Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Realities of Using Drones to Transport Laboratory Samples: Insights from Attended Routes in a Mixed-Methods Study
Authors Comtet HE ![]() , Keitsch M, Johannessen KA
, Keitsch M, Johannessen KA
Received 7 May 2022
Accepted for publication 17 August 2022
Published 31 August 2022 Volume 2022:15 Pages 1871—1885
DOI https://doi.org/10.2147/JMDH.S371957
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hans E Comtet,1,2 Martina Keitsch,2 Karl-Arne Johannessen1,3
1The Intervention Centre, Oslo University Hospital, Oslo, 0424, Norway; 2Department of Design, Norwegian University of Science and Technology (NTNU), Trondheim, 7491, Norway; 3Department of Health Management and Health Economics, Faculty of Medicine, University of Oslo, Oslo, 0318, Norway
Correspondence: Hans E Comtet, The Intervention Centre, Oslo University Hospital, Postboks 4950, Oslo, 0424, Norway, Email [email protected]
Purpose: Drones are an emerging technology with the potential to improve laboratory logistics. This study is based on the hypothesis that the implementation of drones will benefit from an understanding of the current system and that existing transport solutions should be optimized before drone solutions are considered. It focuses on carriers transporting biological material today by car along a traditional circular route. It aims to explore how the current transport service is organized, identify areas for improvement, and investigate carriers’ perceptions of how drones could be integrated into or substituted for their services.
Methods: A mixed-methods approach was applied, combining a questionnaire, shadowing of nine transport trips, semi-structured interviews, and time assessments.
Results: The carriers shared insights into how to optimize existing transport solutions in terms of structure, culture, attitudes, and overall functionality. Most carriers expressed in the questionnaire that they were little involved in innovation work. The time assessment revealed that not the driving times, but the loading times had the highest deviations from plans and thus represented the area with the greatest potential for simple improvements. Questions about the use and organizational impact of drones are generated, and their prospects are discussed from a broad sociotechnical perspective.
Conclusion: Our concept was to broaden our understanding of implementing drones into existing systems in a fairly simple setting. Although improved logistics may take place without complex processes, future research opportunities such as the impact of drones on organizational processes and social dynamics in the adoption of drones may be needed if more complex systems are involved. The paper proposes experimenting with, and learning from, transport with “road vehicles” and drones in combination and suggests that improvements should be made to existing transport solutions before drones are implemented.
Keywords: logistics, transportation of laboratory samples, reconfiguration, sociotechnical systems, participation
Introduction
The healthcare sector is influenced by an increasing stream of new technological solutions that aim to improve medical treatment and care offerings.1,2 These new technologies promise a variety of possibilities for healthcare but also come with certain technical, functional, and operational challenges.
Such emerging technologies may be enthusiastically welcomed by health professionals. Doctors are eagerly implementing new robots for microsurgeries,3 radiologists embrace the use of new and improved in-hospital three-dimensional printing,4 and surgeons implement new features and functionalities in mixed-reality applications.5
One area that has a long history of applying automation and technical solutions is clinical laboratories. There are developments in point-of-care analyses (POC) that may revolutionize the sector, both by simplifying hospital analyses and providing access to important analyses in a home care setting for patient follow-ups. An emerging technology that, it has been suggested, could disrupt laboratory services is unmanned aerial vehicles (UAVs, drones).6–9 Oslo University Hospital plans to construct new hospital buildings by 2030, and considers the use of drones an element of its future transport logistics.10,11 Although the realistic potential and value of drone transport remain unknown, it is well established that both infrastructure for landing and take-off, drone surveillance as well as structures for loading will be needed for efficient and robust drone transport. Few studies have reported on the potential of drone transport to influence hospital logistics from an extended perspective.
The value of the drone services offered by companies such as Zipline12 and other providers in Africa, where drone transport may provide services to remote and hard-to-reach areas, is easy to appreciate.13 Even with open roads, delivery by drone transport may be faster and cheaper than ground transport in these areas. Although drone technology is developing quickly, drones will show their full potential only when they are able to fly beyond the line of sight (BVLOS)14 and fully autonomously for long distances. Nentwich et al15 predicted that autonomous drones would need to be programmed to reach their targets, to have self-reliant route planning, and to be self-sufficient in averting obstacles. A combination of different technologies may be necessary to reach this level of automation.16 Although Mion17 reported in a Swiss case study that the implementation of drones had only minor effects on organizational processes, he also argued that a broader perspective should be taken when integrating drones.
A widespread adoption of telehealth solutions18 or the acceptance of machine learning applications for clinical laboratories19 may require taking a broader sociotechnical perspective to fully understand how these technologies can be integrated into existing health care systems. However, whether traditional and existing clinical processes, logistics, and patient care can be adapted to drone solutions taking a similar approach, and if and how drones contribute to sustainable healthcare systems, is currently not completely understood.20,21
New solutions and approaches may challenge the status quo, namely, established work processes and routines. Existing systems may survive for long periods if they are locked in by traditional ways of operation. In an early phase, new technologies may develop without consensus being reached on their overall benefits if, for example, it is challenging to comprehend how the new tool can be integrated into existing workflows in a way that takes advantage of the technology to improve existing processes.
Awad et al22 and Bongomin et al23 illustrate a future vision of a connected healthcare system, and in their scenarios, drones may play an important role. Although it is not obvious that the future scenarios they sketch out will take place, the combination of multiple future technologies will certainly generate new solutions that we were not able to foresee only a few years ago. In Norway, political guidelines for future patient treatment aim to increase the use of digital patient contacts, enabling digital home treatment for 30% of patients by 2030.24 This ambition was sparked after the boost of such patient contact during the COVID-19 pandemic. Whether the extensive transitions visioned by Awad et al and Bongomin et al may be enabled by single technologies or will need transformational changes in multiple technologies and between multiple actors,25–27 remains to be seen. Focusing on the interplay of multiple singular disruptions, with greater attention paid to complete concepts, may be helpful in observing add-ons that may trigger further innovations.24,27
One approach that has demonstrated its usefulness in approaches to extensive transformations is the multi-level perspective (MLP). This may be considered a part of transition studies that is useful for providing a holistic perspective on system changes, as the MLP takes into consideration both the involvement of different actors and multiple interactions in a system and dynamic alteration at different systemic levels.
According to Geels, a restricted focus on innovations often ignores in-depth interests in system innovation.26 In comparison, system innovation has a broader analytical view that may include aligning with more overall ongoing processes or multiple innovations. Together and over time, these innovations may lead to system innovations. This study aims to mitigate this gap by focusing on drones and a reconfiguration pathway of system innovation.
Sociotechnical approaches emphasize understanding the work practices in which technology will be used.28 Following this argument, this article focuses on the carriers at OUS today who transport biological material by “road vehicles” along a traditional circular route.
The hospital transport services’ carriers are employees who should be considered potential stakeholders and resources in implementing drone solutions. Automated transport of drones may influence the carriers’ future job positions, and they may represent knowledge of how new solutions should be designed if drones are to be implemented as hybrid solutions that combine existing practices with a new transport modality.
This study is based on the hypothesis that the implementation of drones will benefit from an understanding of the current system, and that existing transport solutions should be examined and possibly optimized before drone solutions are considered.
Our research ambitions are as follows:
- To explore how the current transport service is organized and identify areas for potential improvement; and
- To study what the carriers perceive as important factors related to how drones could be integrated into or substituted for their service offerings.
Background
Institutions
Oslo University Hospital (OUS) comprises four hospitals located within Oslo: The National Hospital (providing local, regional, and national services), Ulleval Hospital (providing local, regional, and national services), Radium Hospital (a specialized cancer hospital), and Aker Hospital (a local and central hospital). The current ground transport provides transport of both biological test samples, blood, and other items across differing locations.
Route Organization
Figure 1 shows a map of the institutions. The routes today are mostly organized in a circular design with multi-stop routings except for some on-to-one trips. The different lines indicate the distance between the locations, together with the number of trips.
 |
Figure 1 The National Hospital, Ulleval Hospital, Radium Hospital, Aker Hospital, and the Blood Bank in the Red Cross house. |
Four routes from the National Hospital to Radium Hospital are served by a bus today that transports patients but also carries payloads of various types. This part of the OUS transport service was not considered in our study.
The article proceeds as follows. The following section introduces the MLP framework and reconfiguration pathways. The next section describes the methods, followed by presenting the results and a discussion. Then, continuing with the limitations of our study, we conclude with our findings.
Is a Reconfiguration Approach Relevant for Drone Implementation?
This paper assumes that drone solutions are initiated by innovators and technologically oriented enthusiasts at the clinical level and that their initiatives will influence the institutional levels of clinics, departments, and institutions. This process may create upstream driving forces in the institution, which in turn may create pressure from above to regulate, adapt, and form the potential implementations and consequences of the innovation. Such processes parallel the hypothesis and sociotechnical approach of the MLP and transition management theory.29–32
The potential value of a reconfiguration pathway, as depicted in the MLP, is generated by the method’s hypothesis that transitions are not caused by the breakthrough of one technology but by a combination of multiple component innovations.33 These new components are initially developed in what MLP denotes as “niches”, which are equivalent to the clinical units in our system. In the system discussed in this paper, the MLP approach would identify clinics as a protected space for radical innovations that need protection because of their strict regulations regarding medical soundness and documentation.34 Different forms of subsidies may provide protection. Simultaneously, the more a technology is developed and used, the more is learned about it, and the more it improves.35 Clinics are also the level that provides space for experimentation and learning processes. Thus, they may also be significant arenas for building socio-technological networks to develop organizational cultures that support innovation.36
This requires adequate adoption of the innovations at the clinical department level to solve the challenges caused by unfamiliar innovations at the institutional level, namely, the hospital (equivalent to the regime level in the MLP system).33,37 To obtain a gradual implementation of innovations at the healthcare level (parallel to the MLP landscape level), deeper structural trends must be triggered to create opportunities and pressure for further change. The expectations and ambitions of political guidelines are examples of such structural trends.
Multiple technologies, including drones, are being continuously developed in combination with each other. Many stepwise changes may add up to reconfigurations that, over time, may create major system changes. Figure 2 illustrates the reconfiguration pathway.
 |
Figure 2 The reconfiguration pathway of the MLP theory translated into a healthcare concept, adapted from Geels FW, Schot J. Typology of sociotechnical transition pathways. Res Policy. 2007;36(3):399–417 Copyright 2007, with permission from Elsevier.55 |
Methods
A mixed-methods approach was applied, combining a questionnaire, shadowing of nine transport trips, semi-structured interviews, and time assessments with carriers from the transport department.
The findings in this article are based on 16 questionnaires, 9 reports from shadowing, 8 interviews, and multiple time measures from the transports. By combining both quantitative and qualitative data, the objective was to picture the current services and the carrier’s work.38,39 Self-administered questionnaires were given directly to the participants.
Ethical Considerations
The study was approved by the hospital’s Institutional Review Board and complied with required ethical and legal standards relating to participant anonymity and confidentiality. The data material does not contain any identifying characteristics. Furthermore, data aggregation is only on group-level information. Participation in the survey and interviews was voluntary. All interviewees gave informed consent orally. The actual participation, and the information provided to the participants, imply consent based on conclusive behavior. As the study is conducted anonymously, it is outside the Regional Committees for Medical and Health Research Ethics (REK) mandate. Therefore, ethical approval from REK was not considered necessary.
Attended Routes for Observation
Three internal routes were attended three times. Information about arrival and departure times, stops, delays, and disturbances, as well as a general assessment of the transport flow, was gathered by interviewing the driver as well as measuring actual time intervals during the trips.
To ensure that identical questions were presented to all drivers, an interview guide was used to funnel the conversation with the carriers into the questions while accompanying them.
We asked about their opinions of (1) their workday, (2) factors that influence time, (3) changes in routes, (4) barriers and opportunities regarding their work, and (5) their thoughts about the future.
Questionnaire
A self-administered questionnaire containing 36 structured questions was distributed amongst the carriers in the transport department to understand the transport department better. Subsequently, participants were selected using purposive sampling,40 with the main interest of exploring the range of opinions.41 As a result, we received a total of 16 responses.
Transport Department, Routes, and Work Process
The transportation department at OUS is organized as part of the OUS Hospital Service Division (OSS). The transportation department is located at Ulleval Hospital, from where carriers drive across the different institutions. The transport department has 20 carriers who operate different routes using “road vehicles”, covering the transport of various biological materials, supplies, clothes, and food. The carpool ranges from normal-sized delivery vans used the most (eg, Renault Kangoo) to trucks (eg, Mercedes 3.5 ton).
The routes cover both internal and external clients. Our study focuses on the internal routes between the National Hospital, Ulleval University Hospital, Radium Hospital, and Aker Hospital.
The carriers are based at Ulleval Hospital, where they start their daily routes for trips across the institutions. The loading is done manually by the carriers, who do both the pick-up and delivery at the different laboratories. The pick-up is organized differently in different locations, and the payload is also stored differently. As we followed the routes, we observed that three major factors influenced the transport time; delays in the traffic, delays when the cars had to wait at the loading site, causing varying and prolonged loading times, and the transfer of delays for the next trip. This sparked the hypothesis that the multi-stop routing with layovers was not always efficient. Furthermore, such multiple routings would not be relevant for future drone services because such serial transports would include legs with multiple drone takeoffs and landings, consuming significant energy for hovering and transport times.14 We, therefore, intended to consider direct routings, ie, round trip tours between two locations. We measured all time intervals during the shadowing of the tours and also interviewed the drivers about the delays as they occurred. Based on the time measurements, we could experiment with different alternative direct routings, always ensuring that current transport routings were covered to the same extent as in existing routings. Time assessments were analyzed by a simple model using Microsoft EXCEL 2016. Mean, maximum and minimum driving and loading times were calculated.
The current transport system involves a daily driving distance of approximately 290 km. We followed each route three times on weekdays from Monday to Thursday in June 2021. Table 1 below illustrate the current work processes.
 |
Table 1 Route Description |
Analysis
The analyses followed a convergent design, in which the quantitative and qualitative data were analyzed separately and then merged to combine the results.40 This design allowed us to link different findings and gain a complete understanding of the transport system.
The interviews were noted, transcribed, and entered into Atlas.ti (www.atlasti.com), which is a qualitative data analysis software package. However, Atlas.ti was not used to analyze the data but primarily to organize the data.
The transcripts were analyzed, and the data was structured into relevant categories.42,43 The categories emerged from the review and were selected for their relevance to drones.
The round-trip transport times across the locations were assessed, except for the Ulleval–Aker route, which did not have a return trip but was a one-way transport. The measured time intervals in the current routes include driving times (the time from departure from one location to arrive at the next location) and loading times (assessed as the time from arrival to departure for the next leg in the route). The loading time thus includes both the waiting time and the time for delivering/collecting the payloads at each stop. These time intervals were used to assess total transport times in the existing trips across the different locations and to estimate theoretically optimized transport times based on minimal time intervals.
Results
Observations
Six categories emerged from the review of the transcripts, together with the findings and consequences (Table 2).
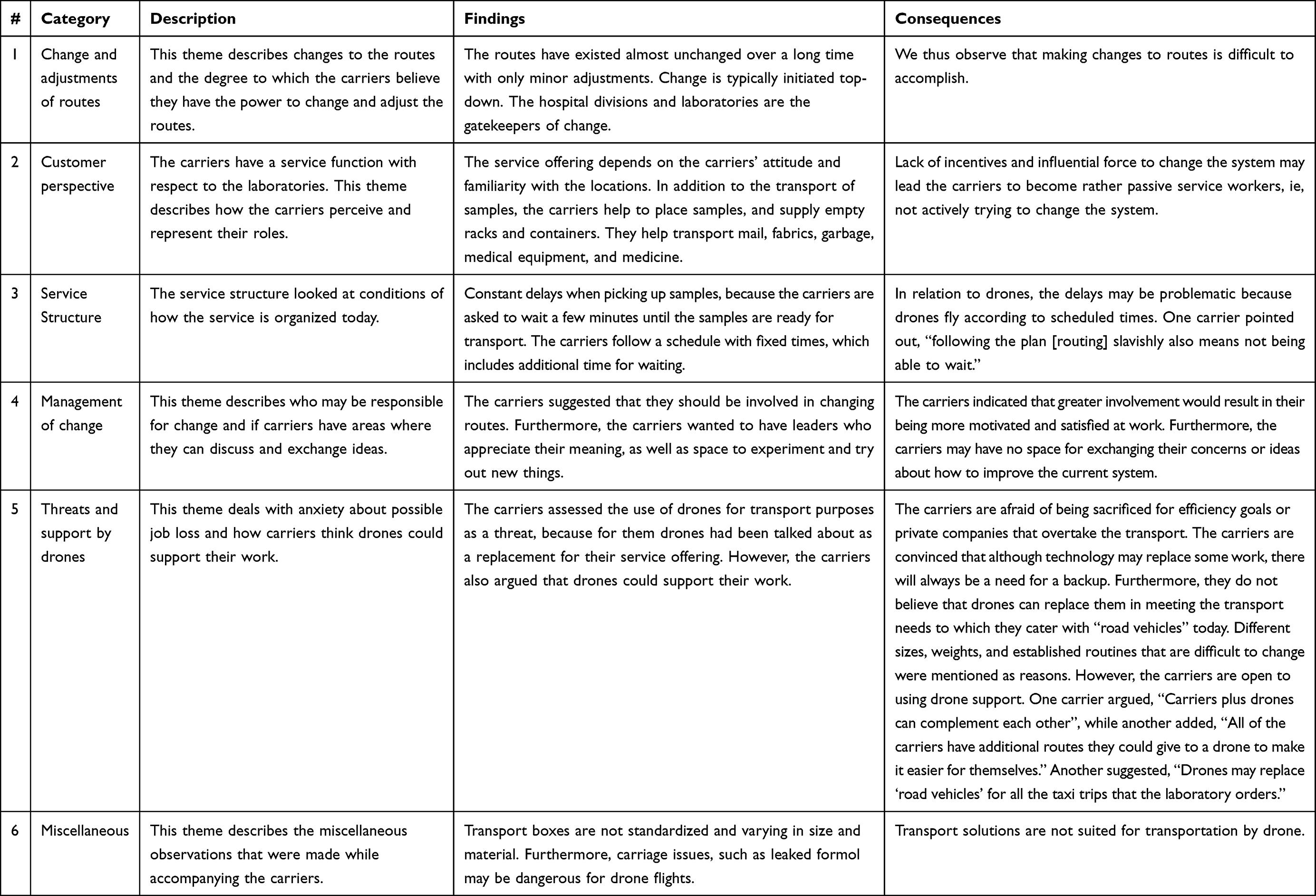 |
Table 2 Categories That Emerged from the Transcripts |
Questionnaire
Sample Characteristics
The mean age of the 16 participants was 48.34 years (SD 2.88). The mean number of years worked at OUS was 11.75 years (SD 3.18).
A summary of the most relevant questions in the questionnaire is presented below in Table 3.
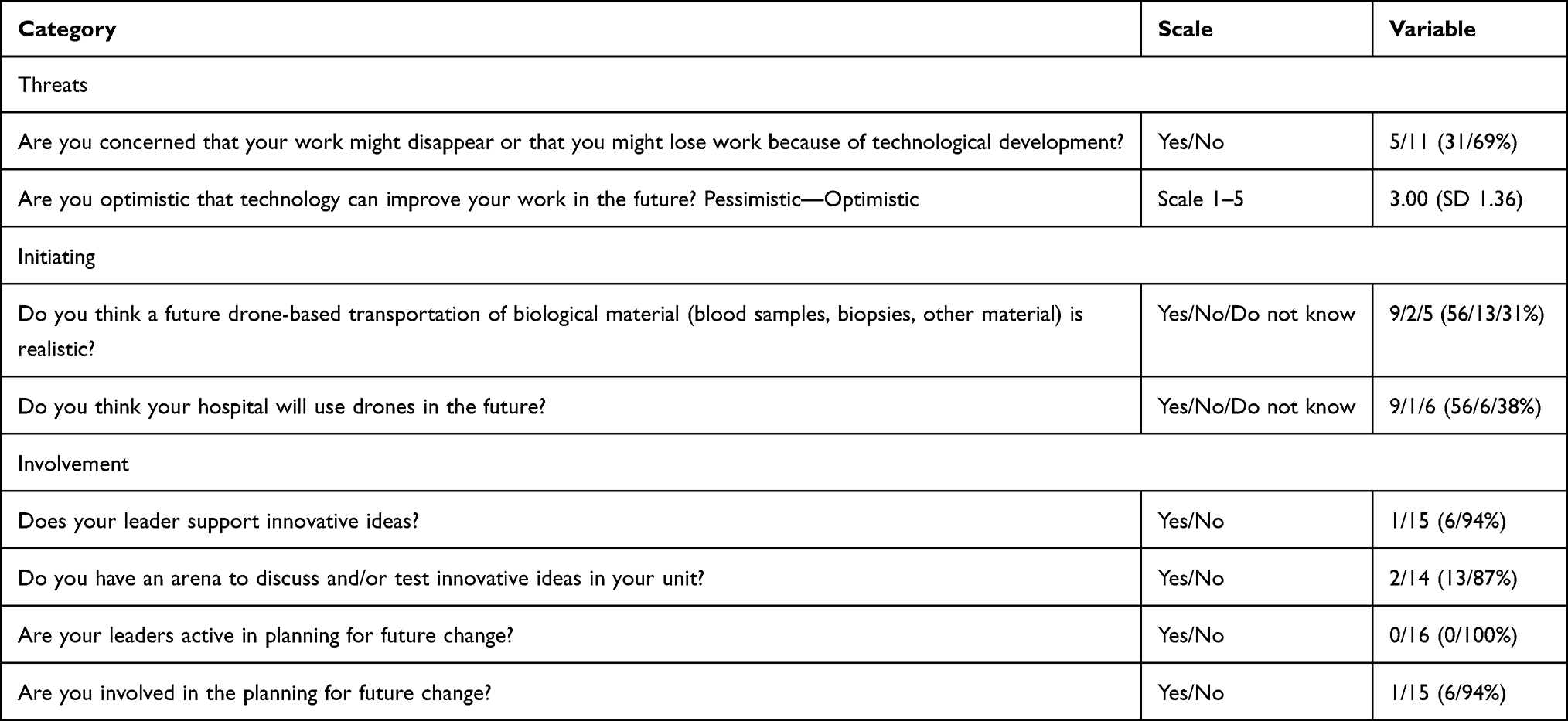 |
Table 3 Summary of the Most Relevant Questions in the Questionnaire |
Time Measures of the Routings
The routes that we joined were driven daily between 07:30 and 16:30. Table 4 shows the mean, maximum, and minimum driving times and loading times and the estimated total transport times. In the multi-leg routings, the loading times are the sum of all loading times at each site.
 |
Table 4 Driving, Loading, and Optimized Times |
Table 4 shows that the loading time represented 33–64% of the total transport times, and the high loading times were often caused by one delay at one of the stations. In our assessments for improvements of the transport routings, we used the mean driving time in direct routes and the shortest loading time, assuming that the latter represented a realistic improvement if better logistics are implemented.
Times from the current and suggested new routings are compared in the upper part of Table 5, the direct routings in the lower part. The most profound gain was observed by transforming the multi-leg routing to direct routings. This is illustrated in Figure 3 for the two most complex routings; the Ulleval-Aker transport with four legs and the Radium-Aker with three legs.
 |
Table 5 Current and Direct Route |
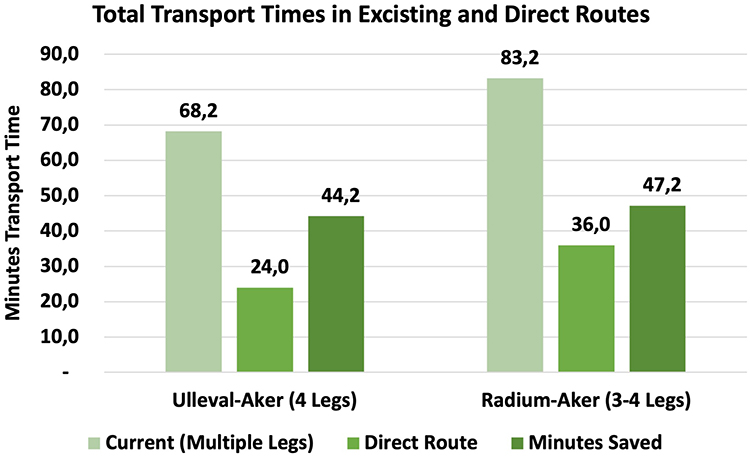 |
Figure 3 Total transport times in existing and direct routes. |
A simple illustration is shown in Figure 3.
Using such modifications to the existing routings, it was theoretically possible to use one less car compared with the current system.
As a summary of our findings, we observed that the carriers had substantial knowledge of how the current transports could be improved, they were interested in how new solutions should be developed, and not least, the timelines of the current ground transport could be substantially improved by simple changes.
Discussion
This study examined basic topics related to logistics, service levels, and personnel involved in an existing ground transport system that it has been suggested could be substituted for by drone transport. Our findings showed that insights from the carriers who perform the current ground transport contributed knowledge helpful in optimizing the existing transport solution concerning the overall functionality. More general, our generated insights on structure, culture, and attitudes may be relevant to obtaining a more innovative transport system. This, in turn, provides information about how drones should be implemented, either as a substitution for or as an integrated part of current ground transport.
The carriers had a somewhat passive attitude toward the system performance, which seemed to be associated with their perception that they had little influence on how the existing system is developed and improved. The current solutions have mostly remained unchanged for 20 years, although the carriers stated that they had presented several ideas for improvement. Their impression was that although the external framework for transport had changed in many ways over the period, their proposals for improvements for example HUBs were rarely discussed. The carriers said that they were open-minded regarding involvement in solving problems and improving quality, but that they perceived the institution as having a deficit in open-minded management.
From our interviews, we concluded that the carriers have suggestions regarding how to reduce transport times and improve regularity and how drone transport should be integrated with current solutions in the future. They are motivated to contribute to the implementation of drone services with a positive attitude, but their expectations of being involved are low because they feel that their workplace does not involve in the innovative processes. Although this perception was strong among the carriers, we suspect that this is not representing the actual state of the department and assume that the carriers’ statements that none of the leaders are active in planning for future change are considerably biased. Furthermore, the fact that only 31% of the carriers had some worries about their future jobs if drones were implemented is not equivocally telling they are scarcely involved in system development and organization. Nevertheless, we conclude that involvement should be considered because carriers do more than just transport goods; they also significantly influence how this transport works concerning how their customers are acting and the service quality perception of the customers.
We observe that the current ground transport system is not primarily focused on transport times, but rather on maintaining flexibility for the laboratories that are their customers. If the laboratories ask for the transport to wait and postpone a given departure, this is accommodated, despite that this will cause a delay. This flexibility may be part of the explanation for some of the long loading times that we observed. Whereas such flexibility may seem valuable for the actual site requesting elasticity of the transport at an actual time, there is scarce knowledge of whether this reduces the total service when all transport legs are considered as a whole.
This was also reported by the carriers. They had multiple examples of how the flexible departures were often caused by insufficient planning and processes in the laboratories to prepare for the pick-up. This indicates that, whereas the routings are organized as regular trips, the laboratories may act as if the transports are tailored to the laboratories’ insufficient preparations. Accordingly, a consequence of their efforts to satisfy their customers is that there are often delays, with consequences for subsequent trips.
We, therefore, conclude that the current transport system is not considered time-critical; that is, the total transport times are not being monitored or processed for standardization or optimization. This, in turn, sparks the question of whether the “timely” demand of the current transport system makes it a good candidate for drone solutions. With the short distances between transport sites, the time savings from drones will be limited. The optimized times in Table 5 show an improvement of 17–38%, calculated in minutes saved; this indicates an improvement between 5.4 and 16.3 minutes. It may be argued that any minutes saved by a drone carrying a cardiac defibrillator could save a life. However, it may be doubted that this is equally crucial to transporting routine blood samples. Some minutes saved may have marginal clinical significance in specific healthcare systems where patients may wait for months for their first contact with healthcare provisions.14 Furthermore, to what extent faster transport will influence the efficiency of healthcare to any significant degree may be an open research question.
If the variations in the transport times and loading times that we observed are acceptable, this may indicate a limited willingness to pay for drone solutions. The potential competitiveness of drones will therefore be related to whether they have lower costs than the current ground transport system for comparable service times or result in real-time savings.
If large cities have frequent future drone trips and routings for multiple sectors and with many operators, drone transport should be expected to be strictly regulated by time slots and trajectories of unmanned BVLOS flights. This may, in turn, demand strict and timely routings with minimal deviations, and the “flexible departures” in the current ground transport system at OUS may violate such regulatory criteria. This may have a significant impact on how drone solutions are organized in urban locations.
The potential of drones to avoid ground traffic congestion has also been used as an argument for the time savings achieved by drone implementations.13,44–47 Furthermore, in this context, stricter organization of the routings may be needed. In our system, it was the loading times and not the driving times that caused the highest deviations from plans and may thus represent the area with the greatest need for improvement. The minimum loading times as benchmark times promise considerable potential for time savings. However, whether such improvements, with only minutes, gained per leg, have any clinical value at all remains to be evaluated.
Theoretically, building a revised model with optimized transport times could change the existing route organization. The optimized total transport times show that hourly routings may be a realistic alternative to the current model and that one round-trip leg with one car could handle transport needs with shorter transport times than the existing ones. In our theoretical redesign, one car and carrier could be made redundant, thereby having some gains. Such improvements should be implemented before comparison between drone and ground transport is performed. However, our theoretical model would demand strict loading and departure times; otherwise, substantial delays may occur. The value of strictly regular departures is that missing a specific departure, and thus waiting for the next one, will cause minimal delays.
Will Drone Implementation Need Specific Organizational Processes for Implementation?
The current transport routes are not complex, and they are not focused primarily on transport times. Improvements should be realistic either with or without drones. Drones may therefore represent a logistical solution with relatively little impact on organizational processes and may have little effect on other clinical services apart from the transportation service. This suggests that the implementation of drones may be rather uncomplicated concerning the pure transport topic. Therefore, we conclude that the institutionalization of drones, ie, the process of innovation,48 may be achieved without many complex processes. This is in accordance with our findings, as only five of 16 carriers expressed concern in the questionnaire.
Our study showed that the current system focuses on flexibility, but although the current solution has not been changed extensively in the last 20 years, there should be a regular assessment of which topics are the most valuable for the laboratories.
An alternative to a simplistic approach to drone implementations in simple models like ours, is the hypothesis that in more complex systems, such solutions should be considered from a broader organizational perspective. The combination of micro-behaviors as individuals adopt an innovation, ongoing regime developments and landscape pressures may, over time, result in more significant system changes. One perspective could be that the transport department rebrands itself as an innovation hub for logistics with an open culture for experiments and change. As a carrier put it, “The old structure needs to be cracked to be more innovative.”
The theory, however, is that socio-technologic transitions require the interplay of technological and social processes that reinforce each other.25 In our setting, our insights into the technological process are scarce because drone technology solutions are developed externally and not from a hospital perspective. Diffusion across technology and medical processes related to drones may therefore be rather limited. Although drones may seem promising, there is no guarantee for drones to break through and disrupt laboratory transports.
Getting support from drones was discussed as a valuable add-on to the service offering of the transport department. According to the carriers, drones may be used for specific routes, ie, as a replacement for taxi trips that today are used for emergency analysis or outside of regular working hours. However, economic, or technological considerations may strongly influence whether this is realistic, and there are not many scientific data to enlighten this topic.
However, the carriers seemed to have the essential knowledge about logistics and the continuous transport of biological material and other goods and they believed that a combination of drones and the current system may be beneficial. Including them in the introduction of drones may support the acceptance of drones, a topic that has gained much interest in the literature.49–54
Limitations of the Study
The small volume of data in the current study may of course be observed as a significant limitation. Small volumes may both challenge the validity of scientific conclusions as well as the soundness for generalization across differing systems. However, our conclusions are not depending on complex scientific deductions but logical conclusions from simple observations and we intended to elaborate on possible ideas for simple approaches. We hypothesize that the generalizability of such findings across differing systems may depend more on systemic differences related to service need and structure, than on the specific findings in each setting.
Although Oslo University Hospital is a large hospital, compared to European standards, the distances between the various locations are short. Furthermore, traffic congestion is probably less than in many larger cities. Therefore, some of our findings may not apply to other locations. Large hospitals in other cities may have quite different structures and transport needs. Nevertheless, involving the workforce in providing transport solutions may reveal important insights.
Our finding that current ground transport could easily be improved is therefore specific to a rather plain model. The interviews were conducted at the OUS transport division and are ultimately not representative of other hospitals or transport departments. Furthermore, the existing ground system with “road vehicles” at Oslo University Hospital is not based on transport times but flexibility for the laboratories. Although these factors may limit the generalization of our actual findings, it may be of value for other transport departments and hospitals to conduct similar research to understand how carriers value drones. Their narratives provided insights and underscore the necessity of open-minded and innovative leadership to facilitate change and acceptance.
This study focused on topics related to current transport solutions and showed that a comparison of drones with optimized ground transport shows close competition. The argument about avoiding ground traffic congestion and the value of time efficiency has been put into perspective. Of course, if drone transport shall be implemented in future transport solutions, multiple infrastructures are needed such as landing sites and automatic solutions for loading and unloading, drone surveillance and drone maintenance. Unfortunately, the study of such topics is currently challenging to perform today because of the immaturity of such solutions. It should also be expected that various types of drones and drone sizes will be used for differing purposes, demanding differing solutions for the mentioned structures. No doubt, such perspectives will be necessary to define in future studies. Nevertheless, the advantages of drones in other settings may be more evident. For example, drone transports in rural districts and on-demand services in emergencies have proven valuable and may have more significant clinical value, resulting in greater willingness to pay, than short-distance transports.
Although a sociotechnical perspective with the MLP and transitions research has a powerful analytical force, transitions do happen without it. The purpose of our conceptualization was to broaden our understanding of how to implement drones into existing systems. We believe that several future research opportunities, such as the impact of drones on organizational processes and social dynamics in the adoption of drones, may extend the understanding of these questions and nudge transitions in the desired directions, and have significant relevance in more complex settings.
Conclusion
The carriers involved in this study had useful knowledge of how future drone solutions should be implemented and were positive about the use of drones as part of their future services. They showed that existing transport solutions should be analyzed carefully to realize possible improvements before drones are implemented. The lesson learned from their input is that drone implementations should be evaluated in context with current ground solutions, either as integrations into or partial substitutions for current services, and that involved personnel should be involved in developing such solutions.
We conclude that in straightforward transport systems such as the one we examined, improvements to current solutions may be obtained without complex processes. This may of course vary between different locations, service demands, and the complexity of the services. Whether an extended organizational perspective of drone implementations is needed in more complex settings needs further research. We also conclude that although improvements may be obtained by unsophisticated changes, the potential for added organizational and innovative processes should always be considered, in particular, if multiple new technologies are included.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We are grateful to the transport department at Ulleval Hospital for their cooperation and participation in this research project. Furthermore, we thank Ole Andreas Alsos from NTNU for helpful comments regarding the visualization and David Mulrooney, Ph.D., from Edanz for editing a draft of this manuscript.
Funding
The current work has been funded by the Norwegian Research Council under Grant 282207/2018.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ćwiklicki M, Duplaga M, Klich J. The digital transformation of healthcare: health 4. 0. Milton: Taylor & Francis Group; 2021.
2. Greaves RF, Bernardini S, Ferrari M, et al. Key questions about the future of laboratory medicine in the next decade of the 21st century: a report from the IFCC-Emerging technologies division. Clin Chim Acta. 2019;495:570–589. doi:10.1016/j.cca.2019.05.021
3. Arezzo A, Gagliardi G. Transanal endoscopic microsurgery: is robotics the way to go? Tech Coloproctol. 2021;25(11):1179–1182. doi:10.1007/s10151-021-02514-8
4. Mitsouras D, Liacouras PC, Wake N, Rybicki FJ. RadioGraphics update: medical 3D printing for the radiologist. Radiographics. 2020;40(4):E21–E23. doi:10.1148/rg.2020190217
5. Kumar RP, Pelanis E, Bugge R, et al. Use of mixed reality for surgery planning: assessment and development workflow. J Biomed Inform. 2020;112S:100077. doi:10.1016/j.yjbinx.2020.100077
6. Otto A, Agatz N, Campbell J, Golden B, Pesch E. Optimization approaches for civil applications of unmanned aerial vehicles (UAVs) or aerial drones: a survey. Networks. 2018;72(4):411–458. doi:10.1002/net.21818
7. Sanfridsson J, Sparrevik J, Hollenberg J, et al. Drone delivery of an automated external defibrillator - A mixed method simulation study of bystander experience. Scand J Trauma Resusc Emerg Med. 2019;27(1):40. doi:10.1186/s13049-019-0622-6
8. Wulfovich S, Rivas H, Matabuena P. Drones in Healthcare. In: Digital Health. Springer; 2018:159–168.
9. Scalea JR, Restaino S, Scassero M, Blankenship G, Bartlett ST, Wereley N. An Initial Investigation of Unmanned Aircraft Systems (UAS) and real-time organ status measurement for transporting human organs. IEEE J Transl Eng Health Med. 2018;6:4000107. doi:10.1109/JTEHM.2018.2875704
10. Johannessen K-A, Comtet H, Fosse E. A drone logistic model for transporting the complete analytic volume of a large-scale university laboratory. Int J Environ Res Public Health. 2021;18(9):4580. doi:10.3390/ijerph18094580
11. Services MoHaC. National health and hospital plan 2020–2023. The Norwegian Government; 2019. Available from: https://www.regjeringen.no/en/dokumenter/meld.-st.-7-20192020/id2678667/.
12. Ackerman E, Koziol M. The blood is here: zipline’s medical delivery drones are changing the game in Rwanda. IEEE Spectr. 2019;56(5):24–31. doi:10.1109/MSPEC.2019.8701196
13. Mateen FJ, Leung KHB, Vogel AC, Cisse AF, Chan TCY. A drone delivery network for antiepileptic drugs: a framework and modelling case study in a low-income country. Trans R Soc Trop Med Hyg. 2020;114(4):308–314. doi:10.1093/trstmh/trz131
14. Johannessen KA. A conceptual approach to time savings and cost competitiveness assessments for drone transport of biologic samples with unmanned aerial systems (Drones). Drones. 2022;6(3):62. doi:10.3390/drones6030062
15. Nentwich M, Hórvath DM Delivery drones from a technology assessment perspective. Overview report; 2018.
16. Ferreras LE. iTRANS: proactive ITS based on drone technology to solve urban transportation challenge. In: Meyer G, Shaheen S, editors. Disrupting Mobility. Cham: Springer International Publishing; 2017:323–333.
17. Mion FU Flying drones to exchange lab samples service innovation by the Swiss multisite hospital EOC. 2019.
18. Taylor J, Coates E, Wessels B, Mountain G, Hawley MS. Implementing solutions to improve and expand telehealth adoption: participatory action research in four community healthcare settings. BMC Health Serv Res. 2015;15(1):529. doi:10.1186/s12913-015-1195-3
19. De Bruyne S, Speeckaert MM, Van Biesen W, Delanghe JR. Recent evolutions of machine learning applications in clinical laboratory medicine. Crit Rev Clin Lab Sci. 2021;58(2):131–152. doi:10.1080/10408363.2020.1828811
20. Eichleay M, Evens E, Stankevitz K, Parker C. Using the unmanned aerial vehicle delivery decision tool to consider transporting medical supplies via drone. Glob Health Sci Pract. 2019;7(4):500–506. doi:10.9745/GHSP-D-19-00119
21. Barbero S, Pallaro A. Systemic design for sustainable healthcare. Design J. 2017;20(sup1):S2473–S2485. doi:10.1080/14606925.2017.1352762
22. Awad A, Trenfield SJ, Pollard TD, et al. Connected healthcare: improving patient care using digital health technologies. Adv Drug Deliv Rev. 2021;178:113958. doi:10.1016/j.addr.2021.113958
23. Bongomin O, Yemane A, Kembabazi B, et al. Industry 4.0 disruption and its neologisms in major industrial sectors: a state of the art. J Eng. 2020;2020:1–45. doi:10.1155/2020/8090521
24. Authority S-ENRH. Regional utviklingsplan 2035 [Regional development plan 2035 - New ways of working and better use of technology]. South-Eastern Norway Regional Health Authority; 2021.https://helse-sorost.no/regional-utviklingsplan-2035#nye-arbeidsformer-og-bedre-bruk-av-teknologi.
25. J-P V, Bauknecht D, Kemp R. Reflexive Governance for Sustainable Development. Cheltenham: Edward Elgar; 2006.
26. Geels FW. Disruption and low-carbon system transformation: progress and new challenges in socio-technical transitions research and the multi-level perspective. Energy Res Soc Sci. 2018;37:224–231. doi:10.1016/j.erss.2017.10.010
27. Geels FW, McMeekin A, Mylan J, Southerton D. A critical appraisal of sustainable consumption and production research: the reformist, revolutionary and reconfiguration positions. Glob Environ Change. 2015;34:1–12. doi:10.1016/j.gloenvcha.2015.04.013
28. Berg M. Patient care information systems and health care work: a sociotechnical approach. Int J Med Inform. 1999;55(2):87–101. doi:10.1016/S1386-5056(99)00011-8
29. Geels FW. Socio-technical transitions to sustainability: a review of criticisms and elaborations of the multi-level perspective. Curr Opin Environ Sustain. 2019;39:187–201. doi:10.1016/j.cosust.2019.06.009
30. Loorbach D, Schwanen T, Doody BJ, Arnfalk P, Langeland O, Farstad E. Transition governance for just, sustainable urban mobility: an experimental approach from Rotterdam, the Netherlands. J Urban Mobil. 2021;1:100009. doi:10.1016/j.urbmob.2021.100009
31. Whitmarsh L. How useful is the multi-level perspective for transport and sustainability research? J Transp Geogr. 2012;24:483–487. doi:10.1016/j.jtrangeo.2012.01.022
32. Geels FW. Technological Transitions and System Innovations: A Co-Evolutionary and Socio-Technical Analysis. Edward Elgar Publishing; 2005.
33. Geels FW. Major system change through stepwise reconfiguration: a multi-level analysis of the transformation of American factory production (1850–1930). Technol Soc. 2006;28(4):445–476. doi:10.1016/j.techsoc.2006.09.006
34. Leväsluoto J, Määttä H, Hyytinen K. Challenges of customer oriented health care service models: perspectives from the renewal of a primary health care and in; 2014.
35. Geels FW. From sectoral systems of innovation to socio-technical systems: insights about dynamics and change from sociology and institutional theory. Res Policy. 2004;33(6):897–920. doi:10.1016/j.respol.2004.01.015
36. Geels FW, Kemp R. Dynamics in socio-technical systems: typology of change processes and contrasting case studies. Technol Soc. 2007;29(4):441–455. doi:10.1016/j.techsoc.2007.08.009
37. Loorbach D, Frantzeskaki N, Avelino F. Sustainability transitions research: transforming science and practice for societal change. Annu Rev Environ Resour. 2017;42(1):599–626. doi:10.1146/annurev-environ-102014-021340
38. Greene JC, Caracelli VJ, Graham WF. Toward a conceptual framework for mixed-method evaluation designs. Educ Eval Policy Anal. 1989;11(3):255–274. doi:10.3102/01623737011003255
39. Andrew S, Halcomb EJ. Mixed Methods Research for Nursing and the Health Sciences. Chichester: Wiley-Blackwell; 2009.
40. Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research.
41. Gaskell G. dividual and Group Interviewing. In: Bauer MW, Gaskell G, editors. Qualitative Researching with Text, Image and Sound. London: SAGE Publications Ltd; 2000.
42. Dey I. Qualitative Data Analysis: A User-Friendly Guide for Social Scientists. London: Routledge; 1993.
43. Miles MB, Huberman AM, Saldaña J. Qualitative Data Analysis: A Methods Sourcebook.
44. Ling G, Draghic N. Aerial drones for blood delivery. Transfusion. 2019;59(S2):1608–1611. doi:10.1111/trf.15195
45. Hwang J, Lee JS, Kim H. Perceived innovativeness of drone food delivery services and its impacts on attitude and behavioral intentions: the moderating role of gender and age. Int J Hosp Manag. 2019;81:94–103. doi:10.1016/j.ijhm.2019.03.002
46. Park J, Kim S, Suh K. A Comparative analysis of the environmental benefits of drone-based delivery services in urban and rural areas. Sustainability. 2018;10(3):5.
47. Rejeb A, Rejeb K, Simske SJ, Treiblmaier H. Drones for supply chain management and logistics: a review and research agenda. Int J Logist Res Appl. 2021;1–24. doi:10.1080/13675567.2021.1981273
48. Vargo SL, Akaka MA, Wieland H. Rethinking the process of diffusion in innovation: a service-ecosystems and institutional perspective. J Bus Res. 2020;116:526–534. doi:10.1016/j.jbusres.2020.01.038
49. Tan LKL, Lim BC, Park G, Low KH, Yeo VCS. Public acceptance of drone applications in a highly urbanized environment. Technol Soc. 2021;64:101462. doi:10.1016/j.techsoc.2020.101462
50. Johnson AM, Cunningham CJ, Arnold E, Rosamond WD, Zegre-Hemsey JK. Impact of using drones in emergency medicine: what does the future hold? Open Access Emerg Med. 2021;13:487–498. doi:10.2147/OAEM.S247020
51. Komasová S. Possible inspiration: drone-related literature and its potential for public perception research. J Intell Robot Syst. 2021;103(3). doi:10.1007/s10846-021-01498-9
52. Smith A, Dickinson JE, Marsden G, Cherrett T, Oakey A, Grote M. Public acceptance of the use of drones for logistics: the state of play and moving towards more informed debate. Technol Soc. 2022;68:101883. doi:10.1016/j.techsoc.2022.101883
53. Comtet HE, Johannessen KA. The moderating role of pro-innovative leadership and gender as an enabler for future drone transports in healthcare systems. Int J Environ Res Public Health. 2021;18(5):2637. doi:10.3390/ijerph18052637
54. Comtet HE, Johannessen KA. A socio-analytical approach to the integration of drones into health care systems. Information. 2022;13(2):62. doi:10.3390/info13020062
55. Geels FW, Schot J. Typology of sociotechnical transition pathways. Res Policy. 2007;36(3):399–417. doi:10.1016/j.respol.2007.01.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.