")
Back to Journals » International Journal of Nanomedicine » Volume 18
Recent Advances in Nano-Drug Delivery Systems for the Treatment of Diabetic Wound Healing
Authors Liu M , Wei X, Zheng Z, Li Y, Li M , Lin J, Yang L
Received 12 December 2022
Accepted for publication 14 March 2023
Published 27 March 2023 Volume 2023:18 Pages 1537—1560
DOI https://doi.org/10.2147/IJN.S395438
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Anderson Oliveira Lobo
Mengqian Liu, Xuerong Wei, Zijun Zheng, Yicheng Li, Mengyao Li, Jiabao Lin, Lei Yang
Department of Burns, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China
Correspondence: Lei Yang, Department of Burns, Nanfang Hospital, Southern Medical University, Jingxi Street, Baiyun District, Guangzhou, 510515, People’s Republic of China, Tel +86-20-6164-1841, Email [email protected]
Abstract: Diabetes mellitus (DM) induced wound healing impairment remains a serious health problem and burden on the clinical obligation for high amputation rates. Based on the features of wound microenvironment, biomaterials loading specific drugs can benefit diabetic wound treatment. Drug delivery systems (DDSs) can carry diverse functional substances to the wound site. Nano-drug delivery systems (NDDSs), benefiting from their features related to nano size, overcome limitations of conventional DDSs application and are considered as a developing process in the wound treatment field. Recently, a number of finely designed nanocarriers efficiently loading various substances (bioactive and non-bioactive factors) have emerged to circumvent constraints faced by traditional DDSs. This review describes various recent advances of nano-drug delivery systems involved in mitigating diabetes mellitus-based non-healing wounds.
Keywords: drug delivery system, nanotechnology, diabetic wound healing, nanoparticles
Introduction
Diabetes mellitus (DM) is a complex chronic metabolic disease. Currently, over 300 million people suffer from DM, with an increasingprevalence in the upcoming years.1,2 Diabetic patients in high glucose conditions always bear many secondary complications, and diabetic foot ulceration (DFU) is a frequently recognized complication, which increases amputation rates, and shortens lifespans.3,4 Many therapeutics have been applied in diabetic non-healing wounds, such as hyperbaric oxygen therapy (HBO) and smart wound dressings.5 Diabetic wounds are heterogeneous, so the treatment and outcome depend very much on precise strategies.6 Most of the current treatments are inadequate and incur a massive financial burden to the patient. Therefore, the discovery of new therapeutic methods for diabetic wound healing is urgently required.
A drug delivery system that delivers therapeutic molecules in a sustained release manner could be a promising method of improving diabetic wound healing. These advanced systems can control drug release over a long time period, maintain drug concentration and release drugs in a target site. Nevertheless, conventional drug delivery systems are not always designed optimally for various drugs and inadequate to protect drugs from probable degradation, which causes the waste of a large number of drugs.
Current developments of nanotechnology benefit the design and fabrication of drug delivery systems for diabetic wound healing.7 With various nanostructures, such as liposomes, nanoparticles, nanofibers and nano hydrogels, these nano-drug delivery systems are being studied to provide better drug performances and achieve maximum drug encapsulation efficiency. Since NDDSs loading various carriers exhibit anti-inflammatory action, ROS scavenging, reduction of local blood sugar levels and senescence cell clearance, their applications in diabetic wound treatment are receiving increasing attention.8–10 A polycaprolactone (PCL)-based nanofiber has been fabricated to generate oxygen and stimulate angiogenesis to improve diabetic wound healing.11 A Methacrylate Gelatin (GelMA) hydrogel based patch carrying NO has been designed to accelerate diabetic wound healing.12 many other studies have also been reported to explore the utilization of NDDSs in the field of diabetic wound healing.
In general, the reviews currently published on nano-drug delivery systems describe their unique properties and novel fabrication technology. They give general insight into the application of nanomaterials in the wound healing field; nevertheless, information about the application in specific wounds such as diabetic wounds is currently limited. In this review, we cover all recent nano-scale drug delivery systems used for diabetic wound treatment. Additionally, it details the major substances loaded in these nanocarriers and their function in accelerating diabetic wound healing, which would help in selecting suitable drugs to meet the need of different diabetic wound conditions.
Wound Healing Pathophysiology
Normal Wound Healing
Wound healing is a complex and stepwise process and involves many different cell types releasing cytokines and growth factors (GFs). The healing process is divided into the following overlapping stages: hemostasis, inflammation, proliferation and remodeling (Figure 1).13–15
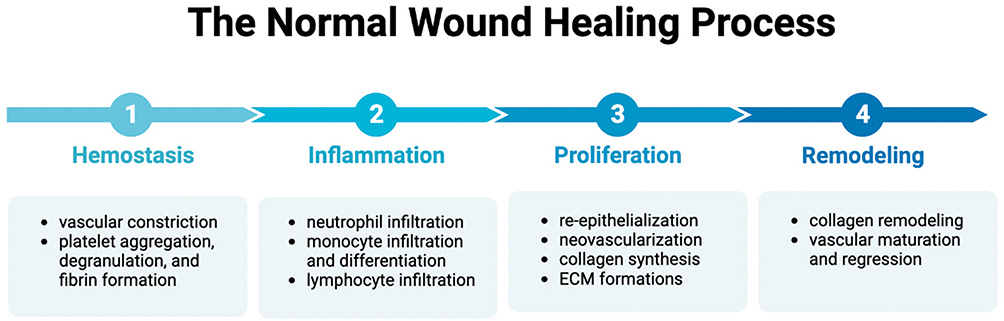 |
Figure 1 The physiological process of normal wounds. (figure was created with BioRender.com). |
Fibrin plug formation can block bacteria and provide immediate coverage in the wound area.15 Platelets aggregate and release proinflammatory mediators such as growth factor, cytokines and chemokines. These mediators can recruit neutrophils and monocytes to the wound area, which support the armamentarium for the inflammatory period.16
The inflammation phase occurs immediately after injury and the focus of this phase is on destroying bacteria and removing debris.17 This phase usually lasts four to six days, while in some pathological conditions (e.g., diabetic foot ulcers), it can last for weeks or even months. Cell recruitment and chemotaxis (the movement of an organism in response to a chemical stimulus) are key events in this phase. These cells have various functions. Increasing endothelial expression of selectins slows down blood cells (e.g., leucocytes) and binding to integrins to help their adhesion. Neutrophils and macrophages are involved in wound debridement, which also fuels the healing process by releasing cytokines, GFs and other mediators.18 Circulating monocytes convert to tissue macrophages to aid wound contraction in the begin of granulation tissue formation.19
The proliferation phase focuses on filling and covering the wound site, and it includes four distinct stages: re-epithelialization, neovascularization, collagen synthesis and extracellular matrix (ECM) formations.20 This phase often lasts for a few weeks. Granulation tissue formation is essential for wound contraction, and fibroblasts, endothelial cells and keratinocytes are the most prominent cell types present and support the formation of granulation tissue, which is an essential component of contraction.21 Physical contraction mediated by myofibroblasts also plays an important role in achieving wound closure.22 Cross-talk between integrins, cells, cytokines and matrix metalloprotein (MMP) promotes cell migration and ECM production.
In the tissue remodeling phase, tissue slowly gains strength and flexibility. In this phase, many newly formed capillaries subside, normalizing the vascular density of the wound site. To achieve proper tensile strength, ECM is reshaped to a structure that approaches normal tissue.23 Gradually, the immature collagen (type lll) is converted into the more stable collagen type l, and the ratio of type III and type I decreases. Collagen forms tight cross-links with collagen and other protein molecules and deposits in a physiological alignment.24,25 This phase is relatively long, usually lasting 21 days to 1 year.
Diabetic Wound Healing
Under diabetic pathological conditions, the orderly and reliable healing process is disturbed and the wound becomes a chronic wound.2,26 Some parts of the chronic condition may get stuck at different stages, losing the ideal synchrony of healing progression that leads to rapid healing.27 There are intrinsic pathobiological abnormalities and extrinsic factors that contribute to the occurrence of a diabetic wound (Figure 2).
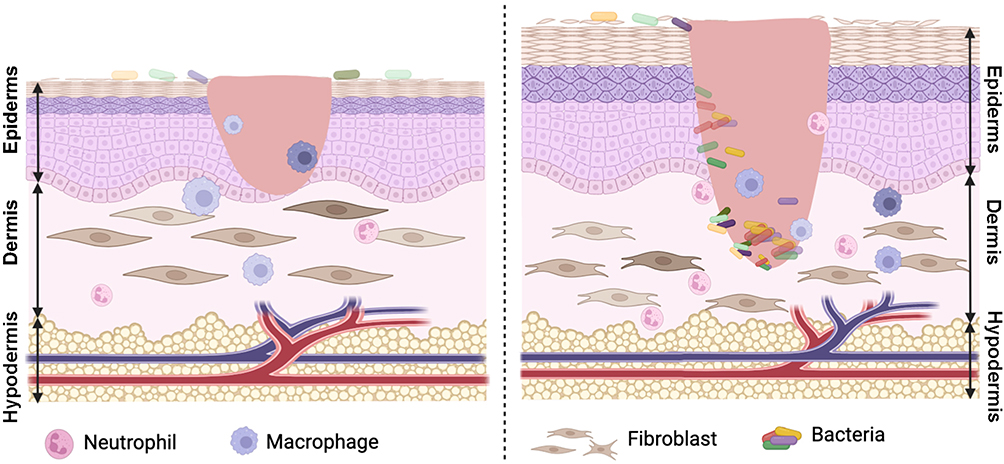 |
Figure 2 The pathophysiological processes of wound healing and diabetic wound healing. (figure was created with BioRender.com). |
Hypoxia is a major factor that causes a non-healing wound.28,29 In addition to inadequate oxygen supply, a prolonged inflammation phase causes high oxygen consumption of wound cells.30 Diabetic neuropathy (DN) is the most common complication of diabetes, and patients with an injured nerve system are more likely to develop diabetic foot ulcers. DN presents a variety of manifestations, which include segmental demyelination, degradation of peripheral neuron axons, poor nerve conduction and nutrient supply, culminating in dry skin and gangrene.31 Without pain perception, the patient is unable to feel the injury site, consequently increasing the risk of infection and enlargement of the wound. Vasculopathy and endothelial cell abnormalities, together with neuropathy, cause limited oxygen support to the wound area.32 Additional nerve damage, diminished pain sensation and insufficient blood supply can amplify the disorder of the diabetic foot microenvironment. Wound healing mediators can be influenced by high blood levels. The M2 type macrophage polarization is disturbed, the keratinocyte migration is reduced, and the re-epithelialization stage is stagnant.33 Recent works revealed that a prolonged inflammatory phase is an iconic feature of diabetic chronic wounds. With impaired phagocytic function, excess macrophages infiltrate the wound site and influence MMPs regulation, which blocks deposition of intact, healthy collagen and formation of ECM.34
Current Diabetic Wound Treatment
Debridement
Debridement involves removing foreign debris, blood clots and the inactivated or infected tissue from a wound bed.35 The applied methods of debridement include surgery, wet-to-dry dressings, and enzymatic method.36 Sharp debridement has been well acknowledged as the gold standard for diabetic wounds, and it is reported that callus removal can rapidly reduce pressure by 30%.37 Although debridement has been found to be efficacious in several clinical trials, its limitations such as unacceptable pain and potential of second trauma are still a concern.38
Wound Dressings
Wound dressings are traditional elements of wound care, including natural, modified or synthetic materials and therapeutic substances. Diabetic wounds are heterogenous, and there is no single dressing that has been reported to be ideal for all wound types.39 An ideal wound dressing should provide a moist environment that promotes granulation, revascularization, keratinocyte migration and tissue regeneration.40 It is a substantial challenge to develop an efficient wound dressing, and many dressings has been created with novel bioengineering technology. However, current designed dressings face various problems, such as cellular toxicity, allergic reactions, decreased angiogenesis and physiological rejection.
Pressure Off-Loading
Pressure off-loading is a widely used treatment for patients with DFUs.41 The treatment can be distinguished in non-removable, removable and surgical interventions.42 Several prospective controlled studies have shown that non-removable, pressure off-loading casts are more effective, and a combination with surgical interventions (e.g., Achilles tendon lengthening) can achieve more successful outcomes.43
Revascularization
Peripheral arterial disease (PAD) is the most common early-onset cardiovascular complication of diabetes. PAD is also one of the strongest predictors of developing chronic wound and increasing risk of dying from cardiovascular disease. It has been reported that PAD occurs in 40% of patients with DFUs.44 One of the most common treatments of PAD is revascularization. Both pharmaceutical methods and surgical technologies (angioplasty, endarterectomy, grafting or bypass) can be performed to achieve revascularization.
Treatment of Wound Infection
Infection is common in wound healing progress, especially in diabetic patients. Antimicrobial therapy is a common method of wound infection, but it is not always necessary and does not apply in clinically uninfected wounds.45 Treatment of diabetic wound infection has been outlined by the IDSA, which recommends treatment of wounds with two or more signs or symptoms of inflammation (erythema, fever, tenderness, pain and induration) or purulent discharge.46 Due to antibacterial resistance and improper use of antibiotics, treatment of DFU infection can have adverse outcomes. The strategy of applying narrow spectrum antibiotics within a short period can reduce healing time and amputation rate. Besides oral or intravenous administration of antibiotics, nanomaterial-based systems have emerged as a promising method for antibiotic delivery, which improve therapeutic index and avoid antibacterial resistance.47
General Measures
In addition to medication and surgical treatment, good glycemic control is a very important general therapeutic method for DFU. Patients should also pay attention to normalization of blood indicators, the management of blood fat, drinking and smoking cessation and diet control.48 Since hyperglycemia plays the most important role in DM pathology, good blood sugar control can not only have a positive effect on DFU outcomes but also delay the onset of other complications of diabetes.49 Also, several observational studies have found that there is a linear correlation between appropriate nutrition supplement and DFU prognosis.50
Substances
The pathological process of diabetic wound healing includes complex changes and some key factors associated with successful healing are in disorder. Thus, various substances should be applied to support this progress. Substances loaded in NDDSs for diabetic wound healing can be classified into two categories: bioactive molecules and non-bioactive substances.
Bioactive Molecules
Growth Factors
Growth factors are multi-functional polypeptides, which bind to specific, high-affinity cell membrane receptors to mediate, coordinate and control cellular interactions.51 Growth factors can stimulate cell proliferation and differentiation to benefit overlapping phases of wound healing and accelerate this process.52 The transforming growth factor (TGF-β) superfamily has mainly three isoforms, TGF-β1, β2 and β3, and TGF-β1 has been recognized as a key modulator of cutaneous wound healing. Preclinical studies showed that low expressions of TGF-β1 and TGF-β2 reduced scar formation and improved dermal architecture.53 The vascular endothelial growth factor (VEGF) acts as a signaling mediator in neovascularization.54 By interacting with VEGF receptors (VEGFR) to stimulate downstream signaling cascades, VEGF controls fibroblasts and endothelial cells function and promotes their proliferation.55 The platelet-derived growth factor (PDGF), mainly secreted from platelets, mediates wound healing throughout all phases. PDGF targets dermal fibroblasts and many other cells to promote collagen synthesis and dermal regeneration. The epidermal growth factor (EGF) activates downstream signaling pathways and induces cell migration and proliferation. EGF interacts with keratinocytes to promote their migration, which is crucial for the re-epithelialization process.56 The fibroblast growth factor (FGF) can promote endothelial cell migration and smooth muscle cell proliferation. Among the subfamilies of FGF, FGF2 has been applied for scarless wound healing.57
An impaired balance of many growth factors and disturbance of various cellular responses mediated by GFs have been reported in chronic non-healing wounds.58 Therefore, locally applying exogenous growth factors can achieve positive outcomes of wound injury treatment.59 There are medications containing recombinant human EGF (rhEGF) that are commercially available and have been used in clinical treatment, such as Heberprot-P®,60 Regen-D™ 150, and Easyef®.61 Many studies have suggested that the function of GFs is spatially related,62 however conventional systems lack the ability to control the release of GFs spatially and temporally. Currently, various sophisticated delivery systems for delivery growth factors have been reported for diabetic wounds (Table 1).63–70
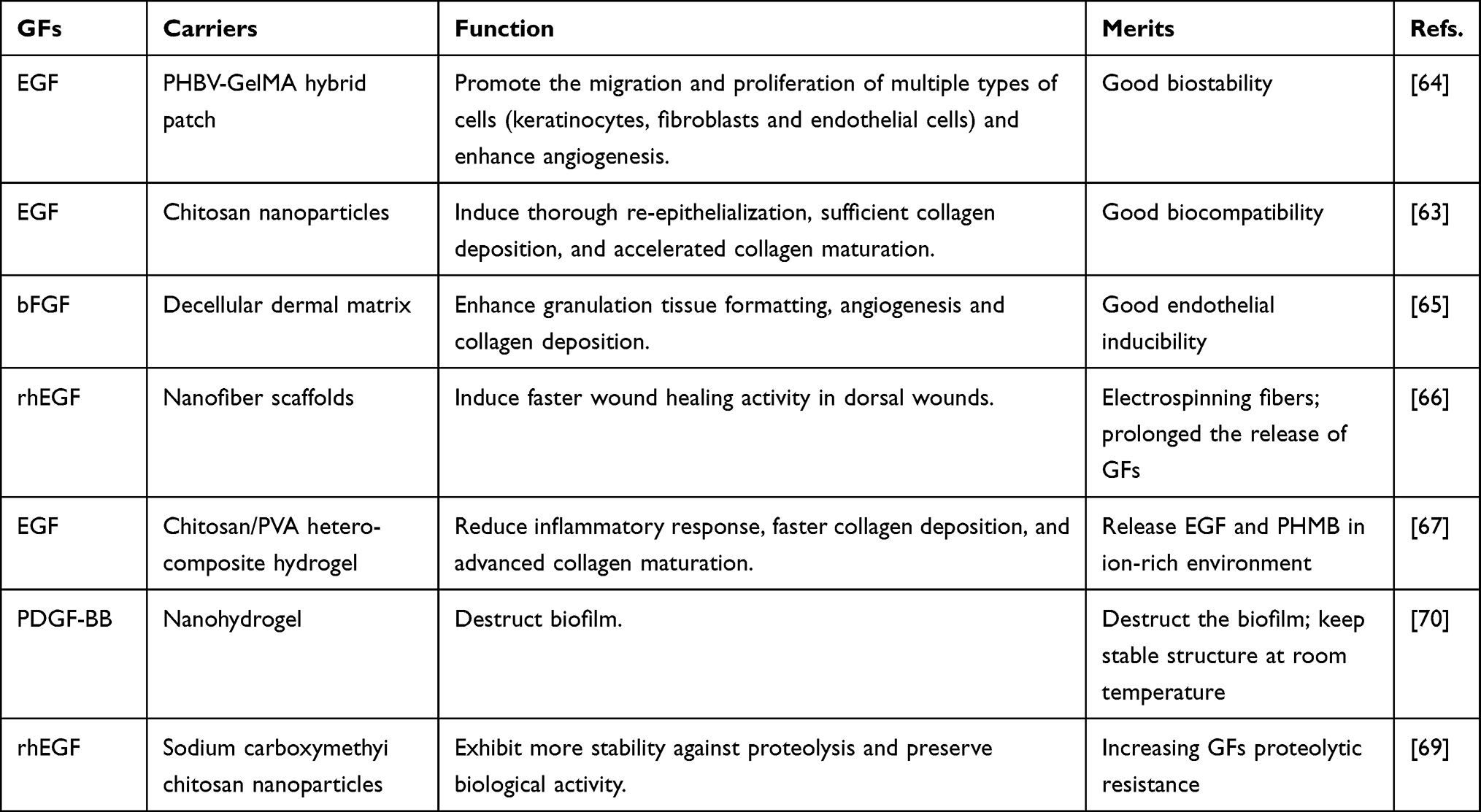 |
Table 1 Delivery of Growth Factors with Nanocarriers |
EGF has an excellent mitogenic effects on epithelial, fibroblastoid and endothelial cells.68 It is interesting to note that the complex microenvironment of DFU is hostile for the production and secretion of EGF and exhibits downregulation of EGF and its receptor.71 Current challenges facing the additional EGF treatment is short half-life and repeated administration.72 A hybrid biomaterial patch is a promising approach for loading the GFs.73 Auguastine et al64 encapsulated EGF in porous nanofiber membranes and hybrid with GelMA hydrogel to form a biodegradable polymeric patch for diabetic wound healing.
Genes/Proteins/Peptides
A gene therapy involves transfection of specific genes to correct genetic disorders. Diabetic wound environments have a complicated genetic disorder, and manipulating gene levels can be promising for the non-healing wound. Several studies have showed microRNAs (miRNAs) regulate post transcriptional gene expression and can be a promising nucleic acid drug for diabetic wound.74 Recently, miR-129 and −335 have been identified as a negative regulator of MMP-9 expression by targeting specific protein-1 (Sp1).74 Gene therapy faces many challenges, transfection via virus has carcinogenic potential.75 Rapid degradation and repeated administration of gene therapy agents (e.g., nucleic acids, proteins, peptides) can amplify the adverse effect. NDDSs can provide a system for better circulating concentration and precise modulation at the target site. Yan et al76 reported milk-derived exosomes to deliver miRNA, which are fabricated through electroporation and achieved higher cell uptake and were able to resist degradation.76 In vivo results showed this novel system promoted angiogenesis and enhanced diabetic wound healing.76 Small interfering RNA (siRNA) mainly involves the RNA interference (RNAi) phenomenon and induces gene silencing post-transcriptionally.77 Shaabani et al78 formulated siRNA into a layer-by-layer platform with a tunable outer surface to increase angiogenesis factors in diabetic wound area. They focused on the stabilization of HIF-1α, which is crucial for activating angiogenesis factors. Layer-by-layer self-assembled siRNA-loaded nanocarriers can delivery siRNA downregulating PHD-2 to stabilize HIF-1α and then increase pro-angiogenic factors level. The report also found these layer-by-layer nanoparticles can prevent endosomal escape and improve transfection efficiency. Currently, various nanocarriers loaded gene therapy agents have been reported. See Table 278–96 for other systems.
 |
Table 2 Delivery of Genes/Proteins/Peptides with Nanocarriers for Diabetic Wound Healing |
Stem Cells/Exosomes
Stem cells (SCs) are a class of cells with multiple differentiation potential and self-renewal ability, and their main features are pluripotency, indefinite division and the ability to promote cytokines secretion.97 Due to their immunomodulatory properties and easily controlled dosage, stem cells therapy has flourished in the field of regenerative medicine and wound healing.98 The mesenchymal stem cells (MSCs) can be derived from various sites, and their ability of multilineage differentiation makes them good candidates for wound healing. Their immune response properties should be considered, and studies have showed that the immune modulation can enhance wound healing.99 Most of the MSCs are derived from bone marrow, compared with MSCs, the adipose-derived stem cells (ADSCs) are less invasive and have no ethical limitations. ADSCs can differentiate to endothelial cells and secrete VEGF to promote wound healing.100 Although many studies have showed that stem cell therapy can improve skin regeneration, their poor survival rate and proliferation capacity shrink their application efficiency. Thus, the mixture of SCs or stem cells exosomes (SCs-exos) with finely-designed NDDSs could be an ideal strategy. Xu et al101 developed an injectable hydrogel with hyperbranched PEG macromer for stable delivery of ADSCs that promote tissue regeneration. Moreover, hypoxia-induced conductive hydrogel incorporating ADSCs can promote the reconstruction of blood vessels, hair follicles and dermal collagen matrix.102 However, stem cells face some limitations such as issues of storage and transportation and risks of tumor formation.103 Exosomes are 40–100 nm sized extracellular vesicles, derived from paracrine secretion of most cell types.104 With stable and easily stored characteristics, they can overcome limitations of stem cells therapy.105 See Table 38,106–113 for more information.
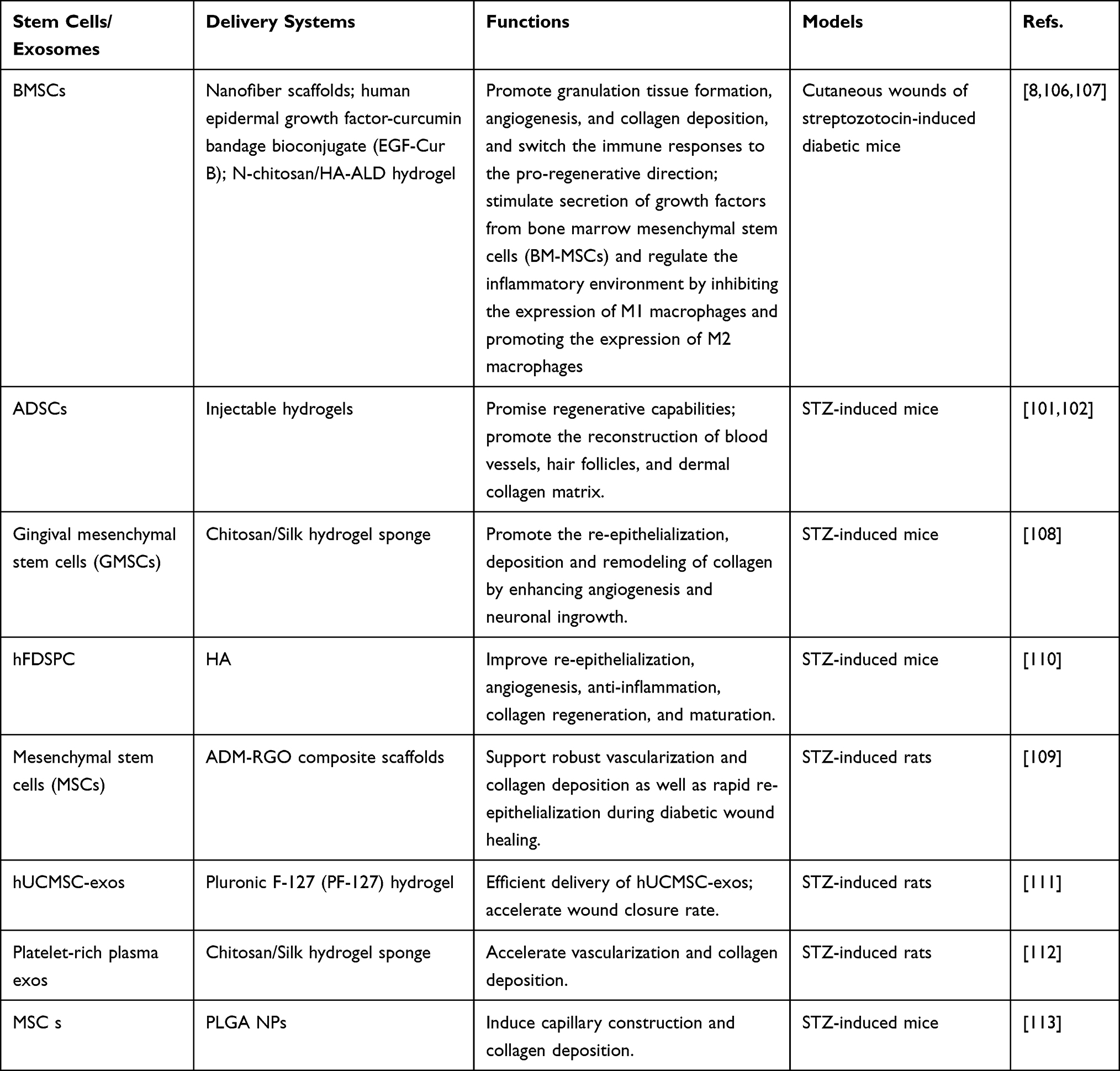 |
Table 3 Stem Cell/Exosomes Loading Nanomaterial for Diabetic Wounds |
Yang et al111 reported Pluronic F127 hydrogel loaded with human umbilical cord-derived mesenchymal stem cell-derived exosomes (hUCMSC-exos). This delivery system efficiently delivered hUCMSC-exos and promoted diabetic wound healing. It can also increase expression of proliferating cells related signals, enhance granulation tissue formation and upregulate growth factor expression.
Thus, biomaterial-based exosomes therapy holds great promise in cutaneous wound treatment and regenerative medicine.114
Drugs
A wide range of drugs have been proved to exhibit significant efficacy for wound healing. The nanoscale local drug delivery system, as an ideal carrier, has been fabricated to overcome the limitations (such as low physico-chemical stability, low bioactive absorption, poor pharmacokinetics etc.) of these drugs (Table 4).10,111,115–131
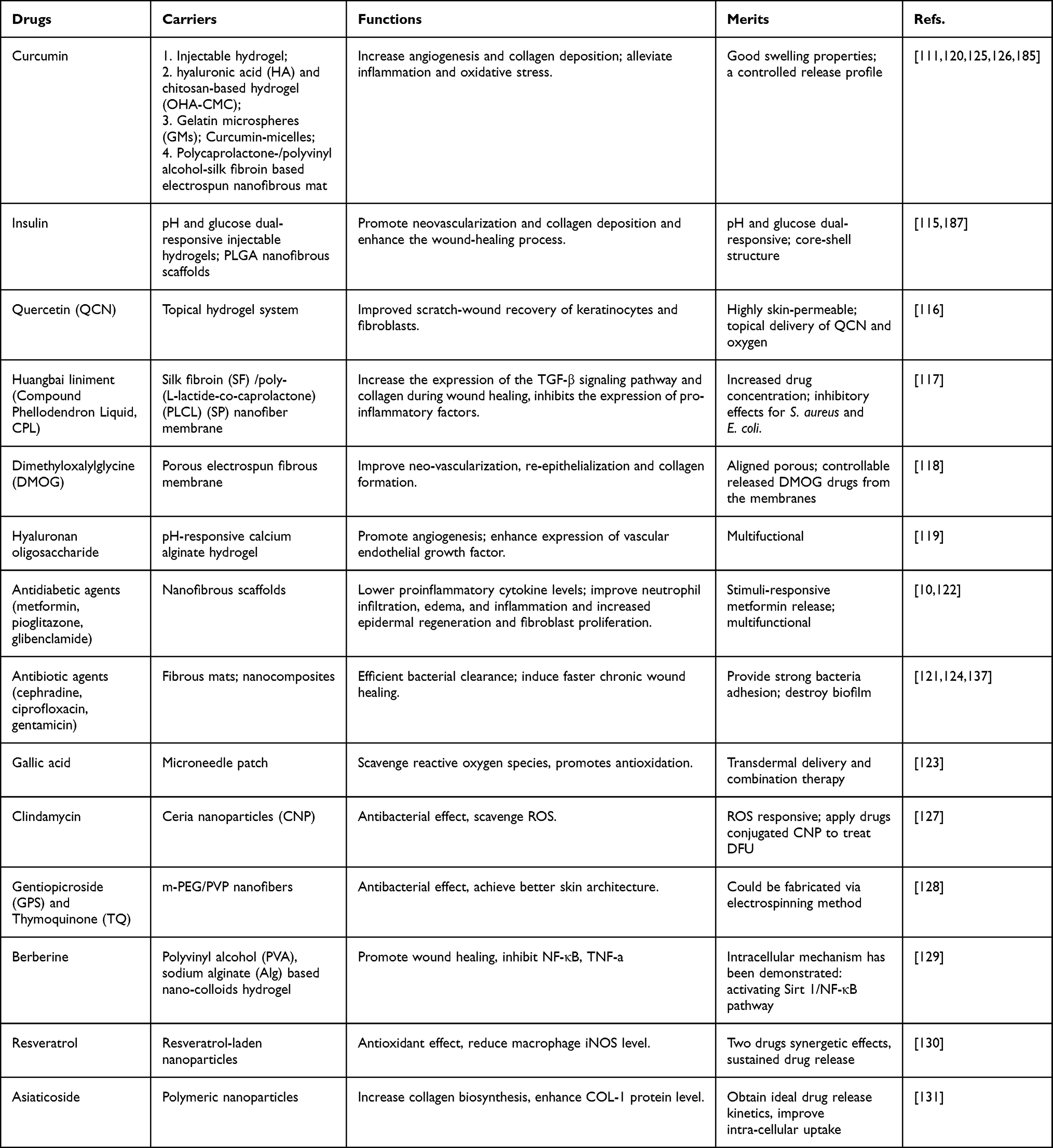 |
Table 4 Delivery of Drugs for Efficient Diabetic Wound Healing |
Curcumin is a natural polyphenol obtained from turmeric.132 This natural bio-substance is often used as an antioxidant and anti-inflammatory agent, and can aid various stages of the wound healing process.133 However, just like other small hydrophobic molecules, curcumin shows low stability in wound healing treatment, especially for topical application.134 Liu et al125 enclosed self-carried Cur nanoparticles (CNPs) in gelatin microspheres (GMs), which can respond to the overexpression of MMP-9 in the wound environment, and the CNPs@GMs have been loaded into a thermo-sensitive hydrogel to facilitate the healing process. Recently Hu et al120 reported a hyaluronic acid (HA) and chitosan-based hydrogel (OHA-CMC) for loading and delivering CNPs. Benefiting from the encapsulated CNPs, this formulation exhibited excellent antioxidant and anti-inflammatory ability and presented on-demand drug release. Antidiabetic agents such as metformin (MET), pioglitazone (PHR) and glibenclamide (GB) have been confirmed to exhibit strong anti-inflammatory effects, which can be applied in the research of accelerating diabetic wound healing. Cam et al10 loaded three types of oral antidiabetic agents into nanofibrous scaffolds based on two different polymer composites mixtures (CS/GEL/PCL and PVP/PVL), to improve type I diabetic wound healing. In a previous study, Cam et al122 have confirmed PHR loaded fibrous mats have high potential for targeting inflammatory and proliferation phases of DFU; in follow-up studies, they further demonstrated that PHR&MET and PHR&GB exhibited better healing rate then single usage of PHR.
Non-Bioactive Substances
Metal Ion
Metal ion nanoparticles have attracted extensive attention as an appreciable option to antibiotics.135 Among various metallic elements, silver (Ag) is the most studied for its strong and long-lasting antibacterial properties against various pathogens and microorganisms.136 Though the inherent mechanisms of AgNPs antibiotic ability are still unclear, it is recognized that AgNPs can destroy the cell wall or cell membrane. Wang et al137 showed that Ag nanocubes with a virus-like mesoporous silica coating improved cell wall adhesion and completely eradicated pathogenic bacteria in the wound site. Gold (Au) nanoparticles are also reported as an anti-infection agent. Their inert and nontoxic nature makes them an ideal material as the core of NPs. Researchers have demonstrated AuNPs can strongly resist both Gram-negative and Gram-positive pathogens and do not develop drug resistance.138 Currently, copper NPs (CuNPs) are drawing considerable attention as antibiotic agents for wound healing. Their high redox potential makes them effective against a broad-range spectrum of bacterial species, and they have relatively low cost compared with Ag and Au.139 Our review gives more information of metal ion nanoparticles in the drug delivery system section.
Oxygen
With more in-depth understanding of the mechanism of chronic wound healing progress, a prolonged hypoxic environment has been confirmed as one of the causes of healing impediment.140
Several advanced treatments for proper oxygen supply are currently available on the market, such as hydrofiber® dressings.141,142 Nanomedicine have been introduced to fabricate oxygen-releasing systems, and scientific studies have emerged to design and fabricate tunable platforms in terms of controlling oxygen supplementation.29 Currently, various oxygen-containing nanocarriers have been shown to reverse the hypoxic environment of diabetic wounds (Table 5).9,11,12,67,143–154
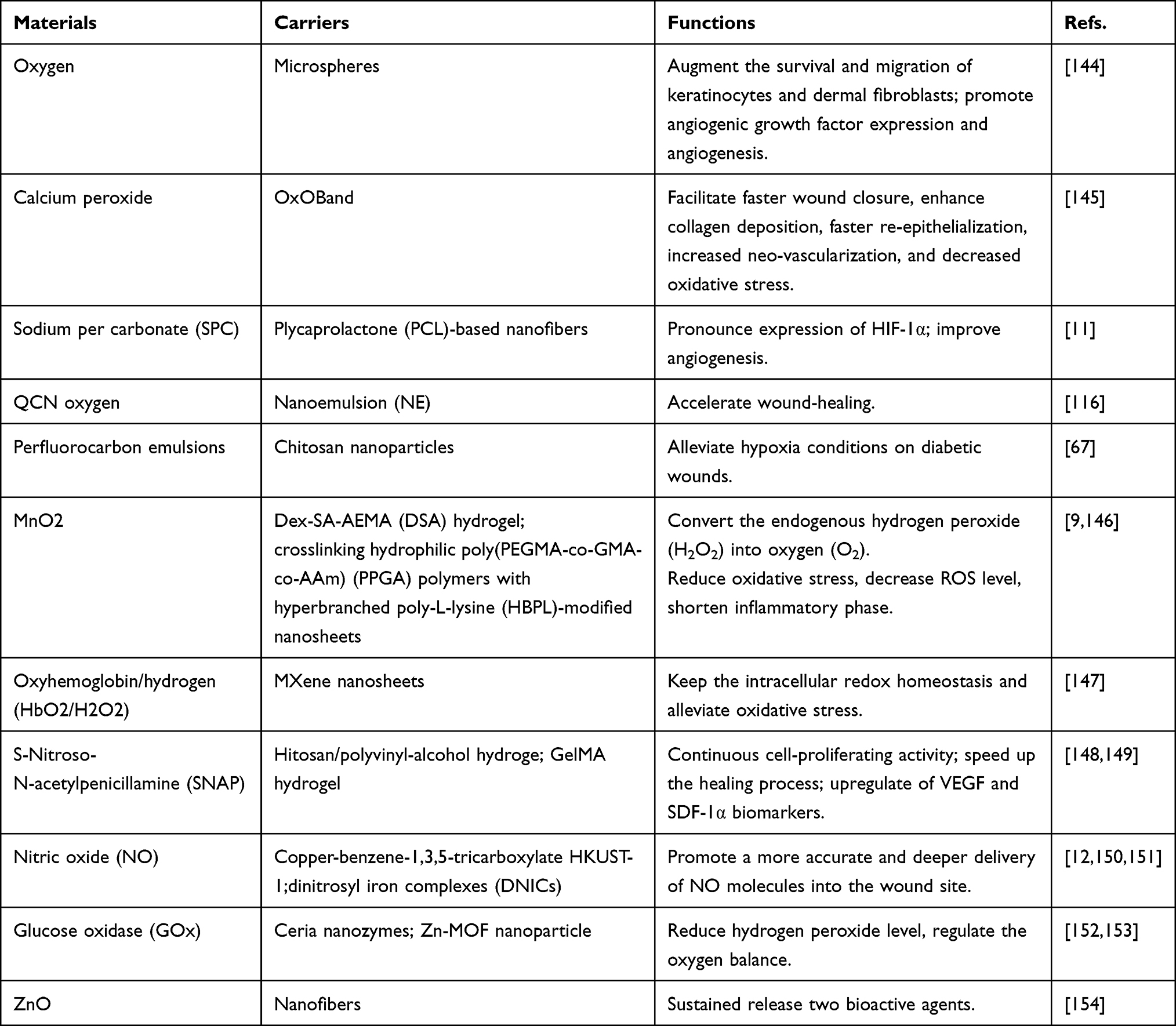 |
Table 5 Delivering Oxygen/NO for Diabetic Wound Treatment |
Sodium percarbonate (SPC), as a strong oxidant, has been found to be a potential oxygen-generating agent to accelerate healing in a chronic non-healing wound. Oxygen generation of SPC is peroxide-based, releasing hydrogen peroxide in water solution and ultimately oxygen on decomposition.143 Zehra et al11 reported a PCL polymer-based dressing, which encapsulated oxygen generator SPC to improve the hypoxia in wound site. Their results showed that the novel dressing could release sufficient oxygen at the wound site for a long period and significantly improve angiogenesis.
However, reactive oxygen species (ROS) is another existing form of oxygen element in the wound microenvironment, and abnormally high levels of ROS can inhibit wound healing processes and cause a non-healing wound. Recently, nitric oxide (NO), as an important ROS scavenger, is considered to play a pivotal role in healing process pathology of diabetic wounds. Hyperglycemic conditions in the diabetic wound environment can inhibit the synthesis of endogenous NO. Topical NO delivery have received more and more attention, and there are several donors that have been investigated for NO delivery such as organic nitrates and nitrites, metal-NO, diazeniumdiolates (NONOates) and S-nitrosothiols (RSNOs).155 Zhang et al12 recently developed HKUST-1, a novel MOF system with unsaturated Cu metal site, to deliver NO. With highly designable structure, the nanomaterial scaffold released NO with an ideal concentration and promoted angiogenesis and collagen deposition.
Nano-Drug Delivery System
NDDSs refer to drug delivery systems with particle diameter within the nanoscale, which have the feature of improving drug stability, sustained release and controlled release of drugs, and they can be fabricated with a variety of biomaterials.156 An unprecedented number of NDDSs loading therapeutic agents have emerged and these are being used in diabetic wound treatment. NDDSs can be classified into liposomes, polymeric nanoparticles, inorganic nanoparticles, lipid nanoparticles, nanofibrous structures and nanohydrogel (Figure 3).
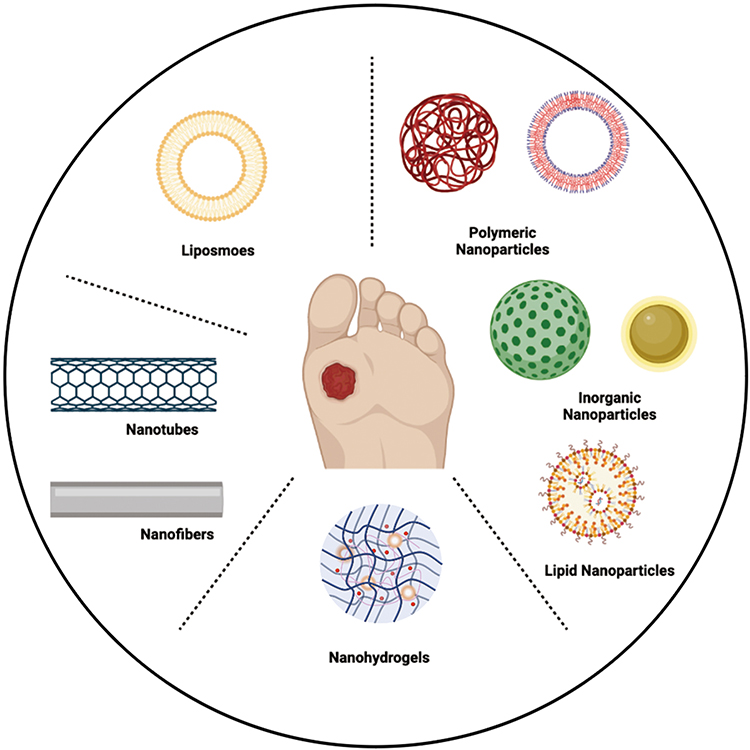 |
Figure 3 Schematic representation of nano-drug delivery system used for diabetic wound healing: Liposomes, Polymeric nanoparticles, inorganic nanoparticles, lipid nanoparticles, nanofibers, nano-hydrogels. (figure was created with BioRender.com). |
Liposomes
Liposomes are artificial membranes mainly composed of amphiphilic molecules, which form a bilayer structure similar to the structure of skin cell membranes. With drugs encapsulated in the hollow part of the lipid-like bilayer, liposomes are advanced nano-carriers for drug delivery.157
With their intrinsic merits such as biodegradability, lower systemic toxicity and targeted delivery, liposomes have been universally applied in drug delivery and made their way to the market.158 A total of 14 liposome products have been approved for marketing.159 These liposomal products are primarily focused on oncology treatment. Currently, increasing novel liposomes with modified surfaces are springing up to cover the shortage of conventional vesicles in the field of chronic wounds.160
Chhibber et al161 prepared a novel liposome which efficiently entrapped bacteriophages. The vehicles remarkably improved phage persistence in situ. The results showed that liposomal entrapment of phage cocktail significantly reduces wound bioburden, accelerates wound contraction and speeds tissue healing. It was fully confirmed that the liposome entrapped with phage cocktail overcomes the major drawback of phage therapy and addresses a Staphylococcus aureus-induced chronic wound infection.
Rabbani et al79 reported a lipoproteoplex (LPP) siRNA delivery vehicle, targeting the Keap1/Nrf2 pathway associated with impaired diabetic wound pathology, thereby promoting wound healing. A stable LPP nanoparticle is produced of a cationic lipid nanoparticle (CLN) as a primarily lipid-based vehicle, and a cationic engineered supercharged coiled-coil protein (CSP) has been engineered to enhance transfection efficacy. The novel system overcomes traditional challenges facing RNAi therapy, which uses lipid or peptide alone as siRNA delivery vehicles. The results showed that LPP complexing siKeap 1 restored Nrf2 antioxidant function, augmented reduction-oxidation homeostasis in the wound area and accelerated diabetic tissue regeneration.
Although liposomes are a well-studied drug delivery system, its application on transdermal drug delivery is limited since they are unable to penetrate through the deep layers of skin. The rigid structure of the conventional liposomes makes them stay in the stratum corneum (SC) layer and achieve low drug delivery efficiency.162 Deformable liposomes, as a new generation of liposomes, have been developed to overcome this limitation.160 They are generally prepared by embedding edge activators, such as surfactant and ethanol, into traditional liposomes, which can destabilize the original lipid layers to achieve a flexible membrane. With a high flexibility, deformable liposomes can change the homeostasis of the cells in the stratum corneum and squeeze into the deeper viable epidermis.163,164
Polymeric Nanoparticles
Polymeric NPs are colloidal systems that are biocompatible and have simple formulation parameters.165 Drugs embedded or conjugated with biodegradable polymers can achieve lower degradation rates and release in a controlled manner in the wound area. These merits make polymeric nanoparticles draw increasing attention in the nano-drug delivery system field.166 Polymeric nanoparticles possess a core-shell structure with drugs encapsulated in the core and hydrophilic polymeric outer surface which provides stearic stability.167 Currently, the preparation of polymeric nanoparticles is majorly based on polylactic-co-glycolic acid (PLGA), polyglycolic acid and other synthetic polymers, as well as natural polymers (alginate, gelatin, chitosan, etc.).168
To overcome the low solubility and the high susceptibility to oxidation of melatonin, Lopes et al169 incorporated melatonin into a lecithin-chitosan nanoparticles for diabetic wound healing. The particle size of MEL-NPs was within proper nanoscale (160 nm), and the therapeutic melatonin was efficiently entrapped in the nanocarrier. The study concluded that the MEL-NPs delivery system can improve pharmacokinetics of melatonin, thus promotes the vascular system and accelerates re-epithelization and angiogenesis. Polymeric nanoparticles obtain a low viscosity and dispersion ability due to their intrinsic structure, which makes them unsuitable candidates for topical administration. To ease the application of polymeric nanoparticles on topical treatment, Bairagi et al170 have developed ferulic acid nanoparticles and converted the nano-system into hydrogel. The ferulic acid with antidiabetic and antioxidant properties was encapsuled in PLGA by nano precipitation method, and then the drug-loaded NPs were mixed into hydrogel for topical treatment. The results showed that diabetic wounds treated with FA loaded polymeric nanoparticles achieve faster epithelialization, significantly increasing hydroxyproline content. It is confirmed that FA-PLGA nanoparticles overcome the pharmacokinetic limitations of FA and significantly promote diabetic wound healing.
Inorganic Nanoparticles
The main component of inorganic nanoparticles are inorganic materials, and inorganic substances include metal, carbon and ceramics.165 Benefiting from various inorganic components and the nanoscale structure, inorganic NPs exhibit better biological behaviors than their macroscale counterparts. Many inorganic NPs achieve great success in antitumor therapy, which highlights their promise in nanomedicine. Therefore, a diverse array of inorganic NPs system has been studied to explore their prospect in the field of diabetic wound treatment.
Quercetin (QCT) is known as free radical scavenger and anti-inflammatory agent, and AgNPs are effective antimicrobial agents. To investigate the synergistic therapeutic performance of QCT and AgNPs, Badhwar et al171 fabricated QCT loaded Ag nanoparticles and subsequently hybridized the QCT-AgNPs into hydrogel matrices for diabetic wound treatment. Compared with marked Ag-loaded dressings, QCT-AgNPs revealed superior therapeutic efficiency in killing S. aureus and E. coli and reducing oxidative stress. The histopathological evaluation showed that QCT-AgNPs could significantly reduce the wound gap and promote migration of keratinocytes in DFU models in vivo. Some NDDSs formulations have focused on the synergistic effect of both the inorganic nanoparticles and the encapsulated drugs. Kaur et al172 fabricated AgNPs loading with insulin to achieve a mutually reinforcing effect of the two components. The IAgNPs exhibited appropriate nano size and structure. When applied to diabetic wounds, it notably stimulated healing activity, which could be explained by downregulating pro-inflammatory factors (IL-6, TNFα) levels at the injured site (Figure 4). Researchers are extending their studies to the blending application of various types of NPs systems to achieve multi-functionality. Choudhary et al173 developed chitosan-based hydrogel co-encapsulated with fresh blood and nanoparticles (Ca-AlgNps and AgNPs) for diabetic wound healing. The co-encapsulated nanocarrier contributes to much higher closure rate, the Chitosan/Ca-AlgNps/AgNPs hydrogel exhibiting a higher closure rate then separate AlgNps or AgNPs loaded hydrogels. The antimicrobial studies confirmed that Chitosan/Ca-AlgNps/AgNPs hydrogel has broad spectrum antibacterial properties. All the evidence supported that Chitosan/Ca-AlgNps/AgNPs hydrogel might become a potential candidate for diabetic wound healing.
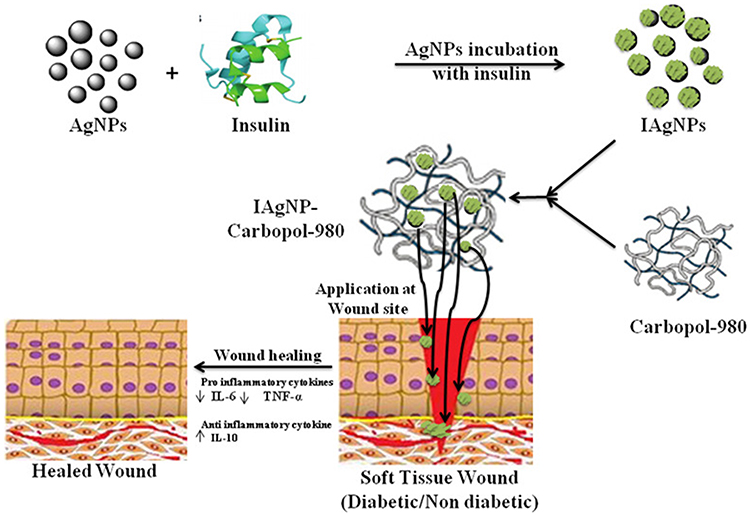 |
Figure 4 Schematic diagram of wound healing by nano-insulin formulation (IAgNPs). IAgNPs accelerated the wound healing in diabetic conditions by inhibiting pro-inflammatory cytokines and activating anti-inflammatory cytokines. Notes: Reprinted from Nanomedicine, 15(1), Kaur P, Sharma AK, Nag D, et al. Novel nano-insulin formulation modulates cytokine secretion and remodeling to accelerate diabetic wound healing. 47–57, Copyright 2019, with permission from Elsevier.172 |
Lipid Nanoparticles
Lipid nanoparticles were generally synthesized by glycerophospholipids, cationic lipids, sterol lipids and PEGylated lipids coated with oligonucleotides.174 Solid lipid nanoparticles (SLNs) and nanostructured lipid carriers (NLCs) are two representatives of LNPs, and both of them can increase solubility and stability of encapsulating drugs.175 Recently, researchers have had great interest in application of LNPs in topical treatment.
Arantes et al176 fabricated SLNs loading with retinoic acid to reduce adverse reactions of the all-trans retinoic acid. The SLN-ATRA were developed through a hot melting homogenization method, and based on the optimized method, SLN-ATRA can be prepared without organic solvents and achieve high encapsulation rate and lower polydispersity index (PDI). The results showed that the SLN-ATRA had superior ability to free ATRA in reducing leukocyte infiltration and accelerating wound closure, collagen deposition and reducing scar tissue when applied on excisional wounds of diabetic mice. In another scientific report, pioglitazone-loaded LNPs were designed, fabricated, then successfully encapsulated into a collagen/chitosan (COL-CS) scaffold.177 This scaffold possessed optimum porosity, high encapsulation efficiency and low degradation rate. When applied in full-thickness diabetic wounds, it significantly improved the wound contraction rate, and the data of enzyme-linked immunosorbent assay indicated the MMP9 level is decreased. Sun et al178 reported 20 (S)-protopanaxadiol-loaded nanostructured lipid carriers were successfully incorporated in a silicone elastomer. The results showed that the formulation exhibited remarkable in vitro anti-inflammatory and proangiogenic activity. When applied to diabetic mice with chronic non-healing wounds, it notably achieves an ordered recovery through suppressing inflammatory infiltration, promoting angiogenesis and increasing collagen deposition. Huseh et al92 designed and synthesized nanostructured lipid carrier formulations encapsulating recombinant human thrombomodulin (rhTM) for diabetic wound healing. RhTM-loaded NLCs were characterized by much higher encapsulation efficiency and exhibited a controlled drug release behavior for more than 72 h. The in vitro study showed that rhTM-NLC could induce cell migration of keratinocyte cells to promote SC formation. Therefore, this formulation may warrant promising delivery systems for diabetic wound healing. However, LNP systems also have several disadvantages, such as low drug loading and biodistribution, which lead to high uptake to the liver and spleen and limit their application in clinical trials.179
Nanofibers
Nanofibers comprise an important class of nanomaterials, and generally have a diameter less than 100 nm.180 Nanofibers provide many remarkable properties such as large surface area, variable porous rate, great flexibility in selecting materials, and fine fabrication technology.181 These wonderful features make nanofibers a potential candidate for biomedical application, especially in drug delivery. Electrospinning, as a simple and versatile method, is widely used to format nanofibers.182 There are a wide range of drugs that can be incorporated into nanofibers, including antibiotics, proteins, DNA, RNA and growth factors.183 Electrospun nanofibers can achieve high surface to volume ratio, and have different controlled drug release profiles.182,184
Agarwal et al185 prepared curcumin-loaded silk fibroin and combined this nanofiber with polycaprolactone (PVC) and polyvinyl alcohol (PVA) via electrospinning nanotechnology. This nanofiber showed rapid healing efficacy in a streptozotocin-induced diabetic mice wound model. Also, data of the histopathological studies revealed that in vivo the normal skin structure and tissue arrangement were restored in NDDSs-treated group.
Liu et al186 electrospun sesamol into cellulose acetate-zein (CA/zein) nanofiber membranes to fabricate efficient vehicles for cutaneous wound healing. In vivo observation depicted significant stimulation of myofibroblasts via activating TGF-β signaling pathway transduction. The nanofiber membranes also downregulated inflammatory factors (IL-1β, TNF-α, NOS2) levels and upregulated IL-6 secretion, which promotes keratinocyte growth, and thus enhances wound healing. In some cases, nanofibers were combined with stem cell therapy; Chen et al106 reported BMSCs-laden 3D scaffolds for a personalized diabetic wound treatment. The 3D scaffolds were electrospun with radially or vertically aligned nanofibers to achieve customizable structures to fit different wounds. The results showed that this nanofiber scaffold can replace damaged skin and act as a temporary barrier and has good biodegradability. Thus, these scaffolds were regarded as a potential customizable platform for managing diabetic wounds. Lee et al187 developed insulin-loaded PLGA scaffolds via coaxial electrospinning (Figure 5). The core-shell nanofibrous scaffolds were confirmed to feature with better biodegradability, hydrophilicity and water-containing capacity. In vivo study showed that this core-shell nanofiber affects TGF-β expression and promotes diabetic wound repair. Nanofibers delivering more than one drug draw increasing attention as a potential substrate for biomedical application, especially in diabetic wound healing fields. Dwivedi et al66 reported a novel nanofiber scaffold, which carried the antibiotic agent gentamicin sulfate (GS) and rhEGF. The results of scanning electron microscopy, Fourier transform infrared spectroscopy and X-ray diffraction confirmed that GS was successfully loaded into scaffolds and the rhEGF was covalently immobilized on the surface of the nanofiber scaffolds. In vivo work found that the nano-scaffolds induced faster reepithelialization activity in dorsal wounds of diabetic mice. According to the report of Lee et al,188 nanofibrous scaffolds were developed with poly(lactide-co-glycolide) (PLGA) loaded with bioactive antibiotics and platelet-derived growth factor (PDGF), and the scaffolds obtained a coaxial sheath-core architecture. The nano-scaffolds were characterized with excellent biocompatibility, and sustainably released vancomycin, gentamicin and growth factor for over 3 weeks. Furthermore, reduced phosphatase and tensin homolog content and enhanced angiogenesis marker (CD31) were detected to provide evidence for benefiting infected diabetic wound healing.
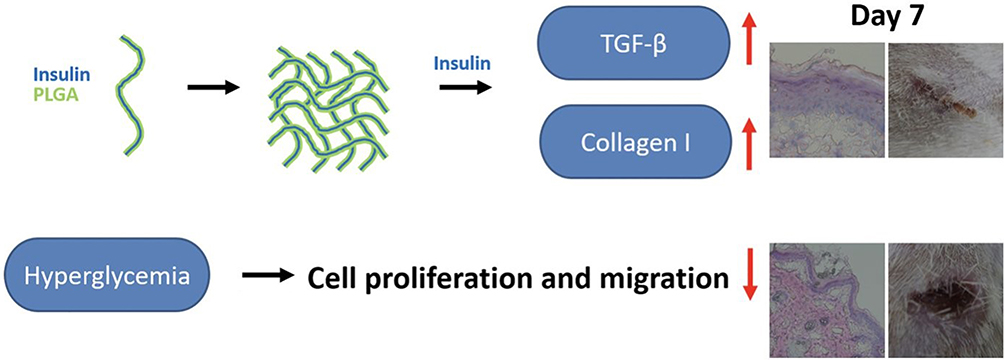 |
Figure 5 Accelerate the healing wound following treatment using functionally active insulin released from insulin-loaded nanofibrous scaffolds. Notes: Reprinted from Nanomedicine, 24, Lee CH, Hung KC, Hsieh MJ, et al. Core-shell insulin-loaded nanofibrous scaffolds for repairing diabetic wounds. 102123, Copyright 2020, with permission from Elsevier.187 |
Nanohydrogel
Nanohydrogel is a multicomponent system composed of a polymeric three-dimensional network and water.189,190 The porous structure endows nanohydrogels with the ability of rapidly swelling and retaining large amounts of water.167 In recent years, various hydrogel products have been designed in application of drug delivery for accelerating diabetic wound healing.191 Nanohydrogel provides a moist environment for the wound area, and with soft texture and suitable mechanical strength, it provides a beneficial environment for wound healing.69,192
Zhang et al193 introduced a polyvinyl alcohol (PVA)/alginate (Alg) nanohydrogel encapsulating HUCMSCs-derived exosomes to regulate diabetic wound healing (Figure 6). The results showed that the nanohydrogel significantly facilitates the proliferation, migration and angiogenesis of HUVECs and affects wound healing related molecules (SMA, SR-B1 and CD31). Further investigation revealed that this novel formation accelerated wound healing via regulating ERK1/2 pathway, and thus promoting angiogenesis. A multifunctional hydrogel was reported by Xiong et al194 to accelerate oxidative diabetic wound healing. This HA-based hydrogel consisted of MnO2/ε-PL nanosheet, FGF-2 and M2-derived exosomes (M2 Exos). With the addition of MnO2, this nanocomposite eliminates excess H2O2 production and provides O2 for the wound site. Moreover, specially encapsulated FGF-2 and M2 Exos respectively promote angiogenesis and epithelization. Thus, this hydrogel could be a viable nano-biomaterial for chronic diabetic wound repair. Nidadavolu et al195 designed a novel peptide-based hydrogel, using nanotechnology to self-assemble valsartan amphiphiles into a filamentous structure (val-filaments). The results of in vivo observation showed the nanohydrogel provided a localized and sustained release of valsartan amphiphiles over 24 days. Moreover, this scaffold downregulated Tgf-β signaling pathway mediators (pSmad2, pSmad3 and Smad4) and increased mitochondrial metabolic pathway intermediates.
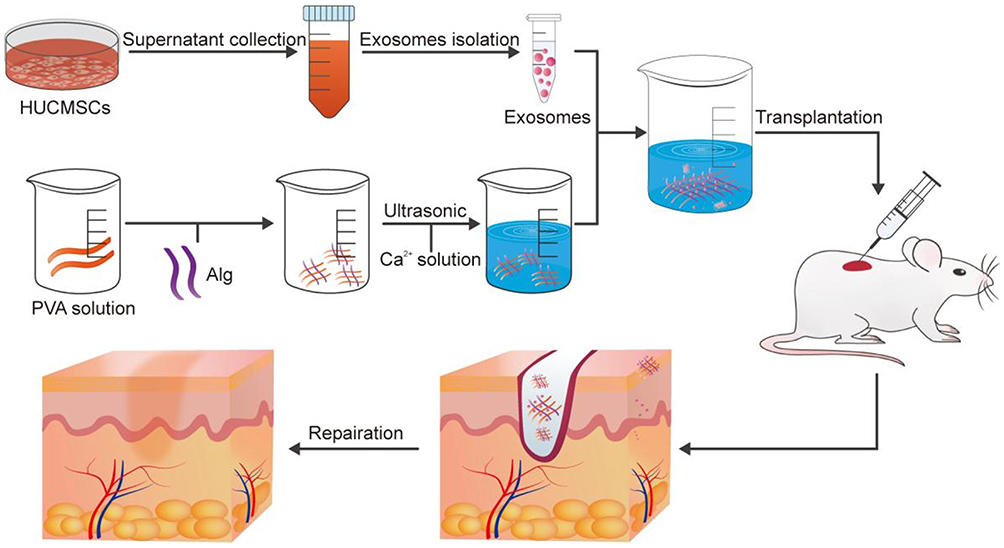 |
Figure 6 The schematic diagram of the method of making exo@H and the process that exosomes were applied to the wound area and promoted wound healing. Notes: Reprinted from Mater Sci Eng C Mater Biol Appl, 120, Zhang Y, Zhang P, Gao X, Chang L, Chen Z, Mei X. Preparation of exosomes encapsulated nanohydrogel for accelerating wound healing of diabetic rats by promoting angiogenesis. 111671, Copyright (2021), with permission from Elsevier.193 |
Discussion
The treatment of diabetic wounds faces many challenges and new insights are needed in this field. Drug delivery system combined with nanotechnology and biomaterials offers a rich toolbox for the treatment of complex pathophysiology of diabetic wound and tissue repair. In this review, we summarized pathology progress of diabetic wound healing, loading substances of NDDSs and loading systems of NDDSs.
Most of the encapsulated drugs are subject to impaired function of different cells and unbalanced levels of key healing mediator. The understanding of specific molecules function in diabetic wound healing progress facilitates the design of drug delivery systems. However, the etiopathogenesis of diabetic ulcers is diverse and complex, the confirmed positive effect of one therapy on one model might have no effect on other models or individuals.
Recently, novel NDDSs, such as liposomes, nanoparticles, nanofibers and nano-hydrogels loaded with bioactive molecules and non-bioactive elements, have been reported and these studies confirmed NDDSs with therapeutic substances benefit diabetic wound healing. In this context, various smart nano hydrogel system have been investigated, but few of them mention the interactive effect between the carrier and the cargo and horizontal comparison with other types of systems. So, there is still no confirmed conclusion of which system performs the best.
To date, various in vitro and in vivo studies have demonstrated the great therapeutic potential of NDDSs, while most of them illustrate treatment benefits through animal models. Few studies, however, consider the irregular shape and different depths of wounds in clinical patients; the animal models usually include only one condition.
Although there are large numbers of studies focusing on therapeutic potential of NDDSs, effective management of diabetic wound healing remains insufficient. Depending on the current gaps above, researchers need to pay more attention to factors in different angles. First, as in diabetic patients, people develop chronic non-healing wounds often accompanied with unregulated hyperglycaemia and vascular lesions. The ideal NDDSs should load drugs which can ameliorate the basic diabetic pathological conditions, besides drugs that directly accelerate wound healing processes. Also, the interaction between carried drugs and pathological stages should be clearly clarified. Since there is no single substance that can perform best and suits all kind of diabetic wound conditions, future studies should focus on multi-drug systems to provide synergic effects at different stages, especially the application of gene therapy for precise treatment. The methods of NDDSs preparation are also important, so, researchers should build systems with more simple methods for manufacturing and marketing. To complete clinical translation, more preclinical and clinical studies on the benefit on humans should be carried out.
Conclusion
Today, the treatment of diabetic non-healing wounds faces many difficulties. The complex pathological process of diabetic wound healing and various conditions of diabetic patients create obstacles to current treatment results. Many therapeutic agents (GFs, genes, stem cells, drugs, metal ions and oxygen) related to healing stages and mechanisms have been studied to make an equilibrium level of key mediator for better wound healing. The field of drug delivery systems has shown great performance in delivering therapeutic drugs for diabetic wound treatment. Over the past few years, nanomedicine has facilitated the development of drug delivery systems, and various nano-drug delivery systems (liposomes, NPs, nanofibers and nanohydrogel) have been formed to deal with diabetic non-healing wounds. Overall, the nano-drug delivery system with therapeutic agents can accurately provide agents to the wound site and achieve great therapeutic potential for diabetic wound management.
Abbreviations
DM, diabetes mellitus; DDSs, drug delivery systems; NDDs, nano-drug delivery systems; DFU, diabetic foot ulceration; HBO, hyperbaric oxygen therapy; PCL, polycaprolactone; GelMA, Methacrylate Gelatin; GF, growth factor; ECM, extracellular matrix; MMP, matrix metalloprotein; DN, diabetic neuropathy; PAD, peripheral arterial disease; IDSA, Infectious Diseases Society of America; TGF-β, transforming growth factor-β; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factor receptors; PDGF, platelet-derived growth factor; EGF, epidermal growth factor; FGF, fibroblast growth factor; miRNAs, microRNAs; siRNA, small interfering RNA; RNAi, RNA interference; MSCs, mesenchymal stem cells; ADSCs, adipose-derived stem cells; hUCMSC-exos, umbilical cord-derived mesenchymal stem cell-derived exosomes; CNPs, Cur nanoparticles; GMs, gelatin microspheres; HA, hyaluronic acid; SPC, sodium percarbonate; ROS, reactive oxygen species; NO, nitric oxide; LPP, lipoproteoplex; CLN, cationic lipid nanoparticle; SC, stratum corneum; PLGA, polylactic-co-glycolic acid; QCT, quercetin; SLNs, solid lipid nanoparticles; NLCs, nanostructured lipid carriers; rhTM, recombinant human thrombomodulin; PVC, polycaprolactone; PVA, polyvinyl alcohol.
Acknowledgments
We acknowledge funding by the National Key R&D Program of China [No. 2018YFE0194300], the Natural Science Foundation of Guangdong Province [No. 2020A1515010107], the Guangdong Province Key Field R&D Program Project [No. 2020B1111150001], and the Science and Technology Innovation Project of Guangdong Province [No. 2018KJYZ005]. We acknowledge Mr Yanbin Gao, Dr Jun Ma for their supervision of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4–14. doi:10.1016/j.diabres.2009.10.007
2. Gao D, Zhang Y, Bowers DT, Liu W, Ma M. Functional hydrogels for diabetic wound management. APL Bioeng. 2021;5(3):031503. doi:10.1063/5.0046682
3. Tecilazich F, Dinh T, Veves A. Treating diabetic ulcers. Expert Opin Pharmacother. 2011;12(4):593–606. doi:10.1517/14656566.2011.530658
4. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–2375. doi:10.1056/NEJMra1615439
5. Sunkari VG, Lind F, Botusan IR, et al. Hyperbaric oxygen therapy activates hypoxia-inducible factor 1 (HIF-1), which contributes to improved wound healing in diabetic mice. Wound Repair Regen. 2015;23(1):98–103. doi:10.1111/wrr.12253
6. Madhukiran D, Jha A, Kumar M, Ajmal G, Bonde GV, Mishra B. Electrospun nanofiber-based drug delivery platform: advances in diabetic foot ulcer management. Expert Opin Drug Deliv. 2021;18(1):25–42. doi:10.1080/17425247.2021.1823966
7. Farokhzad OC, Langer R. Impact of nanotechnology on drug delivery. ACS Nano. 2009;3(1):16–20. doi:10.1021/nn900002m
8. Bai H, Kyu-Cheol N, Wang Z, et al. Regulation of inflammatory microenvironment using a self-healing hydrogel loaded with BM-MSCs for advanced wound healing in rat diabetic foot ulcers. J Tissue Eng. 2020;11:2041731420947242. doi:10.1177/2041731420947242
9. Tu C, Lu H, Zhou T, et al. Promoting the healing of infected diabetic wound by an anti-bacterial and nano-enzyme-containing hydrogel with inflammation-suppressing, ROS-scavenging, oxygen and nitric oxide-generating properties. Biomaterials. 2022;286:121597. doi:10.1016/j.biomaterials.2022.121597
10. Cam ME, Ertas B, Alenezi H, et al. Accelerated diabetic wound healing by topical application of combination oral antidiabetic agents-loaded nanofibrous scaffolds: an in vitro and in vivo evaluation study. Mater Sci Eng C Mater Biol Appl. 2021;119:111586. doi:10.1016/j.msec.2020.111586
11. Zehra M, Zubairi W, Hasan A, et al. Oxygen generating polymeric nano fibers that stimulate angiogenesis and show efficient wound healing in a diabetic wound model. Int J Nanomedicine. 2020;15:3511–3522. doi:10.2147/IJN.S248911
12. Zhang P, Li Y, Tang Y, et al. Copper-based metal-organic framework as a controllable nitric oxide-releasing vehicle for enhanced diabetic wound healing. ACS Appl Mater Interfaces. 2020;12(16):18319–18331. doi:10.1021/acsami.0c01792
13. Lazarus GS, Cooper DM, Knighton DR, Percoraro RE, Rodeheaver G, Robson MC. Definitions and guidelines for assessment of wounds and evaluation of healing. Wound Repair Regen. 1994;2(3):165–170. doi:10.1046/j.1524-475X.1994.20305.x
14. Robson MC, Steed DL, Franz MG. Wound healing: biologic features and approaches to maximize healing trajectories. Curr Probl Surg. 2001;38(2):72–140. doi:10.1067/msg.2001.111167
15. Martin P. Wound healing--aiming for perfect skin regeneration. Science. 1997;276(5309):75–81. doi:10.1126/science.276.5309.75
16. Kurkinen M, Vaheri A, Roberts PJ, Stenman S. Sequential appearance of fibronectin and collagen in experimental granulation tissue. Lab Invest. 1980;43(1):47–51.
17. Werner S, Grose R. Regulation of wound healing by growth factors and cytokines. Physiol Rev. 2003;83(3):835–870. doi:10.1152/physrev.2003.83.3.835
18. Daley JM, Reichner JS, Mahoney EJ, et al. Modulation of macrophage phenotype by soluble product(s) released from neutrophils. J Immunol. 2005;174(4):2265–2272. doi:10.4049/jimmunol.174.4.2265
19. Koh TJ, DiPietro LA. Inflammation and wound healing: the role of the macrophage. Expert Rev Mol Med. 2011;13:e23. doi:10.1017/S1462399411001943
20. Veith AP, Henderson K, Spencer A, Sligar AD, Baker AB. Therapeutic strategies for enhancing angiogenesis in wound healing. Adv Drug Deliv Rev. 2019;146:97–125. doi:10.1016/j.addr.2018.09.010
21. Rippa AL, Kalabusheva EP, Vorotelyak EA. Regeneration of dermis: scarring and cells involved. Cells. 2019;8(6):607. doi:10.3390/cells8060607
22. Hinz B. Formation and function of the myofibroblast during tissue repair. J Invest Dermatol. 2007;127(3):526–537. doi:10.1038/sj.jid.5700613
23. Sorg H, Krueger C, Vollmar B. Intravital insights in skin wound healing using the mouse dorsal skin fold chamber. J Anat. 2007;211(6):810–818. doi:10.1111/j.1469-7580.2007.00822.x
24. Gonzalez AC, Costa TF, Andrade ZA, Medrado AR. Wound healing - a literature review. An Bras Dermatol. 2016;91(5):614–620. doi:10.1590/abd1806-4841.20164741
25. Midwood KS, Williams LV, Schwarzbauer JE. Tissue repair and the dynamics of the extracellular matrix. Int J Biochem Cell Biol. 2004;36(6):1031–1037. doi:10.1016/j.biocel.2003.12.003
26. Eming SA, Martin P, Tomic-Canic M. Wound repair and regeneration: mechanisms, signaling, and translation. Sci Transl Med. 2014;6(265):265sr266. doi:10.1126/scitranslmed.3009337
27. Brem H, Tomic-Canic M. Cellular and molecular basis of wound healing in diabetes. J Clin Invest. 2007;117(5):1219–1222. doi:10.1172/JCI32169
28. Schreml S, Szeimies RM, Prantl L, Karrer S, Landthaler M, Babilas P. Oxygen in acute and chronic wound healing. Br J Dermatol. 2010;163(2):257–268. doi:10.1111/j.1365-2133.2010.09804.x
29. Desmet CM, Preat V, Gallez B. Nanomedicines and gene therapy for the delivery of growth factors to improve perfusion and oxygenation in wound healing. Adv Drug Deliv Rev. 2018;129:262–284. doi:10.1016/j.addr.2018.02.001
30. Gurtner GC, Werner S, Barrandon Y, Longaker MT. Wound repair and regeneration. Nature. 2008;453(7193):314–321. doi:10.1038/nature07039
31. Feldman EL, Callaghan BC, Pop-Busui R, et al. Diabetic neuropathy. Nat Rev Dis Primers. 2019;5(1):41. doi:10.1038/s41572-019-0092-1
32. Bauer SM, Bauer RJ, Velazquez OC. Angiogenesis, vasculogenesis, and induction of healing in chronic wounds. Vasc Endovascular Surg. 2005;39(4):293–306. doi:10.1177/153857440503900401
33. Huang SM, Wu CS, Chiu MH, et al. High glucose environment induces M1 macrophage polarization that impairs keratinocyte migration via TNF-alpha: an important mechanism to delay the diabetic wound healing. J Dermatol Sci. 2019;96(3):159–167. doi:10.1016/j.jdermsci.2019.11.004
34. Khanna S, Biswas S, Shang Y, et al. Macrophage dysfunction impairs resolution of inflammation in the wounds of diabetic mice. PLoS One. 2010;5(3):e9539. doi:10.1371/journal.pone.0009539
35. Baltzis D, Eleftheriadou I, Veves A. Pathogenesis and treatment of impaired wound healing in diabetes mellitus: new insights. Adv Ther. 2014;31(8):817–836. doi:10.1007/s12325-014-0140-x
36. Gordon KA, Lebrun EA, Tomic-Canic M, Kirsner RS. The role of surgical debridement in healing of diabetic foot ulcers. Skinmed. 2012;10(1):24–26.
37. Cavanagh PR, Bus SA. Off-loading the diabetic foot for ulcer prevention and healing. J Vasc Surg. 2010;52(3 Suppl):37S–43S. doi:10.1016/j.jvs.2010.06.007
38. Tecilazich F, Dinh TL, Veves A. Emerging drugs for the treatment of diabetic ulcers. Expert Opin Emerg Drugs. 2013;18(2):207–217. doi:10.1517/14728214.2013.802305
39. Dumville JC, Deshpande S, O’Meara S, Speak K. Hydrocolloid dressings for healing diabetic foot ulcers. Cochrane Database Syst Rev. 2013;2013(8):CD009099. doi:10.1002/14651858.CD009099.pub3
40. Moura LI, Dias AM, Carvalho E, de Sousa HC. Recent advances on the development of wound dressings for diabetic foot ulcer treatment--a review. Acta Biomater. 2013;9(7):7093–7114. doi:10.1016/j.actbio.2013.03.033
41. Cavanagh PR, Bus SA. Off-loading the diabetic foot for ulcer prevention and healing. Plast Reconstr Surg. 2011;127(Suppl 1):248S–256S. doi:10.1097/PRS.0b013e3182024864
42. Spencer S. Pressure relieving interventions for preventing and treating diabetic foot ulcers. Cochrane Database Syst Rev. 2000;(3):CD002302. doi:10.1002/14651858.CD002302
43. Fernando ME, Crowther RG, Pappas E, et al. Plantar pressure in diabetic peripheral neuropathy patients with active foot ulceration, previous ulceration and no history of ulceration: a meta-analysis of observational studies. PLoS One. 2014;9(6):e99050. doi:10.1371/journal.pone.0099050
44. Albayati MA, Shearman CP. Peripheral arterial disease and bypass surgery in the diabetic lower limb. Med Clin North Am. 2013;97(5):821–834. doi:10.1016/j.mcna.2013.03.009
45. Lipsky BA, Peters EJ, Berendt AR, et al. Specific guidelines for the treatment of diabetic foot infections 2011. Diabetes Metab Res Rev. 2012;28(Suppl 1):234–235. doi:10.1002/dmrr.2251
46. Lipsky BA, Berendt AR, Cornia PB, et al. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;54(12):e132–173. doi:10.1093/cid/cis346
47. Gonzalez Gomez A, Hosseinidoust Z. Liposomes for antibiotic encapsulation and delivery. ACS Infect Dis. 2020;6(5):896–908. doi:10.1021/acsinfecdis.9b00357
48. Steed DL, Attinger C, Colaizzi T, et al. Guidelines for the treatment of diabetic ulcers. Wound Repair Regen. 2006;14(6):680–692. doi:10.1111/j.1524-475X.2006.00176.x
49. Fernando ME, Seneviratne RM, Tan YM, et al. Intensive versus conventional glycaemic control for treating diabetic foot ulcers. Cochrane Database Syst Rev. 2016;2016(1):CD010764. doi:10.1002/14651858.CD010764.pub2
50. Maier HM, Ilich JZ, Kim JS, Spicer MT. Nutrition supplementation for diabetic wound healing: a systematic review of current literature. Skinmed. 2013;11(4):217–224; quiz 224–215.
51. Park JW, Hwang SR, Yoon IS. Advanced growth factor delivery systems in wound management and skin regeneration. Molecules. 2017;22(8):1259. doi:10.3390/molecules22081259
52. Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Growth factors and cytokines in wound healing. Wound Repair Regen. 2008;16(5):585–601. doi:10.1111/j.1524-475X.2008.00410.x
53. Borena BM, Martens A, Broeckx SY, et al. Regenerative skin wound healing in mammals: state-of-the-art on growth factor and stem cell based treatments. Cell Physiol Biochem. 2015;36(1):1–23. doi:10.1159/000374049
54. Apte RS, Chen DS, Ferrara N. VEGF in signaling and disease: beyond discovery and development. Cell. 2019;176(6):1248–1264. doi:10.1016/j.cell.2019.01.021
55. Johnson KE, Wilgus TA. Vascular endothelial growth factor and angiogenesis in the regulation of cutaneous wound repair. Adv Wound Care. 2014;3(10):647–661. doi:10.1089/wound.2013.0517
56. Haase I, Evans R, Pofahl R, Watt FM. Regulation of keratinocyte shape, migration and wound epithelialization by IGF-1- and EGF-dependent signalling pathways. J Cell Sci. 2003;116(Pt 15):3227–3238. doi:10.1242/jcs.00610
57. Yun YR, Won JE, Jeon E, et al. Fibroblast growth factors: biology, function, and application for tissue regeneration. J Tissue Eng. 2010;2010:218142. doi:10.4061/2010/218142
58. Cooper DM, Yu EZ, Hennessey P, Ko F, Robson MC. Determination of endogenous cytokines in chronic wounds. Ann Surg. 1994;219(6):688–691;discussion 691–682. doi:10.1097/00000658-199406000-00012
59. Koria P. Delivery of growth factors for tissue regeneration and wound healing. BioDrugs. 2012;26(3):163–175. doi:10.2165/11631850-000000000-00000
60. Fernandez-Montequin JI, Betancourt BY, Leyva-Gonzalez G, et al. Intralesional administration of epidermal growth factor-based formulation (Heberprot-P) in chronic diabetic foot ulcer: treatment up to complete wound closure. Int Wound J. 2009;6(1):67–72. doi:10.1111/j.1742-481X.2008.00561.x
61. Hong JP, Jung HD, Kim YW. Recombinant human epidermal growth factor (EGF) to enhance healing for diabetic foot ulcers. Ann Plast Surg. 2006;56(4):394–398;discussion 399–400. doi:10.1097/01.sap.0000198731.12407.0c
62. Quatresooz P, Henry F, Paquet P, Pierard-Franchimont C, Harding K, Pierard GE. Deciphering the impaired cytokine cascades in chronic leg ulcers (review). Int J Mol Med. 2003;11(4):411–418.
63. Lee YH, Hong YL, Wu TL. Novel silver and nanoparticle-encapsulated growth factor co-loaded chitosan composite hydrogel with sustained antimicrobility and promoted biological properties for diabetic wound healing. Mater Sci Eng C Mater Biol Appl. 2021;118:111385. doi:10.1016/j.msec.2020.111385
64. Augustine R, Hasan A, Dalvi YB, et al. Growth factor loaded in situ photocrosslinkable poly(3-hydroxybutyrate-co-3-hydroxyvalerate)/gelatin methacryloyl hybrid patch for diabetic wound healing. Mater Sci Eng C Mater Biol Appl. 2021;118:111519. doi:10.1016/j.msec.2020.111519
65. Shi X, Jiang L, Zhao X, et al. Adipose-derived stromal cell-sheets sandwiched, book-shaped acellular dermal matrix capable of sustained release of basic fibroblast growth factor promote diabetic wound healing. Front Cell Dev Biol. 2021;9:646967. doi:10.3389/fcell.2021.646967
66. Dwivedi C, Pandey I, Pandey H, et al. In vivo diabetic wound healing with nanofibrous scaffolds modified with gentamicin and recombinant human epidermal growth factor. J Biomed Mater Res A. 2018;106(3):641–651. doi:10.1002/jbm.a.36268
67. Lee YH, Lin SJ. Chitosan/PVA hetero-composite hydrogel containing antimicrobials, perfluorocarbon nanoemulsions, and growth factor-loaded nanoparticles as a multifunctional dressing for diabetic wound healing: synthesis, characterization, and in vitro/in vivo evaluation. Pharmaceutics. 2022;14(3). doi:10.3390/pharmaceutics14030537
68. Tiaka EK, Papanas N, Manolakis AC, Georgiadis GS. Epidermal growth factor in the treatment of diabetic foot ulcers: an update. Perspect Vasc Surg Endovasc Ther. 2012;24(1):37–44. doi:10.1177/1531003512442093
69. Hajimiri M, Shahverdi S, Esfandiari MA, et al. Preparation of hydrogel embedded polymer-growth factor conjugated nanoparticles as a diabetic wound dressing. Drug Dev Ind Pharm. 2016;42(5):707–719. doi:10.3109/03639045.2015.1075030
70. Santhini E, Parthasarathy R, Shalini M, Dhivya S, Mary LA, Padma VV. Bio inspired growth factor loaded self assembling peptide nano hydrogel for chronic wound healing. Int J Biol Macromol. 2022;197:77–87. doi:10.1016/j.ijbiomac.2021.12.026
71. Acosta JB, Savigne W, Valdez C, et al. Epidermal growth factor intralesional infiltrations can prevent amputation in patients with advanced diabetic foot wounds. Int Wound J. 2006;3(3):232–239. doi:10.1111/j.1742-481X.2006.00237.x
72. Tuyet HL, Nguyen Quynh TT, Vo Hoang Minh H, et al. The efficacy and safety of epidermal growth factor in treatment of diabetic foot ulcers: the preliminary results. Int Wound J. 2009;6(2):159–166. doi:10.1111/j.1742-481X.2009.00594.x
73. Augustine R, Kalarikkal N, Thomas S. Advancement of wound care from grafts to bioengineered smart skin substitutes. Prog Biomater. 2014;3(2–4):103–113. doi:10.1007/s40204-014-0030-y
74. Wang W, Yang C, Wang XY, et al. MicroRNA-129 and −335 promote diabetic wound healing by inhibiting Sp1-mediated MMP-9 expression. Diabetes. 2018;67(8):1627–1638. doi:10.2337/db17-1238
75. Pack DW, Hoffman AS, Pun S, Stayton PS. Design and development of polymers for gene delivery. Nat Rev Drug Discov. 2005;4(7):581–593. doi:10.1038/nrd1775
76. Yan C, Chen J, Wang C, et al. Milk exosomes-mediated miR-31-5p delivery accelerates diabetic wound healing through promoting angiogenesis. Drug Deliv. 2022;29(1):214–228. doi:10.1080/10717544.2021.2023699
77. Kaczmarek JC, Kowalski PS, Anderson DG. Advances in the delivery of RNA therapeutics: from concept to clinical reality. Genome Med. 2017;9(1):60. doi:10.1186/s13073-017-0450-0
78. Shaabani E, Sharifiaghdam M, Lammens J, et al. Increasing angiogenesis factors in hypoxic diabetic wound conditions by siRNA delivery: additive effect of LbL-gold nanocarriers and desloratadine-induced lysosomal escape. Int J Mol Sci. 2021;22(17):9216. doi:10.3390/ijms22179216
79. Rabbani PS, Zhou A, Borab ZM, et al. Novel lipoproteoplex delivers Keap1 siRNA based gene therapy to accelerate diabetic wound healing. Biomaterials. 2017;132:1–15. doi:10.1016/j.biomaterials.2017.04.001
80. Lan B, Wu J, Li N, et al. Hyperbranched cationic polysaccharide derivatives for efficient siRNA delivery and diabetic wound healing enhancement. Int J Biol Macromol. 2020;154:855–865. doi:10.1016/j.ijbiomac.2020.03.164
81. Lan B, Zhang L, Yang L, et al. Sustained delivery of MMP-9 siRNA via thermosensitive hydrogel accelerates diabetic wound healing. J Nanobiotechnology. 2021;19(1):130. doi:10.1186/s12951-021-00869-6
82. Yang L, Zhang L, Hu J, Wang W, Liu X. Promote anti-inflammatory and angiogenesis using a hyaluronic acid-based hydrogel with miRNA-laden nanoparticles for chronic diabetic wound treatment. Int J Biol Macromol. 2021;166:166–178. doi:10.1016/j.ijbiomac.2020.10.129
83. Nor Azlan AYH, Katas H, Mohamad Zin N, Fauzi MB. Dual action gels containing DsiRNA loaded gold nanoparticles: augmenting diabetic wound healing by promoting angiogenesis and inhibiting infection. Eur J Pharm Biopharm. 2021;169:78–90. doi:10.1016/j.ejpb.2021.09.007
84. Nor Azlan AYH, Katas H, Habideen NH, Mh Busra MF. Dual-action of thermoresponsive gels containing DsiRNA-loaded gold nanoparticles for diabetic wound therapy: characterization, in vitro safety and healing efficacy. Saudi Pharm J. 2020;28(11):1420–1430. doi:10.1016/j.jsps.2020.09.007
85. Tao SC, Rui BY, Wang QY, Zhou D, Zhang Y, Guo SC. Extracellular vesicle-mimetic nanovesicles transport LncRNA-H19 as competing endogenous RNA for the treatment of diabetic wounds. Drug Deliv. 2018;25(1):241–255. doi:10.1080/10717544.2018.1425774
86. Wang S, Yan C, Zhang X, et al. Antimicrobial peptide modification enhances the gene delivery and bactericidal efficiency of gold nanoparticles for accelerating diabetic wound healing. Biomater Sci. 2018;6(10):2757–2772. doi:10.1039/C8BM00807H
87. Nanditha CK, Kumar GSV. Bioactive peptides laden nano and micro-sized particles enriched ECM inspired dressing for skin regeneration in diabetic wounds. Mater Today Bio. 2022;14:100235. doi:10.1016/j.mtbio.2022.100235
88. Certelli A, Valente P, Uccelli A, et al. Robust angiogenesis and arteriogenesis in the skin of diabetic mice by transient delivery of engineered VEGF and PDGF-BB proteins in fibrin hydrogels. Front Bioeng Biotechnol. 2021;9:688467. doi:10.3389/fbioe.2021.688467
89. Thangavel P, Ramachandran B, Chakraborty S, Kannan R, Lonchin S, Muthuvijayan V. Accelerated healing of diabetic wounds treated with l-glutamic acid loaded hydrogels through enhanced collagen deposition and angiogenesis: an in vivo study. Sci Rep. 2017;7(1):10701. doi:10.1038/s41598-017-10882-1
90. Zheng Z, Liu Y, Huang W, et al. Neurotensin-loaded PLGA/CNC composite nanofiber membranes accelerate diabetic wound healing. Artif Cells Nanomed Biotechnol. 2018;46(sup2):493–501. doi:10.1080/21691401.2018.1460372
91. Hu C, Liu W, Long L, et al. Microenvironment-responsive multifunctional hydrogels with spatiotemporal sequential release of tailored recombinant human collagen type III for the rapid repair of infected chronic diabetic wounds. J Mater Chem B. 2021;9(47):9684–9699. doi:10.1039/D1TB02170B
92. Hsueh YS, Shyong YJ, Yu HC, et al. Nanostructured lipid carrier gel formulation of recombinant human thrombomodulin improve diabetic wound healing by topical administration. Pharmaceutics. 2021;13(9):1386. doi:10.3390/pharmaceutics13091386
93. Dewberry LC, Niemiec SM, Hilton SA, et al. Cerium oxide nanoparticle conjugation to microRNA-146a mechanism of correction for impaired diabetic wound healing. Nanomedicine. 2022;40:102483. doi:10.1016/j.nano.2021.102483
94. Shi R, Li H, Jin X, et al. Promoting Re-epithelialization in an oxidative diabetic wound microenvironment using self-assembly of a ROS-responsive polymer and P311 peptide micelles. Acta Biomater. 2022;152:425–439. doi:10.1016/j.actbio.2022.09.017
95. Jiang JS, Zang J, Ru Y, et al. Patient-driven discovery of CCN1 to rescue cutaneous wound healing in diabetes via the intracellular EIF3A/CCN1/ATG7 signaling by nanoparticle-enabled delivery. Biomaterials. 2022;288:121698. doi:10.1016/j.biomaterials.2022.121698
96. Zha W, Wang J, Guo Z, et al. Efficient delivery of VEGF-A mRNA for promoting diabetic wound healing via ionizable lipid nanoparticles. Int J Pharm. 2022;632:122565. doi:10.1016/j.ijpharm.2022.122565
97. Kolios G, Moodley Y. Introduction to stem cells and regenerative medicine. Respiration. 2013;85(1):3–10. doi:10.1159/000345615
98. Behr B, Ko SH, Wong VW, Gurtner GC, Longaker MT. Stem cells. Plast Reconstr Surg. 2010;126(4):1163–1171. doi:10.1097/PRS.0b013e3181ea42bb
99. Costa LA, Eiro N, Fraile M, et al. Functional heterogeneity of mesenchymal stem cells from natural niches to culture conditions: implications for further clinical uses. Cell Mol Life Sci. 2021;78(2):447–467. doi:10.1007/s00018-020-03600-0
100. Ebrahimian TG, Pouzoulet F, Squiban C, et al. Cell therapy based on adipose tissue-derived stromal cells promotes physiological and pathological wound healing. Arterioscler Thromb Vasc Biol. 2009;29(4):503–510. doi:10.1161/ATVBAHA.108.178962
101. Xu Q, Gao AS, Gao Y, et al. A hybrid injectable hydrogel from hyperbranched PEG macromer as a stem cell delivery and retention platform for diabetic wound healing. Acta Biomater. 2018;75:63–74. doi:10.1016/j.actbio.2018.05.039
102. Jin X, Shang Y, Zou Y, et al. Injectable hypoxia-induced conductive hydrogel to promote diabetic wound healing. ACS Appl Mater Interfaces. 2020;12(51):56681–56691. doi:10.1021/acsami.0c13197
103. Trounson A, McDonald C. Stem cell therapies in clinical trials: progress and challenges. Cell Stem Cell. 2015;17(1):11–22. doi:10.1016/j.stem.2015.06.007
104. Batrakova EV, Kim MS. Using exosomes, naturally-equipped nanocarriers, for drug delivery. J Control Release. 2015;219:396–405. doi:10.1016/j.jconrel.2015.07.030
105. Thery C, Amigorena S, Raposo G, Clayton A. Isolation and characterization of exosomes from cell culture supernatants and biological fluids. Curr Protoc Cell Biol. 2006;Chapter 3:Unit 3 22. doi:10.1002/0471143030.cb0322s30
106. Chen S, Wang H, Su Y, et al. Mesenchymal stem cell-laden, personalized 3D scaffolds with controlled structure and fiber alignment promote diabetic wound healing. Acta Biomater. 2020;108:153–167. doi:10.1016/j.actbio.2020.03.035
107. Mohanty C, Pradhan J. A human epidermal growth factor-curcumin bandage bioconjugate loaded with mesenchymal stem cell for in vivo diabetic wound healing. Mater Sci Eng C Mater Biol Appl. 2020;111:110751. doi:10.1016/j.msec.2020.110751
108. Shi Q, Qian Z, Liu D, et al. GMSC-derived exosomes combined with a chitosan/silk hydrogel sponge accelerates wound healing in a diabetic rat skin defect model. Front Physiol. 2017;8:904. doi:10.3389/fphys.2017.00904
109. Fu J, Zhang Y, Chu J, et al. Reduced graphene oxide incorporated acellular dermal composite scaffold enables efficient local delivery of mesenchymal stem cells for accelerating diabetic wound healing. ACS Biomater Sci Eng. 2019;5(8):4054–4066. doi:10.1021/acsbiomaterials.9b00485
110. Xin Y, Xu P, Wang X, Chen Y, Zhang Z, Zhang Y. Human foreskin-derived dermal stem/progenitor cell-conditioned medium combined with hyaluronic acid promotes extracellular matrix regeneration in diabetic wounds. Stem Cell Res Ther. 2021;12(1):49. doi:10.1186/s13287-020-02116-5
111. Yang J, Chen Z, Pan D, Li H, Shen J. Umbilical cord-derived mesenchymal stem cell-derived exosomes combined pluronic F127 hydrogel promote chronic diabetic wound healing and complete skin regeneration. Int J Nanomedicine. 2020;15:5911–5926. doi:10.2147/IJN.S249129
112. Xu N, Wang L, Guan J, et al. Wound healing effects of a Curcuma zedoaria polysaccharide with platelet-rich plasma exosomes assembled on chitosan/silk hydrogel sponge in a diabetic rat model. Int J Biol Macromol. 2018;117:102–107. doi:10.1016/j.ijbiomac.2018.05.066
113. Zhang Y, Jiang W, Kong L, Fu J, Zhang Q, Liu H. PLGA@IL-8 nanoparticles-loaded acellular dermal matrix as a delivery system for exogenous MSCs in diabetic wound healing. Int J Biol Macromol. 2023;224:688–698. doi:10.1016/j.ijbiomac.2022.10.157
114. Mazini L, Rochette L, Admou B, Amal S, Malka G. Hopes and limits of adipose-derived stem cells (ADSCs) and mesenchymal stem cells (MSCs) in wound healing. Int J Mol Sci. 2020;21(4):1306. doi:10.3390/ijms21041306
115. Zhao L, Niu L, Liang H, Tan H, Liu C, Zhu F. pH and glucose dual-responsive injectable hydrogels with insulin and fibroblasts as bioactive dressings for diabetic wound healing. ACS Appl Mater Interfaces. 2017;9(43):37563–37574. doi:10.1021/acsami.7b09395
116. Jee JP, Pangeni R, Jha SK, Byun Y, Park JW. Preparation and in vivo evaluation of a topical hydrogel system incorporating highly skin-permeable growth factors, quercetin, and oxygen carriers for enhanced diabetic wound-healing therapy. Int J Nanomedicine. 2019;14:5449–5475. doi:10.2147/IJN.S213883
117. Xu X, Wang X, Qin C, Khan AUR, Zhang W, Mo X. Silk fibroin/poly-(L-lactide-co-caprolactone) nanofiber scaffolds loaded with Huangbai Liniment to accelerate diabetic wound healing. Colloids Surf B Biointerfaces. 2021;199:111557. doi:10.1016/j.colsurfb.2021.111557
118. Ren X, Han Y, Wang J, et al. An aligned porous electrospun fibrous membrane with controlled drug delivery - An efficient strategy to accelerate diabetic wound healing with improved angiogenesis. Acta Biomater. 2018;70:140–153. doi:10.1016/j.actbio.2018.02.010
119. Wang T, Zheng Y, Shi Y, Zhao L. pH-responsive calcium alginate hydrogel laden with protamine nanoparticles and hyaluronan oligosaccharide promotes diabetic wound healing by enhancing angiogenesis and antibacterial activity. Drug Deliv Transl Res. 2019;9(1):227–239. doi:10.1007/s13346-018-00609-8
120. Hu B, Gao M, Boakye-Yiadom KO, et al. An intrinsically bioactive hydrogel with on-demand drug release behaviors for diabetic wound healing. Bioact Mater. 2021;6(12):4592–4606. doi:10.1016/j.bioactmat.2021.04.040
121. Razzaq A, Khan ZU, Saeed A, et al. Development of cephradine-loaded gelatin/polyvinyl alcohol electrospun nanofibers for effective diabetic wound healing: in-vitro and in-vivo assessments. Pharmaceutics. 2021;13(3):349. doi:10.3390/pharmaceutics13030349
122. Cam ME, Yildiz S, Alenezi H, et al. Evaluation of burst release and sustained release of pioglitazone-loaded fibrous mats on diabetic wound healing: an in vitro and in vivo comparison study. J R Soc Interface. 2020;17(162):20190712. doi:10.1098/rsif.2019.0712
123. Yin M, Wu J, Deng M, et al. Multifunctional magnesium organic framework-based microneedle patch for accelerating diabetic wound healing. ACS Nano. 2021;15:17842–17853. doi:10.1021/acsnano.1c06036
124. Abdel Khalek MA, Abdel Gaber SA, El-Domany RA, El-Kemary MA. Photoactive electrospun cellulose acetate/polyethylene oxide/methylene blue and trilayered cellulose acetate/polyethylene oxide/silk fibroin/ciprofloxacin nanofibers for chronic wound healing. Int J Biol Macromol. 2021;193(Pt B):1752–1766. doi:10.1016/j.ijbiomac.2021.11.012
125. Liu J, Chen Z, Wang J, et al. Encapsulation of curcumin nanoparticles with MMP9-responsive and thermos-sensitive hydrogel improves diabetic wound healing. ACS Appl Mater Interfaces. 2018;10(19):16315–16326. doi:10.1021/acsami.8b03868
126. Shah SA, Sohail M, Karperien M, Johnbosco C, Mahmood A, Kousar M. Chitosan and carboxymethyl cellulose-based 3D multifunctional bioactive hydrogels loaded with nano-curcumin for synergistic diabetic wound repair. Int J Biol Macromol. 2023;227:1203–1220. doi:10.1016/j.ijbiomac.2022.11.307
127. Saha K, Ghosh A, Bhattacharya T, Ghosh S, Dey S, Chattopadhyay D. Ameliorative effects of clindamycin - nanoceria conjugate: a ROS responsive smart drug delivery system for diabetic wound healing study. J Trace Elem Med Biol. 2023;75:127107. doi:10.1016/j.jtemb.2022.127107
128. Almukainzi M, El-Masry TA, Negm WA, et al. Co-delivery of gentiopicroside and thymoquinone using electrospun m-PEG/PVP nanofibers: in-vitro and in vivo studies for antibacterial wound dressing in diabetic rats. Int J Pharm. 2022;625:122106. doi:10.1016/j.ijpharm.2022.122106
129. Zhang P, He L, Zhang J, et al. Preparation of novel berberine nano-colloids for improving wound healing of diabetic rats by acting Sirt1/NF-kappaB pathway. Colloids Surf B Biointerfaces. 2020;187:110647. doi:10.1016/j.colsurfb.2019.110647
130. Zhu W, Dong Y, Xu P, et al. A composite hydrogel containing resveratrol-laden nanoparticles and platelet-derived extracellular vesicles promotes wound healing in diabetic mice. Acta Biomater. 2022;154:212–230. doi:10.1016/j.actbio.2022.10.038
131. Narisepalli S, Salunkhe SA, Chitkara D, Mittal A. Asiaticoside polymeric nanoparticles for effective diabetic wound healing through increased collagen biosynthesis: in-vitro and in-vivo evaluation. Int J Pharm. 2023;631:122508. doi:10.1016/j.ijpharm.2022.122508
132. Kant V, Gopal A, Pathak NN, Kumar P, Tandan SK, Kumar D. Antioxidant and anti-inflammatory potential of curcumin accelerated the cutaneous wound healing in streptozotocin-induced diabetic rats. Int Immunopharmacol. 2014;20(2):322–330. doi:10.1016/j.intimp.2014.03.009
133. Phan TT, See P, Lee ST, Chan SY. Protective effects of curcumin against oxidative damage on skin cells in vitro: its implication for wound healing. J Trauma. 2001;51(5):927–931. doi:10.1097/00005373-200111000-00017
134. Wan S, Sun Y, Qi X, Tan F. Improved bioavailability of poorly water-soluble drug curcumin in cellulose acetate solid dispersion. AAPS PharmSciTech. 2012;13(1):159–166. doi:10.1208/s12249-011-9732-9
135. Rai MK, Deshmukh SD, Ingle AP, Gade AK. Silver nanoparticles: the powerful nanoweapon against multidrug-resistant bacteria. J Appl Microbiol. 2012;112(5):841–852. doi:10.1111/j.1365-2672.2012.05253.x
136. Khatoon N, Alam H, Khan A, Raza K, Sardar M. Ampicillin Silver Nanoformulations against Multidrug resistant bacteria. Sci Rep. 2019;9(1):6848. doi:10.1038/s41598-019-43309-0
137. Wang P, Jiang S, Li Y, et al. Virus-like mesoporous silica-coated plasmonic Ag nanocube with strong bacteria adhesion for diabetic wound ulcer healing. Nanomedicine. 2021;34:102381. doi:10.1016/j.nano.2021.102381
138. Li X, Robinson SM, Gupta A, et al. Functional gold nanoparticles as potent antimicrobial agents against multi-drug-resistant bacteria. ACS Nano. 2014;8(10):10682–10686. doi:10.1021/nn5042625
139. Tao B, Lin C, Deng Y, et al. Copper-nanoparticle-embedded hydrogel for killing bacteria and promoting wound healing with photothermal therapy. J Mater Chem B. 2019;7(15):2534–2548. doi:10.1039/C8TB03272F
140. Hong WX, Hu MS, Esquivel M, et al. The role of hypoxia-inducible factor in wound healing. Adv Wound Care. 2014;3(5):390–399. doi:10.1089/wound.2013.0520
141. Jude EB, Apelqvist J, Spraul M, Martini J. Prospective randomized controlled study of Hydrofiber dressing containing ionic silver or calcium alginate dressings in non-ischaemic diabetic foot ulcers. Diabet Med. 2007;24(3):280–288. doi:10.1111/j.1464-5491.2007.02079.x
142. Huang YY, Lin CW, Cheng NC, et al. Effect of a novel macrophage-regulating drug on wound healing in patients with diabetic foot ulcers: a randomized clinical trial. JAMA Netw Open. 2021;4(9):e2122607. doi:10.1001/jamanetworkopen.2021.22607
143. Chandra PK, Ross CL, Smith LC, et al. Peroxide-based oxygen generating topical wound dressing for enhancing healing of dermal wounds. Wound Repair Regen. 2015;23(6):830–841. doi:10.1111/wrr.12324
144. Guan Y, Niu H, Liu Z, et al. Sustained oxygenation accelerates diabetic wound healing by promoting epithelialization and angiogenesis and decreasing inflammation. Sci Adv. 2021;7(35). doi:10.1126/sciadv.abj0153
145. Shiekh PA, Singh A, Kumar A. Exosome laden oxygen releasing antioxidant and antibacterial cryogel wound dressing OxOBand alleviate diabetic and infectious wound healing. Biomaterials. 2020;249:120020. doi:10.1016/j.biomaterials.2020.120020
146. Wang Q, Qiu W, Li M, et al. Multifunctional hydrogel platform for biofilm scavenging and O2 generating with photothermal effect on diabetic chronic wound healing. J Colloid Interface Sci. 2022;617:542–556. doi:10.1016/j.jcis.2022.03.040
147. Li Y, Fu R, Duan Z, Zhu C, Fan D. Artificial nonenzymatic antioxidant mxene nanosheet-anchored injectable hydrogel as a mild photothermal-controlled oxygen release platform for diabetic wound healing. ACS Nano. 2022;16:7486–7502.
148. Ahmed R, Afreen A, Tariq M, et al. Bone marrow mesenchymal stem cells preconditioned with nitric-oxide-releasing chitosan/PVA hydrogel accelerate diabetic wound healing in rabbits. Biomed Mater. 2021;16(3):035014. doi:10.1088/1748-605X/abc28b
149. Zahid AA, Augustine R, Dalvi YB, et al. Development of nitric oxide releasing visible light crosslinked gelatin methacrylate hydrogel for rapid closure of diabetic wounds. Biomed Pharmacother. 2021;140:111747. doi:10.1016/j.biopha.2021.111747
150. Yao S, Wang Y, Chi J, et al. Porous MOF microneedle array patch with photothermal responsive nitric oxide delivery for wound healing. Adv Sci. 2022;9(3):e2103449. doi:10.1002/advs.202103449
151. Chen YJ, Wu SC, Wang HC, et al. Activation of angiogenesis and wound healing in diabetic mice using NO-delivery dinitrosyl iron complexes. Mol Pharm. 2019;16(10):4241–4251. doi:10.1021/acs.molpharmaceut.9b00586
152. Yu X, Fu X, Yang J, et al. Glucose/ROS cascade-responsive ceria nanozymes for diabetic wound healing. Mater Today Bio. 2022;15:100308. doi:10.1016/j.mtbio.2022.100308
153. Deng M, Zhang M, Huang R, et al. Diabetes immunity-modulated multifunctional hydrogel with cascade enzyme catalytic activity for bacterial wound treatment. Biomaterials. 2022;289:121790. doi:10.1016/j.biomaterials.2022.121790
154. Khan AUR, Huang K, Khalaji MS, et al. Multifunctional bioactive core-shell electrospun membrane capable to terminate inflammatory cycle and promote angiogenesis in diabetic wound. Bioact Mater. 2021;6(9):2783–2800. doi:10.1016/j.bioactmat.2021.01.040
155. Riccio DA, Schoenfisch MH. Nitric oxide release: part I. Macromolecular scaffolds. Chem Soc Rev. 2012;41(10):3731–3741. doi:10.1039/c2cs15272j
156. Qamar Z, Qizilbash FF, Iqubal MK, et al. Nano-based drug delivery system: recent strategies for the treatment of ocular disease and future perspective. Recent Pat Drug Deliv Formul. 2019;13(4):246–254. doi:10.2174/1872211314666191224115211
157. Ahmed KS, Hussein SA, Ali AH, Korma SA, Lipeng Q, Jinghua C. Liposome: composition, characterisation, preparation, and recent innovation in clinical applications. J Drug Target. 2019;27(7):742–761. doi:10.1080/1061186X.2018.1527337
158. Akbarzadeh A, Rezaei-Sadabady R, Davaran S, et al. Liposome: classification, preparation, and applications. Nanoscale Res Lett. 2013;8(1):102. doi:10.1186/1556-276X-8-102
159. Barenholz Y. Doxil(R)--The first FDA-approved nano-drug: lessons learned. J Control Release. 2012;160(2):117–134. doi:10.1016/j.jconrel.2012.03.020
160. Zhang ZJ, Michniak-Kohn B. Flavosomes, novel deformable liposomes for the co-delivery of anti-inflammatory compounds to skin. Int J Pharm. 2020;585:119500. doi:10.1016/j.ijpharm.2020.119500
161. Chhibber S, Kaur J, Kaur S. Liposome entrapment of bacteriophages improves wound healing in a diabetic mouse MRSA infection. Front Microbiol. 2018;9:561. doi:10.3389/fmicb.2018.00561
162. Arora A, Byrem TM, Nair MG, Strasburg GM. Modulation of liposomal membrane fluidity by flavonoids and isoflavonoids. Arch Biochem Biophys. 2000;373(1):102–109. doi:10.1006/abbi.1999.1525
163. Cevc G. Rational design of new product candidates: the next generation of highly deformable bilayer vesicles for noninvasive, targeted therapy. J Control Release. 2012;160(2):135–146. doi:10.1016/j.jconrel.2012.01.005
164. Ternullo S, Basnet P, Holsaeter AM, Flaten GE, de Weerd L, Skalko-Basnet N. Deformable liposomes for skin therapy with human epidermal growth factor: the effect of liposomal surface charge. Eur J Pharm Sci. 2018;125:163–171. doi:10.1016/j.ejps.2018.10.005
165. Huang S, Fu X. Naturally derived materials-based cell and drug delivery systems in skin regeneration. J Control Release. 2010;142(2):149–159. doi:10.1016/j.jconrel.2009.10.018
166. Bonifacio BV, Silva PB, Ramos MA, Negri KM, Bauab TM, Chorilli M. Nanotechnology-based drug delivery systems and herbal medicines: a review. Int J Nanomedicine. 2014;9:1–15. doi:10.2147/IJN.S52634
167. Discher DE, Eisenberg A. Polymer vesicles. Science. 2002;297(5583):967–973. doi:10.1126/science.1074972
168. Ahlawat J, Henriquez G, Narayan M. Enhancing the delivery of chemotherapeutics: role of biodegradable polymeric nanoparticles. Molecules. 2018;23(9):2157. doi:10.3390/molecules23092157
169. Lopes Rocha Correa V, Assis Martins J, Ribeiro de Souza T, et al. Melatonin loaded lecithin-chitosan nanoparticles improved the wound healing in diabetic rats. Int J Biol Macromol. 2020;162:1465–1475. doi:10.1016/j.ijbiomac.2020.08.027
170. Bairagi U, Mittal P, Singh J, Mishra B. Preparation, characterization, and in vivo evaluation of nano formulations of ferulic acid in diabetic wound healing. Drug Dev Ind Pharm. 2018;44(11):1783–1796. doi:10.1080/03639045.2018.1496448
171. Badhwar R, Mangla B, Neupane YR, Khanna K, Popli H. Quercetin loaded silver nanoparticles in hydrogel matrices for diabetic wound healing. Nanotechnology. 2021;32(50):505102. doi:10.1088/1361-6528/ac2536
172. Kaur P, Sharma AK, Nag D, et al. Novel nano-insulin formulation modulates cytokine secretion and remodeling to accelerate diabetic wound healing. Nanomedicine. 2019;15(1):47–57. doi:10.1016/j.nano.2018.08.013
173. Choudhary M, Chhabra P, Tyagi A, Singh H. Scar free healing of full thickness diabetic wounds: a unique combination of silver nanoparticles as antimicrobial agent, calcium alginate nanoparticles as hemostatic agent, fresh blood as nutrient/growth factor supplier and chitosan as base matrix. Int J Biol Macromol. 2021;178:41–52. doi:10.1016/j.ijbiomac.2021.02.133
174. Witzigmann D, Kulkarni JA, Leung J, Chen S, Cullis PR, van der Meel R. Lipid nanoparticle technology for therapeutic gene regulation in the liver. Adv Drug Deliv Rev. 2020;159:344–363. doi:10.1016/j.addr.2020.06.026
175. de Souza ML, Dos Santos WM, de Sousa A, et al. Lipid nanoparticles as a skin wound healing drug delivery system: discoveries and advances. Curr Pharm Des. 2020;26(36):4536–4550. doi:10.2174/1381612826666200417144530
176. Arantes VT, Faraco AAG, Ferreira FB, et al. Retinoic acid-loaded solid lipid nanoparticles surrounded by chitosan film support diabetic wound healing in in vivo study. Colloids Surf B Biointerfaces. 2020;188:110749. doi:10.1016/j.colsurfb.2019.110749
177. Natarajan J, Sanapalli BKR, Bano M, Singh SK, Gulati M, Karri V. Nanostructured lipid carriers of pioglitazone loaded collagen/chitosan composite scaffold for diabetic wound healing. Adv Wound Care. 2019;8(10):499–513. doi:10.1089/wound.2018.0831
178. Sun D, Guo SY, Yang L, et al. Silicone elastomer gel impregnated with 20(S)-protopanaxadiol-loaded nanostructured lipid carriers for ordered diabetic ulcer recovery. Acta Pharmacol Sin. 2020;41(1):119–128. doi:10.1038/s41401-019-0288-7
179. Fenton OS, Olafson KN, Pillai PS, Mitchell MJ, Langer R. Advances in biomaterials for drug delivery. Adv Mater. 2018;e1705328. doi:10.1002/adma.201705328
180. Xue J, Xie J, Liu W, Xia Y. Electrospun nanofibers: new concepts, materials, and applications. Acc Chem Res. 2017;50(8):1976–1987. doi:10.1021/acs.accounts.7b00218
181. Rasouli R, Barhoum A, Bechelany M, Dufresne A. Nanofibers for biomedical and healthcare applications. Macromol Biosci. 2019;19(2):e1800256. doi:10.1002/mabi.201800256
182. Hu X, Liu S, Zhou G, Huang Y, Xie Z, Jing X. Electrospinning of polymeric nanofibers for drug delivery applications. J Control Release. 2014;185:12–21. doi:10.1016/j.jconrel.2014.04.018
183. Cheng H, Yang X, Che X, Yang M, Zhai G. Biomedical application and controlled drug release of electrospun fibrous materials. Mater Sci Eng C Mater Biol Appl. 2018;90:750–763. doi:10.1016/j.msec.2018.05.007
184. Zhang Y, Lim CT, Ramakrishna S, Huang ZM. Recent development of polymer nanofibers for biomedical and biotechnological applications. J Mater Sci Mater Med. 2005;16(10):933–946. doi:10.1007/s10856-005-4428-x
185. Agarwal Y, Rajinikanth PS, Ranjan S, et al. Curcumin loaded polycaprolactone-/polyvinyl alcohol-silk fibroin based electrospun nanofibrous mat for rapid healing of diabetic wound: an in-vitro and in-vivo studies. Int J Biol Macromol. 2021;176:376–386. doi:10.1016/j.ijbiomac.2021.02.025
186. Liu F, Li X, Wang L, et al. Sesamol incorporated cellulose acetate-zein composite nanofiber membrane: an efficient strategy to accelerate diabetic wound healing. Int J Biol Macromol. 2020;149:627–638. doi:10.1016/j.ijbiomac.2020.01.277
187. Lee CH, Hung KC, Hsieh MJ, et al. Core-shell insulin-loaded nanofibrous scaffolds for repairing diabetic wounds. Nanomedicine. 2020;24:102123. doi:10.1016/j.nano.2019.102123
188. Lee CH, Liu KS, Cheng CW, et al. Codelivery of sustainable antimicrobial agents and platelet-derived growth factor via biodegradable nanofibers for repair of diabetic infectious wounds. ACS Infect Dis. 2020;6(10):2688–2697. doi:10.1021/acsinfecdis.0c00321
189. Seliktar D. Designing cell-compatible hydrogels for biomedical applications. Science. 2012;336(6085):1124–1128. doi:10.1126/science.1214804
190. Omrani M, Naimi-Jamal MR, Far BF. The design of multi-responsive nanohydrogel networks of chitosan for controlled drug delivery. Carbohydr Polym. 2022;298:120143. doi:10.1016/j.carbpol.2022.120143
191. Haque ST, Saha SK, Haque ME, Biswas N. Nanotechnology-based therapeutic applications: in vitro and in vivo clinical studies for diabetic wound healing. Biomater Sci. 2021;9(23):7705–7747. doi:10.1039/D1BM01211H
192. Francesko A, Petkova P, Tzanov T. Hydrogel dressings for advanced wound management. Curr Med Chem. 2018;25(41):5782–5797. doi:10.2174/0929867324666170920161246
193. Zhang Y, Zhang P, Gao X, Chang L, Chen Z, Mei X. Preparation of exosomes encapsulated nanohydrogel for accelerating wound healing of diabetic rats by promoting angiogenesis. Mater Sci Eng C Mater Biol Appl. 2021;120:111671. doi:10.1016/j.msec.2020.111671
194. Xiong Y, Chen L, Liu P, et al. All-in-one: multifunctional hydrogel accelerates oxidative diabetic wound healing through timed-release of exosome and fibroblast growth factor. Small. 2022;18(1):e2104229. doi:10.1002/smll.202104229
195. Nidadavolu LS, Stern D, Lin R, et al. Valsartan nano-filaments alter mitochondrial energetics and promote faster healing in diabetic rat wounds. Wound Repair Regen. 2021;29(6):927–937. doi:10.1111/wrr.12974
196. Li Y, Zhang X, He D, Ma Z, Xue K, Li H. 45S5 Bioglass(R) works synergistically with siRNA to downregulate the expression of matrix metalloproteinase-9 in diabetic wounds. Acta Biomater. 2022;145:372–389. doi:10.1016/j.actbio.2022.04.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.