Back to Journals » Journal of Inflammation Research » Volume 19
Red Cell Distribution Width to Albumin Ratio: A Novel and Potential Biomarker for Rheumatoid Arthritis
Authors Li X ![]() , Zhu H, Fu Y, Yin H
, Zhu H, Fu Y, Yin H
Received 1 April 2026
Accepted for publication 26 May 2026
Published 10 June 2026 Volume 2026:19 611056
DOI https://doi.org/10.2147/JIR.S611056
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shouya Feng
Xuefei Li, Huiling Zhu, Yao Fu, Haiqin Yin
Department of Rheumatology and Immunology, Jiujiang University Affiliated Hospital, Jiujiang, People’s Republic of China
Correspondence: Haiqin Yin, Email [email protected] Xuefei Li, Email [email protected]
Dear editor
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by symmetrical polyarthritis affecting multiple joints, with potential systemic manifestations including interstitial pneumonia, rheumatoid nodules, vasculitis, and osteoporosis, posing a significant threat to patients’ quality of life and long-term health outcomes.1 Therefore, early diagnosis and accurate disease activity assessment are critical for controlling disease progression, delaying joint damage, and improving prognosis. Current biomarkers for RA evaluation include rheumatoid factor (RF), anti-cyclic citrullinated peptide antibody (ACPA), C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR). However, these conventional markers exhibit limitations in clinical practice: up to 20–30% of RA patients test negative for RF/ACPA,2 and the specificity of these markers is not absolutely ideal either. Recent studies have also explored genetic susceptibility factors in RA, including vitamin D receptor gene polymorphisms, highlighting the multifaceted etiology of the disease.3 This complex pathogenesis has motivated the search for novel, easily accessible biomarkers that can capture the integrated inflammatory, immune, and metabolic disturbances in RA.
In recent years, composite hematological indices, which reflect the integrated inflammatory, immune, and metabolic disturbances characteristic of RA, have emerged as a promising frontier in biomarker research. Among the more established ratios, the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) have demonstrated correlations with RA disease activity and treatment response.4 More recently, the red cell distribution width-to-albumin ratio (RAR) has gained attention as a novel, integrative marker. It synergistically combines a parameter of chronic inflammation and oxidative stress, namely red cell distribution width (RDW), with a key negative acute-phase reactant and nutritional indicator, serum albumin (ALB). Evidence from large-scale epidemiological studies, including analyses of the NHANES database, has linked elevated RAR to increased all-cause mortality in RA patients.5 However, a direct, comprehensive comparison of RAR’s diagnostic efficacy against other ratios, and an evaluation of their combined utility in a single model, remains relatively underexplored. While previous studies have examined RAR primarily in relation to mortality risk in RA, and NLR/PLR have been individually associated with disease activity, the present study provides the first direct, head-to-head comparison of RAR with NLR, PLR, and MHR in a single, well-characterized RA cohort. Moreover, we constructed and rigorously validated a four-marker composite diagnostic model that captures multiple distinct pathophysiological domains, achieving superior diagnostic accuracy over any single or dual-marker combination.Therefore, this study aims to rigorously evaluate the diagnostic performance of RAR, both individually and in a composite panel with NLR, PLR, and MHR, for distinguishing RA patients from healthy controls and for assessing disease activity.
This retrospective study enrolled 193 RA patients according to the 2010 ACR/EULAR criteria and 193 age- and sex-matched healthy controls. Patients with other autoimmune diseases (including but not limited to Sjögren’s syndrome, systemic lupus erythematosus, and ankylosing spondylitis), active infections, malignancies, chronic kidney disease (stage 4–5), hepatic dysfunction (Child-Pugh score ≥B), hematological disorders, blood transfusion within the past 6 months, cardiovascular or metabolic comorbidities (eg, acute myocardial infarction, diabetes mellitus), pregnancy, lactation, or active smoking were excluded. Laboratory parameters from complete blood counts and biochemical profiles were collected. The composite biomarkers were calculated as follows: RAR = RDW(%)/ALB(g/L); NLR = neutrophil count/lymphocyte count; PLR = platelet count/lymphocyte count; MHR = monocyte count/HDL-C(mmol/L). Disease activity was assessed using DAS28-ESR and DAS28-CRP. Statistical analyses were performed using R 4.5.3, employing non-parametric tests, Spearman correlation, ROC curve analysis, and metrics for model comparison (NRI, IDI). The four biomarkers (RAR, NLR, PLR, MHR) were combined into a composite diagnostic panel using binary logistic regression, with RA diagnosis as the dependent variable and the four biomarker values as continuous independent variables. The predicted probabilities from this model were used to generate the ROC curve for the combined panel. This model was unadjusted for demographic or treatment-related confounders, as the primary aim was to evaluate the intrinsic diagnostic discrimination of the biomarkers themselves. A post-hoc power analysis confirmed that the sample size was sufficient for the ROC analyses performed.
RA patients exhibited a distinct hematological and inflammatory profile. Key biomarkers were significantly elevated compared to controls (Table 1). Both RAR and NLR demonstrated significant positive correlations with established disease activity measures. Spearman correlation analysis revealed that both RAR and NLR were significantly correlated with key disease activity measures, including DAS28-ESR (RAR: r = 0.390, P < 0.001; NLR: r = 0.286, P < 0.001) and DAS28-CRP (RAR: r = 0.388, P < 0.001; NLR: r = 0.316, P < 0.001). Notably, patients with moderate-to-high disease activity (DAS28-ESR ≥ 3.2) had significantly higher levels of RAR, NLR, and PLR than those in remission or with low activity (all p < 0.05), suggesting a role in disease stratification.
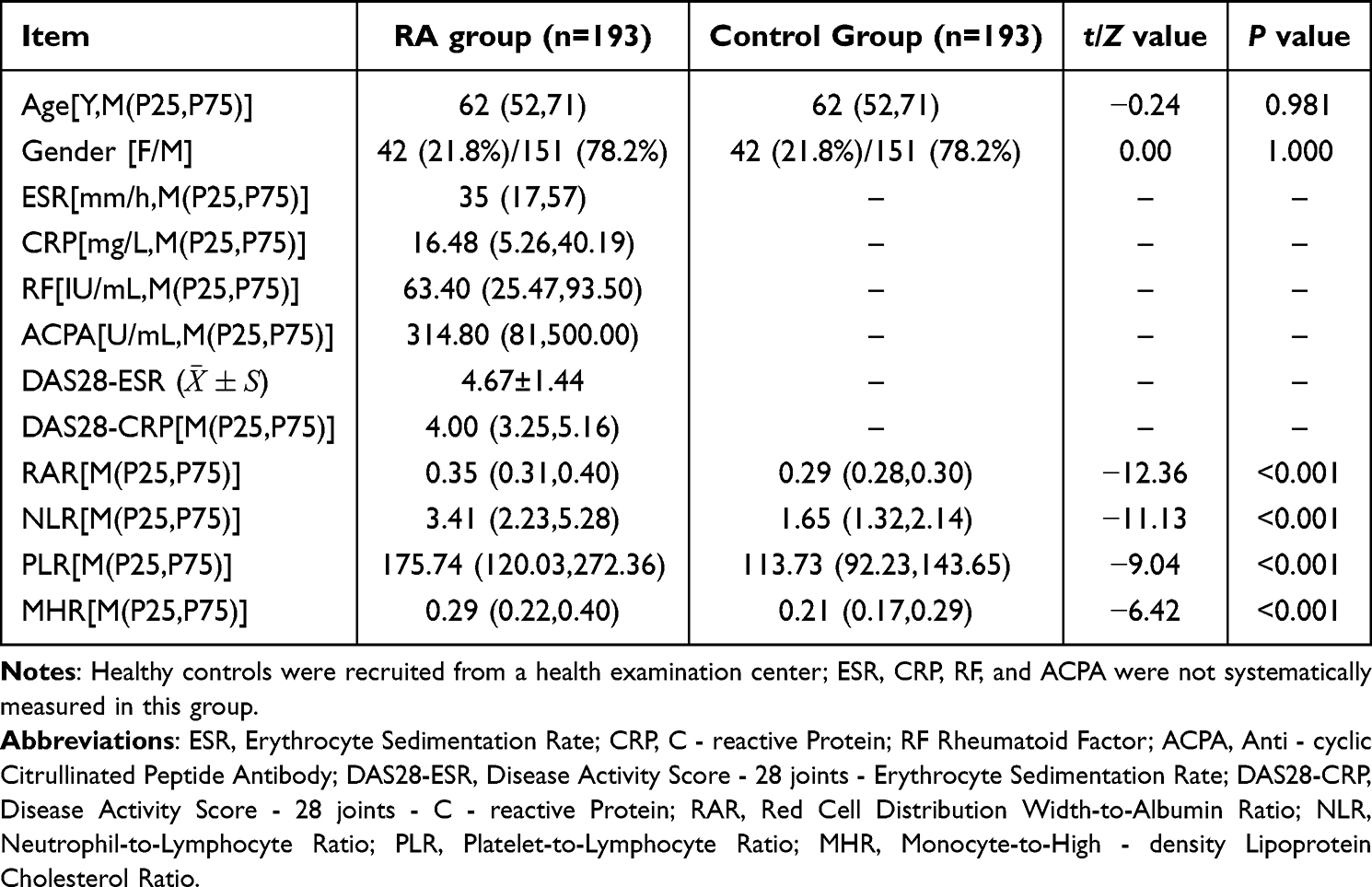 |
Table 1 Participants’ Clinical Parameters |
ROC analysis revealed strong diagnostic performance for individual markers, with RAR achieving an AUC of 0.864 (95% CI: 0.826–0.901). A model combining all four biomarkers (RAR+NLR+PLR+MHR) demonstrated superior performance, yielding an AUC of 0.919 with 81.9% sensitivity and 89.6% specificity. This combined model provided a significant improvement over a dual-marker (RAR+NLR) model, as evidenced by net reclassification improvement (NRI=0.466, p<0.001) and integrated discrimination improvement (IDI=0.023, p=0.004) (Figure 1 and Table 2).
 |
Table 2 Diagnostic performance of individual and combined hematological biomarkers in differentiating RA patients from healthy controls. |
 |
Figure 1 ROC curves. |
In rheumatoid arthritis, chronic inflammation affects erythrocyte and ALB metabolism through multiple pathways. On the one hand, proinflammatory cytokines such as IL-6 suppress erythrocyte maturation in the bone marrow via the gp130 receptor, leading to the release of immature erythrocytes into the circulation and increased heterogeneity of erythrocyte volume, which manifests as elevated RDW.6 On the other hand, inflammation increases capillary permeability, allowing serum ALB to escape into the interstitial space, and significantly shortens the half-life of ALB, hypoalbuminemia ensues.7 Given that RDW and ALB reflect the chronic inflammatory state of RA from two distinct dimensions—impaired erythropoiesis and disordered ALB metabolism—and that both are closely associated with levels of proinflammatory cytokines such as IL-6 and TNF-α, we speculate that the RDW/ALB ratio may integrate the information from these two aspects and thus serve as a potential composite marker for evaluating inflammatory activity in RA.
Our findings, which align with previous studies linking NLR and PLR to RA activity,4,8 confirm that these biomarkers reflect the underlying systemic inflammatory burden and immune cell dysregulation. Consistent with these mechanistic links, A systematic review and meta-analysis by Mangoni and Zinellu reported pooled AUCs of 0.76 for NLR and 0.80 for PLR in diagnosing RA, comparable to the values observed in our cohort. Importantly, our four-marker composite model achieved a substantially higher AUC (0.919), directly addressing the recommendation by Mangoni and Zinellu that the combined use of these markers should be further explored.9 Moreover, in line with the elevated NLR and PLR reported in RA-associated interstitial lung disease,10 our data support the versatility of these indices as systemic inflammatory markers. However, as noted by Erre et al, blood cell-derived indexes may primarily reflect chronic inflammatory burden rather than being RA-specific, a limitation that we acknowledge and that our multi-marker panel is designed to partially mitigate.11
A primary contribution of this study is the comprehensive comparison of RAR with established ratios and the construction of an integrated diagnostic panel, which has not been extensively reported previously. The enhanced diagnostic accuracy of the four-marker composite model suggests a powerful synergistic effect, as each ratio interrogates a distinct yet interconnected pathophysiological axis: RAR (inflammation and nutritional status), NLR (innate-adaptive immune balance and systemic inflammation), PLR (platelet activation and immunothrombosis), and MHR (monocyte-driven inflammation and impaired anti-inflammatory capacity of HDL).12 This readily available and inexpensive biomarker panel, derived entirely from routine blood tests, presents a pragmatic and highly scalable tool for improving RA diagnosis and severity stratification. It offers particular utility in primary care and resource-constrained settings where access to specialized serological testing is limited. Beyond diagnosis, this composite panel could aid in stratifying disease activity and monitoring treatment response, thereby informing clinical decision-making and potentially improving patient outcomes.
We acknowledge limitations in our study, including its retrospective, single-center design, the lack of an external validation cohort, and the absence of a formal a priori sample size calculation for diagnostic accuracy endpoints, as this study was designed as an exploratory analysis; this may limit the precision of the reported cut-off values. A post-hoc power calculation based on the observed AUC of RAR (0.864, n=193 per group, α=0.05) yielded a power exceeding 0.99 for detecting a deviation from the null hypothesis, indicating adequate sample size for the primary analyses. Nonetheless, future prospective studies should incorporate formal a priori sample size calculations tailored to specific diagnostic accuracy endpoints.
Additionally, as RAR may be elevated in various chronic inflammatory conditions, its disease specificity is limited; our integrated multi-marker panel, however, partially compensates for this by capturing multiple distinct pathophysiological domains, yielding improved overall diagnostic accuracy (AUC 0.919, specificity 89.6%). Furthermore, although we observed significantly higher RAR, NLR, and PLR levels in patients with moderate-to-high disease activity compared to those in remission or with low activity (all p < 0.05), finer stratification into more detailed disease activity categories was limited by small subgroup sample sizes. Future prospective, multi-center studies with larger cohorts and longitudinal follow-up are needed to validate our proposed cut-off values in independent cohorts, to evaluate these biomarkers across finer gradations of disease severity, and to explore the dynamic changes of these biomarkers in response to treatment, which could further establish their utility in clinical management.
In conclusion, our study identifies RAR as a robust and novel biomarker for RA. Its incorporation into a composite model with NLR, PLR, and MHR creates an integrative tool reflecting RA’s inflammatory-metabolic interplay. This combined use enhances diagnostic precision and provides a pragmatic framework for resource-optimized RA management in diverse clinical settings.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study adhered to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Jiujiang University Affiliated Hospital (Approval No.: jjuhmer-b-2025-06002). The requirement for written informed consent to review patient medical records was waived by the Ethics Committee because of the retrospective nature of the study and the exclusive use of fully anonymized data, which involved no more than minimal risk to participants. All patient data were handled in strict confidentiality and were used solely for the purposes of this research.
Author Contributions
Xuefei Li: Conceptualization, Data curation, Formal analysis, Writing – original draft.
Huiling Zhu: Resources, Data curation, Formal analysis, Writing – review and editing.
Yao Fu: Resources, Data curation, Writing – review and editing.
Haiqin Yin: Investigation, Resources, Supervision, Writing – review and editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this research.
Disclosure
The authors declare that they have no competing interests.
References
1. Di Matteo A, Bathon JM, Emery P. Rheumatoid arthritis. Lancet. 2023;402(10416):2019–5. doi:10.1016/S0140-6736(23)01525-8
2. De Stefano L, D’Onofrio B, Gandolfo S, et al. Seronegative rheumatoid arthritis: one year in review 2023. Clin Exper Rheumatol. 2023;41(3):554–564. doi:10.55563/clinexprheumatol/go7g26
3. Qadir RR, Shnawa BH, Ahmed MH. Exploring the potential link between vitamin D receptor Cdx2 gene polymorphism and rheumatoid arthritis in female patients: a study in Erbil, Kurdistan Region, Iraq. Revista Colombiana de Reumatología. 2025. doi:10.1016/j.rcreu.2025.03.004
4. Masoumi M, Bozorgi M, Nourmohammadi Z, Mousavi MJ, Shariati A, Karami J. Evaluation of hematological markers as prognostic tools in rheumatoid arthritis. BMC Rheumatol. 2024;8(1):75. doi:10.1186/s41927-024-00444-0
5. Zhang C, Lu S, Kang T, et al. Red cell distribution width/albumin ratio and mortality risk in rheumatoid arthritis patients: insights from a NHANES study. Int J Rheu Dis. 2024;27(9):e15335. doi:10.1111/1756-185X.15335
6. He Y, Liu C, Zeng Z, Ye W, Lin J, Ou Q. Red blood cell distribution width: a potential laboratory parameter for monitoring inflammation in rheumatoid arthritis. Clin Rheumatol. 2018;37(1):161–167. doi:10.1007/s10067-017-3871-7
7. Chen Y, Chen Y, Zhao L, et al. Albumin/globulin ratio as Yin-Yang in rheumatoid arthritis and its correlation to inflamm-aging cytokines. J Inflamm Res. 2021;14:5501–5511. doi:10.2147/JIR.S335671
8. Zengin O, Onder ME, Kalem A, et al. New inflammatory markers in early rheumatoid arthritis. Neue inflammatorische Marker für die frühe rheumatoide Arthritis. Zeitschrift fur Rheumatologie. 2018;77(2):144–150. doi:10.1007/s00393-016-0187-y
9. Mangoni AA, Zinellu A. Diagnostic accuracy of the neutrophil-to-lymphocyte ratio and the platelet-to-lymphocyte ratio in rheumatoid arthritis: a systematic review and meta-analysis. Clin Exp Med. 2024;24(1):207. doi:10.1007/s10238-024-01478-x
10. Cui P, Cheng T, Yan H, Xu D, Ren G, Ma S. The value of NLR and PLR in the diagnosis of rheumatoid arthritis combined with interstitial lung disease and assessment of treatment effect: a retrospective cohort study. Int J Gene Med. 2025;18:867–880. doi:10.2147/IJGM.S509546
11. Erre GL, Buscetta G, Mangoni AA, et al. Diagnostic accuracy of different blood cells-derived indexes in rheumatoid arthritis: a cross-sectional study. Medicine. 2020;99(44):e22557. doi:10.1097/MD.0000000000022557
12. Romo-Cordero A, González-Sierra M, Quevedo-Abeledo JC, et al. The ratio of monocytes to HDL-cholesterol is associated with cardiovascular risk and insulin resistance in patients with rheumatoid arthritis. Life. 2023;13(10):1995. doi:10.3390/life13101995
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Identification of Disulfidptosis-Related Genes and Molecular Subgroups in Rheumatoid Arthritis for Diagnostic Model and Patient Stratification
Liu X, Wang S, Du X, Wang Y, Mo L, Li H, Qu Z, Wang X, Sun J, Li Y, Wang J
Journal of Inflammation Research 2025, 18:4157-4175
Published Date: 19 March 2025