Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Relationship Between Cognitive Functions and Decision-Making Capacity in Older Institutionalized Patients with Schizophrenia: A Preliminary Study
Authors Sugawara N ![]() , Yasui-Furukori N
, Yasui-Furukori N ![]() , Yamada S, Aoki M, Takeuchi Y, Miyazaki K
, Yamada S, Aoki M, Takeuchi Y, Miyazaki K ![]() , Shimoda K
, Shimoda K ![]()
Received 24 January 2022
Accepted for publication 6 April 2022
Published 15 April 2022 Volume 2022:18 Pages 891—897
DOI https://doi.org/10.2147/NDT.S357067
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Norio Sugawara,1– 3 Norio Yasui-Furukori,1,3 Sonoko Yamada,3 Mei Aoki,3 Yoshitaka Takeuchi,1,4 Kensuke Miyazaki,5 Kazutaka Shimoda1
1Department of Psychiatry, Dokkyo Medical University School of Medicine, Tochigi, Japan; 2Department of Clinical Epidemiology, Translational Medical Center, National Center of Neurology and Psychiatry, Tokyo, Japan; 3Department of Neuropsychiatry, Hirosaki University, School of Medicine, Aomori, Japan; 4Shiseikai, Takizawa Hospital, Tochigi, Japan; 5Department of Neuropsychiatry, Hirosaki-Aiseikai Hospital, Aomori, Japan
Correspondence: Norio Sugawara, Department of Psychiatry, Dokkyo Medical University School of Medicine, 880 Kitakobayashi, Mibu, Tochigi, 321-0293, Japan, Tel +81-28-287-2153, Fax +81-28-286-5187, Email [email protected]
Background: Decision-making capacity for patients with psychiatric disorders is an important and controversial issue in clinical care settings. The aim of this study was to (1) evaluate the level of decision-making capacity of older institutionalized patients suffering from schizophrenia and (2) determine whether their diminished capacity is associated with specific aspects of cognitive impairment.
Methods: Using a cross-sectional design, we recruited 48 older institutionalized patients (mean age ± standard deviation: 60.0 ± 14.0 years) who were diagnosed with schizophrenia. Participants underwent the assessments by the MacArthur Competence Assessment Tool for Treatment (MacCAT-T) and the Japanese version of the Brief Assessment of Cognition in Schizophrenia (Japanese-BACS).
Results: The understanding summary scores of the MacCAT were found to have a significant positive correlation with the attention and verbal fluency subscale scores of the Japanese-BACS and negative correlations with age and duration of illness. In addition, the appreciation and reasoning summary scores had a significant negative correlation with age. In a linear regression model with a stepwise selection procedure, age, sex, and verbal fluency subscale scores were associated with understanding summary scores.
Conclusion: The generally poor cognitive performance of inpatients with chronic schizophrenia indicated that the informed consent process for their treatment might pressure these patients on the basis of cognitive demands. It is necessary for psychiatrists to assess individual decision-making capacity and to increase their patients’ involvement in the treatment process.
Keywords: cognitive function, competence to consent, decision-making capacity, schizophrenia
Introduction
Schizophrenia is a severe psychiatric illness that generally appears when a person is in his or her late teens and early twenties, with a lifetime prevalence of approximately 1% in the worldwide population.1,2 Although the longitudinal outcome of schizophrenia may be heterogeneous, a nonnegligible number of patients have a chronic course of illness.3,4 Schizophrenia has three types of symptoms: positive symptoms (delusions, hallucinations, and disorganized speech or behaviors), negative symptoms (restricted emotional expression and lack of motivation), and cognitive symptoms (dysfunction for processing speed, executive functions, and memory). When schizophrenia was first defined by Kraepelin, it was called dementia praecox, with a focus on cognitive alterations that accompanied other symptoms.5
Psychiatrists are required to obtain informed consent from their patients before initiating clinical care or research. Informed consent is premised on the disclosure of appropriate information to a patient who has the freedom and capacity to provide consent. Involving patients in the decision-making process is central to the debate on patient autonomy. In general, patients with following abilities are considered competent to provide consent: (1) an understanding of the situation, (2) an appreciation of the consequences of their decision; (3) reasoning in their thought process; and (4) the expression of a choice.6 Decision-making capacity for patients with schizophrenia is an important and controversial issue in clinical care settings. Several studies have shown that individuals with schizophrenia are less able to offer proper consent than those without it.7,8 However, a diagnosis of schizophrenia does not mean that individuals suffering from this disease are incompetent to consent.9 Previous studies investigating the association between decision-making capacity and symptoms of schizophrenia have suggested that competence to consent could be explained more largely by neurocognitive functioning than by the positive and negative symptoms of schizophrenia.10–12 However, most of these studies were conducted among relatively young patients.6 Although decision-making competence is impaired not only by disease but also by aging,13 there is limited information regarding the relationship between cognitive function and competence to consent among older patients with schizophrenia.
The objective of this study was to (1) assess the degree of decision-making competence of older institutionalized patients with schizophrenia and (2) investigate the association between specific domains of cognitive impairments and diminished competence. We hypothesized that specific cognitive function domains may be associated with decision-making competence among older patients with schizophrenia. To our knowledge, this is the first investigation focusing on the relationship between cognitive function and decision-making capacity among patients with schizophrenia in Japan.
Methods
Participants
Participants consisted of 48 patients (32 males and 16 females) who were diagnosed with either schizophrenia or schizoaffective disorder according to the 10th Revision of the International Classification of Diseases and Related Health Problems (ICD-10) or the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnostic criteria. Patient diagnoses were recorded from their medical charts, where psychiatrists responsible for the patients’ treatment established the diagnoses. We included patients admitted to three psychiatric hospitals in Japan between April 2018 and January 2019. Those who had a diagnosis of dementia were excluded. The participants were all prescribed antipsychotics. Prior to the initiation of the study, the study protocol was approved by the institutional review board of the ethics committee of Dokkyo Medical University School of Medicine (approval number: R-27-4J) and Hirosaki University School of Medicine (approval number: 2018-1096), and all participants provided written informed consent before voluntarily participating in the study. The study procedures were conducted according to the Japanese Ethical Guidelines for Medical and Health Research Involving Human Subjects and the Declaration of Helsinki.
Demographic and Clinical Characteristics
The medical records were reviewed to obtain data on demographics (age and sex), medical histories (duration of illness and length of hospital stay), current medications and amount of education. The doses of the antipsychotics were converted to chlorpromazine (CP) equivalent doses.14
Assessment of Decision-Making Capacity
To evaluate the patients’ competence to consent for their own treatment, we employed a semi-structured interview: the MacArthur Competence Assessment Tool for Treatment (MacCAT-T). In the interview process, relevant treatment information was disclosed for a patient, and the patient’s mental capacity regarding treatment decisions was evaluated.7 The MacCAT-T is validated in patients with schizophrenia,15 and is widely used for evaluating decision-making capacity in this population.16 Assessment of the MacCAT-T consists of four summary scores, which are named according to the dimensions of the treatment-related decision-making capacity as follows: (1) understanding (the ability to comprehend disclosed information regarding the condition and proposed treatment); (2) appreciation (the ability to appreciate the significance of the disclosed information for one’s own condition and situation); (3) reasoning (the ability to manipulate the relevant information rationally, eg, in comparing the risks and benefits of treatment options and the likely consequences of one’s choices); and (4) expression of a choice (the ability to arrive at and communicate a choice regarding a proposed treatment).12 Each summary score has a different score range: 0–6 for understanding, 0–4 for appreciation, 0–8 for reasoning, and 0–2 for expressing a choice. Although the MacCAT-T has no cutoff scores, a high score on the summary scale indicates that the patient has a better decision-making capacity.
Cognitive Assessment
Participants were administered the Japanese version of the Brief Assessment of Cognition in Schizophrenia (Japanese-BACS) according to a previous report.17 The BACS evaluates verbal memory (list learning), working memory (digit sequencing task), motor speed (token motor task), verbal fluency (category instances and controlled oral word association test), attention (symbol coding), and executive function (tower of London task). Based on Japanese healthy control subjects,18 z scores for each Japanese-BACS subscale were calculated from the raw scores.
Statistical Analysis
Descriptive analyses were conducted to characterize the patient demographic and clinical characteristics profile. The means ± SD or percentages data are used to summarize a group. Correlations were examined by Spearman’s rho test. The strength of the association is considered as very weak (0 to 0.19), weak (0.2 to 0.39), moderate (0.4 to 0.59), strong (0.6 to 0.79) or very strong (0.8 to 1). A linear regression model with a forced entry procedure was employed to examine the relationship between MacCAT-T understanding summary scores and the scores of six cognitive subscales of the Japanese-BACS. A linear regression model with a stepwise selection procedure was used to evaluate the effects of the scores of the six cognitive subscales of the Japanese-BACS, demographic variables (age, sex, and amount of education) and clinical variables (duration of illness, length of hospital stay, and total CP equivalent dose) on MacCAT-T understanding summary scores. A p value less than 0.05 (< 0.05) indicates statistical significance. There were no adjustments for multiple comparisons to avoid making a priori assumptions about group differences. We do not want to strongly control the rate of false positive findings at the expense of false negative findings.19 The results should be considered as exploratory findings. The analyses were conducted by using SPSS software for Windows Version 27 (IBM Corp., Armonk, NY, USA).
Results
Clinical and Demographic Characteristics
All 48 participants (32 male and 16 female) in this study were Japanese (Table 1). Their average age was 60.0 (SD = 14.0) years. The average illness duration and length of hospital stay of the participants were 34.1 (SD = 16.9) years and 12.6 (SD = 14.2) years, respectively. The average total CP equivalent dose was 792.8 (SD = 488.7) mg, and the average number of antipsychotics was 1.8 (SD = 0.7). The average years of schooling was 10.2 (SD = 1.7) years. The distribution of MacCAT-T summary scores is shown in Table 2. One participant marked perfect scores in four MacCAT-T dimensions, demonstrating that she was competent to consent.
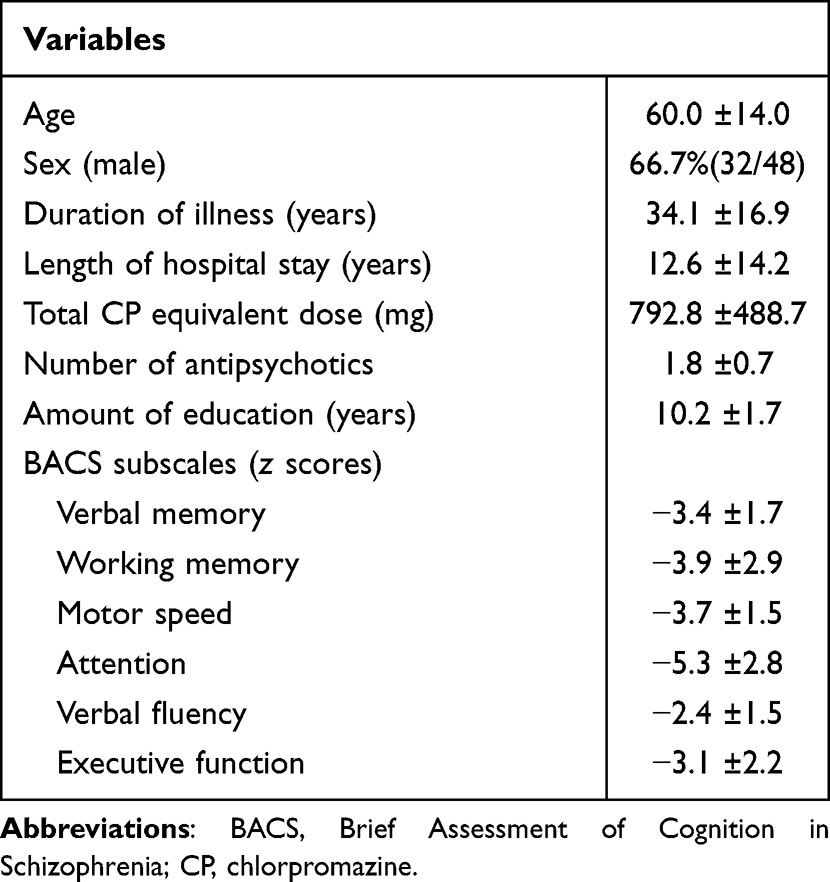 |
Table 1 Clinical and Demographic Characteristics |
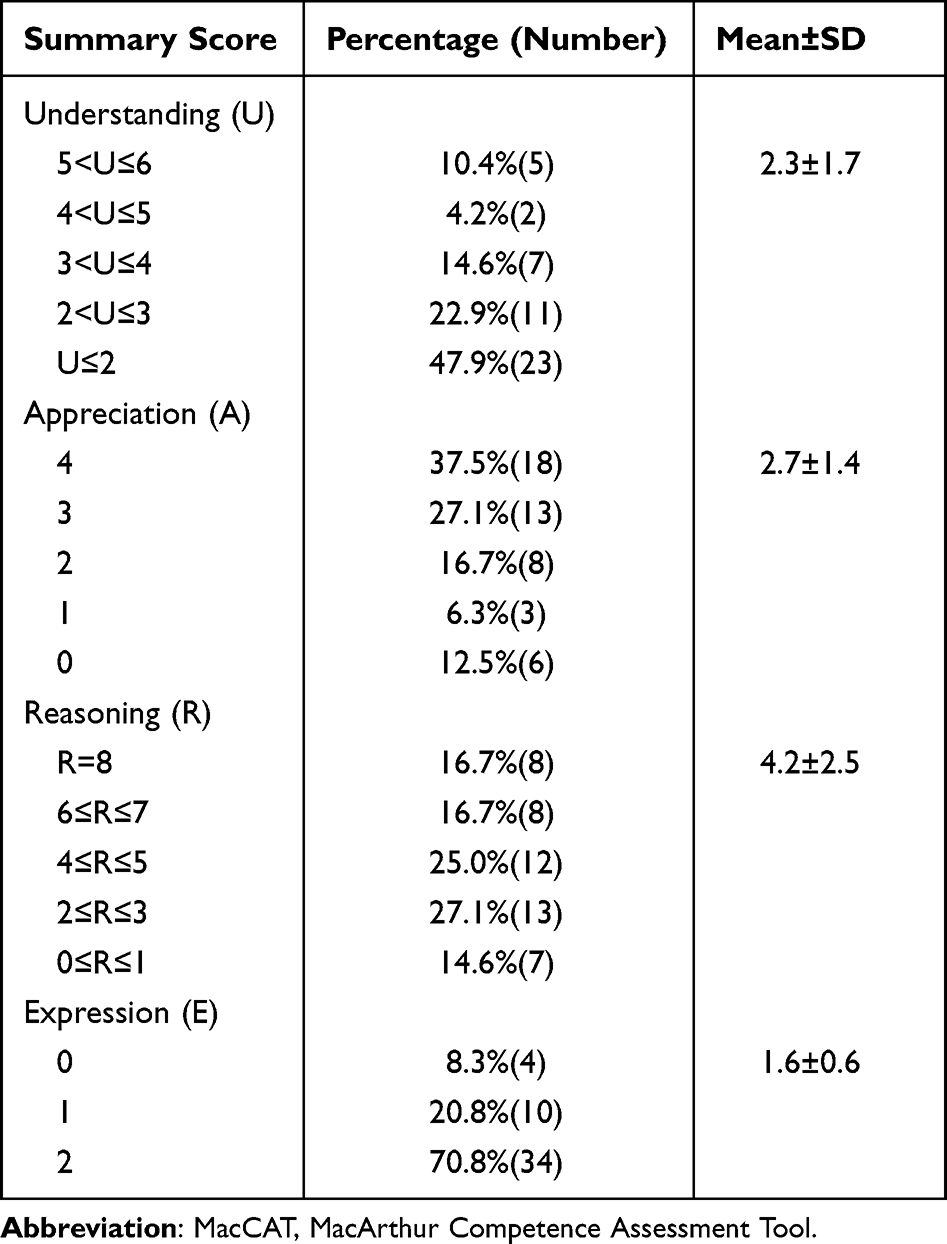 |
Table 2 Distribution of MacCAT-T Summary Scores |
Cognition and Decision-Making Abilities
Correlations between participants’ characteristics and MacCAT-T summary scores are presented in Table 3. The understanding summary scores of the MacCAT were found to have a significant positive correlation with attention and verbal fluency subscale scores of the Japanese-BACS and negative correlations with age and duration of illness. In addition, the appreciation and reasoning summary scores had a significant negative correlation with age.
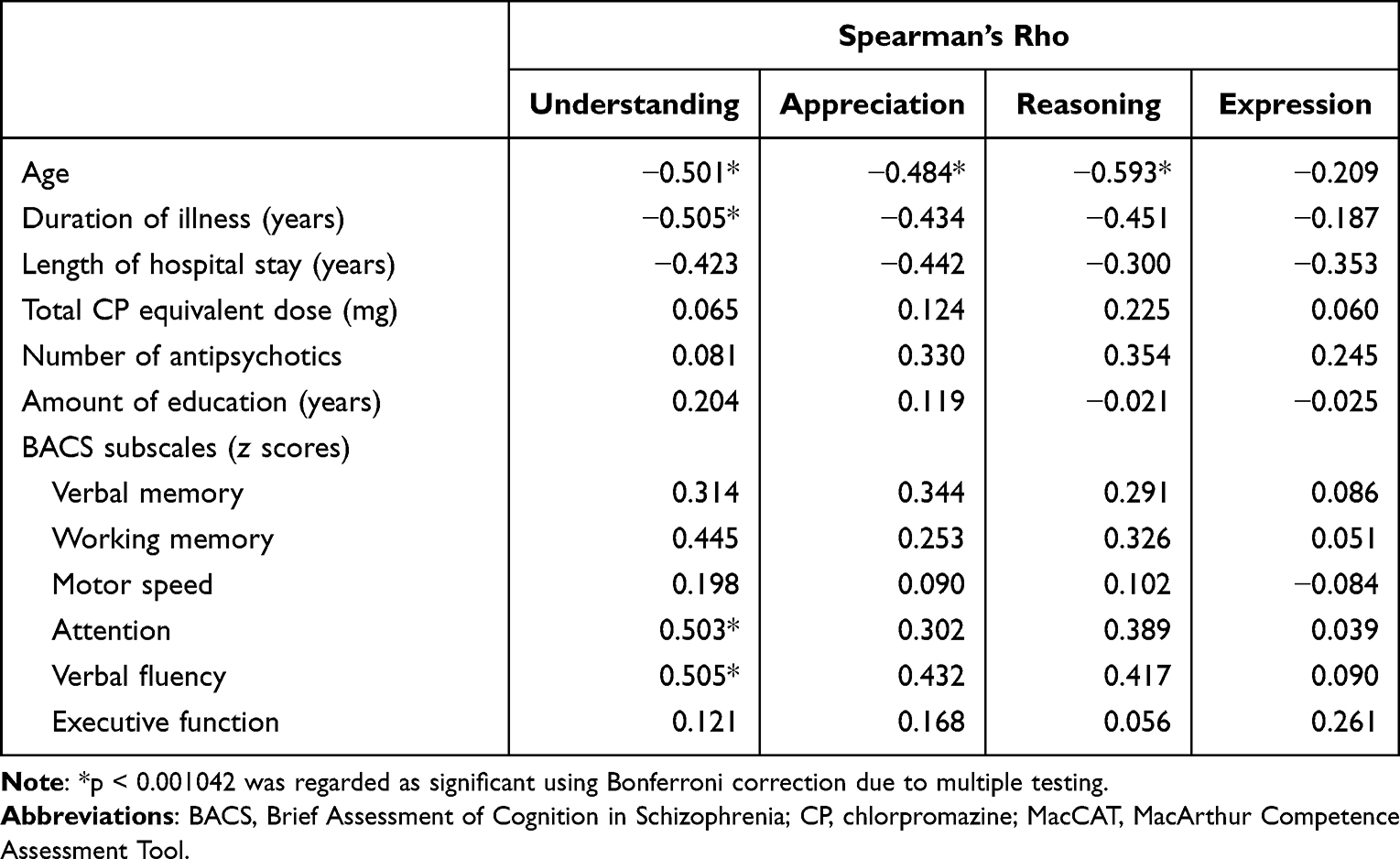 |
Table 3 Relationship of MacCAT Summary Scores to Observed Variables |
When a linear regression model consisted of all six cognitive subscales of the Japanese-BACS, 42% (adjusted R2 = 0.416; p < 0.001) of the variance in understanding summary scores of the MacCAT-T was accounted for by them. In a linear regression model with a stepwise selection procedure (adjusted R2 = 0.484; p < 0.001), age (beta = −0.366, p = 0.005), sex (being male) (beta = −0.253, p = 0.042), and the verbal fluency score of the Japanese-BACS (beta = 0.456, p = 0.001) were associated with MacCAT-T understanding summary scores.
Discussion
Competent patients have the right to make decisions about their treatment options, while incompetent patients also have to be protected from the potential harm of their choices. Psychiatrists have a responsibility to protect these two aspects of human rights. To promote adequate decision support, psychiatrists should have a comprehensive understanding of the degree of decision-making competence and the association between specific aspects of cognitive impairments and reduced capacity in patients with schizophrenia. In our results, 47.9% of participants had poor understanding summary scores (of 2 or less) on the MacCAT-T, while 64.6% of them had appreciation summary scores of 3 or more. Age, sex, and verbal fluency were associated with the MacCAT-T understanding summary scores in a linear regression model with a stepwise selection procedure.
In our results, nearly half of the participants had poor understanding summary scores on the MacCAT-T, and their mean score was 2.3. However, previous studies using the MacCAT-T have reported mean understanding summary scores that range from 4 to 6,12,20,21 and it seems that our participants had poorer understanding abilities than those in previous studies. One possible explanation for this outcome is the difference in the mean age of the participants. Older patients with schizophrenia might have poorer understanding abilities. In addition, the clinical setting of our participants, who were institutionalized patients, could explain the differences in the outcomes. A previous study, which reported lower cognitive function among institutionalized patients with schizophrenia, might support our results.22 Having a diminished ability to understand concepts cannot be equated with decisional incapacity. Thus, supported decision-making for older patients with schizophrenia is warranted.23
In contrast to a diminished ability to understand information on their treatment, our participants retained appreciation ability. The MacCAT-T appreciation summary scores showed participants’ abilities to appreciate not only the personal meaning of their own illness but also the probable consequences of treatment choices. The mean length of hospital stay of our participants was 12.6 years. Long-term institutionalization might have caused hospital dependency and elevated the MacCAT-T appreciation summary scores.24,25
In our analysis, verbal fluency was associated with MacCAT-T understanding summary scores. Verbal fluency is defined as the efficiency of planning and performing a sequence of nonautomatic actions under a given condition without repeating those actions.26 Cognitive self-control, efficient retrieval and recall of words, mental flexibility, multitasking, reaction initiation and inhibition are needed to carry out verbal fluency tasks.27 There have been no reports investigating the relationship between verbal fluency and competence to consent. Some studies have shown that lowered activity in the frontal lobes is associated with reduced verbal fluency performance among patients with schizophrenia.28,29 Interestingly, it has also been highlighted that schizophrenia patients have different characteristics of connections in the anterior cingulate cortex during the word fluency task.30 Because some factors, such as age or negative symptoms, might also affect verbal fluency,26 it is not easy to interpret the main causes of verbal fluency impairment in a clinical context.
Japan still has a hospital-centered mental health system, and its number of psychiatric beds per person is highest in the world.31,32 More than half of psychiatric inpatients had schizophrenia, and approximately 45% of inpatients with schizophrenia had been institutionalized for more than 5 years.33 In addition, mental healthcare systems in Japan are facing the problems of an increasing number of elderly patients with schizophrenia as the population ages.31 Because increasing age in patients with schizophrenia could increase physical comorbidities,34 assessment of patients’ decision-making competence could be more necessary for physicians and psychiatrists.
The current study also has several limitations. First, the parameters regarding patient characteristics were limited. This study focused on the association between specific aspects of cognitive impairments and reduced capacity in patients with schizophrenia. However, our study could not investigate the effect of positive and negative symptoms of schizophrenia. Clinical symptoms, as well as social cognitive abilities that were not assessed in our study, might increase the variance of decision-making capacity in the regression model. Second, this study was limited by its cross-sectional design. Thus, we could not determine causal relationships among variables. Third, the lack of associations detected among specific aspects of cognitive impairments and reduced capacity might be caused by statistical beta error. We could not completely rule this possibility due to our small sample size. Fourth, the imbalanced sex ratio in our study may have influenced the results.
In conclusion, our results show that inpatients with chronic schizophrenia have poor cognitive performance. Moreover, the informed consent process with higher cognitive demands might become a burden on older patients with schizophrenia. Our findings need to be verified in a larger sample of patients with schizophrenia. Furthermore, it is necessary for psychiatrists to assess individual decision-making competence and to increase their patients’ involvement in the treatment process.
Data Sharing Statement
Although the data underlying the study’s findings are anonymized, they contain potentially identifying or sensitive patient information. Under the ethical restrictions and legal framework of Japan, the data are unsuitable for public deposition. Please contact the Ethics Committees of Dokkyo Medical University School of Medicine and Hirosaki University School of Medicine, which have set restrictions on data sharing. Upon request, the ethics committees will assess whether researchers meet the criteria for access to confidential data.
Acknowledgments
The authors wish to acknowledge all coworkers for their help with the study.
Funding
Funding for this study was provided by a Grant-in-Aid for Scientific Research (C) (17K10347). The Ministry of Education, Culture, Sports, Science and Technology, Japan. The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
Dr Norio Sugawara reports grants from The Ministry of Education, Culture, Sports, Science and Technology, during the conduct of the study. Dr Kensuke Miyazaki reports personal fees from Sumitomo Dainippon Pharma Co., Ltd., outside the submitted work. Professor Kazutaka Shimoda reports grants from Novartis Pharma KK, Dainippon Sumitomo Pharma Co., Astellas Pharma Inc., Meiji Seika Pharma Co., Ltd., Eisai Co., Ltd., Pfizer Inc., Otsuka Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Takeda Pharmaceutical Co., Ltd.; personal fees from Eisai Co., Ltd, Mitsubishi Tanabe Pharma Corporation, Takeda Pharmaceutical Co., Ltd., Meiji Seika Pharma Co., Ltd., Janssen Pharmaceutical Co., Shionogi & Co. Ltd., Dainippon Sumitomo Pharma Co., Daiichi Sankyo Co., and Pfizer Inc., outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Marder SR, Cannon TD. Schizophrenia. N Engl J Med. 2019;381(18):1753–1761. doi:10.1056/NEJMra1808803
2. McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia-an overview. JAMA Psychiatry. 2020;77(2):201–210. doi:10.1001/jamapsychiatry.2019.3360
3. Ogawa K, Miya M, Watarai A, Nakazawa M, Yuasa S, Utena H. A long-term follow-up study of schizophrenia in Japan–with special reference to the course of social adjustment. Br J Psychiatry. 1987;151:758–765. doi:10.1192/bjp.151.6.758
4. Volavka J, Vevera J. Very long-term outcome of schizophrenia. Int J Clin Pract. 2018;72(7):e13094. doi:10.1111/ijcp.13094
5. van Os J, Kapur S. Schizophrenia. Lancet. 2009;374(9690):635–645. doi:10.1016/S0140-6736(09)60995-8
6. Sugawara N, Yasui-Furukori N, Sumiyoshi T. Competence to consent and its relationship with cognitive function in patients with schizophrenia. Front Psychiatry. 2019;10:195. doi:10.3389/fpsyt.2019.00195
7. Grisso T, Appelbaum PS, Hill-Fotouhi C. The MacCAT-T: a clinical tool to assess patients’ capacities to make treatment decisions. Psychiatr Serv. 1997;48(11):1415–1419. doi:10.1176/ps.48.11.1415
8. Jeste DV, Depp CA, Palmer BW. Magnitude of impairment in decisional capacity in people with schizophrenia compared to normal subjects: an overview. Schizophr Bull. 2006;32(1):121–128. doi:10.1093/schbul/sbj001
9. Okai D, Owen G, McGuire H, Singh S, Churchill R, Hotopf M. Mental capacity in psychiatric patients: systematic review. Br J Psychiatry. 2007;191:291–297. doi:10.1192/bjp.bp.106.035162
10. Stroup S, Appelbaum P, Swartz M, et al. Decision-making capacity for research participation among individuals in the CATIE schizophrenia trial. Schizophr Res. 2005;80(1):1–8. doi:10.1016/j.schres.2005.08.007
11. Carpenter WT, Gold JM, Lahti AC, et al. Decisional capacity for informed consent in schizophrenia research. Arch Gen Psychiatry. 2000;57(6):533–538. doi:10.1001/archpsyc.57.6.533
12. Palmer BW, Dunn LB, Appelbaum PS, Jeste DV. Correlates of treatment-related decision-making capacity among middle-aged and older patients with schizophrenia. Arch Gen Psychiatry. 2004;61(3):230–236. doi:10.1001/archpsyc.61.3.230
13. Curley A, Murphy R, Plunkett R, Kelly BD. Concordance of mental capacity assessments based on legal and clinical criteria: a cross-sectional study of psychiatry inpatients. Psychiatry Res. 2019;276:160–166. doi:10.1016/j.psychres.2019.05.015
14. Inada T, Inagaki A. Psychotropic dose equivalence in Japan. Psychiatry Clin Neurosci. 2015;69(8):440–447. doi:10.1111/pcn.12275
15. Raffard S, Lebrun C, Laraki Y, Capdevielle D. Validation of the French Version of the MacArthur Competence Assessment Tool for Treatment (MacCAT-T) in a French Sample of Individuals with Schizophrenia: validation de la version française de l’instrument d’évaluation des compétences MacArthur-traitement (MacCAT-T) dans un échantillon français de personnes souffrant de schizophrénie. Can J Psychiatry. 2021;66(4):395–405. doi:10.1177/0706743720966443
16. Wang SB, Wang YY, Ungvari GS, et al. The MacArthur Competence Assessment Tools for assessing decision-making capacity in schizophrenia: a meta-analysis. Schizophr Res. 2017;183:56–63. doi:10.1016/j.schres.2016.11.020
17. Kaneda Y, Sumiyoshi T, Keefe R, Ishimoto Y, Numata S, Ohmori T. Brief assessment of cognition in schizophrenia: validation of the Japanese version. Psychiatry Clin Neurosci. 2007;61(6):602–609. doi:10.1111/j.1440-1819.2007.01725.x
18. Kaneda Y, Sumiyoshi T, Nakagome K, et al. Evaluation of Cognitive Functions in a Normal Population in Japan using the Brief Assessment of Cognition in Schizophrenia Japanese version (BACS-J). Clini Psychiatry. 2013;55(2):167–175. (in Japanese). doi:10.11477/mf.1405102387
19. Rothman KJ. No adjustments are needed for multiple comparisons. Epidemiology. 1990;1(1):43–46. doi:10.1097/00001648-199001000-00010
20. Wong JG, Cheung EP, Chen EY. Decision-making capacity of inpatients with schizophrenia in Hong Kong. J Nerv Ment Dis. 2005;193(5):316–322. doi:10.1097/01.nmd.0000161685.54077.e4
21. Capdevielle D, Raffard S, Bayard S, et al. Competence to consent and insight in schizophrenia: is there an association? A pilot study. Schizophr Res. 2009;108(1–3):272–279. doi:10.1016/j.schres.2008.12.014
22. Gupta S, Steinmeyer C, Frank B, Lockwood K, Lentz B, Schultz K. Older patients with schizophrenia: nature of dwelling status and symptom severity. Am J Psychiatry. 2003;160(2):383–384. doi:10.1176/appi.ajp.160.2.383
23. Jeste DV, Eglit GML, Palmer BW, Martinis JG, Blanck P, Saks ER. Supported decision making in serious mental illness. Psychiatry. 2018;81(1):28–40. doi:10.1080/00332747.2017.1324697
24. Mishra SK, Mishra BR, Mishra S, Verma PK, Praharaj SK. Hospital dependency: an existing concept. Psychiatr Danub. 2010;22(4):548–549.
25. Reuben DB, Tinetti ME. The hospital-dependent patient. N Engl J Med. 2014;370(8):694–697. doi:10.1056/NEJMp1315568
26. Tyburski E, Sokołowski A, Chęć M, Pełka-Wysiecka J, Samochowiec A. Neuropsychological characteristics of verbal and non-verbal fluency in schizophrenia patients. Arch Psychiatr Nurs. 2015;29(1):33–38. doi:10.1016/j.apnu.2014.09.009
27. Henry JD, Crawford JR. A meta-analytic review of verbal fluency performance following focal cortical lesions. Neuropsychology. 2004;18(2):284–295. doi:10.1037/0894-4105.18.2.284
28. Fu CH, Suckling J, Williams SC, Andrew CM, Vythelingum GN, McGuire PK. Effects of psychotic state and task demand on prefrontal function in schizophrenia: an fMRI study of overt verbal fluency. Am J Psychiatry. 2005;162(3):485–494. doi:10.1176/appi.ajp.162.3.485
29. Takizawa R, Kasai K, Kawakubo Y, et al. Reduced frontopolar activation during verbal fluency task in schizophrenia: a multi-channel near-infrared spectroscopy study. Schizophr Res. 2008;99(1–3):250–262. doi:10.1016/j.schres.2007.10.025
30. Boksman K, Théberge J, Williamson P, et al. A 4.0-T fMRI study of brain connectivity during word fluency in first-episode schizophrenia. Schizophr Res. 2005;75(2–3):247–263. doi:10.1016/j.schres.2004.09.025
31. Ministry of Health, Labour and Welfare. Patient survey (in Japanese). Available from: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00450022&tstat=000001031167.
32. Organisation for Economic Cooperation and Development (OECD). Hospital beds (indicator); 2020. Available from: https://data.oecd.org/healtheqt/hospital-beds.htm.
33. Wakuda T, Takei N. ‘Opening doors’ for long-term institutionalised patients with schizophrenia in Japan. Acta Psychiatr Scand. 2021;143(3):277–278. doi:10.1111/acps.13269
34. Hsu MC, Lee SC, Ouyang WC. Use of Charlson comorbidity index and nomogram to predict mortality in elderly patients with late-life schizophrenia. Healthcare. 2021;9(7):783. doi:10.3390/healthcare9070783
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.