Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Relationship Between Metabolic Syndrome and Cognitive Function: A Population-Based Study of Middle-Aged and Elderly Adults in Rural China
Authors Zhan C, Wang Q, Liu J ![]() , Wang L, Chen Z, Pang H, Tu J, Ning X, Wang J
, Wang L, Chen Z, Pang H, Tu J, Ning X, Wang J ![]() , Fei S
, Fei S
Received 24 February 2021
Accepted for publication 31 March 2021
Published 30 April 2021 Volume 2021:14 Pages 1927—1935
DOI https://doi.org/10.2147/DMSO.S308250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Changqing Zhan,1 Qiao Wang,2 Jie Liu,3– 5 Lei Wang,1 Zongsheng Chen,1 Hongbo Pang,1 Jun Tu,3– 5 Xianjia Ning,3– 5 Jinghua Wang,3– 5 Shizao Fei1
1Department of Neurology, The Second People’s Hospital of Wuhu, Wuhu, Anhui, People’s Republic of China; 2Department of Pathology, The Second People’s Hospital of Wuhu, Wuhu, Anhui, People’s Republic of China; 3Department of Neurology, Tianjin Medical University General Hospital, Tianjin, 300052, People’s Republic of China; 4Laboratory of Epidemiology, Tianjin Neurological Institute, Tianjin, 300052, People’s Republic of China; 5Tianjin Neurological Institute, Key Laboratory of Post-Neuroinjury Neuro-Repair and Regeneration in Central Nervous System, Ministry of Education and Tianjin City, Tianjin, 300052, People’s Republic of China
Correspondence: Shizao Fei
Department of Neurology, The Second People’s Hospital of Wuhu, 259 Jiuhuazhong Road, Wuhu, 241000, Anhui Province, People’s Republic of China
Tel +86-553-3909017
Fax +86-553-3832545
Email [email protected]
Jinghua Wang
Laboratory of Epidemiology, Tianjin Neurological Institute, Department of Neurology, Tianjin Medical University General Hospital, 154 Anshan Road, Heping District, Tianjin, 300052, People’s Republic of China
Tel +86-22-60817504
Fax +86-22-60817448
Email [email protected]
Introduction: To explore the relationship between metabolic syndrome (MetS) and cognitive impairment in a low-income and low-education population.
Methods: All residents aged ≥ 45 years in a low-income population in Tianjin, China, were eligible to participate in this study. The Mini-Mental State Examination (MMSE) scale was used to conduct a preliminary screening and assessment of the participants’ cognitive statuses. The MMSE components are orientation, registration, attention and calculation, recall, and language.
Results: In this population, the prevalences of MetS and cognitive impairment were 54.1% and 44.5%, respectively. In the overall population, the registration score was 0.105 points lower in the elevated triglycerides (TG) group than in the normal TG group (β, − 0.105; 95% confidence interval [CI]: − 0.201, − 0.010; P=0.030). In men, high TG was associated with registration scores that were 0.152 points lower than those in the normal TG group (95% CI: − 0.281, − 0.022; P=0.022), while larger WC and lower HDL-C had positive effects on cognitive scores (all P< 0.05). However, in women, there were no significant differences between cognitive scores and MetS or its components.
Conclusion: In this population, first, TG had a great impact on cognition, even greater than the impact of MetS on cognition. Second, the impact of MetS components on cognition was more obvious in men, and not all of the effects were negative. Therefore, the effect of MetS on cognition may need to be analyzed separately for different populations, and it may be that the effect of a single component is greater than the overall effect. When formulating prevention strategies for cognitive impairments, population differences must also be taken into consideration.
Keywords: cognitive impairment, MMSE, metabolic syndrome, aging, population-based study
Introduction
The burden of dementia is huge for society and individuals. It is estimated that there were 43.8 million people with dementia worldwide in 2016, with numbers expected to increase to 100 million by 2050.1 China has 165.58 million people aged 65 years and older, accounting for 12.6% of the total population,2 far exceeding the aging society definition of the United Nations.3 Thus, the burden of dementia may be heavier in China than in other parts of the world. As the early stage of dementia, cognitive impairment has been considered the main intervention stage for preventing dementia. A recent study reported that the prevalence of mild cognitive impairment in China exceeded 15.5%, representing 38.77 million people nationwide.4 Moreover, compared with that in urban areas, the burden of cognitive impairment in rural areas of China is heavier.5 Thus, it is necessary to observe, identify, and manage more closely cognitive dysfunction and its potential risk factors in residents of rural China.
Old age, sex, and genetic factors have been shown to be non–modifiable risk factors for cognitive impairment.6–8 Previous studies have also shown that hypertension, diabetes, and hyperlipidemia were independent risk factors for cognitive impairment.9–11 As a clinical syndrome, metabolic syndrome (MetS) is a combination of metabolic risk factors, and its impact on cognition has recently attracted more and more attention. However, the impact of MetS on cognition is currently controversial. Some studies have indicated that MetS was an independent risk factor for cognitive impairment,12–14 while other studies reported that there were no significant relationships between MetS and global cognitive function, especially in low-income people.15,16 Therefore, this study’s purpose was to explore the associations between MetS and its components with cognition among low-income adults in Northern China.
Methods
Participants and Study Design
This study was a cross-sectional survey conducted between April 2014 and January 2015 in 18 rural administrative villages in Tianjin, China. The population enrolled in this study was a sub-cohort of the Tianjin Brain Study.17 Briefly, approximately 95% of the individuals in this study were low-income farmers with low educational attainment and with a 2014 disposable per capita income of <1600 USD.18 All residents aged ≥45 years without previous histories of dementia or mental disease were invited to participate in the study.
Information Collection and Risk Factor Definition
A pre-designed questionnaire was used to collect participants’ information by uniformly trained investigators through face-to-face interviews. Demographic information included sex, age, educational level, and history of disease. Cognitive function was assessed with the Chinese version of the Mini-Mental State Examination (MMSE).
Each participant underwent a physical examination to determine blood pressure, height, and weight; body mass index (BMI) was calculated as the individual’s weight (kg) divided by the square of the individual’s height (m2). Serum fasting blood glucose (FBG), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) concentrations were measured.
Definition of Variables
Hypertension was defined as a history of hypertension, systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg, or taking antihypertensive drugs.19 Diabetes mellitus (DM) was defined as FBG ≥7.0 mmol/L or 2-hour postprandial glucose (2h-PG) ≥11.1 mmol/L, a previous diagnosis of DM, or having a prescription for insulin or oral antidiabetic drugs.20
BMI was classified into the following groups: low weight, BMI <18.5 kg/m2; normal weight, BMI 18.5–23.9 kg/m2; overweight, BMI 24.0–27.9 kg/m2; and obese, BMI ≥28.0 kg/m2).21
MetS was defined by the presence of three or more of the following criteria: (1) waist circumference (WC) ≥90 cm for men and ≥80 cm for women; (2) TG ≥1.7 mmol/L (150 mg/dL) (hypertriglyceridemia) or using medications for hypertriglyceridemia; (3) HDL-C <1.03 mmol/L for men, HDL-C <1.30 mmol/L for women, or using medications to reduce HDL–C; (4) SBP ≥130 mmHg or DBP ≥85 mmHg (hypertension) or using antihypertensive medications; and (5) FBG ≥5.6 mmol/L (hyperglycemia) or using antidiabetic medications.22 Cognitive impairment was defined by MMSE scores <17 for the group with no formal education, <22 for the group with 1–6 years of education, and <26 for the group with >6 years of education.23 According to the definition of MetS components, participants’ TG, FBG, HDL-C, blood pressure, and WC values were defined as normal or elevated.
The participants were grouped into two age categories: <65 years and ≥65 years. Participants were also classified into three groups on the basis of length of formal education: the group with no formal education (0 years), 1–6 years, and >6 years. Cigarette smoking was defined as smoking more than 1 cigarette/day for ≥1 year; participants were categorized as non-smokers, current smokers, or previous smokers. Alcohol consumption was defined as drinking >500 g of alcohol/week for ≥1 year; participants were categorized as non-drinkers, past drinkers, or current drinkers.24
Statistical Analyses
Continuous variables, including age, educational level, BMI, SBP, DBP, WC, FBG, TC, TG, HDL-C, and LDL-C, were presented as means and standard deviations (SDs). Continuous variables were analyzed using Student’s t-tests. MMSE scores were presented as medians and interquartile ranges (IQs). Categorical variables, including age group, BMI group, educational level group, smoking status, alcohol consumption, hypertension, DM, and MetS and its components, were counted as numbers and frequencies, and between-group comparisons were performed using chi-squared tests.
Multiple linear regression analyses were used to evaluate the associations between MMSE scores with MetS and its components (ie, orientation, registration, attention and calculation, recall, and language). The relationships were presented as standard partial regression coefficients (β) with 95% confidence intervals (CIs). Multiple linear regression analyses were run for each MetS component by age group adjusted for age, education level, smoking status, and the other four MetS components.
All analyses were conducted using SPSS for Windows (version 25.0; SPSS Inc., Chicago, IL, USA). Reported probabilities were two-sided; all tests were set at the 0.05 level of statistical significance.
Results
Participant Characteristics
This study recruited 1286 individuals aged ≥50 years (mean age, 66.84 years), including 595 men (46.3%) and 691 women (53.7%). The average number of years of education in this study population was 4.15 years. Moreover, 27.8% of participants (8.1% of men and 44.7% of women) had not received any formal education. The prevalences of MetS, cognitive impairment, hypertension, DM, and obesity were 54.1%, 44.5%, 80.0%, 29.8%, and 17.9%, respectively. The prevalences of current smoking and current alcohol consumption were 26.4% and 22.6%, respectively. Moreover, the median MMSE score (22) was low in this population (Table 1).
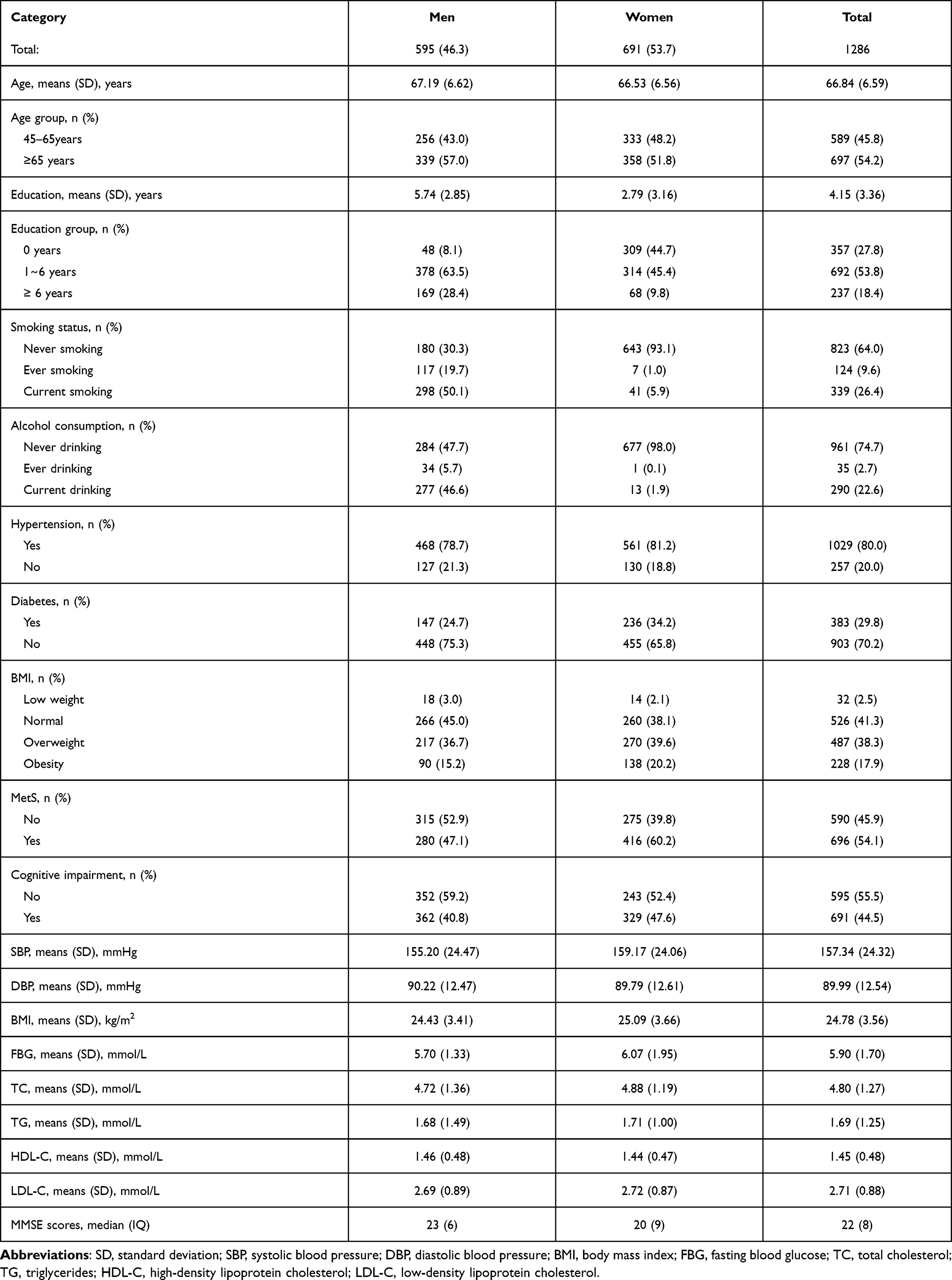 |
Table 1 Characteristics of Demography Among All Participants in This Study |
The Effects of MetS and Its Components on Cognition
Table 2 shows that there were no significant differences between participants with and without MetS in the median scores for total MMSE, orientation, registration, attention and calculation, recall, and language (all P>0.05).
 |
Table 2 The Difference in Cognitive Scores in the Different MetS Groups Under the Age Stratification |
This study also compared the prevalences of MetS and its components in the cognitively impaired group with those in the cognitively normal group. There were no significant relationships between MetS and cognitive status (P=0.962). However, the prevalence of high TG was higher in the normal cognitive status group than in the cognitive impairment group (51.6% vs 48.4%, P=0.032). In the age <65 years group, the prevalence of MetS was higher in the group with cognitive impairment than in the normal cognition group (56.3% vs 49.1%, P=0.170). Additionally, in the age ≥65 years group, the prevalence of MetS was lower in the cognitive impairment group than in the normal cognition group (52.7% vs 60.3%, P=0.266). There were no significant differences between the cognitive impairment group and the normal cognition group in the prevalences of MetS components (all P>0.05) (Table 3).
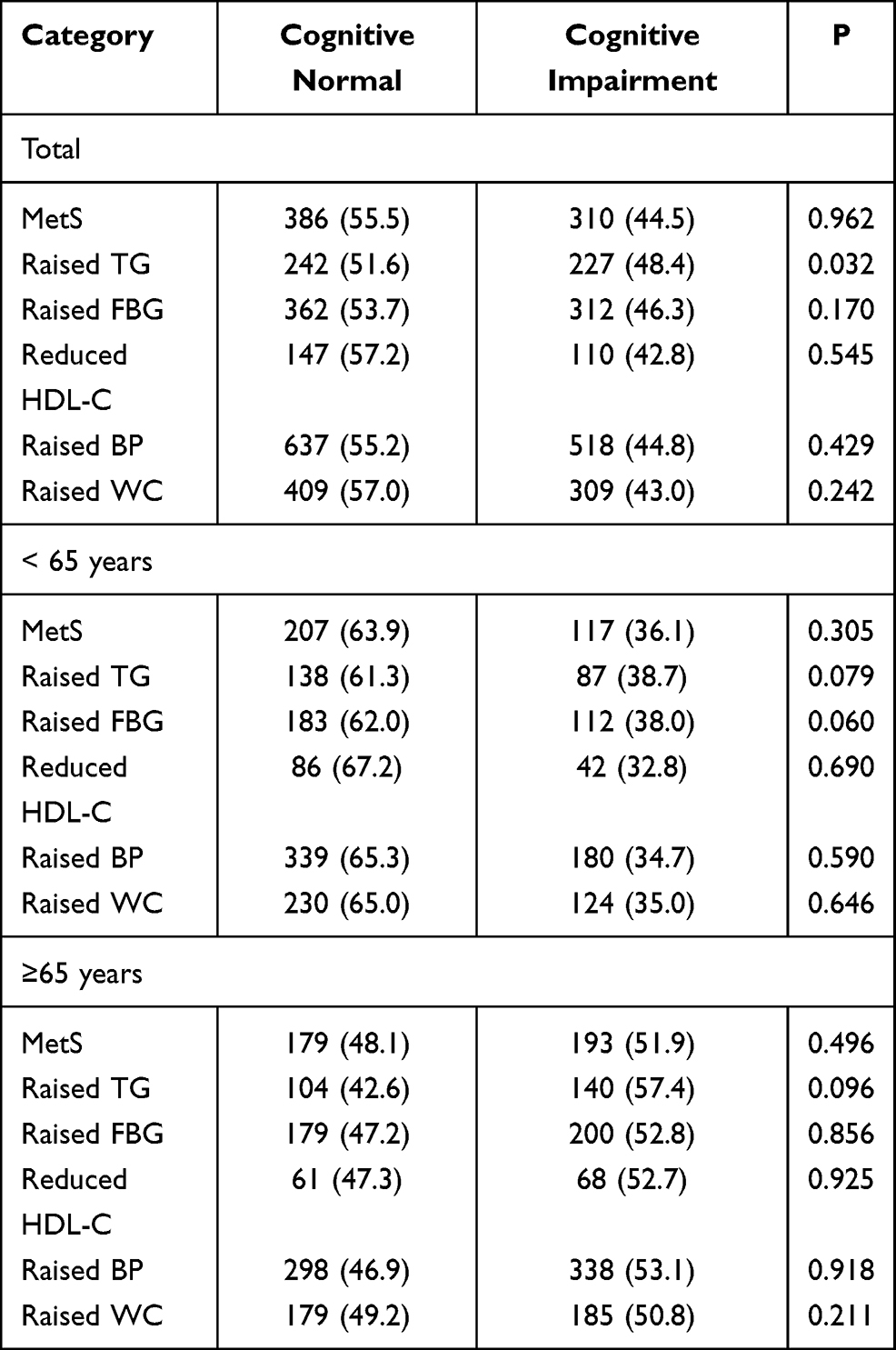 |
Table 3 The Prevalence of Metabolic Syndrome and Its Components in Different Cognitive Function |
Influence of MetS and Its Components on Cognitive Scores in the Multivariate Analysis
In the overall population, there were no significant associations between MetS components and cognitive status after adjusting for age, education level, smoking history, and the other four MetS components (P>0.05). The registration score was 0.105 points lower in the elevated TG group than in the normal TG group (β, −0.105; 95% CI: −0.201, −0.010; P=0.030), while there were no correlations between other MetS components and cognitive status (all P>0.05).
Among men in the study population, compared with those in the normal TG group, the registration scores in the elevated TG group were 0.152 points lower (95% CI: −0.281, −0.022; P=0.022). The orientation scores and language scores were 0.228 points (95% CI: 0.023, 0.433; P=0.029) and 0.331 points (95% CI: 0.061, 0.600; P=0.016) higher, respectively, in the elevated WC group than in the normal WC group. The attention and calculation score was 0.480 points (95% CI: 0.083, 0.878; P=0.018) lower in the decreased HDL group than in the normal HDL group.
However, in women, there were no significant relationships between cognitive status and MetS and its components (all P>0.05) (Table 4).
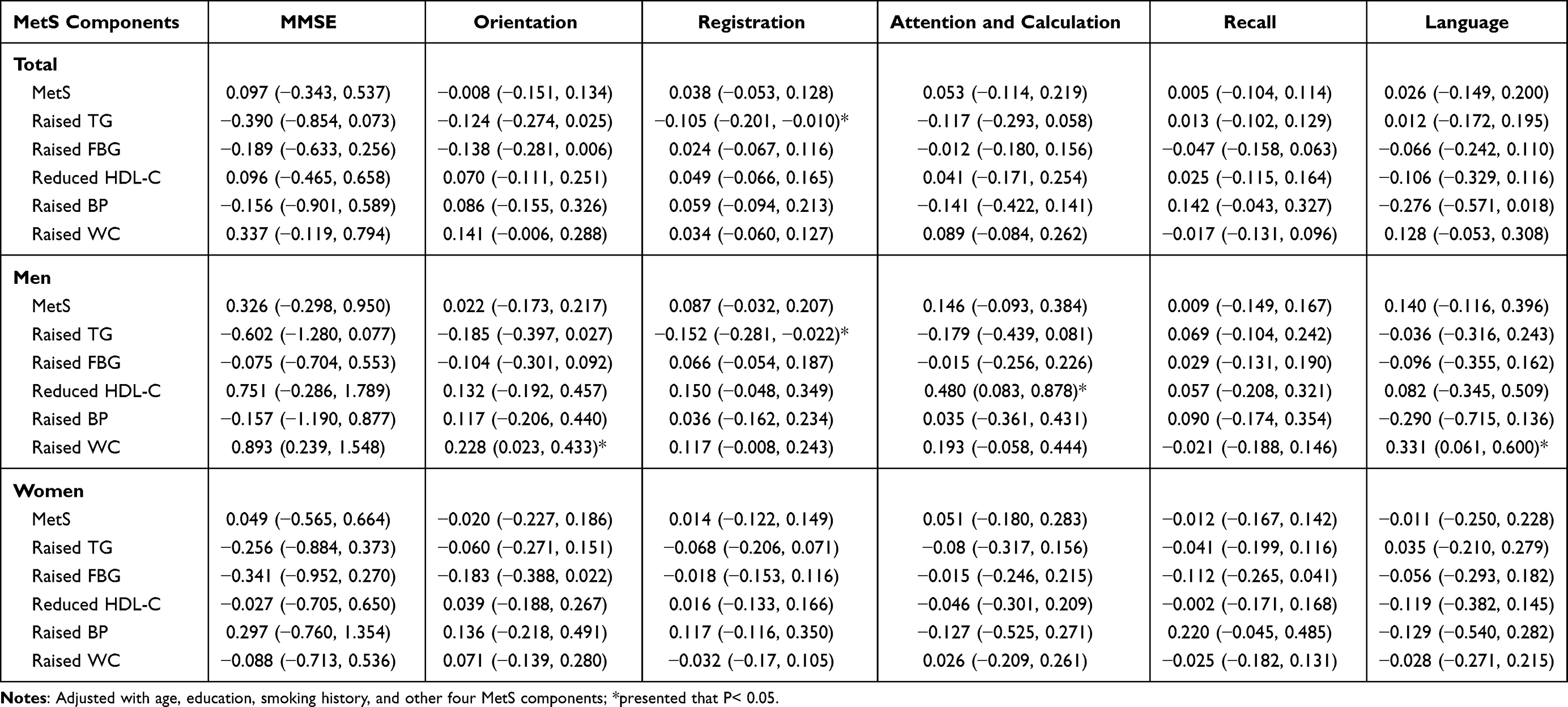 |
Table 4 MMSE Score in Metabolic Syndrome and Its Components Using Multivariate Regression Analysis [β (95% CI)] |
Discussion
This population-based study aimed to explore the associations between MetS components and cognitive function among adults aged ≥45 years in rural Northern China. In this study, the prevalences of MetS and cognitive impairment were 54.1% and 44.5%, respectively. In the overall population, there was a significant negative relationship between high TG and registration. In men, registration scores were significantly lower in the elevated TG population than in the normal TG group, while there was a positive relationship between cognitive status and lower HDL and elevated WC. In women, there was no significant association between MetS and its components with cognitive status.
The impact of MetS on cognitive impairment remains controversial. A Korean study of elderly people over age 65 years pointed out that MetS was an independent risk factor for cognitive impairment.14 A systematic review of prospective population-based studies reported that, compared with individuals without MetS, the risk of cognitive decline was increased 1- to 2-fold in patients with MetS.25 A study in Northeast China also reported that MetS was inversely associated with cognitive function.26 Another study reported that the prevalence of MetS exceeded 50% among Australians with severe mental illness.27 Meanwhile, a recent study also reported that patients with first-episode psychosis and those with schizophrenia had an increased prevalence of MetS.28 However, there have also been some studies that reported no significant association between global cognitive function and MetS.15,16 In this study, MetS had no effect on global cognition status in the overall population. The mechanism for this relationship is not clear, but it may be related to the nutritional and metabolic status of the population. Perhaps in low–income people, nutritional status has a greater impact on cognition, and metabolic syndrome does not reflect the nutritional status of this population well.
The obesity paradox has attracted increasingly more attention. Although obesity is a risk factor for many diseases,29,30 with respect to tumors, cardiovascular disease, and the entire life course, the impact of obesity on health cannot be generalized.31–33 In this study, large WC, as an indicator of abdominal obesity, had a significant positive relationship with registration and language scores. The possible mechanism may be that the relationship between obesity and disease is not only dependent on adiposity but also on endocrine function and adipocyte leptin secretion.34 Therefore, some low-leptin lifestyles independent of obesity (such as health status) may confuse the relationship between obesity and disease. Moreover, an important factor is the development of frailty, which was not considered in the relationship between obesity and disease.31 The average age of this population was older, and the overall population may be more fragile, so the increase in WC may indicate a better nutritional status.
There was a significant negative correlation between high TG and memory score, especially in men, in this study. This is consistent with previous research results. A previous study reported that MMSE scores for men were significantly negatively correlated with TG.15 Another follow-up study also reported that high TG was associated with deterioration in memory and learning ability.13
In this study, MetS and its components had different effects on cognitive function in different age groups. A previous study reported that the prognostic role of the overall MetS score in the elderly was not greater than the sum of its components.35 Moreover, age seems to change the association between MetS and cognitive decline.12 Thus, it is necessary to explore the relationship between MetS and cognition in all age groups.
The score for attention and calculation was higher in the reduced HDL-C group than in the normal HDL-C group, which is contrary to previous research results. HDL-C has always been considered good cholesterol.36 A recent study showed that white matter volume was positively correlated with HDL-C levels, suggesting that elevated that HDL-C levels have a positive effect on brain cognitive function.37 Although a previous study reported that there may be a U-shaped relationship between HDL-C and cardiovascular disease,38 there is no evidence that reduced HDL-C protects cognition. In this study, the mechanism of the positive correlation between reduced HDL-C and cognition is unclear, but it is possible that the quality of HDL-C may be more important than its quantity, because HDL-C loses its antioxidant effect because of changes in its composition, which may reduce the predictive ability of HDL-C.36
There were several limitations in this study. First, an inherent limitation of a cross-sectional study is that it cannot validate causal links between significant variables and MMSE score; thus, further longitudinal studies are needed to determine causality. Second, in this study, the MMSE scale was used to assess the cognitive function of the participants. Because the MMSE scale is so simple, it is easy to miss impaired cognitive function in patients with higher educational levels. However, the research population in this study was a low-income population with low educational attainment; the average education length was 4.15 years. Thus, the assessment of cognitive impairment was likely more accurate. Third, this study did not distinguish the causes of cognitive impairment. In a follow-up study, the scope of information collection of the participants will be expanded, and a deeper analysis of different types of cognitive impairment will be done. Finally, this study did not collect relevant information to assess the frailty of participants; however, age adjustment and the exclusion of participants with severe cardiovascular and cerebrovascular diseases and who are unable to take care of themselves were also excluded. Thus, the influence of frailty on the results can be decreased to a certain extent.
Conclusions
In this study, the prevalence of cognitive impairment was as high as 44.5% among middle-aged and elderly adults, suggesting that the burden of cognitive impairment for people in low-income areas remains heavy in rural Tianjin. Elevated TG was associated with reduced cognitive scores in overall population. Moreover, larger WC and lower HDL-C was associated with increased cognitive scores in men, while there were no significant differences between MetS and cognitive scores in women. Therefore, the influence of MetS on cognition cannot be generalized and must be based on a specific analysis of different populations. When formulating prevention strategies for related cognitive impairments, population differences must also be taken into consideration.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Tianjin Medical University General Hospital; all participants received information on the study and provided written informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We thank all participants of the Tianjin Brain Study, and local medical care professionals for their valuable contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests.
References
1. Nichols E, Szoeke CEI, Vollset SE, GBD 2016 Dementia Collaborators. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(1):88–106. doi:10.1016/S1474-4422(18)30403-4
2. Statistics NBo. China statistical yearbook. Avaialble from: http://www.stats.gov.cn/tjsj/ndsj/2020/indexch.htm.
3. Pichat B. The Aging of Population and Its Economic and Social Implication. International Affairs.1958;34(4):528.
4. Jia L, Du Y, Chu L, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. 2020;5(12):e661–e671. doi:10.1016/S2468-2667(20)30185-7
5. Jia J, Wang F, Wei C, et al. The prevalence of dementia in urban and rural areas of China. Alzheimers Dement. 2014;10(1):1–9. doi:10.1016/j.jalz.2013.01.012
6. Wang J, Xiao LD, Wang K, Luo Y, Li X. Cognitive impairment and associated factors in rural elderly in North China. J Alzheimers Dis. 2020;77(3):1241–1253. doi:10.3233/JAD-200404
7. Wang J, Xiao LD, Wang K, Luo Y, Li X. Gender differences in cognitive impairment among rural elderly in China. Int J Environ Res Public Health. 2020;17(10). doi:10.3390/ijerph17103724
8. Jia L, Quan M, Fu Y, et al. Dementia in China: epidemiology, clinical management, and research advances. Lancet Neurol. 2020;19(1):81–92. doi:10.1016/S1474-4422(19)30290-X
9. Ferguson AC, Tank R, Lyall LM, et al. Association of SBP and BMI with cognitive and structural brain phenotypes in UK Biobank. J Hypertens. 2020;38(12):2482–2489. doi:10.1097/HJH.0000000000002579
10. Cukierman T, Gerstein HC, Williamson JD. Cognitive decline and dementia in diabetes–systematic overview of prospective observational studies. Diabetologia. 2005;48(12):2460–2469. doi:10.1007/s00125-005-0023-4
11. Shi L, Cheng Y, Xu Y, et al. Effects of hypertension on cerebral cortical thickness alterations in patients with type 2 diabetes. Diabetes Res Clin Pract. 2019;157:107872. doi:10.1016/j.diabres.2019.107872
12. Siervo M, Harrison SL, Jagger C, Robinson L, Stephan BC. Metabolic syndrome and longitudinal changes in cognitive function: a systematic review and meta-analysis. J Alzheimers Dis. 2014;41(1):151–161. doi:10.3233/JAD-132279
13. Przybycien-Gaweda PM, Gwee X, Gao Q, Chua D, Fam J, Ng TP. Metabolic syndrome and cognition: follow-up study of chinese over-55-year-olds. Dement Geriatr Cogn Disord. 2020;49(2):129–137. doi:10.1159/000509124
14. Lee EY, Lee SJ, Kim KM, et al. Association of metabolic syndrome and 25-hydroxyvitamin D with cognitive impairment among elderly Koreans. Geriatr Gerontol Int. 2017;17(7):1069–1075. doi:10.1111/ggi.12826
15. Buyo M, Takahashi S, Iwahara A, et al. Metabolic syndrome and cognitive function: cross-sectional study on community-dwelling non-demented older adults in Japan. J Nutr Health Aging. 2020;24(8):878–882. doi:10.1007/s12603-020-1412-6
16. Kazlauskaite R, Janssen I, Wilson RS, et al. Is midlife metabolic syndrome associated with cognitive function change? The study of women’s health across the nation. J Clin Endocrinol Metab. 2020;105(4). doi:10.1210/clinem/dgaa067.
17. Wang J, Ning X, Yang L, et al. Sex differences in trends of incidence and mortality of first-ever stroke in rural Tianjin, China, from 1992 to 2012. Stroke. 2014;45(6):1626–1631. doi:10.1161/STROKEAHA.113.003899
18. Administration NHS. Statistical bulletin on healthcare security 2014. Avaialble from: http://www.nhsa.gov.cn/art/2019/.
19. Williams B, Mancia G, Spiering W, et al. [2018 ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH)]. G Ital Cardiol (Rome). 2018;19(11 Suppl 1):3S–73S. Italian. doi:10.1714/3026.30245
20. Association DbotCM. China Guidelines for Type II Diabetes Mellitus. Beijing: Peking University Medical Press; 2011.
21. Wang J, Taylor AW, Zhang T, Appleton S, Shi Z. Association between body mass index and all-cause mortality among oldest old Chinese. J Nutr Health Aging. 2018;22(2):262–268. doi:10.1007/s12603-017-0907-2
22. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
23. Nunes B, Silva RD, Cruz VT, Roriz JM, Pais J, Silva MC. Prevalence and pattern of cognitive impairment in rural and urban populations from Northern Portugal. BMC Neurol. 2010;10:42. doi:10.1186/1471-2377-10-42
24. Liu B, Ni J, Shi M, et al. Carotid intima-media thickness and its association with conventional risk factors in low-income adults: a Population-based Cross-Sectional Study in China. Sci Rep. 2017;7:41500. doi:10.1038/srep41500
25. Hao Z, Wu B, Wang D, Liu M. Association between metabolic syndrome and cognitive decline: a systematic review of prospective population-based studies. Acta Neuropsychiatr. 2011;23(2):69–74. doi:10.1111/j.1601-5215.2011.00527.x
26. Wang X, Luan D, Xin S, Liu Y, Gao Q. Association between individual components of metabolic syndrome and cognitive function in Northeast Rural China. Am J Alzheimers Dis Other Demen. 2019;34(7–8):507–512. doi:10.1177/1533317519865428
27. John AP, Koloth R, Dragovic M, Lim SC. Prevalence of metabolic syndrome among Australians with severe mental illness. Med J Aust. 2009;190(4):176–179. doi:10.5694/j.1326-5377.2009.tb02342.x
28. Sahpolat M, Ari M. Higher prevalence of metabolic syndrome and related factors in patients with first-episode psychosis and schizophrenia: a cross-sectional study in Turkey. Nord J Psychiatry. 2021;75(1):73–78. doi:10.1080/08039488.2020.1815080
29. Li X, Wu C, Lu J, et al. Cardiovascular risk factors in China: a nationwide population-based cohort study. Lancet Public Health. 2020;5(12):e672–e681. doi:10.1016/S2468-2667(20)30191-2
30. Mourmoura E, Rigaudière JP, Couturier K, et al. Long-term abdominal adiposity activates several parameters of cardiac energy function. J Physiol Biochem. 2016;72(3):525–537. doi:10.1007/s13105-015-0427-7
31. Strandberg TE, Strandberg AY. Life course explains the ‘obesity paradox’. Eur Heart J. 2020;41(40):3963–3964. doi:10.1093/eurheartj/ehaa717
32. Lee SY, Kim HL, Kim MA, et al. Obesity paradox in Korean male and female patients with heart failure: a report from the Korean Heart Failure Registry. Int J Cardiol. 2020. doi:10.1016/j.ijcard.2020.10.013
33. Gallo M, Adinolfi V, Barucca V, et al. Expected and paradoxical effects of obesity on cancer treatment response. Rev Endocr Metab Disord. 2020. doi:10.1007/s11154-020-09597-y
34. Nicholson E, Allison DJ, Bullock A, Heisz JJ. Examining the obesity paradox: a moderating effect of fitness on adipose endocrine function in older adults. Mech Ageing Dev. 2020;193:111406. doi:10.1016/j.mad.2020.111406
35. Mazza A, Pessina AC, Zamboni S, Casiglia E. Prognostic role of metabolic syndrome in the elderly is not greater than the sum of its components. Aging Health. 2010;6(2):217–228. doi:10.2217/ahe.10.9
36. Ito F, Ito T. High-Density Lipoprotein (HDL) Triglyceride and Oxidized HDL: new lipid biomarkers of lipoprotein-related atherosclerotic cardiovascular disease. Antioxidants (Basel). 2020;9(5). doi:10.3390/antiox9050362
37. Livingston JM, McDonald MW, Gagnon T, et al. Influence of metabolic syndrome on cerebral perfusion and cognition. Neurobiol Dis. 2020;137:104756. doi:10.1016/j.nbd.2020.104756
38. Feng M, Darabi M, Tubeuf E, et al. Free cholesterol transfer to high-density lipoprotein (HDL) upon triglyceride lipolysis underlies the U-shape relationship between HDL–cholesterol and cardiovascular disease. Eur J Prev Cardiol. 2020;27(15):1606–1616. doi:10.1177/2047487319894114
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.