")
Back to Journals » Journal of Inflammation Research » Volume 16
Regulatory Effect and Mechanism of Erythroblastic Island Macrophages on Anemia in Patients with Newly Diagnosed Multiple Myeloma
Authors Huang H, Yu PY, Wei C, Li YW, Liang LJ, Liu YZ, Liu LN, Fang BJ, Wang YM
Received 31 March 2023
Accepted for publication 26 May 2023
Published 17 June 2023 Volume 2023:16 Pages 2585—2594
DOI https://doi.org/10.2147/JIR.S413044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Hao Huang,1,* Peng-Yang Yu,1,* Chen Wei,2 Yang-Wei Li,3 Li-Jie Liang,1 Yu-Zhang Liu,1 Li-Na Liu,1 Bai-Jun Fang,1 Yao-Mei Wang1
1Department of Hematology, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou, Henan, People’s Republic of China; 2Department of Internal Medicine, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou, Henan, People’s Republic of China; 3Central Laboratory, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yao-Mei Wang; Bai-Jun Fang, Email [email protected]; [email protected]
Objective: To examine the clinical characteristics and anemia-related factors in patients with newly diagnosed multiple myeloma (NDMM), as well as the effect and mechanism of erythroblastic islands (EBIs) and EBI macrophages in NDMM patients with anemia.
Methods: We collected and analyzed clinical data to find anemia-related factors. Using flow cytometry, the numbers and ratios of erythroblasts and EBI macrophages were determined. RNA sequencing (RNA-seq) was used to determine the differences of EBI macrophages in NDMM patients with or without anemia.
Results: Based on the clinical characteristics of NDMM patients with anemia, MCV, abnormal levels of albumin, osteolytic lesions, and Durie-Salmon (DS) stage are risk factors for anemia. Patients with anemia have fewer erythroblasts, erythroblastic islands (EBIs), and EBI macrophages in their bone marrow than patients without anemia. RNA-seq analysis of EBI macrophages from the bone marrow of patients with and without anemia revealed that macrophages from patients with anemia are impaired and tend to promote the production of interleukin-6, which has been demonstrated to be an essential survival factor of myeloma cells and protects them from apoptosis.
Conclusion: In NDMM patients with anemia, EBI macrophages are impaired, which causes anemia in those patients. Our finding highlights the significance of EBI macrophages in anemia in NDMM patients and provides a new strategy for recovery from anemia in these patients.
Keywords: anemia, central macrophages, erythroblastic islands, erythropoiesis, multiple myeloma
Introduction
Multiple myeloma (MM) is the second most common type of malignant tumor in the blood system, following lymphoma. It occurs in approximately 1% of malignant tumors and 10% of hematological tumors.1,2 MM is a malignant plasma cell proliferative disease characterized by abnormal proliferation of monoclonal plasma cells in the bone marrow. “CRAB”, which stands for hypercalcemia, renal insufficiency, anemia, and bone lesions, can be used to summarize the clinical manifestations.
More than 60% of newly diagnosed MM (NDMM) patients have anemia.3 Anemia, especially those forms that are difficult to recover from, suggests a poor prognosis.4 Moreover, the condition can have a long term impact on the quality of life of patients, as well as cause persistent organ damage to the body, which in turn affects normal therapy.5 Therefore, a deeper understanding of anemia and its treatment can both improve the health of patients and reduce the risk of other complications. However, current mechanistic studies on anemia caused by MM is still limited.
The microenvironment of erythroid development consists of erythroblastic islands (EBIs), which are composed of a central macrophage and several erythroblasts, where erythroblasts mature and enucleate to become red blood cells.6 Normal EBI macrophages stimulate erythropoiesis, maturation, and enucleation.7–12 However, changes to EBI central macrophages in cases of MM and their effects on erythroid development remain unknown. In this study, we examined the clinical characteristics and associated risk factors for anemia in 202 patients with NDMM, as well as the differences between erythroblasts in non-anemic and anemic patients. In addition, we also compared the EBI central macrophages of non-anemic and anemic patients and analyzed differences in the transcriptome data of these macrophages between the two groups. This aim of this study is to enhance the understanding of clinicians and scientific researchers regarding the symptoms of MM anemia, as well as provide a wider theoretical basis and further ideas for the development of treatment for anemia.
Methods
Clinical Data
From January 2013 to August 2020, a total of 202 newly diagnosed multiple myeloma patients were recorded at Henan Cancer Hospital. The diagnosis was based on the International Myeloma Working Group criteria.13 The patients were followed up until March 16th, 2021. Anemia is diagnosed if the hemoglobin levels are below the lower limit of “normal” by 20 g/L, or by an absolute value of less than 100 g/L according to diagnostic guidelines. Patients were divided into anemia and non-anemia groups. There were 115 cases in the anemia group and 87 cases in the non-anemia group. Details are provided in Table 1.
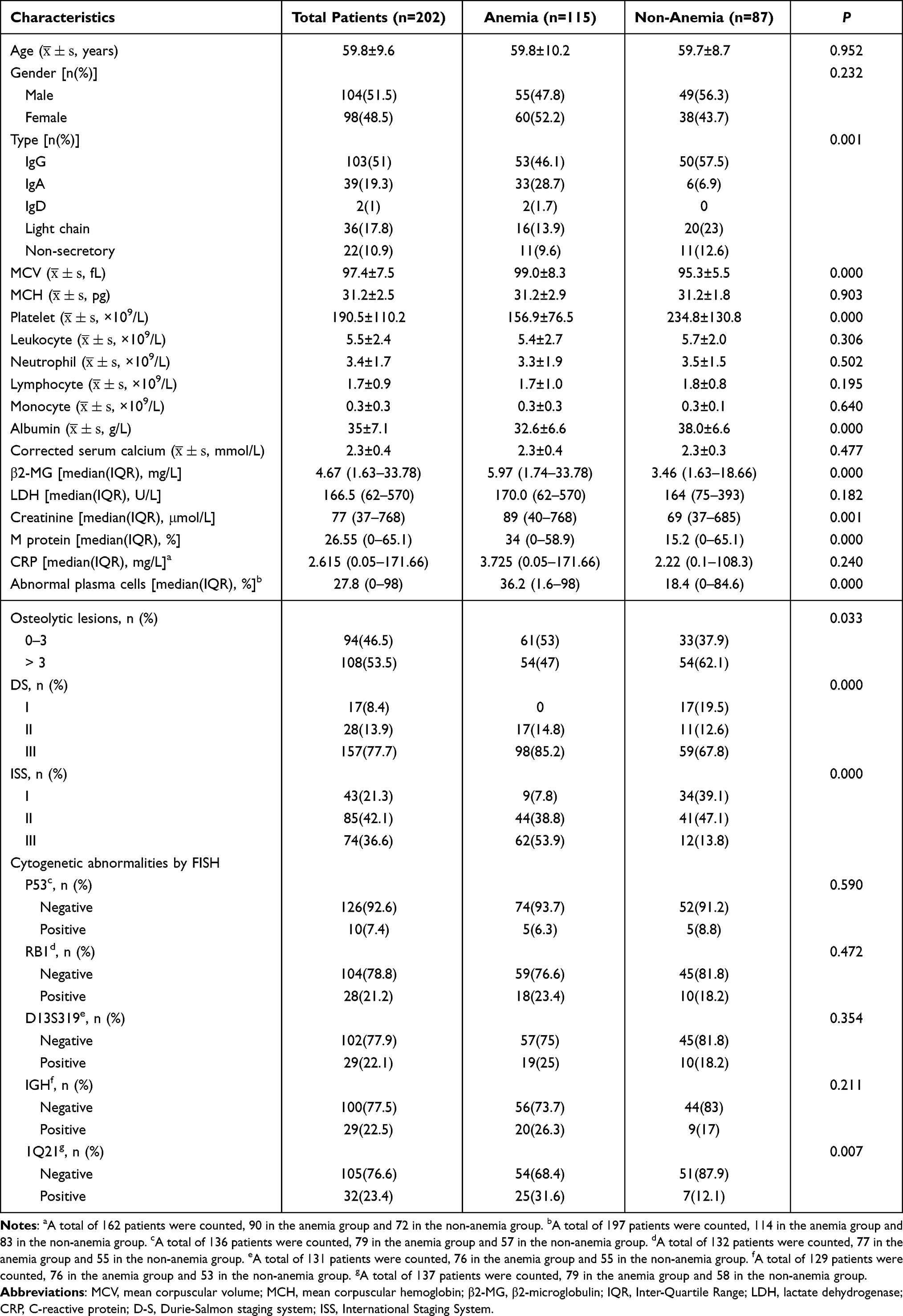 |
Table 1 General Information and Clinical Features of Patients with Newly Diagnosed Multiple Myeloma |
Preparation of Single-Cell Suspension from Bone Marrow
Twelve NDMM patients were selected based on the International Myeloma Working Group criteria and had not been treated. Those patients who were transfused or used drugs to revert anemia were excluded. Among them, six were with anemia and the others were without anemia. Their clinical characteristics were shown in Supplementary Table 1. Approximately 5 mL of bone marrow was aspirated into an anticoagulant EDTA tube during the initial bone marrow puncture for NDMM patients. Using a lymphocyte separation medium (human, Ficoll-Paque), mononuclear cells were obtained according to the manufacturer’s instructions.14 The bone marrow was diluted with 5 mL of phosphate buffered saline (PBS) and 5 mL of Ficoll-Paque was added in a 15 mL tube, which was then centrifuged at 400 g for 30 minutes at room temperature with no braking. The liquid was layered, with the second layer consisting of mononuclear cells. The mononuclear cells were transferred to a new 15 mL tube and centrifuged twice with PBS. This project has been approved by the Medical Ethics Committee of Henan Cancer Hospital (2021-KY-0017).
Flow Cytometry
Using flow cytometry, 2×106 mononuclear cells were analyzed for EBI central macrophages15 and erythrocytes. The cells were washed with PBS by centrifugation at 300 g, for 5 minutes at 4 °C, and then blocked for 10 minutes at room temperature with 90 μL of flow buffer (1× PBS + 0.5% bovine serum albumin) and 10 μL of blocking buffer (1× PBS + 0.5% bovine serum albumin + 0.4% human AB serum). To analyze the erythroid cells, the cells were stained with 2 μL of APC-Cy7-CD45 (Thermo Fisher), and 1 μL of APC-GPA (1:20 dilution, BD Pharmingen). To analyze the EBI central macrophages, the cells were stained with 1 μL of PerCP-Cy5-CD14 (Thermo Fisher), PE–Cy7-CD16 (Thermo Fisher), 1 μL of APC-CD163 (Thermo Fisher), 1 μL of PE-EPOR (R&D), and DAPI (Thermo Fisher). These cells were incubated for 15 minutes at room temperature and were kept away from light. For flow cytometry analysis, cells were washed once with a flow buffer and resuspended in 100 μL of flow buffer. For erythroid cell analysis, approximately 5 μL of 7-AAD (BD Pharmingen) was added to the samples to distinguish between living and nonliving cells.
Transcriptome Analysis
RNA was extracted from CD14+ cells purified using a magnetic-activated cell-sorting system that uses magnetic beads, according to the manufacturer’s instructions. The sequencing was performed at the Annoroad Gene Technology Institute using the Illumina platform and a PE150 strategy. The RNA samples and cDNA libraries were subjected to quality control. Using the Cuffdiff program, gene expression was analyzed pairwise. A volcano plot and gene ontology (GO) pathway were drawn with R.
Statistical Analysis
SPSS25.9 software was used for statistical analysis. The measurement data are expressed as mean ± SD or median (IQR) and two independent samples t-tests were used to compare data. The counting data are expressed as percentages, and the chi-squared test was used to compare them. Using binary logistic regression, independent correlation factors were analyzed, and P < 0.05 indicated that the difference was statistically significant.
Results
Clinical Characteristics of NDMM Patients with or Without Anemia
From January 2013 to August 2020, a total of 202 newly diagnosed multiple myeloma patients were enrolled at Henan Cancer Hospital. Among these patients, 115 presented anemia. Data including their age, gender, type, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), platelet, leukocyte, neutrophil, lymphocyte, monocyte, albumin, corrected serum calcium, β2 microglobulin (β2-MG), lactate dehydrogenase (LDH), creatinine, monoclonal protein, C-reactive protein (CRP), abnormal plasma cells, osteolytic lesions, Durie-Salmon (DS) stage, ISS stage and cytogenetic abnormalities were collected and are shown in Table 1. Anemia was diagnosed in patients with different types, different MCVs, fewer platelets, lower albumin, more β2-MG, higher creatinine, higher levels of M protein, more abnormal plasma cells, fewer bone lesions, and a distribution of different DS and ISS stages.
Analysis of Anemia-Related Factors in NDMM Patients
These statistically different factors and anemia were exposed to multivariable logistic regression in order to analyze the possible correlations between these risk factors and anemia. As shown in Table 2, there was a statistical difference between MCV, albumin, osteolytic lesions, and the DS stage, indicating that these are correlated anemia risk factors. We also compared the survival time of between patients with and without anemia. However, contrary to previous reports suggesting that anemia is a poor prognostic factor, our data showed no statistically significant difference in survival time between patients with and without anemia (Supplementary Figure 1).
 |
Table 2 Binary Multivariate Logistic Regression Analysis of NDMM with Anemia |
Erythropoiesis is Impaired in NDMM Patients with Anemia
Anemia is the phenotype in peripheral blood. To further learn about erythropoiesis in bone marrow where erythroblasts and red blood cells are produced, we performed flow cytometry analysis based on the expression of the erythroid-specific marker, GPA. The gating strategy is shown as Figure 1A. Six NDMM patients without anemia were analyzed (upper panel). Approximately 47.4% of live mononuclear cells in the bone marrow were CD45− cells, while 8.05% of CD45− cells were GPA+ cells (erythroblasts). However, only about 8.05% of live mononuclear cells were CD45− cells in the bone marrow of NDMM patients with anemia, and about 6.49% of CD45− cells were GPA+ cells (lower panel). The quantitative analysis is shown in Figure 1B. While there were 3.383±0.556% of GPA+ cells in live mononuclear cells in the bone marrow of patients without anemia, only 0.3413±0.087% were present in those with anemia, and the difference is statistically significant (P = 0.0087). These data indicate that erythropoiesis in the bone marrow of NDMM patients with anemia is significantly reduced.
 |
Figure 1 Erythroblasts in the bone marrow of NDMM patients. (A) Flow cytometry analysis of erythroblasts in the bone marrow of NDMM patients with and without anemia. (B) Statistical results of the ratio of erythroblasts to live cells in the bone marrow of NDMM patients with and without anemia. N=6. **p<0.01. |
EBIs and EBI Macrophages are Reduced in NDMM Patients with Anemia
Erythroblastic islands (EBIs) are the niche for erythropoiesis, and EBI central macrophages are essential for erythroblast development6,12,15 (refs). EBI central macrophages are immunophenotypically defined as CD14+CD16+CD163+EPOR+,15 as previously documented. Using this flow cytometry-based method, we analyzed EBI central macrophages in NDMM patients with and without anemia (Figure 2A).
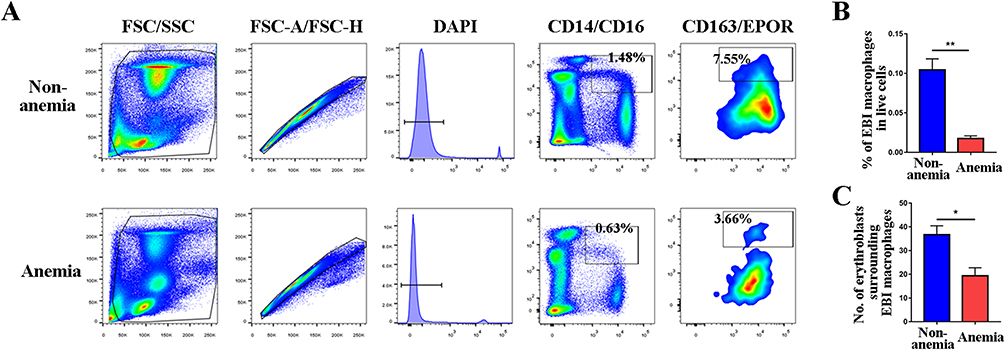 |
Figure 2 EBIs and EBI macrophages in the bone marrow of NDMM patients (A) Flow cytometry analysis of EBI macrophages in the bone marrow of NDMM patients with and without anemia. (B) Statistical results demonstrating the percentage of EBI macrophages in live cells in the bone marrow of NDMM patients with or without anemia. (C) The number of erythroblasts surrounding EBI macrophage in the bone marrow of NDMM patients with and without anemia. N=6. *P < 0.05. **P < 0.01. |
The representative gating strategy for patients without anemia is depicted in the upper panel of Figure 2A. The lower panel of Figure 2A shows the gating strategy for patients with anemia. While patients without anemia had approximately 1.48% of CD14+CD16+ cells in live mononuclear cells and 7.55% of CD163+EPOR+ cells in CD14+CD16+ cells, only 0.63% of CD14+CD16+ cells and 3.66% of CD163+EPOR+ cells were found in patients with anemia. Quantitative analysis is shown in Figure 2B. While there were 0.105±0.014% of EBI central macrophages in live mononuclear cells in the bone marrow of patients without anemia, only 0.018±0.003% were present in those with anemia, and the difference is statistically significant (P = 0.0037). According to this data, NDMM patients with anemia have a significant reduction in EBI central macrophages in their bone marrow.
The number of erythroblasts per EBI indicates the capacity of central macrophages to produce red blood cells. Therefore, we determined the number of erythroblasts surrounding the EBI central macrophage of patients with and without anemia (Figure 2C). The results indicate that there were approximately 36 erythroblasts per EBI in patients without anemia, but only 19 in patients with anemia. The difference is statistically significant (P = 0.02).
RNA-Seq Analyses Suggest EBI Macrophages in Anemia Patients are Impaired
To learn more about EBI macrophages in NDMM patients with anemia, we conducted RNA-seq analyses on the purified CD14+ cells from the bone marrow of NDMM patients with or without anemia. Principal component analysis showed clustering of three biological replicates of each population (Figure 3A), indicating that EBI macrophages from patients with or without anemia are distinct. Approximately 13,919 variables are depicted as a volcano plot (Figure 3B), with the genes listed in Supplementary Table 2.
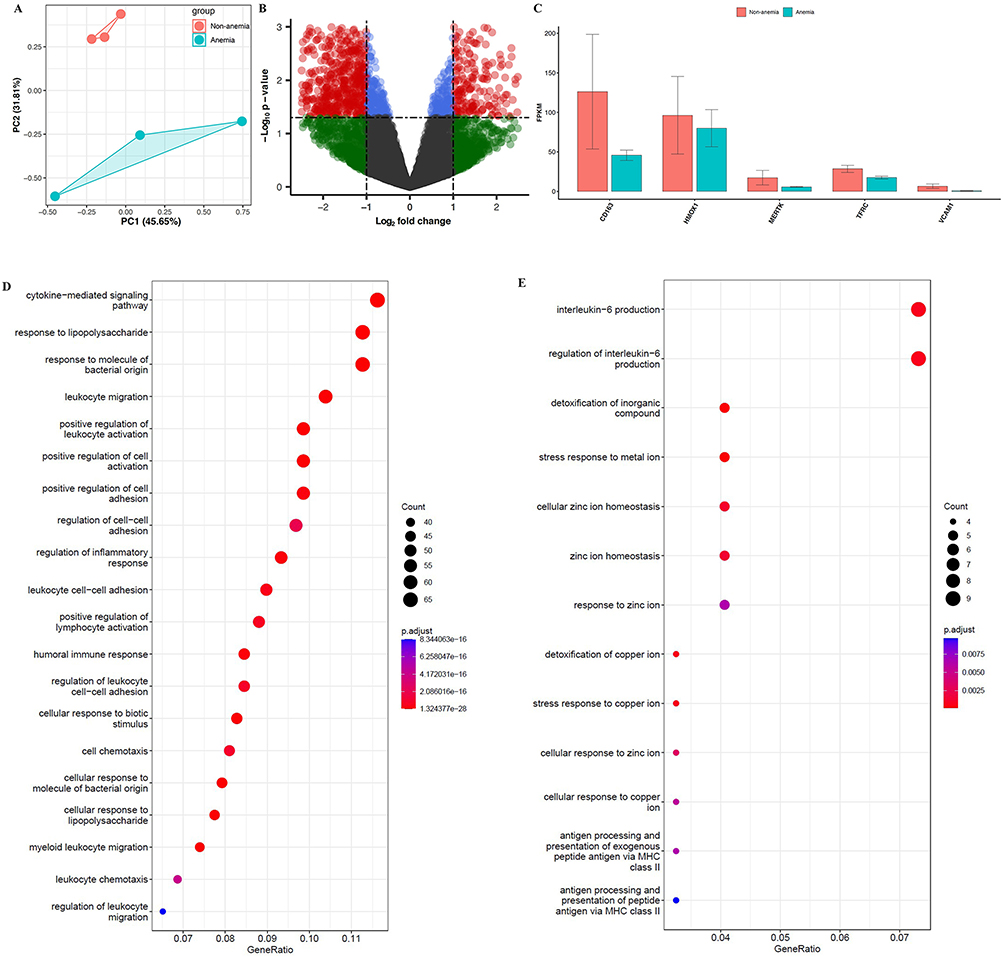 |
Figure 3 RNA-sequencing analysis of EBI macrophages from NDMM patients with or without anemia. (A) Principal component analysis. (B) The volcano plot. (C) The FPKM values for several key genes in EBI macrophages. (D) The most significantly upregulated pathways in EBI macrophages of patients without anemia. (E) The top upregulated pathways in EBI macrophages of patients with anemia; N=3. |
Afterwards, we compared several essential genes encoding proteins known to be essential for EBI macrophage function (Figure 3C). The adhesion molecules CD163 and VCAM1, were downregulated in patients with anemia. Iron metabolism-related genes such as heme oxygenase-1 (HMOX1) and transferrin receptor (Tfrc), as well as the nucleus engulfing tyrosine kinase MERTK, were all downregulated in patients with anemia. Gene ontology analysis of differentially expressed genes revealed that the cytokine-mediated signaling pathway, positive regulation of cell activation, and positive regulation of cell adhesion were the most upregulated pathways in EBI macrophages in patients without anemia (Figure 3D). However, interleukin-6 production and interleukin-6 production regulation are the two most significantly upregulated pathways in EBI macrophages in patients with anemia (Figure 3E). These findings strongly suggest that EBI macrophages in NDMM patients with anemia are impaired and tend to play roles in inflammation, rather than erythropoiesis regulation.
Discussion
MM is a form of hematological cancer with an abnormal proliferation of plasmocytes in the bone marrow. Approximately 60% of NDMM patients exhibit anemia, which worsens as the disease progresses. Eventually, almost all patients present anemia. The immune function and quality of life of MM patients are significantly affected by anemia, according to a previous study. The more severe the anemia, the more severe the immune dysfunction, and poor the quality of life of the patient. Therefore, in order to improve the therapeutic efficacy, quality of life, and prognosis of MM patients, it is crucial to conduct additional research into the mechanisms of anemia in NDMM patients to provide a stronger theoretical foundation and clinical treatment ideas.
Silvestris et al16,17 demonstrated that the levels of FasL and/or TRAIL in MM cells are upregulated and that the level of Fas in erythroid progenitors in advanced MM patients is significantly higher than in non-advanced patients. Anemia could result from FasL and/or TRAIL including apoptosis in these erythroid progenitor cells. Moreover, an abnormally high expression of cytokines such as interleukin (IL)-6,16,18 bone morphogenetic protein (BMP),19,20 and tumor necrosis factor (TNF)-α21–23 in the bone marrow inhibits the proliferation and differentiation of Burst-forming unit-erythroid cells (BFU-E). Reduced erythropoietin (EPO) production, malnutrition, and an accumulation of toxins due to renal insufficiency can also result in abnormal erythropoiesis or impaired hemoglobin synthesis.24,25 In addition, studies have shown that repeated infections and related hemolysis can lead to anemia.25,26
In this study, 115 (56.93%) of the 202 patients had non-treatment related anemia at the time of their initial diagnosis. We compared the clinical characteristics of NDMM patients with and without anemia to improve our understanding of the condition. The lack of a statistically significant difference between the mean ages of the anemia and non-anemic patients ((59.8±10.2) years vs (59.7±8.7) years, P = 0.952), and between different genders, indicate that anemia is a common symptom. IgG was the predominant antibody type in the anemia group (46.1%), followed by the IgA type (28.7%). The IgG type was also predominant in the non-anemia group (57.5%), but in this case, it was followed by the light chain type (23%); the proportion of IgA types in the anemia group was significantly higher than that in the non-anemia group (IgA type 6.9%), indicating that, in clinical work, patients with IgA should receive more attention to ensure the timely prevention of anemia and the provision of appropriate symptomatic support medication. The anemia group had fewer individuals with more than 3-level bone destruction, fewer platelets, higher levels of β2 microglobulin, higher creatinine, more M protein, and more abnormal plasmacytes.
Further statistical analysis indicated that MCV, albumin levels, number of osteolytic lesions and DS staging were identified as risk factors associated with anemia. This study demonstrates that the average MCV in patients with anemia is greater than that of patients without anemia; however, the presence of nutritional anemia still needs further research. Decreased albumin often indicates nutritional deficiencies, and studies have shown that prealbumin combined with serum iron and ferritin testing can diagnose iron deficiency anemia. The results of this study also revealed that there were fewer patients with a degree of bone damage of level 3 or more in the anemia group than that in the non-anemia group (47% vs 60%), which may be due to the fact that patients with bone destruction and bone lesions tend to seek medical attention before anemia develops. These results suggest that NDMM patients with anemia should undergo active nutritional evaluation and imaging tests to correct anemia as soon as possible.
Erythropoiesis is a genetically and environmentally controlled process. EBI, which consists of a central macrophage and several surrounding erythroblasts, is the erythropoietic niche discovered by Bessis in 1958.6 Its essential role during erythropoiesis was first demonstrated in rat models by Mohandas et al in 1978.12 A 2019 study, showed that Epor is the specific marker for EBI macrophages, to distinguish them from other macrophages.15
Based on these and other prior research, the results of our study reveals that, consistent with routine blood examination, the number of erythroid cells in the BM of NDMM patients with anemia is significantly lower than that of patients without anemia. The same can be seen with the number of EBI macrophages, which suggests that the ability of these macrophages to produce mature red blood cells in NDMM patients with anemia decreases significantly. Studies have shown that each EBI macrophage can bind to over 30 erythroid cells.27 To compare the carrying capacity of EBI macrophages in NDMM patients with or without anemia, we performed the appropriate calculations and found that each EBI macrophage in the bone marrow of NDMM patients without anemia bound approximately 36.71±3.704 erythroid cells, while the anemia group gave a result of 19.35±2.298, which was significantly lower than the normal level, indicating that the carrying capacity of EBI macrophages in NDMM patients with anemia decreases.
Results from RNA-sequencing show that EBI macrophages in NDMM patients with or without anemia are functionally distinct. These macrophages in patients without anemia play similar roles in erythropoiesis in patients without anemia as they do in healthy people; however, in patients with anemia, adhesion molecules, iron metabolism-related genes, and a nucleus engulfment-related gene were expressed at lower levels. Moreover, interleukin-6 (IL-6) production is the number one upregulated pathway in EBI macrophages in patients with anemia. Extensive research has demonstrated that IL-6 is an essential survival factor for myeloma cells and protects them from apoptosis,28–31 and inhibits the proliferation and differentiation of BFU-E. Thus, improving the ability of EBI macrophages to produce red blood cells may be a safer and more effective therapy for preventing and treating anemia.
Conclusion
In summary, more than half of NDMM patients present anemia. Albumin, abnormal plasma cells, bone destruction, and DS staging are all independent risk factors for NDMM anemia. Consequently, it is better to prevent or treat anemia in patients with these abnormal factors. Additional mechanistic studies have found that the hematopoietic microenvironment of EBI in the bone marrow of NDMM patients with anemia changes, the central macrophages are reduced, and the ability to bind erythrocytes is decreased. Bioinformatics reveal that EBI macrophages in these patients tend to promote IL-6 production rather than erythropoiesis. Therefore, it is anticipated that research into the effect of EBI central macrophages on erythroid development and the related drugs that improve binding of erythroid cells to EBI central macrophages to promote erythroid development will improve the survival, treatment, efficacy, and prognosis of patients with anemia.
Abbreviations
NDMM, newly diagnosed multiple myeloma; DS, Durie-Salmon; EBIs, erythroblastic islands; RNA-seq, RNA sequence; MM, multiple myeloma; PBS, phosphate buffered saline; GO, gene ontology; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; β2-MG, β2 microglobulin; LDH, lactate dehydrogenase; CRP, C-reactive protein; HMOX1, heme oxygenase 1; Tfrc, transferrin receptor; IL-6, interleukin-6; BMP, bone morphogenetic protein; TNF, tumor necrosis factor; BFU-E, Burst-forming unit-erythroid; EPO, erythropoietin.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of the Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital (No.2021-KY-0017). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
Henan Medical Science and Technology Research Program (No.SBGJ202002024); National Natural Science Foundation of China (No.81900108); Henan Province Young and Middle-aged Health Science and Technology Innovation Outstanding Young Talent Training Project (No. YXKC2022049); Henan Province Young and Middle-aged Health Science and Technology Innovation Leading Talent Training Project (No. YXKC2020007); Zhongyuan Science and Technology Innovation Leadership Program (No.214200510023).
Disclosure
The authors declare that they have no competing interests.
References
1. Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17:e328–e346. doi:10.1016/S1470-2045(16)30206-6
2. Kumar SK, Rajkumar V, Kyle RA, et al. Multiple myeloma. Nat Rev Dis Primers. 2017;3:17046. doi:10.1038/nrdp.2017.46
3. Paitan V, Alcarraz C, Leornado A, et al. Anemia Como Factor Pronóstico En Pacientes con Cáncer [Anemia as a prognostic factor in cancer patients]. Rev Peru Med Exp Salud Publica. 2018;35:250–258. Spanish doi:10.17843/rpmesp.2018.352.3171
4. Solmaz S, Uzun O, Sevindik OG, et al. The effect of haemoglobin, albumin, lymphocyte and platelet score on the prognosis in patients with multiple myeloma. Int J Lab Hematol. 2023;45:13–19. doi:10.1111/ijlh.13958
5. Ludwig H, Zojer N. Supportive care in multiple myeloma. Best Pract Res Clin Haematol. 2007;20:817–835. doi:10.1016/j.beha.2007.10.001
6. Bessis M. Île érythroblastique, unité fonctionnelle de la moelle osseuse [Erythroblastic island, functional unity of bone marrow]. Rev Hematol. 1958;13:8–11. French
7. Soni S, Bala S, Gwynn B, et al. Absence of erythroblast macrophage protein (Emp) leads to failure of erythroblast nuclear extrusion. J Biol Chem. 2006;281:20181–20189. doi:10.1074/jbc.M603226200
8. Rhodes MM, Kopsombut P, Bondurant MC, Price JO, Koury MJ. Adherence to macrophages in erythroblastic islands enhances erythroblast proliferation and increases erythrocyte production by a different mechanism than erythropoietin. Blood. 2008;111:1700–1708. doi:10.1182/blood-2007-06-098178
9. Chow A, Huggins M, Ahmed J, et al. CD169(+) macrophages provide a niche promoting erythropoiesis under homeostasis and stress. Nat Med. 2013;19:429–436. doi:10.1038/nm.3057
10. Porcu S, Manchinu MF, Marongiu MF, et al. Klf1 affects DNase II-alpha expression in the central macrophage of a fetal liver erythroblastic island: a non-cell-autonomous role in definitive erythropoiesis. Mol Cell Biol. 2011;31:4144–4154. doi:10.1128/MCB.05532-11
11. Hanspal M, Hanspal JS. The association of erythroblasts with macrophages promotes erythroid proliferation and maturation: a 30-kD heparin-binding protein is involved in this contact. Blood. 1994;84:3494–3504. doi:10.1182/blood.V84.10.3494.3494
12. Mohandas N, Prenant M. Three-dimensional model of bone marrow. Blood. 1978;51:633–643. doi:10.1182/blood.V51.4.633.633
13. Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15:e538–548. doi:10.1016/S1470-2045(14)70442-5
14. Ali AM, Huang Y, Pinheiro RF, et al. Severely impaired terminal erythroid differentiation as an independent prognostic marker in myelodysplastic syndromes. Blood Adv. 2018;2:1393–1402. doi:10.1182/bloodadvances.2018018440
15. Li W, Wang Y, Zhao H, et al. Identification and transcriptome analysis of erythroblastic island macrophages. Blood. 2019;134:480–491. doi:10.1182/blood.2019000430
16. Silvestris F, Tucci M, Cafforio P, Dammacco F. Fas-L up-regulation by highly malignant myeloma plasma cells: role in the pathogenesis of anemia and disease progression. Blood. 2001;97:1155–1164. doi:10.1182/blood.v97.5.1155
17. Silvestris F, Cafforio P, Tucci M, Dammacco F. Negative regulation of erythroblast maturation by Fas-L(+)/TRAIL(+) highly malignant plasma cells: a major pathogenetic mechanism of anemia in multiple myeloma. Blood. 2002;99:1305–1313. doi:10.1182/blood.v99.4.1305
18. Sharma S, Nemeth E, Chen Y-H, et al. Involvement of hepcidin in the anemia of multiple myeloma. Clin Cancer Res. 2008;14:3262–3267. doi:10.1158/1078-0432.CCR-07-4153
19. Andriopoulos B, Corradini E, Xia Y, et al. BMP6 is a key endogenous regulator of hepcidin expression and iron metabolism. Nat Genet. 2009;41:482–487. doi:10.1038/ng.335
20. Meynard D, Kautz L, Darnaud V, et al. Lack of the bone morphogenetic protein BMP6 induces massive iron overload. Nat Genet. 2009;41:478–481. doi:10.1038/ng.320
21. Buck I, Morceau F, Cristofanon S, et al. Tumor necrosis factor alpha inhibits erythroid differentiation in human erythropoietin-dependent cells involving p38 MAPK pathway, GATA-1 and FOG-1 downregulation and GATA-2 upregulation. Biochem Pharmacol. 2008;76:1229–1239. doi:10.1016/j.bcp.2008.08.025
22. Grigorakaki C, Morceau F, Chateauvieux S, Dicato M, Diederich M. Tumor necrosis factor alpha-mediated inhibition of erythropoiesis involves GATA-1/GATA-2 balance impairment and PU.1 over-expression. Biochem Pharmacol. 2011;82:156–166. doi:10.1016/j.bcp.2011.03.030
23. Pavese I, Satta F, Todi F, et al. High serum levels of TNF-alpha and IL-6 predict the clinical outcome of treatment with human recombinant erythropoietin in anaemic cancer patients. Ann Oncol. 2010;21:1523–1528. doi:10.1093/annonc/mdp568
24. Pasqualetti P, Collacciani A, Casale R. Circadian rhythm of serum erythropoietin in myelodysplastic syndromes. Eur Rev Med Pharmacol Sci. 2000;4:111–115.
25. Beguin Y, Yerna M, Loo M, Weber M, Fillet G. Erythropoiesis in multiple myeloma: defective red cell production due to inappropriate erythropoietin production. Br J Haematol. 1992;82:648–653. doi:10.1111/j.1365-2141.1992.tb06939.x
26. Macdougall IC, Cooper AC. Hyporesponsiveness to erythropoietic therapy due to chronic inflammation. Eur J Clin Invest. 2005;35(Suppl 3):32–35. doi:10.1111/j.1365-2362.2005.01528.x
27. Jin SH, Lee JE, Yun J-H, et al. Isolation and characterization of human mesenchymal stem cells from gingival connective tissue. J Periodontal Res. 2015;50:461–467. doi:10.1111/jre.12228
28. Wang LH, Yang XY, Zhang X, et al. Transcriptional inactivation of STAT3 by PPARgamma suppresses IL-6-responsive multiple myeloma cells. Immunity. 2004;20:205–218. doi:10.1016/s1074-7613(04)00030-5
29. Chatterjee M, Honemann D, Lentzsch S, et al. In the presence of bone marrow stromal cells human multiple myeloma cells become independent of the IL-6/gp130/STAT3 pathway. Blood. 2002;100:3311–3318. doi:10.1182/blood-2002-01-0102
30. Georgii-Hemming P, Strömberg T, Janson ET, et al. The somatostatin analog octreotide inhibits growth of interleukin-6 (IL-6)-dependent and IL-6-independent human multiple myeloma cell lines. Blood. 1999;93:1724–1731.
31. Spets H, Georgii-Hemming P, Siljason J, Nilsson K, Jernberg-Wiklund H. Fas/APO-1 (CD95)-mediated apoptosis is activated by interferon-gamma and interferon- in interleukin-6 (IL-6)-dependent and IL-6-independent multiple myeloma cell lines. Blood. 1998;92:2914–2923. doi:10.1182/blood.V92.8.2914
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.