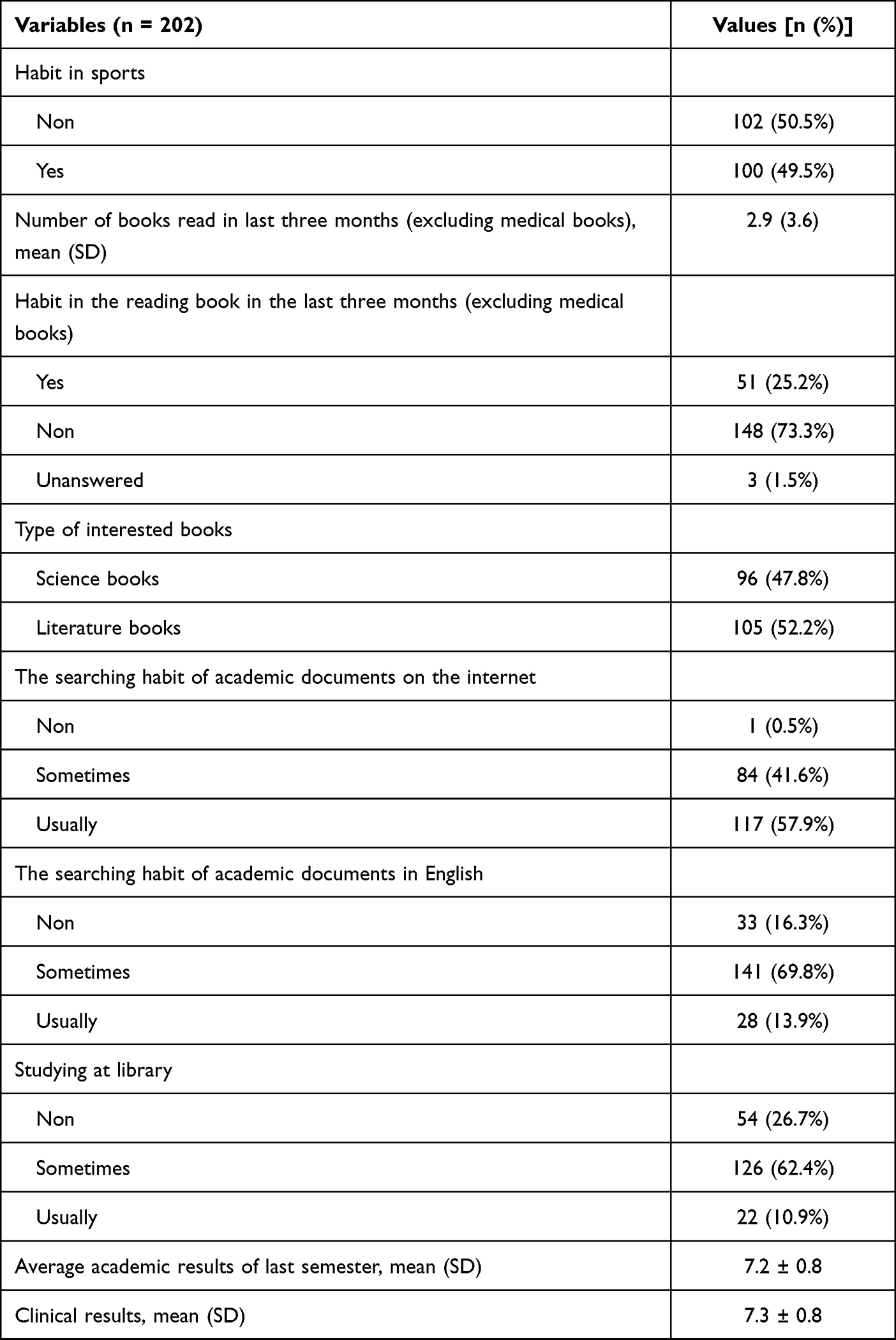 |
Table 2 Characteristics of Favorite, Habits, and Academic Performance |
The metacognitive knowledge score was significantly lower than the metacognitive regulation score (Wilcoxon signed-rank test; p = 0.001). The declarative knowledge score was the lowest at 0.6 (0.5–0.9) within the eight compartments of the MAI score (Table 3).
 |
Table 3 Metacognitive Awareness Score |
Table 4 shows that the proportion of total metacognitive awareness score ≥ 0.8 in military participants was significantly higher than in non-military participants. The fourth school year participants had a significantly lower proportion of metacognitive awareness total score ≥ 0.8 than in other years of academic study (Table 4).
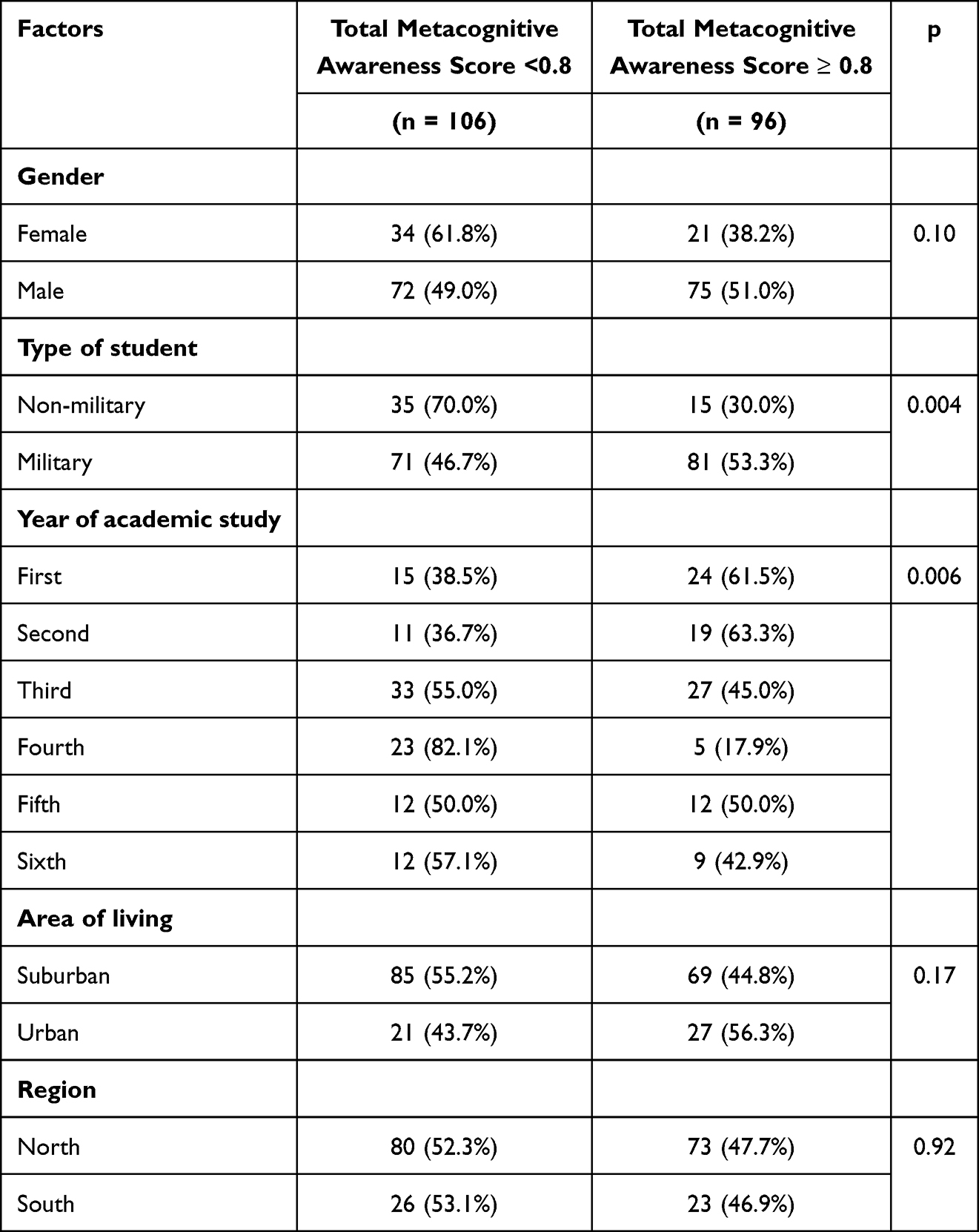 |
Table 4 The Relationship Between Total Metacognitive Awareness Score and Age, Gender, Academic Year, and Geographic Characteristics |
As shown in Table 5, the rate of total metacognitive awareness score ≥ 0.8 in participants with sports habits and searching habits for academic documents in English was significantly higher than in other participants. The participants with a total metacognitive awareness score ≥ 0.8 read more books, particularly the number of books in the last three months (excluding medical books), than others. The participants getting total metacognitive awareness score ≥ 0.8 had significantly higher full exam results (7.4 ± 0.8) and clinical exam results (7.5 ± 0.8) for the last semester than the others (Table 5).
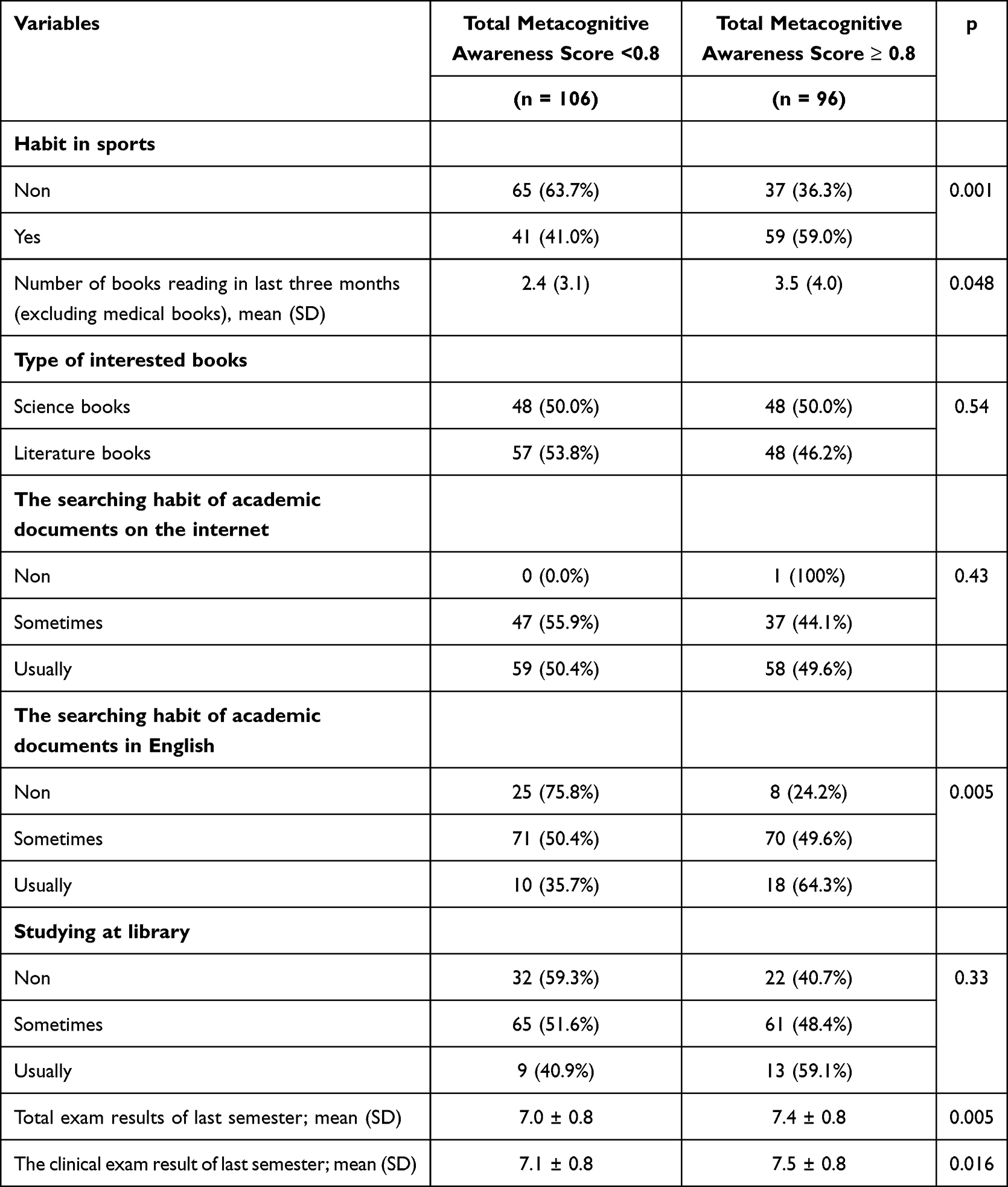 |
Table 5 The Relationship Between Metacognitive Awareness Total Score and Participants’ Habits and Academic Results |
Table 6 showed that a total metacognitive awareness score ≥ 0.8 was relatively significant with military participants, sports, and English academic document searching habits (Table 6).
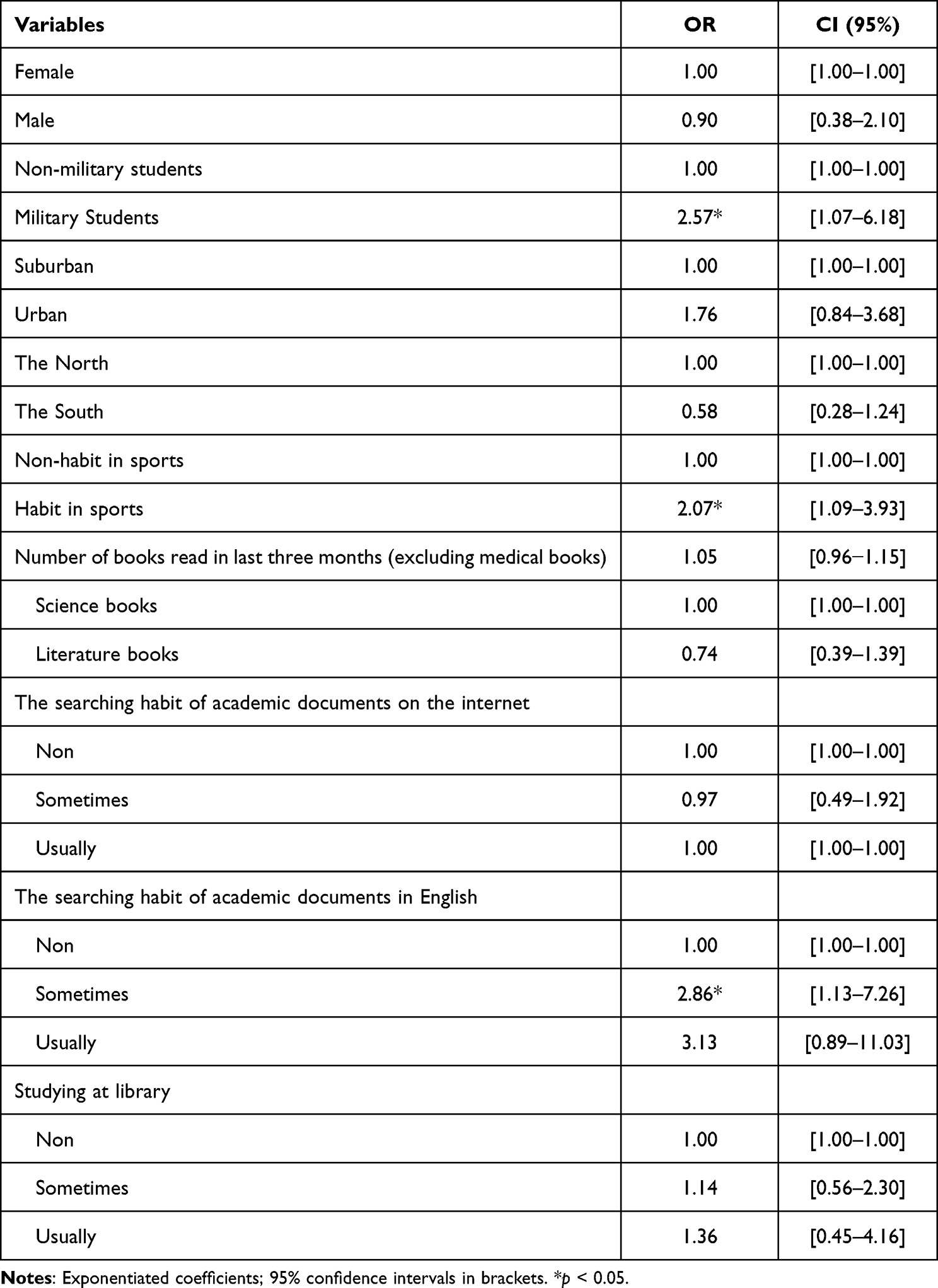 |
Table 6 Multivariable Logistic of Total Metacognitive Awareness Score ≥ 0.8 |
Discussion
Competency-based medical education is the transformation from teaching to self-study, from training to self-training.1,3 Medical students become the center of the educational process. They need to study by themselves to get knowledge and skills according to the competent targets of the curriculum.3,25,26 The ability of students in aware and assess themselves can call the concept of “metacognition”.14,19 Metacognition presents at an early age and increases in ability during the transition from childhood to adolescence.4,10 Metacognition plays an essential role in medical education. Metacognition guides students’ learning strategies during the learning process.20,27,28 The students can focus on acquiring the knowledge or skills they lack if they know what they know and do not know.18,28,29
Our study showed that the median total metacognitive awareness score with 52 questions was 0.8. The median metacognitive knowledge score was 0.7 (17 questions), and the median metacognitive regulation was 0.8 (35 questions). It is exciting that the metacognitive regulation score was more significant than the metacognitive knowledge score. It could be explained that most students were not taught knowledge of metacognition as an independent subject in the curriculum, while metacognitive regulation can be created in learning from childhood in other subjects. Pallavi Panchu et al30 assessed metacognition in 100 first-year medical students in India using by MAI tool and showed that the mean metacognitive knowledge score was 0.645 (10.98/17 questions), the mean metacognitive regulation score was 0.644 (22.55/35 questions). Similar observations are reported by Mishra et al.31 The author showed that the mean metacognitive awareness total score was 0.775 (40.31/52 questions), the mean metacognitive knowledge score was 0.759 (12.91/17 questions), and the mean metacognitive regulation score was 0.78 (27.41/ 35 questions). The value of the MAI score in our observation was equivalent to two previous Indian studies. The results of each component of metacognition in our participants showed that the median declarative knowledge score (0.6) was significantly less than the median procedural knowledge score (0.8). It means that the participants’ awareness of what they know is more complicated than what they can do.
Our results showed that the rate of participants with total metacognitive awareness score ≥ 0.8 was higher in the military than in non-military students (Table 4; p = 0.004). Analyzing another way of comparing the median of the MAI score, the result showed that the military student group had a significantly higher median of the total, knowledge, and regulation scores in metacognition (Table S2). It could be explained that military students study some subjects associated with metacognition in the military curriculum. The rate of participants with a total metacognitive awareness score ≥ 0.8 was the lowest in the fourth academic year. We may suggest that participants begin a clinical study in the fourth academic year, including new knowledge and skill of the clinic. So, they must change their learning methods to deal with clinical objects. Our study did not find any statistical difference in the total metacognitive awareness score between females and males, the living area, and the living regions of participants.
Our results also showed that participants with sports habits and searching for academic documents in English had a higher proportion of total metacognitive awareness score ≥ 0.8 than other participants. The participants with a total metacognitive awareness score of ≥ 0.8 read more books in the last three months than others. Nevertheless, the type of interest books (excluding medical books), the habit of searching academic documents online, and studying at the library were insignificant among participants with a total metacognitive awareness score of ≥ 0.8 and < 0.8. Multivariable logistic analysis results showed three variables, including military students, habits in sports, and searching of English academic documents that significantly affected the rate of participants with total metacognitive awareness score ≥ 0.8. Metacognition is essential in health care, from being a better student to becoming a better doctor.10 So several ways can enhance students’ metacognition in medical school, including lectures, active learning exercises, or pre-planned activities outside of the classroom. Tomporowski reviewed metacognition from previous studies that acute and chronic quantitative exercise affected cognition and metacognition. The quantitative exercise included fitness, physical activity, and sports participation.32 According to this review, we could explain our result that physical activities in sports could encourage cognitive function, including metacognition. Searching for academic documents in English is active action in the learning progress of good students. These students not only study Vietnamese documents in the curriculum but also search for more updated knowledge in English. They had been using more integrated skills and knowledge, including English, computer, information technology, and clinical expertise, to do this job. They usually plan for their work with more detailed jobs to get more and more knowledge and competency in medicine. These students could get better total metacognitive awareness scores. There are detailed competencies of the medical curriculum that all students have to accumulate. Their competencies include science and social compartment. Besides learning from medical documents, they have to learn more soft skills and more knowledge of basic science and society from reading books. It could explain our result that reading more books related to higher total metacognitive awareness scores.
Finally, metacognition with two components (knowledge and regulation) could help students learn, especially in competency-based medical education. Our results showed that participants with a total metacognitive awareness score ≥ 0.8 had significantly higher results in the last semester, including the whole exam and clinical exam. The research of Wei Han Hong on first-year medical students in Malaysia showed that metacognition and its components significantly positively correlated with academic performance results.18 In another study, Chan researched 139 first-year nursing students at a university in Hong Kong. The results showed that total metacognition scores increased significantly after active learning than before.25 Metacognition, including knowledge and regulation, guides the students on what they know and what they do not know but also shows them to get good learning outcomes without mistakes. So they could get better academic performance in the medical course. This previous research could show the relationship between metacognition and students’ academic performance.
Limitation
This study has limitations. The metacognition was measured by MAI score with the native version in English. Therefore, bias could be met when translating into Vietnamese. However, before the study, MAI was translated into Vietnamese by one expert in the English language, and a trial survey was conducted on 32 Vietnamese students to ensure the feasibility and appropriateness of the MAI score for this population. We also strictly followed the instructions described in this test’s manual to make results reliable.
Conclusion
The study showed that medical students at the Vietnamese Military Medical University were likely to have a high metacognitive awareness score. High metacognitive awareness scores might predict higher students’ academic performance. Being military students, playing sports, reading more books, and searching English academic documents could associate better metacognitive awareness scores.
Acknowledgments
We thank the staff in Military Hospital 103, Vietnam Military Medical University for collecting the samples and supporting the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author(s) received no financial support for this article’s research, authorship, and/or publication.
Disclosure
The author(s) declared no potential conflicts of interest to this article’s research, authorship, and/or publication.
References
1. Harris P, Snell L, Talbot M, Harden RM; International CBME Collaborators. Competency-based medical education: implications for undergraduate programs. Med Teach. 2010;32:646–650. doi:10.3109/0142159X.2010.500703
2. Iesa MAM. Medical students’ perception of their education and training to cope with future market trends [retraction]. Adv Med Educ Pract. 2020;11:337–338. doi:10.2147/AMEP.S261451
3. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32:638–645. doi:10.3109/0142159X.2010.501190
4. Colbert CY, Graham L, West C, et al. Teaching metacognitive skills: helping your physician trainees in the quest to ‘know what they don’t know’. Am J Med. 2015;128:318–324. doi:10.1016/j.amjmed.2014.11.001
5. Schraw G. Promoting general metacognitive awareness. Instr Sci. 1998;26:113–125. doi:10.1023/A:1003044231033
6. Beach PT, Anderson RC, Jacovidis JN, Chadwick KL. Making the abstract explicit: the role of metacognition in teaching and learning. Inflexion. 2020;2020:1–57.
7. Fisher M, King J, Tague G. Development of a self-directed learning readiness scale for nursing education. Nurse Educ Today. 2001;21:516–525. doi:10.1054/nedt.2001.0589
8. Mytkowicz P, Goss D, Steinberg B. Assessing metacognition as a learning outcome in a postsecondary strategic learning course. J Postsecond Educ Disabil. 2014;27:51–62.
9. Brown AL. Metacognition, executive control, self-regulation, and other more mysterious mechanisms. Metacognit Motivat Understand. 1987;20:65–116.
10. Medina MS, Castleberry AN, Persky AM. Strategies for improving learner metacognition in health professional education. Am J Pharm Educ. 2017;81:78. doi:10.5688/ajpe81478
11. Deyo ZM, Huynh D, Rochester C, Sturpe DA, Kiser K. Readiness for self-directed learning and academic performance in an abilities laboratory course. Am J Pharm Educ. 2011;75:25. doi:10.5688/ajpe75225
12. Schraw G, Dennison RS. Assessing metacognitive awareness. contemporary educational psychology. Dev Comprehens Learn. 1994;19:460–475.
13. Balcikanli C. Metacognitive awareness inventory for teachers (MAIT). 2011.
14. Bhandari B, Chopra D, Singh K. Self-directed learning: assessment of students’ abilities and their perspective. Adv Physiol Educ. 2020;44:383–386. doi:10.1152/advan.00010.2020
15. Barnard-Brak L, Paton VO, Lan WY. Profiles in self-regulated learning in the online learning environment. Int Rev Res Open Distributed Learn. 2010;11:61–80. doi:10.19173/irrodl.v11i1.769
16. Song JHH, Loyal S, Lond B. Metacognitive Awareness Scale, Domain Specific (MCAS-DS): assessing metacognitive awareness during raven’s progressive matrices. Front Psychol. 2021;11:607577. doi:10.3389/fpsyg.2020.607577
17. Khiat H. Measuring self-directed learning: a diagnostic tool for adult learners. J Univ Teach Learn Pract. 2015;12(2):4–19. doi:10.53761/1.12.2.2
18. Hong WH, Vadivelu J, Daniel EGS, Sim JH. Thinking about thinking: changes in first-year medical students’ metacognition and its relation to performance. Med Educ Online. 2015;20:27561. doi:10.3402/meo.v20.27561
19. Schellenberg S, Negishi M, Eggen P. The effects of metacognition and concrete encoding strategies on depth of understanding in educational psychology. Teach Educ Psychol. 2011;7:17–24.
20. Siqueira MAM, Gonçalves JP, Mendonça VS, et al. Relationship between metacognitive awareness and motivation to learn in medical students. BMC Med Educ. 2020;20:1–10. doi:10.1186/s12909-020-02318-8
21. Premkumar K, Vinod E, Sathishkumar S, et al. Self-directed learning readiness of Indian medical students: a mixed method study. BMC Med Educ. 2018;18:1–10. doi:10.1186/s12909-018-1244-9
22. Elbyaly MYH, Elfeky AIM. The role of metacognition in promoting deep learning in MOOCs during COVID-19 pandemic. Peer J Comput Sci. 2022;8:e945. doi:10.7717/peerj-cs.945
23. Khodaei S, Hasanvand S, Gholami M, Mokhayeri Y, Amini M. The effect of the online flipped classroom on self-directed learning readiness and metacognitive awareness in nursing students during the COVID-19 pandemic BMC. Nursing. 2022;21:22. doi:10.1186/s12912-022-00804-6
24. Hindun I, Husamah H, Nurwidodo N, Fatmawati D, Fauzi A. E-Learning in COVID-19 pandemic: does it challenge teachers’ work cognition and metacognitive awareness? Int J Instruct. 2021;14(3):547–566. doi:10.29333/iji.2021.14332a
25. Chan CWH, Tang FWK, Chow KM, Wong CL. Enhancing generic capabilities and metacognitive awareness of first-year nursing students using active learning strategy. BMC Nurs. 2021;20:1–8. doi:10.1186/s12912-021-00601-7
26. Gutiérrez de Blume AP, Montoya Londoño D. Differences in metacognitive skills among undergraduate students in education, psychology, and medicine. Revista Colombiana de Psicología. 2021;30:111–130. doi:10.15446/rcp.v30n1.88146
27. Cutting MF, Saks NS. Twelve tips for utilizing principles of learning to support medical education. Med Teach. 2012;34:20–24. doi:10.3109/0142159X.2011.558143
28. Tanner KD. Promoting student metacognition. CBE—Life Sci Educ. 2012;11:113–120. doi:10.1187/cbe.12-03-0033
29. Preston R, Gratani M, Owens K, et al. Exploring the impact of assessment on medical students’ learning. Assess Eval High Educ. 2020;45:109–124. doi:10.1080/02602938.2019.1614145
30. Panchu P, Bahuleyan B, Seethalakshmi K, Thomas T. Metacognitive awareness-evaluation and implications in medical students. Int J Res Med Sci. 2016;4:3570–3575. doi:10.18203/2320-6012.ijrms20162331
31. Mishra B. An age and gender-based analysis of ‘Metacognitive Awareness Inventory’ (MCAI) among first-year MBBS students from a Central Indian medical college. J Commun Health Manage. 2019;6:77–81.
32. Tomporowski PD, McCullick B, Pendleton DM, Pesce C. Exercise and children’s cognition: the role of exercise characteristics and a place for metacognition. J Sport Health Sci. 2015;4:47–55. doi:10.1016/j.jshs.2014.09.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.