")
Back to Journals » International Journal of General Medicine » Volume 16
Recent Advancements on Long COVID in China: A Narrative Review
Authors Tang J, Song T , Kuang M, Feng Y, Liu G, Liu H
Received 20 April 2023
Accepted for publication 12 June 2023
Published 19 June 2023 Volume 2023:16 Pages 2585—2593
DOI https://doi.org/10.2147/IJGM.S417692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jia Tang, Tiantian Song, Ming Kuang, Yiping Feng, Guangrong Liu, Hongying Liu
Hangzhou Kang Ming Information Technology Co., Ltd, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Hongying Liu, Hangzhou Kang Ming Information Technology Co., Ltd, 401 Building 4, Haichuang Park (across from Taobao City) 998 Wenyi West Road, Yuhang District, Hangzhou, Zhejiang Province, 310000, People’s Republic of China, Tel +86 021 64045531, Email [email protected]
Abstract: The COVID-19 pandemic is a huge public health crisis in the 21st century. In addition to the acute symptoms, a considerable proportion of patients worldwide have suffered from post-COVID-19 syndrome, commonly known as Long COVID. The impact of Long COVID on individual and public health burden cannot be ignored. According to recent researches, Long COVID has been affecting multiple organ systems throughout the body, with respiratory, mental, nervous and digestive symptoms often seen in Chinese population. Clinical studies have proved that symptoms were alleviated by a variety of treatments, such as physical therapy, rehabilitation training, psychological support, behavioral cognitive therapy, stem cell therapy, etc. Based on the current clinical evidence, it is recommended to strengthen the scientific research on Long COVID and actively carry out early monitoring and intervention in the future, so as to effectively prevent the long-term disease burden and economic pressure.
Keywords: Long COVID, post-COVID conditions, China, clinical characteristics, management strategies
Background
COVID-19 is the most consequential pandemic of the 21st century.1 The first case of COVID-19 infection in China was reported in December 2019 in Wuhan. Human-to-human transmission occurs through common routes such as direct transmission, contact transmission and airborne transmissions through aerosols and during medical procedures. Cough, sneeze, inhalation of droplets, and contact with oral, nasal and eye mucous membranes are the common modes of spread.2
Since the outbreak of COVID-19, a large number of people have been affected worldwide. With the continued prevalence of COVID-19 and the accumulation of COVID-19 rehabilitators, a considerable proportion of COVID-19 patients suffered long-term effects after their nucleic acid tests have turned negative. This condition is commonly referred to post COVID-19 syndrome, also named Long COVID. It is estimated that at least 65 million people worldwide have been affected by Long COVID, with most individuals still not fully recovered one year after the initial infection.3
On December 8, 2022, China optimized its COVID-19 control policies and downgraded management of COVID-19, leading to a surge in the number of infections. According to the statistics from the Chinese Center for Disease Control and Prevention (CCDC),4 the number and rate of people testing positive for the nucleic acid of the SARS-CoV-2 have shown an increasing trend followed by a decreasing trend since December 9, 2022, peaking at of 6.94 million positive cases on December 22nd, and then fluctuating downwards, with 12,738 positive cases reported on February 23rd (Figure 1A). The positive rate of nucleic acid testing reached its peak of 29.2% on December 25th, followed by a fluctuation downwards, and was 1.4% on February 23rd (Figure 1A). The number and positive rate of positive results in COVID-19 antigen tests increased rapidly since December 9, reaching a peak of 337,000 positive cases (21.3%) on December 22nd, and then fluctuated downwards, with 337 positive cases reported on February 23 (positivity rate of 0.5%) (Figure 1B).
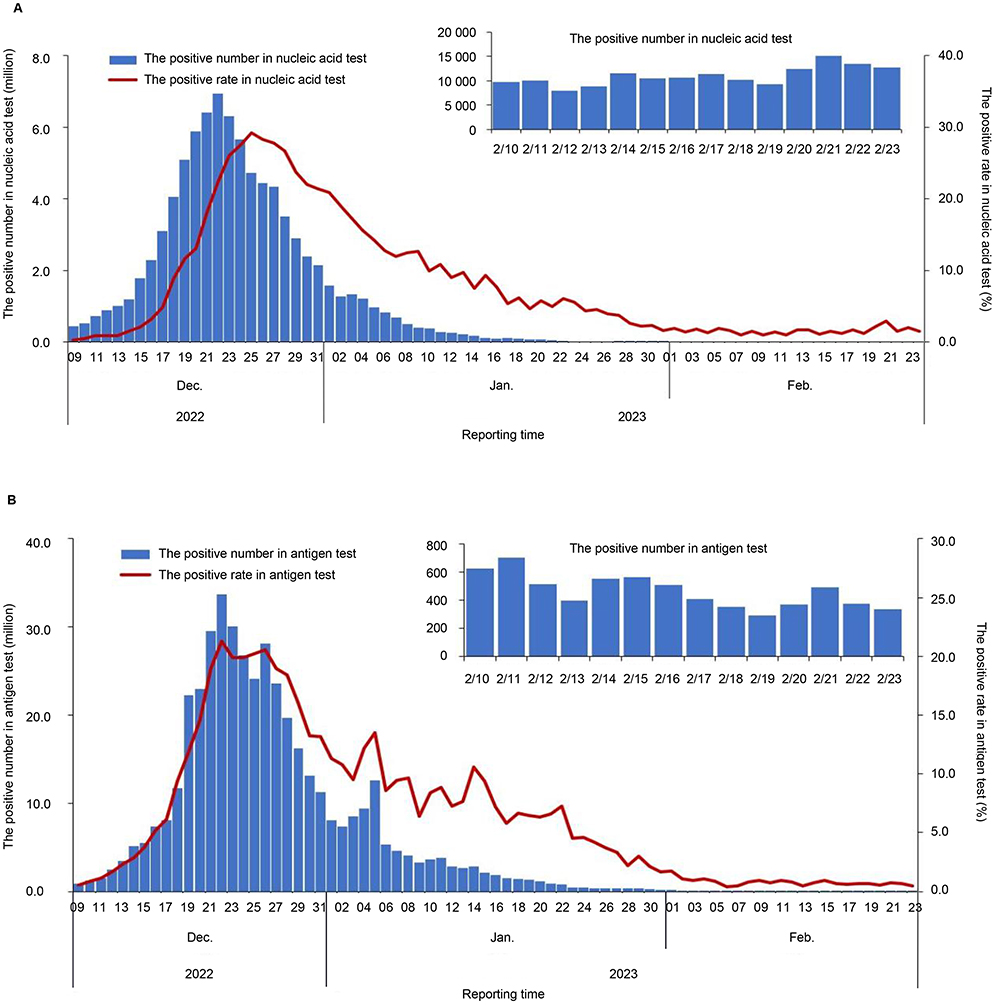 |
Figure 1 National situation of COVID-19 infection in China. (A) Trend in the number and positivity rate of nucleic acid tests positive cases for COVID-19 among the reported population in China. (B) Trend in the number and positivity rate of antigen tests positive cases for COVID-19 among the reported population in China. |
With the large number of infections in the Chinese population, a significant proportion of them may develop Long COVID. In February 2023, The Lancet published a letter from several scholars at Hunan University, China, titled “China needs a scientific Long COVID recovery-support platform”. The letter proposed that post-COVID-19 syndrome, or Long COVID, had become a major public health issue in the post-pandemic era, and timely and comprehensive information guidance and support were key to effectively addressing Long COVID.5
Basic Information About Long COVID
“Long COVID” has been defined by different organizations around the world. The World Health Organization (WHO) defined it as the continuation or development of new symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months with no other explanation.6 The National Institute for Health and Care Excellence (NICE) in the UK defines Long COVID as signs and symptoms that continue or develop after acute COVID-19, including both ongoing symptomatic COVID-19 (4~12 weeks) and post-COVID-19 syndrome (≥12 weeks).7 The US Centers for Disease Control and Prevention (CDC) describes it as signs, symptoms, or conditions that continue or develop after initial COVID-19 or SARS-CoV-2 infection. The signs, symptoms, and conditions are present four weeks or more after the initial phase of infection; may be multisystemic; and may present with a relapsing-remitting pattern and progression or worsening over time, with the possibility of severe and life-threatening events even months or years after infection (Post-COVID Conditions).8
The global prevalence of Long COVID was estimated to be 43%, with 51% in Asia, 44% in Europe, and 31% in North America.9 The estimated global prevalence at 30, 60, 90, and 120 days after infection is 37%, 25%, 32%, and 49%, respectively. The main risk factors for Long COVID include health status, age, gender, abnormal lab results, and potential complications.10–12 The incidence rate in females is twice that in males,13 and the risk of Long COVID increases by 8% for each 10-years increase in age.14 The presence of comorbidities also increases the risk, and individuals who exhibit more than five symptoms during the acute phase of the disease are more likely to develop Long COVID.15 Table 1 summarizes the disease characteristics of Long COVID.3,14,16–19
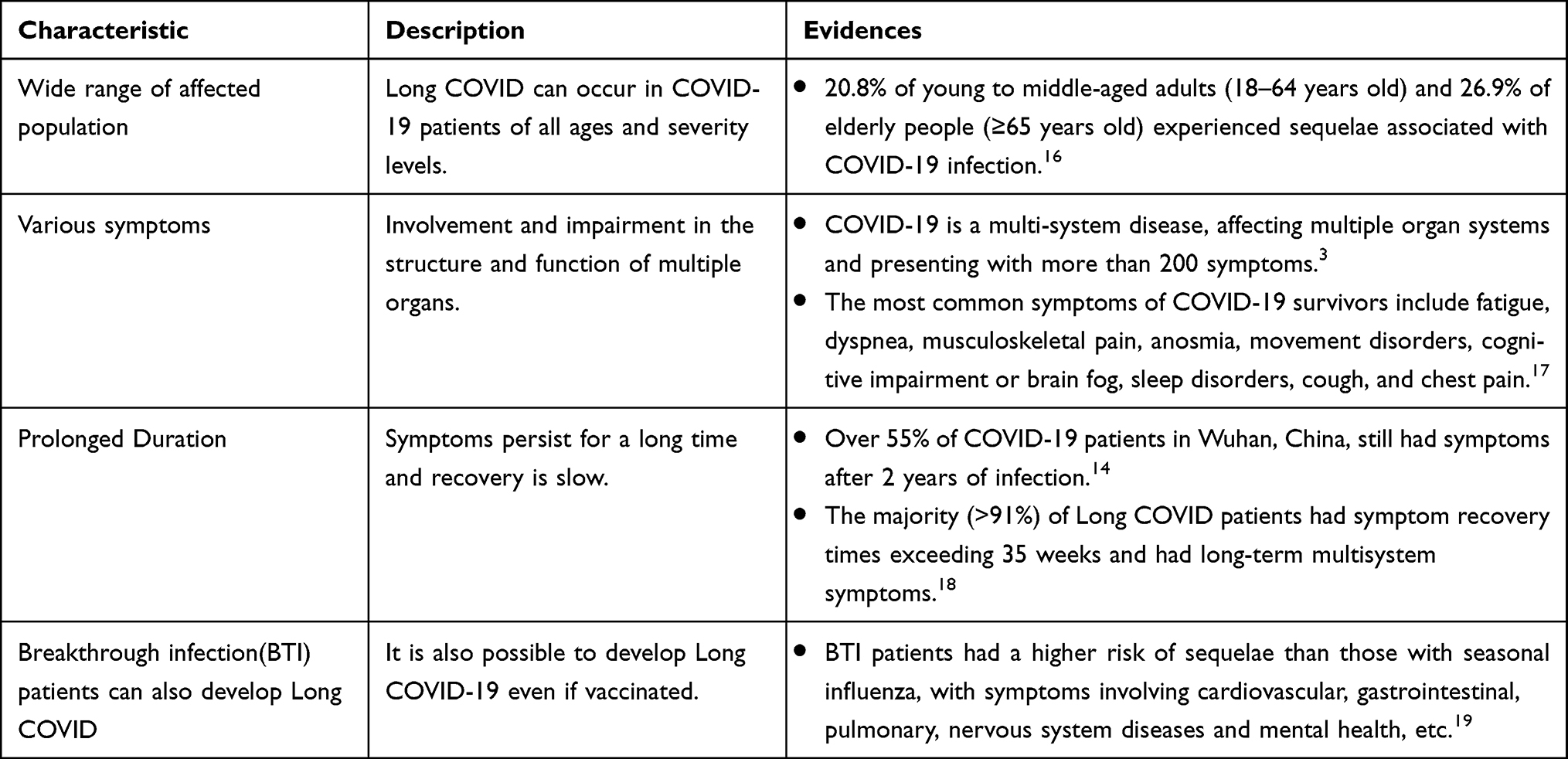 |
Table 1 Characteristics of Long COVID |
With the recurrence and prolongation of the COVID-19 pandemic, the negative impact on individual patients, their families and society is becoming increasingly severe. Long COVID is a poor health condition that usually requires long-term treatment and poses clear long-term risks to the patient’s physical, psychological, and social activities. One survey found that 44% of people with Long COVID were out of the labor force and 51% worked fewer hours.20 The decrease in the quality of life and work capacity of patients with Long COVID will have a profound impact on social employment and economic development.21
Based on the definition of Long COVID by international authoritative health organizations and the existing researches in China, the characteristics and prevention strategies of Long COVID in the Chinese population were discussed.
Common Clinical Symptoms of Chinese Patients with Long COVID
Long COVID can affect various systems and organs throughout the body, such as the respiratory system, nervous system, digestive system, and mental health. The clinical symptoms are complex and diverse. According to a recent epidemiological survey in China,10 the most common symptoms are fatigue (33.7%), cough (31.9%), sore throat (31.0%), lack of concentration (30.5%), anxiety (30.2%), muscle pain (29.9%), and joint pain (29.9%). In addition to the above symptoms, other studies22,23 have also reported phlegm, diarrhea, dyspnea, palpitations, fever, sweating and other symptoms. Severe patients tend to have more symptoms after infection.23
Respiratory System Symptoms/Clinical Manifestations – Cough, Impaired Lung Function, Pulmonary Fibrosis
Before and after the COVID-19 pandemic, there was a high rate of under-reporting of pertussis in Jiangsu province and a large number of reproductive-age adults who were susceptible to pertussis.24 Six to nine months after discharge, 25% of recovered COVID-19 patients in Beijing showed pulmonary ventilation dysfunction, and 35.9% showed diffusion dysfunction; 56.5% of severe cases had reduced lung diffusion capacity. Chest CT results showed nodules in 55.36% of cases, strip-like changes in 44.64% of cases, ground-glass opacity in 37.5% of cases, and grid shadow in 5.36% of cases, with statistically significant differences between severe and non-severe groups.25 COVID-19 recovered patients should undergo regular pulmonary function tests, especially those who were severe cases.
In the period before and after the optimization of COVID control policies, the trend of the number of prescriptions containing the “cough” field in Zhiyun Health Internet Hospital (Figure 2) is basically consistent with the change of COVID-19 nucleic acid/antigen positive population size reported by CCDC (Figure 1). The number of prescriptions began to increase sharply on December 5, 2022, and remained above 60000 from December 9, 2022 to January 6, 2023, which was almost double or more than the same period of the previous year, and the fluctuation decreased after January 5, 2023. From February 20 to March 12, 2023 (about 12 weeks after COVID strategies optimization), the number of cough prescriptions was higher than the number of prescriptions for the same period last year. It is suspected that in China, many patients who were infected with COVID-19 in early December have exhibited symptoms suggestive of Long COVID, with cough being the main clinical symptom.
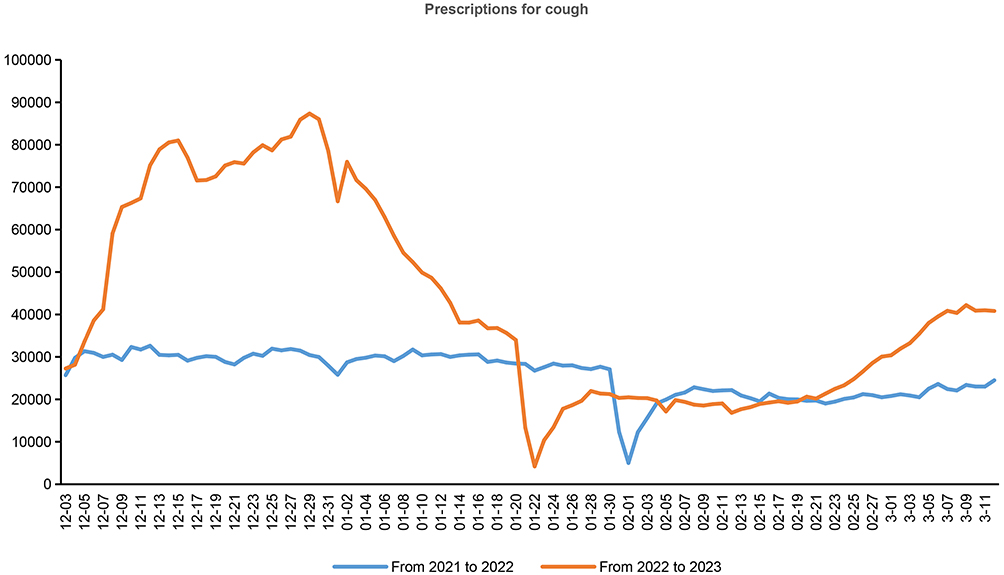 |
Figure 2 The number of cough prescriptions issued by Zhiyun Health Internet Hospital. Notes: The two temporary declines in the number of cough prescriptions around February 01, 2022 and January 22, 2023, respectively, are due to the impact of the Chinese Spring Festival. |
General Manifestations – Fatigue or Weakness
In 2021, the Lancet reported a cohort study26 of 1733 Chinese COVID-19 patients followed for 6 months after discharge, and the most common symptom was fatigue or weakness (63%). This is similar to the results of another meta-analysis including multiple countries, where fatigue (58%) was the most reported of more than 50 Long COVID symptoms.27
Psychological Symptoms – Mental Health Problems, Depression, Anxiety, PTSD, Sleep Disorders, Etc
As COVID-19 infection is a communicable disease, COVID-19 survivors may suffer from discrimination and humiliation, and are more likely to develop social anxiety.28 Compared to healthy controls, COVID-19 survivors reported more feelings of shame, financial insecurity, and social isolation.29 When assessing the psychological status of COVID-19 survivors 6 months after discharge in 5 cities in China, the proportions of patients with depression symptoms <5 and ≥5 were 76.9% and 23.1%, respectively. The proportions of patients with anxiety symptoms <5 and ≥5 were 77.4% and 22.6%, respectively.30 Among 144 COVID-19 discharged patients in Tianjin, 16.0% had post-traumatic stress disorder (PTSD), a severe mental health condition caused by a terrifying event.31 A cross-sectional survey evaluated the sleep quality of 199 COVID-19 survivors six months after discharge. About 62.8% were dissatisfied with sleep quality, and 33.7% had sleep disorders. Factors associated with poor sleep quality included witnessing the suffering or death of other COVID-19 patients during hospitalization, depression, anxiety, PTSD, and social support.32
Neurological Symptoms – Cognitive and Memory Impairment
Elderly COVID-19 patients were assessed for cognitive decline at 6 months after discharge, with their non-infected spouses as controls. Higher IQCODE scores indicated more severe cognitive decline. It was found that the IQCODE score of COVID-19 patients was higher than that of the control group.33 A six-month follow-up study of severe COVID-19 recovery patients discovered that the incidence of memory loss was higher in critically ill patients than in severe patients (15.1% vs 8.0%, p = 0.041), and critical illness was an independent risk factor for forgetfulness (p = 0.045).34
Digestive Symptoms – Loss of Appetite, Diarrhea, Nausea/Vomiting, Abdominal Pain
A total of 117 patients with COVID-19 were followed up for 3 months after discharge from 12 hospitals in Hubei and Guangdong Province. The gastrointestinal sequelae reported included loss of appetite, nausea, acid reflux, diarrhea, abdominal distension, belching, vomiting, and abdominal pain.35
Strategies and Methods for Prevention and Treatment of Long COVID
Vaccination and adopting a healthy lifestyle can reduce the risk of developing Long COVID. The treatment strategies for Long COVID mainly focused on symptom relief. As early as 2020, the National Health Commission of China issued “Rehabilitation Program for Discharged COVID-19 Patients”,36 which recommended a series of rehabilitation treatment methods for respiratory dysfunction (such as coughing, sputum production, and breathing difficulties), physical dysfunction (such as fatigue, weakness, and muscle soreness), and psychological dysfunction (such as fear, anger, anxiety, and depression) that may occur in patients discharged from COVID-19, including respiratory function training, physical function exercise, psychological rehabilitation intervention and daily life ability practice.
Early Monitoring and Diagnosis
Early monitoring and diagnosis are essential for effective treatment and improved prognosis. Recently, South Korea published its first preliminary management guidelines for Long COVID,37 which suggested that the possibility of Long COVID should be assessed in patients with symptoms lasting more than 12 weeks after COVID-19 diagnosis. Other underlying diseases, complications, or diseases with similar symptoms should be excluded, and suspected diseases should be tested. NICE guidelines recommend a complete evaluation, including a full blood count, kidney and liver function tests, C-reactive protein, B-type natriuretic peptide (BNP), ferritin and thyroid function tests.7 Systemic inflammatory markers, such as d-dimer, C-reactive protein, interleukin-6, procalcitonin, and neutrophil counts are associated with persistent symptoms.38–43 In addition, having received 2 or more doses of COVID-19 vaccine in the past was a protective factor.10
Vaccination Against COVID-19
The best way to prevent Long COVID is to avoid infection with the virus, and vaccination remains the most effective way to protect against the virus. The virus infectivity within the population can be retarded by adequate vaccination coverage.44 Interestingly, vaccination was found to be consistently associated with lower odds and rates of Long COVID clinical diagnosis.45 A large meta-analysis showed that the vaccinated group had a total of 29% lower risk of developing Long COVID compared with the unvaccinated group, including cognitive dysfunction/symptoms, kidney disease/problems, myalgia, and sleep disorders/problems.46 China has been implementing a policy of COVID-19 vaccination since mid-December 2020. To September 18, 2021, a total of 1100.8442 million people have been vaccinated in China, accounting for 78% of the country’s total population.47 The vaccination coverage was much higher than the world average of 12.7%.48 In fact, vaccination rates remain low in many parts of the world, and vaccine hesitancy is emerging as a major barrier to tackling the recurrent pandemic. Effectively tackling poor compliance to COVID-19 prevention measures and vaccine hesitancy is of paramount importance in the battle against the urgent management of the pandemic.49
Healthy Lifestyle
Women with five to six healthy lifestyles were reported to have a 49% lower risk of developing post-COVID conditions, including healthy weight, never smoking, at least 150 minutes of moderate to vigorous exercise per week, a high-quality diet, moderate alcohol intake and adequate sleep, with BMI and sleep independently associated with risk of Long COVID.50
Respiratory Training
Medical experts recommended appropriate treatment based on clinical symptoms. Chest imaging, electrocardiogram, and pulmonary function tests should be considered for patients presenting with cardiopulmonary symptoms. Patients with respiratory distress and during pulmonary rehabilitation usually require supplemental oxygen. Adequate patient support and building a good relationship are essential for recovery.11 For critically ill COVID-19 patients in the ICU or patients over 65 years old with prolonged COVID-19 symptoms, consultation with rehabilitation experts for appropriate and specific respiratory rehabilitation therapy is recommended.37
Physical Function Training
An unsupervised home exercise program (TERECO) that includes respiratory control and chest expansion, aerobic exercise, and lower limb muscle strength (LMS) training was implemented through a smartphone app and remote heart rate telemetry monitoring for COVID-19 survivors with persistent dyspnea symptoms. Patients who received TERECO intervention showed improvements in exercise capacity, lower limb muscle strength (LMS), and health-related quality of life (HRQOL) compared with the control group.51
Mental Health Interventions
Cognitive behavioral therapy (CBT) is recommended as a first-line psychological treatment for clinical therapy.52 Studies have shown that the mean decreases in depression, anxiety, stress, and total DASS-21 scores were greater in the CBT intervention group than in the control group, highlighting the effectiveness of CBT in improving the psychological health of COVID-19 patients.53 XiaoE, a CBT-based mental health chatbot, is a viable and engaging digital therapy that can provide accessible and self-guided mental health assistance for young people with depressive symptoms.54 Compared with the treatment as usual (TAU) group, the computerized CBT (cCBT) + TAU group showed significantly reduced scores on the Hamilton Depression Rating Scale (HAMD17), Hamilton Anxiety Scale (HAMA), Self-Rating Depression Scale (SDS), Self-Rating Anxiety Scale (SAS), and Athens Insomnia Scale (AIS) after intervention (all P < 0.001).52 These studies demonstrate the importance of CBT in alleviating psychological distress among COVID-19 patients. In addition, promoting social support and social inclusion may be effective strategies to improve the psychological health of COVID-19 survivors.28
Other Strategies and Methods for Managing Long COVID That Can Be Learned
In a study published in “Preprints with The Lancet” in March 2023, metformin was used to treat COVID-19 patients with a 300-days followed up. Compared with placebo, metformin reduced the risk of COVID-19 sequelae by 42%, and up to 63% when administered within 4 days of symptom onset.55
In 2020, Japan approved for the first time the use of autologous adipose mesenchymal stem cells to treat the sequelae of COVID-19. Patients received three intravenous injections of 200 million stem cells every 2–4 weeks, and symptoms such as lung function, oxygenation index, inflammation level, and pain degree were relieved.56 In 2022, a prospective study in China used human umbilical cord mesenchymal stem cells (UC-MSCs) to treat severe COVID-19 patients and followed up for one year and found that stem cells had long-term benefits on the recovery of lung disease and symptom relief, with good tolerance.57
Besides, hyperbaric oxygen therapy can induce neuroplasticity and improve cognitive, mental, fatigue, sleep, and pain symptoms in Long COVID patients diagnosed with infection for at least three months.58 Aromatherapy blend of thyme, orange, clove bud, and frankincense can boost energy levels in post-COVID-19 female patients.59 Treatment combining olfactory rehabilitation with oral supplementation with Palmitoylethanolamide and Luteolin was associated with improved recovery of olfactory function, most marked in patients with longstanding olfactory dysfunction.60 Histamine receptor antagonists can be used to alleviate allergic reactions caused by COVID-19, but care should be taken to avoid drug abuse.61,62 Supplementation with various vitamins can improve the clinical symptoms of Long COVID patients.63
In order to tackle Long COVID efficiently, people should keep up with current developments and take proactive action. A balanced diet, regular physical exercise, appropriate personal protective equipment and vaccination are protective measures for preventing SARS-CoV-2 infection and the development of Long COVID. Early viral clearance during acute phase of COVID-19 may mitigate viral infection and prevent poor clinical outcomes. For individuals with Long COVID, targeted treatment should be provided based on evaluation and a comprehensive management plan should be offered.11 In addition, appropriate use of protective drugs is recommended for patients with high risk of COVID-19. A multicenter cohort study demonstrated that statins significantly reduced mortality in hospitalized COVID-19 patients, with favorable laboratory findings and clinical outcomes.64
Conclusion and Prospects
Studies of Long COVID in Chinese population have found that the most common symptom is fatigue, followed by cough, sore throat, attention disorder, anxiety, muscle or joint pain. To date, treatment strategies for Long COVID mainly focused on symptom relief. Clinical practices have proved that physical therapy, rehabilitation training, psychological support, behavioral cognitive therapy, stem cell therapy and other therapies are beneficial to control the development of Long COVID, which is likely to be a challenge to global healthcare systems and economies for some time. Future researches on Long COVID should be actively carried out, focusing on several directions: 1. Have infected people been vaccinated against COVID-19? 2. Which viral variant is most likely to infect? Are there differences in persistent symptoms among variant infections? 3. What are the long-term organ function changes of the patient? 4. How is the patient’s long-term recovery? 5. Are there any specific organ or tissue injuries? What are the possible pathogenic mechanisms? For the management of Long COVID, a combination of early prevention and active treatment should be adopted to reduce the risk of disease, alleviate clinical symptoms, and improve the quality of life for the potential large population of patients with Long COVID.
Acknowledgments
We would like to thank all those who participated in the project research and paper writing, as well as the reviewers and experts who provided valuable comments.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Caldera-Crespo LA, Paidas MJ, Roy S, et al. Experimental models of COVID-19. Front Cell Infect Microbiol. 2022;11:792584. doi:10.3389/fcimb.2021.792584
2. Umakanthan S, Sahu P, Ranade AV, et al. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96(1142):753–758. doi:10.1136/postgradmedj-2020-138234
3. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133–146. doi:10.1038/s41579-022-00846-2
4. Chinese Center For Disease Control And Prevention. National novel coronavirus infection epidemic situation; 2023. Available from: https://www.chinacdc.cn/jkzt/crb/zl/szkb_11803/jszl_13141/202302/t20230225_263964.html.
5. Tan H, Liu J, Zeng F. China needs a scientific long COVID recovery-support platform. Lancet. 2023;401(10374):344–345. doi:10.1016/S0140-6736(23)00138-1
6. World Health Organization. Post COVID-19 condition (Long COVID). Available from: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition.
7. National Institute for Health and Care Excellence (NICE). COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. London: National Institute for Health and Care Excellence (NICE); 2020.
8. covid.gov. What is Long COVID? Available from: https://www.covid.gov/longcovid/definitions.
9. Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B. Global prevalence of post-coronavirus disease 2019 (COVID-19) condition or long COVID: a meta-analysis and systematic review. J Infect Dis. 2022;226(9):1593–1607. doi:10.1093/infdis/jiac136
10. Wong MC, Huang J, Wong YY, et al. Epidemiology, symptomatology, and risk factors for long COVID symptoms: population-based, multicenter study. JMIR Public Health Surveill. 2023;9:e42315. doi:10.2196/42315
11. Koc HC, Xiao J, Liu W, Li Y, Chen G. Long COVID and its management. Int J Biol Sci. 2022;18(12):4768–4780. doi:10.7150/ijbs.75056
12. Garg M, Maralakunte M, Garg S, et al. The conundrum of ‘long-COVID-19’: a narrative review. Int J Gen Med. 2021;14:2491–2506. doi:10.2147/IJGM.S316708
13. Nabavi N. Long covid: how to define it and how to manage it. BMJ. 2020;370:m3489. doi:10.1136/bmj.m3489
14. Huang L, Li X, Gu X, et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: a longitudinal cohort study. Lancet Respir Med. 2022;10(9):863–876. doi:10.1016/S2213-2600(22)00126-6
15. Sudre CH, Murray B, Varsavsky T, et al. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626–631. doi:10.1038/s41591-021-01292-y
16. Bull-Otterson L, Baca S, Saydah S, et al. Post-COVID conditions among adult COVID-19 survivors aged 18–64 and ≥65 years - United States, March 2020-November 2021. Morb Morta Weekly Rep. 2022;71(21):713. doi:10.15585/mmwr.mm7121e1
17. Yelin D, Moschopoulos CD, Margalit I, et al. ESCMID rapid guidelines for assessment and management of long COVID. Clin Microbiol Infect. 2022;28(7):955–972. doi:10.1016/j.cmi.2022.02.018
18. Davis HE, Assaf GS, McCorkell L, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine. 2021;38:101019. doi:10.1016/j.eclinm.2021.101019
19. l-Aly Z, Bowe B, Xie Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med. 2022;28(7):1461–1467. doi:10.1038/s41591-022-01840-0
20. Cutler DM. The Costs of Long COVID. JAMA Health Forum. 2022;3(5):e221809. doi:10.1001/jamahealthforum.2022.1809
21. Hu F, Zhao Y, Li M, et al. Adverse effects of long COVID and its countermeasures: a review. Chin J Public Health. 2022;38(09):1229–1232.
22. Liang L, Yang B, Jiang N, et al. Three-month follow-up study of survivors of coronavirus disease 2019 after discharge. J Korean Med Sci. 2020;35(47):e418. doi:10.3346/jkms.2020.35.e418
23. Zhang X, Wang F, Shen Y, et al. Symptoms and health outcomes among survivors of COVID-19 infection 1 year after discharge from hospitals in Wuhan, China. JAMA Netw Open. 2021;4(9):e2127403. doi:10.1001/jamanetworkopen.2021.27403
24. Chen Q, Wang W, Shi X, et al. Seroepidemiology of pertussis in the east of China: estimates of incidence of infection in adolescents and adults pre- and post-COVID-19. Front Public Health. 2022;10:1054617. doi:10.3389/fpubh.2022.1054617
25. Tang YF, Han JY, Ren AM, et al. Assessment of long-term effects on pulmonary functions between severe and non-severe convalescent COVID-19 patients: a single-center study in China. J Inflamm Res. 2022;15:4751–4761. doi:10.2147/JIR.S371283
26. Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–232. doi:10.1016/S0140-6736(20)32656-8
27. Lopez-Leon S, Wegman-Ostrosky T, Perelman C, et al. More than 50 Long-term effects of COVID-19: a systematic review and meta-analysis. medRxiv. 2021;2021:21250617 doi:10.1101/2021.01.27.21250617.
28. Ju N, Yang X, Ma X, et al. Hospitalization, interpersonal and personal factors of social anxiety among COVID-19 survivors at the six-month follow-up after hospital treatment: the minority stress model. Eur J Psychotraumatol. 2022;13(1):2019980. doi:10.1080/20008198.2021.2019980
29. Yuan Y, Zhao YJ, Zhang QE, et al. COVID-19-related stigma and its sociodemographic correlates: a comparative study. Global Health. 2021;17(1):54. doi:10.1186/s12992-021-00705-4
30. Xiao X, Yang X, Zheng W, et al. Depression, anxiety and post-traumatic growth among COVID-19 survivors six-month after discharge. Eur J Psychotraumatol. 2022;13(1):2055294. doi:10.1080/20008198.2022.2055294
31. Mei Z, Wu X, Zhang X, et al. The occurrence and risk factors associated with post-traumatic stress disorder among discharged COVID-19 patients in Tianjin, China. Brain Behav. 2022;12(2):e2492. doi:10.1002/brb3.2492
32. Fu L, Fang Y, Luo D, et al. Pre-hospital, in-hospital and post-hospital factors associated with sleep quality among COVID-19 survivors 6 months after hospital discharge: cross-sectional survey in five cities in China. BJPsych Open. 2021;7(6):e191. doi:10.1192/bjo.2021.1008
33. Liu YH, Wang YR, Wang QH, et al. Post-infection cognitive impairments in a cohort of elderly patients with COVID-19. Mol Neurodegener. 2021;16(1):48. doi:10.1186/s13024-021-00469-w
34. Shang YF, Liu T, Yu JN, et al. Half-year follow-up of patients recovering from severe COVID-19: analysis of symptoms and their risk factors. J Intern Med. 2021;290(2):444–450. doi:10.1111/joim.13284
35. Weng J, Li Y, Li J, et al. Gastrointestinal sequelae 90 days after discharge for COVID-19. Lancet Gastroenterol Hepatol. 2021;6(5):344–346. doi:10.1016/S2468-1253(21)00076-5
36. General Office of the National Health Commission(China), Rehabilitation Program for discharged COVID-19 Patients (Trial). Available from: http://www.nhc.gov.cn/xcs/zhengcwj/202003/d4558d2cc35e44d5b9adba7c911e0b4c.shtml.
37. Kim Y, Kim SE, Kim T, et al. Preliminary guidelines for the clinical evaluation and management of long COVID. Infect Chemother. 2022;54(3):566–597. doi:10.3947/ic.2022.0141
38. Mandal S, Barnett J, Brill SE, et al. ‘Long-COVID’: a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax. 2021;76(4):396–398. doi:10.1136/thoraxjnl-2020-215818
39. Cervia C, Zurbuchen Y, Taeschler P, et al. Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome. Nat Commun. 2022;13(1):446. doi:10.1038/s41467-021-27797-1
40. Liao B, Liu Z, Tang L, et al. Longitudinal clinical and radiographic evaluation reveals interleukin-6 as an indicator of persistent pulmonary injury in COVID-19. Int J Med Sci. 2021;18(1):29–41. doi:10.7150/ijms.49728
41. Zhao YM, Shang YM, Song WB, et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine. 2020;25:100463. doi:10.1016/j.eclinm.2020.100463
42. Marvisi M, Ferrozzi F, Balzarini L, Mancini C, Ramponi S, Uccelli M. First report on clinical and radiological features of COVID-19 pneumonitis in a Caucasian population: factors predicting fibrotic evolution. Int J Infect Dis. 2020;99:485–488. doi:10.1016/j.ijid.2020.08.054
43. Phetsouphanh C, Darley DR, Wilson DB, et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol. 2022;23(2):210–216. doi:10.1038/s41590-021-01113-x
44. Umakanthan S, Patil S, Subramaniam N, Sharma R. COVID-19 vaccine hesitancy and resistance in India explored through a population-based longitudinal survey. Vaccines. 2021;9(10):1064. doi:10.3390/vaccines9101064
45. Brannock MD, Chew RF, Preiss AJ, et al. Long COVID risk and pre-COVID vaccination in an EHR-based cohort study from the RECOVER program. Nat Commun. 2023;14(1):2914. doi:10.1038/s41467-023-38388-7
46. Gao P, Liu J, Liu M. Effect of COVID-19 vaccines on reducing the risk of long COVID in the real world: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19(19):12422. doi:10.3390/ijerph191912422
47. National Health Commission of the People’s Republic of China. The dynamics of epidemic prevention and control. Available from: http://www.nhc.gov.cn/xcs/yqfkdt/202109/bf2cf785ce0544ae818a76ffbb18ca79.shtml.
48. Umakanthan S, Bukelo MM, Gajula SS. The Commonwealth Caribbean COVID-19: regions resilient pathway during pandemic. Front Public Health. 2022;10:844333. doi:10.3389/fpubh.2022.844333
49. Umakanthan S, Lawrence S. Predictors of COVID-19 vaccine hesitancy in Germany: a cross-sectional, population-based study. Postgrad Med J. 2022;98(1164):756–764. doi:10.1136/postgradmedj-2021-141365
50. Wang S, Li Y, Yue Y, et al. Adherence to healthy lifestyle prior to infection and risk of post-COVID-19 condition. JAMA Intern Med. 2023;183(3):232–241. doi:10.1001/jamainternmed.2022.6555
51. Li J, Xia W, Zhan C, et al. A telerehabilitation programme in post-discharge COVID-19 patients (TERECO): a randomised controlled trial. Thorax. 2022;77(7):697–706. doi:10.1136/thoraxjnl-2021-217382
52. Liu Z, Qiao D, Xu Y, et al. The efficacy of computerized cognitive behavioral therapy for depressive and anxiety symptoms in patients with COVID-19: randomized controlled trial. J Med Internet Res. 2021;23(5):e26883. doi:10.2196/26883
53. Li J, Li X, Jiang J, et al. The effect of cognitive behavioral therapy on depression, anxiety, and stress in patients with COVID-19: a randomized controlled trial. Front Psychiatry. 2020;11:580827. doi:10.3389/fpsyt.2020.580827
54. He Y, Yang L, Zhu X, et al. Mental health chatbot for young adults with depressive symptoms during the COVID-19 pandemic: single-blind, three-arm randomized controlled trial. J Med Internet Res. 2022;24(11):e40719. doi:10.2196/40719
55. Bramante C, Buse JB, Liebovitz D, et al. Outpatient treatment of COVID-19 and the development of long COVID Over 10 Months: A multi-center, quadruple-blind, parallel group randomized phase 3 trial. Lancet. 2023.
56. EINPRESSWIRE. Adult stem cell therapy for COVID-19 sequelae begins in Japan for the first time in the world; 2020. Available from: https://www.einpresswire.com/article/532284733/adult-stem-cell-therapy-for-covid-19-sequelae-begins-in-japan-for-the-first-time-in-the-world.
57. Shi L, Yuan X, Yao W, et al. Human mesenchymal stem cells treatment for severe COVID-19: 1-year follow-up results of a randomized, double-blind, placebo-controlled trial. EBioMedicine. 2022;75:103789 doi:10.1016/j.ebiom.2021.103789.
58. Zilberman-Itskovich S, Catalogna M, Sasson E, et al. Hyperbaric oxygen therapy improves neurocognitive functions and symptoms of post-COVID condition: randomized controlled trial. Sci Rep. 2022;12(1):11252.
59. Hawkins J, Hires C, Keenan L, Dunne E. Aromatherapy blend of thyme, Orange, clove bud, and frankincense boosts energy levels in post-COVID-19 female patients: a randomized, double-blinded, placebo controlled clinical trial. Complement Ther Med. 2022;67:102823.
60. D’Ascanio L, Vitelli F, Cingolani C, Maranzano M, Brenner MJ, Di Stadio A. Randomized clinical trial “olfactory dysfunction after COVID-19: olfactory rehabilitation therapy vs. intervention treatment with Palmitoylethanolamide and Luteolin”: preliminary results. Eur Rev Med Pharmacol Sci. 2021;25(11):4156–4162.
61. Glynne P, Tahmasebi N, Gant V, Gupta R. Long COVID following mild SARS-CoV-2 infection: characteristic T cell alterations and response to antihistamines. J Investig Med. 2022;70(1):61–67. doi:10.1136/jim-2021-002051
62. Pinto MD, Lambert N, Downs CA, et al. Antihistamines for Postacute Sequelae of SARS-CoV-2 Infection. J Nurse Pract. 2022;18(3):335–338 doi:10.1016/j.nurpra.2021.12.016.
63. Naureen Z, Dautaj A, Nodari S, et al. Proposal of a food supplement for the management of post-COVID syndrome. Eur Rev Med Pharmacol Sci. 2021;25(1 Suppl):67–73 doi:10.26355/eurrev_202112_27335.
64. Umakanthan S, Senthil S, John S, et al. The effect of statins on clinical outcome among hospitalized patients with COVID-19: a multi-centric cohort study. Front Pharmacol. 2022;13:742273. doi:10.3389/fphar.2022.742273
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.