Back to Journals » Infection and Drug Resistance » Volume 12
Recent advances in Staphylococcus aureus infection: focus on vaccine development
Authors Ansari S ![]() , Jha RK, Mishra SK
, Jha RK, Mishra SK ![]() , Tiwari BR
, Tiwari BR ![]() , Asaad AM
, Asaad AM ![]()
Received 26 February 2019
Accepted for publication 19 April 2019
Published 13 May 2019 Volume 2019:12 Pages 1243—1255
DOI https://doi.org/10.2147/IDR.S175014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eric Nulens
Shamshul Ansari,1 Rajesh Kumar Jha,2 Shyam Kumar Mishra,3 Birendra Raj Tiwari,4 Ahmed Morad Asaad5
1Department of Microbiology, Chitwan Medical College and Teaching Hospital, Bharatpur, Chitwan, Nepal; 2Department of Systems and Diseases (Pharmacology), Saba University School of Medicine, Saba, Dutch Caribbean; 3Department of Microbiology, Maharajgunj Medical Campus, Institute of Medicine, Tribhuvan University, Kathmandu, Nepal; 4Department of Microbiology, Saint James School of Medicine, Anguilla, BWI; 5Department of Microbiology, Faculty of Medicine, Zagazig University, Zagazig, Egypt
Abstract: Staphylococcus aureus normally colonizes the nasal cavity and pharynx. After breaching the normal habitat, the organism is able to cause a number of infections at any site of the body. The development of antibiotic resistance has created a global challenge for treating infections. Therefore, protection by vaccines may provide valuable measures. Currently, several vaccine candidates have been prepared which are either in preclinical phase or in early clinical phase, whereas several candidates have failed to show a protective efficacy in human subjects. Approaches have also been made in the development of monoclonal or polyclonal antibodies for passive immunization to protect from S. aureus infections. Therefore, in this review we have summarized the findings of recently published scientific literature to make a concise report.
Keywords: active immunization, passive immunization, Staphylococcus aureus, vaccine
Introduction
A scenario of Staphylococcus aureus infection
Staphylococcus aureus is a common human pathogen which can colonize the skin, nose, and pharynx with anterior nares as the main reservoir.1,2 S. aureus is one of the major disease-causing organisms due to its unique ability to escape the innate immune response such as phagocytic, complement or antimicrobial peptide (AMP)-mediated killing, which assists survival in blood and other tissue during persistent infections.3 S. aureus has been found to be associated with a high rate of health care-associated infections (HAIs) in hospitalized and immuno-compromised patients as well as community-acquired infections (CAIs).4 A report found the nasal colonization of S. aureus in 37.8% of adults which rose up to 54.7% when throat samplings were added for detection.5 In fact, the challenges of HAIs and CAIs have increased in the last two decades. This organism has acquired an ability to cause a wide range of infections, from minor infections such as skin and eye infections to major infections such as bloodstream infections (BSIs) and pneumonia.6–8 Multi-drug-resistant S. aureus has been found to be one of the major organisms causing BSIs which are associated with high morbidity and mortality worldwide.9 Among BSIs, neonatal septicemia has been reported to be most commonly caused by this organism.10 Epidemiological studies found that BSIs-causing pathogen differs significantly between developed and developing countries.11 A recent Europen report from a Finnish Hospital Infection Program which was conducted during 1999–2001 and 2005–2010, found that S. aureus ranked among the top three organisms causing BSIs.12 Moreover, in another nationwide observational study conducted recently in Switzerland on all intravascular catheter (IVC) tip culture cases, S. aureus was reported as one of the most prevalent organisms causing subsequent BSIs in non-intensive care (non-ICU) and ICU patients. The findings also highlighted that particular attention should be paid if Candida albicans, S. aureus, Serratia marcescens, and Pseudomonas aeruginosa are isolated from IVC tips, as these organisms are associated with a higher frequency of subsequent BSIs than other pathogens.13 It has also been found that S. aureus was the leading organism causing native and prosthetic valve infection in high-income countries.14 Besides, S. aureus has also been isolated from lower respiratory tract infections such as pneumonia. Several clinical studies have highlighted its role as the predominant organism causing ventilator-associated pneumonia (VAP),15–17 which is the single most common HAI in ICUs around the world.18,19 A surveillance study conducted in European Union (EU) and European-Economic Area countries on health care-associated pneumonia (HAP) reported that 12% of cases were caused by S. aureus, which was the second most prevalent bacteria causing HAP, with 47% isolates resistant to methicillin.20 Despite causing infections in seriously ill patients, S. aureus has also been reported as the most predominant bacterial causative agent of community-acquired pneumonia.21 Cystic fibrosis, a predominantly P. aeruginosa-associated disease, has also been found to be caused by S. aureus.22
S. aureus and antimicrobial resistance
The emergence of infections caused by drug-resistant bacteria is a serious and growing global health concern. Therefore, significant efforts are being made in the development of new antimicrobial compounds with improved efficacy.23,24 However, despite these efforts, an increasing number of multi-drug-resistant bacteria including methicillin-resistant S. aureus (MRSA), extended-spectrum beta-lactamase (ESBL) producing Enterobacteriaceae, and carbapenem-resistant Gram-negative bacteria are being reported continuously.25–27 Once, beta-lactams, aminoglycosides, fluoroquinolones, macrolides, and trimethoprim-sulfamethoxazole were considered effective antibiotics to treat infections caused by S. aureus. However, its abuse and misuse have caused resistance and up to 85% of isolates have been reported to be non-susceptible to most of these antibiotics in current clinical use.28–30
In recent years, antimicrobial resistance has become a major public health issue and MRSA strains which have developed resistance to all beta-lactam antibiotics including penicillins, cephalosporins (except ceftaroline and ceftobiprole), and carbapenems have been reported to represent around 25% and even in some regions greater than 50%. The Centers for Disease Control and Prevention has reported 80,000 severe MRSA infections in the United States alone in 2011, with a rate of 11,000 deaths every year.31,32 More than half of hospital-acquired infections are caused by S. aureus in most Asian countries.33,34 Similarly, in 2012, MRSA was estimated to have caused infections in over 75,000 patients leading to the death of more than 9,600 in the United States.35 In the EU, the proportion of fatal cases is about 50,000 caused by multi-drug-resistant staphylococci out of approximately 3 million nosocomial infection cases, as reported by the European Centre for Disease Prevention and Control.36 A Chinese surveillance study reported S. aureus as one of the major pathogens causing BSIs, with more than half of the strains isolated being resistant to penicillin, erythromycin, cefazolin, and cefuroxime, whereas proportions of MRSA ranged from 30%–40%.37 In another study, conducted in 26 public hospitals in Hong Kong between January 2010 and December 2012, an increasing rate of MRSA was reported.38 In a recent meta-analysis report from Asia Pacific regions, the proportion of MRSA among all tested samples was reported to be up to 39% and the proportion of MRSA among all S. aureus isolates was reported to be up to 89%.39 Multi-drug-resistant S. aureus, including MRSA, can easily spread from the hospital setting to the community and within the community and poses additional problems for infection control strategies.40 However, infection control programs have been implemented recently in several countries. In the United States, Europe, and many other countries, multiple infection control “bundles“ such as allotting single rooms for MRSA-colonized or infected patients, targeted admission screening for high-risk patients and health care workers at high risk for infection with multi-drug-resistant pathogens, molecular typing of all MRSA strains, and decolonization of MRSA carriers, have been initiated and tested to control the spread. As a result of these strategies, a decreasing rate of MRSA has been reported. However, the pattern of drug resistance still remains a great challenge. Empirical treatment of presumptive S. aureus diseases with an alternative to the anti-staphylococcal beta-lactams such as clindamycin and trimethoprim-sulfamethoxazole, became widespread during the 1990s when community-associated MRSA was on the rise until 2000s.41,42 However, due to the overuse of these antibiotics, an increasing resistance continued to be reported and currently the resistance to these antibiotics pose a great threat to the treatment of infections.43,44 However, in a recent observational study on pediatric clinical cultures performed between 2005 and 2017 in the United States, a declining trend of MRSA from 41% to 27% over the study period, yet an increasing trend of clindamycin (from 21%–38% in MRSA and 5%–40% in MSSA) and trimethoprim-sulfamethoxazole (from 2%–13% in MRSA and relatively stable in MSSA) resistance were reported.45 Moreover, other studies have reported an increased incidence of MRSA as well as antibiotic resistance.46–49 Multiple factors have been implicated in the development of antibiotic resistance, such as over- and misuse of antibiotics mostly in developing countries; however, biofilm-mediated drug resistance in bacteria is another major mechanism and it has been predicted that if the current treatment practice continues unchanged, the infections caused by antibiotic-resistant bacteria would be a major cause of death in 2050 where the expected number of deaths will be around 10 million every year.50
To cope with these multi-drug resistance problems, several anti-staphylococcal drugs such as vancomycin, teicoplanin, linezolid, tedizolid, daptomycin, tigecycline, ceftaroline, ceftobiprole, oritavancin, and dalbavancin have been approved for treating the life-threatening infections caused by multi-drug-resistant S. aureus. Moreover, currently, in some countries vancomycin and teicoplanin are the most commonly used drugs to treat MRSA infections.51 However, increased MICs and reduced susceptibility to these antibiotics, poor tissue penetration, and adverse reactions due to the use of these antibiotics, have been reported to cause a limitation of its use in clinical practice.43,44,52–58 Because of the emerging problem of resistance, the World Health Organization (WHO) has listed MRSA and recently emerged vancomycin-intermediate and resistant S. aureus (VRSA) as “high-priority” deadly bacterial pathogens.59 To overcome the challenging situations in the management of multi-drug-resistant S. aureus infections, alternative therapeutic strategies are of utmost importance.
Recent advances in therapeutic strategies
The increasing resistance to conventional antibiotics is the most common health issue worldwide. To overcome this problem, many natural antimicrobial compounds have been attracting many researchers’ attention in the development of novel therapies for infections caused by the multi-drug-resistant organisms. Several such compounds with antimicrobial properties have been reported recently in many studies.
Peptides (amino acids) and their drug-conjugated derivatives
AMPs are small peptides of less than 50 amino acids with a net positive charge, possessing broad-spectrum antibacterial activity, and have attracted considerable attention.60 These AMPs exert antimicrobial activity by pore formation in the cell membrane and disrupting the membrane integrity. Although they do not need a specific ligand to bind, they exhibit capability to inhibit the activity of certain enzymes and prevent the protein and nucleic acid synthesis in bacteria.61,62 The antimicrobial activity of AMPs such as dicentracin-like peptide and moronecidin, against Gram-negative bacteria (such as Escherichia coli, Acinetobacter baumannii, P. aeruginosa), Gram-positive bacteria (such as S. aureus, Staphylococcus epidermidis), and Candida spp. (such as C. glabrata, C. tropicalis, C. albicans) was evaluated and high activity against S. aureus, S. epidermidis, and E. coli and a lower activity were found against other Gram-negative bacteria such as P. aeruginosa and A. baumannii clinical isolates. Moronecidin was found to exert more potency than dicentracin-like peptide against S. aureus including MRSA.63 Another such peptide, Hecate conjugated with vancomycin (Van/Hec) was tested in vancomycin-resistant and susceptible strains of S. aureus, and the microscopic findings revealed the disruption of bacterial cell integrity leading to the killing of all tested strains including wild-type, MRSA, and VRSA which was not observed when vancomycin or Hecate was used alone.64,65 Human cathelicidin (LL-37) and thrombocidin-1 (TC-1) have been found to synergize the activity of amoxicillin/clavulanic acid and teicoplanin against S. aureus.66,67 Xanthones are a class of heterocyclic compounds possessing the oxygen moiety which is widely distributed in nature, including two major plant families, Guttiferae and Gentianaceae, and also in fungi and lichens.68–70 The pharmacological activities of naturally occurring and synthetic xanthone derivatives have been described in several recent pieces of literature.71–73 Antibacterial activities of synthesized xanthone conjugated amino acids were recently evaluated against Gram-positive organisms (S. aureus and Bacillus subtilis) and Gram-negative organisms (E. coli and Klebsiella pneumoniea) as well as against several fungi (Aspergillus niger, C. albicans, and Fusarium oxysporum).74
Anti-staphylococcal phenolic compounds
Anti-staphylococcal phenolic compounds such as polyphenols (flavonols and phenolic acids) have been found to exert antimicrobial activity against several bacterial pathogens by inhibiting the activity of bacterial virulence factors, possessing a capability to interact with cytoplasmic membrane, suppressing the formation of biofilms, and can enhance the antimicrobial activity of antibiotics. The antibacterial activity of polyphenolic compounds against staphylococcal strains has been evaluated and found to exert a promising activity either alone or in combination with antibiotics.75
Anti-biofilm compounds
Biofilm is a thick extracellular polysaccharide material produced by many organisms and its synthesis prevents many antibiotics from penetrating the bacterial cell and renders them resistant. It has been elucidated that more than 25% of infections are associated with the biofilm producing ability of the bacteria. Biofilm producing S. aureus develops the ability to grow within the biofilm and survive phagocytosis and antibiotic action.76 Nano-scale materials such as silver nanoparticles have emerged as novel antimicrobial agents in combination with existing antibiotics and have shown the most effective antimicrobial activity in vitro.77–79 Several recent studies have tested the efficacy of these silver nanoparticles in combination with antibiotics and they have been found to be a novel therapeutic strategy to treat infections caused by multi-drug-resistant organisms.80–82 A synergistic effect increasing the antibiotic activity of penicillin combined with silver nanoparticles has been found against S. aureus including MRSA.83–85 In a recent study, Manukumar et al described the efficacy of thymol-loaded chitosan silver nanoparticles (T-C@AgNPs) against biofilm producing MRSA using disc diffusion method. Using different concentrations of T-C@AgNPs from 10, 25, 50, 100, 200, and 250 μg/mL and comparing the concentration that produced 10.08±0.06 mm of zone of inhibition (ZOI) with the standard antibiotic ciprofloxacin (10 μg) that had 10.95±0.08 mm ZOI, a dose-dependent biocidal and anti-biofilm activity was found.86 Another recent study also described the antibacterial activity of benzodioxane midst piperazine decorated chitosan silver nanoparticles (BP*C@AgNPs). In the study, using well diffusion test by loading different concentrations of synthetic BP*C@AgNPs against biofilm producing MRSA, depicted the dose-dependent membrane damage leading to bacterial killing. The study also depicted the role of BP*C@AgNPs in the inhibition of biofilm synthesis leading to the decreased adherence of bacterial cells to each other.87
Recent developments in active immunization
Because antibiotic resistance has been found as the major issue in the treatment of infections caused by multi-drug-resistant bacteria, vaccination could provide protection against the infections caused by antibiotic resistance as well as susceptible organisms. Primarily, the vaccine development focuses on the driving of antibody response which is able to block the toxins involved in the killing of immune cells as well as helping in the opsonization of bacterial cells. Therefore, several attempts have been made in the development of safe and effective vaccines (Table 1). However, some vaccine candidates failed to show significant protection and this may be because of overreliance on the antibody-mediated protective response.88
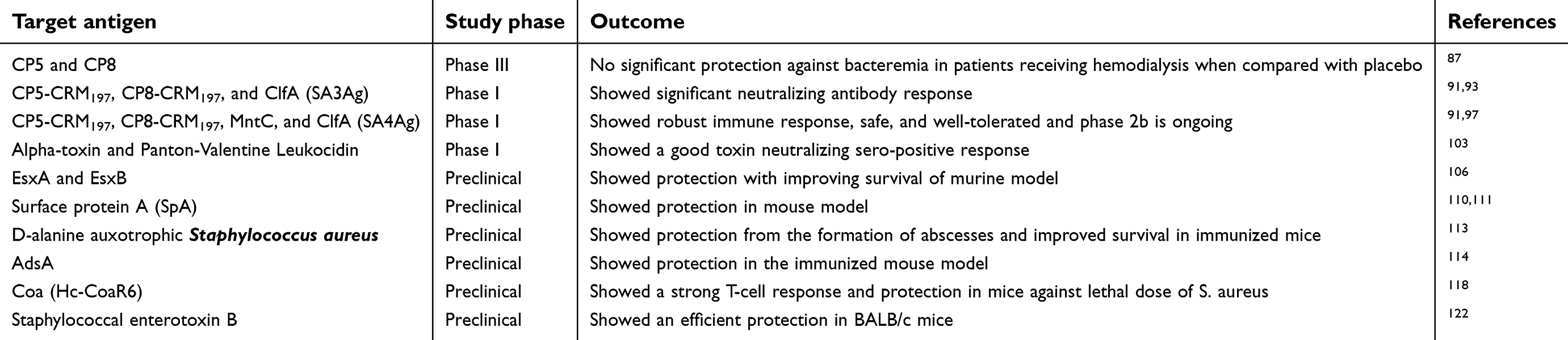 | Table 1 Candidate vaccines for active immunization |
Capsular polysaccharides (CPs) as vaccine candidates
Bacterial capsule is an extra-cellular material, which can be microscopically visualized using special techniques, covering the bacterial cells. Several bacteria have been found to possess the capsules such as E. coli, Neisseria meningitidis, Streptococcus pneumoniae, Haemophilus influenzae as well as S. aureus. Bacterial capsules are composed of long polysaccharide chains known as CPs. Capsules are the bacterial structure first recognized by the immune system, therefore, encapsulated bacteria have developed an immune evasion property which is exploited in the development of vaccines.89 The CPs have been targeted as an effective vaccine candidate for the protection from many bacterial infections such as S. pneumoniae, H. influenzae, and N. meningitidis.90 As many as eight different serotypes of capsules such as CP 1–8 (CP1 to CP8) have been found in S. aureus; however, the majority of the isolates causing diseases possess CP5 and CP8 which are the major effective vaccine targets.91–94 The expression of these CPs can be dynamic during infection, therefore, additional protein antigens are required for adequate protection.95 In 2002, the first S. aureus vaccine StaphVAX, developed by Nabi Biopharmaceuticals, consisting of CP5 and CP8 conjugated to recombinant P. aeruginosa exoprotein A, was used as a vaccine candidate in patients receiving hemodialysis in its initial phase III clinical trials. However, the study failed to show a significant protective effect compared with placebo in a follow-up period of 3–54 weeks post-vaccination. It was suggested that it may be due to many reasons such as the population targeted, production of the sub-optimal conjugate, or varying conjugate manufacture between trials; however, partial protection with a significant reduction in the S. aureus bacteremia number in the follow-up period of 3–40 weeks post-vaccination was found in a subsequent trial.96 Based on this partial protection, Fattom et al conducted a similar study using StaphVAX in the same patient population receiving hemodialysis. The assessment of the protective efficacy in vaccine recipients vs placebo up to 35 weeks after receiving a single dose or up to 60 weeks after receiving one or two vaccine doses suggested no protection against S. aureus bacteremia.97 The failure of this vaccine containing two single-antigens suggested that a multi-antigen vaccine containing several antigens might be successful. As a result, the first generation of multi-antigen vaccine containing three-antigens (S. aureus three-antigen [SA3Ag]) such as CP5, CP8 conjugated to the CRM197 and ClfA was designed.98
Recently, two types of vaccines namely, SA3Ag vaccine possessing CP5, CP8, and ClfA and S. aureus four-antigen (SA4Ag) vaccine possessing CP5, CP8, ClfA, and recombinant P305A developed from a lipoprotein manganese transporter C (MntC) have been successfully developed by the researchers, which have exhibited superior immunogenicity compared to previous vaccines.96,98–104 The studies have revealed that the previous vaccines generated anti-staphylococcal antibodies capable of binding with S. aureus leading to the uptake by phagocytic cells while the multi-antigen vaccines (SA3Ag and SA4Ag) are capable of inducing high level of anti-staphylococcal antibodies that lead to the killing of S. aureus by increasing the phagocytosis of bacteria and were concluded to be safe with no significant increase in systemic adverse effects or local adverse effects in healthy adults.96,104,105 The partial success of the first phase trial encouraged the researchers to design a novel multi-antigen vaccine (SA4Ag) containing CP5 and CP8 conjugated with CRM197 (CP5-CRM197 and CP8-CRM197) together with MntC and ClfA antigens.106 A multicenter phase I/II trial study conducted in the United States evaluated the immunogenicity, safety, and tolerability of SA4Ag vaccine in healthy adult volunteers of 18–64 years of age when injected as a single intramuscular dose.106 The findings of a recent animal model study demonstrated that this vaccine could elicit cytokine production by naive peripheral blood mononuclear cells leading to the induction of anti-staphylococcal antibodies and memory B-cell response.107 A phase II/III study to evaluate the efficacy of the SA4Ag vaccine for the prevention of invasive S. aureus disease in patients between 18–85 years of age who have had elective spinal surgery is under way.108,109 This vaccine was shown to be safe and well tolerated in the early stage of clinical trials inducing high levels of bacterial killing antibodies.101
Alpha-toxin and Panton-Valentine Leukocidin (PVL)
S. aureus alpha-toxin is a highly conserved toxin that disrupts the tissue and endothelial barrier and enhances bacterial penetration.110 PVL is a pore-forming protein exhibiting a cytotoxic nature which destroys leukocytes and causes tissue necrosis.111 A reduced risk of sepsis in adult patients with invasive S. aureus infection has been found with a higher level of IgG antibody against alpha-toxin.112 A recent phase I study was conducted by Landrum et al in healthy adults with an age range of 18–55 years old to evaluate the safety and immunogenicity of recombinant alpha-toxoid (rAT) and recombinant PVL (rLuks-PV) either monovalent or bivalent. The subjects were injected with monovalent form and followed-up on days 7, 14, 28, and 84 and those injected with bivalent form received a second dose on day 84 and were followed-up on days 98 and 112. A sero-positivity for toxin neutralizing antibody was found in a high proportion of subjects against rAT and rLuks-PV. As a result, both the rAT and rLuks-PV vaccine formulations were found to possess a favorable safety profile, were well-tolerated, and had high immunogenicity with neutralizing antibody when administered either alone or in combination in healthy adults.113
Secretory proteins EsxA and EsxB as a vaccine model
The bacterial secretion system helps the bacteria to transport the virulence factors in the host cells. The type VII secretion system is the best-characterized system in S. aureus. Early secreted antigenic target-6 kDa (ESAT-6) secretion system (ESS) is a specialized secretion system similar to the Esx-1 secretion system described in Mycobacterium tuberculosis, also identified in S. aureus. ESS in S. aureus consists of 12 proteins including highly conserved EsxA and EsxB closely related with ESAT-6 and CFP-10 respectively of M. tuberculosis.114 In 2005, these proteins were identified and verified to be secreted and implicated in the development and persistence of staphylococcal abscess formation in the murine model.115 In a recent study, the attenuated Salmonella typhimurium SPI-1 T3SS was utilized to translocate the secretory proteins EsxA and EsxB fused with N-terminal domain of SipA (1–169 amino acids) into the host cells of BALB/c mice. The mice were immunized orally with three doses of S. typhimurium strains N19, N20, and vector control strain N106 on Day 1, Day 8, and Day 22 and 5×1010 CFU of freshly cultured and PBS-washed bacterial cells, and the vaccinated mice were intravenously challenged with 5×107 CFU of S. aureus USA300 strain or Newman strains after 10 days of secondary booster dose. The immunogenicity study showed that the mice immunized with N19 strain generated a high level of EsxA-specific IgG1 and IgG2a antibody, indicating Th1/Th2-type immune response and a Th2-biased response against the EsxB antigen protecting the N20 vaccinated mice while improving the survival rate in N19 vaccinated mice.116
Surface protein A as a vaccine candidate
SpA is an abundant surface protein and a virulence factor which is released during normal cell division. SpA is able to interact with the Fc portion of IgG and suppresses the adaptive immune response by limiting the antibody production by B-cells whereas it enhances the immune response if it binds with B-cell receptor allowing the activation of B-cells.117–119 Therefore, suppression of the IgG binding effects of SpA could be able to mount the immune response. In a study, Kim et al, when immunizing a mouse model with non-toxigenic protein A withg substitutions Gly9Lys, Gln10Lys, Asp36Als, and Asp37Ala in the D-domain of the Ig binding region (SpA-DKKAA), found rising antibody titers and protective efficacy against MRSA and MSSA infection.120 Another recent study depicted the efficacy of the combined vaccine containing recombinant S. aureus surface protein A (SasA) and the internal heavy chain translocation domain C-fragment of tetanus neurotoxin (TenT-Hc). The combined vaccine conferred complete protection to the mouse against lethal intra-peritoneal challenges with 3×109 CFU of MRSA USA300 strains.121
D-alanine auxotrophic strain of S. aureus as a vaccine model
D-alanine is an essential component of the bacterial cell wall polysaccharide. Lacking a gene involved in the D-alanine biosynthesis makes the strains attenuated.122 In a recent study an attempt was made to assess the impact of D-alanine auxotrophy on protection from the parental strains. The S. aureus 132 strain lacking the gene involved in D-alanine biosynthesis was allowed to grow on media supplemented with exogenous D-alanine. The infection with D-alanine auxotrophic strain elicited a protective immune response and generated cross-reactive antibodies which provided protection following administration of different doses of its parental strain in immunized BALB/c mice. The D-alanine auxotroph vaccine exhibited a reduction in the measured bacterial load in vital organs such as kidney, spleen, heart, liver, and lung. The vaccine protected against the formation of abscesses and survival of the immunized mice was enhanced following infection with the parental strain.123
AdsA
AdsA is a cell wall anchored enzyme which plays an important role in immune evasion.3 AdsA deficient strains have been found to be labile after engulfment by polymorphonuclear leukocytes, while wild-type strains remain stable. In a study, active immunization of 6-week-old female BALB/c mice with 25 μg of rAdsA protein by intramuscular injection and subsequent infection with S. aureus Newman or USA300 strain was performed. As a result, a high level of anti-AdsA IgG and a reduced abscess size with little or no dermonecrosis was seen in the mice vaccinated with rAdsA when compared with the control mice. The anti-AdsA antibody was found to promote the killing of S. aureus by immune cells and reduced the intracellular as well as the extracellular number of S. aureus in macrophages of mice.124 Therefore, AdsA is an important antigen candidate for vaccine or therapeutic approach against the S. aureus infection.
Coa as a vaccine model
S. aureus Coa is a protein with enzymatic action which activates prothrombin to convert fibrinogen into fibrin threads via its N-terminal D1-D2 domain. The fibrin threads generate a protective shield on the surface of S. aureus through its C-terminal R domain. The monoclonal antibody against the R domain was found to promote the phagocytosis of S. aureus by immune cells, suggesting its role in the enhancement of bacterial killing and protection of the host.125–127 Regarding these findings, a recent study evaluated the protective efficacy of the R domain of Coa (CoaR6) fused with the carrier protein (Hc), a 66 C-terminal fragment of the heavy chain of tetanus neurotoxin (TT) in a peritonitis mouse model challenged intra-peritoneally with 2×109 CFU of MRSA252 or 1×109 CFU of USA300 4 weeks after the third immunization with Hc-CoaR6 combined with alum and CpG. The TT was used to increase the immunogenicity of the so-called Hc-CoaR6 vaccine. The results suggested that the Hc-CoaR6 vaccine could improve immunogenicity when compared with the immunogenicity elicited by the CoaR6 alone. The findings also suggested that a strong T-cell response and protection of mice against the lethal dose of S. aureus could be elicited by the Hc-CoaR6 vaccine model.128
Staphylococcal enterotoxin B (SEB)
SEB is a stable toxin which exerts powerful effects in humans at a very low dose. When inhaled, SEB can induce several symptoms ranging from headache, myalgia, increased heartbeat, coughing, enteric dysfunction (nausea, vomiting, and diarrhea) to life-threatening toxic shock syndrome.129,130 A previous study used the formalin treated SEB toxoid vaccine, and although it demonstrated some degree of protection of the animal models, it was not approved for use in humans.131 Owing to this protective efficacy, a recent study also evaluated the protection in a mouse model immunized with mutant SEB vaccine candidate produced by site-specific mutagenesis. A substantial level of toxin neutralizing antibody response was elicited, which provided efficient protection to the BALB/c mice against a lethal dose of SEB challenge.132
Recent developments in passive immunization
Anti-staphylococcal monoclonal antibodies as prophylactic agents for patients with a high risk of developing severe S. aureus infections are considered a novel anti-staphylococcal approach. A potential advantage of increasing the effectiveness of the conventional antibiotic treatment has been suggested of the anti-staphylococcal antibody. As alpha-toxin is expressed by the majority of S. aureus strains, the monoclonal antibody against the alpha-toxin may be effective in protecting against infections caused by S. aureus, including MRSA. Several studies have claimed the protective role of anti-alpha-toxin antibody from the S. aureus infections.133–135 A phase II trial of the monoclonal antibody has evaluated the efficacy and safety of a single dose of the human anti-staphylococcal monoclonal antibody against the S. aureus α-toxin under the project entitled “human monoclonal antibody against S. aureus α-toxin in mechanically ventilated adult subjects”. However, the results of this study and whether this approach can have a positive impact on treatment of staphylococcal diseases remain to be evaluated.136 In another recent study, an attempt was made to evaluate the efficacy of anti-staphylococcal antibodies by injecting 200 μL of rAdsA immunized rabbit antisera into the tail vein of 8-week old BALB/c mice 24 hours prior to challenge with S. aureus. As a result, passive immunization with the AdsA-specific antisera reduced the S. aureus Newman or USA300 infection in the mouse model. The AdsA-specific antiserum was found to promote the killing of S. aureus by immune cells while decreasing the infection severity in a different mouse model.120 In a study conducted by Varshney et al, the natural antibody against Staphylococcus protein A (514G3) was found to promote the opsonophagocytic killing of S. aureus by human blood cells, and protected the bacteremia mouse model from the lethal intravenous challenge of 3×107 CFU of MRSA.137 The protective role of passive immunotherapy with polyclonal antibodies against recombinant autolysin (r-autolysin) was recently evaluated by Kalali et al. As a result, the addition of anti-r-autolysin was found to promote the phagocytosis of S. aureus and the number of viable bacterial cells was decreased over 66.5% after 90 minutes compared with the control group; and in the mouse model of sepsis, the addition of anti-r-autolysin IgG fraction significantly enhanced the survival of the animals.138 The role of hemolysin-alpha (Hla)-specific and Hla-leukocidin cross-neutralizing monoclonal antibodies was evaluated for their efficacy in protection from pneumonia. In the study, 6–8 week old female BALB/cJRj mice were intra-nasally challenged with a lethal dose of 8×108 CFU CA-MRSA clones USA300-0114 at 24 hours post-immunization with the monoclonal antibodies and survival was monitored daily for 10 days after post-challenge. The result exhibited a protective efficacy in the induced murine pneumonia model.139 A similar study conducted by Stulik et al, also depicted the prophylactic efficacy of anti-Hla monoclonal antibody in a lethal rabbit pneumonia model challenged with MRSA and MSSA.140 MRSA exhibits methicillin resistance which is conferred by the acquisition of a mobile genetic element, mecA, which encodes an altered protein involved in the cell wall synthesis (PBP2a). Active immunization of mice with recombinant PBP2a (rPBP2a) significantly induces specific antibodies.141 It was assumed that the antibodies against rPBP2a might exhibit a protective activity if used for passive immunization. Naghshbandi et al conducted a study to elucidate the efficacy of passive immunization with anti-rPBP2a IgG fraction in MRSA challenged mice. In the study, the mice were passively immunized with 500 μL of IgG fraction 2 hours before and 24 hours after infection with a lethal dose of 5×105 CFU of MRSA, and were monitored for survival until 30 days after inoculation. As a result, passive immunization was found to play a considerable role in the protection which enhanced the survival of the experimental mice.142 However, despite several vaccine candidate developments, there is a possibility of immune evasion. Recently it was described that the presence of the bacteriophage DNA encoding a TarP protein in MRSA can modify the bacterial cell wall polymers, inhibiting the recognition by the host adaptive immune response, which could make the bacteria resistant to being recognized by the antibodies. Thus, the evasion of bacteria of the immune system might be able to cause severe infections.143
Conclusion
The wide-spread infections caused by multi-drug-resistant S. aureus have demanded priority in the development of an effective therapeutic approach. Although some vaccine candidates have shown protective efficacy in preclinical phase or early clinical phase studies, so far, no vaccine has been approved for human use. In addition to active immunization, the use of novel antibody-based passive immunization strategies might offer hope, as they have shown promising efficacy in the preclinical phase of evaluation.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mermel LA, Cartony JM, Covington P, Maxey G, Morse D. Methicillin-resistant Staphylococcus aureus colonization at different body sites: a prospective, quantitative analysis. J Clin Microbiol. 2011;49(3):1119–1121. doi:10.1128/JCM.02601-10
2. Kaspar U, Kriegeskorte A, Schubert T, et al. The culturome of the human nose habitats reveals individual bacterial fingerprint patterns. Environ Microbiol. 2016;18(7):2130–2142. doi:10.1111/1462-2920.12891
3. Thammavongsa V, Kern JW, Missiakas DM, Schneewind O. Staphylococcus aureus synthesizes adenosine to escape host immune responses. J Exp Med. 2009;206:2417–2427. doi:10.1084/jem.20090097
4. Lowy FD. Antimicrobial resistance: the example of Staphylococcus aureus. J Clin Investig. 2003;111:1265–1273. doi:10.1172/JCI18535
5. Antri K, Akkou M, Bouchiat C, et al. High levels of Staphylococcus aureus and MRSA carriage in healthy population of algiers revealed by additional enrichment and multisite screening. Eur J Clin Microbiol Infect Dis. 2018;37(8):1521–1529. doi:10.1007/s10096-018-3279-6
6. Kazimoto T, Abdulla S, Bategereza L, et al. Causative agents and antimicrobial resistance patterns of human skin and soft tissue infections in Bagamoyo, Tanzania. Acta Trop. 2018;186:102–106. doi:10.1016/j.actatropica.2018.07.007
7. Deguchi H, Kitazawa K, Kayukawa K, et al. The trend of resistance to antibiotics for ocular infection of Staphylococcus aureus, coagulase-negative staphylococci, and corynebacterium compared with 10-years previous: a retrospective observational study. PLoS One. 2018;13(9):e0203705. doi:10.1371/journal.pone.0203705
8. Belyhun Y, Moges F, Endris M, et al. Ocular bacterial infections and antibiotic resistance patterns in patients attending Gondar teaching hospital, Northwest Ethiopia. BMC Res Notes. 2018;11:597. doi:10.1186/s13104-018-3705-y
9. Keihanian F, Saeidinia A, Abbasi K, Keihanian F. Epidemiology of antibiotic resistance of blood culture in educational hospitals in Rasht, North of Iran. Infect Drug Resist. 2018;11:1723–1728. doi:10.2147/IDR.S169176
10. Yadav NS, Sharma S, Chaudhary DK, et al. Bacteriological profile of neonatal sepsis and antibiotic susceptibility pattern of isolates admitted at Kanti children’s hospital, Kathmandu, Nepal. BMC Res Notes. 2018;11:301. doi:10.1186/s13104-018-3394-6
11. Dat VQ, Vu HN, Nguyen The H, et al. Bacterial bloodstream infections in a tertiary infectious diseases hospital in Northern Vietnam: aetiology, drug resistance, and treatment outcome. BMC Infect Dis. 2017;17(1):493. doi:10.1186/s12879-017-2757-2
12. Huttunen R, Attman E, Aittoniemi J, et al. Nosocomial bloodstream infections in a finnish tertiary care hospital: a retrospective cohort study of 2175 episodes during the years 1999–2001 and 2005–2010. Infect Dis. 2015;47(1):20–26. doi:10.3109/00365548.2014.956791
13. Buetti N, Lo Priore E, Atkinson A, et al. Low incidence of subsequent bacteraemia or fungaemia after removal of a colonized intravascular catheter tip. Clin Microbiol Infect. 2018;24:548e1–548e3. doi:10.1016/j.cmi.2017.09.009
14. Pant S, Patel NJ, Deshmukh A, et al. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J Am Coll Cardiol. 2015;65(19):2070–2076. doi:10.1016/j.jacc.2015.03.518
15. Walaszek M, Różańska A, Walaszek MZ, Wójkowska-Mach J. The Polish society of hospital infections team. Epidemiology of ventilator-associated pneumonia, microbiological diagnostics and the length of antimicrobial treatment in the polish intensive care units in the years 2013–2015. BMC Infect Dis. 2018;18:308. doi:10.1186/s12879-018-3109-6
16. Huang Y, Jiao Y, Zhang J, et al. Microbial etiology and prognostic factors of ventilator-associated pneumonia: a multicenter retrospective study in Shanghai. Clin Infect Dis. 2018;67(S2):S146–S152. doi:10.1093/cid/ciy686
17. Bonell A, Azarrafiy R, Huong VTL, et al. A systematic review and meta-analysis of ventilator-associated pneumonia in adults in Asia: an analysis of national income level on incidence and etiology. Clin Infect Dis. 2018;68(3):511–518. doi:10.1093/cid/ciy543
18. Rosenthal VD, Maki DG, Mehta A, et al. International nosocomial infection control consortium members. International report, data summary for 2002–2007. Am J Infect Control. 2008;36:627–637. doi:10.1016/j.ajic.2008.03.003
19. Rosenthal VD, Al-Abdely HM, El-Kholy AA, et al. International nosocomial infection control consortium report, data summary of 50 countries for 2010–2015: device-associated module. Am J Infect Control. 2016;44:1495–1504. doi:10.1016/j.ajic.2016.08.007
20. Jan W, Sebastian H, Chantal Q, et al. Healthcare-associated pneumonia in acute care hospitals in European Union/European Economic area countries: an analysis of data from a point prevalence survey, 2011 to 2012. Euro Surveill. 2018;23(32):1700843.
21. El-Sokkary RH, Ramadan RA, El-Shabrawy M, et al. Community acquired pneumonia among adult patients at an Egyptian university hospital: bacterial etiology, susceptibility profile and evaluation of the response to initial empiric antibiotic therapy. Infect Drug Resist. 2018;11:2141–2150. doi:10.2147/IDR.S182777
22. Akil N, Muhlebach MS. Biology and management of methicillin resistant Staphylococcus aureus in cystic fibrosis. Pediat Pulmonol. 2018;53:S64–S74. doi:10.1002/ppul.24139
23. Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015;109:309–318. doi:10.1179/2047773215Y.0000000030
24. Mannaa D, Mandal AK, Sen IK, et al. Antibacterial and DNA degradation potential of silver nanoparticles synthesized via green route. Int J Biol Macromol. 2015;80:455–459. doi:10.1016/j.ijbiomac.2015.07.028
25. Alabi AS, Frielinghaus L, Kaba H, et al. Retrospective analysis of antimicrobial resistance and bacterial spectrum of infection in Gabon, central Africa. BMC Infect Dis. 2013;13:455. doi:10.1186/1471-2334-13-455
26. Nurjadi D, Friedrich-Jänicke B, Schäfer J, et al. Skin and soft tissue infections in intercontinental travellers and the import of multi-resistant Staphylococcus aureus to Europe. Clin Microbiol Infect. 2015;21:567e1–10. doi:10.1016/j.cmi.2015.01.016
27. Klein EY, Sun L, Smith DL, Laxminarayan R. The changing epidemiology of methicillin-resistant Staphylococcus aureus in the United States: a national observational study. Am J Epidemiol. 2013;177:666–674. doi:10.1093/aje/kws273
28. Santajit S, Indrawattana N. Mechanisms of antimicrobial resistance in ESKAPE pathogens. Biomed Res Int. 2016;2016:2475067. doi:10.1155/2016/2475067
29. Ansari S, Nepal HP, Gautam R, et al. Threat of drug resistant Staphylococcus aureus to health in Nepal. BMC Infect Dis. 2014;14:157. doi:10.1186/1471-2334-14-157
30. Ansari S, Nepal HP, Gautam R, et al. Staphylococcus aureus: methicillin resistance and small colony variants from pyogenic infections of skin, soft tissue and bone. J Nepal Health Res Counc. 2015;13(30):126–132.
31.
32. Najafi A. There is no escape from the ESKAPE pathogens; 2016. Available from:
33.
34. Jean -S-S, Hsueh P-R. High burden of antimicrobial resistance in Asia. Int J Antimicrob Agents. 2011;37(4):291–295. doi:10.1016/j.ijantimicag.2011.01.009
35.
36. Wojtyczka RD, Dziedzic A, Kepa M, et al. Berberine enhances the antibacterial activity of selected antibiotics against coagulase-negative staphylococcus strains in vitro. Molecules. 2014;19:6583–6596. doi:10.3390/molecules19056583
37. Tian L, Sun Z, Zhang Z. Antimicrobial resistance of pathogens causing nosocomial bloodstream infection in Hubei Province, China, from 2014 to 2016: a multicenter retrospective study. BMC Public Health. 2018;18:1121. doi:10.1186/s12889-018-6013-5
38. You JHS, Choi KW, Wong TY, et al. Disease burden, characteristics, and outcomes of methicillin-resistant Staphylococcus aureus bloodstream infection in Hong Kong. Asia Pac J Public Health. 2017;29(5):451–461. doi:10.1177/1010539517717365
39. Lim WW, Wu P, Bond HS, et al. Determinants of MRSA prevalence in the Asia Pacific Region: a systematic review and meta-analysis. J Global Antimicrobial Resist. 2018;16:17–27. doi:10.1016/j.jgar.2018.08.014
40. Gurunathan S, Han JW, Kwon DN, Kim JH. Enhanced antibacterial and antibiofilm activities of silver nanoparticles against gram-negative and gram-positive bacteria. Nanoscale Res Lett. 2014;9:373. doi:10.1186/1556-276X-9-373
41. DeLeo FR, Chambers HF. Re-emergence of antibiotic-resistant Staphylococcus aureus in the genomics era. J Clin Invest. 2009;119:2464–2474. doi:10.1172/JCI38226
42. Herigon JC, Hersh AL, Gerber JS, Zaoutis TE, Newland JG. Antibiotic management of Staphylococcus aureus infections in US children’s hospitals, 1999–2008. Pediatrics. 2010;125(6):e1294–e300. doi:10.1542/peds.2009-2867
43. Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355:666–674. doi:10.1056/NEJMoa055356
44. Mandal SM, Ghosh AK, Pati BR. Dissemination of antibiotic resistance in methicillin-resistant Staphylococcus aureus and vancomycin-resistant S. aureus strains isolated from hospital effluents. Am J Infect Control. 2015;43:e87–e8. doi:10.1016/j.ajic.2015.08.015
45. Khamash DF, Voskertchian A, Tamma PD, et al. Increasing clindamycin and trimethoprim-sulfamethoxazole resistance in pediatric Staphylococcus aureus infections. J Pediatric Infect Dis Soc. 2018;XX(XX):1–3. (Ahead of print).
46. Enstrom J, Froding I, Giske CG, et al. USA300 methicillin resistant Staphylococcus aureus in Stockholm, Sweden, from 2008 to 2016. PLoS One. 2018;13(11):e0205761. doi:10.1371/journal.pone.0205761
47. George M, Iramiot JS, Muhindo R, Olupot-Olupot P, Nanteza A. Bacterial aetiology and antibiotic susceptibility profile of post-operative sepsis among surgical patients in a tertiary hospital in rural Eastern Uganda. Microbiol Res J Int. 2018;24(2):1–8. doi:10.9734/MRJI
48. Sutter DE, Milburn E, Chukwuma U, Dzialowy N, Maranich AM, Hospenthal DR. Changing susceptibility of Staphylococcus aureus in a US pediatric population. Pediatrics. 2016;137:e20153099. doi:10.1542/peds.2015-3099
49. Acree ME, Morgan E, David MZ. Staphylococcus aureus infections in Chicago, 2006–2014: increase in CA-MSSA and decrease in MRSA incidence. Infect Control Hosp Epidemiol. 2017;38:1226–1234. doi:10.1017/ice.2017.177
50. O’Neill J. Tackling drug-resistant infections globally: final report and recommendations. Rev Antimicrob Resist. 2016;84.
51. David MZ, Daum RS. Treatment of Staphylococcus aureus infections. Curr Top Microbiol Immunol. 2017;409:325–383. doi:10.1007/82_2017_42
52. Leong HN, Kurup A, Tan MY, et al. Management of complicated skin and soft tissue infections with a special focus on the role of newer antibiotics. Infect Drug Resist. 2018;11:1959–1974. doi:10.2147/IDR.S172366
53. Tang J, Hu J, Kang L, Deng Z, Wu J, Pan J. The use of vancomycin in the treatment of adult patients with methicillin-resistant Staphylococcus aureus (MRSA) infection: a survey in a tertiary hospital in China. Int J Clin Exp Med. 2015;8(10):19436–19441.
54. Goswami NN, Trivedi HR, Goswami APP, Patel TK, Tripathi CB. Antibiotic sensitivity profile of bacterial pathogens in postoperative wound infections at a tertiary care hospital in Gujarat, India. J Pharmacol Pharmacother. 2011;2:158–164. doi:10.4103/0976-500X.83279
55. Rayner CR, Forrest A, Meagher AK, Birmingham MC, Schentag JJ. Clinical pharmacodynamics of linezolid in seriously ill patients treated in a compassionate use programme. Clin Pharmacokinet. 2003;42(15):1411–1423. doi:10.2165/00003088-200342150-00007
56. Natsumoto B, Yokota K, Omata F, Furukawa K. Risk factors for linezolid-associated thrombocytopenia in adult patients. Infection. 2014;42(6):1007–1012. doi:10.1007/s15010-014-0674-5
57. Lee CH, Wang MC, Huang IW, Chen FJ, Lauderdale TL. Development of daptomycin non susceptibility with heterogeneous vancomycin-intermediate resistance and oxacillin susceptibility in methicillin resistant Staphylococcus aureus during high-dose daptomycin treatment. Antimicrob Agents Chemother. 2010;54:4038–4040. doi:10.1128/AAC.00533-10
58. Sabat AJ, Tinelli M, Grundmann H, et al. Daptomycin resistant Staphylococcus aureus clinical strain with novel non-synonymous mutations in the mprF and vraS genes: A new insight into daptomycin resistance. Front Microbiol. 2018;9:2705. doi:10.3389/fmicb.2018.02705
59.
60. Andersson DI, Hughes D, Kubicek-Sutherland JZ. Mechanisms and consequences of bacterial resistance to antimicrobial peptides. Drug Resist Updates. 2016;26:43–57. doi:10.1016/j.drup.2016.04.002
61. Guilhelmelli F, Vilela N, Albuquerque P, Derengowski LdS, Silva-Pereira I, Kyaw CM. Antibiotic development challenges: the various mechanisms of action of antimicrobial peptides and of bacterial resistance. Front Microbiol. 2013;4:353. doi:10.3389/fmicb.2013.00077
62. Brogden KA. Antimicrobial peptides: pore formers or metabolic inhibitors in bacteria? Nat Rev Microbiol. 2005;3(3):238–250. doi:10.1038/nrmicro1098
63. Taheri B, Mohammadi M, Nabipour I, Momenzadeh N, Roozbehani M, Bhunia A. Identification of novel antimicrobial peptide from Asian sea bass (lates calcarifer) by in silico and activity characterization. PLoS One. 2018;13(10):e0206578. doi:10.1371/journal.pone.0206578
64. Sanches PRS, Carneiro BM, Batista MN, et al. A conjugate of the lytic peptide hecate and gallic acid: structure, activity against cervical cancer, and toxicity. Amino Acids. 2015;47(7):1433–1443. doi:10.1007/s00726-015-1980-7
65. Jelinkova P, Splichal Z, Jimenez AMJ, et al. Novel vancomycin-peptide conjugate as potent antibacterial agent against vancomycin-resistant. Infect Drug Resist 2018;11:1807–1817. doi:10.2147/IDR.S160975
66. Leszczyńska K, Namiot A, Janmey PA, Bucki R. Modulation of exogenous antibiotic activity by host cathelicidin LL-37. APMIS. 2010;118:830–836. doi:10.1111/j.1600-0463.2010.02667.x
67. Koppen BC, Mulder PPG, de Boer L, et al. Synergistic microbicidal effect of cationic antimicrobial peptides and teicoplanin against planktonic and biofilm-encased Staphylococcus aureus. Int J Antimicrob Agents. 2019;53(2):143–151. doi:10.1016/j.ijantimicag.2018.10.002
68. Hostettman K, Hostettman M. Methods in plant biochemistry, in plant phenolics, ed. P. M. Dey and J. B. Harbone. 1989;1:493.
69. Roberts JC. Naturally occurring xanthones. Chem Rev. 1961;61(6):591–605. doi:10.1021/cr60214a003
70. Gales L, Damas AM. Xanthones-a structural perspective. Curr Med Chem. 2005;12(21):2499–2515.
71. Pinto MM, Sousa ME, Nascimento MS. Xanthone derivatives: new insights in biological activities. Curr Med Chem. 2005;12(21):2517–2538.
72. Na Y. Recent cancer drug development with xanthone structures. J Pharm Pharmacol. 2009;61(6):707–712. doi:10.1211/jpp/61.06.0002
73. Panda SS, Chand M, Sakuja R, Jain SC. Xanthones as potential antioxidants. Curr Med Chem. 2013;20(36):4481–4507.
74. Chen X, Leng J, Rakesh KP, et al. Synthesis and molecular docking studies of xanthone attached amino acids as potential antimicrobial and anti-inflammatory agents. Med Chem Commun. 2017;8:1706–1719. doi:10.1039/C7MD00209B
75. Miklasinska-Majdanik M, Kepa M, Wojtyczka RD, et al. Phenolic compounds diminish antibiotic resistance of Staphylococcus aureus clinical strains. Int J Environ Res Public Health. 2018;15:E2321. doi:10.3390/ijerph15061188
76. Shi SF, Jia JF, Guo XK, et al. Reduced Staphylococcus aureus biofilm formation in the presence of chitosan-coated iron oxide nanoparticles. Int J Nanomed. 2017;11:6499–6506. doi:10.2147/IJN.S41371
77. Morones JR, Elechiguerra JL, Camacho A, Ramirez JT. The bactericidal effect of silver nanoparticles. Nanotechnol. 2005;16:2346–2353. doi:10.1088/0957-4484/16/10/059
78. Rai M, Yadav A, Gade A. Silver nanoparticles as a new generation of antimicrobials. Biotechnol Adv. 2008;27:76–83. doi:10.1016/j.biotechadv.2008.09.002
79. Duran N, Marcato P, De Conti R, Alves O. Potential use of silver nanoparticles on pathogenic bacteria, their toxicity and possible mechanisms of action. J Braz Chem Soc. 2010;21:949. doi:10.1590/S0103-50532010000600002
80. Ruden S, Hilpert K, Berditsch M, Wadhwani P, Ulrich A. Synergistic interaction between silver nanoparticles and membrane-permeabilizing antimicrobial peptides. Antimicrob Agents Chemother. 2009;53:3538. doi:10.1128/AAC.01106-08
81. Kora AJ, Rastogi L. Enhancement of antibacterial activity of capped silver nanoparticles in combination with antibiotics, on model gram-negative and gram-positive bacteria. Bioinorg Chem Appl. 2013;2013:871097. doi:10.1155/2013/871097
82. Thirumurugan G, Rao S, Dhanaraju M. Elucidating pharmacodynamics interaction of silver nanoparticle-topical deliverable antibiotics. Sci Rep. 2016;6:29982. doi:10.1038/srep29982
83. Rahim K, Mohamed A. Bactericidal and antibiotic 241 synergistic effect of nanosilver against methicillin-resistant Staphylococcus aureus. Jundishapur J Microbiol. 2015;8:11.
84. Das P, Saulnier E, Carlucci C, Allen-Vercoe E, Shah V, Walker VK. Interaction between a broad-spectrum antibiotic and silver nanoparticles in a human gut ecosystem. J Nanomed Nanotechnol. 2016;7(5):1000408.
85. Surwade P, Ghildyal C, Weikel C, et al. Augmented antibacterial activity of ampicillin with silver nanoparticles against methicillin-resistant Staphylococcus aureus (MRSA). J Antibiotics. 2019;72(1):50–53. doi:10.1038/s41429-018-0111-6
86. Manukumar HM, Chandrasekhar B, Rakesh KP, et al. Novel T-C@AgNPs mediated biocidal mechanism against biofilm associated methicillin-resistant Staphylococcus aureus (Bap-MRSA) 090, cytotoxicity and its molecular docking studies. Med Chem Commun. 2017;8:2181–2194. doi:10.1039/C7MD00486A
87. Xu Z, Manukumar HM, Rakesh KP, et al. Role of BP*C@AgNPs in Bap-dependent multicellular behavior of clinically important methicillin-resistant Staphylococcus aureus (MRSA) biofilm adherence: a key virulence study. Microb Pathog. 2018;123:275–284. doi:10.1016/j.micpath.2018.07.025
88. O’Brien EC, McLoughlin RM. Considering the ‘alternatives’ for next-generation anti-Staphylococcus aureus Vaccine Development. Trends in Mol Med. 2019;25(3):S1471–4914.
89. Willis LM, Whitfield C. Structure, biosynthesis, and function of bacterial capsular polysaccharides synthesized by ABC transporter-dependent pathways. Carbohydr Res. 2013;378:35–44. doi:10.1016/j.carres.2013.05.007
90. Trotter CL, McVernon J, Ramsay ME, et al. Optimising the use of conjugate vaccines to prevent disease caused by Haemophilus influenzae type b, Neisseria meningitidis and Streptococcus pneumoniae. Vaccine. 2008;26:4434–4445. doi:10.1016/j.vaccine.2008.05.073
91. O’Riordan K, Lee JC. Staphylococcus aureus capsular polysaccharides. Clin Microbiol Rev. 2004;17:218–234.
92. Cocchiaro JL, Gomez MI, Risley A, Solinga R, Sordelli DO, Lee JC. Molecular characterization of the capsule locus from non-typeable Staphylococcus aureus. Mol Microbiol. 2006;59:948–960. doi:10.1111/j.1365-2958.2005.04978.x
93. Arbeit RD, Karakawa WW, Vann WF, Robbins JB. Predominance of two newly described capsular polysaccharide types among clinical isolates of Staphylococcus aureus. Diagn Microbiol Infect Dis. 1984;2:85–91.
94. Hochkeppel HK, Braun DG, Vischer W, et al. Serotyping and electron microscopy studies of Staphylococcus aureus clinical isolates with monoclonal antibodies to capsular polysaccharide types 5 and 8. J Clin Microbiol. 1987;25:526–530.
95. Nanra JS, Timofeyeva Y, Buitrago SM, et al. Heterogeneous in vivo expression of clumping factor A and capsular polysaccharide by Staphylococcus aureus: implications for vaccine design. Vaccine. 2009;27:3276–3280. doi:10.1016/j.vaccine.2009.01.062
96. Shinefield H, Black S, Fattom A, et al. Use of a Staphylococcus aureus conjugate vaccine in patients receiving hemodialysis. N Engl J Med. 2002;346:491–496. doi:10.1056/NEJMoa011297
97. Fattom A, Matalon A, Buerkert J, et al. Efficacy profile of a bivalent Staphylococcus aureus glycoconjugated vaccine in adults on hemodialysis: phase III randomized study. HumVaccin ImmunoTher. 2015;11:632–641.
98. Rozemeijer W, Fink P, Rojas E, et al. Evaluation of approaches to monitor Staphylococcus aureus virulence factor expression during human disease. PLoS One. 2015;10(2):e0116945. doi:10.1371/journal.pone.0116945
99. Begier E, Seiden DJ, Patton M, et al. SA4Ag, a 4-antigen Staphylococcus aureus vaccine, rapidly induces high levels of bacteria-killing antibodies. Vaccine. 2017;35(8):1132–1139. doi:10.1016/j.vaccine.2017.01.024
100. Frenck RJ, Creech CB, Sheldon EA, et al. Safety, tolerability, and immunogenicity of a 4-antigen Staphylococcus aureus vaccine (SA4Ag): results from a first-in-human randomised, placebo-controlled phase 1/2 study. Vaccine. 2017;35(2):375–384. doi:10.1016/j.vaccine.2016.11.010
101. Creech CB, Frenck RJ, Sheldon EA, et al. Safety, tolerability, and immunogenicity of a single dose 4-antigen or 3-antigen Staphylococcus aureus vaccine in healthy older adults: results of a randomised trial. Vaccine. 2017;35(2):385–394. doi:10.1016/j.vaccine.2016.11.032
102. Marshall H, Nissen M, Richmond P, et al. Safety and immunogenicity of a booster dose of a 3-antigen Staphylococcus aureus vaccine (SA3Ag) in healthy adults: A randomized phase 1 study. J Infect. 2016;73(5):437–454. doi:10.1016/j.jinf.2016.08.004
103. Nissen M, Marshall H, Richmond P, et al. A randomized phase I study of the safety and immunogenicity of three ascending dose levels of a 3-antigen Staphylococcus aureus vaccine (SA3Ag) in healthy adults. Vaccine. 2015;33(15):1846–1854. doi:10.1016/j.vaccine.2015.02.024
104. Fowler VG, Allen KB, Moreira ED, et al. Effect of an investigational vaccine for preventing Staphylococcus aureus infections after cardiothoracic surgery: a randomized trial. J Am Med Assoc. 2013;309(13):1368–1378. doi:10.1001/jama.2013.3010
105. Xu X, Zhu H, Lv H. Safety of Staphylococcus aureus four-antigen and three-antigen vaccines in healthy adults: a meta-analysis of randomized controlled trials. Hum Vaccin Immunother. 2018;14(2):314–321. doi:10.1080/21645515.2017.1395540
106. Dupont CD, Scully IL, Zimnisky RM, et al. Two vaccines for Staphylococcus aureus induce a B-cell mediated immune response. mSphere. 2018;3:e00217–e18. doi:10.1128/mSphere.00217-18
107. Frenck RW
108. Jansen KU, Knirsch C, Anderson AS. The role of vaccines in preventing bacterial antimicrobial resistance. Nat Med. 2018;24:10–20. doi:10.1038/nm.4465
109. Mohamed N, Wang MY, Le Huec JC, et al. Vaccine development to prevent Staphylococcus aureus surgical-site infections. Br J Surgery. 2017;104:e41–e54. doi:10.1002/bjs.10454
110. Berube BJ, Bubeck Wardenburg J. Staphylococcus aureus alpha-toxin: nearly a century of intrigue. Toxins. 2013;5:1140–1166.
111. Genestier AL, Michallet MC, Prevost G, et al. Staphylococcus aureus Panton-Valentine LEUKOCIDIN directly targets mitochondria and induces bax-independent apoptosis of human neutrophils. J Clin Invest. 2005;115:3117–3127. doi:10.1172/JCI22684
112. Adhikari RP, Ajao AO, Aman MJ, et al. Lower antibody levels to Staphylococcus aureus exotoxins are associated with sepsis in hospitalized adults with invasive S. aureus infections. J Infect Dis. 2012;206:915–923. doi:10.1093/infdis/jis462
113. Landrum ML, Lalani T, Niknian M, et al. Safety and immunogenicity of a recombinant Staphylococcus aureus alpha-toxoid and a recombinant Panton-Valentine leukocidin subunit, in healthy adults. Hum Vaccin Immunother. 2017;13(4):791–801. doi:10.1080/21645515.2016.1248326
114. Korea CG, Balsamo G, Pezzicoli A, et al. Staphylococcal Esx proteins modulate apoptosis and release of intracellular Staphylococcus aureus during infection in epithelial cells. Infect Immun. 2014;82(10):4144–4153. doi:10.1128/IAI.01576-14
115. Burts ML, Williams WA, DeBord K, Missiakas DM. EsxA and EsxB are secreted by an ESAT-6-like system that is required for the pathogenesis of Staphylococcus aureus infections. Proc Natl Acad Sci U S A. 2005;102(4):1169–1174. doi:10.1073/pnas.0405620102
116. Xu C, Zhang B-Z, Lin Q, et al. Live attenuated Salmonella typhimurium vaccines delivering SaEsxA and SaEsxB via type III secretion system confer protection against Staphylococcus aureus infection. BMC Infect Dis. 2018;18:195. doi:10.1186/s12879-018-3104-y
117. Parker D, Prince A. Immunopathogenesis of Staphylococcus aureus pulmonary infection. Semin Immunopathol. 2012;34:281–297. doi:10.1007/s00281-011-0291-7
118. Becker S, Frankel MB, Schneewind O, Missiakas D. Release of protein A from the cell wall of Staphylococcus aureus Proc Natl Acad Sci USA. 2014;111:1574–1579. doi:10.1073/pnas.1317181111
119. Pauli NT, Kim HK, Falugi F, et al. Staphylococcus aureus infection induces protein A-mediated immune evasion in humans. J Exp Med. 2014;211:2331–2339. doi:10.1084/jem.20141404
120. Kim HK, Cheng AG, Kim HY, Missiakas DM, Schneewind O. Nontoxigenic protein A vaccine for methicillin-resistant Staphylococcus aureus infections. J Exp Med. 2010;207:1863–1870. doi:10.1084/jem.20092514
121. Yang Y, Yu R, Yang X, et al. Protection against Staphylococcus aureus and tetanus infections by a combined vaccine containing SasA and TeNT-Hc in mice. Mol Med Rep. 2017;15:2369–2373. doi:10.3892/mmr.2017.6227
122. Cava F, Lam H, de Pedro MA, Waldor MK. Emerging knowledge of regulatory roles of D-amino acids in bacteria. Cell Mol Life Sci. 2011;68:817–831. doi:10.1007/s00018-010-0571-8
123. Moscoso M, Garcıa P, Cabral MP, Rumbo C, Bou G. A D-Alanine auxotrophic live vaccine is effective against lethal infection caused by Staphylococcus aureus. Virulence. 2018;9(1):604–620. doi:10.1080/21505594.2017.1417723
124. Zhang B-Z, Cai J, Yu B, et al. Immunotherapy targeting adenosine synthase a decreases severity of Staphylococcus aureus infection in mouse model. J Infect Dis. 2017;216:245–253. doi:10.1093/infdis/jix290
125. Mcadow M, Dedent AC, Emolo C, et al. Coagulases as determinants of protective immune responses against Staphylococcus aureus. Infect Immun. 2012;80:3389e98. doi:10.1128/IAI.06224-11
126. Pozzi C, Bagnoli F, Rappuoli R. Staphylococcus aureus coagulase R domain, a new evasion mechanism and vaccine target. J Exp Med. 2016;213:292. doi:10.1084/jem.20151916
127. Guggenberger C, Wolz C, Morrissey JA, Heesemann J. Two distinct coagulase dependent barriers protect Staphylococcus aureus from neutrophils in a three dimensional in vitro infection model. PLoS Pathog. 2012;8:e1002434. doi:10.1371/journal.ppat.1002434
128. Qian M, Zhao T, Li R, et al. Targeting the R domain of coagulase by active vaccination protects mice against lethal Staphylococcus aureus infection. Microbes Infect. 2018:S1286–4579. (18)30177-1.
129. Krakauer T, Pradhan K, Stiles BG. Staphylococcal superantigens spark host-mediated danger signals. Front Immunol. 2016;7:23. doi:10.3389/fimmu.2016.00023
130. Kulhankova K, King J, Salgado-Pabon W. Staphylococcal toxic shock syndrome: superantigen-mediated enhancement of endotoxin shock and adaptive immune suppression. Immunol Res. 2014;59:182–187. doi:10.1007/s12026-014-8538-8
131. Mantis NJ. Vaccines against the category B toxins: staphylococcal enterotoxin B, epsilon toxin and ricin. Adv Drug Deliv Rev. 2005;57:1424e1439. doi:10.1016/j.addr.2005.01.017
132. Choi JY, Shin S, Kim NY, et al. A novel staphylococcal enterotoxin B subunit vaccine candidate elicits protective immune response in a mouse model. Toxicon. 2017;131:68–77. doi:10.1016/j.toxicon.2017.03.012
133. Tkaczyk C, Hua L, Varkey R, et al. Identification of anti-alpha toxin mAbs that reduce severity of Staphylococcus aureus dermonecrosis and exhibit a correlation between affinity and potency. Clin Vaccine Immunol. 2012;19:377–385. doi:10.1128/CVI.05589-11
134. Kennedy AD, Bubeck Wardenburg J, Gardner DJ, et al. Targeting of alpha-hemolysin by active or passive immunization decreases severity of USA300 skin infection in a mouse model. J Infect Dis. 2010;202:1050–1058. doi:10.1086/656043
135. Ragle BE, Bubeck Wardenburg J. Anti-alpha-hemolysin monoclonal antibodies mediate protection against Staphylococcus aureus pneumonia. Infect Immun. 2009;77:2712–2718. doi:10.1128/IAI.00115-09
136. Cheung GY, Otto M. The potential use of toxin antibodies as a strategy for controlling acute Staphylococcus aureus infections. Expert Opin Ther Targets. 2012;16(6):601–612. doi:10.1517/14728222.2012.682573
137. Varshney AK, Kuzmicheva GA, Lin J, et al. A natural human monoclonal antibody targeting Staphylococcus Protein A protects against Staphylococcus aureus bacteremia. PLoS One. 2018;13(1):e0190537. doi:10.1371/journal.pone.0190537
138. Kalali Y, Haghighat S, Mahdavi M. Passive immunotherapy with specific IgG fraction against autolysin: analogous protectivity in the MRSA infection with antibiotic therapy. Immunol Lett. 2018;S0165–2478. (18)30132-9.
139. Diep BA, Le VTM, Visram ZC, et al. Improved protection in a rabbit model of community-associated methicillin-resistant Staphylococcus aureus necrotizing pneumonia upon neutralization of leukocidins in addition to alpha-hemolysin. Antimicrob Agents Chemother. 2016;60(10):6333–6340. doi:10.1128/AAC.01213-16
140. Stulik L, Rouha H, Labrousse D, et al. Preventing lung pathology and mortality in rabbit Staphylococcus aureus pneumonia models with cytotoxin-neutralizing monoclonal IgGs penetrating the epithelial lining fluid. Sci Rep. 2019;9:5339. doi:10.1038/s41598-019-41826-6
141. Haghighat S, Siadat SD, Rezayat Sorkhabadi SM, et al. Recombinant PBP2a as a vaccine candidate against methicillin-resistant Staphylococcus aureus: immunogenicity and protectivity. Microb Pathog. 2017;108:32–39. doi:10.1016/j.micpath.2017.04.037
142. Naghshbandi RZ, Haghighat S, Mahdavi M. Passive immunization against methicillin resistant Staphylococcus aureus recombinant PBP2a in sepsis model of mice: comparable results with antibiotic therapy. Int Immunopharmacol. 2018;56:186–192. doi:10.1016/j.intimp.2018.01.035
143. Gerlach D, Guo Y, De Castro C, et al. Methicillin-resistant Staphylococcus aureus alters cell wall glycosylation to evade immunity. Nature. 2018;563(7733):705–709. doi:10.1038/s41586-018-0730-x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.