Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Reimagining Sexual Abuse Prevention for Adolescents with Intellectual Disabilities: A Scoping Review of Educational Gaps and Inclusive Future Directions
Authors Yati D ![]() , Hermayanti Y
, Hermayanti Y ![]() , Solehati T
, Solehati T ![]() , Fitri SYR
, Fitri SYR ![]()
Received 2 November 2025
Accepted for publication 4 March 2026
Published 21 April 2026 Volume 2026:19 578569
DOI https://doi.org/10.2147/JMDH.S578569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Dwi Yati,1,* Yanti Hermayanti,2,* Tetti Solehati,2 Siti Yuyun Rahayu Fitri3,*
1Doctoral Study Program in Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Indonesia; 2Department of Maternity Nursing, Faculty of Nursing Universitas Padjadjaran, Sumedang, Indonesia; 3Department of Pediatric Nursing, Faculty of Medicine, Hasan Sadikin Hospital, Universitas Padjadjaran, Sumedang, Indonesia
*These authors contributed equally to this work
Correspondence: Dwi Yati, Doctoral Study Program in Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Indonesia, Email [email protected]
Background: Sexual abuse remains a pervasive global public health concern, disproportionately affecting adolescents with intellectual disabilities (ID). While numerous educational interventions have been developed, most remain fragmented, context-specific, and rarely account for cultural and systemic disparities across settings. A comprehensive and inclusive synthesis is needed to reimagine prevention strategies for this vulnerable population.
Objective: This scoping review aimed to reimagine sexual abuse prevention by systematically mapping existing educational models, identifying gaps, and outlining inclusive future directions for adolescents with ID.
Methods: Following the PRISMA-ScR guideline, a comprehensive search was conducted across PubMed, Scopus, CINAHL, and ScienceDirect, supplemented by grey literature and reference list screening. Eligibility was guided by the PCC (Population–Concept–Context) framework. Studies published between 2015 and 2025 involving adolescents with diagnosed ID (aged 12– 18) were included. Data were thematically synthesized, and methodological quality descriptively assessed using the MMAT and JBI checklists.
Results: Sixteen studies met inclusion criteria, spanning diverse contexts from high-income to low- and middle-income countries. Interventions included school-based curricula, community workshops, digital platforms, and family-centered programs. While knowledge and awareness improved across most studies, evidence of sustained behavioral change was limited. Key gaps included inadequate cultural adaptation, limited caregiver involvement, and systemic barriers such as stigma and insufficient provider training. Although some programs demonstrated strong content validity, scalability and long-term effectiveness remain underexplored.
Conclusion: This review reimagines sexual abuse prevention as an inclusive, multi-level endeavor that extends beyond knowledge provision to engage caregivers, educators, and health systems. Future research must prioritize longitudinal designs, cultural tailoring, and systemic integration to build sustainable, equitable, and context-sensitive interventions.
Keywords: adolescents, educational models, intellectual disabilities, protective behavior, scoping review, sexual abuse prevention
Introduction
Sexual abuse is a pervasive global public health concern and disproportionately affects vulnerable populations, particularly adolescents with intellectual disabilities (ID). Adolescents with ID face heightened risk due to a combination of cognitive limitations, social vulnerabilities, and environmental barriers that impair their ability to recognize, resist, or report abuse.1,2 Evidence consistently indicates that young people with ID are more likely to experience sexual victimization compared to their non-disabled peers.3 In the United States, children with disabilities are sexually abused at nearly three times the rate of those without disabilities.4 Similar patterns are reported across Europe, where individuals with ID experience high rates of sexual exploitation, while institutional responses remain inadequate in terms of both prevention and protection.5,6
In low- and middle-income countries (LMICs), including Indonesia, the issue is compounded by underreporting, limited surveillance, and fragile protection systems. A 2021 survey by the Indonesian Ministry of Women’s Empowerment and Child Protection revealed that approximately 20% of children with disabilities had experienced various forms of violence, with adolescents being particularly vulnerable to sexual abuse.7 Alarmingly, many of these incidents occur in environments traditionally regarded as safe, such as schools, care institutions, or family homes, underscoring the systemic failure to protect adolescents with ID from exploitation. Contributing factors include limited access to comprehensive sexuality education, persistent stigma surrounding disability and sexuality, insufficient training among professionals, and weak implementation of legal protections.8,9
In response, a variety of educational interventions have been developed over the past decade, ranging from school-based curricula and community workshops to digital platforms and family-centered programs.10,11 These initiatives generally aim to enhance protective behaviors, improve communication skills, and foster awareness of bodily autonomy. However, the interventions remain highly heterogeneous in terms of content, delivery modes, theoretical frameworks, and targeted populations.12 Methodological shortcomings, including small sample sizes, limited follow-up assessments, short intervention durations, and lack of theoretical grounding, further constrain the evidence base. Importantly, most programs originate from high-income contexts, with minimal cultural adaptation or validation for LMIC settings.8,9,13 As a result, the scalability, sustainability, and cultural relevance of these interventions remain largely untested.11,14,15
Despite the growing body of work, there is still no comprehensive synthesis that systematically examines educational approaches to prevent sexual abuse among adolescents with ID, particularly within LMIC contexts. Previous reviews have either focused on general populations or narrowly assessed program outcomes in high-income countries.4 This absence of a unified framework hampers efforts to identify evidence-based, developmentally appropriate, and culturally sensitive practices that could inform both policy and practice. Adolescents with ID require tailored, inclusive interventions that address their unique developmental challenges, strengthen caregiver and educator engagement, and build systemic support mechanisms.8,16
Given the fragmented evidence, a scoping review is the most appropriate methodology to address these gaps. Scoping reviews allow for mapping diverse evidence without requiring uniform outcome measures, enabling the identification of critical gaps and emergent trends17,18 This review aims not only to catalog existing strategies but also to reimagine sexual abuse prevention for adolescents with ID by identifying educational gaps and outlining inclusive, culturally adaptable, and scalable future directions. In doing so, it seeks to provide a foundation for evidence-informed interventions, policy reform, and strengthened protection systems for this highly vulnerable population.
Methods
Study Design and Framework
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines17 and the methodological recommendations of the Joanna Briggs Institute.17,19 The aim was to systematically map and synthesize educational interventions designed to prevent sexual abuse among adolescents with intellectual disabilities (ID). A scoping review was chosen due to the heterogeneity of intervention designs, outcomes, and contexts, allowing the mapping of conceptual and contextual patterns while identifying gaps for inclusive and culturally sensitive future directions.
Eligibility Criteria
The inclusion and exclusion criteria were guided by the Population–Concept–Context (PCC) framework, as recommended by the JBI for scoping reviews.18,19
- Population: Adolescents aged 12–18 years diagnosed with intellectual disabilities according to standard diagnostic classifications using Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).20,21
- Concept: Educational interventions aimed at preventing sexual abuse. Eligible interventions sought to increase knowledge, promote protective behaviors, improve communication, and reduce vulnerability to sexual exploitation.
- Context: Studies conducted in formal and informal educational settings, including schools, clinics, community-based organizations, and family environments.
Eligible studies reported measurable outcomes related to knowledge, behavior, skills, or risk reduction. A broad range of designs were considered, including randomized controlled trials (RCTs), quasi-experimental, observational, qualitative, and mixed-methods studies. To capture both foundational and recent evidence, publications between January 2015 and May 2025 were included. Only peer-reviewed journal articles were synthesized to ensure methodological rigor, while non-English papers were excluded due to limited translation resources.
Information Sources and Search Strategy
A comprehensive search was conducted across four electronic databases: PubMed, Scopus, CINAHL, and ScienceDirect. The initial search was performed in April 2025 and updated on May 12, 2025. Both Medical Subject Headings (MeSH) and free-text terms were applied, using Boolean operators (AND, OR) to combine keywords such as “sexual abuse prevention”, “adolescents with intellectual disabilities”, “educational interventions”, and “educational strategies”. Detailed search strings for each database are provided in Table S1. To enhance comprehensiveness, although grey literature was screened to enhance comprehensiveness, no eligible sources met the inclusion criteria for synthesis. Supplementary searches were performed in Google Scholar and ProQuest Dissertations & Theses for grey literature, and reference lists of included studies were screened. However, only peer-reviewed journal articles were retained in the final synthesis.
Study Selection Proses
Study selection followed a two-stage screening process. In the first stage, two independent reviewers (DY and SY) screened titles and abstracts against the predefined PCC criteria. Studies were excluded if they targeted populations outside the eligible age range, lacked a focus on intellectual disability, or did not address sexual abuse prevention. In cases of disagreement, a third reviewer (YH) was consulted to reach consensus. In the second stage, full-text articles of potentially eligible studies were retrieved and assessed for final inclusion, with reasons for exclusion documented to ensure transparency. The screening process was supported by Rayyan, a web-based tool for systematic reviews, which enabled blinded screening, detection of reviewer conflicts, and systematic documentation of exclusion justifications. To assess the reliability of screening decisions, Cohen’s kappa statistic was calculated after each stage. The level of agreement between reviewers was substantial at the title and abstract screening stage (κ = 0.82) and almost perfect at the full-text review stage (κ = 0.91), indicating strong consistency and reliability in study selection.
Data Extraction
A standardized extraction form was developed based on JBI guidance to capture study characteristics and intervention details. The form included information on author, year, country, study design, sample size, participant characteristics (age, sex, type of intellectual disability), intervention components (materials, strategy, duration, delivery mode), comparison condition (if applicable), and outcomes (eg, knowledge acquisition, behavioral change, communication, or risk reduction). The form was piloted on a subset of studies to ensure clarity and consistency before full implementation. Two reviewers independently extracted data, and discrepancies were resolved through discussion or consultation with a third reviewer. This process ensured accuracy, reproducibility, and reliability of the extracted information.
Quality of Study Assessment
Although scoping reviews do not typically require formal quality assessment, this review applied the Mixed Methods Appraisal Tool (MMAT, 2018 version)22 to provide a descriptive evaluation of methodological rigor across the included studies. The purpose of the appraisal was not to exclude studies but rather to contextualize findings by identifying potential risks of bias that could affect interpretation. The MMAT was selected because it allows the appraisal of diverse study designs using a single framework, making it particularly suitable for a review that included randomized controlled trials, quasi-experimental studies, cross-sectional surveys, qualitative research, and mixed-methods designs. The MMAT appraisal was independently conducted by two reviewers for all included studies. Each study was categorized according to its design and assessed against the five design-specific MMAT criteria, rated as Yes, No, or Cannot tell. Discrepancies were resolved by discussion or with a third reviewer. Results were summarized descriptively, focusing on recurring methodological limitations rather than producing an overall score. This approach enabled the identification of common risks of bias (eg, lack of randomization, small sample sizes, non-validated instruments, and limited follow-up), which were narratively integrated into the synthesis to contextualize interpretation of findings.
Data Analysis
Due to the heterogeneity of study designs, interventions, and outcomes, a meta-analysis was not feasible. Instead, a narrative synthesis was employed using an inductive thematic approach. Extracted data were charted in evidence tables and then iteratively coded to identify recurring patterns, differences, and contextual influences. Studies were compared within and across intervention types to explore similarities and divergences. The synthesis was structured around thematic clusters including intervention delivery, effectiveness, moderators (eg, age, type of ID, cultural context), and systemic factors. In addition, methodological limitations identified through MMAT appraisal were integrated into the analysis to contextualize the robustness of findings. This approach allowed not only the identification of recurring themes but also the mapping of educational gaps and the development of inclusive pathways to reimagine sexual abuse prevention strategies for adolescents with intellectual disabilities.
Ethical Considerations
This review analyzed data from previously published studies and did not involve direct participation of human subjects; therefore, ethical approval was not required. All included studies had received ethical clearance from their respective institutions. The review adhered to principles of research integrity by ensuring accurate reporting, transparent methodology, and complete attribution of sources.
Results
Searching Results
The database search yielded 4261 records. After duplicate removal, 3112 records were excluded during title and abstract screening for not meeting the review objectives. The full texts of the remaining studies were assessed in detail, resulting in the exclusion of articles that did not target the eligible population, lacked a focus on sexual abuse prevention, or failed to report relevant outcomes. A total of 16 studies met all inclusion criteria and were included in the final synthesis. A PRISMA flow diagram summarizing the selection process is provided in Figure 1.
 |
Figure 1 PRISMA flow diagram. |
Characteristics of Included Studies
The included studies represented a broad geographical distribution, spanning high-income countries such as the United States,10,23–27 the United Kingdom,28 the Netherlands,29 Spain,30,31 and Germany.32 Importantly, evidence also emerged from low- and middle-income countries (LMICs) including Samoa,33 Brazil,34 Pakistan,35 Iran,36 and Indonesia,8 (Table 1). This geographical variation underscores both the global recognition of the issue and the diverse socio-cultural and systemic contexts in which prevention strategies are being developed and implemented.
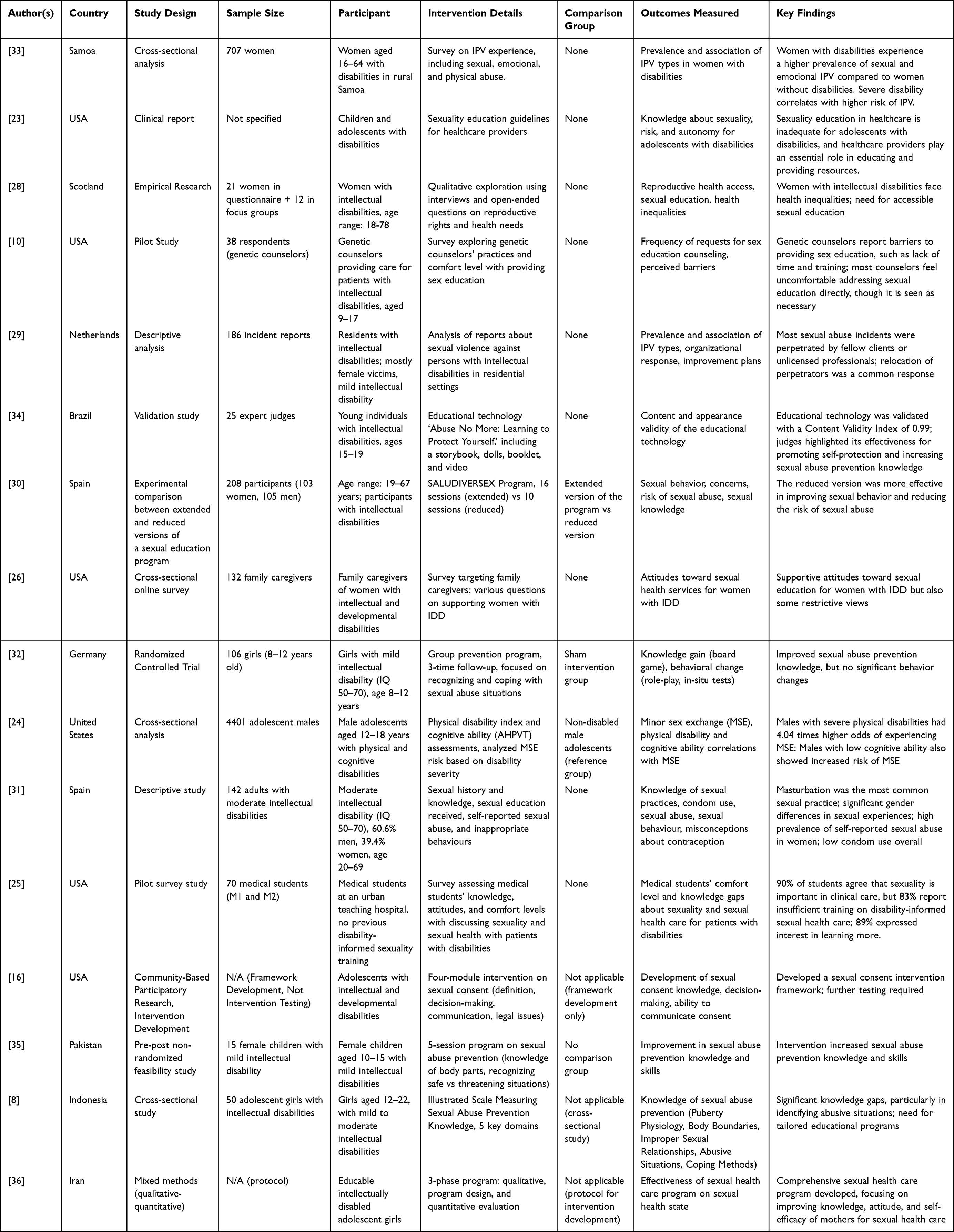 |
Table 1 Characteristics of Included Studies |
Study Designs and Methodological Approaches
The studies employed heterogeneous designs, reflecting the evolving and exploratory nature of research in this field (Table 1). These included randomized controlled trials,32 cross-sectional analyses,8,24,26,33 descriptive or exploratory designs,29,31 mixed-methods protocols,36 pre–post feasibility studies,35 validation studies,34 and participatory intervention development.27 Several studies targeted not only adolescents with ID but also healthcare professionals and caregivers, offering critical perspectives on system readiness and professional training.10,23,25,26
Sample Sizes and Populations
Sample sizes varied substantially across studies, reflecting differences in study aims (Table 1). Large-scale surveys, such as Franchino-Olsen et al24 with 4401 adolescent males with disabilities, provided population-level insights, while smaller feasibility or validation studies, including Warraitch et al (2021; n=15) and da Nóbrega et al (2021; n=25 expert judges), focused on program development or content testing. Most interventions involved adolescents with mild to moderate ID.8,31,32 Other studies extended to broader age groups,28,31 or targeted caregiver,26 healthcare providers,10,25 and medical students.23 Notably, some studies focused exclusively on female participants,8,35 aligning with evidence that females with disabilities are at heightened risk of sexual victimization.
Narrative Synthesis and Thematic Analysis
This review synthesized evidence from 16 studies that used diverse designs, populations, and intervention strategies to prevent sexual abuse among adolescents with ID (Table 1). Owing to heterogeneity in study designs and outcomes, a narrative thematic approach was employed to identify recurring patterns, differences, and contextual influences. Six overarching themes were identified: (1) elevated risk and prevalence of abuse, (2) systemic barriers in service provision, (3) strength of educational content and delivery formats, (4) individual-level moderators of intervention outcomes, (5) attitudes and perceptions of support networks, and (6) intervention development and research gaps.
Elevated Risk and Prevalence of Abuse
Consistent evidence confirmed that individuals with ID, particularly females, face disproportionately high rates of sexual and emotional abuse. Lowe et al33 documented elevated intimate partner violence among Samoan women with severe impairments, while Franchino-Olsen et al24 reported higher odds of minor sex exchange among male adolescents with severe cognitive or physical disabilities. Similarly, Estruch-García et al31 highlighted high rates of sexual abuse among women with moderate ID, compounded by limited knowledge of contraception and inconsistent condom use. These findings underscore the persistent global vulnerability of adolescents with ID and highlight the urgent need for preventive education tailored to this population.
Systemic Barriers in Service Provision
Several studies identified structural challenges that restrict access to appropriate sexual health education and protective services. In the Netherlands, Amelink et al29 found that sexual abuse in residential care settings was frequently perpetrated by peers or inadequately trained staff, with institutional responses often limited to relocation rather than accountability. US-based studies revealed critical training gaps among healthcare providers and students, with most lacking preparation in disability-informed sexual health.23,25 Grove et al10 similarly reported that genetic counselors, despite frequent parental requests for sexual education, felt unprepared due to time constraints and insufficient training. Collectively, these findings reveal systemic weaknesses that compromise effective prevention and reinforce the need for structural reforms in education and healthcare systems.
Educational Content and Delivery Formats
Interventions that were structured, engaging, and developmentally adapted demonstrated greater success in improving protective knowledge and awareness. The multimedia tool “Abuse No More”34 achieved a high Content Validity Index (0.99), supporting its potential utility for self-protection education. Warraitch et al35 showed that a five-session group program enhanced children’s ability to identify body parts and distinguish safe from unsafe situations. In Spain, Gil-Llario et al30 demonstrated that a shorter version of the SALUDIVERSEX program was more effective than the extended format in promoting safe sexual behaviors and reducing abuse risk. Collectively, these findings suggest that brief, focused, and interactive interventions may yield more consistent outcomes than generalized or lengthy programs.
Individual-Level Moderators
Intervention effectiveness varied according to age, gender, and severity of intellectual disability. Reis et al32 observed that while knowledge improved among girls aged 8–12 years with mild ID, behavioral change was inconsistent. Stobbe et al37 and Mansur et al8 similarly emphasized that adolescents with milder cognitive impairments benefited more from educational interventions than those with greater severity. These findings reinforce the importance of tailoring interventions to developmental capacity and communication needs.
Attitudes and Perceptions of Support Networks
Caregiver and family involvement emerged as a crucial factor shaping intervention outcomes. Powell et al26 identified ambivalent attitudes among US caregivers of women with IDD: while some supported sexual education, others expressed restrictive views that could inhibit open discussion. This highlights the dual role of caregivers as both facilitators and potential barriers, underscoring the necessity of parallel caregiver-focused education to foster enabling environments for adolescents with ID.
Intervention Development and Research Gaps
Several included studies were at the development or protocol stage, offering conceptual frameworks or tools rather than fully tested interventions. Greene et al27 proposed a four-module intervention on sexual consent covering communication, decision-making, and legal understanding, though validation remains pending. Goli et al36 developed a three-phase mixed-methods program targeting adolescent girls with ID and their mothers. In Indonesia, Mansur et al8 designed an illustrated knowledge scale, revealing persistent gaps in adolescents’ ability to recognize abusive situations. These developmental efforts illustrate promising directions but also underscore the scarcity of longitudinal trials, culturally adapted content, and rigorous evaluations in LMICs.
Quality of Study
The methodological quality of the included studies was heterogeneous (Table 2). Based on MMAT appraisal, randomized controlled trials and quasi-experimental studies demonstrated the highest rigor, with structured interventions and control groups supporting internal validity. However, even in these designs, gains in knowledge did not consistently translate into sustained behavioral change, underscoring a key gap between cognitive and applied outcomes. Feasibility and pre–post studies contributed valuable pilot evidence, especially for marginalized groups such as girls with ID in LMICs, but were limited by small sample sizes, absence of control groups, and short follow-up. Cross-sectional and descriptive studies primarily provided prevalence estimates and conceptual frameworks but lacked causal inference and standardized measures. Qualitative research enriched the evidence base with insights into lived experiences, caregiver attitudes, and systemic barriers, though reporting weaknesses (eg, unclear coding processes, lack of saturation) reduced analytic rigor. Validation studies, notably the “Abuse No More” tool,34 demonstrated strong methodological standards, while new instruments such as Mansur et al’s8 visual response scale require further psychometric testing. Mixed-methods approaches offered integrated perspectives but often lacked explicit justification of design and clarity on data integration. Across all study types, recurring methodological limitations included small sample sizes, short intervention durations, inadequate validation of outcome measures, and insufficient transparency in analytic procedures. These weaknesses limit the generalizability of findings, particularly in LMIC contexts, and highlight the need for more rigorous, culturally sensitive, and longitudinal research to inform sustainable prevention strategies.
 |
Table 2 Methodological Characteristics and Appraisal of the Included Studies |
Discussion
This scoping review mapped and synthesized evidence on educational interventions aimed at preventing sexual abuse among adolescents with intellectual disabilities (ID) published between 2015 and 2025. The review highlighted the breadth of methodological approaches, intervention formats, and implementation settings across diverse international contexts, while also identifying persistent educational gaps and underexplored areas. Beyond summarizing outcomes, this synthesis reimagines prevention by critically reflecting on what has been achieved, where limitations remain, and how future programs can move toward more inclusive and context-sensitive directions.
The review revealed considerable diversity in educational approaches to sexual abuse prevention for adolescents with intellectual disabilities. Interventions were implemented in varied settings, including schools38 and community programs,3 and employed multiple modalities such as simulations, audiovisual materials, and digital platforms.34 Consistent with earlier findings,30,39 most studies reported positive gains in knowledge and awareness. However, translation of cognitive gains into sustained protective behaviors remained inconsistent.32 This persistent knowledge–behavior gap underscores that information alone is insufficient. Effective prevention requires approaches that build self-efficacy, decision-making skills, and situational competencies, enabling adolescents to apply knowledge in real-world contexts.
Evidence indicated that intervention effectiveness varied according to age, severity of disability, and learning context. Adolescents with milder impairments and younger participants tended to demonstrate greater improvements compared with older youth or those with more profound disabilities.32,40 These findings reinforce the importance of developmentally tailored and ability-sensitive education, in line with inclusive pedagogical principles.41 Interventions that failed to adapt content to cognitive and communicative capacities often struggled to achieve meaningful behavioral outcomes.
Earlier reviews31,39,42 documented the urgent need for sexual education among individuals with ID and noted improvements in knowledge but inconsistent behavioral outcomes. The present review extends these findings in three important ways: 1) Knowledge–behavior gap as a central challenge: This review foregrounds the consistent pattern of limited behavioral change despite knowledge improvements, reframing prevention as a process of building empowerment and applied protective skills rather than merely delivering information. 2) Emerging innovations in pedagogy: The review highlights the increasing use of digital platforms, simulation-based learning, and hybrid delivery formats, which were rarely noted in prior syntheses. These approaches may enhance engagement and accessibility, though evidence of long-term impact remains limited. 3) Underrepresentation of LMIC contexts: This review emphasizes the striking scarcity of research from LMICs, despite disproportionately high risks in these regions. This gap reflects structural inequities in the evidence base and underscores the urgent need for culturally tailored, contextually feasible models of prevention. Most studies assessed outcomes only in the short term, limiting understanding of whether gains endure beyond immediate post-intervention periods. Evidence of sustained behavioral change, real-world application, and scalability remains sparse. Future research must incorporate longitudinal follow-up, validated outcome measures, and implementation studies to determine whether interventions can achieve durable protective effects in routine contexts.
A major gap identified in this review is the scarcity of evidence from low- and middle-income countries (LMICs), including Indonesia, Pakistan, and Brazil—settings where adolescents with intellectual disabilities may face heightened vulnerabilities due to stigma, fragile protection systems, and limited resources. Despite disproportionately high risks in these contexts, most prevention models have been developed in high-income countries and may not translate across sociocultural settings. Expanding research in LMICs is therefore essential to avoid reinforcing global disparities and to ensure that prevention strategies are both equitable and effective. Approaches grounded in cross-cultural validation, participatory co-design, and locally adapted evaluation frameworks are urgently needed. Such efforts are fundamental to advancing inclusive prevention strategies that reflect the lived realities of adolescents with ID and reduce inequities in global health and protection systems.10,34
In sum, this review advances the field by reframing sexual abuse prevention for adolescents with intellectual disabilities as a multidimensional endeavor that extends beyond knowledge delivery. It highlights three critical gaps: the persistent knowledge–behavior divide, the under-evaluated promise of innovative pedagogies, and the striking absence of culturally grounded evidence from LMICs. Together, these insights emphasize that prevention must be designed as an inclusive, participatory, and context-sensitive process that integrates educational innovation with systemic supports. Addressing these gaps is not only a research necessity but also a pressing public health and human rights imperative to ensure equitable protection for one of the world’s most vulnerable adolescent populations.
Study Limitations
This review has several limitations that should be considered when interpreting the findings. First, although the search strategy was comprehensive, restricting inclusion to English-language publications may have excluded relevant evidence from non–English-speaking regions, particularly low- and middle-income countries (LMICs) where this issue is highly pertinent. Second, substantial heterogeneity in study designs, intervention formats, and outcome measures precluded meta-analysis and limited the extent of cross-study comparisons. Third, while methodological rigor was descriptively appraised using the Mixed Methods Appraisal Tool (MMAT), the absence of formal quality grading—consistent with scoping review methodology—may affect the strength of conclusions regarding intervention effectiveness. Finally, several included studies were constrained by small or incompletely reported sample sizes, reliance on self-reported outcomes, and short follow-up periods, which may overestimate intervention effects and limit confidence in the sustainability and generalizability of findings.
Implications for Policy and Practice
Findings from this review underscore the need for policy frameworks that institutionalize sexual abuse prevention for adolescents with ID. Interventions must be embedded within school curricula, community programs, and caregiver training systems, supported by professional development for educators and healthcare providers. Policy efforts should also prioritize validated instruments, inclusive pedagogy, and cultural adaptability to ensure interventions are accessible, sustainable, and scalable. Prevention should be reframed not only as an educational task but also as a structural imperative tied to health promotion, disability rights, and child protection.
Conclusion
This scoping review mapped and synthesized studies on educational interventions for preventing sexual abuse among adolescents with intellectual disabilities. Findings revealed consistent gains in knowledge and awareness, yet limited evidence of sustained behavioral change. While digital, simulation-based, and hybrid formats offer promising innovations, their long-term effectiveness and scalability remain underexplored. Importantly, the evidence base is disproportionately skewed toward high-income countries, with a critical lack of research from LMICs where vulnerabilities are often greater. Future efforts should prioritize culturally adapted interventions, longitudinal evaluations, and participatory approaches that actively involve caregivers, educators, and adolescents themselves. Strengthening methodological rigor, policy integration, and global equity in program design is essential to ensure that prevention strategies are both inclusive and effective.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Acknowledgments
The author appreciates Universitas Padjadjaran, Bandung, West Java, Indonesia, for facilitating research and publication.
Funding
This research was funded through Padjadjaran University.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Blasingame GD. Risk assessment of adolescents with intellectual disabilities who exhibit sexual behavior problems or sexual offending behavior. J Child Sex Abus. 2018;27(8):955–14. doi:10.1080/10538712.2018.1452324
2. Byrne G. Prevalence and psychological sequelae of sexual abuse among individuals with an intellectual disability: a review of the recent literature. J Intellect Disabil. 2018;22(3):294–310. doi:10.1177/1744629517698844
3. Koçtürk N, Yüksel F. Individual and familial characteristics of sexual abuse victims with intellectual disability. Curr Psychol. 2023;42(3):2006–2013. doi:10.1007/s12144-021-01604-y
4. Murray BL. Sexual health education for adolescents with developmental disabilities. Health Educ J. 2019;78(8):1000–1011. doi:10.1177/0017896919859605
5. Malihi ZA, Fanslow JL, Hashemi L, Gulliver PJ, McIntosh TKD. Prevalence of nonpartner physical and sexual violence against people with disabilities. Am J Prev Med. 2021;61(3):329–337. doi:10.1016/j.amepre.2021.03.016
6. Willott S, Badger W, Evans V. People with an intellectual disability: under-reporting sexual violence. J Adult Protection. 2020;22(2):75–86. doi:10.1108/JAP-05-2019-0016
7. Data P. Informasi Kementerian Kesehatan RI (InfoDATIN). Hapuskan Stigma dan Diskriminasi terhadap Kusta Jakarta. 2018.
8. Mansur A, Neherta M, Fajria L, et al. Assessing sexual-abuse prevention knowledge and related factors among adolescent girls with intellectual disabilities in Padang: a cross-sectional study. Healthc Low Resour Settings. 2024;12(4). doi:10.4081/hls.2024.12370
9. da Silva MT, Hino P, Okuno MFP, Taminato M, Barbosa DA, Fernandes H. Successful strategies for preventing and controlling violence against people with intellectual disabilities: a scoping review. BMC Public Health. 2024;24(1):2807. doi:10.1186/s12889-024-20289-z
10. Grove L, Morrison-Beedy D, Kirby R, Hess J. The birds, bees, and special needs: making evidence-based sex education accessible for adolescents with intellectual disabilities. Sex Disabil. 2018;36(4):313–329. doi:10.1007/s11195-018-9547-7
11. Kim GH, Duan Y, Lee SC, Kim HS. Assessment of antioxidant activity of garlic (Allium sativum L.) peels by various extraction solvents. 한국유화학회지. 2016;33(1):204–212.
12. Ballan MS, Freyer MB. Autism spectrum disorder, adolescence, and sexuality education: suggested interventions for mental health professionals. Sex Disabil. 2017;35(2):261–273. doi:10.1007/s11195-017-9477-9
13. Hutchens J, Frawley J, Sullivan EA. The healthcare experiences of women with cardiac disease in pregnancy and postpartum: a qualitative study. Health Expect. 2022;25(4):1872–1881. doi:10.1111/hex.13532
14. Williams T, Anderson C. Social media’s impact on adolescent sexual behaviors: a critical review. Adolesc Res Rev. 2021;6(4):493–506.
15. Hempel S, Gore K, Belsher B. Identifying research gaps and prioritizing psychological health evidence synthesis needs. Med Care. 2019;57(10):S259–S264. doi:10.1097/MLR.0000000000001175
16. Greene A, Baugh M, Sherwood-Laughlin C, et al. Development of a sexual consent intervention for adolescents with intellectual and developmental disabilities. J Appl Res Intellect Disabil. 2024;37(5):e13272. doi:10.1111/jar.13272
17. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
18. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
19. Brennan SE, Munn Z. PRISMA 2020: a reporting guideline for the next generation of systematic reviews. JBI Evid Synth. 2021;19(5):906–908. doi:10.11124/JBIES-21-00112
20. Girimaji S, Pradeep AV. Intellectual disability in international classification of diseases-11: a developmental perspective. Indian J Soc Psychiatry. 2018;34(5):68. doi:10.4103/ijsp.ijsp_35_18
21. Lindsay WR, Steptoe L, McVicker R, Haut F, Robertson C. DSM IV, DSM-5, and the five-factor model: the diagnosis of personality disorder with intellectual and developmental disabilities. J Ment Health Res Intellect Disabil. 2018;11(1):1–15. doi:10.1080/19315864.2017.1350226
22. Hong QN, Pluye P, Fàbregues S, et al. Mixed methods appraisal tool (MMAT), version 2018. Registration Copyright. 2018;1148552(10):1–7.
23. Houtrow A, Elias ER, Davis BE, et al. Promoting healthy sexuality for children and adolescents with disabilities. Pediatrics. 2021;148(1):e2021052043. doi:10.1542/peds.2021-052043
24. Franchino-Olsen H, Silverstein HA, Kahn NF, Martin SL. Physical disabilities and low cognitive ability increase odds of minor sex exchange among adolescent males in the United States. J Child Sex Abus. 2022;31(8):967–986. doi:10.1080/10538712.2022.2146560
25. Murthy A, Hickey E, Pak JJ, Ahern T. Let’s assess how we talk about sex! Results from a single-institution pilot of an original survey that assesses medical student comfort, knowledge gaps, and barriers to speaking to patients with disabilities about sexuality and sexual health. J Sex Med. 2024;21(Supplement_1):
26. Powell RM, Albert SM, Nthenge S, Mitra M. Family caregivers’ attitudes and perspectives about the sexual and reproductive health of women with intellectual and developmental disabilities: an online survey. Am J Intellect Dev Disabil. 2024;129(2):135–150. doi:10.1352/1944-7558-129.2.135
27. Greene A, Simić Stanojević I, Sherwood-Laughlin C, et al. Teachers’ perceptions of barriers to implementing school-based sexual health education for students with intellectual and developmental disabilities. Am J Sex Educ. 2024;1–23.
28. Wiseman P, Ferrie J. Reproductive (in) justice and inequality in the lives of women with intellectual disabilities in Scotland. Scandinavian J Disabil Res. 2020;22(1):318–329. doi:10.16993/sjdr.677
29. Amelink Q, Roozen S, Leistikow I, Weenink JW. Sexual abuse of people with intellectual disabilities in residential settings: a 3-year analysis of incidents reported to the Dutch health and youth care inspectorate. BMJ Open. 2021;11(12):e053317. doi:10.1136/bmjopen-2021-053317
30. Gil-Llario MD, Fernández-García O, Huedo-Medina TB, Estruch-García V, Ballester-Arnal R. Analysis of the differential efficacy of the reduced version over the extended version of an affective-sexual education program for adults with intellectual disabilities. Arch Sex Behav. 2023;52(1):135–147. doi:10.1007/s10508-022-02407-3
31. Estruch-García V, Gil-Llario MD, Fernández-García O. Sexual experiences and knowledge of people with moderate intellectual disability. J Intellectual Disability Res. 2024;68(5):512–523. doi:10.1111/jir.13125
32. Reis O, Häßler F, Daubmann A, Chodan W. Knowledge hardly translates to reality—A randomized controlled trial on sexual abuse prevention for girls with intellectual disabilities. Front Psychiatry. 2022;13:886463. doi:10.3389/fpsyt.2022.886463
33. Lowe H, Utumapu MA, Tevaga P, Ene P, Mannell J. Disability and intimate partner violence experience among women in rural Samoa: a cross-sectional analysis. Disabil Health J. 2024;18(2):101735. doi:10.1016/j.dhjo.2024.101735
34. da Nóbrega KBG, de LC Marinus MW, Belian RB, Gontijo DT. Validation of the educational technology “abuse no more” for young people with intellectual disabilities. Cien Saude Colet. 2021;26(7):2793–2806. doi:10.1590/1413-81232021267.09032021
35. Warraitch A, Amin R, Rashid A. Evaluation of a school-based sexual abuse prevention program for female children with intellectual disabilities in rural Pakistan-A feasibility study. Appl Nurs Res. 2021;57:151391. doi:10.1016/j.apnr.2020.151391
36. Goli S, Noroozi M, Salehi M. A comprehensive sexual health care program for educable intellectually disabled adolescent girls: protocol for a mixed methods study. Reprod Health. 2018;15(1):141. doi:10.1186/s12978-018-0587-3
37. Stobbe KJ, Scheffers M, van Busschbach JT, Didden R. Prevention and intervention programs targeting sexual abuse in individuals with mild intellectual disability: a systematic review. J Ment Health Res Intellect Disabil. 2021;14(2):135–158. doi:10.1080/19315864.2021.1883780
38. Mdikana AA, Phasha NT. School-Based care and support for the intellectually disabled learners at risk for sexual abuse: South African teacher carer perspectives. J Psychol Afr. 2018;28(2):157–160. doi:10.1080/14330237.2018.1455304
39. Braathen SH, Rohleder P, Azalde G. Sexual and reproductive health and rights of girls with disabilities. SINTEF. 2017. Available from: https://www.sintef.no/globalassets/sintefteknologi.
40. Chodan W, Häßler F, Reis O. A randomized controlled trial on the effectiveness of a sexual abuse prevention programme for girls with intellectual disabilities: study protocol. Transl Dev Psychiatry. 2017;5(1):1407192. doi:10.1080/20017022.2017.1407192
41. Horner-Johnson W, Senders A, Tejera CH, McGee MG. Sexual health experiences among high school students with disabilities. J Adolesc Health. 2021;69(2):255–262. doi:10.1016/j.jadohealth.2021.03.001
42. Khemka I, Hickson L, Mallory SB. Evaluation of a decision-making curriculum for teaching adolescents with disabilities to resist negative peer pressure. J Autism Dev Disord. 2016;46(7):2372–2384. doi:10.1007/s10803-016-2770-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.