Back to Journals » Breast Cancer: Targets and Therapy » Volume 15
Recurrent Metaplastic Breast Cancer with Subtype Converted from Triple-Negative to HER2-Positive: A Case Report and Literature Review
Authors Wu J, Jin Y, Liu M, Zhu N, Jing Z, Zeng X
Received 2 November 2022
Accepted for publication 12 January 2023
Published 19 January 2023 Volume 2023:15 Pages 39—45
DOI https://doi.org/10.2147/BCTT.S395944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Jing Wu,1,* Yudi Jin,2,* Mei Liu,1,* Ningsheng Zhu,1 Zhouhong Jing,1 Xiaohua Zeng1
1Department of Breast Center, Chongqing Key Laboratory for Intelligent Oncology in Breast Cancer (iCQBC), Chongqing University Cancer Hospital, Chongqing, 400030, People’s Republic of China; 2Department of Pathology, Chongqing Key Laboratory for Intelligent Oncology in Breast Cancer (iCQBC), Chongqing University Cancer Hospital, Chongqing, 400030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohua Zeng, Department of Breast Center, Chongqing Key Laboratory for Intelligent Oncology in Breast Cancer (iCQBC), Chongqing University Cancer Hospital, Chongqing, 400030, People’s Republic of China, Email [email protected]
Background: Metaplastic breast cancer (MBC) is an extremely rare malignant breast disease that has rarely been reported. The molecular subtype of MBC is mostly triple-negative, with a high recurrence rate and a worse prognosis. Due to its low HR- and HER2-positive rate, reports on endocrine and targeted therapy are very limited.
Case report: We report a case of infrequent triple-negative MBC, which, although at an early stage, quickly developed multiple recurrent lesions in the chest wall. The tumor relapsed repeatedly after comprehensive treatment, including surgery, chemotherapy and radiotherapy. However, pathological results after the third surgery suggested that the molecular subtype had changed from triple-negative to HER2-positive. The previous comprehensive treatment had not been able to effectively control the disease, but the patient achieved a long progression-free survival time through chemotherapy and trastuzumab targeted therapy after the subtype change. To date, there has been no recurrence for over eight years.
Conclusion: Among repeatedly relapsed MBC patients, further investigation should be taken into consideration. As in the case presented in our study, it is possible that the HER2 status can convert from negative to overexpression. Moreover, for HER2-positive MBC patients, anti-HER2 therapy is recommended. The decision-making process requires multidisciplinary involvement.
Keywords: metaplastic breast cancer, triple-negative, HER2-positive, recurrence, targeted therapy
Plain Language Summary
Among breast cancer patients, HER2 status is divided into positive (HER2 protein overexpression on IHC analysis—score 3+ and/or HER2 gene amplification on ISH assay) or negative. However, some patients show low HER2 expression (1+ or 2+ by IHC in the absence of HER2 gene amplification by ISH). Previous studies indicate that the HER2 status of these patients is unstable and might switch. We report a metaplastic breast cancer patient who relapsed repeatedly. After her HER2 status switched from negative to positive, she received anti-HER2 targeted therapy and has been disease-free for more than eight years.
Background
Metaplastic breast cancer (MBC) is a rare subtype of malignant breast tumor that is defined as a heterogeneous tumor with a low degree of differentiation. Currently, MBC is divided into the following subgroups: 1) squamous cell carcinoma; 2) spindle cell carcinoma; 3) low-grade adenosquamous carcinoma; 4) fibromatosis-like metaplastic carcinoma; 5) MBC with mesenchymal differentiation; 6) myoepithelial carcinoma; and 7) mixed metaplastic carcinoma. MBC accounts for less than 5% of all breast cancer cases and is usually characterized by a large primary tumor size, a lower estrogen receptor (ER) and progesterone receptor (PR) positive rate, and a lower rate of human epidermal growth factor receptor 2 (HER2) overexpression.1 In general, MBC is similar to triple-negative breast cancer (TNBC) in some characteristics; it has a higher rate of postoperative recurrence and metastasis, relatively less frequent involvement of the axillary lymph nodes but a worse prognosis than TNBC.2 The recognition and study of MBC are insufficient due to the restriction of uncommon cases and observation data, and the best treatment strategy for MBC is still unclear.
To date, there are no guidelines for MBC, and most treatment protocols are based on the guidelines for breast cancer. MBC is usually accompanied by resistance to chemotherapy, leading to unsatisfactory therapeutic effects.3,4 In a previous study, researchers concluded that, in addition to surgery, chemotherapy, and radiotherapy, targeted therapies are expected to improve the outcome of this aggressive tumor and augment the dismal survival of patients.5–7
We present a rare case in which the molecular type changed from a triple-negative subtype with poor prognosis to a HER2 overexpression subtype with a relatively good prognosis. After comprehensive treatment, the patient achieved progression-free survival (PFS) of more than 8 years, which is remarkably unique given the extremely poor prognosis of MBC. The treatment process is depicted in Figure 1. This case demonstrated that clinicians should pay attention to the possibility of molecular type changes in metaplastic breast cancer during treatment, and thus, repeated biopsy of recurrent lesions is necessary. In addition, this case also suggested that a change in an important therapeutic target may enable patients to regain the chance of cure, and anti-HER2 targeted therapy may play a key role in HER2-positive MBC.
 |
Figure 1 The patient treatment process from September 2012 to December 2022. |
Case Report
In September 2012, a 47-year-old woman came to Chongqing University Cancer Hospital because a 2 cm mass was accidentally found in the outer upper quadrant of the right breast. The patient was in good health before and had no family history of cancer. After completing the medical examination, the results suggested breast cancer without positive findings in distant organs. Biopsy identified it as invasive carcinoma and partial squamous cell carcinoma, and the clinical stage was T1N0M0. Then, she received a modified radical mastectomy. Pathology after the operation revealed that the mass was squamous cell carcinoma and partial ductal carcinoma in situ (Figure 2A), with noninvolvement of the axillary lymph nodes. Immunohistochemical results were negative for ER, PR and HER-2 (Figure 2B–, respectively), and the Ki67 index was 60% (Figure 2E). In addition, CK5/6, P40, P63, Vimentin and E-cadherin were positive (Figure 2F–, respectively). Five cycles of TAC adjuvant chemotherapy (100 mg docetaxel, 50 mg pirarubicin and 700 mg cyclophosphamide) was subsequently administered.
 |
Figure 2 Pathological images of the patient in September 2012: HE, 100x (A); ER, 200x (B); PR, 200x (C); CerbB-2, 200x (D); Ki67, 200x (E); CK5/6, 200x (F); P40, 200x (G); P63, 200x (H); Vimentin, 200x (I); E-cadherin, 200x (J). Pathological images of the patient in July 2014: HE, 200x (K); FISH (L). |
Unfortunately, only four months later, in January 2013, a new lump was discovered in the right chest wall. Fine needle aspiration (FNA) demonstrated squamous cell carcinoma, and an extended lumpectomy was performed. Postoperative pathology confirmed recurrence of MBC in the chest wall and the molecular type was still triple-negative (Supplementary Material). The patient received 4 cycles of NP chemotherapy (35 mg navelbine on both Day 1 and Day 8 and 40 mg cis-platinum from Day 1 to Day 3) in February, April, May and June 2013. In addition, between March and April 2013, she received palliative radiotherapy (right chest wall and right subclavian area, 6 MV with X-ray, PTV: DT50Gy/25F). Unfortunately, the patient still experienced disease progression during chemotherapy. In June 2013, the patient found a 2 cm mass in the right axilla, and FNA showed adenocarcinoma cells. CT revealed a soft tissue mass in the right axillary region (Figure 3A), which was approximately 3 cm in size. In July 2013, the patient received S-1(40 mg, bid, Day 1 to Day 14) chemotherapy and one cycle of biological therapy in an external hospital, which did not achieve good effect. Between August 2013 and September 2013, the patient received palliative radiotherapy again (right axilla, 6 MeV with electronic ray, PGTV: 60 Gy/30 F) due to the obvious enlargement of the right axillary mass (Figure 3B). From October 17, 2013, to June 7, 2014, the patient completed seven cycles of chemotherapy (gemcitabine, 1200 mg, Day 1 and Day 8). CT images showed that the right breast mass, although reduced, was still present (Figure 3C).
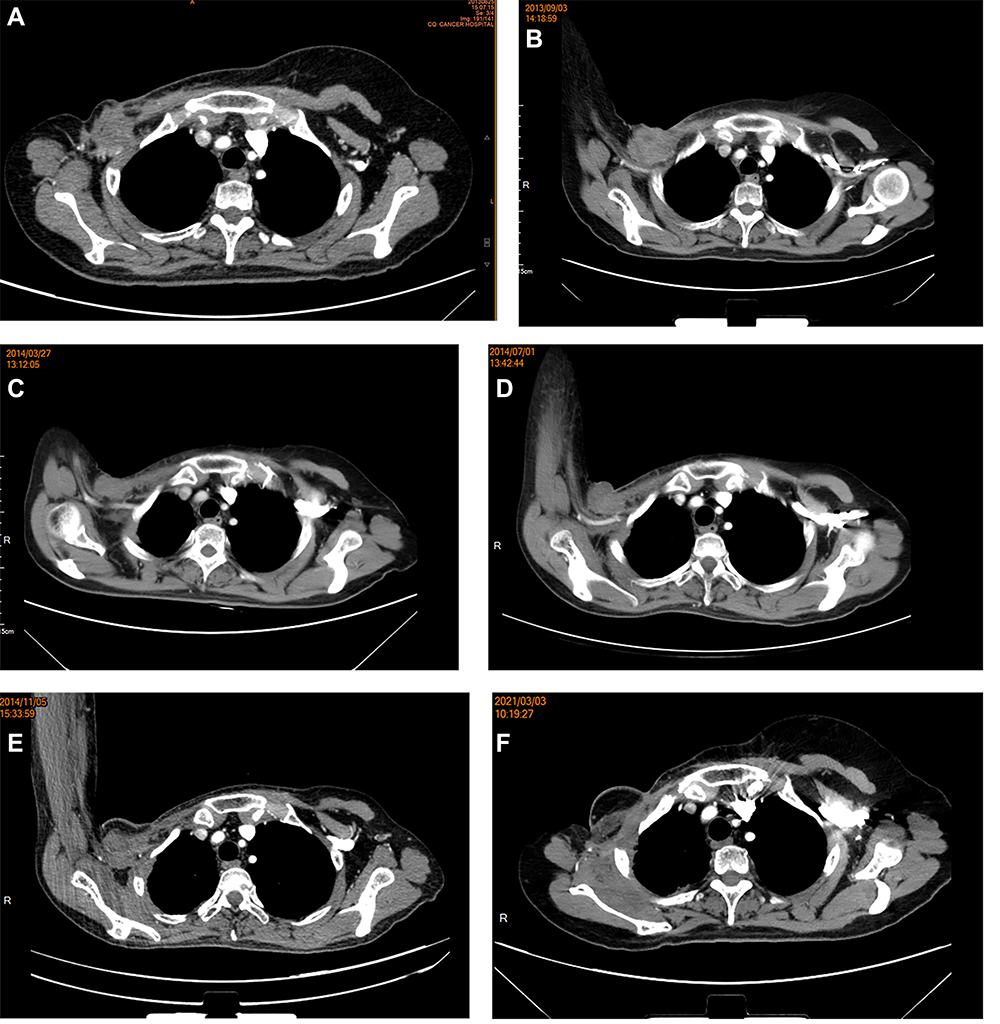 |
Figure 3 CT images of the patient in June 2013 (A); September 2013 (B); March 2014 (C); July 2014 (D); November 2014 (E); and March 2021 (F). |
In July 2014, the chemotherapy regimen for the patient was changed to one cycle of chemotherapy (paclitaxel liposome, 120 mg, qw, and capecitabine, 1500mg, bid, Day 1 to Day 14) due to the gradually increasing lump in the right armpit (Figure 3D), but the mass did not shrink significantly. Subsequently, the patient gave up chemotherapy and underwent extensive surgical resection of the right axillary mass in an external hospital. Pathological results still showed squamous cell carcinoma, histological grade II (Figure 2K). Immunohistochemistry revealed the same results as previously found except HER2 was 2+. Hence, fluorescence in situ hybridization was performed and showed that HER2 was overexpressed (Figure 2L). Thereafter, the patient received trastuzumab targeted therapy combined with capecitabine 1.5 g bid for one year. From July 2015 to the present, the patient has taken oral capecitabine intermittently. Since then, no signs of recurrence have been found (Figure 3Eand Figure 3). A recent follow-up in December 2022 via telephone suggested that the patient was in fair condition.
Discussion
MBC is a very rare malignant breast tumor, accounting for approximately 0.2–5% of malignant breast tumors. Since it was first described in 1973, there have been no large prospective clinical studies of MBC due to its rarity. The largest previous study was conducted by Haque et al, who performed a retrospective study of a total of 5211 MBC patients,6 but other studies have mostly been conducted in a cohort of 100 or dozens of patients.2–5 At present, the treatment of MBC mainly refers to breast cancer treatment regimens and involves comprehensive treatment, such as surgery, chemotherapy and radiotherapy. Surgery is the cornerstone of treatment for early-stage MBC patients. Previous research has demonstrated that MBC patients who undergo breast-conserving surgery plus radiotherapy exhibit a better prognosis than those who undergo mastectomy alone.8,9 Evidence has also suggested that chemotherapy is associated with improved prognosis.5,10 Meanwhile, most current studies agree on the important role of radiotherapy in improving prognosis.11,12 In addition, Kalaw et al13 found that PD-L1 is more likely to be positive in MBC than in TNBC, suggesting that immunotherapy may be an effective treatment for some MBC patients. Notably, several studies have reported that targeted therapy may be a key treatment for MBC patients,10,14,15 which is consistent with our case.
In the case of our study, the remarkable observation was that there was a change in the molecular type during the treatment, namely, a conversion in HER2 status from negative to positive. We carefully reviewed previous studies and found that only a few of them mentioned changes in pathological types,16,17 while none of these reports mentioned changes in molecular type. Miglietta et al highlighted that HER2 expression was highly unstable during disease evolution and reported that HER2 discordance was mostly driven by cases switching from HER2-negative to HER2-low.18 In particular, a recent trial in patients with HER2-low metastatic breast cancer found that trastuzumab deruxtecan (T-DXd) significantly improved prognosis compared with the physician’s choice of chemotherapy.19 Therefore, the transformation from HER2-negative to HER2-low or HER2-overexpressing might provide new opportunities for relapsed or metastatic patients.
To the best of our knowledge, our report is the first to mention a change in the molecular type of MBC, which converted from HER2-negative to HER2-positive. However, there are limitations in our work. First, for various reasons, such as hospital changes for treatment and imaging system changes, some of the CT scans and pathology images were not found. Second, we think that the patient’s HER2 status might have changed before July 2014 because we only performed the FNA in June 2013 considering the patient’s limited economic resources, so we did not catch it in time. Third, we do not know the exact reason for the HER2 status change in the patient, and more research is needed.
Conclusion
Although MBC is a rare and dangerous cancer type, our experience indicated that comprehensive treatment is feasible. In MBC patients, HER2 status may be converted. In patients with tumor recurrence or metastasis, repeated pathological examination is of vital importance. Meanwhile, we highlight that HER2-positive metastatic breast cancer patients should receive anti-HER2 targeted therapy. Notwithstanding, the detailed treatment scheme still requires further research.
Data Sharing Statement
The clinical data related to the study have been included in the manuscript, and further information can be requested from the corresponding author.
Ethics Approval and Informed Consent
Written informed consent was obtained from the patient, and she agreed to publication of the details of her case, as well as any CT and pathological images. This study and the publication of the case report were approved by the ethics committee of Chongqing University Cancer Hospital.
Acknowledgments
The authors thank Dr. Fanlin Zhou (Department of Pathology, Chongqing University Cancer Hospital) for assisting in the interpretation of pathological reports. During the long time span of the described case, the electronic medical system used in our hospital changed; thus, the radiology images obtained before June 2013 could not be collected. Therefore, the CT images of this case started in June 2013.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the foundation of Chongqing University Cancer Hospital (Grant No. LY2019003) and the Talent Program of Chongqing (Grant No. CQYC20200303137).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Reddy TP, Rosato RR, Li X, et al. A comprehensive overview of metaplastic breast cancer: clinical features and molecular aberrations. Breast Cancer Res. 2020;22(1):121. doi:10.1186/s13058-020-01353-z
2. El Zein D, Hughes M, Kumar S, et al. Metaplastic carcinoma of the breast is more aggressive than triple-negative breast cancer: a study from a single institution and review of literature. Clin Breast Cancer. 2017;17(5):382–391. doi:10.1016/j.clbc.2017.04.009
3. Wong W, Brogi E, Reis-Filho JS, et al. Poor response to neoadjuvant chemotherapy in metaplastic breast carcinoma. NPJ Breast Cancer. 2021;7(1):96. doi:10.1038/s41523-021-00302-z
4. Leyrer CM, Berriochoa CA, Agrawal S, et al. Predictive factors on outcomes in metaplastic breast cancer. Breast Cancer Res Treat. 2017;165(3):499–504. doi:10.1007/s10549-017-4367-5
5. Toumi Z, Bullen C, Tang AC, et al. Metaplastic breast carcinoma: a case report and systematic review of the literature. Pathol Int. 2011;61(10):582–588. doi:10.1111/j.1440-1827.2011.02698.x
6. Haque W, Verma V, Naik N, et al. Metaplastic breast cancer: practice patterns, outcomes, and the role of radiotherapy. Ann Surg Oncol. 2018;25(4):928–936. doi:10.1245/s10434-017-6316-2
7. Tray N, Taff J, Adams S. Therapeutic landscape of metaplastic breast cancer. Cancer Treat Rev. 2019;79:101888. doi:10.1016/j.ctrv.2019.08.004
8. Xia LY, Xu WY, Hu QL. The different outcomes between breast-conserving surgery plus radiotherapy and mastectomy in metaplastic breast cancer: a population-based study. PLoS One. 2021;16(9):e0256893. doi:10.1371/journal.pone.0256893
9. Zhang J, Yang C, Lei C, et al. Survival outcomes after breast-conserving therapy compared with mastectomy for patients with early-stage metaplastic breast cancer: a population-based study of 2412 patients. Breast. 2021;58:10–17. doi:10.1016/j.breast.2021.03.010
10. Tadros AB, Sevilimedu V, Giri DD, et al. Survival outcomes for metaplastic breast cancer differ by histologic subtype. Ann Surg Oncol. 2021;28(8):4245–4253. doi:10.1245/s10434-020-09430-5
11. Li Y, Chen M, Pardini B, et al. The role of radiotherapy in metaplastic breast cancer: a propensity score-matched analysis of the SEER database. J Transl Med. 2019;17(1):318. doi:10.1186/s12967-019-2069-y
12. Nowara E, Drosik A, Samborska-Plewicka M, et al. Metaplastic breast carcinomas - analysis of prognostic factors in a case series. Contemp Oncol. 2014;18(2):116–119. doi:10.5114/wo.2014.41392
13. Kalaw E, Lim M, Kutasovic JR, et al. Metaplastic breast cancers frequently express immune checkpoint markers FOXP3 and PD-L1. Br J Cancer. 2020;123(11):1665–1672. doi:10.1038/s41416-020-01065-3
14. Jin C, Hacking S, Sajjan S, et al. GATA binding protein 3 (GATA3) as a marker for metaplastic spindle cell carcinoma of the breast. Pathol Res Pract. 2021;221:153413. doi:10.1016/j.prp.2021.153413
15. Shah VV, Duncan AD, Jiang S, et al. Mammary-specific expression of Trim24 establishes a mouse model of human metaplastic breast cancer. Nat Commun. 2021;12(1):5389. doi:10.1038/s41467-021-25650-z
16. Guo TH, Chen ZY, Xu JP, et al. Change of pathological type to metaplastic squamous cell carcinoma of the breast during disease recurrence: case report and literature review. Front Oncol. 2020;10:32. doi:10.3389/fonc.2020.00032
17. Chuthapisith S, Warnnissorn M, Amornpinyokiat N, et al. Metaplastic carcinoma of the breast with transformation from adenosquamous carcinoma to osteosarcomatoid and spindle cell morphology. Oncol Lett. 2013;6(3):728–732. doi:10.3892/ol.2013.1464
18. Miglietta F, Griguolo G, Bottosso M, et al. Evolution of HER2-low expression from primary to recurrent breast cancer. NPJ Breast Cancer. 2021;7(1):137. doi:10.1038/s41523-021-00343-4
19. Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.