Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Relationship Between Maternal Serum Cortisol and Maternal Insulin Resistance and Fetal Ultrasound Characteristics in Gestational Diabetes Mellitus
Authors Tien Nguyen S ![]() , Bui Minh T, Trung Dinh H
, Bui Minh T, Trung Dinh H ![]() , Dinh Le T
, Dinh Le T ![]() , Phi Thi Nguyen N, Tran TTH
, Phi Thi Nguyen N, Tran TTH ![]() , Hien Vu T, Luong Cong T, Ho Thi Nguyen L, Tuan Pham P, Viet Tran T, Xuan Nguyen K
, Hien Vu T, Luong Cong T, Ho Thi Nguyen L, Tuan Pham P, Viet Tran T, Xuan Nguyen K ![]()
Received 10 December 2022
Accepted for publication 27 January 2023
Published 8 February 2023 Volume 2023:16 Pages 365—372
DOI https://doi.org/10.2147/DMSO.S400995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Son Tien Nguyen,1,* Tien Bui Minh,2,* Hoa Trung Dinh,3,4 Tuan Dinh Le,1 Nga Phi Thi Nguyen,1 Thi Thanh Hoa Tran,3 Trinh Hien Vu,3 Thuc Luong Cong,5 Lan Ho Thi Nguyen,3 Phuong Tuan Pham,3,4 Tien Viet Tran,6 Kien Xuan Nguyen7
1Department of Rheumatology and Endocrinology, Military Hospital 103, Vietnam Military Medical University, Ha Noi, Vietnam; 2Department of Obstetrics and Gynecology, Thai Binh University of Medicine and Pharmacy, Thai Binh, Vietnam; 3Department of Requested Treatment, National Hospital of Endocrinology, Ha Noi, Vietnam; 4National Hospital of Endocrinology, Ha Noi, Vietnam; 5Cardiovascular Center, Military Hospital 103, Vietnam Medical Military University, Ha Noi, Vietnam; 6Department of Infectious Diseases, Military Hospital 103, Vietnam Medical Military University, Hanoi, 10000, Vietnam; 7Department of Military Medical Command and Organization, Vietnam Medical Military University, Ha Noi, Vietnam
*These authors contributed equally to this work
Correspondence: Kien Xuan Nguyen, Department of Military Medical Command and Organization, Vietnam Military Medical University, 160 Phung Hung Street, Phuc La Ward, Ha Dong District, Hanoi city, Vietnam, Email [email protected]
Introduction: Cortisol is proven to play a crucial role in hyperglycemia and fetal development in gestational diabetes mellitus (GDM). This research aims to investigate the relationship between maternal serum cortisol and insulin resistance indices and fetal ultrasound characteristics in women with GDM.
Methods: A cross-sectional and descriptive study on 144 GDM in Vietnam from January 2015 to December 2020. Serum cortisol was measured using electrochemiluminescence immunoassay at 8 a.m. on the examination day in the vicinity of the 24th gestational week. Fetal ultrasound was performed by an experienced person who was blind to the study.
Results: The mean cortisol level in the GDM group was 627.04 nmol/L. Serum cortisol levels positively correlated with abdominal circumference (AC), fasting plasma glucose (FPG), insulin, triglycerides, HOMA2-IR, and Mathew indices (with r of 0.18, 0.22, 0.18, 0.17, 0.18, and 0.22, respectively). Serum cortisol levels negatively correlated with QUICKI and McAuley indices (with r of − 0.19 and − 0.21), respectively. In a univariate linear regression, maternal serum cortisol positively correlated with fetal AC, head circumference (HC), and biparietal diameter (BPD) (with r of 0.21; 0.23; and 0.25, respectively). In a multivariate linear regression analysis, cortisol positively correlated with fetal AC, HC, and BPD after adjusting to maternal McAuley index.
Conclusion: Serum cortisol levels in GDM correlated with fasting blood glucose, triglycerides, and insulin resistance. Besides, serum cortisol levels in GDM positively correlated with fetal development.
Keywords: gestational diabetes mellitus, serum cortisol, insulin resistance indices, fetal ultrasound parameters
Introduction
Elevated cortisol affects both mother and fetus during pregnancy.1–3 Cortisol involves in lipid metabolism and distribution in the body. High level of serum cortisol leads to central lipid accumulation, resulting in insulin resistance.4 Besides, maternal serum cortisol levels affect not only the mother but fetal development as well. Changes in cortisol levels during pregnancy remain unclear in pregnancy. In a study by Lynn et al, cortisol elevated in the setting of anxiety in pregnant women with both depressive and anxiety disorders.5 Many studies have shown that high maternal blood cortisol levels affect the fetus directly (increasing caloric consumption and positively upregulating fetal corticotropin-releasing hormone (CRH)) and indirectly through activation of the fetal hypothalamus-pituitary-adrenal (HPA) axis. The consequence of this process leads to increased fetal calorie consumption.6 Some studies outlined that maternal cortisol levels affect fetal development, such as the effect on fetal weight-for-age development in the first trimester7 and the third-trimester cortisol levels related to an increase in neonatal adiposity up to 1–6 months postpartum.8 A study by Braithwaite et al of 1233 first-time mothers (96.1% White British) at 32 weeks gestation found that maternal cortisol levels were positively related to male infant’ postpartum weight with β of 0.167 and p of 0.0369. However, pregnancy cortisol levels differ between races. The levels was found to be abnormally low in a group of African American women by John et al.10 Moreover, serum cortisol levels are strongly associated with central obesity.11 South Asians have a high percentage of body fat,12 therefore, cortisol levels may differ from other races.
GDM is on the rise worldwide.13 GDM affects fetal development and increases the risk of developing obesity, diabetes, and other metabolic cardiovascular diseases in the fetus14 as a result of multiple factors.15 In women with GDM, the mechanism of insulin resistance is unclear; however, high cortisol levels contribute to insulin resistance,16 and cortisol levels fluctuate.17 Nevertheless, the effects of cortisol on the fetus are unclear in GDM. In GDM, there is a decrease in 5 alpha-reductase activity, a downregulation of placental 11 beta-hydroxysteroid dehydrogenases-2 and an upregulation in placental 11 beta-hydroxysteroid dehydrogenases-2 at both mRNA and protein levels and metabolic function compared with normal pregnancy.18,19 Most studies on cortisol levels and the relationship with fetal changes in pregnancy focus on postpartum children.8,20 Abnormalities in the fetus can be easily assessed by fetal ultrasound during pregnancy, which is valuable in prognosis and later treatment instructions. However, the effects of cortisol on fetal development in GDM have been unclear, with the impacts of GDM on the fetus being different from the normal glucose-tolerant pregnant women.
To the best of our knowledge, there has been a lack of studies regarding maternal cortisol and insulin resistance, and fetal growth characteristics. We conducted this study to investigate the relationship of maternal cortisol with maternal insulin resistance indices and some fetal ultrasound characteristics in Vietnamese women with GDM.
Materials and Methods
Study Population and Design
A cross-sectional and descriptive study was conducted on 144 first-time diagnosed GDM who visited the Department of Examination of the National Hospital of Endocrinology, Vietnam, from January 2015 to December 2020.
The selection criterion was GDM from 24 to 28 weeks of gestation. Exclusion criteria were pregnant women diagnosed with diabetes before pregnancy (type 2 diabetes, type 1 diabetes, and other specific types of diabetes), earlier than 24 weeks of gestation, and with uncontrolled chronic medical conditions (bronchial asthma, impaired renal function, impaired liver function), or ongoingly prescribed with glucocorticoids.
Clinical and Biochemical Assessments
GDM participants were tested clinically and biomedically. Clinical examination and blood collection were conducted conveniently and quickly to minimize patient stress. The participants were asked and examined about pregnancy history, medical history, and family history. Clinical criteria assessed include BMI, waist circumference, and systolic blood pressure. At 8 a.m. (fasting), 5 mL of blood was aspirated for testing, including serum cortisol, FPG, HbA1c, insulin, C-peptide, and lipid profiles. Serum cortisol was measured using an electrochemiluminescence immunoassay. From these values, we calculated the HOMA2-IR, QUICKI, Mathew, and McAuley indices as described in the previous studies.21 According to WHO guidelines, the oral glucose tolerance test with 75 grams of anhydrous glucose (OGTT) was performed on the same day of the clinical visit). Serum glucose was assessed at three-time points, including fasting (8 a.m.), 1 hour, and 2 hours afterward.
According to the American College of Radiology guidelines,22 a fetal ultrasound was performed using a 3–5 MHz transducer at the same time as the clinical examination. An experienced fetal sonographer performed a fetal ultrasound entirely unrelated to the study. Measured parameters include head circumference, abdominal circumference, biparietal diameter, amniotic fluid index, and estimated fetal weight.
Ethical Statement
All participants provided written informed consent and agreed to join our study. The study protocol was approved by the Institutional Review Board of the Thai Binh University of Medicine and Pharmacy (decision no.1262/HĐĐĐ). The study was also conducted using good clinical practice following the Declaration of Helsinki.
Statistical Analysis
Data were expressed as mean (standard deviation), median (Q1-Q3), and percentage. Pearson correlation was employed to measure correlations between serum cortisol and maternal biochemical parameters (abdominal circumference, FPG, insulin, triglyceride, QUICKI, HOMA2-IR, Mathew, and McAuley indices) and fetal ultrasonography parameters such as AC, HC, BDP, amniotic fluid index (AFI), and estimated fetal weight (EFW). Multivariate linear regression was employed to analyze the correlation between maternal cortisol and insulin resistance, and fetal ultrasound characteristics. A P < 0.05 was set as significance. All data were processed with SPSS 26.0.
Results
The mean cortisol level in the GDM was 627.04 nmol/L, with high BMI (25.65±3.6 kg/m2), 1-hour OGTT (10.52±1.26 mmol/L) and 2-hour OGTT (9.17±1.20 mmol/L) (Table 1).
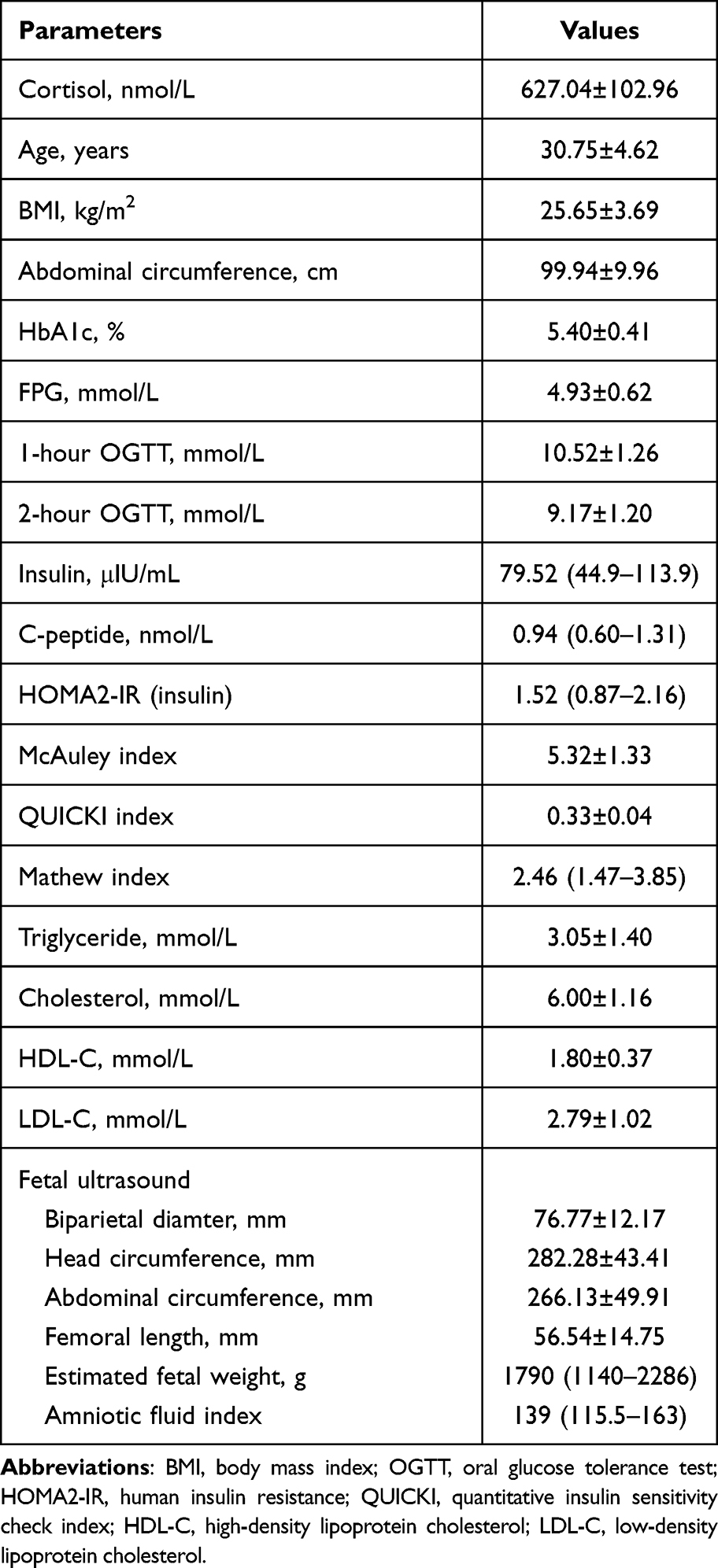 |
Table 1 Maternal and Fetal Characteristics in Gestational Diabetes Mellitus |
Serum cortisol levels positively correlated with AC, FPG, insulin, triglycerides, HOMA2-IR, and Mathew indices (with r of 0.18, 0.22, 0.18, 0.17, 0.18, and 0.22, respectively). Serum cortisol levels negatively correlated with QUICKI and McAuley indices (with r of −0.19 and −0.21, respectively) (Table 2). In a multivariate linear regression analysis, maternal serum cortisol still positively correlated with Mathew index (Table 3).
 |
Table 2 Correlation of Cortisol with Lipid Profiles, Blood Glucose, and Insulin Resistance Indices in GDM |
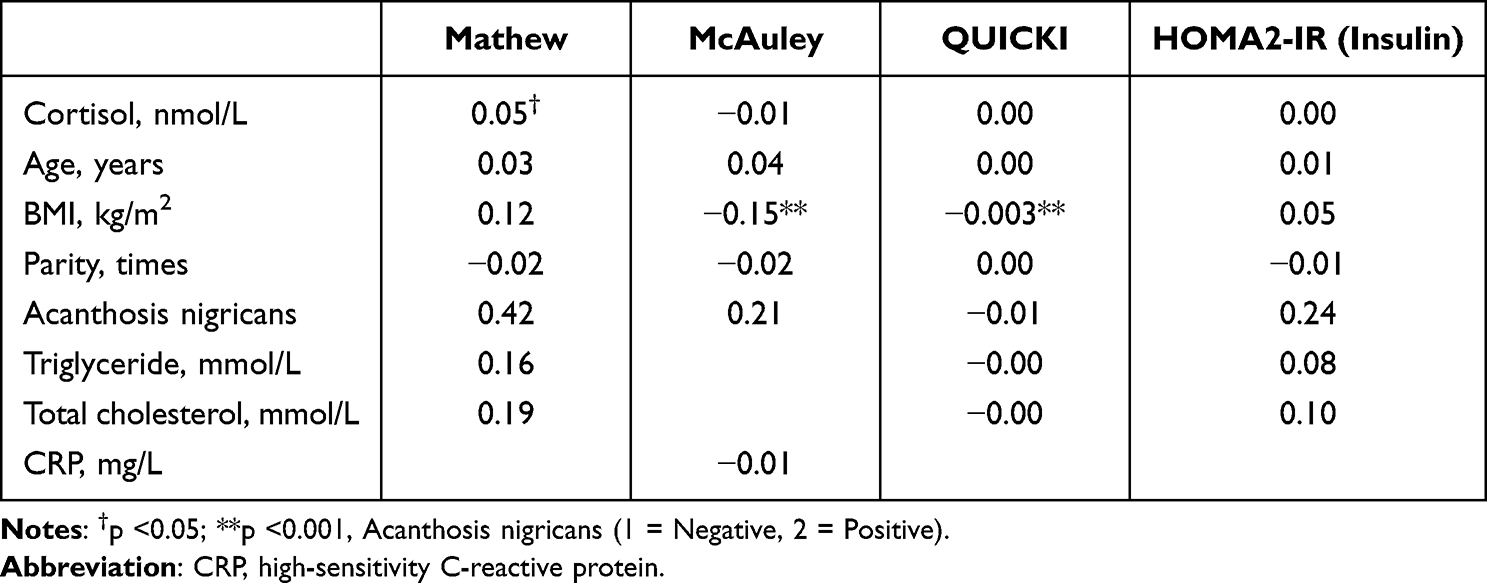 |
Table 3 Multivariate Linear Regression Analysis: Correlation Between Maternal Serum Cortisol and Maternal Insulin Resistance |
Regarding fetal ultrasound parameters, maternal serum cortisol levels positively correlated with fetal BDP, HC, and AC values, with r of 0.25, 0.23, and 0.21, respectively. However, maternal cortisol was not correlated with EFW, FL, and AFI (Table 4).
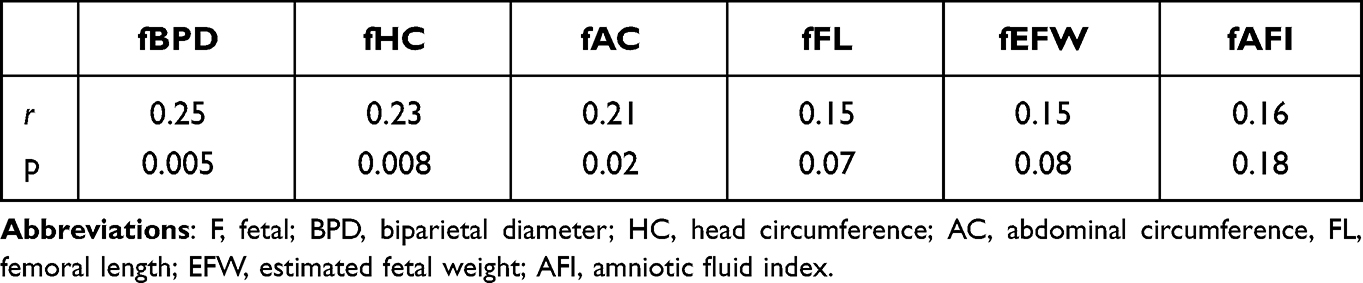 |
Table 4 Correlation of Maternal Cortisol with Fetal Ultrasound Indices in GDM |
In a multivariate linear regression analysis, maternal serum cortisol still positively correlated with fetal AC, HC, and BPD values after adjusting with maternal McAuley, HOMA2-IR indices, and BMI (Table 5).
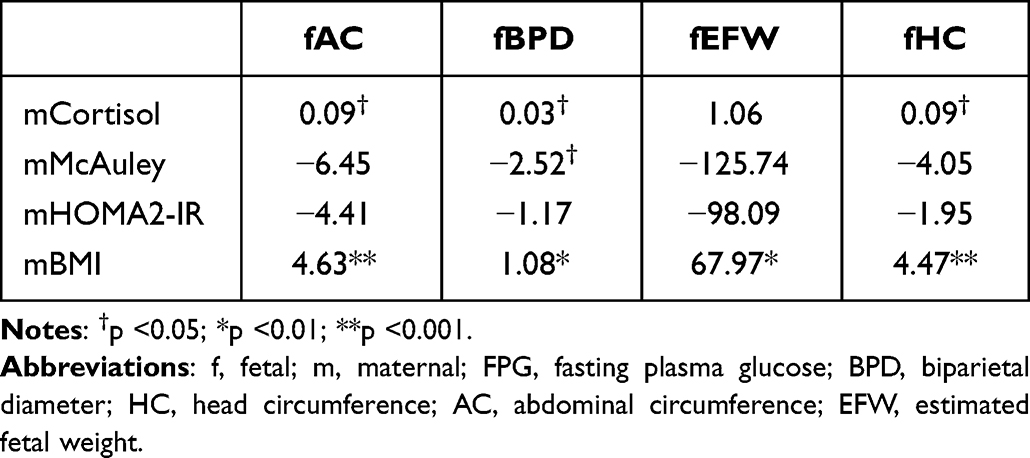 |
Table 5 Multivariate Linear Regression Analysis: Correlation Between Maternal Serum Cortisol and Fetal Ultrasound Indices |
Discussion
Our results outlined that serum cortisol levels in GDM correlated with maternal FPG concentration, triglyceride, insulin resistance, and some fetal development indicators (HC, AC, and BPD).
Cortisol is involved in the pathogenesis of hyperglycemia in GDM, which can be explained by the fact that pregnancy is a long-term stress for mothers and contributes to elevated cortisol levels. On the one hand, increased cortisol during pregnancy increases the antagonism of insulin action. Several observational studies in GDM have found elevated cortisol levels in GDM.17 Elevations of cortisol were detected even during the impaired glucose tolerance phase in pregnant women, contributing to reduced insulin sensitivity in GDM. On the other hand, studies in animal models have also shown that glucocorticoids induce increased insulin resistance in skeletal muscle through a decrease in glucose utilization and an increased shift towards fat for energy supply.23 These factors contribute to increased insulin resistance in GDM. In our study, cortisol levels were negatively correlated with McAuley and QUICKI indices but positively correlated with FPG, insulin, HOMA-2, and Mathew indices. A study by Yan Feng et al on 70 GDM found that serum cortisol levels in GDM had a weak positive correlation with the HOMA-IR index (r = 0.28, p < 0.05).24 Our results reinforce the role of cortisol in the pathogenesis of GDM. Cortisol is involved in the pathogenesis of GDM. During pregnancy, in contrast to its cortisol’s negative feedback on hypothalamic CRH (corticotropin-releasing hormone) secretion when cortisol is elevated, cortisol tends to stimulate CRH secretion from the placenta and thus participates in the cortisol self-increasing spiral. Raised cortisol causes increased stimulation of insulin secretion25 and increased lipid deposition in many organs.26 Cortisol has been shown to be dependent on adiposity and fat distribution.27,28 In our study, cortisol levels were positively correlated with triglyceride levels and maternal AC. Research by Le et al showed that, in GDM, the McAuley index is more meaningful in assessing insulin resistance and fetal abnormalities than other common insulin resistance indices built based on a healthy population and solely on serum glucose and insulin or C-peptide.21 The results above confirm the difference in insulin resistance in GDM with the role of cortisol and serum lipids.
Our results outlined that maternal serum cortisol positively correlates with some fetal development indicators on ultrasound, such as BPD, HC, and AC. After adjusting for maternal insulin resistance and BMI, maternal cortisol was correlated with fetal AC, BPD, and HC. According to the study by Enteringer et al, serum cortisol level in GDM was not significantly correlated with % body fat in the fetus. However, it was related to lipid deposition and the rate of obesity in the neonate.8 Maternal cortisol can cross the placenta, which may affect fetal development through dysregulation of placental CRH and directly into the fetus.29,30 Therefore, in our study, fetal AC, HC, and BPD increased with the increase in maternal cortisol. In normal pregnancy, the correlation between maternal serum cortisol and fetal ultrasound indices is primarily negative or non-sense.9,31–34 On the contrary, in GDM, our results show a positive correlation. In GDM, macrosomia, with a complex mechanism, is one of the complications for the fetus.35 Therefore, in GDM, there could be a harmony between insulin resistance and cortisol in the development of a fetus, with an increase in fetal ultrasound indices. However, with the cross-sectional and descriptive design, we could not separate the role of cortisol and insulin resistance in fetal development and could not draw a conclusion.
Nevertheless, our study found no association between maternal cortisol levels and fetal EFW. The relationship between maternal cortisol and EFW is controversial. Whilst, some studies in normal pregnant women have shown that serum cortisol levels are associated with fetal low birth weight,10,34 some studies showed the reverse results. In the White population, some studies showed maternal cortisol level is a predicted factor for fetal birth weight.9,31,32 On the contrary, a study by D’Anna-Hernandez et al also found the same trend as our study in pregnancy.33 Moreover, a study by Alicia et al in low-income Hispanic pregnancies showed no correlation between maternal serum cortisol and infant birth weight.34 A study by Fenling Fan et al on Chinese pregnant women showed that although maternal serum cortisol levels inversely correlated with EFW in the first and the second trimesters, no correlation between maternal cortisol and EFW was found in the third trimester.36 Although EFW is an indirect estimate of actual fetal weight and is generally overestimated in 65% of the cases, EFW is strongly correlated with actual weight at 2 weeks before birth.37 Therefore, race might contribute to the difference among studies on the correlation between maternal cortisol and fetal development. Besides, the method for collecting and interpreting serum cortisol could lead to the difference. In our study, we measured morning serum cortisol at 8 a.m., associated with lower beta-cell function and higher A1c and FPG in diabetes,38 to reduce the effects of stressors due to blood sampling and duration of the tests related to cortisol measurement.
This study has some limitations. First, the study was cross-sectional and descriptive at a one-time point that did not consider the postnatal change. However, abnormalities in the fetus are strongly associated with the child’s later development. Second, the study sample size was small. Third, we did not employ a control group of healthy pregnant women; therefore, we could not assess whether cortisol levels increased or decreased compared to normal pregnancy. Finally, we did not take the indicators for depression and anxiety in GDM into account. Therefore, we could not separate the effects of stress on maternal cortisol.
Conclusion
Serum cortisol levels in GDM correlated with FPG, triglycerides, and insulin resistance. Besides, serum cortisol levels in GDM positively correlated with fetal development.
Abbreviations
GDM, Gestational Diabetes mellitus; FPG, Fasting plasma glucose; PPG, postprandial glucose; OGTT, oral glucose tolerance test; BPD, Biparietal diameter; HC, Head circumference; AC, Abdominal circumference; FL, Femur length; AFI, Amniotic fluid index; HR, fetal Heart rate; EFW, Estimated fetal weight; CRP, high-sensitivity C-reactive protein.
Acknowledgments
We thank the staff in the Outpatients Department of the Vietnam Endocrinology Hospital and Department of Endocrinology and Rheumatology, Military Hospital 103 for collecting the samples and supporting the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for this article’s research, authorship, and/or publication.
Disclosure
The authors declared no potential conflicts of interest to this article’s research, authorship, and/or publication.
References
1. Duthie L, Reynolds RM. Changes in the maternal hypothalamic-pituitary-adrenal axis in pregnancy and postpartum: influences on maternal and fetal outcomes. Neuroendocrinology. 2013;98(2):106–115. doi:10.1159/000354702
2. Nepomnaschy PA, Welch KB, McConnell DS, et al. Cortisol levels and very early pregnancy loss in humans. Proc Natl Acad Sci. 2006;103:3938–3942. doi:10.1073/pnas.0511183103
3. Romero-Gonzalez B, Caparros-Gonzalez RA, Gonzalez-Perez R, Delgado-Puertas P, Peralta-Ramirez MI. Newborn infants’ hair cortisol levels reflect chronic maternal stress during pregnancy. PLoS One. 2018;13:e0200279. doi:10.1371/journal.pone.0200279
4. Abraham SB, Rubino D, Sinaii N, Ramsey S, Nieman LK. Cortisol, obesity, and the metabolic syndrome: a cross-sectional study of obese subjects and review of the literature. Obesity. 2013;21:E105–E117. doi:10.1002/oby.20083
5. Evans LM, Myers MM, Monk C. Pregnant women’s cortisol is elevated with anxiety and depression — but only when comorbid. Archiv Womens Mental Health. 2008;11:239. doi:10.1007/s00737-008-0019-4
6. Diego MA, Jones NA, Field T, et al. Maternal psychological distress, prenatal cortisol, and fetal weight. Psychosom Med. 2006;68:747–753. doi:10.1097/01.psy.0000238212.21598.7b
7. Lee C, Lee SM, Byun DJ, et al. Maternal signatures of cortisol in first trimester small-for-gestational age. Reproduct Sci. 2022;29(5):1498–1505. doi:10.1007/s43032-021-00822-w
8. Entringer S, Buss C, Rasmussen JM, et al. Maternal cortisol during pregnancy and infant adiposity: a prospective investigation. J Clin Endocrinol Metab;2016:3025. doi:10.1210/jc.2016-3025
9. Braithwaite EC, Hill J, Pickles A, et al. Associations between maternal prenatal cortisol and fetal growth are specific to infant sex: findings from the Wirral Child Health and Development Study. J Dev Orig Health Dis. 2018;9:425–431. doi:10.1017/S2040174418000181
10. Luiza JW, Gallaher MJ, Powers RW. Urinary cortisol and depression in early pregnancy: role of adiposity and race. BMC Pregnancy Childbirth. 2015;15(30). doi:10.1186/s12884-015-0466-7
11. Stewart PM, Boulton A, Kumar S, Clark PMS, Shackleton CHL. Cortisol metabolism in human obesity: impaired cortisone→cortisol conversion in subjects with central adiposity 1. J Clin Endocrinol Metab. 1999;84:1022–1027.
12. Banerji MA, Faridi N, Atluri R, Chaiken RL, Lebovitz HE. Body composition, visceral fat, leptin, and insulin resistance in Asian Indian Men 1. J Clin Endocrinol Metab. 1999;84:137–144.
13. La Verde M, Torella M, Riemma G, et al. Incidence of gestational diabetes mellitus before and after the Covid‐19 lockdown: a retrospective cohort study. J Obstet Gynaecol Res. 2022;48:1126–1131. doi:10.1111/jog.15205
14. Kanguru L, Bezawada N, Hussein J, Bell J. The burden of diabetes mellitus during pregnancy in low- and middle-income countries: a systematic review. Glob Health Action. 2014;7:23987. doi:10.3402/gha.v7.23987
15. Minschart C, Beunen K, Benhalima K. An update on screening strategies for gestational diabetes mellitus: a narrative review. Diabetes Metab Syndr Obes. 2021;14:3047–3076. doi:10.2147/DMSO.S287121
16. Hornnes PJ, Kühl C. Gastrointestinal hormones and cortisol in normal pregnant women and women with gestational diabetes. Acta Endocrinol. 1986;113:S24–S26.
17. Ahmed SA, Shalayel MH. Role of cortisol in the deterioration of glucose tolerance in Sudanese pregnant women. East Afr Med J. 1999;76:465–467.
18. Manjunath-Gowda S, Charles C, Muneyyirci-Delale O, Nacharaju V. Cortisol metabolism in normal pregnancy and pregnancy associated with gestational diabetes. Fertil Steril. 2013;100:S333. doi:10.1016/j.fertnstert.2013.07.915
19. Ma R, Liu J, Wu L, et al. Differential expression of placental 11β-hydroxysteroid dehydrogenases in pregnant women with diet-treated gestational diabetes mellitus. Steroids. 2012;77:798–805. doi:10.1016/j.steroids.2012.03.007
20. Van Dam JM, Garrett AJ, Schneider LA, et al. Reduced cortical excitability, neuroplasticity, and salivary cortisol in 11–13-year-old children born to women with gestational diabetes mellitus. EBioMedicine. 2018;31:143–149. doi:10.1016/j.ebiom.2018.04.011
21. Dinh LT, Minh Bui T, Hien Vu T, et al. Insulin resistance in gestational diabetes mellitus and its association with anthropometric fetal indices. Clin Med Insights Endocrinol Diabetes. 2022;15:117955142210984. doi:10.1177/11795514221098403
22. American College of Radiology. CR–ACOG–AIUM practice guideline for the performance of obstetrical ultrasound. Am Coll Radiol. 2007;294:1–9.
23. Almon RR, DuBois DC, Jin JY, Jusko WJ. Temporal profiling of the transcriptional basis for the development of corticosteroid-induced insulin resistance in rat muscle. J Endocrinol. 2005;184:219–232. doi:10.1677/joe.1.05953
24. Feng Y, Feng Q, Qu H, et al. Stress adaptation is associated with insulin resistance in women with gestational diabetes mellitus. Nutr Diabetes. 2020;10(1):4.
25. Strack AM, Sebastian RJ, Schwartz MW, Dallman MF. Glucocorticoids and insulin: reciprocal signals for energy balance. Am J Physiol Regul Integr Comp Physiol. 1995;268:R142–R149. doi:10.1152/ajpregu.1995.268.1.R142
26. Björntorp P. The regulation of adipose tissue distribution in humans. Int J Obes Relat Metab Disord. 1996;20:291–302.
27. Holt HB, Wild SH, Postle AD, et al. Cortisol clearance and associations with insulin sensitivity, body fat and fatty liver in middle-aged men. Diabetologia. 2007;50:1024–1032. doi:10.1007/s00125-007-0629-9
28. Ammini A. Morning cortisol is lower in obese individuals with normal glucose tolerance. Diabetes Metab Syndr Obes. 2011;347. doi:10.2147/DMSO.S23915
29. Gitau R, Fisk NM, Teixeira JMA, Cameron A, Glover V. Fetal hypothalamic-pituitary-adrenal stress responses to invasive procedures are independent of maternal responses 1. J Clin Endocrinol Metab. 2001;86:104–109.
30. Jones SA, Brooks AN, Challis JRG. Steroids modulate corticotropin-releasing hormone production in human fetal membranes and placenta. J Clin Endocrinol Metab. 1989;68:825–830. doi:10.1210/jcem-68-4-825
31. Crowther CA, Middleton PF, Voysey M, et al. Effects of repeat prenatal corticosteroids given to women at risk of preterm birth. An individual participants data meta-analysis. PloS Med. 2019;16:e1002771. doi:10.1371/journal.pmed.1002771
32. Bolten MI, Wurmser H, Buske-Kirschbaum A, Papousek M, Pirke KM, Hellhammer D. Cortisol levels in pregnancy as a psychological predictor for birth weight. Arch Women’s Ment Health. 2011;14:33–41. doi:10.1007/s00737-010-0183-1
33. D’Anna-Hernandez KL, Hoffman MC, Zerbe GO, et al. Acculturation, maternal cortisol, and birth outcomes in women of Mexican descent. Psychosom Med. 2012;74(3):296–304. doi:10.1097/PSY.0b013e318244fbde
34. Peterson A, Toledo-Corral CM, Chavez T, et al. Prenatal maternal cortisol levels and infant birth weight in a predominately low-income Hispanic cohort. Int J Environ Res Public Health. 2020;17:6896. doi:10.3390/ijerph17186896
35. Kamana KC, Shakya S, Zhang H. Gestational diabetes mellitus and macrosomia: a literature review. Ann Nutr Metab. 2015;66:14–20. doi:10.1159/000371628
36. Fan F, Zou Y, Zhang Y, et al. The relationship between maternal anxiety and cortisol during pregnancy and birth weight of Chinese neonates. BMC Pregnancy Childbirth. 2018;18:265. doi:10.1186/s12884-018-1798-x
37. Stephens K, Al‐Memar M, Beattie‐Jones S, et al. Comparing the relation between ultrasound‐estimated fetal weight and birthweight in cohort of small‐for‐gestational‐age fetuses. Acta Obstet Gynecol Scand. 2019;98:1435–1441. doi:10.1111/aogs.13645
38. Robin O, Bjoern K, James BO, et al. The association of morning serum cortisol with glucose metabolism and diabetes: the Jackson Heart Study. Psychoneuroendocrinology. 2018;103:25–32. doi:10.1016/j.psyneuen.2018.12.237
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Low-Grade Inflammation in Gestational Diabetes Mellitus and Its Correlation with Maternal Insulin Resistance and Fetal Growth Indices
Xuan Nguyen K, Bui Minh T, Dinh HT, Viet Tran T, Dinh Le T, Phi Thi Nguyen N, Tran TTH, Hien Vu T, Ho Thi Nguyen L, Trung Nguyen K, Huy Thong N, Do K, Nguyen TK, Nguyen Dao H, Tien Nguyen S
International Journal of General Medicine 2023, 16:1429-1436
Published Date: 20 April 2023