Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Relationship Between COPD and GERD: A Bibliometrics Analysis
Authors Zou M ![]() , Zhang W, Xu Y, Zhu Y
, Zhang W, Xu Y, Zhu Y
Received 6 October 2022
Accepted for publication 24 November 2022
Published 6 December 2022 Volume 2022:17 Pages 3045—3059
DOI https://doi.org/10.2147/COPD.S391878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Menglong Zou, Wei Zhang, Yin Xu,* Ying Zhu*
Department of Gastroenterology, The First Hospital of Hunan University of Chinese Medicine, Changsha, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Zhu; Yin Xu, The First Hospital of Hunan University of Chinese Medicine, No. 95, Shaoshan Middle Road, Changsha, Hunan, People’s Republic of China, Tel +86-731-85600700, Email [email protected]; [email protected]
Purpose: A growing body of evidence links chronic obstructive pulmonary disease (COPD) to gastroesophageal reflux disease (GERD). In spite of the lack of understanding of the specific cause-effect relationship between COPD and GERD, GERD has been shown to be a significant predictor of acute exacerbations of COPD. In this study, we examined the evolution of the relationship between COPD and GERD over the past decades and provided valuable insights into this topic.
Methods: The Web of Science Core Collection (WoSCC) was searched since its inception until 19 August 2022 to obtain publications related to COPD and GERD. The data was analyzed in Microsoft Excel (version 2021), HisCite (version 2.1), Scimago Graphica (version 1.0.23), VOSviewer (1.6.17), and CiteSpace (version 5.8.R3).
Results: We extracted 545 documents from the WoSCC database. Since 2002, there have been rapid increases in publications. Among countries and institutions, the United States and the University of Manchester were most prolific. The most cited journal was Chest, while Respiratory Medicine had the most publications. Among 2870 related authors, Hasenfuss, Gerd, Lange, Peter, and Martinez, Gerd were the top 3 contributing authors in this field. Aside from “gastroesophageal reflux disease” and “chronic obstructive pulmonary disease”, the terms “quality of life”, “cough”, and “inflammation” were frequently occurred in the title and abstract of articles. Keywords co-occurrence overlay visualization indicated that “refractory chronic cough” was hot topics in recent years.
Conclusion: Research on COPD and GERD has flourished, and its content topics have become more in-depth over time. In the future, this hot topic deserves more attention.
Keywords: chronic obstructive pulmonary disease, gastroesophageal reflux disease, knowledge graph, disease connections
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic and progressive condition in which the airways are inflamed, and airflow is limited in a nonreversible manner.1 There is a high likelihood of acute exacerbations, which increase the risk of COPD morbidity and mortality and contribute to worsening quality of life.2 It has been shown that COPD is increasing in prevalence, particularly among people aged 65 and older.3 Comorbid conditions may complicate the clinical presentation of COPD and impact mortality and morbidity.
A normal physiological occurrence, gastroesophageal reflux (GER) is influenced by the integrity of the gastroesophageal junction. Symptoms of gastroesophageal reflux disease (GERD) result from the reflux of gastric contents.4 Approximately 33% of the general population has this condition, which can either be esophageal or extraesophageal in nature.5 A number of factors have been proposed as contributing to GERD, including increased compliance of the gastroesophageal junction.6 Importantly, it appears that chronic cough associated with GERD is becoming more common as GER itself becomes more prevalent.
There is a long history of recognition of the likelihood of an interaction between COPD and GERD due to their high prevalence.7–9 GERD may aggravate COPD’s clinical status, while mechanical changes caused by COPD may exacerbate GERD’s severity. It is therefore crucial to understand the relationship between the two conditions and the potential consequences of their co-occurrence. Bibliometrics analysis is a quantitative method for evaluating research characteristics and trends within a specific period of time by analyzing published academic literature. With this approach, we can identify the research hotspots and emerging trends associated with a specific field. In this study, the overall status of COPD and GERD research was analyzed using bibliometrics.
Materials and Methods
Data Sources and Search Strategy
The literature search was performed using Web of Science Core Collection (WoSCC) with no specified starting date, but up to 19 August 2022. We limited our search to English-language literatures, and Table 1 details our search strategy. A total of 591 records were retrieved, and we examined only two types of documents: articles and reviews. As a result, 545 retrieval records were analyzed. The flow chart of literature screening is shown in Figure 1.
 |
Table 1 Search Strategy |
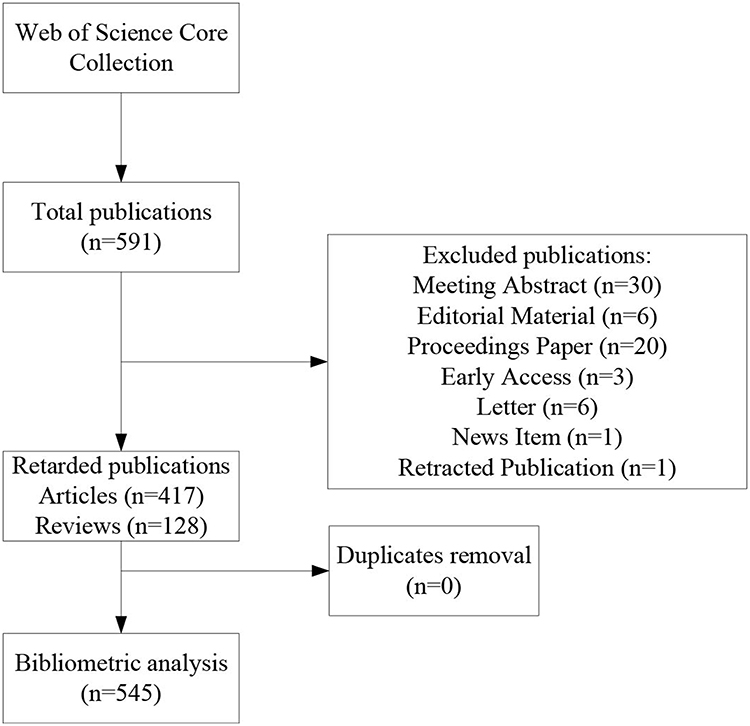 |
Figure 1 The flowchart of literature selection. |
Data Analysis
The WoSCC was used to obtain the information needed, such as the number of publications per year and the number of articles published per country/region, institution, journal, and author. A further evaluation of the scientific impact of a journal was based on the impact factor (IF) and quartiles of the journal categories in the 2021 Journal Citation Reports (JCR). We presented the data in tables or charts using Microsoft Excel (version 2021) and Origin software (version 2021).
VOSviewer and Citespace are bibliometric visualization tools that can help analyze the current state of scientific research and detect its frontiers.10,11 In this study, VOSviewer and Citespace were used to perform (1) countries/regions and institutions co-authorship, (2) authors co-authorship and co-citation, (3) journals citation and co-citation, (4) keywords co-occurrence, (5) citation-burst analysis of references.
History of Cite (HisCite, version 2.1) is an analysis software developed by Garfield for analyzing citation maps.12 Generally, it is used to illustrate relationships between different pieces of literature within a field of study. The software can locate the important literature and depict the field’s developmental process. This study used the HisCite software to analyze GERD’s development in COPD. In this study, we used the HisCite software to analyze the developmental process of the relationship between COPD and GERD.
We also used the Scimago Graphica tool (version 1.0.23) to create collaboration networks between institutions and countries/regions.
Since this was a bibliometric analysis, no approval was required from the Internal Review Board.
Results
Analysis of Publications
The development profile of a field can be reflected in annual publications. Figure 2 shows a general upward trend in this field. In spite of a brief decline phase, publication numbers in this field have exploded since 2002. Researchers have increasingly focused on the relationship between COPD and GERD.
 |
Figure 2 Annual trends in publications. |
Analysis of Collaborations
Five hundred and forty-five documents on COPD and GERD have been co-authored by 1085 institutions from 50 countries/regions. Tables 2 and 3 list the top 10 most productive countries/regions or institutions. Our study indicated that United States (158, 28.99%) was the most productive country, followed by United Kingdom (46, 8.44%), Germany (35, 6.42%), Japan (28, 5.14%), and Italy (27, 4.95%). The most active affiliate was Univ Manchester (16, 2.94%), followed by Univ Michigan (13, 2.39%), Mayo Clin (12, 2.20%), Univ Copenhagen (12, 2.20%), and Brigham & Womens Hosp (11, 2.02%). Our analysis of the total link strength of countries/regions and organizations identifies the United States and Brigham & Womens Hosp as the most influential in this field.
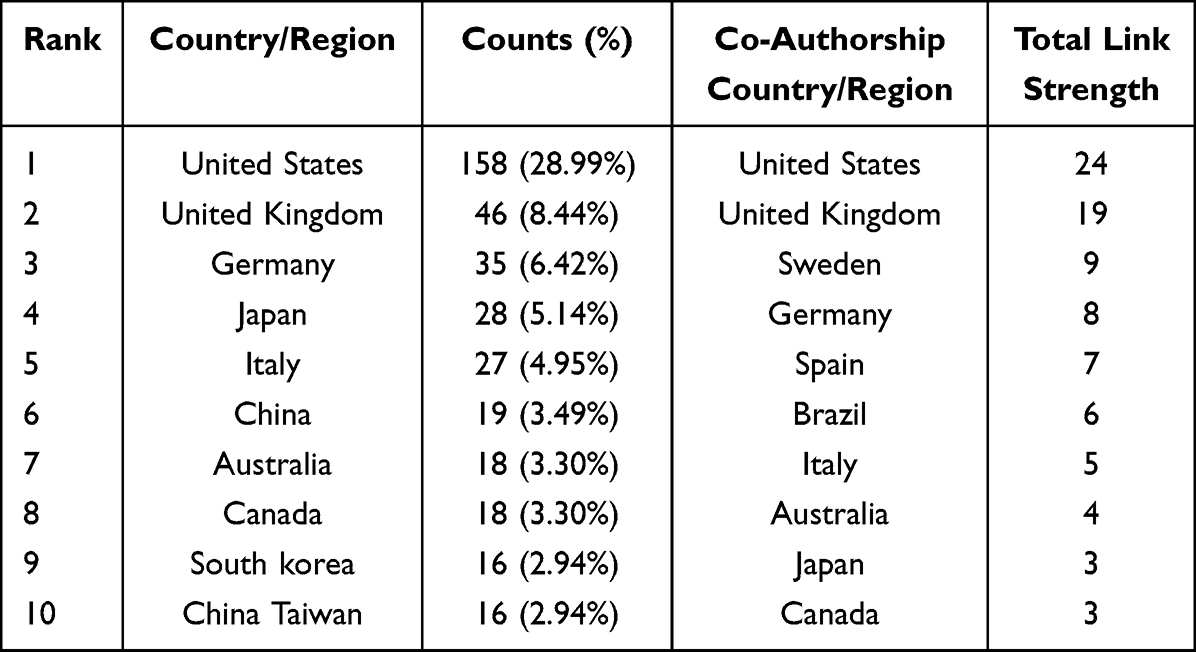 |
Table 2 The 10 Countries/Regions with the Highest Number of Outputs and the Highest Degree of Cooperation |
 |
Table 3 The 10 Institutions with the Highest Number of Outputs and the Highest Degree of Cooperation |
Figures 3 and 4 show the cooperation maps for each country/region and institution. The size of each node correlates with the number of documents, while the link line width and color reflect the degree of cooperation between them. It is readily apparent that the United States works closely with a number of countries, but the United Kingdom is the most important. Furthermore, many research institutions, including Brigham & Womens Hosp, Univ Manchester, and Temple Univ, cooperated actively.
 |
Figure 3 Countries/regions collaboration map. |
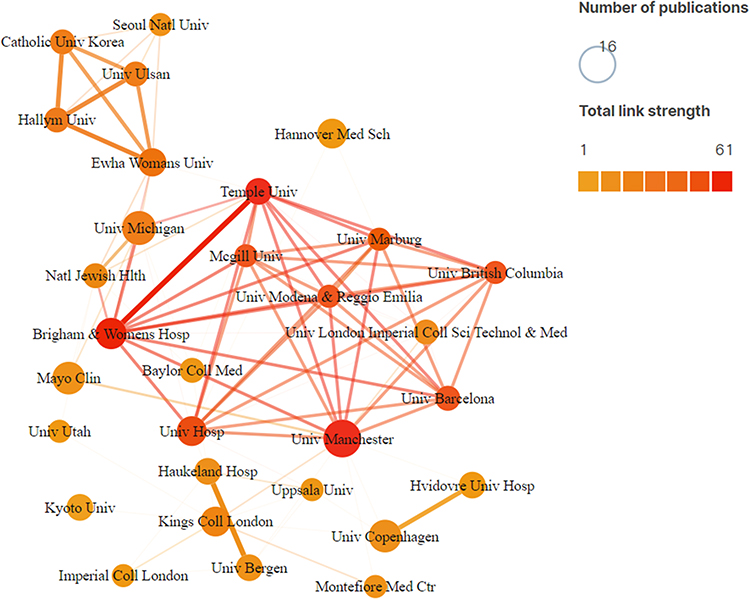 |
Figure 4 Institutions collaboration map. |
Analysis of Journals
There were 283 journals that published the documents included. The majority of the top ten relevant journals (Table 4) had IF above 3 and these journals were classified in the top two quartiles (Q1 and Q2): Respiratory Medicine (N = 28, IF = 4.582, JCR = Q2), Chest (N = 24, IF = 10.262, JCR = Q1), International Journal of Chronic Obstructive Pulmonary Disease (N = 21, IF = 2.893, JCR = Q2), European Respiratory Journal (N = 11, IF = 33.795, JCR = Q1), Respiratory Research (N = 11, IF = 7.162, JCR = Q1).
 |
Table 4 The Top Ten Journals and Co-Cited Journals |
The co-citation analysis of journals is concerned primarily with the relationship between the journals, which reveals whether a journal acts as a bridge in this field.13 As can be seen from Table 4, there were two academic journals with more than 2000 citations, one is Chest (IF = 10.262) and the other is American Journal of Respiratory and Critical Care Medicine (IF = 30.528). The co-citation relationship between Chest and other journals is clearly demonstrated in Figure 5.
 |
Figure 5 Network of co-citation journal analysis. |
Analysis of Authors
In total, 2870 authors contributed to this field. Table 5 lists the top 10 authors who contributed and were cited the most, with 6 authors working in the Univ Manchester. Hasenfuss, Gerd (12, 2.20%), Lange, Peter (11, 2.02%), and Martinez, Gerd (11, 2.02%) are the top three most prolific authors. This field has been the subject of many academic teams, as shown in the author collaborative map (Figure 6). Author co-citation can reveal highly influential scholars. A list of the 10 most co-cited scholars is presented in Table 5. As far as citations are concerned, Irwin, RS ranked first, with 156 citations, followed by Raghu, G (citations = 140), Morice, AH (citations = 103), Hurst, JR (citations = 99), and Terada, K (citations = 94).
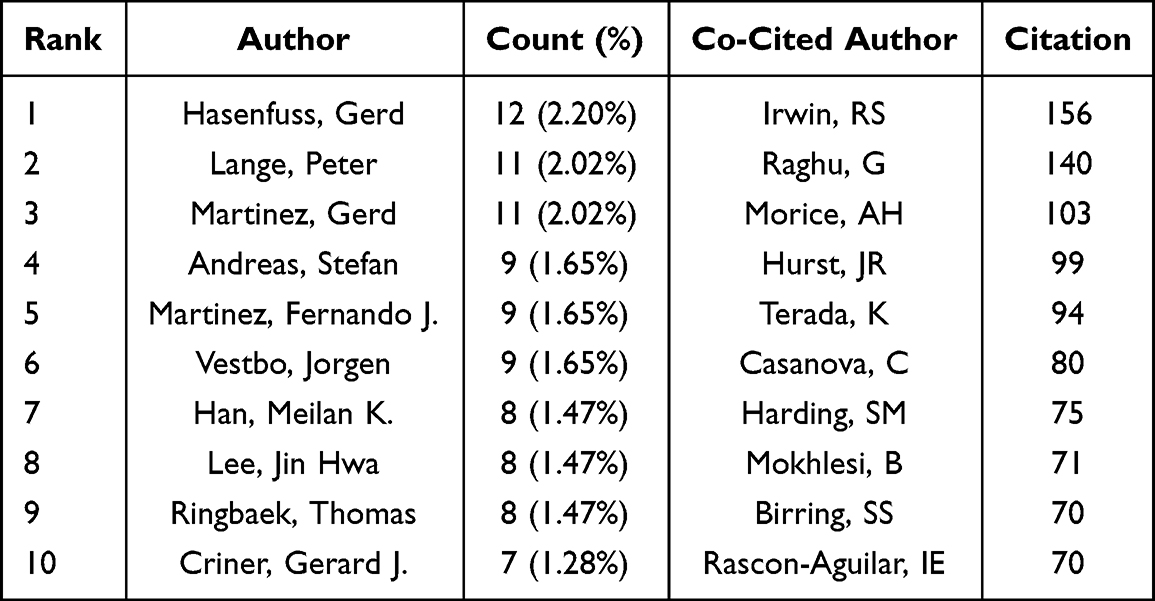 |
Table 5 The Top Ten Authors and Co-Cited Authors |
 |
Figure 6 Inter-author collaborative map. |
Keywords Co-Occurrence Analysis
The keywords in an article indicate the topic of the article, and they can be used to identify research hotspots and frontiers within a field. A co-occurrence map of 62 high-frequency keywords (more than 10 times) was constructed using VOSviewer software (Figure 7). The top 30 keywords associated with COPD and GERD are presented in Table 6. Aside from “gastroesophageal reflux disease” and “chronic obstructive pulmonary disease”, the terms “quality of life”, “cough”, and “inflammation” frequently occurred in the abstract and title of articles.
 |
Table 6 The Top 30 Keywords Related to COPD and GERD |
 |
Figure 7 Keywords co-occurrence visualization map. |
In VOSviewer, keywords were colored based on the average time they appeared in the document. We can find the research hotspots over time in a specific field based on the average time of keywords appearance. Using a co-occurrence overlay visualization, Figure 8 shows the top 15 keywords from 1991 to 2022. In comparison to yellow keywords, blue keywords appeared earlier. Among these keywords, “refractory chronic cough”, “chronic rhinosinusitis”, and “adults” generated the most interest in recent years.
 |
Figure 8 Keywords co-occurrence overlay visualization map. |
Analysis of Hiscite Literature
To analyze the development of COPD and GERD, we selected the top 20 articles using local citation score (LCS) in HisCite (Figure 9, Table 7). From these results, we found the paper authored by Hurst et al14 is the most highly cited. The study evaluated the frequency and associated factors of exacerbation in 2138 patients enrolled in the Evaluation of COPD Longitudinally study. They elucidated the frequency of exacerbations was independently associated with GERD. More remarkable is another result that “Associations between gastro-oesophageal reflux, its management and exacerbations of chronic obstructive pulmonary disease (ID:256)” and “Gastroesophageal reflux disease in COPD: links and risks (ID:235)” were key articles in recent years. The former showed that self-reported GERD in COPD patients was significantly associated with exacerbation risk.15 The later study reviewed the possible causes of GERD in COPD, such as gastroesophageal mechanisms, respiratory mechanisms, respiratory medications, and non-COPD factors.16
 |
Table 7 The Detailed Information of the Top 20 Articles in Literature on COPD and GERD Based on the LCS |
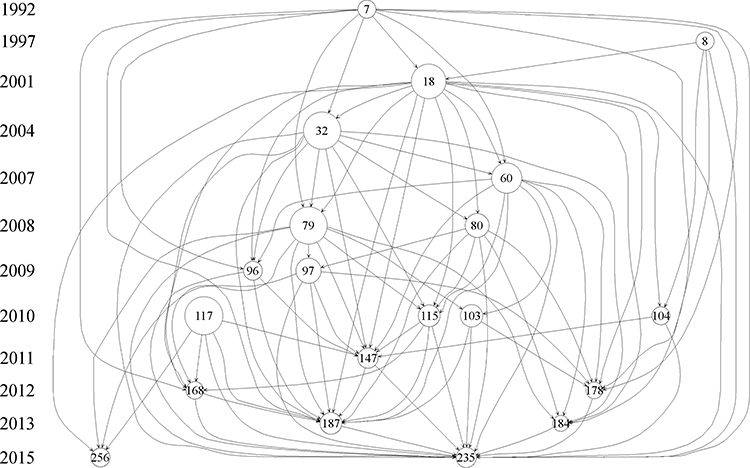 |
Figure 9 Network of the top 20 articles in literature on COPD and GERD based on the LCS. |
Burst Detection of References
In over time, burst detection of references reflects a shift in research focus. Among the top 25 references (Figure 10), the article authored by Baumeler et al17 with a burst strength of 4.92 and another article authored by Broers et al18 with a burst strength of 3.93 were frequently cited in recent years. Despite receiving acid-suppressive therapy, Baumeler et al found that patients with stable COPD were still highly vulnerable to frequent and severe exacerbations. As discussed by Broers et al, there has been a contradictory and inconsistent response to anti-reflux therapy when considering pulmonary outcomes. They call for further research to identify subgroups of COPD patients who would benefit from anti-reflux therapy. Obviously, scholars are taking a more active interest in the relationship between COPD and GERD and examining treatment options.
 |
Figure 10 Burst detection of references. |
Discussion
Over the past decade, the role of GERD in the pathogenesis of chronic pulmonary diseases has garnered a lot of attention. There is a possibility that GERD and chronic respiratory disease are bidirectional, or that the relationship can be caused by changes in latent variables that are correlated. GERD drives respiratory disease, while respiratory mechanics contribute to GERD, making it important to better understand their relationship and possible consequences.
General Information
The current analysis indicates that the relationship between COPD and GERD has not received much attention before 2002. However, the rise in annual publications from 2002 to the present shows that this field of study is a hotspot and continues to draw interest.
Using a map analysis of the distribution of countries/regions and institutions, it is evident that COPD and GERD research has been conducted in many countries and regions. With 158 publications, the United States has contributed the most to this field, followed by the United Kingdom with 46 and Germany with 35. Again, from the Table 2, the United States ranked highest in total link strength, suggesting that articles published in the United States may be more influential. Globally, over 1000 institutions study the relationship between COPD and GERD. The most productive institution was Univ Manchester, according to Table 3. It is likely that the contributions of scholars at this institution, such as such as Lange, Peter, Martinez, Gerd, Martinez, Fernando J, Vestbo, Jorgen, Ringbaek, Thomas, and Criner, Gerard J, have contributed to this result. Although some of these institutions have collaborated closely, others have not, as seen in Figure 4. Thus, the breadth and depth of cooperation between countries and institutions with similar research topics should be strengthened, and this field should be further developed jointly.
In Table 4, it is evident that most of the top 10 journals are from JCR Q1 or Q2, and most of them have IFs higher than 3.0, showing that this field has relatively high levels of research. In our analysis, articles with high co-citations were published in multiple prestigious journals, such as Chest, American Journal of Respiratory and Critical Care Medicine, European Respiratory Journal, New England Journal of Medicine, and Lancet. Due to CORD and COPD’s potential impact, top scholars have shown a keen interest in the topic. It is important, therefore, to pay more attention to these journals in order to acquire new research advancements or discoveries.
Among numerous scholars in this field, Hasenfuss, Gerd, Lange, Peter, and Martinez, Gerd have contributed the most. It is apparent from the network of author cooperation that, while many academic teams have been formed in this field, there is little cooperation. Efforts should be made by all academic teams to improve scholarly communication, investigate the link between COPD and GERD, and promote its rapid development. A particular note of note is Irwin, RS, the most co-cited author in this field who has made significant contributions to this field. An analysis of diagnosis and treatment algorithms of acute, subacute, and chronic cough in adults was carried out by Irwin et al.19
Hotspots and Frontiers
Keyword analysis can provide valuable information about research frontier in a particular field, which is the most valuable aspect of bibliometrics analysis. The top frequency keywords related to COPD and GERD, including quality of life, cough, inflammation, obstructive sleep apnea, obesity, depression, smoking, cardiovascular-disease, and inhaled corticosteroids, are shown in Table 6. According to Figure 8, research in this area has been shifting over time, with recent attention being paid to refractory chronic cough and chronic rhinosinusitis.
COPD comorbidities may negatively impact health-related quality of life (HRQOL). Some studies with a larger group of COPD patients reported poorer HRQOL and more anxiety and depression when self-reported GERD was present.20–22 Increased anxiety is known to exacerbate GERD symptoms by increasing acid production.23 Anxiety is common in COPD, and this may contribute to GERD.
A change in respiratory mechanics may contribute to GERD. Severe hyperinflation requires increased respiratory muscle inspiratory effort to overcome the increased inspiratory load at high lung volume. During severe hyperinflation, respiratory muscles must exert increased inspiratory effort to overcome an increased inspiratory load. It is well known that transient relaxation of the lower esophageal sphincter (LES) is one of the primary causes of GERD. In this case, increased negative pressure enhances the pressure gradient between the thorax and abdomen, which affects the tone of the LES and makes reflux more likely.24,25 During COPD exacerbations, airflow reductions and coughing can exacerbate this pressure gradient.
Vagally mediated reflex bronchoconstriction may influence the severity of COPD by GERD. Bronchoconstriction is innervated by the autonomic innervation between the esophagus and the tracheobronchial tree. Airway irritation and inflammation caused by esophageal acid in the distal esophagus trigger the release of bronchoconstrictors.26
There has also been evidence that certain comorbidities can increase the risk of GERD, including cardiac disease and sleep apnea.20 A higher intrathoracic pressure during an apneic episode is accompanied by a higher transdiaphragmatic pressure, which causes the gastric contents to migrate up the esophagus.27 Additionally, repetitive pressure changes can lead to LES insufficiency.27
COPD patients with a higher body mass index (BMI) are at greater risk of GERD, and this risk increases as the BMI increases.20,28 Having a high BMI affects the contour of the diaphragm and thus affects breathing elastically.29 Hence, GERD may become more likely when respiratory-related factors are combined with a high BMI for people with COPD.
An association has been found between smoking and a reduction in LES tone. As a result of nicotine-induced relaxation of the circular muscle of the LES, there is an increase in acid exposure in the upright position.30,31 In addition, nicotine also interferes with esophageal clearance. A high smoking index has been shown to increase the severity of GERD in COPD patients.28 Due to smoking being a risk factor for GERD as well as a leading cause of COPD, smoking may contribute to GERD in COPD.32
Corticosteroids, anticholinergics, and theophylline preparations are some of the respiratory medications considered to be associated with GERD.20,33,34 Although these medications may reduce LES pressure or esophageal motility, their specific impact on GERD risks varies. In addition, the correlation between GERD and respiratory medications may also reflect the severity of lung disease rather than a physiological reaction to these medications. In COPD, further investigation is needed into the cause-and-effect relationship between respiratory medications and GERD.
In our study, some limitations exist. First, the study retrieved only literature from WoSCC database, so there is a risk of overlooking related studies, resulting in biased results. Our second limitation was that we only included reviews and articles in English, which could lead to bias. Additionally, the downloaded data may also have omitted some important details since it is not in full text.
Conclusion
Our study identified 545 publications on COPD and GERD, revealing influential countries, institutions, and authors that made significant contributions to this field. Moreover, we concentrated on specific topics in order to investigate research trends. According to our analysis, quality of life, cough, and inflammation have been the research frontier in this field. In summary, COPD and GERD are subjects of ongoing research.
Acknowledgments
This study was supported by grants from the National Natural Science Foundation of China (81874466, 81904176), the Natural Science Foundation of Hunan Province (2021JJ30531), the Scientific Research Foundation of Hunan Provincial Department of Education (21B0389), and the Clinical Medical Technology Innovation Guide Project of Hunan Province (2021SK51413).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242.
2. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
3. Rycroft CE, Heyes A, Lanza L, Becker K. Epidemiology of chronic obstructive pulmonary disease: a literature review. Int J Chron Obstruct Pulmon Dis. 2012;7:457–494. doi:10.2147/COPD.S32330
4. Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101(8):1900–1920; quiz 1943. doi:10.1111/j.1572-0241.2006.00630.x
5. El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014;63(6):871–880. doi:10.1136/gutjnl-2012-304269
6. Miller LS, Vegesna AK, Brasseur JG, Braverman AS, Ruggieri MR. The esophagogastric junction. Ann N Y Acad Sci. 2011;1232(1):323–330. doi:10.1111/j.1749-6632.2011.06073.x
7. Ducoloné A, Vandevenne A, Jouin H, et al. Gastroesophageal reflux in patients with asthma and chronic bronchitis. Am Rev Respir Dis. 1987;135(2):327–332. doi:10.1164/arrd.1987.135.2.327
8. Sweet MP, Patti MG, Hoopes C, Hays SR, Golden JA. Gastro-oesophageal reflux and aspiration in patients with advanced lung disease. Thorax. 2009;64(2):167–173. doi:10.1136/thx.2007.082719
9. Casanova C, Baudet JS, Del Valle Velasco M, et al. Increased gastro-oesophageal reflux disease in patients with severe COPD. Eur Respir J. 2004;23(6):841–845. doi:10.1183/09031936.04.00107004
10. Fu R, Xu H, Lai Y, et al. A VOSviewer-based bibliometric analysis of prescription refills. Front Med. 2022;9:856420. doi:10.3389/fmed.2022.856420
11. Liu S, Sun YP, Gao XL, Sui Y. Knowledge domain and emerging trends in Alzheimer’s disease: a scientometric review based on CiteSpace analysis. Neural Regen Res. 2019;14(9):1643–1650. doi:10.4103/1673-5374.255995
12. Shi J, Gao Y, Ming L, et al. A bibliometric analysis of global research output on network meta-analysis. BMC Med Inform Decis Mak. 2021;21(1):144. doi:10.1186/s12911-021-01470-5
13. Guo S, Wang L, Xie Y, et al. Bibliometric and visualized analysis of stem cells therapy for spinal cord injury based on web of science and citespace in the last 20 years. World Neurosurg. 2019;132:e246–e258. doi:10.1016/j.wneu.2019.08.191
14. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
15. Benson VS, Müllerová H, Vestbo J, Wedzicha JA, Patel A, Hurst JR. Associations between gastro-oesophageal reflux, its management and exacerbations of chronic obstructive pulmonary disease. Respir Med. 2015;109(9):1147–1154. doi:10.1016/j.rmed.2015.06.009
16. Lee AL, Goldstein RS. Gastroesophageal reflux disease in COPD: links and risks. Int J Chron Obstruct Pulmon Dis. 2015;10:1935–1949. doi:10.2147/COPD.S77562
17. Baumeler L, Papakonstantinou E, Milenkovic B, et al. Therapy with proton-pump inhibitors for gastroesophageal reflux disease does not reduce the risk for severe exacerbations in COPD. Respirology. 2016;21(5):883–890. doi:10.1111/resp.12758
18. Broers C, Tack J, Pauwels A. Review article: gastro-oesophageal reflux disease in asthma and chronic obstructive pulmonary disease. Aliment Pharmacol Ther. 2018;47(2):176–191. doi:10.1111/apt.14416
19. Irwin RS, French CL, Chang AB, Altman KW. Classification of cough as a symptom in adults and management algorithms: CHEST guideline and expert panel report. Chest. 2018;153(1):196–209. doi:10.1016/j.chest.2017.10.016
20. Martinez CH, Okajima Y, Murray S, et al. Impact of self-reported gastroesophageal reflux disease in subjects from COPDGene cohort. Respir Res. 2014;15(1):62. doi:10.1186/1465-9921-15-62
21. Rascon-Aguilar IE, Pamer M, Wludyka P, et al. Role of gastroesophageal reflux symptoms in exacerbations of COPD. Chest. 2006;130(4):1096–1101. doi:10.1378/chest.130.4.1096
22. Niklasson A, Strid H, Simrén M, Engström CP, Björnsson E. Prevalence of gastrointestinal symptoms in patients with chronic obstructive pulmonary disease. Eur J Gastroenterol Hepatol. 2008;20(4):335–341. doi:10.1097/MEG.0b013e3282f2d0ec
23. Naliboff BD, Mayer M, Fass R, et al. The effect of life stress on symptoms of heartburn. Psychosom Med. 2004;66(3):426–434. doi:10.1097/01.psy.0000124756.37520.84
24. Pauwels A, Blondeau K, Dupont LJ, Sifrim D. Mechanisms of increased gastroesophageal reflux in patients with cystic fibrosis. Am J Gastroenterol. 2012;107(9):1346–1353. doi:10.1038/ajg.2012.213
25. Turbyville JC. Applying principles of physics to the airway to help explain the relationship between asthma and gastroesophageal reflux. Med Hypotheses. 2010;74(6):1075–1080. doi:10.1016/j.mehy.2009.12.030
26. Canning BJ, Mazzone SB. Reflex mechanisms in gastroesophageal reflux disease and asthma. Am J Med. 2003;115(Suppl 3A):45s–48s. doi:10.1016/S0002-9343(03)00192-X
27. Demeter P, Pap A. The relationship between gastroesophageal reflux disease and obstructive sleep apnea. J Gastroenterol. 2004;39(9):815–820. doi:10.1007/s00535-004-1416-8
28. Gadel AA, Mostafa M, Younis A, Haleem M. Esophageal motility pattern and gastro-esophageal reflux in chronic obstructive pulmonary disease. Hepato-Gastroenterology. 2012;59(120):2498–2502. doi:10.5754/hge10433
29. Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2013;108(3):308–328; quiz 329. doi:10.1038/ajg.2012.444
30. Pandolfino JE, Kahrilas PJ. Smoking and gastro-oesophageal reflux disease. Eur J Gastroenterol Hepatol. 2000;12(8):837–842. doi:10.1097/00042737-200012080-00002
31. Kadakia SC, Kikendall JW, Maydonovitch C, Johnson LF. Effect of cigarette smoking on gastroesophageal reflux measured by 24-h ambulatory esophageal pH monitoring. Am J Gastroenterol. 1995;90(10):1785–1790.
32. El-Serag H, Hill C, Jones R. Systematic review: the epidemiology of gastro-oesophageal reflux disease in primary care, using the UK general practice research database. Aliment Pharmacol Ther. 2009;29(5):470–480. doi:10.1111/j.1365-2036.2008.03901.x
33. Ruzkowski CJ, Sanowski RA, Austin J, Rohwedder JJ, Waring JP. The effects of inhaled albuterol and oral theophylline on gastroesophageal reflux in patients with gastroesophageal reflux disease and obstructive lung disease. Arch Intern Med. 1992;152(4):783–785. doi:10.1001/archinte.1992.00400160085016
34. Crowell MD, Zayat EN, Lacy BE, Schettler-Duncan A, Liu MC. The effects of an inhaled beta(2)-adrenergic agonist on lower esophageal function: a dose-response study. Chest. 2001;120(4):1184–1189. doi:10.1378/chest.120.4.1184
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Causal Relationship Between Gastroesophageal Reflux Disease and Chronic Obstructive Pulmonary Disease: A Bidirectional Two-Sample Mendelian Randomization Study
Liu B, Chen M, You J, Zheng S, Huang M
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:87-95
Published Date: 10 January 2024