Back to Journals » International Journal of General Medicine » Volume 15
Reference Intervals for Absolute and Percentage CD4+ T Lymphocytes among an Apparently Healthy Population in Addis Ababa, Ethiopia
Authors Chalchisa D, Belay Y, Befekadu E, Kassaw M ![]() , G/Egzeabher L, Gebremicael G
, G/Egzeabher L, Gebremicael G ![]() , Lengiso B, Chala D
, Lengiso B, Chala D ![]() , Sahlemariam Z, Kebede E, Abate E, Tsegaye A
, Sahlemariam Z, Kebede E, Abate E, Tsegaye A ![]()
Received 10 January 2022
Accepted for publication 27 April 2022
Published 1 June 2022 Volume 2022:15 Pages 5361—5367
DOI https://doi.org/10.2147/IJGM.S357237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dinkenesh Chalchisa,1,2 Yohannes Belay,1 Endalkachew Befekadu,3 Melkitu Kassaw,4 Letebrhan G/Egzeabher,5 Gebremedhin Gebremicael,1 Boki Lengiso,1 Dawit Chala,1 Zewdineh Sahlemariam,6 Estifanos Kebede,6 Ebba Abate,4 Aster Tsegaye2
1National HIV Reference Laboratory, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 2Department of Medical Laboratory Sciences, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Medical Laboratory, Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia; 4Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 5Department of Medical Laboratory, Yekatit 12 Medical College Hospital, Addis Ababa, Ethiopia; 6Jimma University, Jimma, Ethiopia
Correspondence: Dinkenesh Chalchisa, National HIV Reference Laboratory, Ethiopian Public Health Institute, Addis Ababa, 1242, Ethiopia, Tel + 251-91-064-0900, Email [email protected]
Background: Reference intervals for clinical laboratory parameters differ based on several factors, including age, sex, genetic variation, and geographic location. This variation influences clinical decisions and treatment monitoring. Currently, Ethiopia has used adopted reference intervals from manufacturer values derived from non-Africans. Therefore, the aim this study was to determine reference intervals for absolute and percentage CD4+ T cells for an apparently healthy population in Addis Ababa, Ethiopia.
Methods: A community-based cross-sectional study was conducted on 361 apparently healthy people in four subcities in Addis Ababa from January to June 2019. Sociodemographic and clinical data were collected using a structured questionnaire after informed consent had been obtained. Blood samples were collected and CD4+ T-lymphocyte enumeration performed using a BD FACSPresto near-patient CD4 counter. Data were entered and analyzed using SPSS 20. Reference intervals were determined by a nonparametric test estimating percentiles 2.5 (lower limit) and 97.5 (upper limit) with 95% CIs. P< 0.05 was considered statistically significant.
Results: A total of 337 (183 female and 154 male) healthy participants of median age 28 (IQR 17– 35) years were included in the final analysis. Medians of absolute and percentage CD4+ T-cell counts (932.0 and 42.9, respectively) of female participants were significantly higher than male participants (802.5 and 38.7, respectively; P< 0.05). Reference intervals for absolute CD4+ T-cell count and percentages in males were 483.8– 1,310 cells/μL and 18.1– 57.3 and in females 447.8– 1,479.8 cells/μL and 25.6– 58.9, respectively.
Conclusion: The CD4+ T-count reference intervals established in this study showed some inconsistency from the manufacturer’s provided values and other studies and also revealed sex differences, necessitating sex-specific locally established reference intervals.
Keywords: reference interval, CD4 count, %CD4, Ethiopia
Introduction
CD4+ T-cell count is the main parameter in the establishment and monitoring of the immunostatus of a person in both healthy and diseased conditions.1 It had been an important tool in the initiation and monitoring of highly active antiretroviral therapy until recent years, when the strategy was changed so that people received treatment regardless of the count.2 The CD4+ T cell is the centerpiece of adaptive immunoresponses in our body. In addition, the number of CD4+ T cells in circulation provides important information about the immunocompetence of an individual. Clinical applications of enumerating CD4+ T cells include the diagnosis of such immunodeficiency disorders as AIDS and other opportunistic infections.3
HIV infects CD4+ T lymphocytes and causes both direct and indirect destruction, leading to their gradual loss in the peripheral circulation, hence CD4+ T-cell counts are being used to monitor disease progression in HIV infection and to initiate prophylactic treatment for opportunistic infections.4 Because HIV affects and replicates in CD4+ T lymphocytes, the severity is reflected by quantifying absolute CD4+ T-lymphocyte numbers per total blood volume and percentages of CD4+ T cells per total lymphocyte count.5,6 Values are interpreted against reference interval (RIs) specific to the local population.
According to the Clinical and Laboratory Standards Institute (CLSI) and National Committee of Clinical Laboratory Standards, an RI is defined as the value or test result obtained by the observation or measurement of a particular type of quantity on an adequate number of persons (reference sample group) selected to represent the general population. RIs are usually presented as the interval between two reference limits ie, from the lower reference limit to the upper reference limit defined by a specific percentage (usually 95%).7,8
CD4+ T-cell RIs vary and are affected by such factors as sex, age, geographic location, socioeconomic status, ethnicity, time of specimen collection, diet, pregnancy, altitude, and physical and psychological stress.9–13 Ethiopia has a heterogeneous population and there are no national RIs for CD4+ T lymphocytes, except in some studies from different parts of the country.11,14 Currently, there is a difference in RIs used in Ethiopia, which have been adopted from textbooks derived from non-Africans or studies conducted on different population groups and regions in Ethiopia. Since RIs are important for clinical laboratory test interpretation and provision of quality patient care, it is crucial to have well-determined local RIs. The present study thus aimed to determine CD4+ T-cell RIs in apparently healthy individuals in Addis Ababa, Ethiopia.
Methods
Study Design, Period, and Setting
This community-based cross-sectional study was conducted among apparently healthy individuals in Addis Ababa, the capital city of Ethiopia, from January to June, 2019. The city lies at 2200–2500 m above sea level. It is the largest city in the country by population and is 527 km2, with a total population of 3,384,569 according to the 2007 census.15 Probability proportional-to-size sampling was employed to select four subcities (Arada, Kirkos, Akaki, and Yeka). All woredas (lowest administrative units) in these were included. The subcities were sampled based on considerations of cost and feasibility and representation of all subcities of Addis Ababa (four of ten). Study participants were selected using systematic random sampling by considering woreda as a sampling frame and then households the final selection units. Individuals in households fulfilling the eligibility criteria and willing to participate were included. The minimum sample size recommended by the CLSI is 120, but it also recommends sex partition with a power of 90%8 and an assumption of 30% exclusion16 from data analysis, due to various factors when testing for the common viral infections and chronic diseases. Study participants were approached by health extension workers and invited to a nearby health facility.
Apparently healthy participants aged 15–60 years who fulfilled the eligibility criteria were included in the study. Apparently healthy participants were defined as those who had no prior diagnosis of diseases, and were recruited without any clinical symptoms or signs of illness due to diseases. Sociodemographic and clinical data were collected using a structured questionnaire by trained data collectors, and physical examinations and anthropometric measurements were carried out by trained health professionals. Those discovered to have chronic illnesses like diabetes mellitus, chronic renal insufficiency, hypertension, ischemic heart disease, anemia, thyroid abnormalities, liver diseases, or cancer of any type, taking pharmacologically active substances, with a history of smoking and alcohol consumption, intestinal parasites, HIV infection, high CRP, had donated blood within the previous 3 months, had received blood transfusion(s) within the previous year, or pregnant were excluded. These exclusion criteria were diagnosed either clinically and/or through biological diagnosis.
Data Collection
Sample Collection and Laboratory Analysis
Blood samples of about 4 mL were collected in EDTA tubes. To minimize diurnal variation, samples were collected before 11 am. All samples were labeled with a unique identification number, and CD4 analysis was performed at maximum within 8 hours with a FACS Presto (BD, San Jose, CA, USA) point-of-care instrument at the National HIV Reference Laboratory, Ethiopian Public Health Institute. BD FACSPresto™ CD4 point-of-care technology has been in use in Ethiopia since 2016, and has acceptable agreement with the FACSCalibur for CD4+ T-cell counts and CD4%.17 All laboratory tests were carried out following standard operating procedures and the manufacturer’s instructions by trained medical laboratory technologists. The FACSPresto has an inbuilt quality-control system, and the laboratory is participating in an external quality-assurance scheme to determine the accuracy of its results.
Statistical Analysis
Data were entered and analyzed using SPSS 20. The distribution of data was assessed and data were summarized and presented as means ± SD and medians with IQRs for continuous variables and absolute numbers with percentages for categorical variables. RIs were determined by nonparametric test estimating percentiles 2.5 (lower limit) and 97.5 (upper limit) with 95% CIs.8 The 95% range was taken as an RI. P<0.05 was considered statistically significant.
Results
Sociodemographic Characteristics
A total of 361 apparently healthy individuals aged 15–60 years were enrolled for absolute and percentage CD4+ T-cell RI determination. Of these, 24 were excluded due to chronic illness, parasitic and HIV infections, and high CRP. A total of 337 participants were included in the final analysis. More than half (54.3%) were female. Median age was 28 (IQR 17–35) years, while 33.8% were single and 32.9% married. A majority (79.2%) had completed secondary school (44.8%) while those with a college education and above accounted for 34.4%. Of all participants, 36.5% were government employees (Table 1).
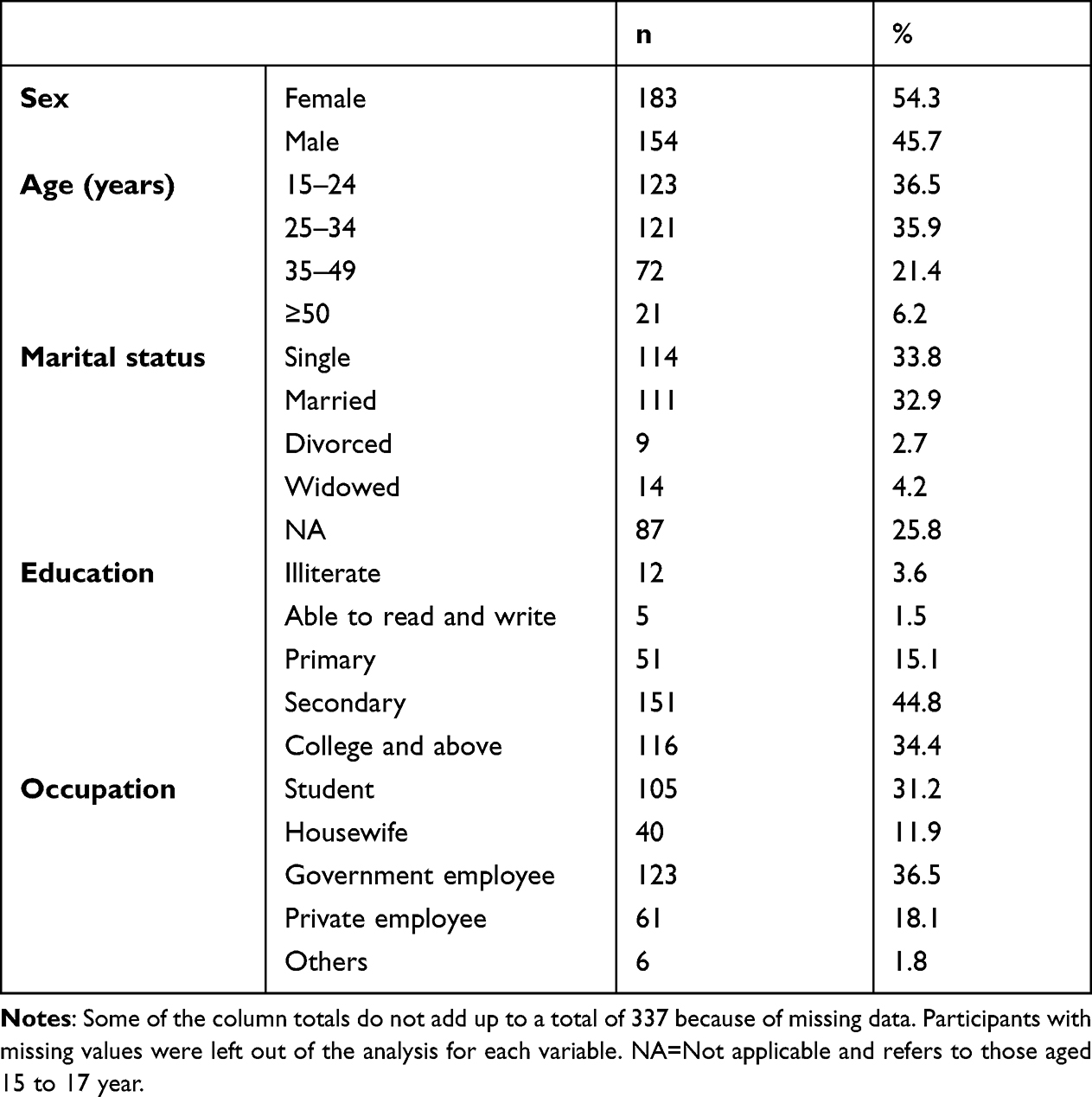 |
Table 1 Sociodemographic characteristics of study participants |
Absolute CD4-Count and -Percentage Reference Intervals
RIs for absolute CD4+ T-cell counts and CD4% of the study participants were 478.6–1434.9 and 26.0–54.7, respectively (Table 2). Absolute CD4+ T-cell counts of female participants (median 932.0, IQR 742.0–1111.0 cells/µL) were significantly higher than those of male participants (median 802.5, IQR 653.5–938.3 cells/µL; P<0.05). CD4+ T-cell percentages were also significantly higher in female participants (mean 42.8±6.5) than male participants (mean 38.1±7). The RIs for absolute CD4+ T-cell counts for female and male participants were 447.8–1479.8 and 483.8–1310 cells/µL, respectively. RIs for CD4+ T-cell percentages were 29.3–56.5 for female participants and 24.3–48.9 for male participants, while RIs for the total study population for absolute CD4+ T-cell counts and CD4+ T-cell percentages were 478.6–1434.9 cells/µL and 26.0–54.7%, respectively (Table 2).
 |
Table 2 Absolute CD4 counts and percentages |
The study also tried to describe the current findings in the context of the RIs given by the manufacturer and other studies in Ethiopia and elsewhere (Table 3). As can be seen in the table, inconsistencies were seen in the RIs from the different countries. For example, while percentages for males were lower for both lower and upper limits, absolute counts were within the range of RIs provided by the manufacturer. In females, the upper CD4-count limit given by the manufacturer was higher than the current finding.
 |
Table 3 Comparison of reference intervals of the current study with other studies in Ethiopia and other countries |
Discussion
Infections like HIV infect CD4+ T lymphocytes and cause both direct and indirect destruction, leading to their gradual loss in peripheral circulation. Therefore, measuring CD4+ T cells is important for the diagnosis of immunodeficiency disorders, including HIV/AIDS, as well as initiating prophylactic treatment for opportunistic infections.4 The FACSPresto is widely available in health facilities and antiretroviral treatment centers in Ethiopia to measure CD4+ T-cell counts, and has been evaluated as having acceptable agreement with the conventional platform (FACSCalibur) for CD4+ T-cell counts and percentages.17 The intervals are also useful for interpreting data in clinical research and vaccine trials to select eligible individuals. There are some efforts underway toestablish RIs in Ethiopia,10,11,14,18 though there are no uniform RIs for absolute CD4+ T-cell counts or percentages at a national or regional level.
The current study aimed to establish RIs for absolute and percentage CD4+ T-cell counts for an apparently healthy population of Addis Ababa. Thus far, most studies have reported that Ethiopian RIs were low compared to other Western populations (eg, healthy Dutch blood donors)11 or other African countries (eg, Uganda),19 due to physiological, environmental, and geographic factors. An earlier study in Ethiopia revealed that there was no difference in CD4+ T-cell counts between cord blood of Ethiopian and Dutch populations, but with apparent differences with increased age, underscoring the fact that differences are due more to environmental factors.20 These indicate that the establishment of CD4+ T-cell count RIs for the local population is critical for the interpretation of laboratory test results and delivering quality health-care services.
This study revealed significant sex differences in absolute CD4+ T-cell counts and percentages: higher in female (median 932.0 and mean 42.8±6.5, respectively) than male(median 802.5 and mean 38.1±7.0, respectively) participants. This result supports findings from previous studies in Ethiopia,11,14,18 Kenya,21 Botswana,22 Nigeria,23 and India.24 This finding might be explained by sex-hormone differences between the sexes influencing both absolute CD4+ T-cell counts and percentages.13 This indicates that the immune system is regulated by sex hormones, since lymphocytes, important cells in the immune system, have receptors for estrogen and androgen.30
Since there were significant differences of absolute CD4+ T-cell count and percentages in male and female participants, it was appropriate to develop different RIs for the male and female populations. Therefore, RIs for male and female participants are reported as 483.8–1310.0 cells/µL and 447.8–1479.8 cells/µL for absolute counts and 24.3–48.9 and 29.3–56.5 for percentages, respectively.
The RIs of absolute CD4 counts and percentages obtained in this study were compared with other studies. In the present study, the lower and upper limits for counts were higher than previous studies in Ethiopia10,11,18 and lower than studies in Italy28 and Brazil.29 The lower and upper limits for percentages were higher than previous studies in Uganda19 and lower than Botswana22 and Italy.28 The lower percentage limit for males is comparable to the Kenyan study.21
The lower male limit for absolute CD4+ T-cell count in this study is higher than that from previous studies in Ethiopia,11,18, other African countries,19,21–23, and India.24 On the other hand, the upper limit is generally lower than values from African countries21 and in India.24 The lower limit for female absolute CD4+ T-cell count in the present study is higher than values from studies in Uganda,19 Nigeria,23 CAR,27 and the user guide,25 while the upper limit is lower than those from studies in Kenya,21 Uganda,19 Nigeria,23 Botswana,22 and India.24
The observed differences from other studies might be due to genetic, ethnic, and study-population variations and differences in methodologies, eg, the FACSPresto platform was used for CD4+ T-cell counts in the present study. The FACSPresto near-patient CD4+ T-cell counter has been distributed among most health facilities in Ethiopia.17 Therefore, determining RIs using this platform is of paramount importance.
This study meets the minimum CLSI requirements for establishing valid RIs, though there are limitations. Participants were recruited from the highland and may not be representative of the lowlands. Also, Ethiopia has a diversity of ethnic groups, and our data represent only a healthy population in Addis Ababa.
Conclusion
Absolute CD4+ T-cell count RIs established in this study were somewhat different from the manufacturer’s kit insert and previous studies. While the absolute count for males was within the range of RIs provided by the manufacturer, in females the upper limit was lower than that given by the manufacturer. Sex differences were also noted, signifying the importance of using separate RIs for male and female populations. For better laboratory test interpretation and patient management, locally established RIs are important. A similar nationwide study is recommended to determine CD4+ T-cell and other lymphocyte RIs for the Ethiopian population as a whole, taking age, geography, and other factors into consideration.
Data Sharing
All necessary data generated or analyzed during this study are included in this article.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was reviewed and approved by the Departmental Research and Ethics Review Committee of the Department of Medical Laboratory Science, Addis Ababa University. All participants provided written informed consent, and assent for those under the age of 18 years was obtained from a parent or legal guardian on their behalf at enrollment. CD4+ and hemoglobin test results obtained using the BD FACSPresto were sent back to participants upon request.
Acknowledgments
The authors would like to thank the Department of Medical Laboratory Sciences of Addis Ababa University and the Ethiopian Public Health Institute and Ministry of Innovation and Technology for sponsoring this work. The Federal Ministry of Health, Central Statistics Agency, Addis Ababa Health Bureau, health extension workers, institutions that facilitated the data-collection process, and all who directly or indirectly contributed to this study are gratefully acknowledged for making this study possible. We also thank all study participants.
Author Contributions
All authors contributed to data collection, analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval to the version to be published, and agree to be responsible for all aspects of the work.
Funding
This research was supported by the Ministry of Science and Technology/Ministry of Innovation and Technology, the Ethiopian Public Health Institution, and partly by Addis Ababa University.
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Anaya J-M, Shoenfeld Y, Rojas-Villarraga A, Levy RA, Cervera R. AUTOIMMUNITY from Bench to Bedside. El Rosario University; 2013.
2. Ford N, Meintjes G, Vitoria M, Greene G, Chiller T. The evolving role of CD4 cell counts in HIV care. Curr Opin HIV AIDS. 2017;12(2):123–128. doi:10.1097/COH.0000000000000348
3. Nicholson JK, McDougal JS, Hearn TL, et al. Revised guidelines for the performance of CD4+ T-cell determinations in persons with human immunodeficiency virus (HIV) infections. Morb Mortal Wkly Rep. 1994;43:1–29.
4. Laboratory guidelines for enumeration CD4 T lymphocytes in the context of HIV/AIDS (revised version 2009). WHO Regional Office for South-East Asia; 2009.
5. Ozarda Y. Reference intervals: current status, recent developments and future considerations. Biochem Med. 2016;26(1):5–16.
6. Hoffbrand AV, Higgs DR, Keeling DM, Mehta AB. Postgraduate Haematology. John Wiley & Sons; 2016.
7. Clinical and Laboratory standards Institute. Defining, Establishing, and Verifying Reference Intervals in the Clinical Laboratory; Approved Guideline. Clinical and Laboratory standards Institute; 2008.
8. NCCLS. How to Define and Determine Reference Intervals in the Clinical Laboratory; Approved Guideline.
9. Shete A, Thakar M, Abraham PR, Paranjape R. A review on peripheral blood CD4+ T lymphocyte counts in healthy adult Indians. Indian J Med Res. 2010;132(6):667.
10. Abera B, Alem A, Cherenet A, Kibret M. Immunological and hematological reference values for apparently healthy HIV-negative adults in Bahir Dar Town, Ethiopia. Ethiop J Health Dev. 2012;26(3):152–159.
11. Tsegaye A, Messele T, Tilahun T, et al. Immunohematological reference ranges for adult Ethiopians. Clin Diagn Lab Immunol. 1999;6(3):410–414. doi:10.1128/CDLI.6.3.410-414.1999
12. Tanjong R, Atashili J, Kamga H, Ikomey G, Akenji N, Ndumbe M. Reference values of CD4-lymphocyte counts in HIV seronegative pregnant women in Buea, Cameroon. African J Clin Exp Microbiol. 2012;13(1):28–34.
13. Maini M, Gilson R, Chavda N, et al. Reference ranges and sources of variability of CD4 counts in HIV-seronegative women and men. Sex Transm Infect. 1996;72(1):27–31. doi:10.1136/sti.72.1.27
14. Mulu W, Abera B, Mekonnen Z, et al. Haematological and CD4+ T cells reference ranges in healthy adult populations in Gojjam zones in Amhara region, Ethiopia. PLoS One. 2017;12(7):e0181268. doi:10.1371/journal.pone.0181268
15. The 2007 population and housing census of Ethiopia: population census commission. Central Statistical Authority. 2012.
16. Stevens W, Kamali A, Karita E, et al. Baseline morbidity in 2990 adult African volunteers recruited to characterize laboratory reference intervals for future HIV vaccine clinical trials. PLoS One. 2008;3(4):e2043. doi:10.1371/journal.pone.0002043
17. Gebremicael G, Belay Y, Girma F, et al. The performance of BD FACSPrestoâ„¢ for CD4 T-cell count, CD4% and hemoglobin concentration test in Ethiopia. PLoS One. 2017;12(4):e0176323. doi:10.1371/journal.pone.0176323
18. Gize A, Mathewos B, Moges B, Workineh M, Gedefaw L. Establishment of normal reference intervals for CD3 +, CD4 +, CD8 +, and CD4 + to CD8 + ratio of T lymphocytes in HIV negative adults from University of Gondar Hospital, North West Ethiopia. AIDS Res Treat. 2014;2014:1–7. doi:10.1155/2014/267450
19. Nanzigu S, Waako P, Petzold M, et al. CD4-T-lymphocyte reference ranges in Uganda and its influencing factors. Lab Med. 2011;42(2):94–101. doi:10.1309/LMFT0VCE1UGO9YGD
20. Tsegaye A, Wolday D, Otto S, et al. Immunophenotyping of blood lymphocytes at birth, during childhood, and during adulthood in HIV-1-uninfected Ethiopians. Clin Immunol. 2003;109(3):338–346. doi:10.1016/j.clim.2003.08.008
21. Bosire EM, Nyamache AK, Gicheru MM, Khamadi SA, Lihana RW, Okoth V. Population specific reference ranges of CD3, CD4 and CD8 lymphocyte subsets among healthy Kenyans. AIDS Res Ther. 2013;10(1):24. doi:10.1186/1742-6405-10-24
22. Mine M, Moyo S, Penny Stevens KM, et al. Immunohaematological reference values for HIV-negative healthy adults in Botswana. Afr J Lab Med. 2012;1(1):1–7.
23. Oladepo D, Idigbe E, Audu R, et al. Establishment of reference values of CD4 and CD8 lymphocyte subsets in healthy Nigerian adults. Clin Vaccine Immunol. 2009;16(9):1374–1377. doi:10.1128/CVI.00378-08
24. Thakar MR, Abraham PR, Arora S, et al. Establishment of reference CD4+ T cell values for adult Indian population. AIDS Res Ther. 2011;8(1):35. doi:10.1186/1742-6405-8-35
25. BD FACSPresto™ Cartridge Kit Insert. BD Biosciences; 2020. Available from: https://www.bdbiosciences.com/ds/europe/tds/23-12814.pdf.
26. Enawgaw B, Birhan W, Abebe M, et al. Haematological and immunological reference intervals for adult population in the state of Amhara, Ethiopia. Trop Med Int Health. 2018;23(7):765–773. doi:10.1111/tmi.13071
27. Menard D, Mandeng MJ, Tothy MB, Kelembho EK, Gresenguet G, Talarmin A. Immunohematological reference ranges for adults from the Central African Republic. Clin Diagn Lab Immunol. 2003;10(3):443–445. doi:10.1128/cdli.10.3.443-445.2003
28. Santagostino A, Garbaccio G, Pistorio A, et al. An Italian national multicenter study for the definition of reference ranges for normal values of peripheral blood lymphocyte subsets in healthy adults. Haematologica. 1999;84(6):499–504.
29. Torres AJL, Angelo ALD, Silva MO, et al. Establishing the reference range for T lymphocytes subpopulations in adults and children from Brazil. Rev Inst Med Trop Sao Paulo. 2013;55(5):323–328. doi:10.1590/S0036-46652013000500005
30. Bouman A, Heineman MJ, Faas MM. Sex hormones and the immune response in humans. Hum Reprod Update. 2005;11(4):411–423. doi:10.1093/humupd/dmi008
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Establishment of Reference Intervals for Serum Protein Electrophoresis of Apparently Healthy Adults in Addis Ababa, Ethiopia
Bikila D, Lejisa T, Tolcha Y, Bashea C, Meles M, Getahun T, Ashebir G, Habtu W, Challa F, Mohammed O, Kassaw M, Kebede A, G/Egzeabher L, Befekadu E, Wolde M, Tsegaye A
International Journal of General Medicine 2022, 15:6701-6711
Published Date: 23 August 2022