")
Back to Journals » International Journal of Women's Health » Volume 15
Reasons for Not Seeking Healthcare Among Students with Dysmenorrhea: A Qualitative Study
Authors Getahun SB , Berhe S , Mekonnen B, Melaku G
Received 26 August 2023
Accepted for publication 8 November 2023
Published 11 November 2023 Volume 2023:15 Pages 1733—1744
DOI https://doi.org/10.2147/IJWH.S437233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Senait Belay Getahun,1,* Semarya Berhe,2,* Bazie Mekonnen,2,* Getnet Melaku1,*
1Department of Midwifery, College of Health Sciences and Medicine, Dilla University, Dilla, Ethiopia; 2School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
*These authors contributed equally to this work
Correspondence: Senait Belay Getahun, Dilla University, College of Health Sciences and Medicine, P.O Box: 419, Dilla, Ethiopia, Tel +251914457474, Email [email protected]
Background: Dysmenorrhea is a significant health burden for women and a global public health issue. Despite its notable prevalence and impact, dysmenorrhea is mostly poorly identified, treated, and accepted as normal by patients themselves. To create strategies that enable care seeking and ideal symptom management for dysmenorrhea, it is vital to have a better understanding of the reasons why women do not seek medical attention. This study aimed to explore the reasons for not seeking healthcare among students with dysmenorrhea at Dilla University in 2023.
Methods: A qualitative phenomenological study was conducted with purposively selected Colleges of Dilla University students with dysmenorrhea. An individual in-depth interview with a semi-structured interview guide was used to collect data from March 1– 30/2023. Snowball sampling was used to obtain study participants, and sampling was determined based on the level of data saturation. The interviews were conducted in a separate private room at Dilla University. Data analysis was started simultaneously with data collection and thematic analysis was performed. ATLAS. ti 9 qualitative software was used to support the data analysis and management.
Results: The study enrolled 20 students with dysmenorrhea, with a mean age of 21.55 years and a mean age of menarche of 14.45 years. It explored three themes for reasons for not seeking healthcare: sociocultural and personal factors, healthcare system-related perceptions and experiences, and preference for self-management of symptoms. The study also reported myths and misconceptions, negative attitudes and experiences, and self-care practices as barriers to accessing and utilizing health care services.
Conclusion: This study identified various reasons for not seeking healthcare among students with dysmenorrhea. Most of these reasons indicate that there is insufficient awareness and misconception of dysmenorrhea and its management. Therefore, this study advances the literature on dysmenorrhea and emphasizes the need for more awareness, education, and quality healthcare services for students with dysmenorrhea. The study also proposes future research directions to address the problem of dysmenorrhea among female students in Ethiopia.
Keywords: reason, dysmenorrhea, healthcare seeking, female students
Introduction
The health of women and girls is a special issue because in many communities, they face discrimination based on socio-cultural factors that disadvantage them. Uneven power relations between men and women, social norms that restrict access to education and paid employment opportunities, a sole focus on women’s reproductive roles, and the potential or actual experience of physical, sexual, and emotional violence are just a few of the socio-cultural factors that prevent women and girls from receiving quality healthcare and achieving the highest level of health including menstrual pain or dysmenorrhea.1,2
Dysmenorrhea, or painful menstruation, is a common gynecological condition that affects many women around the world, which is characterized by intense cramping in the lower abdomen that often comes with other symptoms such as sweating, headaches, nausea, vomiting, diarrhea, and trembling.3,4 Dysmenorrhea can be classified into two types: primary dysmenorrhea, which has no underlying organic cause, and secondary dysmenorrhea, caused by pelvic diseases such as endometriosis. Dysmenorrhea is triggered by the release of prostaglandins, which cause uterine contractions and inflammation.3–6
The prevalence of primary dysmenorrhea among women of reproductive age varies widely across countries and regions, ranging from 50 to 90%, which means that more than 855 million women worldwide suffer from this condition.7,8 Among female students in Ethiopia, the prevalence of primary dysmenorrhea is estimated to be 71.69% (66.82–76.56%).8,9 Dysmenorrhea has a significant negative impact on the physical, psychological, social, and academic aspects of women’s lives, which can impair their daily functioning and productivity, reduce their quality of life and well-being, and increase their risk of depression and anxiety.6 Dysmenorrhea can also affect their educational attainment and career opportunities, as it may cause them to miss classes or work–1-3 days every month. Dysmenorrhea can lead to serious health complications if left untreated or misdiagnosed. For example, secondary dysmenorrhea caused by endometriosis can result in infertility, chronic pelvic pain, ovarian cysts, and adhesions.6,8,10
Health-seeking behavior (HSB) is defined as any action taken by individuals who perceive themselves as having a health problem or illness to find suitable treatment. HSB is influenced by several factors, such as availability, affordability, accessibility, acceptability, and quality of healthcare services, as well as individual characteristics, such as knowledge, attitude, beliefs, preferences, severity of illness, and coping strategies. Understanding HSB is important for designing effective interventions to improve health outcomes and reduce health disparities.11–13
Although dysmenorrhea is a treatable health condition, different studies in different parts of the world, including Ethiopia, revealed poor health-seeking behavior, ranging from (5.8% to-50.6%) among females with this condition.14–18
For early diagnosis, successful treatment, and implementation of relevant interventions, planning for health care policies and programs necessitates knowledge of reasons for not seeking health care.
Despite several studies that conducted on the prevalence and impact of dysmenorrhea in Ethiopia, there is limited information on why women with dysmenorrhea do not seek healthcare in Ethiopia. This study aimed to explore the reasons for not seeking healthcare among students with dysmenorrhea at Dilla University, Ethiopia. This study has several implications for future research, policy, practice, and education. This study contributes to the existing literature on dysmenorrhea by providing insights into the socio-cultural and personal factors that influence HSB among Ethiopian women with this condition. It will also inform policymakers and practitioners about the need for greater awareness, education, and quality healthcare services for women with dysmenorrhea in Ethiopia. Furthermore, it suggests future research directions to explore the perspectives of other stakeholders, such as families, communities, and healthcare providers, and evaluate the effectiveness of different interventions to improve the awareness and management of dysmenorrhea among female students in Ethiopia.
Methods
Study Setting
This was a qualitative study with a phenomenological design conducted at Dilla University from March 1–30, 2023. Dilla University is located in Dilla Town, Gedeo Zone, SNNPR, Ethiopia, 360 km from Addis Ababa. The university has four campuses, seven colleges, two institutes, and three schools that offer more than 47 undergraduate and 24 postgraduate programs with a student population of more than 31,000 in regular and continuing education programs. Among the total number of students, about 35.5% are females.19
Study Participants and Sampling
The study participants were female undergraduate students with dysmenorrhea from two purposively selected colleges of Dilla University (College of Engineering and Technology and College of Business and Economics) who were active in teaching and learning activities during the study period. The inclusion criteria were having dysmenorrhea, being willing to participate in the study, and providing informed consent. The exclusion criterion was severe illness at the time of data collection.
The sample size was determined based on the level of saturation during data collection. To prevent data saturation, we have tried to diversify the study participants by including those from various departments, academic years, and previous residences. Snowball sampling was used to recruit participants who could provide rich and detailed information on their reasons for not seeking healthcare for menstrual pain. The first two participants were recruited from the zero plan of Dilla University. All potential participants were asked to describe their symptoms of dysmenorrhea and healthcare-seeking behavior, and we then selected participants based on the operational definition of the study. The total number of study participants on which the level of saturation achieved was 20 students with dysmenorrhea.
Data Collection Tool and Procedure
Data was collected through individual in-depth interviews using an interview guide developed based on the relevant areas necessary to address the study aim. Before beginning the research interviews, pilot interviews were conducted with three participants other than the main participants. The interview guide has been modified in line with the pilot test. Open-ended questions were used to lead the discussion. The principal investigator and a trained female research assistant in the Amharic language in a separate private room where the participants felt comfortable and free from interruption conducted the interviews. The interviews lasted for approximately 20–40 minutes each. Probing questions were used to elicit more information and clarify the participants. The interviews were audio-recorded with the consent of the participants and field notes were taken. The audio recordings were transcribed verbatim and translated into English by a language expert on the same day.
Operational Definitions
Dysmenorrhea: Is defined as painful menstruation involving cramps in the lower abdomen, groin pain, backache, waist pain, and thigh pain occurring just before or during menstruation.3 Health-seeking behavior: For this study, it is defined as seeking medical treatment from health care facilities (hospital, health center, clinics) for their dysmenorrhea.
Data Processing and Analysis
The ATLAS.ti 9 software supported the data analysis. A thematic analysis approach was used to identify and organize themes and subthemes from the data. The following six steps were followed during data analysis.20
- Verbatim transcription: Audio recordings of the interviews were transcribed and translated verbatim from Amharic to English by a language expert. The transcripts were read repeatedly to familiarize us with the data and to check for accuracy and completeness.
- Coding: The data were organized into meaningful and systematic codes using ATLAS.ti 9 software. Both priori codes and inductive codes emerging from the data were used.
- Generating themes: We examined the codes for clarity and consistency by selecting a given text, and several codes were combined into a single theme.
- Reviewing themes: We tested the themes for usefulness and accurate representation of the data.
- Interpretation: We interpreted the coded data and described their themes and categories. In this step, the final list of themes was named and defined.
- Write-up: We presented the analyzed data with the selected verbatim transcriptions of respondents embedded within each theme and subtheme.
Trustworthiness
Four criteria were considered to ensure the trustworthiness of the findings: credibility, dependability, transferability, and conformability.
Credibility: To enhance credibility, we used prolonged engagement with the study site and participants to gain an in-depth understanding of the context and phenomena under study. We also used peer debriefing to discuss our findings with peers who were trained in qualitative research and received feedback on our interpretations. An audio recorder was used during the data collection to capture the exact words of the participants.
Dependability: To ensure dependability, we used an audit trial to document all the steps involved in data collection and analysis. We also saved audio records of the interviews, field notes, transcripts, codes, and themes for crosschecking and verification purposes. We also used a code-recode method to check for consistency in coding by recording transcripts after a period.
Transferability: To enhance transferability, we provided a thick description of the research context, method, participants, and findings so that readers could judge the applicability of our findings to other settings or populations.
Conformability: To establish conformability, we reflected on our prior personal expectations and experiences to reduce bias during the data collection and analysis. We also used verbatim quotes from participants to support our findings and show that they reflected their views rather than ours.
Result
The findings of this study have been presented in two sections with the aim of exploring the reasons for not seeking healthcare among students with dysmenorrhea at Dilla University Dilla, Ethiopia. The first portion provides socio-demographic and menstrual characteristics of the participants, and the second part presents the themes, subthemes, and codes that emerged.
Socio-Demographic Profiles of Participants
Twenty participants with dysmenorrhea were enrolled in this study. The mean age of the participants was 21.55 (±SD = 1.191) years, and all of them were single in marital status. Three-quarters of them had previously resided in urban areas. Regarding the duration of menstrual bleeding, 95% of the students bleed for 2–7 days and 90% of them reported a menstrual cycle of 21–35 days. In contrast, the mean age of menarche among the students was 14.45 years (±SD = 1.504), and their average monthly income was 1000 ETB (Table 1).
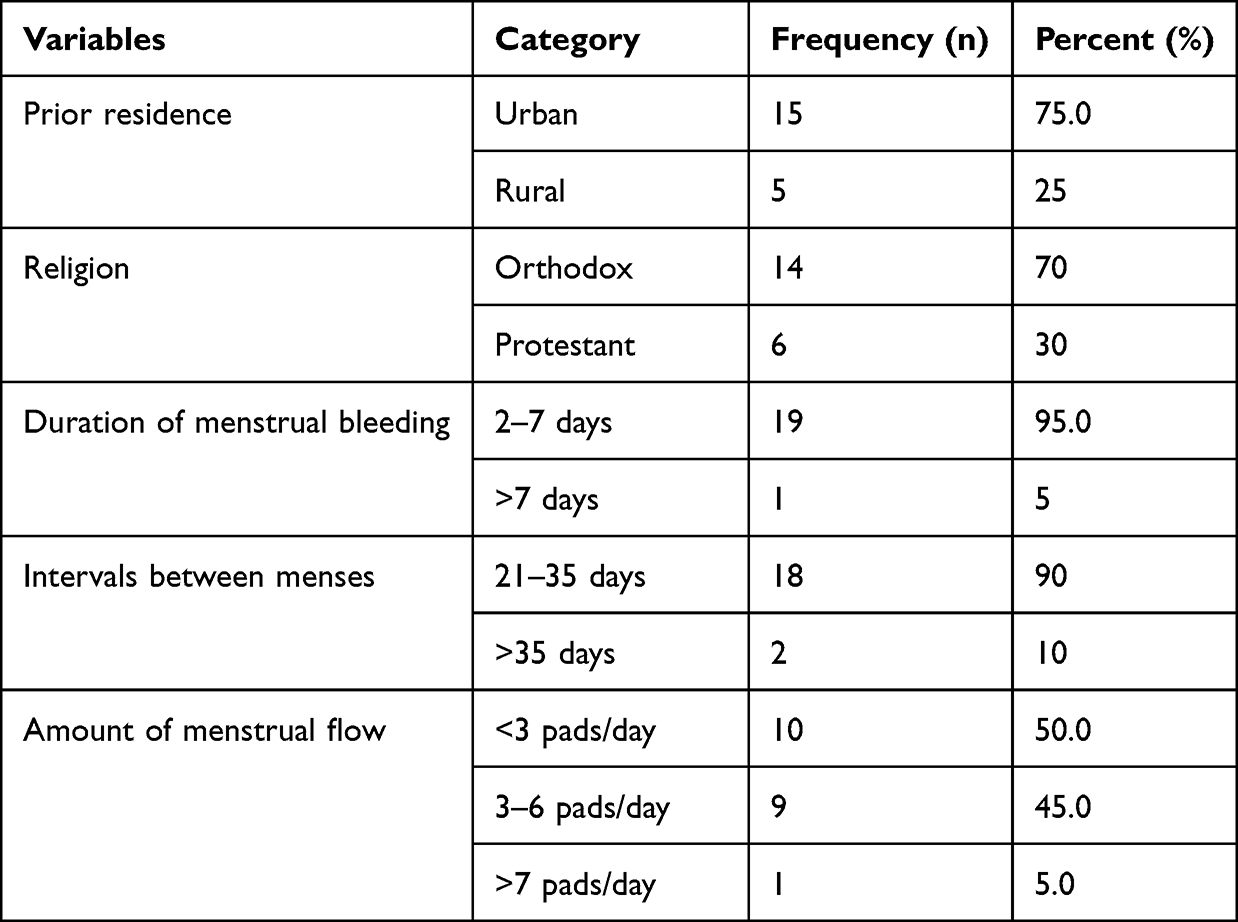 |
Table 1 Socio-Demographic and Menstrual Characteristics of Participants Who Suffered from Dysmenorrhea (n=20) |
Emerged Themes
In this study, three themes were emerged from the analysis of students in depth interviews. The themes were identified as rich and detailed accounts of the reasons for not seeking healthcare among students with dysmenorrhea at Dilla University. The following table (Table 2) summarizes these themes with their respective subthemes and codes.
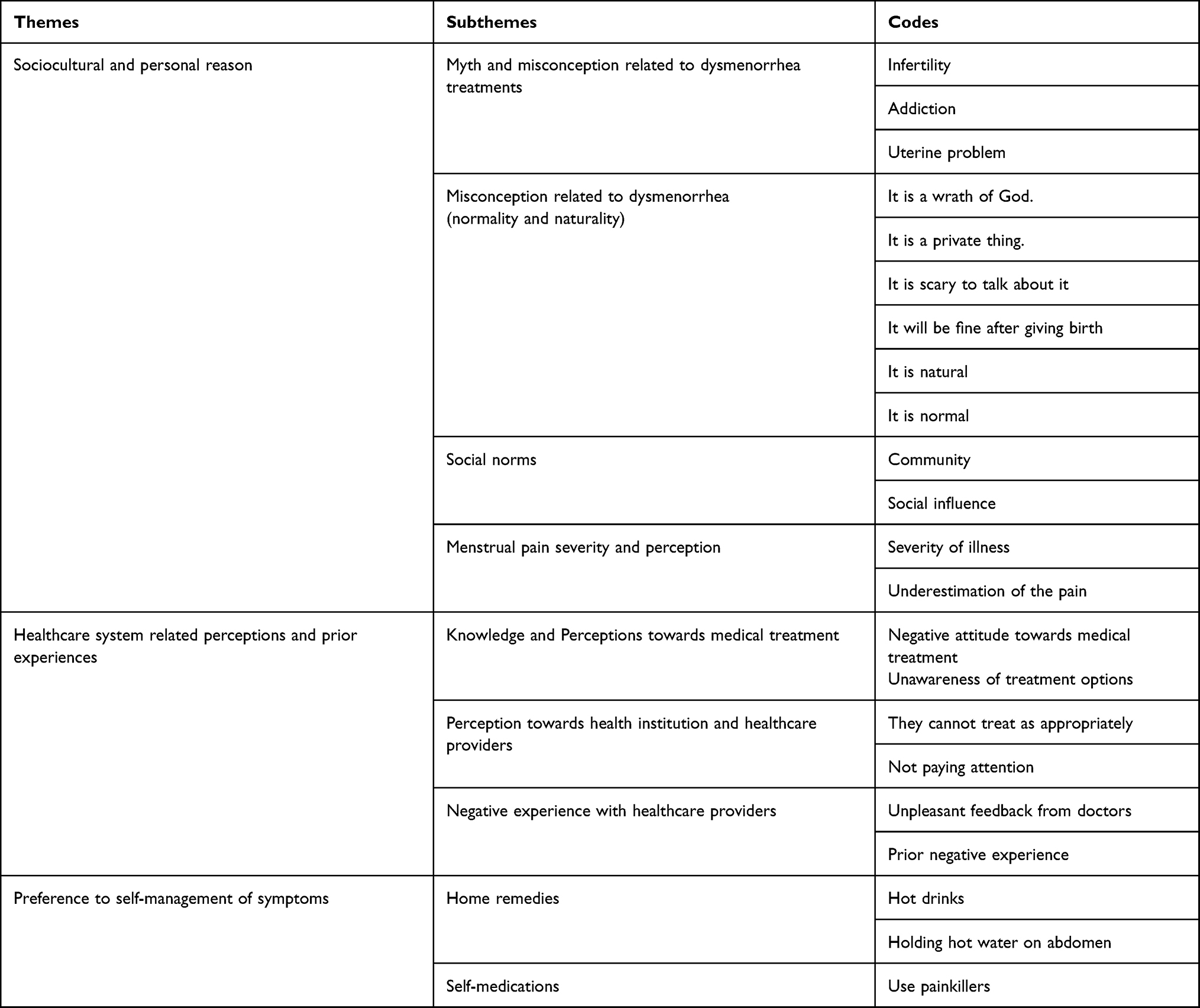 |
Table 2 Themes, Subthemes, and Codes Emerged from the in-Depth Interviews of Student with Dysmenorrhea About Reasons for Not Seeking Healthcare at Dilla University in 2023 |
Theme 1: Sociocultural and Personal Reasons for Not Seeking Healthcare
In this study, most participants stated that social, cultural, and personal reasons are the one that makes them not utilize healthcare services for their pain during menstruation. Under this main theme, myths and misconceptions related to medications for dysmenorrhea, misconceptions related to dysmenorrhea, belief that dysmenorrhea is natural and normal, and social norms were grouped as subthemes.
Myths and Misconceptions Related to Medications for Dysmenorrhea
Study participants listed that fear of being infertile; fear of being addicted to medications, and fear of the medication used to treat menstrual pain causing uterine damage are some of the reasons for not seeking healthcare. This study found that participants believed that the medications used to treat dysmenorrhea could eventually result in infertility and other uterine problems.
A 23-year-old student said that
I was very willing to go, but when I consulted with my friends, they told me that it prevents birth, if I take that medication too often, I may not be able to give birth. (IDI 5)
Some study participants also said that they were not going to go to healthcare facilities because of fear of the habit of the medication used for menstrual pain. Believing that once they started to use these medications, they could not survive without them or even worsen the pain. A 22-year student said she had a fear of using drugs because she lived in a rural area where the healthcare facilities are not assessable, so if she becomes addicted, where they should receive those treatments. She expressed her fear like,
When I wanted to go and consult my friends, they always told me that if I use treatment, I might become addicted, so I gave up going. I mean, I live in a rural area where there is no medical treatment, so I did not go. (IDI 4)
Others also stated that they fear long-term damage from the medications used to treat dysmenorrhea and are not willing to seek medical treatment.
One student stated her concern like
…You may not know anything at this point, but I have heard people say that it could cause uterine damage in the future. I heard the family talking about it (IDI 17).
Misconception Related to Dysmenorrhea
When students described their reason for not seeking healthcare under this subtheme, they said that menstruation pain is a wrath of God, a personal thing, and a scary to talk about it. Some study participants also perceived dysmenorrhea as a curse, so they believed it did not have treatment and considered it a personal thing that was never communicated comfortably.
One student said
…we used to associate menstruation with curses. We considered it a shame. Because of this, I would not go to seek treatment, I would not talk about it to people, and I would consider it a curse. (IDI 18)
Another student believed that menstruation problems are a personal issue, and it is not good to expose our secrets to others
I don’t think it is useful to expose a personal secret or a private matter because menstruation is a privacy issue (IDI 20).
Belief That Dysmenorrhea is Natural and Normal
This subtheme captures how the participants perceive dysmenorrhea as a natural, tolerable, and normal phenomenon that does not have a specific cause or solution and their attitude towards dysmenorrhea. Most students in this study accepted menstrual pain as a normal part of their life, and it is believed to be a gift for being a woman. One student as mentions it
… It is something that happens to everyone, I think that when the period comes, everyone gets sick because it is an inevitable thing; so, I have never thought about whether there is a solution. (IDI 11)
Others even think that complaints about menstrual pain are a sign of not accepting nature.
I do not think we should think that this issue is difficult, because it is given to us by nature. Thinking that menstrual pain is serious shows that we cannot accept what is given to us by nature. (IDI 18).
The other thing mentioned in this subtheme is the severity of menstrual pain and pain perception, and respondents believed that menstruation pain is not something that can cause any harm, and it is not necessary to go to healthcare. Some of these students believe that visiting healthcare facilities is necessary for those who are severely ill, which means that they are incapable of treating themselves otherwise better to tolerate it.
A 20-year-old student said,
I advised those who are severely ill to have a follow-up with doctors; otherwise, I thought they could get better by using natural remedies like ginger tea (IDI 2).
Social Norms/Reasons
In this study, some students said that the community in which they grew up and their families influenced their healthcare-seeking behavior. In most cases, it is considered a path that every woman passes through, so it is difficult to seek care, even if you are willing to do so.
A 20-year-old student said
…many times, health centers and hospitals only give you birth control and I do not go to see a doctor thinking that it is not good from a community perspective because that stuff would make us sick. (IDI 6)
Some students also claimed that it is difficult to talk about menstrual pain in their culture because it is unfamiliar to them; they did not grow up communicating such things openly. Therefore, they thought it was not good to talk about it.
A 21-year-old student said,
it is hard to talk openly about it outside of your peer group and outside of your gender. I do not think they will have a pleasant view if we talk about menstruation openly. (IDI 20).
Theme 2: - Healthcare System Related Perceptions and Prior Experiences
Healthcare-related reasons are one of the most mentioned reasons for not seeking healthcare among students with dysmenorrhea and three subthemes emerged prior negative experience with healthcare providers, knowledge, and Perceptions towards the medical management of menstrual pain and perception toward health institutions.
Prior Negative Experience from Healthcare Providers
Students who have negative experiences previously while seeking healthcare for other diseases did not prefer to go to health facilities for their menstruation pain because they believed healthcare providers would not do any better.
As witnessed by a 3rd year student
I do not want to go to the doctor’s office. I have developed a lot of hatred toward doctors. I go to the doctor’s office many times when our friends get sick. I know many of them are unprofessional; they show us so uncaring faces and do not bother. which is an ugly thing. I do not know why they neglect us. (IDI 10)
Some of the respondents had also experienced healthcare providers who would joke about their concerns instead of being supportive and that makes them not to utilizing healthcare services for their pain. A 2nd-year student supports this:
My friends used to go clinic and tell me that the health professionals joked about their condition; For example, one time one of my friends went to seek help, and the health professional said to her— ‘Go with men, and don’t go anymore’—joking about her concern and she came back embarrassed; They made her not to go a second time (IDI 17).
Knowledge and Perception Towards the Medical Management of Menstrual Pain
According to the responses of some study participants, they had a negative attitude toward the medication for menstrual pain. They believed that the pain has no medical treatment, and they would not get better by seeking healthcare. A 4th-year student says,
I don’t think I will ever find a treatment for it, and I don’t regard it as an illness; therefore, I didn’t think to go to seek treatment do you to my beliefs. (IDI 9)
Some of the study participants are also uninformed of the availability of treatments for their pain during menstruation. They did not have any idea about the medical treatment of menstrual pain.
As a 3rd-year student mentioned,
I have no idea. I have not even thought about getting treated. When you came and told us you came to ask about it, I had just started to think about it. Does this condition have a medicine? Isn’t being sick normal? You made me think about it. (IDI 11)
Perception Towards Health Institutions and Healthcare Providers
Most students perceived healthcare facilities are not capable of treating their pain; healthcare professionals and even the healthcare system have not paid attention to this issue. They believed that if concerned bodies are not working on treating our pain it cannot be possible in this situation. 5th year student mentions it,
The clinics and health stations are not organized; it would be nice to pay more attention to Menstruation pain (IDI 2).
Another student expressed her concern
I do not think it is possible to get the necessary help in our healthcare institutions; because we used to go to the clinics, not for menstrual pain but for other conditions, and the doctors were not giving appropriate care. So, I do not think they will give you anything good for menstrual pain. (IDI 5)
Moreover, some study participants claimed the healthcare provider’s willingness to treat their menstruation pain was a barrier to seeking healthcare. They believed that the healthcare providers are not ready to give care to us. A 3rd-year student supports this idea,
I do not think so. I am referring to the health services in my institution, for example. The staff members do not care about menstrual pain. It is uncomfortable the way they welcome us to even another sickness, let alone the most crucial thing. This is why, since it is a women’s specific case, I believe they do not treat it appropriately. (IDI 6)
Theme 3: - Preference to Self-Management of Symptoms
In this study, almost all (19 out of 20) used various methods to manage their symptoms by themselves either using home remedies or self-medication with over-The-counter analgesics, such as diclofenac, ibuprofen, and meloxicam.
Home Remedies
Most students attempted to manage their symptoms during menstruation by using diverse mechanisms at home. They drank hot beverages, such as tea made of ginger, nut, or coca, and juice. A 3rd-year student supports this,
Yes, I’ve seen something from people and my sisters, I drink Coca, and now I massage my stomach with hot water and drink hot things like ginger tea (IDI 6).
Another student states that she used Ethiopian traditional alcohol called Areqi, and lemon to relieve the pain
I have tried many times to treat period pain. For example, when I use sour things, like lemon, liquor, etc., on the first day of my period, the pain will go away. (IDI 18)
Others would hold hot water on their abdomen, sleep, and wear additional clothes during menstruation.
As a 5th-year student says,
For the illness, we drink coca and hot thing, but it has back pain, we tie the waist, hold hot water, and we wear additional clothes.
Self-Medication
Among twenty students interviewed in this study, five students prefer to self-medicate instead of visiting healthcare for their menstrual pain. They believed that menstruation pain is not something that makes us unwell once it occurs monthly, thus it is inappropriate to visit healthcare facilities every month. They thought it was better to take painkillers instead of going to the doctor.
As one student said,
I take painkillers on my own; it reduces my pain and then I move on, so I do not pay that much attention. I have tried to treat it at home, but I have never gone to a doctor’s office. (IDI 2)
Students with dysmenorrhea mentioned drugs, such as Advil, diclofenac, ibuprofen, and meloxicam.
Discussion
This qualitative study aimed to explore the reasons for not seeking healthcare for dysmenorrhea among Dilla University students. Understanding the reasons why students with dysmenorrhea may avoid healthcare is essential for developing effective prevention and management strategies. We found that sociocultural and personal reasons, prior negative experiences and perceptions towards the healthcare institutions and healthcare professionals, and preference for self-management of symptoms were the major reasons for not seeking healthcare among students with a history of dysmenorrhea.
In this study, fear of side effects of medications used to treat menstruation pain was a notable reason for not seeking healthcare. Even though evidence proved that delayed diagnosis and management of secondary dysmenorrhea influences women’s fertility in this study students perceived that the drugs which are prescribed for menstrual pain treatment may result in infertility, and unable to get pregnant. These findings were also reported by a study done in Lebanon in which sociocultural obstacles, including worries about potential infertility, are the reasons why students choose not to utilize oral contraceptives as a treatment for menstrual pain.16 Another reason for not seeking healthcare for menstrual pain was fear of uterine problems in the future. Moreover, students’ fear of becoming addicted to drugs was another reason related to myths and misconceptions. However, there is no scientific base for this; it may be due to inadequate knowledge and misinformation about menstrual pain management strategies.
Misconceptions such as considering menstruation pain as a curse that comes from God, personal things that are not talked to others, and it is just a scary thing to talk about were the other reasons for poor healthcare-seeking behavior among students. These findings agree with previous studies in the United States, and Lebanon, which reported that they are hesitant to seek medical attention because they are ashamed or embarrassed to discuss their menstrual problems with others.4,16
Others in this study thought that menstrual pain is a natural and expected aspect of womanhood and that it is not necessary to seek medical attention. These results are comparable to studies conducted in Spain, Australia, and the United States, which showed that people’s access to information may be limited and skewed by their own experiences and/or those of their family members, who may influence their perceptions of what is “normal”.5,20,21 These misconceptions may stem from a lack of adequate education and awareness about menstrual health, as well as cultural and religious influences that stigmatize menstruation and dysmenorrhea. Indicating the gap that our teaching and learning activities are not emphasizing reproductive health.
Social norms, and the community in which they grew up, including their families, were the other undeniable reasons for not seeking healthcare among students with dysmenorrhea in this study. Accordingly, menstrual pain has not been given that much emphasis in our community or it has not been considered a disease; they have just accepted it as it is. These findings are in parallel with previous studies that found menstrual stigma restricts access to precise management advice in the home and medical sectors.22,23 It indicates that community-wide initiatives are needed to raise knowledge of menstruation pain and its treatment. The severity of the menstrual pain of students was also the other reason preventing them from seeking healthcare. They believed that seeking healthcare is only necessary for those who are severely ill. This is in line with the study conducted in Hong Kong, India, and Ethiopia, in which a decision to seek healthcare among girls with dysmenorrhea is associated with the severity of pain, the more they have severe kinds of symptoms the more they seek medical care.24–26 It might be associated with how each person experiences pain and suggest that making people aware of normal and abnormal menstruation is essential.
In this study, perceptions towards health institutions and healthcare providers were also found as significant reasons for not seeking healthcare for their menstrual pain. They perceived healthcare facilities and providers are not capable of treating their pain; even the healthcare system has not paid attention to this issue. These findings are consistent with studies in the United States and Spain, which reported young women do not expect much from healthcare professionals and healthcare providers did not view dysmenorrhea as a legitimate problem and often show little empathy.4,20,27 This shows that women are not comfortable with the care and endeavors are needed to correct the healthcare provision.
Moreover, study participants claimed they were not aware of the available treatment options for dysmenorrhea. These findings are in line with a study conducted in the United States which reported inadequate knowledge of women about the existence of treatments that could ease their symptoms. Besides, some of our participants had negative perceptions of medical treatments and the medication given for dysmenorrhea. This might be due to a lack of awareness or misconception about dysmenorrhea and its treatment.
Prior negative experiences with healthcare providers while seeking healthcare for other diseases were also notable reasons for poor healthcare-seeking behavior for menstrual pain in this study. They believed healthcare providers would not do any better and would be a waste of time to visit health facilities. Similarly, a study from the United States found that participants who had bad experiences with previous providers who did not help them with other medical problems confirmed their beliefs that providers would be useless in treating dysmenorrhea.4 It indicates a lack of empathy, respect, or competence among some healthcare workers who deal with women’s reproductive health issues. In addition, they should always be compassionate and respectful of their patients.
Finally, self-management of dysmenorrhea symptoms by home remedies and painkillers was found to be another main reason for not visiting healthcare in this study. Participants use hot drinks, and coca, apply hot water on the abdomen, and wear additional clothes are among those remedies. This is in line with the study conducted in Nigeria and Ethiopia, which says most respondents, used non-pharmacological therapy like sleep, hot water bottles, and exercise.14,15 In addition, our participants also used over the counter drugs such as ibuprofen, diclofenac, and meloxicam at home to treat their pain during menstruation. This finding is consistent with other studies in Spain and Ethiopia, which reported non-steroidal anti-inflammatory drugs (NSAIDs) use is the “self-medication” practice that is most frequently used and Lebanon, which reported mefenamic acid, ibuprofen, paracetamol, ketoprofen, and diclofenac were the most common medications used by females with dysmenorrhea.16,27 Even though one of the suggested treatments for women with dysmenorrhea is the use of NSAIDs, it is best to consult with medical professionals to determine the right dosage and method of therapy.
This study explores the reasons why women with dysmenorrhea do not seek healthcare, making a significant contribution to the maternal and reproductive health literature. However, it has limitations, such as focusing only on the perspectives of women with dysmenorrhea and not considering the views of healthcare workers who provide care and treatment. The snowball sampling technique, which relies on referrals from existing participants, could introduce selection bias and limit the representativeness and generalizability of the findings. Future research should consider more representative and random sampling methods and incorporate the views of healthcare workers and women with dysmenorrhea to better understand the reasons behind this lack of healthcare.
Conclusion
This study explored the reasons for not seeking healthcare among students with dysmenorrhea. The study found that the main reasons were socio-cultural and personal factors, prior negative experiences and perceptions towards the healthcare system and providers, and preference for self-management of symptoms. The study revealed the need for more awareness, education, and quality healthcare services for women with dysmenorrhea in Ethiopia. The study also suggested future research directions to explore the perspectives of other stakeholders and evaluate the effectiveness of different interventions. The study contributed to the existing literature on dysmenorrhea by providing insights into the socio-cultural and personal factors that influence health-seeking behavior among women with this condition in Ethiopia.
Abbreviations
AAU, Addis Ababa University; BMI, Body Mass Index; CHS, College of Health Sciences; DC, Data Collector; DU, Dilla University; HSB, Health Seeking Behavior; IRB, Institutional Review Board; PD, Primary Dysmenorrhea.
Data Sharing Statement
The data that supports this study is not publicly available due to ethical and privacy concerns. However, the first author and corresponding author will share the data upon reasonable request. The data include anonymized demographic and clinical data of the participants and questionnaires. The data will be accessible for 10 years after the publication of this paper. To request data access, please contact the first and corresponding author Senait Belay Getahun: [email protected].
Ethics Approval and Consent to Participate
This study followed the Declaration of Helsinki and considered the potential benefits for the participants. It involved some ethical and methodological challenges related to studying reasons for not seeking healthcare among students with dysmenorrhea. Therefore, Addis Ababa University College of Health Sciences Institutional Review Board (IRB) approved (with protocol number of SNM/MID/032/15) this study ethically, and permission was obtained from Dilla University to conduct the study. The study communicated its aims, rationale, and expected outcomes to the concerned departments for their cooperation. Each participant gave written informed consent after receiving information about the purpose, procedures, benefits, risks, confidentiality, voluntariness, and the right to withdraw from the study at any time without any consequences. The study assured anonymity and confidentiality for each participant and kept the data securely in a password-protected computer accessible only by the researchers. The principal investigator also provided health education for participants with dysmenorrhea on various aspects of their condition, such as types, causes, treatment options, self-care practices, and when to seek healthcare. Moreover, we obtained written informed consent from the study participants for publication of the anonymized results.
Acknowledgments
We would like to thank Addis Ababa University College of Health Science, School of Nursing and Midwifery for allowing us to conduct this thesis and advance our academic aspirations. Our heartfelt gratitude goes to our respected advisors Semarya Berhe and Bazie Mekonen for their excellent guidance, feedback, and support during the entire process of choosing and developing this thesis topic. We also appreciate the cooperation and help of Dilla University zero-plan coordinators who helped the successful completion of this thesis. Lastly, We are grateful to our study participants for their valuable responses and
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received funding from Addis Ababa University Research and Dissemination Office. The sponsor participated in the study conception, design, data collection and interpretation, and gave permission for publication.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Heise L, Greene ME, Opper N, et al. Gender inequality and restrictive gender norms: framing the challenges to health. The Lancet. 2019;393(10189):2440–2454. doi:10.1016/S0140-6736(19)30652-X
2. Langer A, Fleck F. The new women’s health agenda. Bull World Health Organ. 2013;91(9):628–629. doi:10.2471/blt.13.030913
3. Lobo RA, Gershenson DM, Lentz GM, Valea FA. Comprehensive Gynecology. Elsevier; 2016.
4. Chen CX, Shieh C, Draucker CB, Carpenter JS. Reasons women do not seek health care for dysmenorrhea. J Clin Nurs. 2018;27(1–2):e301–e8. doi:10.1111/jocn.13946
5. Armour M, Hyman MS, Al-Dabbas M, et al. Menstrual health literacy and management strategies in young women in Australia: a national online survey of young women aged 13–25 years. J Pediatr Adolesc Gynecol. 2021;34(2):135–143. doi:10.1016/j.jpag.2020.11.007
6. Thakur P, Pathania AR. Relief of dysmenorrhea: a review of different types of pharmacological & non-pharmacological treatments. Mater Today. 2022;48:1157–1162. doi:10.1016/j.matpr.2021.08.207
7. Tadese M, Kassa A, Muluneh AA, Altaye G. Prevalence of dysmenorrhoea, associated risk factors and its relationship with academic performance among graduating female university students in Ethiopia: a cross-sectional study. BMJ open. 2021;11(3):e043814. doi:10.1136/bmjopen-2020-043814
8. Mendiratta V, Lentz G. Primary and secondary dysmenorrhea, premenstrual syndrome, and premenstrual dysphoric disorder. In: Comprehensive Gynecology
9. Molla A, Duko B, Girma B, et al. Prevalence of dysmenorrhea and associated factors among students in Ethiopia: a systematic review and meta-analysis. Women’s Health. 2022;18:17455057221079443. doi:10.1177/17455057221079443
10. Iacovides S, Avidon I, Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. 2015;21(6):762–778. doi:10.1093/humupd/dmv039
11. Wang L, Yan Y, Qiu H, et al. Prevalence & risk factors of primary dysmenorrhea in students: a meta-analysis. Value in Health. 2022;25(10):1678–1684. doi:10.1016/j.jval.2022.03.023
12. Allyn K, Evans S, Seidman LC, Payne LA. “Tomorrow, I’ll be fine”: impacts and coping mechanisms in adolescents and young adults with primary dysmenorrhoea. J Adv Nurs. 2020;76(10):2637–2647. doi:10.1111/jan.14460
13. Hailemeskel S, Demissie A, Assefa N. Primary dysmenorrhea magnitude, associated risk factors, and its effect on academic performance: evidence from female university students in Ethiopia. Int J Women’s Health. 2016:489–496. doi:10.2147/IJWH.S112768
14. Oluwole EO, Agha OO, Ogunyemi A, Bakare OQ. Perception and Healthcare seeking practices regarding dysmenorrhea among public secondary school students in Lagos, Nigeria: prevalence and healthcare seeking practice of dysmenorrhea among secondary school adolescents. Babcock Univ Med J. 2020;3(2):34–44. doi:10.38029/bumj.v3i2.46
15. Gebeyehu MB, Mekuria AB, Tefera YG, et al. Prevalence, impact, and management practice of dysmenorrhea among University of Gondar Students, Northwestern Ethiopia: a cross-sectional study. Int J Rep Med. 2017;2017:1–8. doi:10.1155/2017/3208276
16. Karout S, Soubra L, Rahme D, Karout L, Khojah HM, Itani R. Prevalence, risk factors, and management practices of primary dysmenorrhea among young females. BMC Women’s Health. 2021;21(1):1–14. doi:10.1186/s12905-021-01532-w
17. Campbell AJ. The prevalence and impact of dysmenorrhea in young women within the United States; 2019.
18. Yesuf TA, Eshete NA, Sisay EA. Dysmenorrhea among university health science students, northern Ethiopia: impact and associated factors. Int J Rep Med. 2018;2018:1–5. doi:10.1155/2018/9730328
19. Tesfaye TS, Alemu W, Mekonen T. Perceived clinical practice competency and associated factors among undergraduate students of medicine and health science collage in Dilla University, SNNPR, Ethiopia. Adv Med Edu Pratc. 2020;Volume 11:131–137. doi:10.2147/AMEP.S235823
20. Chen CX, Draucker CB, Carpenter JS. What women say about their dysmenorrhea: a qualitative thematic analysis. BMC Women’s Health. 2018;18(1):1–8. doi:10.1186/s12905-018-0538-8
21. Abreu-Sánchez A, Parra-Fernández ML, Onieva-Zafra MD, Fernández-Martínez E. Perception of menstrual normality and abnormality in Spanish female nursing students. Int J Environ Res Public Health. 2020;17(17):6432. doi:10.3390/ijerph17176432
22. Ní Chéileachair F, McGuire BE, Durand H. Coping with dysmenorrhea: a qualitative analysis of period pain management among students who menstruate. BMC Women’s Health. 2022;22(1):407. doi:10.1186/s12905-022-01988-4
23. Hennegan J, Shannon AK, Rubli J, Schwab KJ, Melendez-Torres G. Women’s and girls’ experiences of menstruation in low-and middle-income countries: a systematic review and qualitative metasynthesis. PLoS Med. 2019;16(5):e1002803. doi:10.1371/journal.pmed.1002803
24. Begashaw B, Tessema F, Gesesew HA. Health care seeking behavior in Southwest Ethiopia. PLoS One. 2016;11(9):e0161014. doi:10.1371/journal.pone.0161014
25. Bhattarai K, Karkee R, Ghimire A, et al. A qualitative study to explore adolescent girls belief on menstruation and health seeking behavior. Biomed Sci. 2020;6(2):31. doi:10.11648/j.bs.20200602.13
26. Chan S, Yiu KW, Yuen PM, Sahota DS, Chung T. Menstrual problems and health-seeking behaviour in Hong Kong Chinese girls. Hong Kong Med J. 2009;15(1):18–23.
27. Ramos-Pichardo JD, Ortega-Galán ÁM, Iglesias-López MT, Abreu-Sánchez A, Fernández-Martínez E. Why do some Spanish nursing students with menstrual pain fail to consult healthcare professionals? Int J Environ Res Public Health. 2020;17(21):8173. doi:10.3390/ijerph17218173
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.