Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Recent Advances in Antibody-Drug Conjugates and Immunotherapy Combinations for Treatment of Triple-Negative Breast Cancer
Authors Chen H, Lu W, Zhou Y ![]() , Guo X, Wu S, Chen Y
, Guo X, Wu S, Chen Y ![]()
Received 29 September 2025
Accepted for publication 4 January 2026
Published 14 January 2026 Volume 2026:18 571054
DOI https://doi.org/10.2147/BCTT.S571054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Huihui Chen,1– 3,* Wei Lu,2– 4,* Yunxiang Zhou,1– 3,* Xianan Guo,1– 3 Shijie Wu,1– 3 Yiding Chen1– 3
1Department of Breast Surgery and Oncology (Key Laboratory of Cancer Prevention and Intervention, China National Ministry of Education, Key Laboratory of Molecular Biology in Medical Sciences), The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Zhejiang Provincial Clinical Research Center for Cancer, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 3Cancer Center, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Colorectal Surgery and Oncology (Key Laboratory of Cancer Prevention and Intervention, China National Ministry of Education, Key Laboratory of Molecular Biology in Medical Sciences), The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yiding Chen, Email [email protected] Wei Lu, Email [email protected]
Abstract: Triple-negative breast cancer (TNBC) remains a therapeutic challenge due to its aggressive nature and lack of ER, PR and HER2 expression. Recent advances, however, are reshaping its treatment landscape, particularly with antibody-drug conjugates (ADCs) and immunotherapies. ADCs such as sacituzumab govitecan and datopotamab deruxtecan have demonstrated superior efficacy over standard chemotherapy in metastatic TNBC. Furthermore, combining these ADCs with immune checkpoint inhibitors is emerging as a powerful strategy to enhance antitumor activity, as evidenced by encouraging results from trials like MORPHEUS-panBC and BEGONIA. While most evidence currently centers on metastatic disease, these novel combinations are also being rapidly evaluated in neoadjuvant and adjuvant settings. Given this rapid progress, this article aims to summarize recent advances in ADCs and immunotherapy combinations for TNBC, discuss their synergistic mechanisms, and provide insights for future personalized therapeutic strategies.
Keywords: triple-negative breast cancer, antibody-drug conjugates, immunotherapy
Introduction
Breast cancer is the most common malignancy among women throughout the world, with an estimated 2.31 million new cases diagnosed and more than 0.66 million deaths worldwide in 2022.1 Triple-negative breast cancer (TNBC) is an aggressive subtype of breast cancer characterized by the lack of expression of estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2).2 Predominantly occurred in young women, TNBC has a greater likelihood of recurrence and is associated with worse prognosis compared with other subtypes of breast cancer.3–5 Since TNBC patients cannot benefit from endocrine and anti-HER2 therapies, surgery, radiotherapy and conventional chemotherapy were considered as the state of the art for TNBC treatment.6 Fortunately, recent studies have unveiled the complex microenvironment and high tumor heterogeneity of TNBC. In response, multiomics-based classification systems like the “Fudan typing” have been proposed.7–10 This system classifies TNBC into four subtypes with distinct molecular features: (1) luminal androgen receptor (LAR), (2) immunomodulatory (IM), (3) basal-like immune-suppressed (BLIS), and (4) mesenchymal-like (MES).10 Consequently, these molecular alterations were assessed to identify various potential targets for TNBC treatment, such as epidermal growth factor receptor (EGFR) inhibitors, poly ADP‐ribose polymerase (PARP) inhibitors, androgen receptor inhibitors and immune checkpoint inhibitors (ICIs) for TNBC patients.10,11
In the past few years, ICIs have emerged as promising therapeutics for various solid tumors such as malignant melanoma, lung cancer, gastrointestinal cancers and cervical cancer,12,13 and TNBC is characterized by genomic instability, higher rates of mutation and more tumor-infiltrating lymphocytes (TILs), which implied that ICIs may be effective for TNBC.14,15 Previous clinical trials such as KEYNOTE-012 (NCT01848834) and KEYNOTE-086 (NCT02447003) reported Pembrolizumab monotherapy had durable anti-tumor activity in PD-L1-positive metastatic TNBC patients,16,17 however the effect of ICI montherapy is limited in PD-L1-positive patients (about 20% of TNBC patients) and the KEYNOTE-119 trial (NCT02555657) showed Pembrolizumab did not significantly improve overall survival (OS) in metastatic TNBC patients compared with investigator-choice chemotherapy.18 Current efforts are concentrating on exploring ICIs combined with other therapies (radiotherapy, chemotherapy, PARP inhibitors, anti-angiogenic therapy and small molecule inhibitors) that may have synergistic benefits to improve patient outcomes, and expanding the patient population eligible for ICIs.19
Antibody-drug conjugates (ADCs) are innovative biopharmaceutical antibodies targeted to specific cell surface antigen (sAg) and conjugated to specific cytotoxic agents (payloads) via synthetic linkers. ADCs selectively deliver highly cytotoxic agents to tumors, offering a promising treatment approach for a range of cancers.20,21 For instance, Trophoblast cell-surface antigen 2 (Trop2) encoded by the TACSTD2 gene is a transmembrane glycoprote and highly expressed in TNBC patients.22 Sacituzumab govitecan (SG) is a first-in-class ADC that targets Trop-2 and conjugated with cytotoxic compound SN-38, which is the active metabolite of topoisomerase I inhibitor irinotecan, and SG monotherapy significantly improved PFS, OS and ORR in metastatic TNBC patients compared with chemotherapy.23 In addition to ADC monotherapy, the current research focus is on the combinations of ADC with other therapies for the treatment of TNBC. Considering the rapid progress of TNBC research, we summarized recent advances in ADCs and immunotherapy combinations in TNBC, discussed the mechanisms underlying their synergistic effect and intended to provide a reference for crafting personalized therapeutic strategies for TNBC patients in the future.
Antibody-Drug Conjugates (ADCs) in TNBC
Trop2 is highly expressed in TNBC patients and over-expression of Trop2 is predictive of worse prognosis. SG was the first FDA-approved ADC drug targeting Trop2 for metastatic TNBC patients who received prior lines of treatment.22 Unlike most ADCs that carry highly potent payloads with picomolar IC50 values and a limited therapeutic window, the relative lower potency of SN38 (with nanomolar IC50) allows for a higher drug-to-antibody ratio (DAR).24 In the multicenter Phase I/II basket trial IMMU-132-01 (NCT01631552), patients with various refractory metastatic epithelial cancers who had at least one prior line standard therapy received SG monotherapy. The results of TNBC subgroup showed the ORR of SG was 33.3%, and median OS and PFS were reported as 13.0 and 5.5 months, respectively.25 After the inspiring results of the IMMU-132-01 trial, the Phase III ASCENT trial (NCT02574455) was designed to investigate the efficacy of SG as subsequent-line treatment in metastatic TNBC patients compared with treatment of physician’s choice (TPC) chemotherapy. In the final analysis of the ASCENT trial, SG showed significantly improved PFS (4.8 months vs 1.7 months), OS (11.8 months vs 6.9 months) and ORR (31% vs 4%) in metastatic TNBC patients compared with TPC chemotherapy.23 The subgroup analysis of ASCENT trial revealed that SG improved PFS, OS and ORR compared with TPC chemotherapy across all levels of Trop2 expression, and the improvement was more significant with higher Trop2 levels. The efficacy of SG in the Trop2 low expression group could be attributed to ADCs’ bystander effect, which means the killing of neighboring antigen-negative cells by antigen-positive cells that are targeted by ADCs and drugs are released.26 Following the inspiring results of the ASCENT trial, the ASCENT-03 trial (NCT05382299) was designed to further investigate the efficacy of SG as first-line treatment in metastatic TNBC patients compared with TPC chemotherapy.27 This study included patients with either PD-L1-negative or PD-L1-positive tumors who received an anti-PD-(L)1 inhibitor in the curative setting. The primary endpoints are PFS, and the study will enroll about 540 participants. Apart from metastatic TNBC, the ongoing SASCIA trial (NCT04595565) was designed to evaluate the efficacy of SG in primary HER2-negative breast cancer patients with residual disease after standard neoadjuvant treatment.28 There are growing numbers of clinical trials investigating the combinations of SG with other agents, and the combinations of SG and immune therapies will be discussed in the following sections.
Another Trop2-targeted ADC is Datopotamab deruxtecan (Dato-DXd), a humanized anti-Trop2 antibody conjugated with a potent topoisomerase I inhibitor DXd.29 Dato-DXd has longer half-life than SG, and it can remain in the circulation for a more prolonged duration.30 The TROPION-PanTumor01 trial (NCT03401385) was a Phase I study that investigated the efficacy and safety of Dato-DXd in patients with previously treated solid tumors, and the ORR was 31.8% and the median PFS was 4.4 months in the TNBC subgroup.31 This promising result led to the design of the ongoing TROPION-Breast02 trial (NCT05374512), which evaluated the efficacy and safety of Dato-DXd compared with chemotherapy in previously untreated locally recurrent inoperable or metastatic TNBC, who were ineligible for immune therapy.32
Sacituzumab tirumotecan, also known as SKB264 or MK-2870, is also a Trop2-targeted ADC developed with a novel linker and conjugated with a belotecan-derivative topoisomerase I inhibitor KL610023. The phase III trial OptiTROP-Breast01 (NCT05347134) was designed to compare the efficacy of SKB264 monotherapy with TPC chemotherapy in locally recurrent or metastatic TNBC.33 The interim analysis showed that the primary endpoint of PFS was met, and SKB264 significantly improved PFS compared with TPC chemotherapy (5.7 months vs 2.3 months), and better PFS benefits were observed regardless of Trop2 expression levels according to subgroup analysis. The median OS was not reached with SKB264 and 9.4 months with TPC chemotherapy, and the ORR was 43.8% with SKB264 and 12.8% with TPC chemotherapy.
Trastuzumab deruxtecan, also known as DS-8201a or T-DXd, is an ADC formed by conjugating an anti-HER2 monoclonal antibody with Dxd.34 Previous phase II/III clinical trials have demonstrated that T-DXd showed reliable anti-tumor effect in HER2-postive metastatic breast cancer patients, leading to its approval for HER2-postive metastatic breast cancer.35,36 As an ADC targeting HER2, T-DXd also showed significant anti-tumor activity in HER2 low expression breast cancers.36 This phenomenon is also attributed to ADCs’ bystander effect, since about 60% of HER2- breast cancers are considered as HER2 low expression (score of 1+ on IHC or score of 2+ on IHC without gene amplification confirmed by FISH).37 The phase III DESTINY-Breast04 trial (NCT03734029) compared the efficacy of T-DXd with TPC chemotherapy in previously treated HER2-low metastatic breast cancer, and the results showed that T-DXd significantly improved PFS (8.5 months vs 2.9 months) and OS (18.2 months vs 8.3 months) compared with TPC chemotherapy in the metastatic TNBC subgroup.38 In addition, T-DXd is also effective in breast cancer patients with ultralow HER2 expression (score of 0 on IHC membrane staining). The DESTINY-Breast06 trial (NCT04494425) compared T-DXd with TPC chemotherapy in HR+, HER2 low and HER2 ultralow metastatic breast cancer patients who received prior endocrine therapy.39 In the HER2 ultralow group, T-DXd significantly improved PFS (13.2 months vs 8.3 months) and ORR (61.8% vs 26.3%) compared with TPC chemotherapy. The NCCN guideline has recommended T-DXd and SG as second-line therapies for metastatic TNBC.
Combining ADCs and Immunotherapies for Locally Advanced/Metastatic TNBC
The success of ADC monotherapy in metastatic TNBC led to the progression of a series of studies investigating the combination of ADCs and other therapies in metastatic TNBC, especially ICIs (Table 1). The MORPHEUS-panBC (NCT03424005) was a phase Ib/II umbrella study that evaluated the efficacy and safety of multiple treatment combinations in inoperable locally advanced/metastatic breast cancer. Since Atezolizumab + nab-paclitaxel was approved for first-line treatment of PD-L1-positive locally advanced/metastatic TNBC, and SG was approved for second-line of metastatic TNBC, researchers compared the efficacy of Atezolizumab + SG with Atezolizumab + nab-paclitaxel in previously untreated PD-L1-positive locally advanced/metastatic TNBC. The interim analysis was inspiring, and it showed that the ORR was 76.7% (23/30) in the Atezolizumab + SG group and 66.7% (6/9) in the Atezolizumab + nab-paclitaxel group.40 It was notable that there were 5 complete responses (CR) among all responders in the Atezolizumab + SG group (5/26), while all responders were partial responses (PR) in the Atezolizumab + nab-paclitaxel group (6/6). Although follow-up data were immature, there was a trend towards benefit with the Atezolizumab + SG group over the Atezolizumab + nab-paclitaxel group in terms of PFS (12.2 months vs 5.9 months). The safety of Atezolizumab + SG combination was consistent with the individual drug.
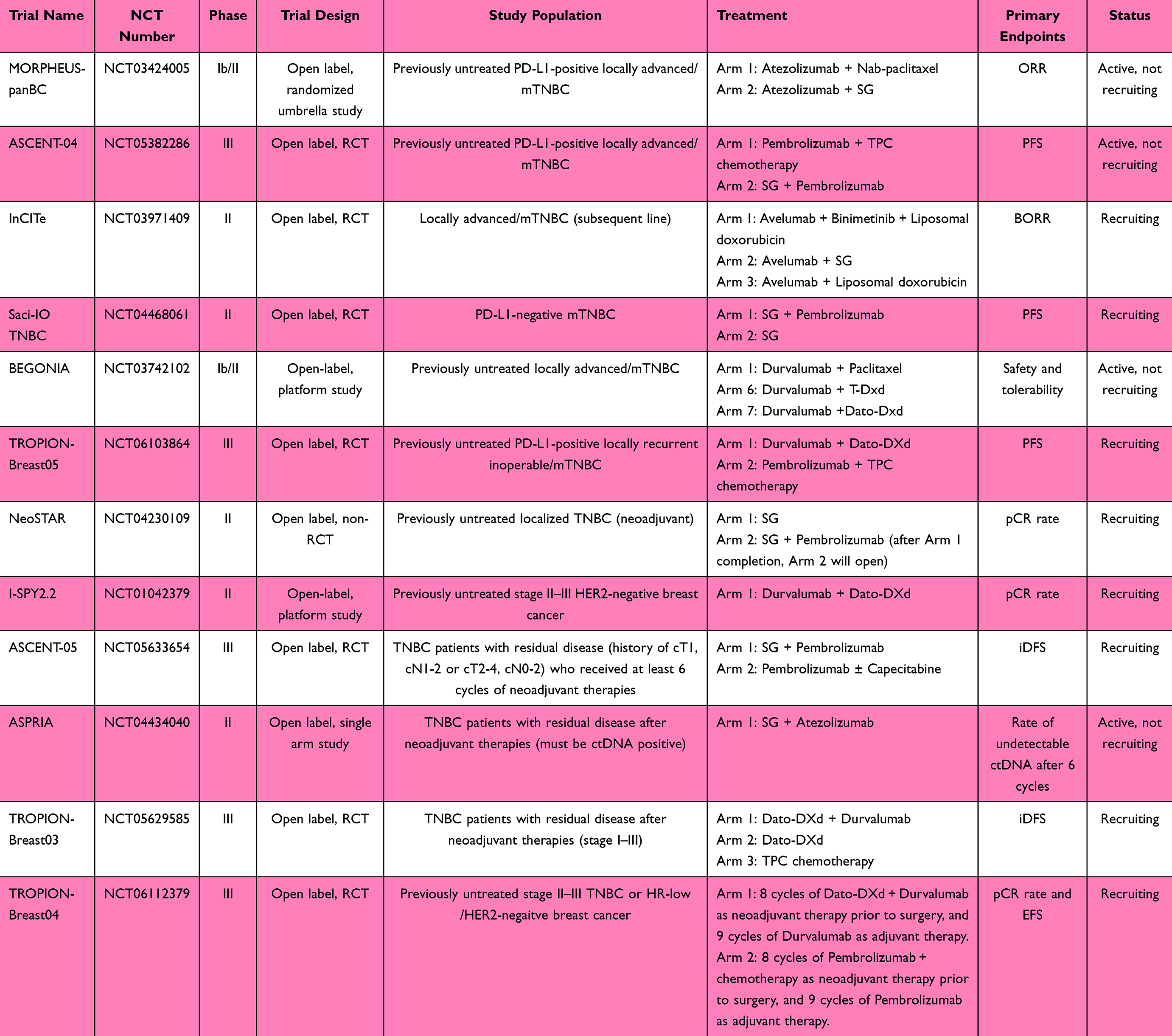 |
Table 1 The Clinical Trials of ADCs and Immunotherapy Combinations in TNBC |
There are other ongoing trials investigating the efficacy of SG and ICIs combination in locally advanced/metastatic TNBC. The ASCENT-04 trial (NCT05382286) is a phase III study investigating whether SG + Pembrolizumab could improve efficacy outcomes over Pembrolizumab + TPC chemotherapy in first-line treatment in PD-L1-positive locally advanced/metastatic TNBC.41 The primary endpoint is PFS and secondary endpoints are OS, ORR, quality of life and safety, and it will enroll about 440 participants. The InCITe trial (NCT03971409) is a Phase II study exploring the combination of SG with Avelumab in metastatic or unresectable TNBC. The included patients should have received no more than two prior lines of therapies, have never been treated with SG and have not used more than one ICI. Patients are randomized into once of three arms: patients in arm A will receive avelumab, binimetinib (MEK 1/2 inhibitor) and liposomal doxorubicin, patients in arm B will receive avelumab and SG and patients in arm C will receive avelumab and liposomal doxorubicin. The primary endpoint is BORR (best overall response rate).
Since ICI monotherapy is not effective in PD-L1-negative metastatic TNBC, the phase II Saci-IO TNBC trial (NCT04468061) was designed to compare the efficacy and safety of SG + Pembrolizumab with SG monotherapy in PD-L1-negative metastatic TNBC.42 The included patients in the trial are treatment naïve (previously treated brain metastases were permitted) and the study will enroll about 220 participants, and the primary endpoint is PFS.
In addition to SG, there are also trials investigating other ADCs in combination with ICIs in locally advanced/metastatic TNBC. The BEGONIA trial (NCT03742102) is an ongoing 2-part, open-label platform study in first-line treatment of locally advanced/metastatic TNBC. Initial results from arm 1 (Durvalumab + Paclitaxel) and arm 6 (Durvalumab + T-Dxd for HER2-low-expressing TNBC patients) showed that ORR was 57% in arm 1 and 100% (4/4, only 4 patients completed 2 on-treatment disease assessments) in arm 6.43 Although the sample size is limited, it showed promising safety and efficacy of Durvalumab + T-Dxd in first-line treatment of HER2-low-expressing metastatic TNBC, and the enrollment of patients in arm 6 is ongoing. Arm 7 of the BEGONIA trial evaluated the safety and efficacy of Dato-Dxd in combination with Durvalumab in first-line treatment of locally advanced/metastatic TNBC. The updated analysis showed that ORR was 79% (49/62) in arm 7 and 10% (6/62) of patients had a complete response, and ORR was not associated with PD-L1 expression.44 Median PFS was 13.8 months, and no new safety signals were observed. The TROPION-Breast05 (NCT06103864) is an ongoing trial comparing the efficacy of Dato-DXd + Durvalumab and chemotherapy + Pembrolizumab for first-line treatment in PD-L1-positive metastatic TNBC patients.45 In selected countries, there will be another arm of Dato-DXd monotherapy, which will include about 75 patients. The primary endpoint is PFS, and the study will enroll about 625 participants.
Combining ADCs and Immunotherapies for TNBC Neoadjuvant and Adjuvant Therapies
The KEYNOTE-522 trial (NCT03036488) demonstrated neoadjuvant Pembrolizumab + chemotherapy followed by surgery and adjuvant Pembrolizumab monotherapy was the current standard of care for stage II–III TNBC patients.46 However, about 37% TNBC patients still had residual cancer burden after neoadjuvant therapy. After demonstrating the promising efficacy and safety of the combinations of ADCs and immunotherapies in metastatic TNBC, there are emerging clinical trials investigating their potential benefits in the context of neoadjuvant and adjuvant therapies.47 The NeoSTAR trial (NCT04230109) enrolled 50 stage I–III TNBC patients who completed four cycles of neoadjuvant SG (after the SG cohort completion, the SG + Pembrolizumab cohort will open), and the results showed that the pCR rate was 30% (15/50), and the ORR was 64% (32/50).48 It was noteworthy that the pCR rate was 66.7% (6/9) in patients with a germline BRCA mutation. The 2-year event-free survival (EFS) was 95% in the whole cohort, and it was 100% among pCR patients.
I-SPY2.2 (NCT01042379), an adaptive platform trial for neoadjuvant breast cancer, utilizes biomarker-driven patient selection through its response predictive subtype (RPS) classification. Within this framework, the combination of Dato-DXd and durvalumab demonstrated significant activity, particularly in defined S1-S4 subgroups. The estimated pCR rate was 46% in TNBC cohort, and it exceeded the subtype-specific threshold of 40%.49 Most notably, in RPS S3 (HER2-Immune+) subtype, the pCR rate reached 72%, meeting the trial’s criterion for “graduation”, and the efficacy of Dato-Dxd + Durvalumab for TNBC neoadjuvant therapy warranted further investigation in RCT trials.
Given the high risk of recurrence in TNBC patients with residual disease after neoadjuvant therapies, it is urgent to explore innovative treatment combinations in the adjuvant setting for them. The ongoing phase III ASCENT-05 trial (NCT05633654) evaluates the safety and efficacy of SG in combination with Pembrolizumab compared to Pembrolizumab ± Capecitabine in TNBC patients with residual disease.50 In addition, circulating tumor DNA (ctDNA) is an important prognostic factor for breast cancer who received neoadjuvant therapies, and ctDNA-negative non-pCR breast cancer patients had similar survival to those who achieved pCR.51 The ongoing single arm phase II ASPRIA trial (NCT04434040) investigates the safety and efficacy of SG in combination with Atezolizumab in patients with detectable ctDNA after completion of all local and systemic neoadjuvant therapy.
The TROPION-Breast03 (NCT05629585) is an ongoing phase III trial assessing the efficacy and safety of Dato-DXd ± Durvalumab compared to investigator’s choice of therapy (Capecitabine, Pembrolizumab, or Capecitabine + Pembrolizumab) as adjuvant treatment in patients with residual disease after neoadjuvant therapies and surgery.52 Following TROPION-Breast03, the TROPION-Breast04 (NCT06112379) is an ongoing phase III trial assessing neoadjuvant Dato-DXd + Durvalumab followed by adjuvant Durvalumab compared to Pembrolizumab-based standard of care in treatment-naïve stage II–III TNBC or HR-low/HER2-negaitve breast cancer.53 The included patients in the experimental arm will receive 8 cycles of Dato-DXd + Durvalumab followed by surgery and receive 9 cycles of Durvalumab as adjuvant therapy. For those patients who had residual disease after surgery, adjuvant chemotherapy will be given in combination with Durvalumab. Olaparib will be given in combination with Durvalumab in gBRCA-positive tumours and residual disease, but may not be given concurrently with chemotherapy. These ongoing studies hold the promise of pivotal breakthroughs, aiming to deliver tangible improvements in patient outcomes.
Mechanisms of ADCs and Immunotherapy Combinations
ADCs exert complex mechanisms of action which extend beyond the direct induction of cancer cell death through their cytotoxic payloads. Antibody-mediated receptor signaling blockade, the killing of neighboring antigen-negative cells (referred to as the bystander effect) and the activation of immune effector cells are additional mechanisms contributing to ADCs’ anti-tumor efficacy.20 Cancer cell death triggered by cytotoxic payloads of ADCs can be immunogenic or non-immunogenic, and certain cytotoxic compounds such as Anthracyclines, Oxaliplatin and Irinotecan have been reported to induce immunogenic cell death (ICD),54–56 which characterizes a specific type of cell death which triggers an immune response to antigens released by dying cells.57 Most of the cytotoxic payloads of ADCs could induce immunogenic cell death and enhance the anti-tumor efficacy of ICIs both in vitro and in vivo.58 Reasons for combining ADCs and immunotherapy are as follows: In the process of ICD, damage-associated molecular patterns (DAMPs) such as calreticulin (CRT), heat-shock proteins (HSPs), HMGB1 and ATP will be released into tumor microenvironment (TME).59 Immature dendritic cells (DCs) will be stimulated by DAMPs via CD91, TLR4 and P2RY2/P2RX7, and mature DCs will migrate into lymph nodes and activate naïve T-cells.60 Finally, antigen specific CD8+ T-cells infiltrate TME, then recognize and attack cancer cells. Since PD-L1 is widely expressed on cancer cells and other cells such as macrophages in the TME, activated CD8+ T-cells will be inhibited by PD-L1. At this point, ICIs could block the immune cell suppression and have the potential to achieve durable anti-tumor activity (Figure 1). In addition, certain cytotoxic compounds such as tubulin inhibitor Vinblastine could directly activate DCs, which is independent of its anti-mitotic activity on cancer cells.61,62
 |
Figure 1 Mechanisms of ADCs and immunotherapy combinations. Cancer cell are killed by cytotoxic payloads of ADCs and dying cells released DAMPs into TME. DCs will be stimulated by DAMPs and migrate into lymph nodes and activate naïve T-cells. Antigen specific CD8+ T-cells infiltrate TME, then recognize and attack cancer cells. Activated CD8+ T-cells will be inhibited by PD-L1 which is widely expressed on cancer cells. At this point, ICIs could block the immune cell suppression and have the potential to achieve durable anti-tumor activity. (The Figure was created by Figdraw). |
ADCs are antibody and cytotoxic payloads conjugates, whereas the antibody moiety is not only just a vehicle for cytotoxic payloads delivery. The two antigen-binding fragments (Fabs) are responsible for target antigen recognition, while the crystallizable fragment (Fc) could promote macrophage-mediated antibody-dependent cell-mediated phagocytosis (ADCP), NK cell-mediated antibody-dependent cell-mediated cytotoxicity (ADCC) and complement-dependent cytotoxicity (CDC).63 For example, preclinical studies reported that T-DXd had similar binding activity to HER2 and ADCC activity compared with anti-HER2 antibody.34 In addition, SG could induce strong ADCC activity in cancer cells with high Trop2 expression, but not in Trop2-negative cancer cells.64
Challenges in Combining ADCs and Immunotherapies for TNBC Treatment
Despite promising efficacy from preliminary clinical trials, the combination therapy of ADCs and immunotherapies still faces challenges spanning biological complexity and real-world clinical implementation. First, potential overlapping adverse events of ADCs and immunotherapies combination therapy should be concerned. The common ADCs-related adverse events include hematologic (eg, neutropenia), gastrointestinal (eg, diarrhea, nausea), and oral mucositis, as well as rash and ocular surface events.31,65,66 Severe toxicities, particularly grade ≥3 oral mucositis and treatment-related diarrhea, hematologic adverse events, are leading causes of dose reductions, interruptions, or discontinuations, thereby directly impacting treatment intensity and clinical outcomes.31,66 Additionally, immune-mediated adverse events encompass hypothyroidism, hyperthyroidism, pneumonitis, severe skin reactions and so on.67 The overlapping adverse events of particular concern include pneumonitis and dermatologic reactions, which may be more frequent or severe when ADCs are combined with ICIs. Therefore, proactive toxicity management strategies such as rigorous patient selection, early biomarker monitoring and standardized algorithms for toxicity mitigation are essential.
Drug resistance represents one of the most formidable challenges in antineoplastic therapy. The antitumor activity of ADCs depends on both the antibody and the payload, thus the resistance mechanisms may include target antigen downregulation, payload resistance, impaired immune infiltration or upregulation of alternative immune checkpoints.68 Research identified that absence of TROP2 expression was associated with de novo resistance to SG, while mutated TACSTD2 drove acquired resistance, which led to reduced binding due to an altered subcellular localization of TROP2.69 As for immunotherapy, loss of tumor-specific antigens, antigen presentation deficiency, and failure to initiate an immune response can all lead to immune evasion, resulting in resistance to PD-1/PD-L1 antibodies.70 Future research should focus on identifying resistance biomarkers to guide therapy adaptation, such as ctDNA, antigen expression patterns or T-cell clonality.
Due to the heterogeneity of TNBC, the success of ADCs and ICIs varies among patients. Identifying reliable biomarkers to predict therapeutic response is essential for tailoring treatments to individual patients. Clinical trials, including BEGONIA, NeoSTAR and ASCENT, incorporated the assessment of TILs, PD-L1 and TROP2 expression status as exploratory predictive biomarkers for pathological response, while TROP2 expression failed to demonstrate its predictive value.44,48,71 The investigation of these biomarkers is primarily target-based, potentially leading to oversight of resistance mechanisms or predictive factors residing outside the primary drug-target axis. Recent years, the advancement of technologies such as liquid biopsy and genetic testing has driven significant progress, some emerging biomarkers, such as immune signatures, tumor mutation burden, and ctDNA, show potential for predicting the efficacy of anti-tumor therapy.49,72,73 Integrating genomic, transcriptomic and proteomic data may help identify patient subgroups who most likely to benefit from specific ADCs and immunotherapy combinations. Moreover, dynamic monitoring of ctDNA and immune markers during treatment may provide early insights into response and resistance, enabling adaptive therapy modifications.
Future Perspectives
The rapidly evolving landscape of TNBC treatment holds great promise for the combinations of ADCs and immunotherapies. While significant progress has been made, several unresolved challenges and emerging opportunities may influence the future of TNBC treatment. First, there is a pressing need for a deeper understanding of the complex mechanisms underlying the synergistic effect between ADCs and immunotherapies. Future studies should aim to clarify how ADCs interact with TME and improve the effectiveness of ICIs, which could provide insights into optimizing combination strategies. Novel combinations of ADCs and immunotherapies such as Sacituzumab tirumotecan and Pembrolizumab need to be further explored. Second, despite that the combinations of ADCs and immunotherapies have acceptable toxicity in multiple clinical trials, ICIs may increase the risk of immune-associated disease such as interstitial lung disease and skin reactions, so more attention needs to be paid to the toxicity management of combination therapies. Third, overcoming resistance to combinations of ADCs and immunotherapies will be a major challenge. TNBC is a heterogeneous disease and understanding the mechanisms of resistance is a priority for future research, which could involve the identification of resistance biomarkers and the development of novel combination therapies. Advances in multi-omics profiling and liquid biopsy technologies may facilitate the treatment of TNBC towards personalized medicine.
In the near future, the treatment paradigm for metastatic TNBC is expected to evolve from sequential monotherapy towards biomarker-informed combination regimens, like ADC + ICI, aiming for more durable responses. As for early-stage TNBC patients, these combinations hold the potential to redefine neoadjuvant therapy, moving beyond traditional chemotherapy towards targeted, “chemo-minimizing” protocols to improve pathological complete response rates. The success of these combinations will be critically dependent on the routine adoption of advanced molecular profiling (eg, target expression, immune signatures and ctDNA) to stratify patients into optimal therapeutic pathways. In conclusion, the combinations of ADCs and immunotherapies represent a promising treatment modality for TNBC. As more evidence from ongoing trials accumulates, the future of TNBC treatment may lie in personalized approaches that exploit the full potential of ADCs and immunotherapies.
Acknowledgments
We appreciate the funding from the National Natural Science Foundation of China for this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, literature search, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the Key Research and Development Program of Zhejiang Province (Grant No. 2024C03183), the National Natural Science Foundation of China (Grant No. 82373437, 82303382), and the Jingyi Research Fund Phase II of Beijing Vlove Charity Foundation (Grant No. JVII2025-0200304035).
Disclosure
The authors declared no competing interests in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–12. doi:10.3322/caac.21834
2. Borri F, Granaglia A. Pathology of triple negative breast cancer. Semin Cancer Biol. 2021;72:136–145. doi:10.1016/j.semcancer.2020.06.005
3. Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13:4429–4434. doi:10.1158/1078-0432.CCR-06-3045
4. Loibl S, Poortmans P, Morrow M, Denkert C, Curigliano G. Breast cancer. Lancet. 2021;397:1750–1769. doi:10.1016/S0140-6736(20)32381-3
5. Fonseca VC, Sidiropoulou Z. Geriatric breast cancer: staging, molecular surrogates, and treatment. A review & meta-analysis. Aging Dis. 2024;15:1602–1618. doi:10.14336/AD.2023.1002
6. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363:1938–1948. doi:10.1056/NEJMra1001389
7. Zhang Y, Chen H, Mo H, et al. Single-cell analyses reveal key immune cell subsets associated with response to PD-L1 blockade in triple-negative breast cancer. Cancer Cell. 2021;39:1578–1593.e1578. doi:10.1016/j.ccell.2021.09.010
8. Lee A, Djamgoz MBA. Triple negative breast cancer: emerging therapeutic modalities and novel combination therapies. Cancer Treat Rev. 2018;62:110–122. doi:10.1016/j.ctrv.2017.11.003
9. Guo L, Kong D, Liu J, et al. Breast cancer heterogeneity and its implication in personalized precision therapy. Exp Hematol Oncol. 2023;12:3. doi:10.1186/s40164-022-00363-1
10. Jiang YZ, Ma D, Suo C, et al. Genomic and transcriptomic landscape of triple-negative breast cancers: subtypes and treatment strategies. Cancer Cell. 2019;35:428–440.e425. doi:10.1016/j.ccell.2019.02.001
11. Zhu S, Wu Y, Song B, et al. Recent advances in targeted strategies for triple-negative breast cancer. J Hematol Oncol. 2023;16:100. doi:10.1186/s13045-023-01497-3
12. Bagchi S, Yuan R, Engleman EG. Immune checkpoint inhibitors for the treatment of cancer: clinical impact and mechanisms of response and resistance. Annu Rev Pathol. 2021;16:223–249. doi:10.1146/annurev-pathol-042020-042741
13. Wang W, Bi X, Feng Y, et al. Efficacy and safety of immune checkpoint inhibitors on advanced cervical cancer: a systematic review and meta-analysis. J Immunother. 2025;48:78–88. doi:10.1097/CJI.0000000000000545
14. Stanton SE, Adams S, Disis ML. Variation in the incidence and magnitude of tumor-infiltrating lymphocytes in breast cancer subtypes: a systematic review. JAMA Oncol. 2016;2:1354–1360. doi:10.1001/jamaoncol.2016.1061
15. Safonov A, Jiang T, Bianchini G, et al. Immune gene expression is associated with genomic aberrations in breast cancer. Cancer Res. 2017;77:3317–3324. doi:10.1158/0008-5472.CAN-16-3478
16. Adams S, Loi S, Toppmeyer D, et al. Pembrolizumab monotherapy for previously untreated, PD-L1-positive, metastatic triple-negative breast cancer: cohort B of the phase II KEYNOTE-086 study. Ann Oncol. 2019;30:405–411. doi:10.1093/annonc/mdy518
17. Nanda R, Chow LQ, Dees EC, et al. Pembrolizumab in patients with advanced triple-negative breast cancer: phase Ib KEYNOTE-012 Study. J Clin Oncol. 2016;34:2460–2467. doi:10.1200/JCO.2015.64.8931
18. Winer EP, Lipatov O, Im SA, et al. Pembrolizumab versus investigator-choice chemotherapy for metastatic triple-negative breast cancer (KEYNOTE-119): a randomised, open-label, Phase 3 trial. Lancet Oncol. 2021;22:499–511. doi:10.1016/S1470-2045(20)30754-3
19. Liu Y, Hu Y, Xue J, et al. Advances in immunotherapy for triple-negative breast cancer. Mol Cancer. 2023;22:145. doi:10.1186/s12943-023-01850-7
20. Drago JZ, Modi S, Chandarlapaty S. Unlocking the potential of antibody-drug conjugates for cancer therapy. Nat Rev Clin Oncol. 2021;18:327–344.
21. Dumontet C, Reichert JM, Senter PD, Lambert JM, Beck A. Antibody-drug conjugates come of age in oncology. Nat Rev Drug Discov. 2023;22:641–661.
22. Cortesi M, Zanoni M, Maltoni R, et al. TROP2 (trophoblast cell-surface antigen 2): a drug target for breast cancer. Expert Opin Ther Targets. 2022;26:593–602.
23. Bardia A, Rugo HS, Tolaney SM, et al. Final results from the randomized phase III ASCENT clinical trial in metastatic triple-negative breast cancer and association of outcomes by human epidermal growth factor receptor 2 and trophoblast cell surface antigen 2 expression. J Clin Oncol. 2024;42:1738–1744. doi:10.1200/JCO.23.01409
24. Rossi V, Turati A, Rosato A, Carpanese D. Sacituzumab govitecan in triple-negative breast cancer: from bench to bedside, and back. Front Immunol. 2024;15:1447280. doi:10.3389/fimmu.2024.1447280
25. Bardia A, Messersmith WA, Kio EA, et al. Sacituzumab govitecan, a Trop-2-directed antibody-drug conjugate, for patients with epithelial cancer: final safety and efficacy results from the phase I/II IMMU-132-01 basket trial. Ann Oncol. 2021;32:746–756.
26. Kovtun YV, Audette CA, Ye Y, et al. Antibody-drug conjugates designed to eradicate tumors with homogeneous and heterogeneous expression of the target antigen. Cancer Res. 2006;66:3214–3221.
27. Bardia A, Punie K, Barrios CH, et al. 275TiP ASCENT-03: phase III study of sacituzumab govitecan (SG) vs treatment of physician’s choice (TPC) in first-line (1L) metastatic triple-negative breast cancer (mTNBC). Ann Oncol. 2022;33:S663–S664.
28. Marmé F, Stickeler E, Furlanetto J, et al. Phase III postneoadjuvant study evaluating sacituzumab govitecan, an antibody drug conjugate in primary HER2-negative breast cancer patients with high relapse risk after standard neoadjuvant treatment: SASCIA. J Clin Oncol. 2021;39:TPS602–TPS602. doi:10.1200/JCO.2021.39.15_suppl.TPS602
29. Shastry M, Jacob S, Rugo HS, Hamilton E. Antibody-drug conjugates targeting TROP-2: clinical development in metastatic breast cancer. Breast. 2022;66:169–177. doi:10.1016/j.breast.2022.10.007
30. Okajima D, Yasuda S, Maejima T, et al. Datopotamab deruxtecan, a novel TROP2-directed antibody-drug conjugate, demonstrates potent antitumor activity by efficient drug delivery to tumor cells. Mol Cancer Ther. 2021;20:2329–2340. doi:10.1158/1535-7163.MCT-21-0206
31. Bardia A, Krop IE, Kogawa T, et al. Datopotamab deruxtecan in advanced or metastatic HR+/HER2- and triple-negative breast cancer: results from the phase I TROPION-PanTumor01 Study. J Clin Oncol. 2024;42:2281–2294.
32. Dent RA, Cescon DW, Bachelot T, et al. TROPION-Breast02: datopotamab deruxtecan for locally recurrent inoperable or metastatic triple-negative breast cancer. Future Oncol. 2023;19:2349–2359. doi:10.2217/fon-2023-0228
33. Xu B, Yin Y, Fan Y, et al. Sacituzumab tirumotecan (SKB264/MK-2870) in patients (pts) with previously treated locally recurrent or metastatic triple-negative breast cancer (TNBC): results from the phase III OptiTROP-Breast01 study. J Clin Oncol. 2024;42:104. doi:10.1200/JCO.2024.42.16_suppl.104
34. Ogitani Y, Aida T, Hagihara K, et al. DS-8201a, A novel HER2-targeting ADC with a novel DNA Topoisomerase I inhibitor, demonstrates a promising antitumor efficacy with differentiation from T-DM1. Clin Cancer Res. 2016;22:5097–5108. doi:10.1158/1078-0432.CCR-15-2822
35. Cortés J, Kim SB, Chung WP, et al. Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. N Engl J Med. 2022;386:1143–1154.
36. Hurvitz SA, Hegg R, Chung WP, et al. Trastuzumab deruxtecan versus trastuzumab emtansine in patients with HER2-positive metastatic breast cancer: updated results from DESTINY-Breast03, a randomised, open-label, phase 3 trial. Lancet. 2023;401:105–117. doi:10.1016/S0140-6736(22)02420-5
37. Tarantino P, Hamilton E, Tolaney SM, et al. HER2-low breast cancer: pathological and clinical landscape. J Clin Oncol. 2020;38:1951–1962. doi:10.1200/JCO.19.02488
38. Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387:9–20. doi:10.1056/NEJMoa2203690
39. Curigliano G, Hu X, Dent RA, et al. Trastuzumab deruxtecan (T-DXd) vs physician’s choice of chemotherapy (TPC) in patients (pts) with hormone receptor-positive (HR+), human epidermal growth factor receptor 2 (HER2)-low or HER2-ultralow metastatic breast cancer (mBC) with prior endocrine therapy (ET): primary results from DESTINY-Breast06 (DB-06. J Clin Oncol. 2024;42:LBA1000–LBA1000.
40. Schmid P, Loi S, De la Cruz Merino L, et al. 181O Interim analysis (IA) of the atezolizumab (atezo) + sacituzumab govitecan (SG) arm in patients (pts) with triple-negative breast cancer (TNBC) in MORPHEUS-pan BC: a phase Ib/II study of multiple treatment (tx) combinations in pts with locally advanced/metastatic BC (LA/mBC). ESMO Open. 2024;9:103203.
41. Tolaney SM, de Azambuja E, Emens LA, et al. 276TiP ASCENT-04/KEYNOTE-D19: phase III study of sacituzumab govitecan (SG) plus pembrolizumab (pembro) vs treatment of physician’s choice (TPC) plus pembro in first-line (1L) programmed death-ligand 1-positive (PD-L1+) metastatic triple-negative breast cancer (mTNBC). Ann Oncol. 2022;33:S664–S665.
42. Garrido-Castro AC, Keenan TE, Li T, et al. Saci-IO TNBC: randomized phase II trial of sacituzumab govitecan (SG) ± pembrolizumab in PD-L1– metastatic triple-negative breast cancer (mTNBC. J Clin Oncol. 2021;39:TPS1106–TPS1106. doi:10.1200/JCO.2021.39.15_suppl.TPS1106
43. Schmid P, Im S-A, Armstrong A, et al. BEGONIA: phase 1b/2 study of durvalumab (D) combinations in locally advanced/metastatic triple-negative breast cancer (TNBC)—Initial results from arm 1, d+paclitaxel (P), and arm 6, d+trastuzumab deruxtecan (T-DXd). J Clin Oncol. 2021;39:1023. doi:10.1200/JCO.2021.39.15_suppl.1023
44. Schmid P, Wysocki PJ, Ma CX, et al. 379MO Datopotamab deruxtecan (Dato-DXd) + durvalumab (D) as first-line (1L) treatment for unresectable locally advanced/metastatic triple-negative breast cancer (a/mTNBC): updated results from BEGONIA, a phase Ib/II study. Ann Oncol. 2023;34:S337. doi:10.1016/j.annonc.2023.09.556
45. Schmid P, Oliveira M, O’Shaughnessy J, et al. 261TiP TROPION-Breast05: phase (Ph) III study of datopotamab deruxtecan (Dato-DXd) ± durvalumab (D) vs chemotherapy (CT) + pembrolizumab (pembro) in patients (pts) with PD-L1+ locally recurrent inoperable or metastatic triple-negative breast cancer (TNBC). ESMO Open. 2024;9:103282. doi:10.1016/j.esmoop.2024.103282
46. Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382:810–821. doi:10.1056/NEJMoa1910549
47. Li P, Guo X, Ruan W, et al. Neoadjuvant immunotherapy in triple-negative breast cancer: striking potential or need for caution? Aging Dis. 2025.
48. Spring LM, Tolaney SM, Fell G, et al. Response-guided neoadjuvant sacituzumab govitecan for localized triple-negative breast cancer: results from the NeoSTAR trial. Ann Oncol. 2024;35:293–301. doi:10.1016/j.annonc.2023.11.018
49. Shatsky RA, Trivedi MS, Omene CO, et al. Rates of pathologic complete response (pCR) after datopotamab deruxtecan (Dato) plus durvalumab (Durva) in the neoadjuvant setting: results from the I-SPY2.2 trial. J Clin Oncol. 2024;42:LBA501–LBA501. doi:10.1200/JCO.2024.42.17_suppl.LBA501
50. Tolaney SM, DeMichele A, Takano T, et al. ASCENT-05/OptimICE-RD (AFT-65): phase 3, randomized, open-label study of adjuvant sacituzumab govitecan (SG) + pembrolizumab (pembro) vs pembro ± capecitabine (cape) in patients (pts) with triple-negative breast cancer (TNBC) and residual disease after neoadjuvant therapy (NAT) and surgery. J Clin Oncol. 2023;41:TPS619–TPS619.
51. Magbanua MJM, Swigart LB, Wu HT, et al. Circulating tumor DNA in neoadjuvant-treated breast cancer reflects response and survival. Ann Oncol. 2021;32:229–239. doi:10.1016/j.annonc.2020.11.007
52. Bardia A, Pusztai L, Albain K, et al. TROPION-Breast03: a randomized phase III global trial of datopotamab deruxtecan ± durvalumab in patients with triple-negative breast cancer and residual invasive disease at surgical resection after neoadjuvant therapy. Ther Adv Med Oncol. 2024;16:17588359241248336. doi:10.1177/17588359241248336
53. McArthur H, Tolaney S, Loibl S, et al. Abstract PO1-20-13: TROPION-Breast04: a phase 3 study of neoadjuvant datopotamab deruxtecan (Dato-DXd) + durvalumab followed by adjuvant durvalumab vs the standard of care in treatment-naive early-stage triple negative or HR-low/HER2– breast cancer. Cancer Res. 2024;84:PO1–20–13–PO21–20–13.
54. Casares N, Pequignot MO, Tesniere A, et al. Caspase-dependent immunogenicity of doxorubicin-induced tumor cell death. J Exp Med. 2005;202:1691–1701. doi:10.1084/jem.20050915
55. Tesniere A, Schlemmer F, Boige V, et al. Immunogenic death of colon cancer cells treated with oxaliplatin. Oncogene. 2010;29:482–491. doi:10.1038/onc.2009.356
56. Yan W, Li Y, Zou Y, et al. Co-delivering irinotecan and imiquimod by pH-responsive micelle amplifies anti-tumor immunity against colorectal cancer. Int J Pharm. 2023;648:123583.
57. Galluzzi L, Kepp O, Hett E, Kroemer G, Marincola FM. Immunogenic cell death in cancer: concept and therapeutic implications. J Transl Med. 2023;21:162. doi:10.1186/s12967-023-04017-6
58. Bauzon M, Drake PM, Barfield RM, Cornali BM, Rupniewski I, Rabuka D. Maytansine-bearing antibody-drug conjugates induce in vitro hallmarks of immunogenic cell death selectively in antigen-positive target cells. Oncoimmunology. 2019;8:e1565859. doi:10.1080/2162402X.2019.1565859
59. Garg AD, Galluzzi L, Apetoh L, et al. Molecular and translational classifications of DAMPs in immunogenic cell death. Front Immunol. 2015;6:588.
60. Krysko DV, Garg AD, Kaczmarek A, Krysko O, Agostinis P, Vandenabeele P. Immunogenic cell death and DAMPs in cancer therapy. Nat Rev Cancer. 2012;12:860–875.
61. Mizumoto N, Gao J, Matsushima H, Ogawa Y, Tanaka H, Takashima A. Discovery of novel immunostimulants by dendritic-cell-based functional screening. Blood. 2005;106:3082–3089.
62. Tanaka H, Matsushima H, Nishibu A, Clausen BE, Takashima A. Dual therapeutic efficacy of vinblastine as a unique chemotherapeutic agent capable of inducing dendritic cell maturation. Cancer Res. 2009;69:6987–6994. doi:10.1158/0008-5472.CAN-09-1106
63. Tiller KE, Tessier PM. Advances in Antibody Design. Annu Rev Biomed Eng. 2015;17:191–216. doi:10.1146/annurev-bioeng-071114-040733
64. Han C, Perrone E, Zeybek B, et al. In vitro and in vivo activity of sacituzumab govitecan, an antibody-drug conjugate targeting trophoblast cell-surface antigen 2 (Trop-2) in uterine serous carcinoma. Gynecol Oncol. 2020;156:430–438. doi:10.1016/j.ygyno.2019.11.018
65. Bardia A, Mayer IA, Diamond JR, et al. Efficacy and safety of anti-trop-2 antibody drug conjugate sacituzumab govitecan (IMMU-132) in heavily pretreated patients with metastatic triple-negative breast cancer. J Clin Oncol. 2017;35:2141–2148. doi:10.1200/JCO.2016.70.8297
66. Rugo HS, Tolaney SM, Loirat D, et al. Safety analyses from the phase 3 ASCENT trial of sacituzumab govitecan in metastatic triple-negative breast cancer. NPJ Breast Cancer. 2022;8:98.
67. Cortes J, Cescon DW, Rugo HS, et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet. 2020;396:1817–1828. doi:10.1016/S0140-6736(20)32531-9
68. Chen YF, Xu YY, Shao ZM, Yu KD. Resistance to antibody-drug conjugates in breast cancer: mechanisms and solutions. Cancer Commun. 2023;43:297–337. doi:10.1002/cac2.12387
69. Coates JT, Sun S, Leshchiner I, et al. Parallel genomic alterations of antigen and payload targets mediate polyclonal acquired clinical resistance to sacituzumab govitecan in triple-negative breast cancer. Cancer Discov. 2021;11:2436–2445.
70. Zheng Y, Li S, Tang H, Meng X, Zheng Q. Molecular mechanisms of immunotherapy resistance in triple-negative breast cancer. Front Immunol. 2023;14:1153990.
71. Bardia A, Tolaney SM, Punie K, et al. Biomarker analyses in the phase III ASCENT study of sacituzumab govitecan versus chemotherapy in patients with metastatic triple-negative breast cancer. Ann Oncol. 2021;32:1148–1156.
72. Morganti S, Kusmick RJ, Hughes ME, et al. Survival outcomes and the role of DNADX ctDNA testing in patients treated with sacituzumab govitecan for metastatic breast cancer. ESMO Open. 2025;10:105828. doi:10.1016/j.esmoop.2025.105828
73. Zhou Y, Zhang Z, Chen H, et al. Efficacy, safety, and biomarkers of neoadjuvant dalpiciclib (CDK4/6 inhibitor) plus aromatase inhibitors in operable HER2-negative luminal b breast cancer: a prospective, single-center, single-arm, phase II trial (DANCER). MedComm. 2025;6:e70402. doi:10.1002/mco2.70402
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.