")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Recombinant Neorudin for the Prevention of Deep-Vein Thrombosis After Spinal-Cord Injury
Authors Liu YB , Liu Y, Zhang L, Zhou XC, Ren BY, Zheng C, Hao CH, Wang WT, Xia X, Zhou GQ, Wu CT, Jin JD
Received 10 February 2023
Accepted for publication 28 July 2023
Published 23 August 2023 Volume 2023:17 Pages 2523—2535
DOI https://doi.org/10.2147/DDDT.S408078
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Yu-Bin Liu,1,2 Yun Liu,1,3 Lin Zhang,1 Xing-Chen Zhou,1 Bo-Yuan Ren,1 Can Zheng,1 Chun-Hua Hao,4 Wei-Ting Wang,4 Xia Xia,5 Gang-Qiao Zhou,1,3 Chu-Tse Wu,1 Ji-De Jin1
1Department of Experimental Hematology and Biochemistry, Beijing Institute of Radiation Medicine, Beijing, People’s Republic of China; 2Division of (Bio) Pharmaceutics, Institute of Zhejiang University - Quzhou, Zhejiang, People’s Republic of China; 3School of Medicine, Guizhou University, Guiyang, People’s Republic of China; 4Center for Pharmacodynamic Research, Tianjin Institute of Pharmaceutical Research, Tianjin, People’s Republic of China; 5Beijing SH Biotechnology Co., Ltd., Beijing, People’s Republic of China
Correspondence: Chu-Tse Wu; Ji-de Jin, Email [email protected]; [email protected]
Background: Whether anticoagulant therapy should be used after spinal-cord injury (SCI) surgery was controversial. The anticoagulation characteristics of a newly developed anticoagulant, recombinant neorudin (EPR-hirudin (EH)), were explored using a rat model of SCI to provide a basis for clinical anticoagulation therapy of SCI.
Methods: A rat model of SCI was developed by Allen’s method. Then, thrombosis in the inferior vena cava was induced by ligation. The low-bleeding characteristics of EH were explored by investigating dose–response and time–effect relationships, as well as multiple administration of EH, on thrombus formation complicated with SCI.
Results: EH inhibited thrombosis in a dose-dependent manner by reducing the wet weight and dry weight of the thrombus. An inhibiting action of EH on thrombosis was most evident in the group given EH 2 h after SCI. After multiple intravenous doses of EH, thrombosis inhibition was improved to that observed with low molecular weight heparin (LMWH) (87% vs 90%). EH administration after SCI neither increased bleeding in the injured spine nor damaged to nerve function. Bleeding duration and activated partial thromboplastin time were increased in the high-dose EH group compared with that in the normal-saline group, but were lower than those in the LMWH group.
Conclusion: EH can reduce thrombus formation in a rat model of SCI, and bleeding is decreased significantly compared with that using LMWH. EH may prevent thrombosis after SCI or spinal surgery.
Keywords: recombinant neorudin, rat model, thrombosis, spinal-cord injury, low-bleeding anticoagulation
Introduction
Deep-vein thrombosis (DVT) is a common early complication after spinal-cord injury (SCI) and spinal surgery, but it can also occur in the chronic period.1 DVT causes long-term swelling and ulcers in the lower limbs, and affects the rehabilitation and prognosis of patients. DVT can even lead to a fatal pulmonary embolism,2 the third most common cause of death in patients with SCI, whose worldwide prevalence is estimated to be ≤5%.3 In recent years, the prevalence of DVT after SCI has been increasing.4–6 The overall prevalence of symptomatic or asymptomatic DVT in untreated SCI patients ranges from 50% to 100%, which is highest within the first 2 weeks following injury.7–11
Full attention should be paid to the evaluation and prevention of DVT after SCI because efficacious treatment is lacking and the early clinical symptoms of DVT are not obvious. Whether anticoagulant therapy should be used in surgery for SCI was controversial, and different clinical opinions have been documented. Anticoagulant therapy may reduce the risk of DVT, but may increase the risk of epidural hematomas.12 Application of anticoagulants before surgery, in general, can lead to bleeding, which interferes with anticoagulant therapy for patients with SCI. In particular, some scholars believe that intraoperative use of anticoagulants can lead to increased bleeding from wounds, formation of epidural hematomas, and other complications.13
However, many scholars believe that patients with SCI should receive anticoagulants as soon as possible after SCI. Clinical studies have indicated that rational use of anticoagulants, such as low-molecular-weight heparin (LMWH), could reduce the occurrence of thrombosis without increasing the risk of bleeding.3,14–19
Recombinant neorudin (EPR-hirudin (EH))20 is a newly developed anticoagulant. It is obtained by adding EPR short peptide (which is composed of three amino acids, Glu–Pro–Arg) to the N-terminal of hirudin (the most potent natural inhibitor of thrombin). Hirudin has been approved by the US Food and Drug Administration for the prevention of thrombosis after major orthopedic surgery. However, its clinical application has been limited because it causes bleeding.21 The anticoagulant effect of EH is blocked totally by EPR, which can be identified and cleaved by coagulation factor Xa (FXa) and/or coagulation factor XIa (FXIa).22 The anticoagulant action of hirudin is released from EH after hydrolysis by FXa or FXIa at the thrombus site.23 Thus, EH exerts its antithrombotic effects by releasing its active metabolite (hirudin) at the thrombus site via FXIa-mediated cleavage of EPR, thereby resulting in direct inhibition of thrombin. Through its structure and mechanism of action, EH can be targeted to the local thrombus, thereby reducing systemic bleeding. The low-bleeding characteristics of EH have been demonstrated using a beagle model of coronary artery thrombosis,24 as well as a rat model of thrombosis due to cerebral infarction25 and thrombosis of the posterior vena cava (PVC). Furthermore, the safety and low-bleeding characteristics of EH have been shown in healthy volunteers.26
In the present study, the effects of EH on thrombus inhibition and safety were evaluated in a rat model of SCI complicated with venous thrombosis. We aimed to provide clues for thrombus prophylaxis in patients with SCI or who have undergone spinal surgery.
Materials and Methods
Ethical Approval of the Study Protocol
The experimental protocol was approved (2020021601) by the Animal Ethics Committee of Tianjin Institute of Pharmaceutical Research (Tianjin, China) and complied with the Guide for the Care and Use of Laboratory Animals published by the Chinese Ministry of Public Health. Experiments were carried out in accordance with relevant regulations and guidelines, including Animals in Research: Reporting In Vivo Experiments (ARRIVE) guidelines. Rats were killed humanely by cervical vertebrae luxation, according to ARRIVE guidelines.
Materials
EH (lot: 20190428) was obtained from Beijing Institute of Radiation Medicine (Beijing, China). LMWH-sodium injection (Fluxum™; AlphaSigma, Covington, LA, USA) was purchased from 307th Hospital (Beijing, China). The reagents used to determine the thrombin time (TT) (lot: 031912A), prothrombin time (PT) (lot: 011910A), activated partial thromboplastin time (APTT) (lot: 022001A), and fibrinogen (lot: 042003A) were sourced from Mede Pacific (Tianjin) Biotechnology (Tianjin, China). A plasma free hemoglobin (fHb) determination kit (lot: 20200612) was obtained from Nanjing Jiancheng Bioengineering Institute (Nanjing, China).
A Parber Coagulation Factor Analyzer was purchased from Beijing Shidi Scientific Instruments (Beijing, China). A microplate reader (RT6100 series) was obtained from Rayto Life Sciences (Shenzhen, China). An ultrasonic cell shredder (SCIENTZ-IID) was sourced from Xinzhi Biological Technology (Zhejiang, China). A 3.0-T magnetic resonance scanner (Discovery MR750) was obtained from General Electric (Boston, MA, USA).
Animals
Male Sprague–Dawley rats (license number: SCXK (Beijing) 2019–0010) purchased from Spef (Beijing Biological) Technology (Beijing, China) were bred under standard conditions of care (12-h day–night cycle, 40–70% humidity, 22–26°C) and had free access to water and chow.
Animal Model of SCI Combined with DVT
Male Sprague–Dawley rats (260 g) were anesthetized with isoflurane and fixed in the ventral-decubitus position. Fur around the tenth thoracic vertebra (T10) was shaved and routine disinfection undertaken. The spinous processes of T9–T11 were exposed by surgical incision. Then, the spinous process of T10 was resected, and half of the back of the T10 vertebral body was cleaned to expose the spinal cord. SCI was developed using Allen’s method.27 Briefly, the T10 thoracic spinal cord was impacted with a 10-g rod by a free fall from a height of 5 cm. At the moment of injury, a spastic swing of the rat tail, as well as retraction and flutter of both hind limbs and trunk, demonstrated that the SCI model had been developed.
To initiate DVT, rats were first anesthetized with 3% pentobarbital sodium (60 mg/kg) and then fixed supine on an operating table. The abdominal cavity was opened along the midline to expose the inferior vena cava (IVC). PVC branches (third lumbar veins, left iliac lumbar veins, fourth lumbar veins, right internal spermatic vein, right iliac vena cava) were ligated successively. Then, the PVC was ligated below the branch of the renal vein to induce venous thrombosis by venous stagnation. The duration of thrombosis was 1 h.
Dose–Response Relationship
Sixty rats were divided randomly into six groups of 10. They underwent surgery to induce SCI and DVT (except rats in the sham-operation group). Rats in the sham-operation group and model control group were injected with physiological (0.9%) saline (“normal saline” (NS)) in the tail vein. Rats in treatment groups were injected with EH (0.3, 1.0, 3.0 mg/kg) in the tail vein, respectively. Rats in the positive control group were injected (s.c.) with LMWH (440 IU AXa/kg bodyweight; clinically equivalent dose). Drugs were administered 2 h after SCI, and the DVT model was created 5-min later for 1 h. Thereafter, the dose–effect relationship was evaluated (Figure 1A).
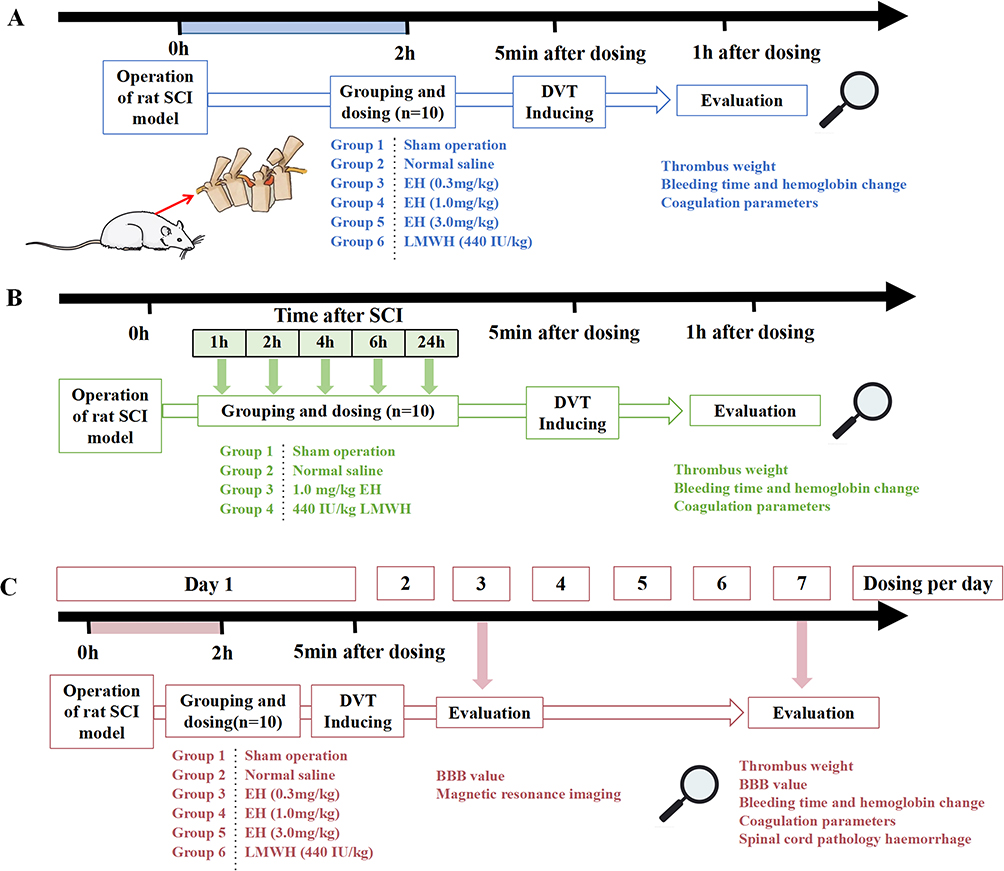 |
Figure 1 Time-line of EH for the prevention of deep-vein thrombosis after spinal-cord injury. (A) Dose–response relationship. (B) Time–effect relationship. (C) Effect of multiple administration of EH. |
Time–Effect Relationship of a Drug
This experiment was divided into five time points (1, 2, 4, 6, 24 h) after SCI modeling, and each time point was divided into five groups, which yielded a total of 20 groups with 10 rats in each (A total of 200 rats). Rats underwent surgery to induce SCI and DVT (except rats in the sham operation group). Rats in the sham-operation group and model control group were injected (i.v.) with NS. Rats in treatment groups were injected (i.v.) with EH (1.0 mg/kg). Rats in the positive control group were injected (s.c.) with LMWH (440 IU AXa/kg bodyweight).
Drugs were administered 1, 2, 4, 6, and 24 h after SCI, respectively. A thrombosis in the IVC was created 5-min later for 1 h. Thereafter, the time–effect relationship was evaluated (Figure 1B).
Effect of Multiple Administration of EH
Sixty rats were divided randomly into six groups of 10. Rats in each group underwent surgery to induce SCI and DVT (except for rats in the sham-operation group). The induction of DVT was identical to that described above except that a polyethylene tube was placed under the silk thread used to ligate the PVC and was removed carefully after DVT had been induced for 1 h to recover part of the blood flow, and then muscle and skin were sutured.
Rats in the sham-operation group and model control group were injected (i.v.) with NS. Rats intreatment groups were injected (i.v.) with EH (0.3, 1.0, 3.0 mg/kg). Ras in the positive control group were injected (s.c.) with LMWH (440 IU AXa/kg bodyweight). Two hours after SCI, drugs were administered, and then a thrombosis in the IVC was created 5-min later for 1 h. Thereafter, the drug was administered once a day for 7 days, and the effect of multiple administration of EH was evaluated. The experimental design and time-line were shown in Figure 1C.
Determination of the Wet Weight and Dry Weight of Thrombus
The IVC was clipped 2-cm below the ligation after DVT induction for 1 h, and then dissected to remove the thrombus. The wet weight of the thrombus was measured after drainage of residual fluid, and then dried in a 50°C oven. Thereafter, the dry weight of the thrombus was measured and percent inhibition of thrombus formation calculated according to the following formula:

Determination of Bleeding Duration in the Peripheral Circulation
One hour after IVC ligation, the tail of a rat was cut 2-mm away from the tail tip and placed in 10 mL of NS. Then, the bleeding duration was documented.
Determination of Blood Volume in the Injured SC
One hour after IVC ligation, the SC at T9–T11 was removed and made into a 10% homogenate with NS. The volume of blood in the SC was measured using the fHb determination kit, according to manufacturer’s instructions.
Determination of Parameters of Plasma Coagulation
After removal of the thrombus, blood was drawn from the abdominal aorta into tubes with 3.8% sodium citrate (ratio of whole blood: anticoagulant = 9:1). The tube was centrifuged at 1240 g for 10 min at 4°C to collect plasma for determination of TT, PT, APTT, and fibrinogen level by the solidification method, as described previously.24,25
Basso–Beattie–Bresnahan Locomotor Rating Scale (BBBLRS)
Deficits in rat behavior were scored according to the BBBLRS score28 3 and 7 days after treatment in the multiple-administration study. The BBBLRS score is composed of three parts: the score in the first part ranges from 0 to 7 and evaluates the activity of each joint of hind limbs; the second ranges from 8 to 13 and evaluates the gait and coordination function of hind limbs; the third ranges from 14 to 21 and evaluates fine movement of paws during movement. The total score of the three parts is 21.
Detection of SC Pathology by Magnetic Resonance Imaging (MRI)
Three days after treatment in the multiple-administration study, imaging data of the T9–T11 segments of the SC were collected using a 3.0-T magnetic resonance scanner and phased array coil for animal studies. Sagittal and transverse spin–spin relaxation time T2-weighted images (T2WIs) were obtained.
The scanning parameters for sagittal spin and spin relaxation time T2WIs were repetition time (TR)/echo time (TE) = 3338/74 ms; field of view (FoV) = 80 mm × 80 mm; matrix = 256 × 256; number of excitations (NEX) = 3; layer thickness = 1 mm; interval = 0.5 mm.
The scanning parameters for transverse spin and spin relaxation time T2WIs were TR/TE = 2967/83 ms; FoV = 60 mm × 60 mm; matrix = 256 × 256; NEX = 3; layer thickness = 1 mm; interval = 0.5 mm.
The criterion for the diagnosis of lesions was a high signal area on a visually distinguishable T2WI. The percentage of total lesion volume in the SC was determined using Dcm2niigui and Mricron 12122012.
Determination of Hemorrhage in the Injured SC
Seven days after treatment in the multiple-administration study, T9–T11 SC segments of rats were removed, fixed in 10% formaldehyde, and embedded in paraffin along the coronal surface. 5 sections were cut at 1-mm intervals for each tissue at a thickness of 5 μm, and conventional hematoxylin and eosin (H&E) staining was undertaken. Each section was photographed with a microscope at ×400 magnification. The number of red blood cells (RBCs) in the lesion area was counted.
Data Collection and Statistical Analyses
Data are the mean ± standard deviation. Significant differences between groups were analyzed by ANOVA. P < 0.05 was considered significant.
Results
Dose–Response Relationship
Effects on the Wet Weight and Dry Weight of the Thrombus
A thrombus was formed in the ligated blood vessels of rats in the NS group. After intravenous administration of EH (0.3, 1.0, 3.0 mg/kg), the wet weight and dry weight of thrombus were reduced significantly in a dose-dependent manner. Compared with the NS group, the wet weight was reduced by 28.0% (P < 0.05), 57.3% (P < 0.01), and 59.2% (P < 0.001), and the dry weight was reduced by 28.5% (P < 0.05), 57.5% (P < 0.001), and 60.7% (P < 0.001), respectively, after EH had been given at 0.3, 1.0, or 3.0 mg/kg. The wet weight and dry weight of the thrombus of rats treated with LMWH were reduced significantly by 83.8% (P < 0.001) and 83.5% (P < 0.001), respectively, compared with that in rats in the NS group. Percent thrombus inhibition after EH (0.3, 1.0 mg/kg) had been administered was lower than that after LMWH had been given (Figure 2A).
 |
Figure 2 Dose–effect relationship between EH and thrombosis (n=10). (A) Effects on the wet and dry weight of the thrombus. (B) Effects on bleeding in the spinal cord. (C) Effects on bleeding duration after tail amputation. (D) Effects on coagulation parameters. ΔΔΔP < 0.001, compared with the sham-operation group; *P < 0.05, **P < 0.01, ***P < 0.001, compared with the normal-saline group; #P < 0.05, ###P < 0.001, compared with the LMWH group. |
Effects on the Blood Volume in the Injured SC
Dark-red blood oozed rapidly on the SC surface at the impact site. The volume of blood in the NS group was significantly higher than that in the sham-operation group (P < 0.001) according to the fHb level in the injured SC. There was no significant effect upon bleeding in the SC in rats after intravenous administration of EH (0.3, 1.0, 3.0 mg/kg). Blood loss in the LMWH group showed an increasing trend, but not significantly so (Figure 2B).
Effects on Bleeding Duration After Tail Amputation
Intravenous administration of EH (0.3, 1.0, 3.0 mg/kg) in rats had no significant effect on bleeding duration after tail amputation (Figure 2C). However, bleeding duration was prolonged significantly after LMWH administration compared with that in the NS group (P < 0.01) and in groups administered EH (0.3, 1.0 mg/kg) (P < 0.05).
Effects on Coagulation Parameters
Intravenous administration of EH (3.0 mg/kg) prolonged TT significantly (P < 0.05), and LMWH administration prolonged TT (P < 0.01) and APTT (P < 0.001) significantly, compared with those in the NS group (Figure 2D).
Time–Effect Relationship
Effects on the Wet Weight and Dry Weight of the Thrombus
After administration of EH (1 mg/kg) and LMWH at each time point after SCI, the wet weight and dry weight of the thrombus were reduced significantly compared with those in the NS group (P < 0.01–0.001) (Figure 3A). There was no significant difference in thrombus inhibition between 1 h and 6 h, but there was an increasing trend in the wet weight and dry weight of the thrombus from 2 h to 6 h. These results implied that thrombosis was closely related to the time of damage and anticoagulation therapy; earlier treatment with EH may reduce the thrombus size. The thrombus-inhibition effect of LMWH given 2 h and 4 h after SCI was greater than that of EH (P < 0.05).
 |
Figure 3 Time–effect relationship between EH and thrombosis (n=10). (A) Effects on the wet and dry weight of the thrombus. (B) Effects on bleeding in the spinal cord. (C) Effects on bleeding duration after tail amputation. ΔΔΔP < 0.001, compared with the sham-operation group; *P < 0.05, **P < 0.01, ***P < 0.001, compared with the normal-saline group; #P < 0.05, ##P < 0.01, compared with the LMWH group. |
Effects on Blood Volume in the SC
Blood volume (expressed by the fHb level in the injured SC) was increased significantly at each time point after SCI in the NS group compared with that in the sham-operation group (P < 0.001). However, there was no significant increase in the blood volume in the group given EH (1 mg/kg) or the group given LMWH, though the extent of bleeding in the LMWH group showed an increasing trend (Figure 3B).
Effects on Bleeding Duration After Tail Amputation
The duration of bleeding after tail amputation was not influenced if rats were given EH (1 mg/kg) 1, 2, 4, 6, or 24 h after SCI. However, the duration of bleeding was prolonged significantly after LMWH administration at all time points compared with that in the NS group (P < 0.05–0.01) at 2 h and 4 h compared with rats treated with EH (P < 0.05) (Figure 3C).
Effect of Multiple Administration of EH
Effects on the Wet Weight and Dry Weight of the Thrombus
After drugs had been administered for 7 days, the thrombus was removed for examination. The wet weight and dry weight of the thrombus were reduced significantly in groups administered EH (0.3, 1.0, 3.0 mg/kg) on multiple occasions. Compared with the NS group, the wet weight was reduced by 87.8% (P > 0.05), 88.3% (P < 0.05), and 89.7% (P < 0.05), and the dry weight was reduced by 87.1% (P < 0.001), 86.6% (P < 0.001), and 87.0% (P < 0.001), respectively, for EH given at 0.3, 1.0, and 3.0 mg/kg. The wet weight and dry weight of the thrombus were reduced by 95.3% (P < 0.05) and 90.2% (P < 0.001), respectively, in the group given LMWH compared with the group given NS (Figure 4A).
 |
Figure 4 Effect of multiple administration of EH on thrombus formation (n=10). (A) Effects on the wet weight and dry weight of the thrombus. (B) Effects on bleeding duration after tail amputation. (C) Effects on coagulation parameters. *P < 0.05, ***P < 0.001, compared with the normal-saline group; #P<0.05, compared with LMWH group. |
Effects on Bleeding Duration After Tail Amputation
Intravenous administration of EH (0.3, 1, 3 mg/kg) for 7 days did not increase bleeding duration (Figure 4B). However, bleeding duration was prolonged significantly in rats treated with LMWH (P < 0.05) compared with rats given NS.
Effects on Coagulation Parameters
Intravenous administration of EH (3 mg/kg) for 7 days prolonged TT significantly (P < 0.05) and LMWH administration prolonged TT and APTT significantly (P < 0.001) compared with the group given NS (Figure 4C).
Effects on the BBBLRS Score
The BBBLRS score of the NS group was reduced significantly 3 days and 7 days after SCI (P < 0.001) compared with the sham-operation group (Figure 5A). These results showed that SC damage was induced and the movement of rats was influenced after SCI. The BBBLRS score was not significantly affected in groups given EH (0.3, 1.0, 3.0 mg/kg) multiple times, or the group given LMWH.
 |
Figure 5 Effect of multiple administration of EH on the spinal cord (n=10). (A) The BBBLRS score showed that the movement of rats after SCI was limited in the normal-saline group compared with that in the sham-operation group (P < 0.001) and there was no significant effects on the BBBLRS score upon treatment with EH or LMWH. (B) The RBC count in the lesion area of the spinal cord revealed obvious bleeding after SCI, and treatment with EH or LMWH did not increase bleeding in the lesion area. (C) The range of spinal lesions (%) analyzed by Dcm2niigui and Mricron with MRI showed spinal lesions to be induced and that these lesions were not significantly affected by treatment with EH or LMWH. (D) Pathologic sections dyed with H&E. (Di) Normal tissue structure of the spinal cord. (Dii) Intact tissue structure of the spinal cord was destroyed after SCI, and some cells experienced apoptosis or necrosis, thereby resulting in infiltration of immune cells (blue arrow), and many RBCs (red arrow) appeared in the lesion area. (Diii) EH (0.3 mg/kg). (Div) EH (1.0 mg/kg). (Dv) EH (3.0 mg/kg). (Dvi) LMWH (440 IU AXa/kg bodyweight). After treatment with three doses of EH or LMWH, lesions in the spinal cord were not altered obviously. ΔΔΔP < 0.001, compared with the sham-operation group. |
Effects on Lesions and Bleeding in the Injured SC
The normal and intact tissue structure of SC is displayed in Figure 5Di: there were virtually no RBCs among SC cells. The intact tissue structure of the SC was destroyed after SCI, and some cells experienced apoptosis or necrosis, which resulted in the infiltration of immune cells (Figure 5Dii). Moreover, many RBCs were in the lesion area of the SC. There was no significant difference in the number of SC lesions among treatment groups (Figure 5Dii–Dvi).
The number of RBCs in the injured area of the SC in the NS group was increased significantly compared with that in the sham-operation group (P < 0.001), which demonstrated significant bleeding after SCI. The RBC number did not increase in groups treated with EH (0.3, 1.0, 3.0 mg/kg) for 7 days, or in the group treated with LMWH (though an increasing tendency in the LMWH group was observed) (Figure 5B).
Lesion Analysis in the SC by MRI
Significant spinal lesions were observed by MRI of rats in the NS group 7 days after SCI compared with those in the sham-operation group (P < 0.001). There was no significant difference in the number of SC lesions in rats treated with EH (0.3, 1.0, 3.0 mg/kg) for 7 days, or those treated with LMWH, compared with rats treated with NS (Figure 5C).
Discussion
SCI is associated with an increased risk of venous thromboembolism due to Virchow’s triad (stasis, hypercoagulable state and intimal injury)29 because patients undergo an invasive surgical procedure and can suffer extensive damage to tissue. However, there are greater concerns about hemorrhage or bleeding (especially around nerve tissue) because a minor hematoma in spinal cord can lead to devastating consequences (eg, paralysis).12 Hence, implementation of appropriate anticoagulation strategies to reduce the risk of DVT and pulmonary embolism without increasing the risk of hemorrhagic complications is a major task.30 Although American College Chest Physicians Evidence-Based Clinical Practice (9th ed) recommends prevention of venous thromboembolism (VTE) in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis.31 However, the similar guideline of the application of anticoagulants such as LMWH to prevent DVT in SCI patients has not been formulated so far.
We investigated the role of the EH in preventing DVT after SCI. EH reduced IVC thrombosis in a dose-dependent manner without an increase in the risk of hemorrhage in the injured SC.
Consensus regarding the time to start thromboprophylaxis using anticoagulants after injury or surgery is lacking. Several authors have suggested that the “ideal” time to start chemoprophylaxis is immediately/very short time after injury.7,32 Furthermore, few reports have focused on the effect of duration of anticoagulant use after SCI.33,34 Some studies35 have indicated that the risk for DVT is greatest during the first 2 weeks after SCI. Arnold et al30 reported that thrombus prophylaxis with anticoagulants and mechanical means initiated within 72 h of SCI resulted in lower risk of DVT than after 72 h. Aito et al36 found the risk of DVT to be 13-times greater if prophylaxis (anticoagulant with mechanical procedures) was employed 72 h after injury compared with that within 72 h. Hence, administration of LMWH within 72 h of SCI is recommended to minimize the DVT risk.6 Furthermore, in a recent propensity score-matched analysis, the optimal time of initiation of thromboprophylaxis was investigated in 3554 patients with acute SCI. They were divided equally into two groups of early (<48 h after surgery) versus late (≥48 h after surgery) initiation of thromboprophylaxis: DVT prevalence was significantly lower in the early group than in the late group (2.1% vs 10.8%, respectively, P < 0.01).37,38
In our time effect study, there was an increasing trend of wet weight and dry weight of the thrombus from 2 h to 6 h after SCI, though there was no significant difference in the thrombus-inhibition effect between 1 h and 6 h. This result implied that thrombosis was closely related to the time of damage and anticoagulation therapy and that earlier treatment may help to reduce the thrombus size. Therefore, given the combined results of thromboprophylaxis and bleeding in the SC, EH could be administered <6 h in clinic after SCI to prevent thrombosis, which is earlier than LMWH.
In terms of the dose response relationship, different from our previous studies,24,25 the percent of thrombus inhibition using high-dose EH was lower than that using LMWH (60.7% vs 87.5%), though the bleeding risk of EH was lower than that of LMWH. This disparity in results may arise from different thrombus models and different times of intervention. However, after multiple administration of EH for 7 days, the thrombus-inhibiting effect of EH was similar to that of LMWH (87.2% vs 90.2%) without an increase in bleeding or lesions in the injured SC, or damage to nerve function. EH, as a new anticoagulant with low bleeding, can effectively inhibit thrombosis without increasing the risk of bleeding after SCI, so it has a good clinical application prospect and multiple administration of EH is recommended to inhibit thrombosis in patients with SCI.
Conclusions
EH inhibited thrombosis after SCI in a dose-dependent manner. Application of EH did not increase bleeding in the injured SC or damage nerve function. Therefore, it would be beneficial to apply EH to reduce thrombosis after SCI or SC surgery. We suggest initiation of EH therapy <6 h after SCI. EH may provide a safe and effective anticoagulant drug choice for patients with SCI. The results of this study are promising but require further research before EH is accepted to perform clinical trials in SCI patients.
Acknowledgments
This study was supported in part by a grant from the Beijing Science and Technology Plan (No. Z181100002218004).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mackiewicz-Milewska M, Jung S, Kroszczyński AC, et al. Deep venous thrombosis in patients with chronic spinal cord injury. J Spinal Cord Med. 2016;39(4):400–404. doi:10.1179/2045772315y.0000000032
2. Dahl OE, Caprini JA, Colwell CW
3. Teasell RW, Hsieh JT, Aubut JA, et al. Venous thromboembolism after spinal cord injury. Arch Phys Med Rehabil. 2009;90(2):232–245. doi:10.1016/j.apmr.2008.09.557
4. Rojas-Tomba F, Gormaz-Talavera I, Menéndez-Quintanilla IE, et al. [Incidence and risk factors of venous thromboembolism in major spinal surgery with no chemical or mechanical prophylaxis]. Rev Esp Cir Ortop Traumatol. 2016;60(2):133–140. Spanish. doi:10.1016/j.recot.2015.10.002
5. Smith MD, Bressler EL, Lonstein JE, et al. Deep venous thrombosis and pulmonary embolism after major reconstructive operations on the spine. A prospective analysis of three hundred and seventeen patients. J Bone Joint Surg Am. 1994;76(7):980–985. doi:10.2106/00004623-199407000-00004
6. Brohi K, Cohen MJ, Ganter MT, et al. Acute coagulopathy of trauma: hypoperfusion induces systemic anticoagulation and hyperfibrinolysis. J Trauma. 2008;64(5):1211–7; discussion 1217. doi:10.1097/TA.0b013e318169cd3c
7. Christie S, Thibault-Halman G, Casha S. Acute pharmacological DVT prophylaxis after spinal cord injury. J Neurotrauma. 2011;28(8):1509–1514. doi:10.1089/neu.2009.1155-A
8. Chen HL, Wang XD. Heparin for venous thromboembolism prophylaxis in patients with acute spinal cord injury: a systematic review and meta-analysis. Spinal Cord. 2013;51(8):596–602. doi:10.1038/sc.2013.48
9. Zhang HR, Xu MY, Yang XG, et al. Nomogram for predicting the postoperative venous thromboembolism in spinal metastasis tumor: a multicenter retrospective study. Front Oncol. 2021;11(629823). doi:10.3389/fonc.2021.629823
10. Dibiasi C, Gratz J, Wiegele M, et al. Anti-factor Xa activity is not associated with venous thromboembolism in critically Ill patients receiving enoxaparin for thromboprophylaxis: a retrospective observational study. Front Med. 2022;9(888451). doi:10.3389/fmed.2022.888451
11. Chung SB, Lee SH, Kim ES, et al. Incidence of deep vein thrombosis after spinal cord injury: a prospective study in 37 consecutive patients with traumatic or nontraumatic spinal cord injury treated by mechanical prophylaxis. J Trauma. 2011;71(4):867–70; discussion 870–1. doi:10.1097/TA.0b013e31822dd3be
12. Nanclares BVC, Padilla-Zambrano HS, El-Menyar A, et al. WACEM consensus paper on deep venous thrombosis after traumatic spinal cord injury. J Emerg Trauma Shock. 2019;12(2):150–154. doi:10.4103/jets.Jets_125_18
13. Bernsen RA, Hoogenraad TU. A spinal haematoma occurring in the subarachnoid as well as in the subdural space in a patient treated with anticoagulants. Clin Neurol Neurosurg. 1992;94(1):35–37. doi:10.1016/0303-8467(92)90116-k
14. Piran S, Schulman S. Incidence and risk factors for venous thromboembolism in patients with acute spinal cord injury: a retrospective study. Thromb Res. 2016;147:97–101. doi:10.1016/j.thromres.2016.09.030
15. Marciniak CM, Kaplan J, Welty L, et al. Enoxaparin versus tinzaparin for venous thromboembolic prophylaxis during rehabilitation after acute spinal cord injury: a retrospective cohort study comparing safety and efficacy. PMR. 2012;4(1):11–17. doi:10.1016/j.pmrj.2011.10.007
16. Gerlach R, Raabe A, Beck J, et al. Postoperative nadroparin administration for prophylaxis of thromboembolic events is not associated with an increased risk of hemorrhage after spinal surgery. Eur Spine J. 2004;13(1):9–13. doi:10.1007/s00586-003-0642-8
17. Bono CM, Watters WC 3rd, Heggeness MH, et al. An evidence-based clinical guideline for the use of antithrombotic therapies in spine surgery. Spine J. 2009;9(12):1046–1051. doi:10.1016/j.spinee.2009.09.005
18. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315–352. doi:10.1016/j.chest.2015.11.026
19. Rogers FB, Cipolle MD, Velmahos G, et al. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: the EAST practice management guidelines work group. J Trauma. 2002;53(1):142–164. doi:10.1097/00005373-200207000-00032
20. Zhang C, Yu A, Yuan B, et al. Construction and functional evaluation of hirudin derivatives with low bleeding risk. Thromb Haemost. 2008;99(2):324–330. doi:10.1160/th07-07-0453
21. Greinacher A, Lubenow N. Recombinant hirudin in clinical practice: focus on lepirudin. Circulation. 2001;103(10):1479–1484. doi:10.1161/01.cir.103.10.1479
22. Dong X, Gu R, Zhu X, et al. Evaluating prodrug characteristics of a novel anticoagulant fusion protein neorudin, a prodrug targeting release of hirudin variant 2-Lys47 at the thrombosis site, by means of in vitro pharmacokinetics. Eur J Pharm Sci. 2018;121:166–177. doi:10.1016/j.ejps.2018.05.025
23. Dong X, Meng Z, Gu R, et al. Predicting the metabolic characteristics of neorudin, a novel anticoagulant fusion protein, in patients with deep vein thrombosis. Thromb Res. 2020;194:121–134. doi:10.1016/j.thromres.2020.05.048
24. Liu YB, Zhou XC, Liu Y, et al. Inhibitory role of recombinant neorudin on canine coronary artery thrombosis. Pharmacol Res Perspect. 2022;10(3):e00956. doi:10.1002/prp2.956
25. Liu YB, Zhang L, Zhou XC, et al. The antithrombotic effect of recombinant neorudin on thrombi. Drug Des Devel Ther. 2022;16:1667–1678. doi:10.2147/dddt.S353088
26. Liu Y, Wang M, Dong X, et al. A Phase I, single and continuous dose administration study on the safety, tolerability, and pharmacokinetics of neorudin, a novel recombinant anticoagulant protein, in healthy subjects. Pharmacol Res Perspect. 2021;9(3):e00785. doi:10.1002/prp2.785
27. Li S, Zhou J, Zhang J, et al. Construction of rat spinal cord injury model based on Allen’s animal model. Saudi J Biol Sci. 2019;26(8):2122–2126. doi:10.1016/j.sjbs.2019.09.033
28. Basso DM, Beattie MS, Bresnahan JC. A sensitive and reliable locomotor rating scale for open field testing in rats. J Neurotrauma. 1995;12(1):1–21. doi:10.1089/neu.1995.12.1
29. Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I9–16. doi:10.1161/01.Cir.0000078469.07362.E6
30. Arnold PM, Harrop JS, Merli G, et al. Efficacy, safety, and timing of anticoagulant thromboprophylaxis for the prevention of venous thromboembolism in patients with acute spinal cord injury: a systematic review. Global Spine J. 2017;7(3 Suppl):138s–150s. doi:10.1177/2192568217703665
31. Falck-Ytter Y, Francis CW, Johanson NA, et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e278S–e325S. doi:10.1378/chest.11-2404
32. Green D. Prophylaxis of thromboembolism in spinal cord-injured patients. Chest. 1992;102(6 Suppl):649s–651s. doi:10.1378/chest.102.6_supplement.649s
33. Alabed S, Belci M, Van Middendorp JJ, et al. Thromboembolism in the sub-acute phase of spinal cord injury: a systematic review of the literature. Asian Spine J. 2016;10(5):972–981. doi:10.4184/asj.2016.10.5.972
34. Matsumoto S, Suda K, Iimoto S, et al. Prospective study of deep vein thrombosis in patients with spinal cord injury not receiving anticoagulant therapy. Spinal Cord. 2015;53(4):306–309. doi:10.1038/sc.2015.4
35. Hull RD. Venous thromboembolism in spinal cord injury patients. Chest. 1992;102(6 Suppl):658s–663s. doi:10.1378/chest.102.6_supplement.658s
36. Aito S, Pieri A, D’Andrea M, et al. Primary prevention of deep venous thrombosis and pulmonary embolism in acute spinal cord injured patients. Spinal Cord. 2002;40(6):300–303. doi:10.1038/sj.sc.3101298
37. Piran S, Schulman S. Thromboprophylaxis in patients with acute spinal cord injury: a narrative review. Semin Thromb Hemost. 2019;45(2):150–156. doi:10.1055/s-0039-1678720
38. Zeeshan M, Khan M, O’Keeffe T, et al. Optimal timing of initiation of thromboprophylaxis in spine trauma managed operatively: a nationwide propensity-matched analysis of trauma quality improvement program. J Trauma Acute Care Surg. 2018;85(2):387–392. doi:10.1097/ta.0000000000001916
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.