Back to Journals » OncoTargets and Therapy » Volume 9
Recurrence pattern of squamous cell carcinoma in the midthoracic esophagus: implications for the clinical target volume design of postoperative radiotherapy
Authors Wang X, Luo Y, Li M, Yan H, Sun M, Fan T
Received 3 July 2016
Accepted for publication 29 August 2016
Published 3 October 2016 Volume 2016:9 Pages 6021—6027
DOI https://doi.org/10.2147/OTT.S116348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samir Farghaly
Xiaoli Wang,1,2,* Yijun Luo,1,2,* Minghuan Li,2 Hongjiang Yan,2 Mingping Sun,2 Tingyong Fan2
1School of Medicine and Life Sciences, Jinan University-Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 2Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Background: Postoperative radiotherapy has shown positive efficacy in lowering the recurrence rate and improving the survival rate for patients with esophageal squamous cell carcinoma (ESCC). However, controversies still exist about the postoperative prophylactic radiation target volume. This study was designed to analyze the patterns of recurrence and to provide a reference for determination of the postoperative radiotherapy target volume for patients with midthoracic ESCC.
Patients and methods: A total of 338 patients with recurrent or metastatic midthoracic ESCC after radical surgery were retrospectively examined. The patterns of recurrence including locoregional and distant metastasis were analyzed for these patients.
Results: The rates of lymph node (LN) metastasis were 28.4% supraclavicular, 77.2% upper mediastinal, 32.0% middle mediastinal, 50.0% lower mediastinal, and 19.5% abdominal LNs. In subgroup analyses, the rate of abdominal LN metastasis was significantly higher in patients with histological node-positive than that in patients with histological node-negative (P=0.033). Further analysis in patients with histological node-positive demonstrated that patients with three or more positive nodes are more prone to abdominal LN metastasis, compared with patients with one or two positive nodes (χ2=4.367, P=0.037). The length of tumor and histological differentiation were also the high-risk factors for abdominal LN metastasis.
Conclusion: For midthoracic ESCC with histological node-negative, or one or two positive nodes, the supraclavicular and stations 2, 4, 5, and 7 LNs should be delineated as clinical target volume of postoperative prophylactic irradiation, and upper abdominal LNs should be excluded. While for midthoracic ESCC with three or more positive nodes, upper abdominal LNs should also be included. The length of tumor and histological differentiation should be considered comprehensively to design the clinical target volume for radiotherapy.
Keywords: esophagus cancer, radiotherapy, recurrence and metastasis, clinical target volume
Introduction
Esophageal carcinomas (ECs) are one of the most malignant gastrointestinal cancers worldwide; they are the sixth most common cause of cancer-related mortality.1,2 In the People’s Republic of China, the predominant pathological type of EC is esophageal squamous cell carcinoma (ESCC), which is characterized by rapid development and fatal prognosis in most cases, and many tumors locate in the middle third thoracic.
Surgery is an extremely important initial treatment for patients with ESCC. For patients with locally advanced ESCC, the standard treatment is neoadjuvant chemotherapy or chemoradiotherapy followed by esophagectomy with lymphadenectomy. However, most patients in the People’s Republic of China generally prefer surgery to neoadjuvant therapy as their initial therapeutic strategy, and surgery alone has shown rather disappointed survival rates, of which the 5-year survival rate is only 20%–50%.3–5 The recurrence rate of ESCC is as high as 40%–50% after radical resection, and locoregional recurrence is the main reason for treatment failure, not excepting patients with histological node-negative (pN0 stage).4,6,7 The current National Comprehensive Cancer Network (NCCN) guidelines still recommend surveillance for ESCC patients who have undergone curative resection. Therefore, it is extremely essential to evaluate the efficacy of adjuvant radiotherapy. According to multiple retrospective analyses, the addition of postoperative radiotherapy (PORT) has been associated with survival benefit in patients with positive lymph node (LN) metastasis (N+) or stage III.8–11
However, up until now, the appropriate LN clinical target volume (CTVn) for postoperative prophylactic irradiation therapy still remains disputed, especially for midthoracic ESCC. Recent and previous studies are consistent in revealing that the anastomosis, supraclavicular, and mediastinal lymph drainage areas should be delineated as the postoperative prophylactic irradiation target volume, while little effort has been made to study the patterns of recurrence of midthoracic ESCC according to the pathological LN status. To our knowledge, to date, only Zhang et al12 indicated that upper abdominal LNs should also be included as the postoperative prophylactic irradiation target volume for midthoracic ESCC patients with pathological node-positive.
Based on the study by Zhang et al,12 we further analyzed the patterns of recurrence and metastasis of the midthoracic ESCC according to the pathological LN status after radical surgery, which was detected with follow-up computed tomography (CT), to identify the risk factors responsible for recurrence and to provide a reference for determination of the PORT target volume.
Patients and methods
Patients
After obtaining approval from the Medical Ethics Committee of Shandong Cancer Hospital and Institute, we retrospectively studied 1,540 patients with midthoracic ESCC who had undergone radical esophagectomy at the Department of Thoracic Surgical Oncology in Shandong Cancer Hospital during January 2008 through December 2012. All participants provided written informed consent for the current study. According to the seventh edition of the American Joint Committee on Cancer (AJCC) criteria, typical endoscopic measurements for the midthoracic esophagus measured from the incisors range from 25 cm to <30 cm. The inclusion criteria enrolled in this study were as follows: 1) the tumor was confirmed by preoperative esophageal endoscopy and postoperative pathology as a clearly diagnosed squamous cell carcinoma; 2) upper bound of the tumors located in the middle is summarized as middle EC; 3) all the patients were pathologically confirmed with R0 resection; 4) no evidence of cervical or supraclavicular LN metastasis before surgery; and 5) no active malignancy in other organs. The exclusion criteria were as follows: 1) a histological diagnosis of adenocarcinoma or other histological types; 2) patients who received preoperative radiotherapy and/or chemotherapy; 3) inadequate survival information; and 4) patients who received PORT before recurrence.
Adjuvant therapies
Up until now, the generally accepted guidelines of postoperative adjuvant therapy for ESCC have not been established in the People’s Republic of China. In our institution, the indications of adjuvant treatment are mainly based on tumor stage, high-risk factors, doctors’ habits, and patients’ willingness or economic status. In total, 26.6% (90/338) of patients received one to six cycles of postoperative chemotherapy (mainly 5-fluorouracil and cisplatin/carboplatin) in our study. Patients who have received adjuvant chemotherapy after surgery in histological node-negative and histological node-positive comprised 17.9% and 11.8%, respectively.
Diagnosis standard
The modes of tumor recurrence after radical surgery among patients with thoracic ESCC were divided into three types: locoregional recurrence, distant metastasis, and combined recurrence (locoregional plus distant metastasis found within 30 days). Locoregional recurrences included tumor bed, anastomotic site, or LN metastasis, which was based on the site of recurrence. Distant metastasis was defined as tumor that presented in the distant organs, such as lungs, liver, bones, or brain, through hematogenous spread. The diagnosis of recurrent mediastinal and abdominal LNs was mainly based on follow-up CT or positron emission tomography/CT images. However, the recurrences of suspected esophageal and neck/supraclavicular node were confirmed using histological or cytologic evaluation. In this study, the supraclavicular, mediastinal, and upper abdominal LNs were considered as regional LNs. The boundaries of LN regions were divided into ten areas on the basis of the CT-based definition of anatomical landmarks:13 Station 1, highest mediastinal nodes; Station 2, upper paratracheal nodes; Station 3, prevascular nodes and retrotracheal nodes; Station 4, lower paratracheal nodes; Station 5, subaortic (aortic-pulmonary window) nodes; Station 6, para-aortic nodes or anterior aortic nodes; Station 7, subcarinal nodes; Station 8, paraesophageal nodes; Station 9, pulmonary ligament nodes; and Station 10, hilar nodes. And the site of upper abdominal LN metastasis depends on gastric LN partition. When the evidence of a single LN with a short axis >10 mm or a single LN with a short axis <10 mm combined with hoarseness or vocal cord paralysis was defined as recurrent disease, the diagnosis of regional LN recurrence was clear.
Statistical analyses
Statistical analyses were performed with the Statistical Program for Social Sciences for Windows, version 20.0 (IBM Corporation, Armonk, NY, USA). A χ2 test was used for categorical data analyses. Univariate and multivariate logistic regression analyses were used to analyze the relationship between clinicopathological factors and upper abdominal LN recurrence. A P-value <0.05 was considered statistically significant for all procedures.
Results
Patient characteristics
Among the 1,540 patients, 896 patients who received preoperative radiotherapy/PORT or a histological diagnosis of adenocarcinoma or other histological types were excluded from the study. A total of 338 (338/644, 52.5%) patients who experienced recurrent or metastatic midthoracic ESCC were enrolled in this study, and the remaining (306, 47.5%) patients who did not have any sign of recurrence were also excluded. The eligible patients included 291 males and 47 females, with a median age of 56 years (range 45–79 years). According to the seventh edition of the AJCC criteria, 1.8% patients were stage I, 35.5% patients were stage II, and 62.7% patients were stage III. In our study, 297 (87.9%) patients underwent extended radical esophagectomy with two-field lymphadenectomy (including mediastinal and abdominal lymphadenectomy), and only 41 patients underwent radical esophagectomy with three-field lymphadenectomy. Overall, 146 patients (43.2%) had node-negative disease and 192 patients (56.8%) had nodal metastases. The patients’ clinical and pathological characteristics are summarized in Table 1.
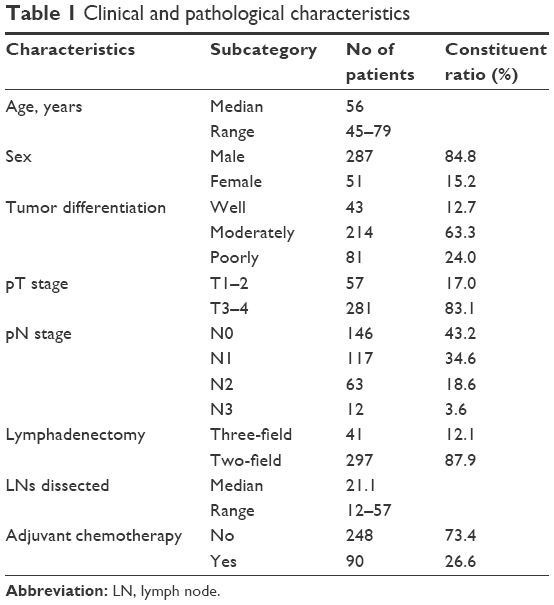 | Table 1 Clinical and pathological characteristics |
Recurrence types
A total of 7,084 LNs were resected in all enrolled patients. The mean number of dissected LNs was 10.6 per person (range 12–57). Among them, 72 patients had one positive node, 42 patients had two positive nodes, and 78 patients had three or more positive nodes. The most common pattern of recurrence was locoregional recurrence, which was found in 299 patients (88.4%); 39 patients (11.6%) had distant recurrence, and 24 patients (7.1%) had combined recurrence. The mediastinal LNs had the highest metastatic rates (83.1%), followed by supraclavicular LNs (28.4%) and abdominal LNs (19.5%). The main sites of hematogenous recurrence were the liver (38.5%, 15/39), and similar rates were observed in the lung (30.8%, 12/39) and pleural membrane (30.8%, 12/39), but the least in the bone (15.4%, 4/39). The distribution of recurrence and metastasis in 338 patients with middle thoracic ESCC is summarized in Table 2.
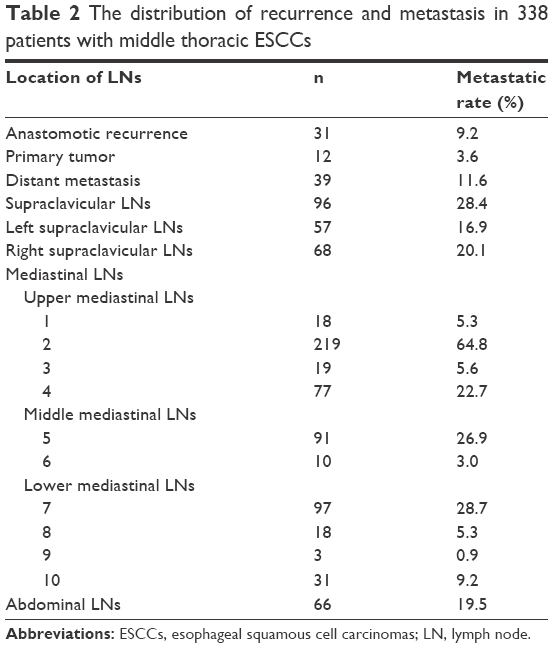 | Table 2 The distribution of recurrence and metastasis in 338 patients with middle thoracic ESCCs |
Subgroup analysis
Although the metastatic rate of abdominal LNs was relatively low, in subgroup analysis, the abdominal LN metastasis rate was significantly higher in patients with histological node-positive than that in patients with histological node-negative (P=0.033). Further analysis in patients with histological node-positive demonstrated that patients with three or more positive nodes are more prone to upper abdominal LN metastasis, compared with patients with one or two positive nodes (χ2=4.367, P=0.037; Table 3). Univariate and multivariate analyses of risk factors related to upper abdominal LN metastasis were summarized in Table 4. The sites of midthoracic ESCC patients experiencing recurrent abdominal LNs are mainly in the retroperitoneal region. The LNs in the left gastric artery, common hepatic artery, celiac artery, and retropancreatic and para-aortic regions are high-risk areas for locoregional metastasis, demonstrating that the target volume of the adjuvant radiotherapy following surgery should include the above-mentioned regions.
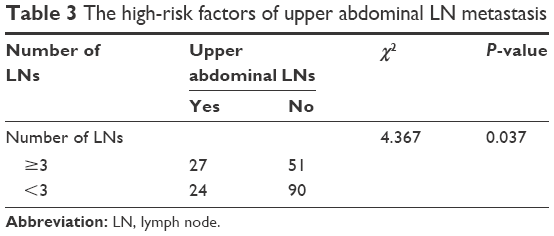 | Table 3 The high-risk factors of upper abdominal LN metastasis |
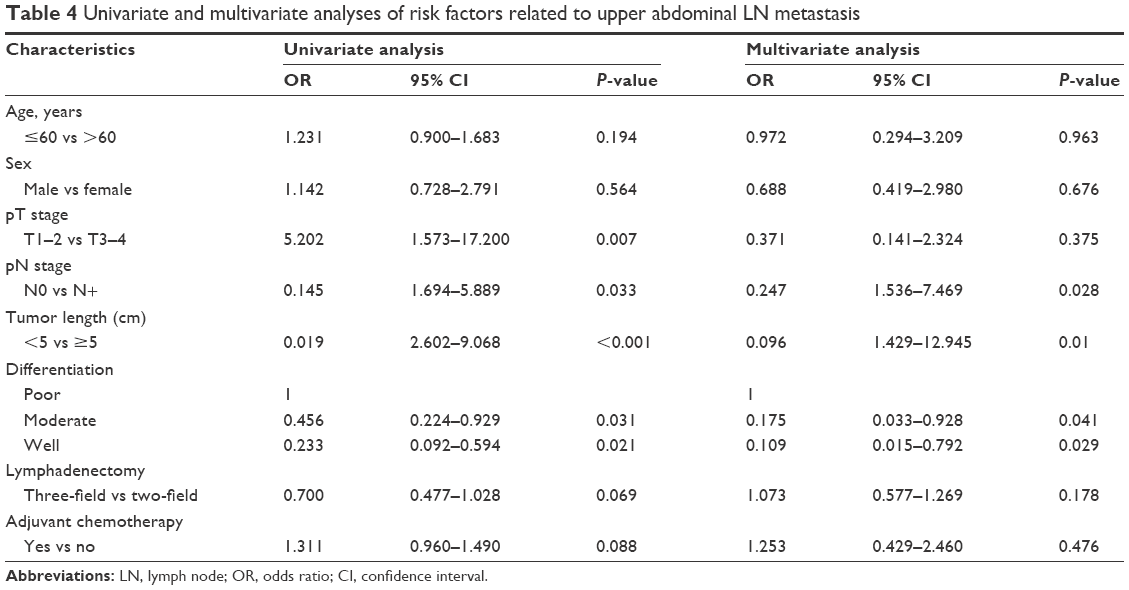 | Table 4 Univariate and multivariate analyses of risk factors related to upper abdominal LN metastasis |
Discussion
Currently, surgery is the mainstay treatment for thoracic ESCC. However, the overall 5-year survival rate remains dissatisfied because of the early and high recurrence after surgery. Moreover, the growing popularity of multimodality treatments has added to the debate of the role and the optimal extent of surgery. In addition, radiation therapy, acted as a local treatment strategy, became more and more popular in the treatment of EC, especially for the lesions in locally advanced ESCC.
Although the current NCCN guidelines still recommend surveillance for ESCC patients who have undergone curative resection, several trials and retrospective studies have assessed the survival impact of adjuvant radiation therapy and revealed that patients with stage III disease or LN metastasis, particularly those with three or more positive nodes, can benefit from receiving adjuvant radiotherapy.14–17
In this study, more than half (62.5%) of recurrent patients were in stage III; therefore, the addition of PORT is necessary to reduce the recurrence rate. However, the optimal CTVn of postoperative prophylactic irradiation for thoracic ESCC remains disputed, especially the midthoracic target volume. Because midthoracic EC has the characteristics that can not only metastasize upward to neck and upper mediastinal LNs but also metastasize downward to lower mediastinal and upper abdominal LNs, and certain efforts have been paid to the pattern of failure after radical surgery among patients with thoracic ESCC. However, the optimal CTVn of postoperative prophylactic irradiation for thoracic ESCC has not drawn to a conclusion. In a study, Li et al18 revealed that supraclavicular nodes, recurrent laryngeal nerve nodes, azygos nodes, and subcarinal nodes are the high-risk lymphatic drainage areas. Therefore, supraclavicular nodes and upper mediastinal LN regions should be delineated as the CTVn of PORT. Cai and Xin19 found that the recurrence rate of upper abdominal LNs was 12.8% for midthoracic ESCC. What should be incorporated into CTV of postoperative prophylactic irradiation for thoracic ESCC is that the sites with LN metastasis rate >15% (an empirical cutoff value), which were considered as high-risk areas. Therefore, they recommend that the target volumes of PORT should include anastomosis, supraclavicular, and stations 1–5 and 7 LNs, with upper abdominal LNs excluded for midthoracic ESCC.19 Lu et al20 in a retrospective study indicated that the left gastric area is unnecessarily delineated as the PORT target volume when the primary tumor site locates in the middle or middle upper thirds of the thoracic esophagus; similarly, the bilateral supraclavicular area is unnecessarily delineated as the PORT target volume when the primary site locates in the middle lower thirds. However, Zhang et al12 revealed that for the midthoracic ESCC with histological node-negative, the target volume of PORT recommended to include the supraclavicular nodes, upper mediastinal LN region, and the site of primary tumor, while for the middle thoracic EC with histological node-positive, the PORT target volume recommended to include the supraclavicular nodes, mediastinal LN region, left gastric artery LNs, and celiac artery LNs. For upper abdominal LNs, our findings were consistent with the result of Zhang et al. However, the primary tumor recurrence rate in our study is 3.6%, which is not recommended to be included in the CTVn of postoperative prophylactic irradiation.
In our data, the rate of abdominal LN metastasis was 19.5%. The possible reason was that some patients with middle-low thoracic ESCC were also enrolled in this study. Our results confirmed that tumor length was an independent high-risk factor for celiac lymph node metastasis. The low EC has the characteristics of high upper abdominal LN metastasis rate. What has reached a consensus is that the sites with LN metastasis rate >15% were deemed as high-risk areas and were included in CTVn of thoracic ESCC patients for PORT. That is, the abdominal LNs should be irradiated after radical surgery. However, large radiation field damages normal tissues extensively, which would seriously affect the patients’ quality of life. Therefore, for upper abdominal LNs, we conducted subgroup analysis on the basis of histological node status. The outcomes found that the rate of abdominal LN metastasis was significantly higher in patients with histological node-positive than that in patients with histological node-negative. The results also revealed that patients with three or more positive nodes are more prone to celiac LN metastasis, compared with patients with one or two positive nodes. Wu et al21 in a retrospective study also showed that celiac LN recurrence was more frequent among patients with advanced pathological nodal (pN) stage (pN2, P=0.034; pN3, P=0.009), which was consistent with our study. Therefore, histological node-positive and the number of LN metastases are high-risk factors for patients with postoperative abdominal LN metastasis. For patients presented with histological node-positive, especially for midthoracic ESCC with three or more positive nodes or histological node-positive, upper abdominal LNs should be delineated as CTV of postoperative prophylactic irradiation. Similar to the study of Huang et al,22 our outcome also revealed that the length of tumor and the histological differentiation are high risk factors to upper abdominal LN metastasis for midthoracic ESCC, which should be considered comprehensively to design the CTV for adjuvant radiotherapy.
In this study, the incidence of supraclavicular and upper mediastinal, particularly the recurrent laryngeal nerve, is high. The following two possible reasons can explain this. First, the complex anatomical structures and the abundance of large blood vessels and nerves in the upper mediastinal, particularly the surrounding of the recurrent laryngeal nerve, which greatly increase the technical difficulty of surgery and may lead to the omission of LNs during lymphadenectomy. Second, in our study, the majority of patients underwent extended radical esophagectomy with two-field lymphadenectomy and the difficulty to remove subclinical lesions in the recurrent laryngeal nerve, which lead to the high recurrence of the supraclavicular site. Our data showed that the recurrence rates of anastomosis and primary tumor bed were too low and do not have the necessity to receive PORT (9.8% and 3.6%, respectively). In addition, the addition of PORT may lead to anastomotic stricture, which will seriously affect the patients’ quality of life in the future. However, some studies23 in the literature revealed that anastomosis relapse rates are as high as 29% of treatment failure with small volume. Therefore, the anastomosis included in the CTV of postoperative radiation therapy is of necessity.23 Whether the anastomosis and primary tumor bed require to be irradiated should be further evaluated via prospective clinical research.
Limitations
There are several potential limitations in this study. First, the study we presented was a retrospective study with potential bias. Second, recurrent LNs in our findings are mainly based on an interpretation of CT or positron emission tomography/CT imaging and not on pathology assessments. Therefore, we cannot prove that all the identified enlarged LNs contain metastatic disease. Third, with respect to the PORT target volume, our conclusion was obtained on the basis of the initial regional relapse of patients without observing the entire period of natural death. In addition, ~26.6% of patients in this study received adjuvant chemotherapy. Our results indicated that adjuvant chemotherapy after radical resection did not affect nodal relapse. However, whether adjuvant chemotherapy would affect tumor control still needs further study.
Conclusion
Locoregional recurrence was the most common and potentially preventable type of initial treatment failure after curative surgery among patients with midthoracic ESCC. For midthoracic ESCC with histological node-negative, or one or two positive nodes, the supraclavicular and stations 2, 4, 5, and 7 LNs should be delineated as CTV of postoperative prophylactic irradiation, and upper abdominal LNs should be excluded. While for midthoracic ESCC with three or more positive nodes, the supraclavicular, stations 2, 4, 5, and 7, and upper abdominal LNs should be delineated as CTV of postoperative prophylactic irradiation. For upper abdominal LNs, the LNs in the left gastric artery, common hepatic artery, celiac artery, and retropancreatic and para-aortic regions are high-risk areas for locoregional metastasis, which should be included in the target volume of the adjuvant radiotherapy following surgery. Tumor bed and anastomotic are not recommended to be incorporated into the target volume. The length of tumor and histological differentiation influence the pattern of LN metastases in midthoracic ESCC, which should be considered comprehensively to design the CTV for radiotherapy. Prospective studies with large sample size are needed to further evaluate the optimal target volume of postoperative prophylactic irradiation for midthoracic ESCC.
Disclosure
The authors report no conflicts of interest in this work.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. | ||
Kumagai K, Rouvelas I, Tsai JA, et al. Meta-analysis of postoperative morbidity and perioperative mortality in patients receiving neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal and gastro-oesophageal junctional cancers. Br J Surg. 2014;101(4):321–338. | ||
Kurashige J, Kamohara H, Watanabe M, et al. Serum microRNA-21 is a novel biomarker in patients with esophageal squamous cell carcinoma. J Surg Oncol. 2012;106(2):188–192. | ||
Mirinezhad SK, Somi MH, Seyednezhad F, et al. Survival in patients treated with definitive chemo-radiotherapy for non-metastatic esophageal cancer in north-west Iran. Asian Pac J Cancer Prev. 2013;14(3):1677–1680. | ||
Lv J, Cao XF, Zhu B, Ji L, Tao L, Wang DD. Long-term efficacy of perioperative chemoradiotherapy on esophageal squamous cell carcinoma. World J Gastroenterol. 2010;16(13):1649–1654. | ||
Nakagawa S, Kanda T, Kosugi S, Ohashi M, Suzuki T, Hatakeyama K. Recurrence pattern of squamous cell carcinoma of the thoracic esophagus after extended radical esophagectomy with three-field lymphadenectomy. J Am Coll Surg. 2004;198(2):205–211. | ||
Chen G, Wang Z, Liu XY, Liu FY. Recurrence pattern of squamous cell carcinoma in the middle thoracic esophagus after modified Ivor-Lewis esophagectomy. World J Surg. 2007;31(5):1107–1114. | ||
Xiao ZF, Yang ZY, Miao YJ, et al. Influence of number of metastatic lymph nodes on survival of curative resected thoracic esophageal cancer patients and value of radiotherapy: report of 549 cases. Int J Radiat Oncol Biol Phys. 2005;62(1):82–90. | ||
Chen J, Pan J, Zheng X, et al. Number and location of positive nodes, postoperative radiotherapy, and survival after esophagectomy with three-field lymph node dissection for thoracic esophageal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2012;82(1):475–482. | ||
Xu Y, Liu J, Du X, et al. Prognostic impact of postoperative radiation in patients undergoing radical esophagectomy for pathologic lymph node positive esophageal cancer. Radiat Oncol. 2013;8:116. | ||
Schreiber D, Rineer J, Vongtama D, et al. Impact of postoperative radiation after esophagectomy for esophageal cancer. J Thorac Oncol. 2010;5(2):244–250. | ||
Zhang WC, Wang QF, Xiao ZF, et al. The guiding effect of failure mode of thoracic esophageal squamous cell carcinoma after radical operation on the field of radiotherapy. Chin J Radiat Oncol. 2012;21(1):38–41. | ||
Chapet O, Kong FM, Quint LE, et al. CT-based definition of thoracic lymph node stations: an atlas from the University of Michigan. Int J Radiat Oncol Biol Phys. 2005;63(1):170–178. | ||
Xiao ZF, Yang ZY, Liang J, et al. Value of radiotherapy after radical surgery for esophageal carcinoma: a report of 495 patients. Ann Thorac Surg. 2003;75(2):331–336. | ||
Worni M, Martin J, Gloor B, et al. Does surgery improve outcomes for esophageal squamous cell carcinoma? An analysis using the surveillance epidemiology and end results registry from 1998 to 2008. J Am Coll Surg. 2012;215(5):643–651. | ||
Chen J, Zhu J, Pan J, et al. Postoperative radiotherapy improved survival of poor prognostic squamous cell carcinoma esophagus. Ann Thorac Surg. 2010;90(2):435–442. | ||
Guo ZM, Liu WW, He JH. A retrospective cohort study of nasopharyngeal adenocarcinoma: a rare histological type of nasopharyngeal cancer. Clin Otolaryngol. 2009;34(4):322–327. | ||
Li CL, Zhang FL, Wang YD, et al. Characteristics of recurrence after radical esophagectomy with two-field lymph node dissection for thoracic esophageal cancer. Oncol Lett. 2013;5(1):355–359. | ||
Cai WJ, Xin PL. Pattern of relapse in surgical treated patients with thoracic esophageal squamous cell carcinoma and its possible impact on target delineation for postoperative radiotherapy. Radiother Oncol. 2010;96(1):104–107. | ||
Lu JC, Tao H, Zhang YQ, et al. Extent of prophylactic postoperative radiotherapy after radical surgery of thoracic esophageal squamous cell carcinoma. Dis Esophagus. 2008;21(6):502–507. | ||
Wu SG, Dai MM, He ZY, et al. Patterns of regional lymph node recurrence after radical surgery for thoracic esophageal squamous cell carcinoma. Ann Thorac Surg. 2015;101(2):551–557. | ||
Huang W, Li BS, Gong HY, et al. Pattern of lymph node metastases and its implication in radiotherapeutic clinical target volume in patients with thoracic esophageal squamous cell carcinoma: a report of 1077 cases. Radiother Oncol. 2010;95(2):229–233. | ||
Yu E, Dar R, Rodrigues GB, et al. Is extended volume external beam radiation therapy covering the anastomotic site beneficial in post-esophagectomy high risk patients. Radiother Oncol. 2004;73(2):141–148. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.