Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Receptor Discordance and Molecular Subtype Changes in Visceral Metastases of Breast Cancer
Authors Tian Z ![]() , Chen X, Li H, Li C, Qiu W, Wang X
, Chen X, Li H, Li C, Qiu W, Wang X ![]() , Song X, Hou B, Liu Z, Yu J
, Song X, Hou B, Liu Z, Yu J ![]() , Yu Z
, Yu Z
Received 25 September 2025
Accepted for publication 16 January 2026
Published 23 January 2026 Volume 2026:18 565375
DOI https://doi.org/10.2147/BCTT.S565375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Zhaokun Tian,1,2,* Xiaojie Chen,1,2,* Haojia Li,2,* Chao Li,2 Wenyan Qiu,1,2 Xinzhao Wang,2 Xiang Song,2 Boyang Hou,2 Zhaoyun Liu,2 Jinming Yu,1,2 Zhiyong Yu1,2
1First Clinical Medical College, Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China; 2Breast Cancer Center, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinming Yu, Email [email protected] Zhiyong Yu, Email [email protected]
Background: Visceral metastases in breast cancer demonstrate considerable molecular heterogeneity. This study examines changes in receptor status and molecular subtypes between primary breast cancer and visceral metastases.
Methods: A retrospective analysis was conducted on 430 patients diagnosed with breast cancer and visceral metastases, including 138 with lung metastases and 292 with liver metastases. Receptor statuses (estrogen receptor [ER], progesterone receptor [PR], human epidermal growth factor receptor 2 [HER2]) were assessed in both primary and metastatic tumors. Discordance in molecular subtypes was assessed, and factors influencing receptor changes were identified. Survival outcomes were estimated using Kaplan–Meier analysis.
Results: Receptor discordance was observed in 47.9% (206/430) of patients, with a higher frequency in liver metastases (51.0%) than in lung metastases (41.3%). PR discordance was the most frequent (36.2%), followed by ER (18.9%) and HER2 (7.2%). Molecular subtype discordance occurred in 36.1% of patients, with the highest rate in Luminal A tumors (85.7%). Multivariate analysis identified pN3 stage and molecular subtype as independent predictors. Kaplan–Meier survival analysis showed that patients with ER gain had significantly improved disease-free survival (DFS) compared with those with ER loss (75.4 vs 44.5 months, P = 0.0092). Moreover, molecular subtype discordance was associated with longer DFS (63.9 vs 49.1 months, P = 0.0079).
Conclusion: This study emphasizes that there are significant differences in receptor expression and molecular subtypes between primary breast tumors and their visceral metastases. The receptor is more likely to change in patients with liver metastasis and Luminal A or Luminal B (HER2+) tumors, highlighting the importance of repeat biopsy in the metastatic environment. These findings can be used to identify high-risk patients and provide them with better treatment plans.
Keywords: breast cancer, receptor discordance, molecular subtype, visceral metastasis, survival analysis
Introduction
Breast cancer remains the most prevalent malignancy among women globally and is a leading cause of cancer-related mortality in this population.1,2 Despite substantial advancements in early detection and systemic treatment, approximately 20–30% of patients with early-stage disease eventually develop metastatic breast cancer (MBC).3–5 Among metastatic sites, involvement of visceral organs, particularly the liver and lungs, is frequently associated with aggressive disease behavior and a significantly poorer prognosis.6–8 Therapeutic decision-making in MBC is primarily guided by the status of key molecular markers, including estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2). Critically, these biomarkers not only dictate treatment strategies but also serve as essential prognostic indicators, underscoring their pivotal role in clinical management.9,10
However, mounting evidence highlights a phenomenon known as “receptor heterogeneity”, which refers to the differences in biomarker expression between primary tumors and their matched metastatic lesions. This has crucial clinical implications for disease management and patient prognosis.10–12 Specifically, such discordance can lead to a reclassification of the molecular subtype, consequently affecting subsequent treatment selection and influencing both progression-free survival (PFS) and overall survival (OS).12,13 These changes further reflect the inherent heterogeneity of tumors, posing difficulties in selecting treatment plans.14–16 Therefore, relying solely on the receptor characteristics of the primary tumor to select treatment plans for metastatic lesions may not be ideal, which further emphasizes the clinical necessity of reassessing the tumor receptor status during the metastasis process.17,18
While previous studies have consistently reported notable discrepancies between primary breast tumors and their matched metastases across various sites,3,19–23 the prevalence and prognostic significance of receptor discordance specifically in visceral metastases remain critically underexplored.24,25 Furthermore, the exact extent of receptor discordance in highly aggressive sites like liver and lung metastases, and its direct impact on patient prognosis, remain insufficiently defined.
This study utilized a large real-world cohort system to assess changes in receptor status (ER, PR, and HER2) between primary breast tumors and their visceral metastases. Our main objective is to determine the probability and prognostic impact of changes in this receptor and molecular subtype inconsistency. A key secondary objective is to describe potential clinical and pathological factors associated with observed subtype changes.
Methods
Patient Characteristics
We retrospectively evaluated the clinical and pathological data of 430 patients with visceral metastatic breast cancer at Shandong Cancer Hospital from 2020 to 2025, and analyzed and assessed the changes in receptor status and molecular subtypes between the primary breast tumor and visceral metastasis.
Eligible participants were female patients aged 18 years or older who had undergone surgical treatment for primary breast cancer. Inclusion required a confirmed pathological diagnosis of primary breast carcinoma and the availability of postoperative immunohistochemical (IHC) data for HER2, ER, PR, and Ki-67. Only patients with histopathologically confirmed visceral metastases limited to the lungs or liver were considered, based on imaging and biopsy, with no evidence of metastases at other sites at the time of diagnosis. In addition, IHC data for the metastatic lesions (HER2, ER, PR, Ki-67) and complete medical records detailing clinical examinations, treatments, and follow-up were required for inclusion.
Patients were excluded if they had not undergone surgery for both the primary tumor and metastatic lesions, if they had bilateral primary breast cancers, or if they were male. Cases of primary occult breast cancer (T0 stage) and patients with incomplete or missing medical records were also excluded. All patients signed informed consent forms, agreeing that their clinicopathological data could be used for clinical research. This study was approved by the Medical Ethics Committee of Shandong Cancer Hospital and Institute, Shandong First Medical University, and the Shandong Academy of Medical Sciences. The ethics approval number: SDTHEC 202508037. The study was conducted in full compliance with the principles of the Declaration of Helsinki.
Receptor Status Evaluation and Clinical Variable Collection
Receptor status was determined using IHC, following the American Society of Clinical Oncology (ASCO) guidelines. ER and PR positivity were defined by nuclear staining in at least 1% of tumor cells. HER2 positivity was defined as IHC 3+, or IHC 2+ with confirmed HER2 gene amplification by fluorescence in situ hybridization (FISH). HER2-negative status included IHC 1+ or IHC 2+ without FISH-confirmed amplification. Additionally, HER2-zero was defined as an IHC score of 0, while HER2-low included IHC scores of 1+ or 2+ without HER2 gene amplification. Molecular subtypes were classified according to the 2021 St. Gallen Breast Cancer Guidelines as Luminal A, Luminal B (HER2-negative), Luminal B (HER2-positive), HER2-enriched, and triple-negative breast cancer (TNBC). According to the immunohistochemical instructions, the antibodies are as follows: CONFIRM™ anti-Progesterone Receptor (PR)(1E2) Rabbit Monoclonal Primary Antibody (Ventana Medical Systems, USA).
CONFIRM anti-Estrogen Receptor (ER) (SP1) Rabbit Monoclonal Primary Antibody (Ventana Medical Systems, USA); VENTANA ati-HER2/neu (4B5) Rabbit Monoclonal Primary Antibody (Ventana Medical Systems, USA); KI67 Rabbit Monoclonal Primary Antibody (Qiming Gene Technology Co., Ltd, China).
Assessment of Receptor and Molecular Subtype Discordance
Receptor discordance was defined as any change in ER, PR, or HER2 expression between the primary tumor and its corresponding visceral metastases. These changes were categorized into three types: loss of expression (conversion from positive to negative), gain of expression (conversion from negative to positive), and concordance (no change in status). The frequencies of receptor and molecular subtype discordance were calculated, with further analysis stratified by metastatic site (lung versus liver). Molecular subtype discordance was defined as any shift in subtype classification between the primary and metastatic tumors.
Clinical and pathological variables extracted from patient records included age at diagnosis, type of breast surgery (mastectomy or breast-conserving surgery), lymphovascular invasion (LVI), histological tumor grade (G1–G3), pathological tumor (pT) stage, pathological nodal (pN) stage, receptor status (ER, PR, HER2), molecular subtype, time to visceral metastasis, and follow-up information.
Statistical Analysis
Categorical variables were presented as frequencies and percentages, while continuous variables were reported as medians with interquartile ranges (IQRs). Univariate and multivariate logistic regression analyses were performed to identify factors associated with receptor discordance and molecular subtype shifts. Adjusted odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated. Kaplan-Meier survival analysis was used to evaluate disease-free survival (DFS) in relation to receptor discordance, and survival curves were compared using the Log rank test. A two-tailed P-value of less than 0.05 was considered statistically significant. All statistical analyses were conducted using R software (version 4.2.2) and SPSS (version 26.0; IBM Corp., Chicago, IL, USA).
Results
Patient Characteristics
A total of 430 women with visceral metastases from breast cancer were analyzed, comprising 138 patients with lung metastases and 292 with liver metastases. All patients underwent histopathological evaluation of both primary and metastatic tumor sites, including assessment of ER, PR, and HER2 status. The median follow-up duration was 55 months, and the median age at diagnosis was 46 years (range, 32–78 years). The most prevalent molecular subtype was Luminal B (HER2-negative), identified in 230 patients (53.5%), followed by Luminal B (HER2-positive) in 59 (13.7%), triple-negative breast cancer (TNBC) in 56 (13.0%), Luminal A in 49 (11.4%), and HER2-enriched in 36 (8.4%). Baseline demographic and clinicopathological features are summarized in Tables 1 and 2.
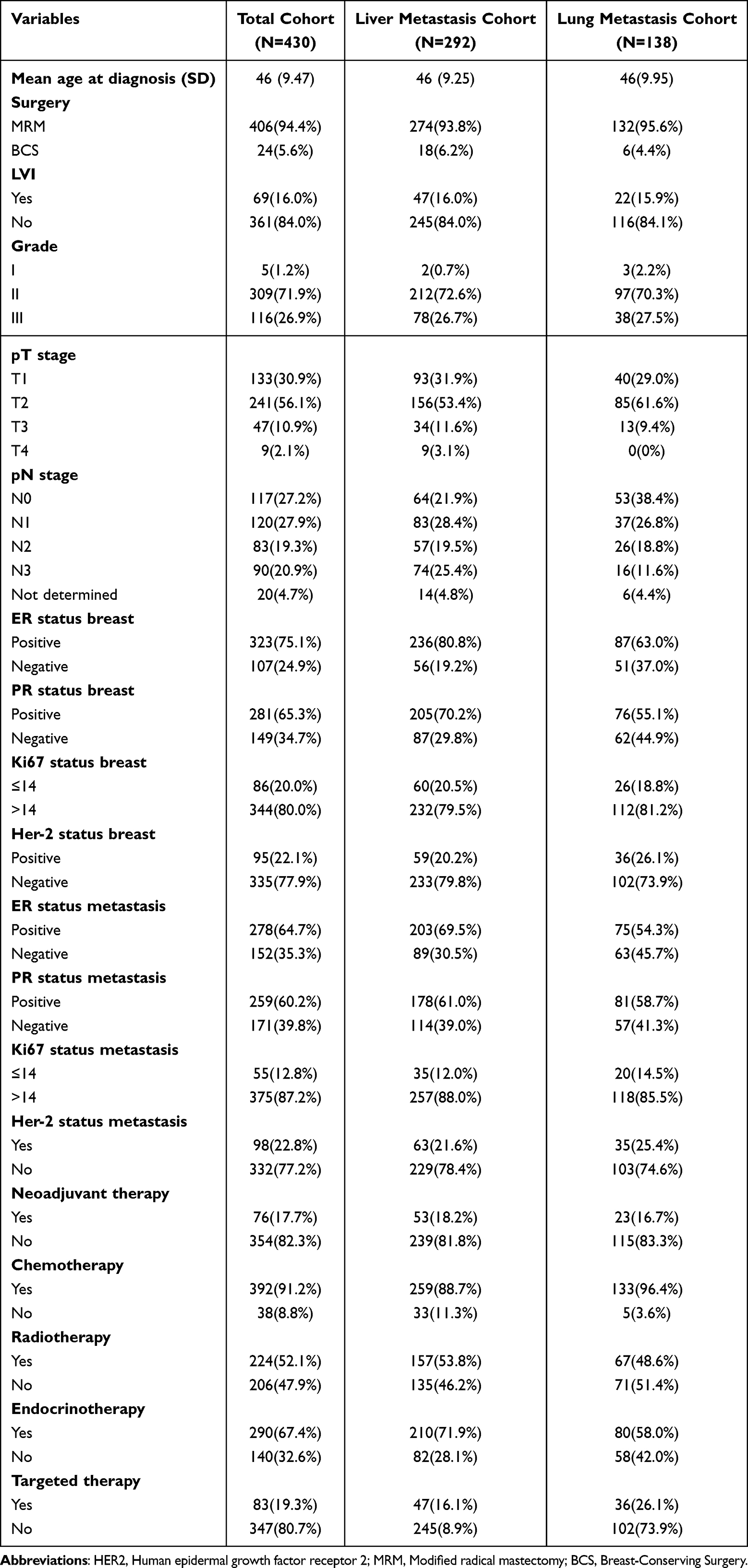 |
Table 1 Demographic and Clinicopathologic Baseline Characteristics |
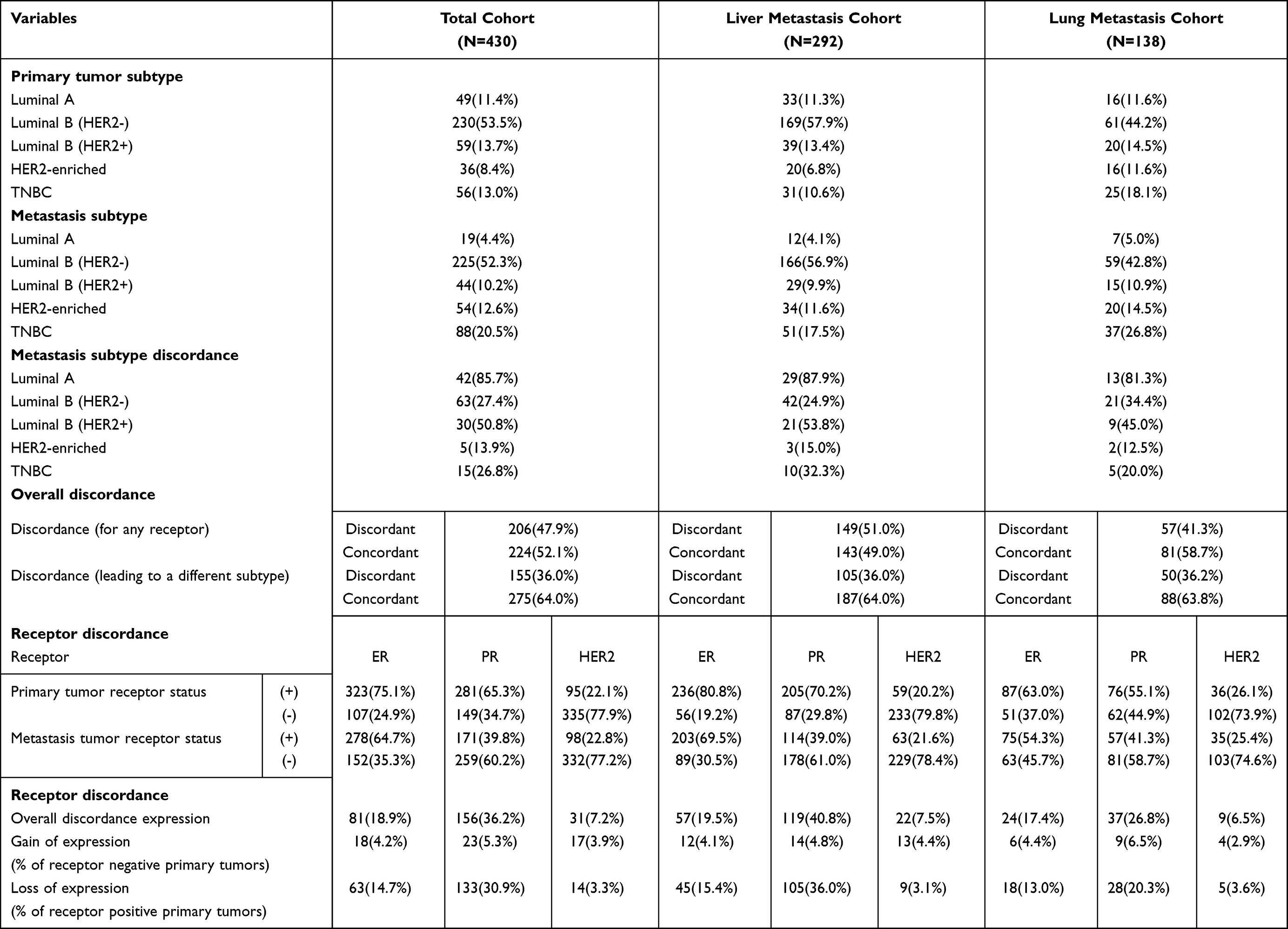 |
Table 2 Tumor Subtypes and Discordance |
Receptor Status Discordance
Among the 430 patients with visceral metastases, receptor discordance—defined as a change in at least one receptor status (ER, PR, or HER2) between the primary and metastatic tumors—was observed in 206 patients (47.9%). Within the liver metastasis subgroup, receptor discordance was seen in 149 of 292 patients (51.0%), with a molecular subtype discordance rate of 36.0% (105 of 292). In the lung metastasis subgroup, 57 of 138 patients (41.3%) exhibited receptor discordance, and 50 of 138 (36.2%) showed molecular subtype discordance. Detailed receptor discordance rates across ER, PR, and HER2 are shown in Table 2 and visualized in Figure 1. Analysis of ER, PR, and the proliferation marker Ki67 revealed significant differences between primary and metastatic tumors. ER expression showed no significant difference across the overall cohort (p > 0.05). However, PR expression was significantly lower and Ki67 expression significantly higher in metastatic tumors than in their primary counterparts (p < 0.0001). Subgroup analyses for liver and lung metastases demonstrated similar expression trends. These findings are illustrated in Figure 2, while changes in HER2 status are presented in Figure 3.
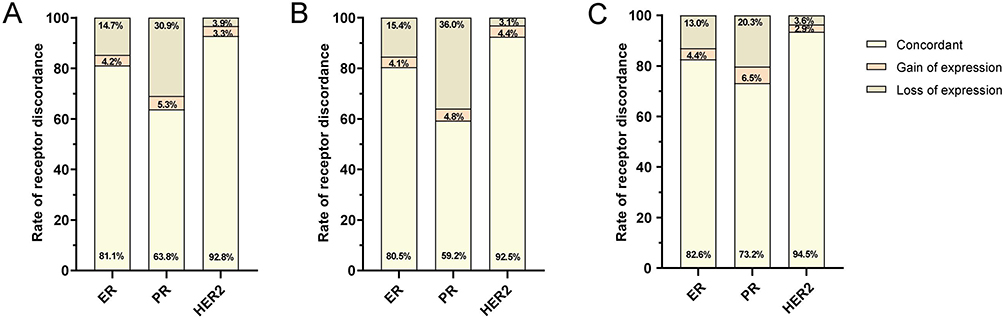 |
Figure 1 The rate of receptor discordance in ER, PR, and HER2 statuses. (A) Receptor discordance total cohort. (B) Receptor discordance Liver metastasis cohort. (C) Receptor discordance Lung metastasis cohort. |
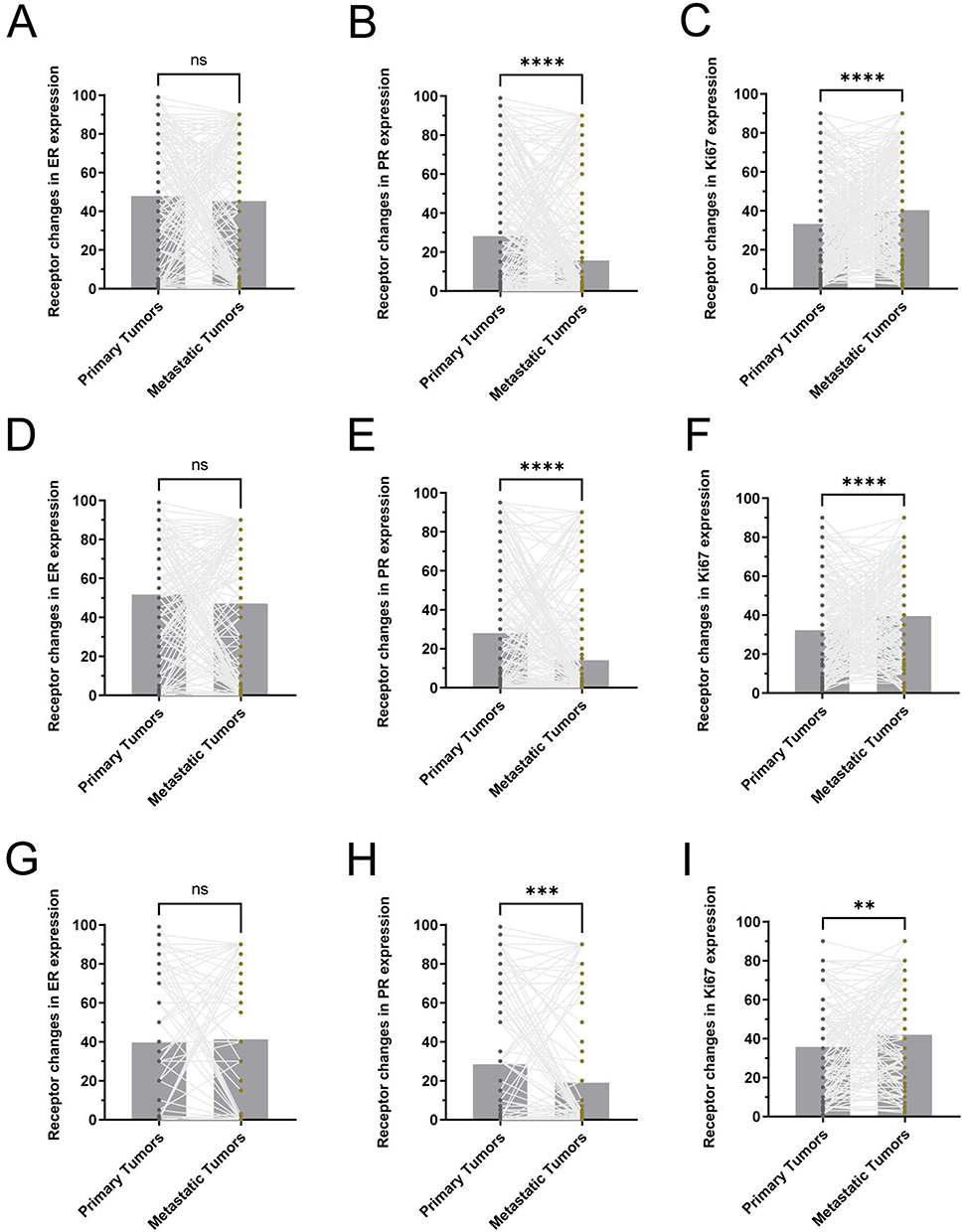 |
Figure 2 Receptor changes in ER, PR, and Ki67 expression. (A) Receptor changes in ER in total cohort. (B) Receptor changes in PR in total cohort. (C) Receptor changes in Ki67 in total cohort. (D) Receptor changes in ER in liver metastasis cohort. (E) Receptor changes in PR in liver metastasis cohort. (F) Receptor changes in Ki67 in liver metastasis cohort. (G) Receptor changes in ER in lung metastasis cohort. (H) Receptor changes in PR in lung metastasis cohort. (I) Receptor changes in Ki67 in lung metastasis cohort. ****p < 0.0001, ***p < 0.001, **p < 0.01. Abbreviation: ns, not significant. |
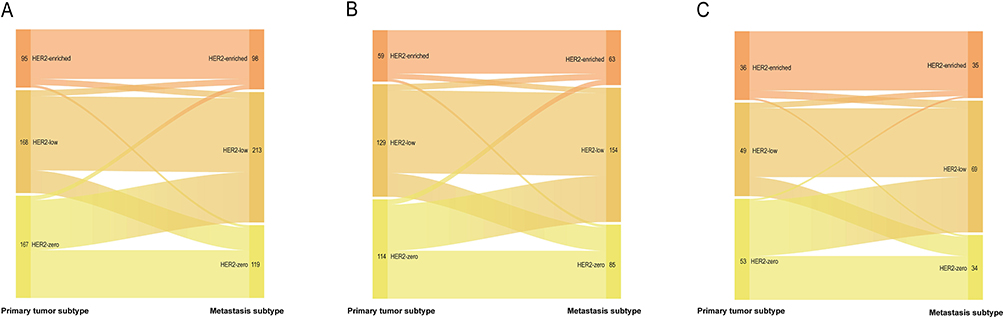 |
Figure 3 Distribution of HER2 status in primary and metastatic tumors. (A) Total cohort. (B) Liver metastasis cohort. (C) Lung metastasis cohort. |
Specifically, ER discordance occurred in 81 of 430 patients (18.9%), with loss of ER expression (positive to negative) in 63 patients (14.7%) and gain of ER expression (negative to positive) in 18 patients (4.2%). PR discordance was most frequent, observed in 156 patients (36.2%), with 133 (30.9%) showing a loss and 23 (5.3%) showing a gain in PR expression. HER2 discordance was the least common, found in 31 patients (7.2%), including 17 (3.9%) with loss and 14 (3.3%) with gain of expression. In the liver metastasis subgroup, ER discordance was found in 57 of 292 patients (19.5%), with 45 (15.4%) showing loss and 12 (4.1%) showing gain. PR discordance occurred in 119 patients (40.8%), with 105 (36.0%) experiencing loss and 14 (4.8%) showing gain. HER2 discordance was identified in 22 patients (7.5%), with 9 (3.1%) showing loss and 13 (4.4%) showing gain. In the lung metastasis subgroup, ER discordance was observed in 24 of 138 patients (17.4%), including 18 (13.0%) with loss and 6 (4.4%) with gain. PR discordance was noted in 37 patients (26.8%), with 28 (20.3%) showing loss and 9 (6.5%) showing gain. HER2 discordance occurred in 9 patients (6.5%), including 5 (3.6%) with loss and 4 (2.9%) with gain. Overall, PR exhibited the highest discordance rate among receptors, while HER2 exhibited the lowest. Across all receptors, loss of expression was more common than gain.
Molecular Subtype Discordance
Molecular subtype discordance—defined as reclassification due to receptor status changes—was observed in 155 of 430 patients (36.0%) in the overall cohort. Subgroup analyses revealed subtype discordance in 105 of 292 patients (36.0%) with liver metastases and in 50 of 138 patients (36.2%) with lung metastases. The probability of subtype change varied according to the molecular profile of the primary tumor, as shown in Table 2 and Figure 4.
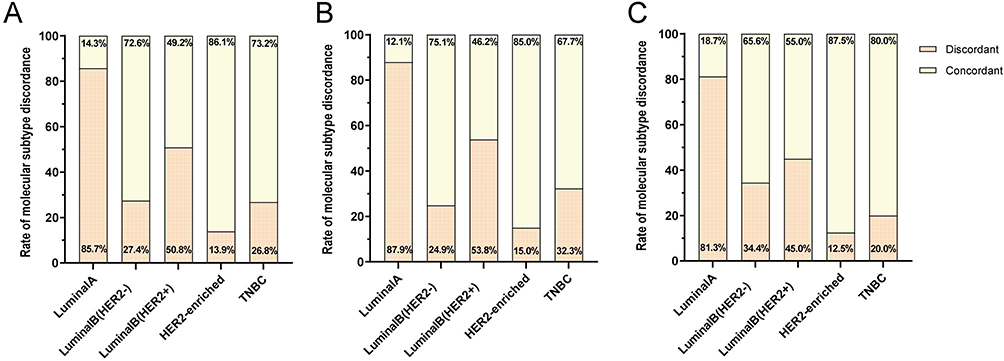 |
Figure 4 The rate of molecular subtype discordance. (A) Molecular subtype discordance total cohort. (B) Molecular subtype discordance liver metastasis cohort. (C) Molecular subtype lung metastasis cohort. |
Patients initially diagnosed with Luminal A had the highest rate of subtype discordance, observed in 42 of 49 cases (85.7%), followed by Luminal B (HER2-positive) in 30 of 59 cases (50.8%). The discordance rates for Luminal B (HER2-negative), TNBC, and HER2-enriched subtypes were 63 of 230 (27.4%), 15 of 56 (26.8%), and 5 of 36 (13.9%), respectively. In the liver metastasis group, Luminal A subtype showed the highest discordance rate at 29 of 33 (87.9%), followed by that of Luminal B (HER2-positive) at 21 of 39 (53.8%). Discordance rates for TNBC, Luminal B (HER2-negative), and HER2-enriched subtypes were 10 of 31 (32.3%), 42 of 169 (24.9%), and 3 of 20 (15.0%), respectively. In the lung metastasis group, Luminal A remained the most discordant (13 of 16; 81.3%), followed by Luminal B (HER2-positive) (9 of 20; 45.0%), Luminal B (HER2-negative) (21 of 61; 34.4%), TNBC (5 of 25; 20.0%), and HER2-enriched (2 of 16; 12.5%). Molecular subtype crossover patterns are visualized in Figure 5. Notably, patients with initial Luminal A or Luminal B (HER2-positive) subtypes were more likely to undergo molecular subtype conversion during metastatic progression, particularly in the liver and lung. Conversely, HER2-enriched tumors showed the lowest likelihood of subtype change.
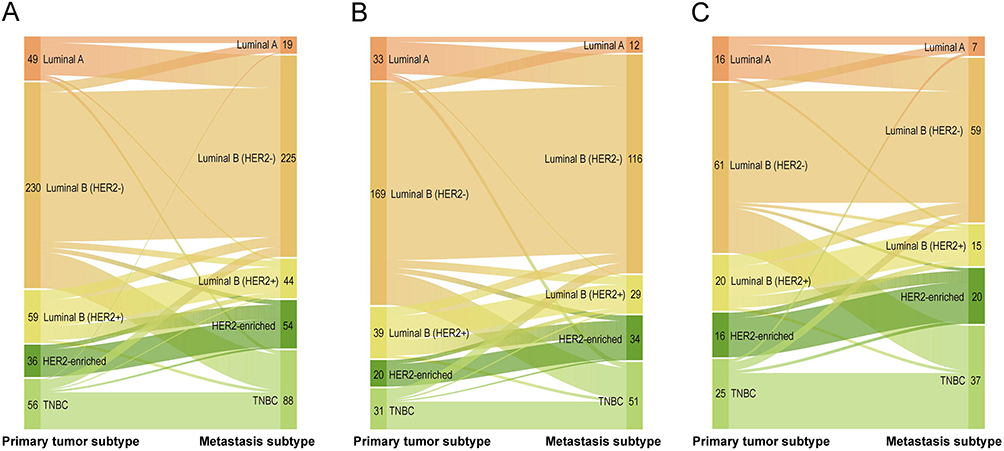 |
Figure 5 Visualizes molecular subtype crossover. Legend: Width of the bands indicates number of patients crossing over. (A) Total cohort. (B) Liver metastasis cohort. (C) Lung metastasis cohort. |
Factors Associated with Receptor Discordance
Univariate logistic regression analysis in the overall visceral metastasis cohort showed pN stage, Ki67 index, and primary molecular subtype were significantly associated with discordance. Multivariate analysis identified pN3 stage and molecular subtype as independent predictors of molecular subtype discordance. Compared to pN0, patients with pN3 stage had a significantly higher likelihood of subtype discordance (OR = 0.512, P =0.050). Compared with Luminal A, discordance was significantly associated with Luminal B (HER2-negative) (OR = 0.051, P < 0.001), Luminal B (HER2-positive) (OR = 0.135, P = 0.001), HER2-enriched (OR = 0.025, P < 0.001), and TNBC (OR = 0.045, P < 0.001). Full logistic regression results are presented in Table 3.
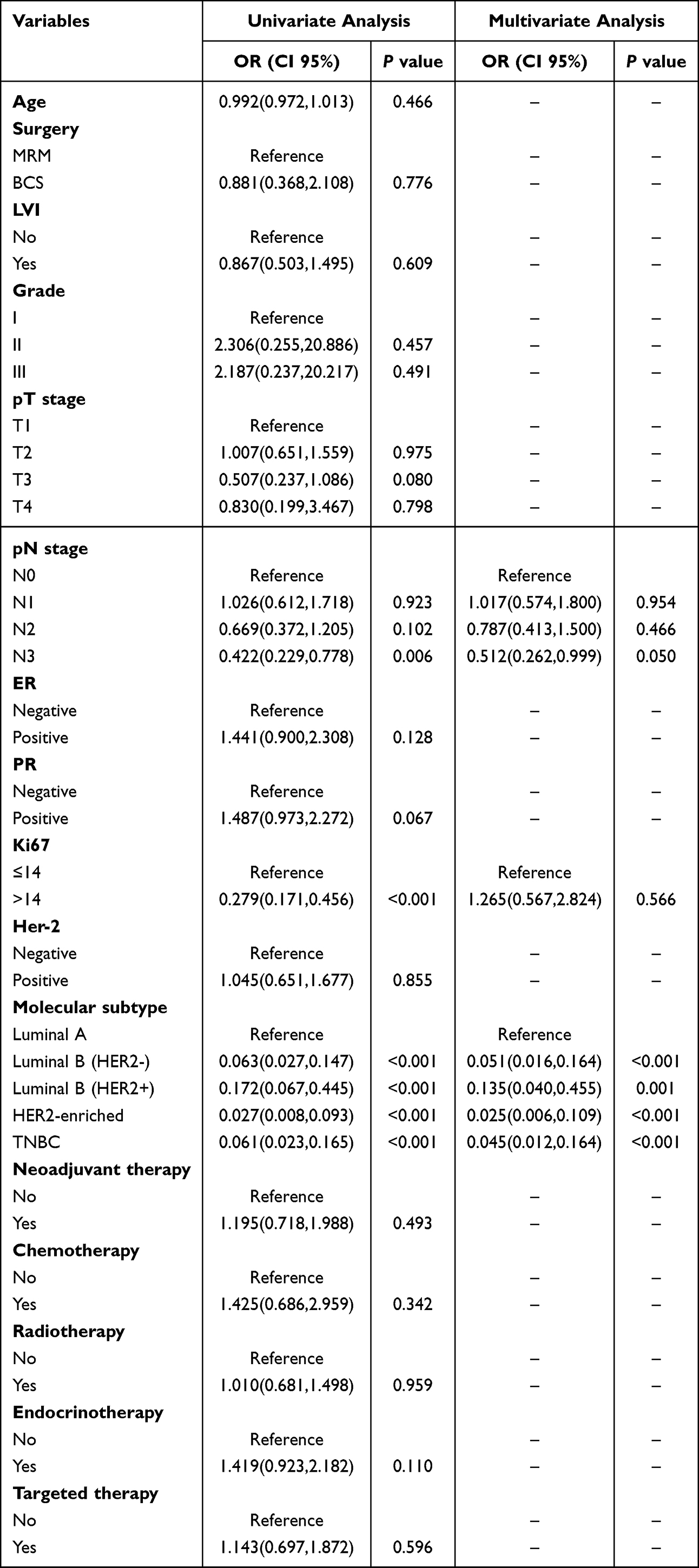 |
Table 3 Univariate and Multivariable Logistic Regression Analysis Based on Molecular Subtype Discordance for Visceral Metastasis Cohort |
Survival Analysis
Kaplan–Meier analysis for ER status revealed a median DFS of 55.0 months (95% CI: 48.8–61.2) in the receptor-concordant group, 44.5 months (95% CI: 21.0–67.9) in the ER-loss group, and 75.4 months (95% CI: 11.8–138.9) in the ER-gain group. The difference in DFS between the ER-gain and ER-loss groups was statistically significant (P = 0.0092). When stratified by molecular subtype concordance, the discordant group showed a median DFS of 63.9 months (95% CI: 49.9–77.8), compared to 49.1 months (95% CI: 43.0–55.3) in the concordant group. This difference was also statistically significant (P = 0.0079). Kaplan–Meier DFS curves for patients with visceral metastases are presented in Figure 6.
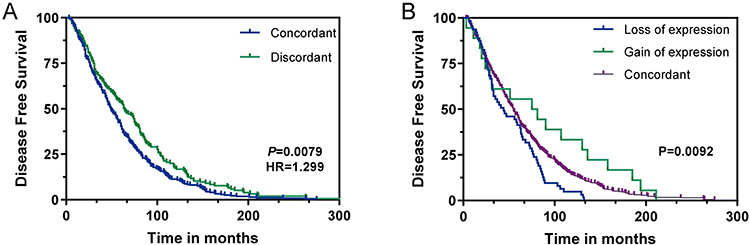 |
Figure 6 (A) Kaplan-Meier Disease-Fee Survival curves based on molecular subtype discordance in patients with visceral metastasis. (B) Kaplan-Meier Disease-Fee Survival curves based on ER receptor discordance in patients with visceral metastasis. |
Discussion
This study highlights a profound biological divergence in receptor status and molecular subtypes between primary breast tumors and corresponding visceral metastatic tumors, a phenomenon with critical implications for therapeutic optimization and patient prognosis. Receptor discordance was identified in 47.9% of the cohort, predominantly driven by shifts in PR status (36.2%), followed by ER (18.9%) and HER2 (7.2%). Notably, patients with Luminal A or Luminal B (HER2+) subtypes exhibited a higher propensity for discordance, reflecting significant intra-patient receptor heterogeneity during metastatic progression. These findings underscore the clinical imperative of reassessing biomarker expression at metastatic sites, reinforcing the necessity of repeat biopsies to refine treatment strategies and improve clinical outcomes.
Receptor discordance defined as any change in ER, PR, or HER2 status between primary and metastatic tumors. PR discordance was most common (36.2%), with PR loss (30.9%) occurring more frequently than PR gain (5.3%). ER changes followed a similar trend, with ER loss (14.7%) more prevalent than ER gain (4.2%). Given that PR expression is transcriptionally regulated by intact ER signaling, loss of PR likely reflects early disruption of estrogen pathway activity rather than an isolated biomarker fluctuation. Accordingly, PR discordance may serve as a sensitive surrogate indicator of impaired hormone responsiveness and emerging endocrine resistance, where ER expression appears to be preserved by immunohistochemistry. In such settings, Prolonged estrogen deprivation or selective estrogen receptor modulation may promote the expansion of ER-negative or functionally inactive subclones.17,26 Beyond its biological implications, receptor discordance also carries substantial prognostic relevance. Survival analyses further demonstrated that patients who acquired ER expression in metastatic lesions experienced significantly prolonged disease-free survival, whereas loss of ER expression was associated with poorer prognosis. These findings suggest that reacquisition of hormone receptor expression may partially restore endocrine treatment sensitivity,4,26 while receptor loss reflects more aggressive tumor biology and therapeutic resistance.9,27 By contrast, HER2 status exhibited relatively high concordance between primary and metastatic tumors, supporting the concept that HER2 amplification represents a genomically more stable oncogenic driver.8,28 Concomitant with receptor alterations, Ki67 expression was significantly higher in metastatic lesions than in primary tumors. Elevated Ki67 provides functional evidence of increased proliferative capacity accompanying receptor loss. Importantly, the simultaneous occurrence of hormone receptor loss—particularly PR—and increased Ki67 expression indicates a coordinated biological shift toward a more proliferative and less hormone-dependent phenotype.29 Notably, receptor inconsistency observed in liver metastasis is more common than in lung metastasis (51.0% vs 41.3%), indicating that organ specific metastatic microenvironment may lead to changes in molecular typing. The unique immune, metabolic, and interstitial environment of the liver may promote receptor instability. Overall, these findings emphasize that changes in receptor status are not only driven by intrinsic tumor factors, but also influenced by the tumor microenvironment of the target organ at the site of metastasis.3,12,13
Receptor discordance has crucial prognostic implications, possibly leading to reclassification of the tumor’s molecular subtype and necessitate alterations in therapeutic strategies. Notably, Luminal A tumors showed the highest propensity for subtype conversion, followed by Luminal B (HER2+) tumors, whereas HER2-overexpressing tumors demonstrated the greatest stability during metastatic progression. This is attributed to the increased possibility of ER, PR and HER2 deletion in metastatic lesions, as well as the corresponding increase in Ki67 levels, which contributes to the shift in molecular classification. Notably, PR receptors have the highest frequency of deletions. Therefore, in metastatic lesions, Luminal A tumors are more likely to be converted to Luminal B (HER2-) molecular typing, and Luminal B (HER2-) tumors also tend to develop TNBC molecular typing. These insights have enhanced our understanding of the clinical management of metastatic tumors. As disease evolution proceeds, loss of hormone receptor expression or functional inactivation of estrogen signaling pathways may facilitate a transition toward more aggressive molecular phenotypes.16,30 In contrast, the molecular typing of HER2 overexpressing tumors is relatively stable, and HER2 amplification is a powerful oncogenic driver on the genome, making it less susceptible to changes during metastasis and spread.9,31 Importantly, molecular subtype discordance is not merely a descriptive phenomenon but may substantially influence therapeutic decision-making.32 Of particular clinical relevance, metastatic biopsy evaluation may be particularly beneficial for patients diagnosed with Luminal A or Luminal B (HER2+) breast cancer. Collectively, these findings underscore that molecular subtype should be regarded as a dynamic rather than static characteristic, with direct implications for precision treatment selection in metastatic breast cancer.
Although this study provides valuable insights into the inconsistency between receptors and molecular subtypes, it has some limitations. Due to its retrospective study design, this research focuses more on the frequency and prognosis of receptor and molecular typing inconsistencies in clinical immunohistochemistry. Therefore, it lacks functional verification at the protein level and research on the molecular mechanisms of receptor inconsistencies. In addition, retrospective studies of cohorts may also have selection bias and limit causal inference. Therefore, it is necessary to conduct prospective studies, including the assessment of ESR1 mutations in ER loss cases, to clarify the biological drivers of receptor instability and optimize treatment strategies. Despite these limitations, we also found significant differences in receptor expression and molecular typing between primary breast tumors and their visceral metastases. The rate of receptor inconsistency is higher in patients with liver metastases and Luminal A or Luminal B (HER2+) tumors, highlighting the importance of repeated biopsies in metastatic environments. These findings can be used to identify high-risk patients and provide them with better treatment plans.
Conclusion
This study emphasizes that there are significant differences in receptor expression and molecular subtypes between primary breast tumors and their visceral metastases. The receptor is more likely to change in patients with liver metastasis and Luminal A or Luminal B (HER2+) tumors, highlighting the importance of repeat biopsy in the metastatic environment. These findings can be used to identify high-risk patients and provide them with better treatment plans.
Abbreviations
MBC, Metastatic breast cancer; ER, Estrogen Receptor; PR, Progesterone Receptor; HER2, Human Epidermal Growth Factor Receptor 2; DFS, Disease-Free Survival; OS, Overall Survival; TNBC, Triple-Negative Breast Cancer; IHC, immunohistochemical; FISH, fluorescence in situ hybridization; LVI, lymphovascular invasion; CI, confidence intervals; ASCO, American Society of Clinical Oncology; NCCN, National Comprehensive Cancer Network.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author (Zhiyong Yu) on reasonable request. The data are sourced from Shandong Cancer Hospital and Institute.
Acknowledgments
Thanks to all doctors for their efforts, and thanks to Shandong Cancer Hospital for the data provided.
Author Contributions
Zhaokun Tian, Xiaojie Chen, and Haojia Li contributed equally to this work as co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the foundation of National Natural Science Foundation of China (82030082), the foundation of Natural Science Foundation of Shandong (ZR2023ZD26) and Noncommunicable Chronic Diseases-National Science and Technology Major Project and Shandong Provincial Natural Science Foundation for Youths (ZR2024QH022).
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–14. doi:10.3322/caac.21834
2. Loibl S, Poortmans P, Morrow M, Denkert C, Curigliano G. Breast cancer. Lancet. 2021;397(10286):1750–1769. doi:10.1016/S0140-6736(20)32381-3
3. Sperduto PW, Mesko S, Li J, et al. Estrogen/progesterone receptor and HER2 discordance between primary tumor and brain metastases in breast cancer and its effect on treatment and survival. Neuro Oncol. 2020;22(9):1359–1367. doi:10.1093/neuonc/noaa025
4. Shiino S, Ball G, Syed BM, et al. Prognostic significance of receptor expression discordance between primary and recurrent breast cancers: a meta-analysis. Breast Cancer Res Treat. 2022;191(1):1–14. doi:10.1007/s10549-021-06390-6
5. Gao Y, Fang Y, Huang Y, et al. MIIP functions as a novel ligand for ITGB3 to inhibit angiogenesis and tumorigenesis of triple-negative breast cancer. Cell Death Dis. 2022;13(9):810. doi:10.1038/s41419-022-05255-0
6. Camargo S, Moskowitz O, Giladi A, et al. Neutrophils physically interact with tumor cells to form a signaling niche promoting breast cancer aggressiveness. Nat Cancer. 2025;6(3):540–558. doi:10.1038/s43018-025-00924-3
7. Nussinov R, Yavuz BR, Jang H. Molecular principles underlying aggressive cancers. Signal Transduct Target Ther. 2025;10(1):42. doi:10.1038/s41392-025-02129-7
8. Giordani E, Allegretti M, Sinibaldi A, et al. Monitoring changing patterns in HER2 addiction by liquid biopsy in advanced breast cancer patients. J Exp Clin Cancer Res. 2024;43(1):182. doi:10.1186/s13046-024-03105-9
9. Kao JY, Tsai JH, Wu TY, Wang CK, Kuo YL. Receptor discordance and phenotype change in metastatic breast cancer. Asian J Surg. 2021;44(1):192–198. doi:10.1016/j.asjsur.2020.05.032
10. Zheng A, Guo BL, Zhang JG, Jin F. Clinical information and management status of de novo stage IV breast cancer patients: a Chinese multicenter investigation (CSBrS-002). Chin Med J. 2021;134(13):1569–1575. doi:10.1097/CM9.0000000000001415
11. Raghavendra AS, Zakon DB, Jin Q, et al. Clinical outcomes of early-stage triple-negative breast cancer after neoadjuvant chemotherapy according to HER2-low status☆. ESMO Open. 2024;9(11):103973. doi:10.1016/j.esmoop.2024.103973
12. Lin M, Jin Y, Lv H, Hu X, Zhang J. Incidence and prognostic significance of receptor discordance between primary breast cancer and paired bone metastases. Int J Cancer. 2023;152(7):1476–1489. doi:10.1002/ijc.34365
13. Walter V, Fischer C, Deutsch TM, et al. Estrogen, progesterone, and human epidermal growth factor receptor 2 discordance between primary and metastatic breast cancer. Breast Cancer Res Treat. 2020;183(1):137–144. doi:10.1007/s10549-020-05746-8
14. Trillo P, Sandoval J, Trapani D, et al. Evolution of biological features of invasive lobular breast cancer: comparison between primary tumour and metastases. Eur J Cancer. 2023;185:119–130. doi:10.1016/j.ejca.2023.02.028
15. Jin J, Li B, Cao J, et al. Analysis of clinical features, genomic landscapes and survival outcomes in HER2-low breast cancer. J Transl Med. 2023;21(1):360. doi:10.1186/s12967-023-04076-9
16. Zhan H, Antony VM, Tang H, et al. PTEN inactivating mutations are associated with hormone receptor loss during breast cancer recurrence. Breast Cancer Res Treat. 2025;211(2):441–447. doi:10.1007/s10549-025-07660-3
17. Grinda T, Joyon N, Lusque A, et al. Phenotypic discordance between primary and metastatic breast cancer in the large-scale real-life multicenter French ESME cohort. NPJ Breast Cancer. 2021;7(1):41. doi:10.1038/s41523-021-00252-6
18. Khedr M, Gandhi S, Roy AM, et al. Breast biomarkers evolution between primary and distant metastasis: incidence and significance. Histopathology. 2025;86(5):793–804. doi:10.1111/his.15387
19. Sundén M, Norgren S, Lundqvist R, Andersson A, Sund M, Hemmingsson O. Receptor conversion and survival in breast cancer liver metastases. Breast Cancer Res. 2023;25(1):105. doi:10.1186/s13058-023-01706-4
20. Dowling GP, Keelan S, Cosgrove NS, et al. Receptor discordance in metastatic breast cancer; a review of clinical and genetic subtype alterations from primary to metastatic disease. Breast Cancer Res Treat. 2024;207(3):471–476. doi:10.1007/s10549-024-07431-6
21. Bloom JA, Sekigami Y, Young R, et al. Discordance in oncotype DX breast recurrence score(®) results for bilateral breast cancer. Ann Surg Oncol. 2021;28(13):8711–8716. doi:10.1245/s10434-021-10387-2
22. Yi ZB, Yu P, Zhang S, et al. Profile and outcome of receptor conversion in breast cancer metastases: a nation-wide multicenter epidemiological study. Int J Cancer. 2021;148(3):692–701. doi:10.1002/ijc.33227
23. Hu S, Zhao Y, Xie Y, et al. Clinicopathological characteristics, evolution, and treatment outcomes of hormone receptor-negative/HER2-low metastatic breast cancer: a pooled analysis of individual patient data from three prospective clinical trials. Front Endocrinol. 2024;15:1449278. doi:10.3389/fendo.2024.1449278
24. Boman C, Liu X, Eriksson Bergman L, et al. A population-based study on trajectories of HER2 status during neoadjuvant chemotherapy for early breast cancer and metastatic progression. Br J Cancer. 2024;131(4):718–728. doi:10.1038/s41416-024-02777-6
25. Rüschoff J, Penner A, Ellis IO, et al. Global study on the accuracy of human epidermal growth factor receptor 2-low diagnosis in breast cancer. Arch Pathol Lab Med. 2025;149(5):431–438. doi:10.5858/arpa.2024-0052-OA
26. Yeung C, Hilton J, Clemons M, et al. Estrogen, progesterone, and HER2/neu receptor discordance between primary and metastatic breast tumours-a review. Cancer Metastasis Rev. 2016;35(3):427–437. doi:10.1007/s10555-016-9631-3
27. Bardia A, Cortés J, Bidard FC, et al. Elacestrant in ER+, HER2- metastatic breast cancer with ESR1-mutated tumors: subgroup analyses from the phase III EMERALD trial by prior duration of endocrine therapy plus CDK4/6 inhibitor and in clinical subgroups. Clin Cancer Res. 2024;30(19):4299–4309. doi:10.1158/1078-0432.CCR-24-1073
28. Cai M, Li M, Lv H, et al. HER2-low breast cancer: evolution of HER2 expression from primary tumor to distant metastases. BMC Cancer. 2023;23(1):656. doi:10.1186/s12885-023-11134-4
29. Lu Z, Wang T, Wang L, Ming J. Research progress on estrogen receptor-positive/progesterone receptor-negative breast cancer. Transl Oncol. 2025;56:102387. doi:10.1016/j.tranon.2025.102387
30. Jung J, Lee SH, Park M, et al. Discordances in ER, PR, and HER2 between primary breast cancer and brain metastasis. J Neurooncol. 2018;137(2):295–302. doi:10.1007/s11060-017-2717-0
31. Chen R, Qarmali M, Siegal GP, Wei S. Receptor conversion in metastatic breast cancer: analysis of 390 cases from a single institution. Mod Pathol. 2020;33(12):2499–2506. doi:10.1038/s41379-020-0615-z
32. Gong Y, Liu YR, Ji P, Hu X, Shao ZM. Impact of molecular subtypes on metastatic breast cancer patients: a SEER population-based study. Sci Rep. 2017;7:45411. doi:10.1038/srep45411
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Clinical Prognostic Model for Breast Cancer Patients with Malignant Pleural Effusion: Avoiding Chemotherapy in Low-Risk Groups?
Wang Y, Zhou T, Zhao S, Li N, Sun S, Li M
Cancer Management and Research 2023, 15:409-422
Published Date: 11 May 2023