")
Back to Journals » International Journal of General Medicine » Volume 12
Reflection Of Reflections: Building Diagnostic Expertise
Authors Shimizu T
Received 19 August 2019
Accepted for publication 18 September 2019
Published 7 October 2019 Volume 2019:12 Pages 363—365
DOI https://doi.org/10.2147/IJGM.S227859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Taro Shimizu
Department of Diagnostic and Generalist Medicine, Dokkyo Medical University, Tochigi 321-0297, Japan
Correspondence: Taro Shimizu
Department of Diagnostic and Generalist Medicine, Dokkyo Medical University, 880 Kitakobayashi, Mibu, Shimotsuga, Tochigi 321-0297, Japan
Tel +81 80 3518 8884
Email [email protected]
Abstract: The ability to make a correct diagnosis is one of the physicians’ core competencies. In view of continuous medical education, the way to establish and maintain this expertise has been explored. Reflection has been reported to serve as an effective measure of remediating individual diagnostic skill. This article highlights three reflections which are reflection in action, reflection on action, and reflection for action, evidenced by past reports. Applying these reflections allows physicians to revisit the link between fundamental and interdisciplinary medical knowledge in conjunction with prior experience, thereby developing enhanced levels of diagnostic expertise and mastery.
Keywords: reflection, diagnostic error, diagnostic reasoning, continuous medical education, applied expertise
The diagnostic reasoning expertise, one of the physicians’ core competencies, should be developed throughout his/her career. Despite its importance, no concrete method of lifelong education for cultivating this expertise has been established in the history of medical education.1 It is worth noting that physicians have been relying on incomplete experiences during pre- and postgraduate training, reflecting that there has been no definite method for this training.2 It is said that the common practice for physicians is to train themselves on their own and see more patients, thus building their expertise based on the popularly known rule of 10,000 hrs of experience or the law of transformation of quantity into quality; another technique is to directly or indirectly imitate other physicians with superior skills.3 However, when a physician learns general competency, which requires multifaceted abilities such as communication and logical thinking, through random experience based on clinical situations that are full of complexities, context-specificity, and bias confounding, the acquired clinical skills has a large variance among physicians in quality. It is because of this that we believe that guidelines and principles should exist for training on diagnostic expertise. The dual process theory(DPT), which is based on a complementary relationship between intuitive processes and analytical processes, has been internationally recognized as a fundamental principle concerning diagnostic reasoning, underpinning diagnostic process and supporting diagnostic expertise.4 Indeed, the principle or the "form" of diagnostic reasoning, so-called Diagnostic Strategy established and proposed from Japan, is currently based on the DPT.5 The effectiveness of applying diagnostic reasoning strategy to daily practice, however, has not been well recognized and utilized in the daily clinical setting. By adhering to the Diagnostic Strategy as the basic guideline for practicing physicians to make correct and swift diagnoses than what they have done, they should be able to equip solid diagnostic skills.
In contrast, how should we construct a principle theory for the lifelong training of diagnosis, not for the theory of diagnosis itself? Physicians’ growth patterns can be categorized into two, one for experts who strive for constant growth and another for experienced non-experts who gain experience.6 This growth patterns can be applied in the way of growth in diagnostic reasoning expertise. The difference between the two is whether or not the physician is devoted to his/her self-improvement even after becoming accustomed to clinical practice to a certain extent. In other word, the difference between the two groups of physicians can be found in self-reflection, a powerful motivating tool that enhances physicians’ growth. Based on the above theory, the growth curve of the two groups are depicted as steep growth curve or flattened growth curve, representing that the steep curve as "with self-reflection" and the flattened curve as "without self-reflection" or "lack of input of new insights," respectively (Figure 1). Self-reflection has been reported as successful in enhancing physicians’ diagnostic reasoning.7
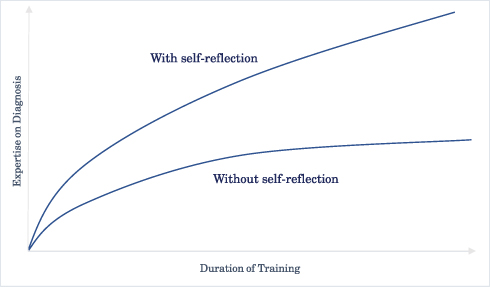 |
Figure 1 Two growth curves of building diagnostic expertise: With versus without self-reflection. |
Recently, we have been experiencing incremental complex multimorbidity in daily clinical practice.8 This condition may impede diagnostic reasoning because of the potential involvement of multiple biases in clinical decision making, which render training on diagnostic reasoning challenging. Hence, physicians should acknowledge these biases and learn the way to manage them for the successful establishment of diagnostic expertise. Moreover, physicians should develop adaptive expertise, which refers to a level of expertise that is flexible enough to function in novel situations.9 Adaptive expertise in the context of diagnostic reasoning may mean comprehensive and flexible thinking in making a diagnosis, that is expected to act effectively not only for solving simple cases but for solving complex cases. Reflection has been reported to allow physicians for enhancing diagnostic thinking process, including the adaptive expertise.10 Therefore, reflection may serve as a substantial guide to cultivate the diagnostic expertise even in the complex medical situation.
Besides, physicians should revisit a link between fundamental and interdisciplinary medical knowledge in conjunction with prior experience in reflecting diagnostic reasoning. The diagnostic thinking process needs to encompass the link between science and art, analytic thinking and intuition, and knowledge and the possibility of delineating the truth. This comprehensive relationship should be noted in the practice of reflection, thereby fostering sophisticated levels of diagnostic expertise.
Stemming from the reflective thinking advocated by Dewey in the early 20th century, reflection was emphasized by Schön in his book, "The Reflective Practitioner". Specifically, this is an education model of "reflection in action" and "reflection on action", in which professionals turn actual challenges into self-lessons.11 Furthermore, another concept of reflection, "reflection for action" was made by Killion and Todnem, involving forethought for planning actions.12 The sequential model of these reflections is expected to be quite essential in the training of diagnostic expertise.
In the context of diagnostic reasoning expertise, the practice of reflection in action means to handle difficulties and to permit modification of actions while reflecting on the matter: somehow making a diagnosis on the spot while simultaneously activating analytical processes (e.g., in cooperation with the Internet or other people) if the intuitive process does not work at the time of the actual diagnosis. However, this alone is just a makeshift solution; as pointed out by Schön, it is necessary for the reflective practitioner to further reflect on action. That is, the physician or the team should reflect on the behavior after the occurrence of the failure in the diagnostic process, thereby utilizing the experience and preventing errors in similar situations in the future. Diagnostically challenging cases would be great to discuss at a conference for the reflection. Such cases would be ones which were experienced by the case presenter or discussants. In the conference, participating physicians would compare the final diagnosis to their initial diagnosis, and try to be creative to develop diagnostic principles and to find clinical pearls learned from the diagnostic errors, thus improving diagnostic skills and avoiding unexpected diagnostic errors in the future.
The more important skill is the reflection for action. This mode of reflection allows physicians to set verbalized and explicit tasks to improve their manner of the diagnostic thinking and hence to avoid biases causing diagnostic errors; doctors can thus repeatedly train themselves based on those tasks focusing on their growth. The above mentioned gap between experts and non-experts in the growth curve may very well be closed by the practice of "on" and "for" rather than "in". The practice of "in" alone just renders phisicians a stopgap problem-solving technique; there is no potential for performance improvement unless some inspiration is fortunately acquired. On the other hand, with the inclusion of "on" and "for", the growth curve can become steeper. This concept can lead to the explanation of a model for lifelong continuous medical education on diagnostic expertise.
There have been studies reporting reflection is beneficial in education on diagnostic skill to medical resident physicians, while the effect is reported to be inconclusive for students.13–16 For residency curriculum, reflection for action can be introduced into two phases: problem-based case discussion during off the job training; during patient encounters in the outpatient clinic, urgent care clinic, emergency room, or in-hospital rotation. Such application throughout medical career will enable learners to have well-grounded growth.
Although further investigations of comparative effectiveness among three reflections, applying these reflections, emphasizing reflection for action, can be speculated as more effective than the conventional and non-focused reflection because this focused reflection will lead to a guideline to one’s continuous medical education. By applying reflection for action, physicians would also become to make it a habit to verbalize the diagnostic thinking process and extrapolate ideas taken from specific cases to generalize and replicate or apply a better diagnostic thinking process. In this way, physicians will be able to steadily develop their diagnostic reasoning skill by identifying learning issues that are specifically clarified in daily clinical settings. While there is no shortcut, the implementation of the concept of the three reflections is a solid and feasible strategy for the mastery in diagnosis.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Swing SR, Beeson MS, Carraccio C, et al. Educational milestone development in the first 7 specialities to enter the next accreditation system. J Grad Med Educ. 2013;5:98–106. doi:10.4300/JGME-05-01-33
2. Norman G. Building on experience-the development of clinical reasoning. N Engl J Med. 2006;355:2251–2252. doi:10.1056/NEJMe068134
3. Trowbridge R, Rencic J, Durning S. Teaching Clinical Reasoning. American College of Physician; 2015.
4. Croskerry P, Petrie DA, Reilly JB, Tait G. Deciding about fast and slow decisions. Acad Med. 2014;89(2):197–200. doi:10.1097/ACM.0000000000000121
5. Shimizu T. The Art and Strategy of Diagnostic Medicine. Igaku shoin;2014:5–7. (Japanese)
6. Bereiter C, Scardamalia M. Surpassing Ourselves. Peru (IL): Open Court; 1993.
7. Lambe KA, O’Reilly G, Kelley BD, Curristan S. Dual-process cognitive interventions to enhance diagnostic reasoning: a systematic review. BMJ Qual Saf. 2016;25(10):808–820. doi:10.1136/bmjqs-2015-004417
8. Harrison C, Britt H, Miller G, Henderson J. Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice. BMJ Open. 2014;4(7):e004694. doi:10.1136/bmjopen-2013-004694
9. Hatano G. Social and motivational bases for mathematical understanding. New Dir Child Adolesc Dev. 1988;1988(41):55–70. doi:10.1002/cd.23219884105
10. Croskerry P. Adaptive expertise in medical decision making. Med Teach. 2018;40(8):803–808. doi:10.1080/0142159X.2018.1484898
11. Schön DA. The Reflective Practitioner: How Professionals Think in Action; 1984. Basic Books.
12. Killion J, Todnem G. A process for personal theory building. Educ Leadersh. 1991;48(7):14–16.
13. Mamede S, van Gog T, Moura AS, et al. Reflection as a strategy to foster medical students’ acquisition of diagnostic competence. Med Educ. 2012;46(5):464–472. doi:10.1111/j.1365-2923.2012.04217.x
14. Mamede S, van Gog T, van den Berge K, et al. Effect of availability bias and reflective reasoning on diagnostic accuracy among internal medicine residents. JAMA. 2010;304(11):1198–1203. doi:10.1001/jama.2010.1276
15. Ogdie AR, Reilly JB, Pang WG, et al. Seen through their eyes: residents’ reflections on the cognitive and contextual components of diagnostic errors in medicine. Acad Med. 2012;87(10):1361–1367. doi:10.1097/ACM.0b013e31826742c9
16. Wright B, Faulkner N, Bragge P, Graber M. What interventions could reduce diagnostic error in emergency departments? A review of evidence, practice and consumer perspectives. Diagnosis(Berl). 2019. doi:10.1515/dx-2018-0104
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.