")
Back to Journals » Patient Related Outcome Measures » Volume 12
Refractive Outcome of Cataract Surgery Done at University of Gondar Tertiary Eye Care and Training Center, North West Ethiopia
Authors Mengistu M, Admassu F, Wondale T, Tsegaw A
Received 28 February 2021
Accepted for publication 1 June 2021
Published 10 June 2021 Volume 2021:12 Pages 173—179
DOI https://doi.org/10.2147/PROM.S308816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Masresha Mengistu, Fisseha Admassu, Teshager Wondale, Asamere Tsegaw
Department of Ophthalmology, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Asamere Tsegaw
Department of Ophthalmology, College of Medicine and Health Sciences, University of Gondar, P.O.Box 196, Gondar, Ethiopia
Tel +251939912863
Email [email protected]
Purpose: According to World Health Organization (WHO), cataract is the leading cause of blindness and visual impairment throughout the world. Post-operative refractive error is one of the commonest reasons for poor visual outcome after cataract surgery especially in developing countries where the standard modern biometry equipments are not available. The objective of this study was to assess the refractive outcome of cataract surgery done at University of Gondar (UoG) Tertiary Eye Care and Training Center, North West Ethiopia.
Methods: A descriptive cross-sectional study was done on 66 patients who had undergone manual small incision cataract surgery (MSICS) and fulfilled the inclusion criteria at UoG Tertiary Eye Care and Training Center from July 15 2019 to October 15 2019.
Results: From 90 post-operatively refracted eyes, 58 (64.4%) eyes achieved a target refraction of ± 1.00 Diopter (D). The right and left eyes achieved mean post-operative refraction SE of − 0.073± 1.45D and − 0.93± 1.70 D, respectively. But only 54 (60%) eyes were implanted with the calculated IOL power and for the remaining 40% the calculated IOL was not available at the store. And the target (Good) post-operative uncorrected visual acuity (UCVA) and best corrected visual acuity (BCVA) was achieved in 66.7% and 82.2% eyes, respectively.
Conclusion: The post-operative refractive outcome after cataract surgery at the center is low. For over one-third of operated eyes, the calculated IOL was not implanted due to the absence of the required IOL power at the store and, therefore, a wide range of IOL power should be available at the center.
Keywords: cataract surgery, outcome, Gondar, Ethiopia
Introduction
Cataract is the leading cause of avoidable blindness worldwide. Global estimates from 2002 reported that cataract was responsible for almost half of the 37 million blind individuals.1 In developing countries, cataracts account for 50% of blindness, while in developed countries it accounts for 5% of blindness.2,3 According to the 2006 national Survey on Blindness, the national prevalence of blindness in Ethiopia was 1.6% and cataracts account for 49% of national blindness.4,5
Cataract blindness is associated with considerable disability and mortality, with economic and social consequences. It greatly affects the quality of life of both the blind and those who care for them.6–8
Cataract surgery is a successful and cost-effective intervention. The patients’ post-operative visual satisfaction, vision-related quality of life, ability to function in daily activities and their overall productivity mainly depends on the visual outcome.9–11
Post-operative refractive error is one of the commonest reasons for poor visual outcome after cataract surgery.12 Unintended post-operative refractive error may be the result of a pre-operative error in measurement of axial length, error in keratometry reading, incorrect formula choice, wrong IOL insertion, incorrect positioning of IOL or post-operative induced astigmatism.11,13–15 Post-operative refraction is one of the best measures of cataract surgery outcome. Attaining a target post-operative refraction increases the number of operations by promoting eye care as well as increasing demand for operation.
Benchmark standards for National Health Service of England dictate that 85% of eyes should be within 1D and 55% within 0.5D of target spherical equivalent (SE) refraction following cataract surgery.13
A study from India about reduction in astigmatism after MSICS through change of incision site on patients showed that the mean astigmatism induced by surgery was 1.28 D × 2.9 degrees for superior incision, 0.20 D × 23.7 degrees for supero-temporal incision and 0.37 D × 90 degrees for temporal incision. The study found that induced astigmatism was lower in the temporal and supero-temporal groups compared to that in the superior group.16
A study done on visual outcome after cataract surgery in Nigeria on 184 consecutive patients revealed that the best corrected vision after refraction eight weeks post-operatively showed that 127 patients (78.8%) had good vision while 28 patients (17.4%) had borderline vision, and six patients (3.8%) had severe visual impairment after refraction. Uncorrected refractive error was the commonest cause of poor vision prior to refraction.17
A prospective observational study of all routine extracapsular cataract extractions with posterior chamber lens implants carried out at Kikuyu Eye Unit, Kenya, revealed the average SE of about –1.5D and the mean post-operative cylinder of 2.16D.18
A retrospective study from Nigeria revealed post-operative spherical refractive error ranging from −6.75D to +4.50D (mean 1.61 ± 1.41D) while cylindrical error ranged from 0.00DC to 6.00DC (mean 2.33 ± 1.80DC).19
According to 2017 data obtained from University of Gondar (UoG) Tertiary Eye Care and Training Center, the annual number of cataract surgeries done at the base hospital and outreach sites was 8064. Even though large number of cataract surgeries is done at the center annually, the refractive outcome is not known. This study was aimed at determining the refractive outcome of cataract surgery performed in the study center.
Patients and Methods
Study Design and Period
A cross-sectional descriptive study was conducted to assess the refractive outcome of cataract surgery at the UoG Tertiary Eye Care and Training Center, North West Ethiopia from July 15 2019 to October 15 2019.
Study Area
The study was conducted at the UoG Tertiary Eye Care and Training Center, a major eye care and training center in Ethiopia. It is an ophthalmic referral center for an estimated 14 million people living in North-West Ethiopia. The center provides eye care services both at base hospital and rural outreach sites. The base hospital has 8 outpatient clinics, facilities for in-patient care with 30 beds and five operation theatres. Currently, the center has 10 ophthalmologists, 5 of them with subspecialty fellowship training. There are also 26 Ophthalmology residents, 21 optometrists, 5 ophthalmic officers, and 29 general clinical nurses actively working in the outpatient clinics and operation theatres of the Tertiary Eye Care and Training Center.
Study Population
All patients who had undergone cataract surgery at the base hospital and fulfilling the inclusion criteria during the study period were included in the study.
Inclusion Criteria and Exclusion Criteria
Inclusion Criteria-Patients above 18 years and older for whom cataract surgery was done at the study center.
Exclusion Criteria
Any patients who were not willing to participate in the study
Any degree of corneal opacity
Sublaxated or Dislocated IOL
Any retinal or optic nerve disease and other ocular comorbidity
Post-operative day earlier than fifth week
Those patients who lack complete recording of biometry
Sample Size Determination
All patients who fulfilled the inclusion criteria during the study time were included.
Operational Definitions
Good visual acuity; BCVA of better than 6/24
Borderline visual acuity; BCVA of 6/24–6/60
Poor visual acuity; BCVA of worse than 6/60
SE; the sum of spherical and one half of the Cylinder power
Emmetropia; Post-operative refraction SE ±0.5D
Hyperopia; Post-operative refraction SE >+0.5D
Myopia; Post-operative refraction SE<-0.5D
Astigmatism; Post-operative refraction cylinder less than or greater than ±1D
Mature cataract – Cataract dense enough to prevent visualization of the retina
Target Refractive Outcome; To achieve Post-operative refraction within ±1D in at least 85% of operated eyes.13
Surgical Technique
Cataract surgery was done after obtaining informed consent. Keratometry reading was obtained by using auto refractor (Righton retinomax K plus 3 autorefractor, Hutama Medical, Indonesia) and axial length was measured by using a contact A scan (Pac Scan 300A contact A scan ultrasound, Sonomed Escalon, NY, USA). After entering keratometry readings into A-scan ultrasound, the IOL power was calculated by using SRK/T formula and A constant 118.5. The eye to be operated was marked by placing a piece of plaster on the eye brow and the eye lashes were trimmed. After the eyes were anesthetized with retrobulbar anesthesia, the periocular area was cleaned with 10% povidone iodine and draped. Speculum was inserted and then by using operating microscope superior or temporal incision was made to perform conjunctival peritomy using conjunctival scissors and bleeding was controlled by gently applying boll-point cautery.
A 6–7 mm Scleral incision was made 2 mm away from the limbus using a crescent blade and a 3–4 mm long and 6–7 mm wide sclera-corneal tunnel was created using a crescent blade and anterior chamber was entered using a Keratome knife.
Anterior chamber was maintained using methyl cellulose visco elastics and then can opener anterior capsulotomy was done. After capsulotomy, hydro dissection was done and the nucleus delivered into anterior chamber by flipping it up. Lens loop was used to deliver the nucleus of the cataractous lens out of the anterior chamber. Remnant lens cortical remnant was washed from anterior chamber by using Simcoe cannula. Then the IOL was inserted into the posterior capsular bag. Visco elastic substances, which was used to form the anterior chamber and protect the corneal endothelium during each step, was washed out and anterior chamber was formed using normal saline. Finally combination of antibiotic and steroid was injected into the sub-conjunctival space as prophylaxis for infection and reduce post-operative inflammation. All surgeries were done by senior ophthalmologists. Biometry was done by junior (1st and 2nd year) residents.
Data Collection Procedure
Data were taken using a structured and pretested questionnaire which contains socio-demographic data, clinical history, visual acuity (UCVA and best corrected visual acuity [BCVA]), biometric readings and post-operative refractive power of patients. Post-operative objective and subjective refraction was done by senior optometrists. All data were collected by ophthalmologists.
Data Analysis Procedure
After completion of data collection, the data were cleaned, coded and entered into Statistical Package for Social Sciences (SPSS) version 21.0 and analyzed. Independent variables were Age, Sex, Address, Occupation, Type of cataract, Incision site and the dependent variable was Refractive outcome.
Descriptive statistical analysis was performed and percentages, standard deviation, means and medians were used to describe the findings. Results were displayed in tables. An Independent Sample t-test was computed to compare between means of different groups for significant differences. P value of 0.05 was used to determine statistical significance.
Ethical Consideration
Ethical clearance was obtained from the Ethical Review Board of the UoG. All methods were adherent to the tents of the Declaration of Helsinki principles for research in humans. Informed verbal and written consent were taken from the study participants.
Results
Socio-Demographic Characteristics
The study included a total of 90 eyes (45 right eyes and 45 left eyes) of 66 patients. The male to female ratio was 1.3:1. Most of the patients were in the age range of 51–80 years (81.7%) and farmers accounted for 30.3% and 61 patients (90.2%) followed orthodox Christianity. (Table 1).
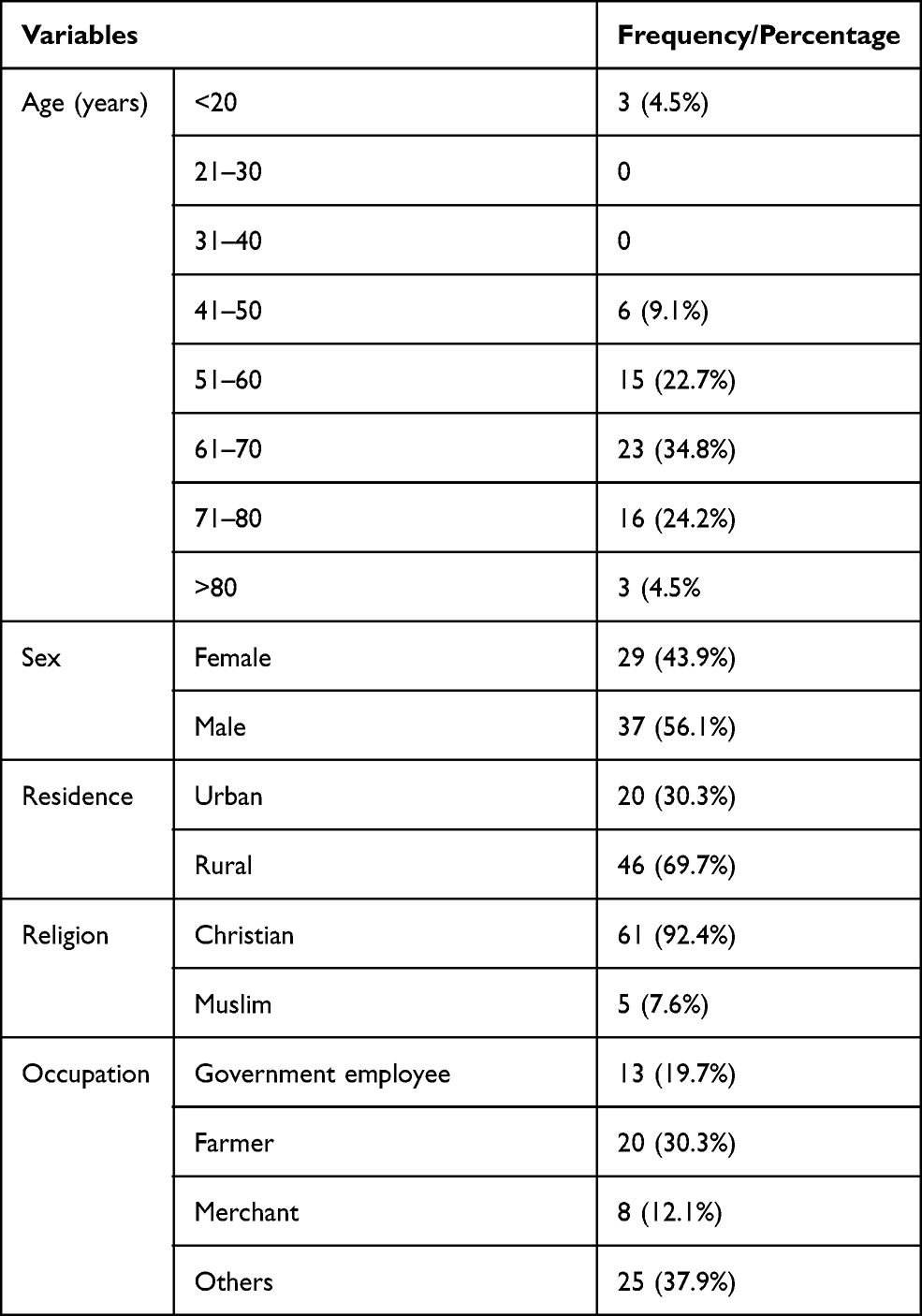 |
Table 1 Socio-Demographic Characteristics of Patients Operated for Cataract with MSICS Technique at University of Gondar Tertiary Eye Care and Training Center, NW Ethiopia (n = 90). |
Pre-operative Clinical Profile
All operated eyes had mature cataract with pre-operative uncorrected visual acuity (UCVA) of worse than 6/60 or poor. Sixty-six (73.3%) eyes were operated through temporal incision site and 24 (26.7%) eyes were operated on through a superior incision site. (Table 2)
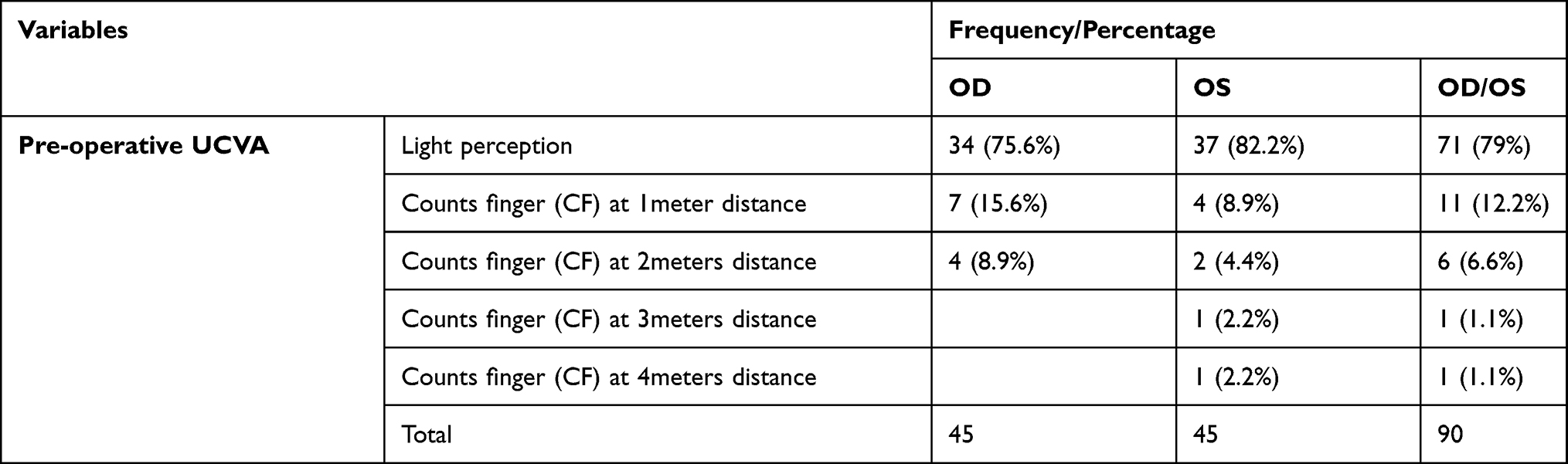 |
Table 2 Pre-Operative UCVA of Patients Operated for Cataract with MSICS Technique at University of Gondar Tertiary Eye Care and Training Center, NW Ethiopia (n = 90). |
In all operated 90 eyes polymethylmetha-acrylate (PMMA) IOL with A constant of 118.5 was implanted. The mean IOL power calculated to achieve a post-operative target refraction of emmetropia was 20.21D (range 2.00D to 24.00D, SD of 4.16) and 20.65D (range 5.50D to 26.50D SD of 4.00) for the right and left eyes respectively. However the mean IOL power inserted was 20.88D (SD of 2.72) and 20.45D (SD of 3.65) for the right and left eyes respectively. The IOL power inserted was the same as that of IOL power calculated in 54 (60%) eyes (27 right eyes and 27 left eyes). (Table 3)
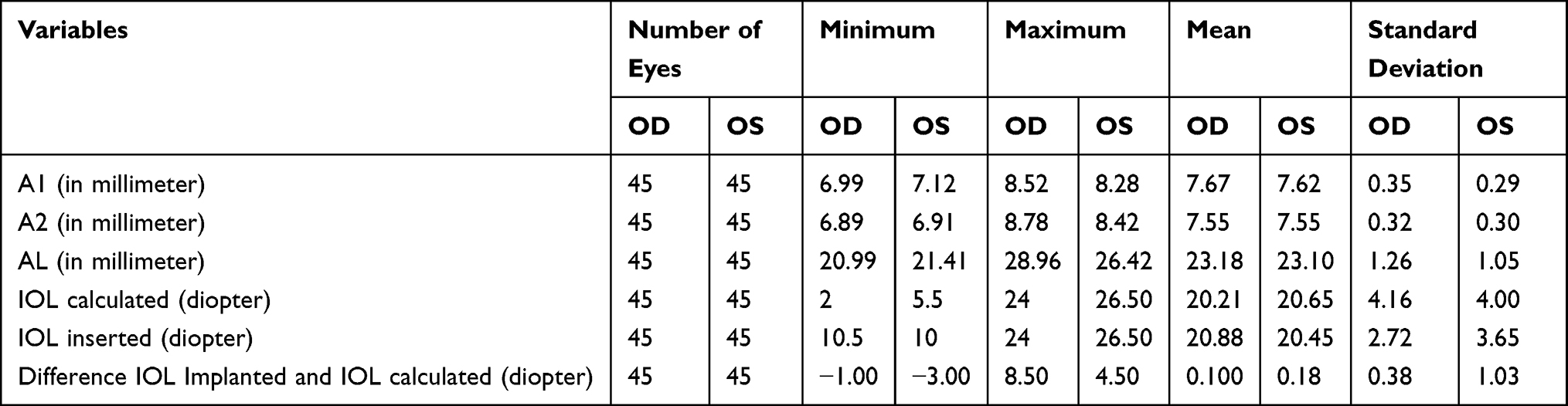 |
Table 3 Pre-Operative Biometric Profile in Millimeter and Diopter of Eyes of Patients Operated for Cataract with MSICS Technique at University of Gondar Tertiary Eye Care and Training Center, NW Ethiopia (n = 90). |
The mean of A1 (Curvature of cornea along the vertical meridian), A2 (Curvature of cornea along the horizontal meridian), Axial length (AL) and IOL power was 7.67mm, 7.54mm, 23.18mm and 20.21D for the right eye and it was 7.62mm, 7.55mm, 23.10mm and 20.65D for the left eye.(Table 3).
Post-operative Clinical Profile
A total of 90 eyes of 66 patients were refracted post-operatively at a mean follow up time of 41 days and 46 days for the right and left eyes respectively.
Of operated 90 right and left eyes combined, 60 (66.7%) eyes had better than 6/24 or good UCVA and 74 (82.2%) eyes had better than 6/24 or good BCVA.
Of 45 operated right eyes, 32 (71.1%) eyes achieved a post-operative UCVA of better than 6/24 or good outcome and 28 (62.2%) of 45 operated left eyes achieved a post op UCVA of better than 6/24 or good outcome. After refraction, 38 (84.4%) right eyes and 36 (80%) left eyes achieved a post-operative BCVA of better than 6/24 or good outcome. (Table 4).
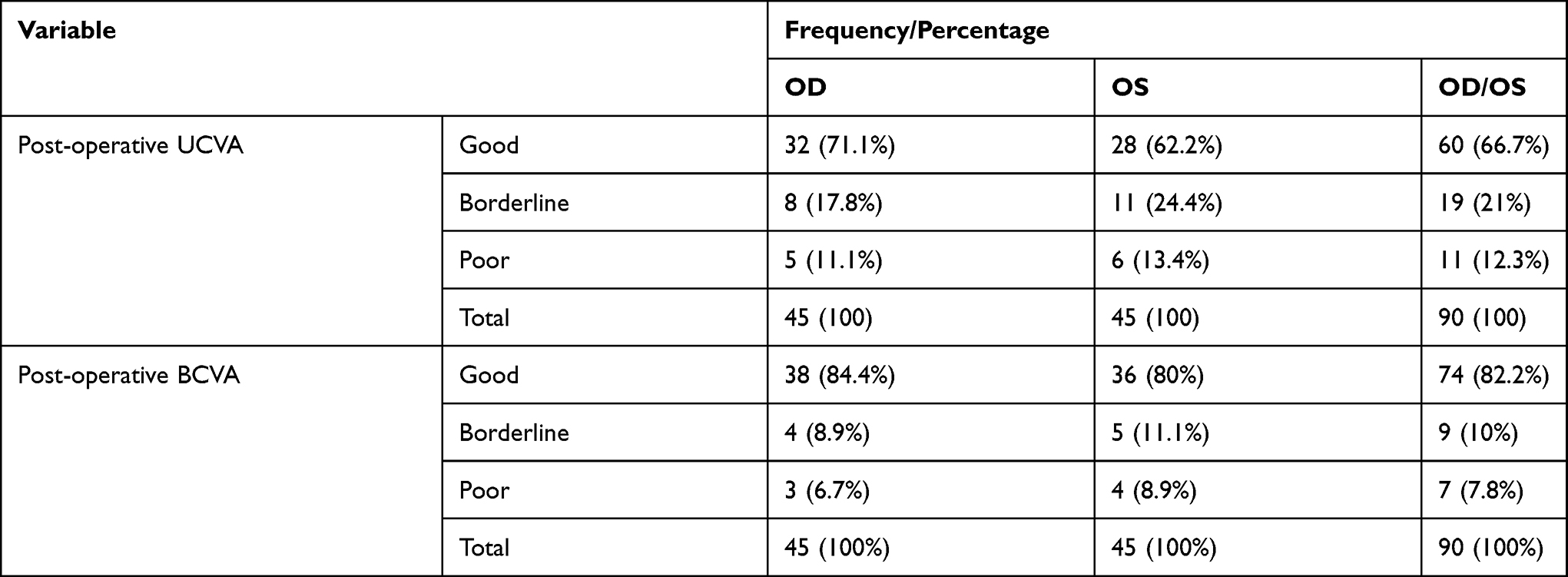 |
Table 4 Postoperative Visual Acuity of Patients Operated for Cataract with MSICS Technique at University of Gondar Tertiary Eye Care and Training Center, NW Ethiopia (n = 90). |
From 90 refracted eyes, 58 (64.4%) eyes (30 right and 28 left eyes) achieved a post operative refraction of ±1.00D (Table 5) and the mean SE of right and left eyes were −0.73D and −0.93D respectively (Table 6).
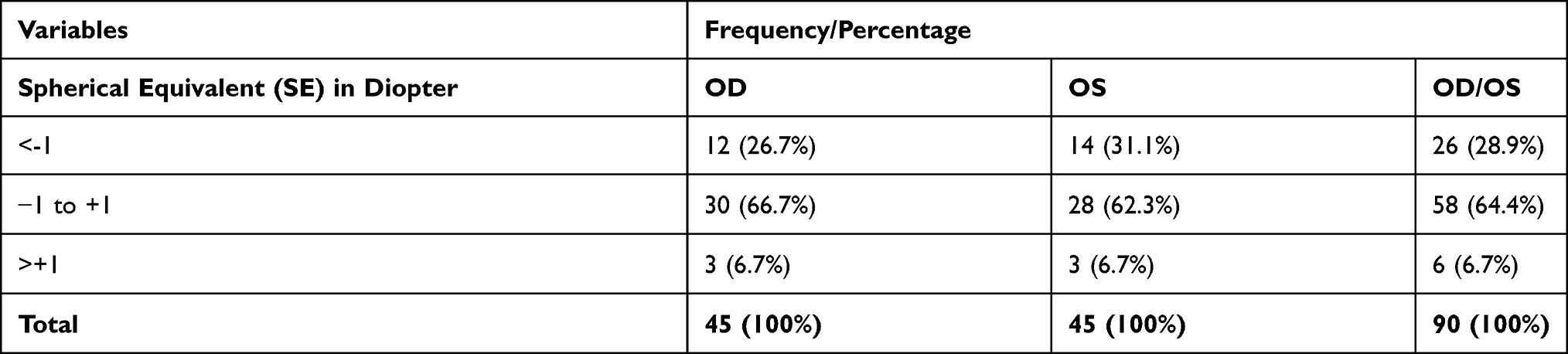 |
Table 5 Post-Operative Refractive Outcome of Patients Operated for Cataract with MSICS Technique at University of Gondar Tertiary Eye Care and Training Center, NW Ethiopia (n = 90). |
 |
Table 6 Comparison of Post-Operative Refraction SE Between the Right and Left Eyes of Patients Operated for Cataract with MSICS Technique at University of Gondar Tertiary Eye Care and Training Center, NW Ethiopia (n = 90). |
After the Independent Samples t-test was computed, the mean SE in eyes with AL of 23mm to 25mm and that of eyes with AL >25mm or <23mm showed no significant variation (p value =0.115 for right eye and 0.569 for the left eye).
The Independent Samples t-test was also done to compare the mean post operative refraction between the superior and temporal surgical approach which was −0.97D and −0.65D respectively and it revealed insignificant difference (p-value of 0.603 and 0.548 for right and left eyes respectively).
Discussion
Refractive error is a common cause of poor visual outcome following cataract surgery. Its incidence and severity depends on various factors including the type of surgery, skill of the surgeon, pre-operative refractive status of eyes and techniques of biometry used, the formula used to calculate IOL power and the degree of cataract opacity.11,13 In this study the right and left eyes achieved mean post-operative refraction SE of −.073D and −0.93D respectively. It is better as compared to a study done in Kenya, between 1 January 1999 and 31 December 1999 in which the average SE was about –1.5D.18 Another study conducted in Boston USA, January through December of 2010 revealed a better outcome in which 94% of eyes achieved ±1.0D of target refraction after cataract surgery.19 This difference may be because they used the IOL master equipment to calculate the IOL power and the surgery was phacoemulsification.
The present study achieved SE of ±1D in 64.4% of eyes which is lower as compared to the National Health Service benchmark standard which is 85% or better.13 The lower value in this study may be ascribed to the dense cataract causing poor fixation during biometry, the biometry was taken by junior residents (year 1 and 2), the same formula was used for all axial lengths of the eye and the calculated IOL power may not be present at the store.
Some studies have shown that superior approach during cataract surgery induces more astigmatism than temporal approach.16,20 This study reveals insignificant variation with regard to post-operative refractive outcome in both approaches. This may be due to the small sample size in the present study.
In this study the Mean and Standard deviation of IOL power calculated was 20.87D±2.7D and 20.64D±3.9D for the right and left eyes respectively. The mean IOL power inserted was 20.88D (SD of 2.72) and 20.45D (SD of 3.65) for the right and left eyes respectively. This is comparable to a Kenyan study of which the mean power of PC-IOL inserted was 21.9D (SD 2.1D).18
Before the surgery all operated eyes had poor visual acuity. This was reduced to 7 (7.8%) eyes post-operatively. Post-operative UCVA of better than 6/24 or good was achieved in 66.7% eyes and BCVA in 82.2% which is low as compared to WHO target guideline where the target proportion of patients with UCVA should be greater than 80% and BCVA of greater than 90%. A study from Nepal achieved BCVA of better than 6/24 or good in 95.9%.14 The poor outcome in the present study may be due to post-operative refractive error or surgery related issues. A study done in Nigeria revealed BCVA in 76.8% which is comparable to the present study.21
Our study has better results when compared to two previous studies done in Ethiopia, one in 2015 Gondar and the other in Goro District, Central Ethiopia 2008, with UCVA of better than 6/24 or good in 26.6% and 23.7% respectively.12,22
The small sample size and absence of pre-operative refractive status of the operated eyes are the major limitation of this study. Comparison of our study findings with other reports is limited as most of the studies have examined a change in refractive error from pre-operative refractive status and most of the studies focused on astigmatic change with different cataract surgical technique as well as the majority lack biometric profile.
Conclusion and Recommendation
Although the post-operative visual outcome is better than previous reports in Ethiopia, the post-operative refractive outcome after cataract surgery is still lower when compared to target post-operative refractive benchmarks such as the recommendations of National Health Service of England. The best way to manage post-operative refractive error is to prevent it through accurate biometry, IOL formula selection and avoiding wrong IOL power insertion. Thus, consideration should be given to repeating biometry when the findings differ significantly between the two eyes or from the population mean. Wrong IOL implantation should be avoided by making available a wide range of IOL powers at the center.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Resnikoff S, Pascolini D, Etya’ale D, Kocur I, Pararajasegaram R, Pokharel GP. Global data on visual impairment in year 2002. Bull World Health Organ. 2002;82:844–851.
2. Lawani R, Pommier S, Roux L, Chazalon E, Meyer F. Magnitude and strategies of cataract management in the world. Med Trop (Mars). 2007;67:644–650.
3. Lewallen S, Williams TD, Dray A, et al. Estimating incidence of vision-reducing cataract in Africa: a new model with implications for program targets. Arch Ophthalmol. 2010;128(12):1584–1589. doi:10.1001/archophthalmol.2010.307
4. Berhane Y, Worku A, Bejiga A National survey on blindness, low vision and Trachoma in Ethiopia. Addis Ababa: Federal Ministry of Health of Ethiopia; September, 2006.
5. Berhane Y, Worku A, Bejiga A, et al. Prevalence and causes of blindness and low vision in Ethiopia. Ethiop J Health Dev. 2008;21(3):204–210. doi:10.4314/ejhd.v21i3.10050
6. Foster A. Cataract and “Vision 2020—the right to sight” initiative. Br J Ophthalmol. 2001;85(6):635–637. doi:10.1136/bjo.85.6.635
7. IAPB, World Health Organization. Vision 2020: the Right To Sight Global Initiative for the Elimination of Avoidable Blindness Action Plan, 2006–2011. Geneva: World Health Organization; 2007.
8. World Health Organization. Prevention of blindness and visual impairment: global cataract surgical rate, 2006. Geneva: World Health Organization; 2011.
9. Baltussen R, Sylla M, Mariotti SP. Cost-effectiveness analysis of cataract surgery: a global and regional analysis. Bull World Health Organ. 2004;82(5):338–345.
10. Kuper H, Polack S, Mathenge W, et al. Does cataract surgery alleviate poverty? Evidence from a multi-centre intervention study conducted in Kenya, the Philippines and Bangladesh. PLoS One. 2010;5(11):15431. doi:10.1371/journal.pone.0015431
11. American Academy of Ophthalmology; The Eye M.D Association. Fundamentals and principles of ophthalmology. BCSC section 2; 2015–2016.
12. Bejiga A, Tadesse S. Cataract surgical coverage and outcome in Goro District, Central Ethiopia. Ethiop Med J. 2008;46(3):205–210.
13. Shalchi Z, Restori M, Flanagan D, Watson M. Managing refractive surprise Moorfields Eye Hospital. Ann Ophthalmol (Skokie). 2007;39:209–216.
14. Hennig A, Kumar J, Yorston D, Foster F. Sutureless cataract surgery with nucleus extraction: outcome of a prospective study in Nepal. Br J Ophthalmol. 2003;87(3):266–270. doi:10.1136/bjo.87.3.266
15. Wilkins MR, Allan B, Rubin G; Moorfields IOL Study Group. Spectacle use after routine cataract surgery. Br J Ophthalmol. 2009;93(10):1307–1312. doi:10.1136/bjo.2008.151829
16. Gokhale NS, Sawhney S. Reduction in astigmatism in manual small incision cataract surgery through change of incision site. Indian J Ophthalmol. 2005;53:201–203. doi:10.4103/0301-4738.16684
17. Olawoye OO, Ashaye AO, Bekibele CO, Ajayi BGK.Visual outcome after cataract surgery at the university college hospital, Ibadan. Ann Ib Postgrad Med. 2011;9(1):8–13. doi:10.4314/aipm.v9i1.72428
18. Yorston D, Gichuhi S, Wood M, Foster A. Does prospective monitoring improve cataract surgery outcomes in Africa? Br J Ophthalmol. 2002;86(5):543–547. doi:10.1136/bjo.86.5.543
19. Simon SS, Chee YE, Haddadin RI, et al. Achieving target refraction after cataract surgery. Ophthalmology. 2013;86(5):543–547.
20. Reddy B, Raj A, Singh VP. Site of incision and corneal astigmatism in conventional SICS versus phacoemulsification. Ann Ophthalmol (Skokie). 2007;39:209–216. doi:10.1007/s12009-007-0020-y
21. Fasina O, Okwudishu IA, Bekibele CO. Cataract surgery in Ibadan, Nigeria: visual outcome and postoperative refractive error. Ann Health Res. 2017;3(1):43–49.
22. Hussen MS, Gebreselassie KL, Seid MA, Belete GT. Visual outcome of cataract surgery at Gondar University Hospital Tertiary Eye Care and Training Center, North West Ethiopia. Clin Optom. 2017;9:19–21. doi:10.2147/OPTO.S122953
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.