Back to Journals » Journal of Pain Research » Volume 16
Real-World Treatment Patterns and Outcomes Among Patients with Episodic Migraine in China: Results from the Adelphi Migraine Disease Specific Programme™
Authors Zhao H, Xiao Z, Zhang L, Ford J, Zhong S, Ye W, Li J, Tockhorn-Heidenreich A ![]() , Cotton S
, Cotton S ![]() , Chen C
, Chen C
Received 22 April 2022
Accepted for publication 22 December 2022
Published 3 February 2023 Volume 2023:16 Pages 357—371
DOI https://doi.org/10.2147/JPR.S371887
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Hongru Zhao,1 Zheman Xiao,2 Lei Zhang,3 Janet Ford,4 Shiying Zhong,3 Wenyu Ye,4 Jinnan Li,3 Antje Tockhorn-Heidenreich,4 Sarah Cotton,5 Chunfu Chen6,7
1The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China; 2Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China; 3Eli Lilly China, Shanghai, People’s Republic of China; 4Eli Lilly and Company, Indianapolis, IN, USA; 5Adelphi Real World, Bollington, UK; 6Department of Neurology, Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University Jinan, Jinan, People’s Republic of China; 7Department of Neurology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, People’s Republic of China
Correspondence: Chunfu Chen, Department of Neurology, Shandong Provincial Hospital, # 324 Jingwuweiqi, Road, Shandong, 250021, People’s Republic of China, Tel +86 13853153248, Email [email protected]
Objective: This study assessed treatment patterns, disease burden, outcomes, and unmet needs among patients with episodic migraine (EM) in China using Adelphi Migraine Disease Specific Programme™ (DSP) real-world data.
Background: Migraine is a prevalent and debilitating neurological disorder which presents a major public health burden globally. Research on characteristics, disease burden, and treatment patterns in EM patients in China is limited.
Methods: Data were drawn from an existing data set Adelphi Migraine DSP, a point-in-time survey conducted in China (January-June 2014). Internists/neurologists completed patient record forms for the next 9 patients who consulted them in clinical practice; these same patients completed the ‘patient self-completion questionnaires’. Descriptive analyses were used to assess key variables: patient demographics, treatment patterns (current acute and preventive medication [AM/PM]), effectiveness, issues with existing treatment, Migraine Disability Assessment (MIDAS) scores, and Work Productivity and Activity Impairment scores.
Results: Total of 125 internists/neurologists provided data on 1113 patients with EM (headache days/month < 15). Mean (standard deviation [SD]) age was 43.8 (13.1) years; mean (SD) number of migraine days/month was 3.2 (1.7). AM was prescribed in 86.1% of patients (non-steroid anti-inflammatory drugs [NSAIDs]: 62.7%; triptans: 7.7%), PM in 38.5%, and both in 24.9% of patients. Approximately 55% of patients experienced ≥ 1 issue with their current AM or PM. Migraine-related symptoms (including nausea, photophobia, and phonophobia) were fully controlled in < 50% of patients receiving NSAIDs (21.7– 38.4%) or triptans (32.4– 43.5%). Insufficient response to current AM (migraine headache fully resolved within 2 hours in ≤ 3/5 attacks) was reported by 42.5% of patients. Mild-to-severe disability was reported by 36.8% of patients with a mean (SD) MIDAS score of 5.8 (7.3). Overall, 58.0% of work time was impaired (including time missed and impairment while working).
Conclusion: This analysis suggests, despite existing treatment options, disease burden and unmet medical needs remain substantial in Chinese patients with EM.
Keywords: episodic migraine, clinical practice, patient-reported outcomes, real-world, disease burden
Introduction
Migraine is a debilitating primary headache disorder characterized by intense, recurrent unilateral or bilateral and pulsatile headaches. According to the Headache Classification Committee of the International Headache Society, episodic migraine (EM) is characterized by having 0 to 14 headache days per month (HDM).1,2
Migraine presents a major public health burden globally with substantial impact on various aspects of life including health-related quality of life (HRQoL), day-to-day functioning, and financial burden.3 Findings from the Global Burden of Disease study 2019 reported that migraine remains second among the world’s causes of disability, and first among young women (15–49 years).4 Migraine is more prevalent than diabetes, epilepsy, and asthma combined,5 with a substantial disease burden reported globally and across countries.6,7 In China, the estimated 1-year prevalence of migraine was 9.3%.8 A comprehensive review among patients with migraine in China reported that 52.9% to 68.6% had previously consulted a physician for migraine treatment and, among these, only about 13.5% to 18.0% had been previously diagnosed with migraine.9
Migraine treatment guidelines in China vary from guidelines in the United States (US)10 and Europe.11 Chinese guidelines recommend both a stratified and stepped approach to acute treatment. In a stratified approach, the choice of medication is based on attack severity and symptoms, drug efficacy, side effects, and patient response to previous acute treatment. In a stepped approach, a non-specific drug such as non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, or compound analgesics containing caffeine (cautioning caffeine could increase the risk of drug addiction and medication overuse headache) is given, however, treatment is changed to specific drugs (mechanism of action is developed according to the underlying mechanism of migraine), such as triptans if non-specific drugs fail. Drugs not recommended for use as first-line choice include opioids, barbiturates (non-specific drugs), and ergotamine and derivatives (specific drugs). Recommended preventive medications include calcium antagonists, antiepileptic drugs, beta-blockers, antidepressants, and onabotulinumtoxinB.12
Although treatment guidelines aid healthcare professionals in the management of migraine, there is a paucity of real-world data and limited availability of information on the characteristics, disease burden, and treatment patterns of patients with migraine in China. We sought to fill this research gap by analyzing real-world data captured through the Adelphi Migraine Disease Specific Programme™ (DSP). DSPs are large, multinational, observational studies of clinical practice for a range of common chronic diseases that can support clinical understanding of how diseases are managed including rationale for doctor decision-making and patient attitudes to their condition.13 The study focused on key variables including patient demographics, treatment patterns (acute and preventive treatment), response to acute treatment measured by migraine pain freedom, unmet medical needs with current acute treatment, level of non-pain related symptom control (nausea, photophobia, and phonophobia), Migraine Disability Assessment (MIDAS) scores, and Work Productivity and Activity Impairment (WPAI) questionnaire scores in Chinese patients with EM.
Materials and Methods
Study Design and Population
Data for this analysis were drawn from an existing data set, Adelphi Migraine DSP, a point-in-time survey conducted in China between January and June 2014, which involved internists and neurologists and their consulting patients with migraine (median time to diagnosis was 16 weeks). The DSP is designed to be representative of real-world consulting patients, hence this study enrolled patients who were newly diagnosed as well as those patients diagnosed years previously. The DSP included data pertaining to treatment practice, symptom prevalence, patient demographics, clinical outcomes, medication utilization, adherence patterns, healthcare utilization, productivity, and HRQoL. The survey was conducted according to the Adelphi DSP methodology,13 which has been previously validated.14,15
The DSP surveys are designed to be representative of current clinical practice, with all data derived without prior hypothesis. The study population included physicians and their patients with migraine. Physicians were identified and recruited through networks of field-based interviewers, using public and internal databases, and physicians were eligible to participate if they were personally responsible for treatment decisions and management of patients with migraine. Eligible physicians were either neurologist who consulted with at least 10 patients with migraine in a typical week, or internists who consulted with at least 5 patients with migraine in a typical week.
Physician-reported questionnaires: Eligible physicians completed physician-reported questionnaires for the next 9 patients (≥18 years) who consulted them in clinical practice and who had a diagnosis of migraine; these same patients completed the ‘patient self-completion questionnaires’. Completion of the physician-reported questionnaire was undertaken through consultation of existing patient clinical records, as well as the judgement and diagnostic skills of the respondent physician, which was entirely consistent with decisions made in routine clinical practice. Physician-reported questionnaires captured details on patient demographics, migraine diagnosis, severity of migraine, number of headache days, comorbidities, monitoring, and treatment history (acute and preventive).
Patient-reported questionnaires: Patients for whom the physician completed a physician-reported questionnaire were invited to complete a voluntary, confidential, patient self-completion questionnaire. Using a check box, patients provided informed consent for use of their anonymized and aggregated data and answered questions on demographics, current medical conditions, level of migraine treatment satisfaction, compliance, and health insurance status. Patients also provided data on levels of headache-related disability via the MIDAS and work and activity impairment via the WPAI questionnaire. It should be noted, patient-reported questionnaire forms were completed by the patient independently from their physician and were returned in a sealed envelope, ensuring the patient’s responses were kept confidential from their physician. Specifically, patients gave information regarding their level of response to acute treatment, with each patient answering the question ‘in approximately how many migraine attacks would you say your prescription of acute medicine stops the migraine pain entirely within 2 hours of taking the medication?’ (Options: 0 to 5 of 5 attacks). Patients who reported having no pain within 2 hours of taking their acute medication in ≤3 of 5 attacks were defined as “insufficient responders”.16,17
The MIDAS score measured headache disability over a 3-month period.18,19 It included 5 items regarding the number of days patients reported missing work or experiencing reduced productivity at work or home and missing social events because of headache. The sum of responses to the 5 items gave a total MIDAS score that could be mapped to the following categories: 0–5 = I: little or no disability; 6–10 = II: mild disability; 11–20 = III: moderate disability; 21–40 = IV-A: severe disability; and ≥41 = IV-B: very severe disability. Possible scores ranged from 0 to 270, with lower scores indicating lower headache-related disability. WPAI measured work and activity impairment related to headache-related health problems over the previous 7 days wherein 4 scores were calculated: absenteeism (work time missed), presenteeism (reduced effectiveness while at work), overall work impairment, and activity impairment.20 These were measured on a scale of 0–100%, with higher scores indicating greater impairment and less productivity.
Patients experiencing EM (0–14 average HDM over the previous 6 months) were included in the analysis. EM was defined by average HDM (0–3, 4–7, 8–14).
Statistical Methods
Descriptive summary statistics were generated for all assessments including demographics, clinical characteristics, treatment patterns, and healthcare resource utilization for the overall EM population. All assessments were reported as mean (standard deviation [SD]); for non-missing observations, percentages were calculated as proportion of non-missing data. The survey was designed to facilitate understanding of real-world clinical practice and was non-interventional in nature. No additional tests, treatments, or investigations were performed as part of this survey outside of the normal care provided at the point of recruitment, and thus physicians could only report on data they had at the time of the consultation. Therefore, the data represents the evidence the physicians had when making any clinical treatment and other management decisions at that consultation. Missing data were not imputed; therefore, the base of patients for analysis could vary from variable to variable and was reported separately for each analysis. Continuous variables were compared using analysis of variance and categorical variables were compared using Pearson’s Chi-squared test. Fisher’s exact test was conducted for small sample sizes. Analyses were conducted using Stata version 16.1 or later (StataCorp, College Station, TX, US).
The DSP was conducted in accordance with the European Pharmaceutical Market Research Association code of conduct and, as such, did not require ethical review.
Results
Patient Characteristics
The study recruited 85 (67.8%) neurologists and 40 (32.2%) internists who completed 1113 (HDM 0–3: 599, 4–7: 474, 8–14: 40) physician-reported questionnaires for patients with EM; 951 (HDM 0–3: 527, 4–7: 391, 8–14: 33) of these patients completed a patient-self-completion questionnaire.
As reported in the physician-reported questionnaires, the mean age of patients with EM was 43.8 years, 43.9% were male, and 56.1% were female. The mean number of migraine HDM was 3.2, with tension-type headache in 18.2% of patients and medication overuse headache in 1.6% of patients. Approximately half the patients had at least 1 comorbidity; comorbidities reported in over 5% of patients were hypertension (15.2%), diabetes (9.2%), sleep disorders (7.9%), anxiety (6.8%), and hyperlipidemia (6.6%). A detailed list of patient characteristics and comorbidities is presented in Table 1.
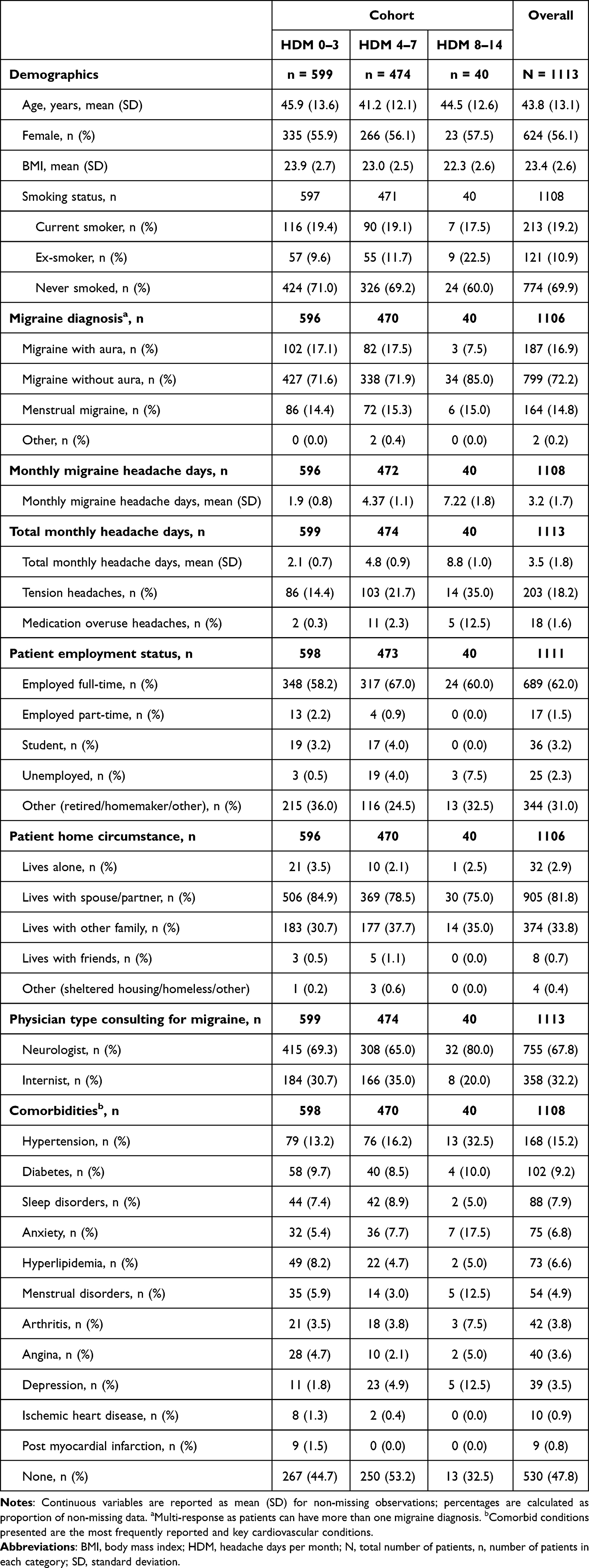 |
Table 1 Demographic and Clinical Characteristics of Patients with Episodic Migraine (Physician-Reported Data) |
The most commonly reported troublesome migraine-related symptoms were unilateral pain (53.2%), bilateral pain (10.6%), pulsating/throbbing pain (10.3%), pain worsened by activity (8.5%), light-headedness (7.1%), nausea (4.4%), muscle weakness/fatigue (1.4%), sensory aura (1.4%), phonophobia (1.2%), and photophobia (1.0%) (Supplementary Table 1).
Treatment
The physician-reported data showed that, in the previous 12 months, the mean number of patient consultations conducted was 3.7 (Supplementary Table 2). The majority of patients were currently prescribed an acute (only) treatment (61.2%), 24.9% were prescribed acute and preventive treatment, while only 13.6% were prescribed a preventive (only) treatment. Among patients with a known acute treatment history (n=1050), 10.3% had never received an acute treatment, 84.0% had received 1 acute treatment regimen but no prior treatment, and 5.7% had received ≥2 different acute treatment regimens. Similarly, among patients with a known preventive treatment history (n=1053), 64.6% had never received a preventive treatment, 32.3% had received 1 preventive treatment regimen, and 3.1% had received ≥2 preventive treatment regimens. Furthermore, data showed that 64.6% of patients were currently using non-pharmacological interventions (such as exercise, massages, change in diet) to help alleviate their migraine symptoms, while fewer patients were administered with an over-the-counter medication (22.7%) and/or a traditional Chinese medication (22.4%) (Table 2).
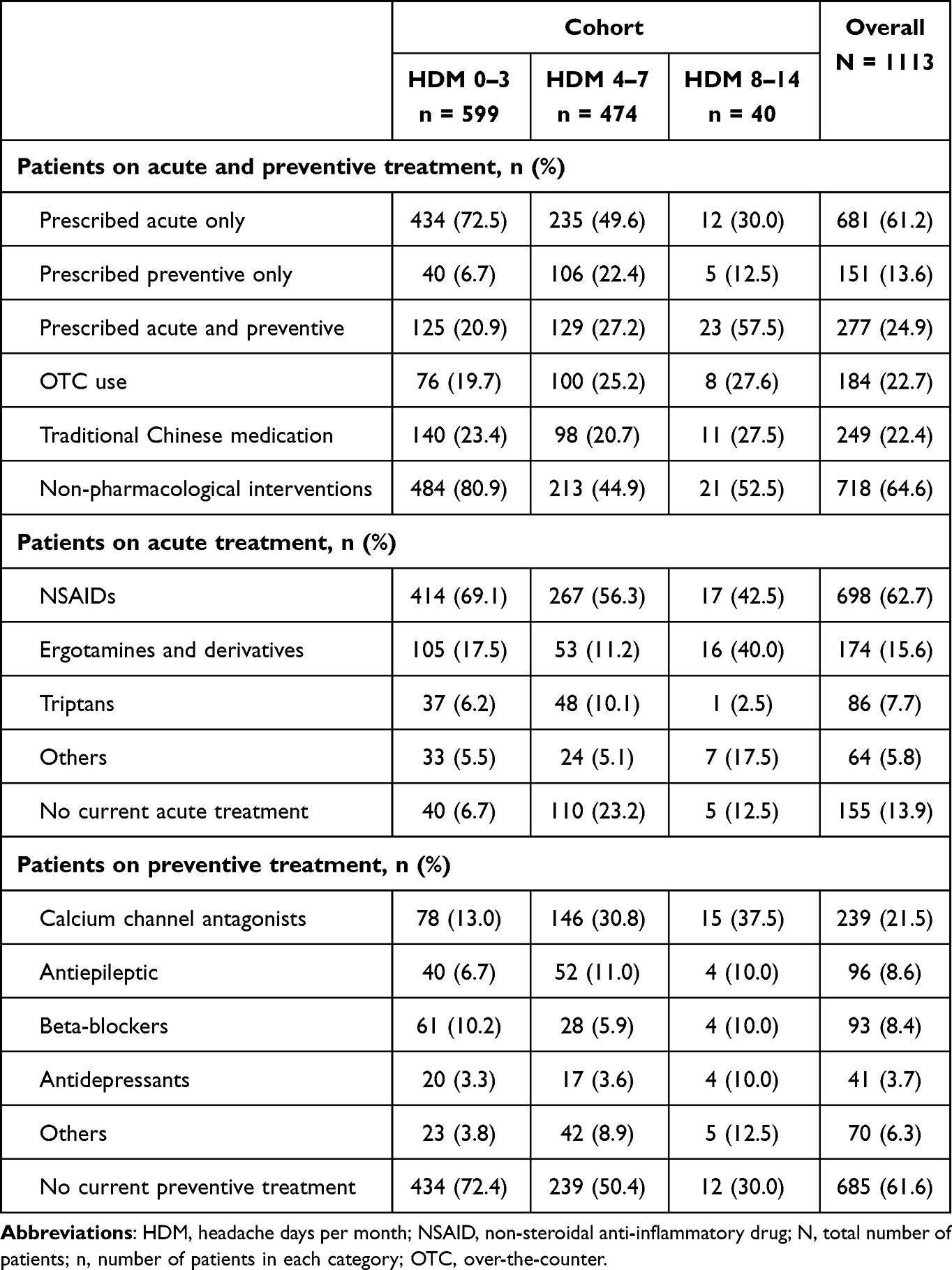 |
Table 2 Medications Currently Prescribed in Patients with Episodic Migraine (Physician-Reported Data) |
In patients currently receiving acute treatment, the majority were prescribed NSAIDs (62.7%), while the use of ergotamines and derivatives (15.6%), triptans (7.7%), and others (5.8%) were relatively low. Most prescriptions among patients receiving preventive treatment were calcium channel antagonists (21.5%), followed by antiepileptics (8.6%), beta-blockers (8.4%), others (6.3%), and antidepressants (3.7%) (Table 2).
According to the physician-reported questionnaire, data indicated that as many as 55% of patients on current acute treatment had at least 1 issue with the treatment. For the current acute treatment population, according to physician reports, lack of efficacy was reported by 4.5% of patients, with the other most common (≥5%) issues being gastrointestinal side effects (20.6%), drowsiness (16.5%), fatigue (12.2%), and dizziness (11.4%). Other reported issues with current acute treatment included paresthesia (4.5%), hypertension (0.9%), chest pains/tightness (2.3%), and other cardiovascular issues (0.7%). Similarly, 55% of patients on current preventive treatment had at least 1 issue with the treatment. For current preventive treatment, according to physician report, 3.5% of patients reported lack of efficacy, and the most common (≥5%) issues included drowsiness (20.0%), dizziness (10.8%), gastrointestinal side effects (13.2%), fatigue (10.3%), and dry mouth (6.1%). Other reported issues with current preventive treatment were paresthesia (1.9%), hypertension (1.6%), and other cardiovascular issues (0.9%) (Figure 1).
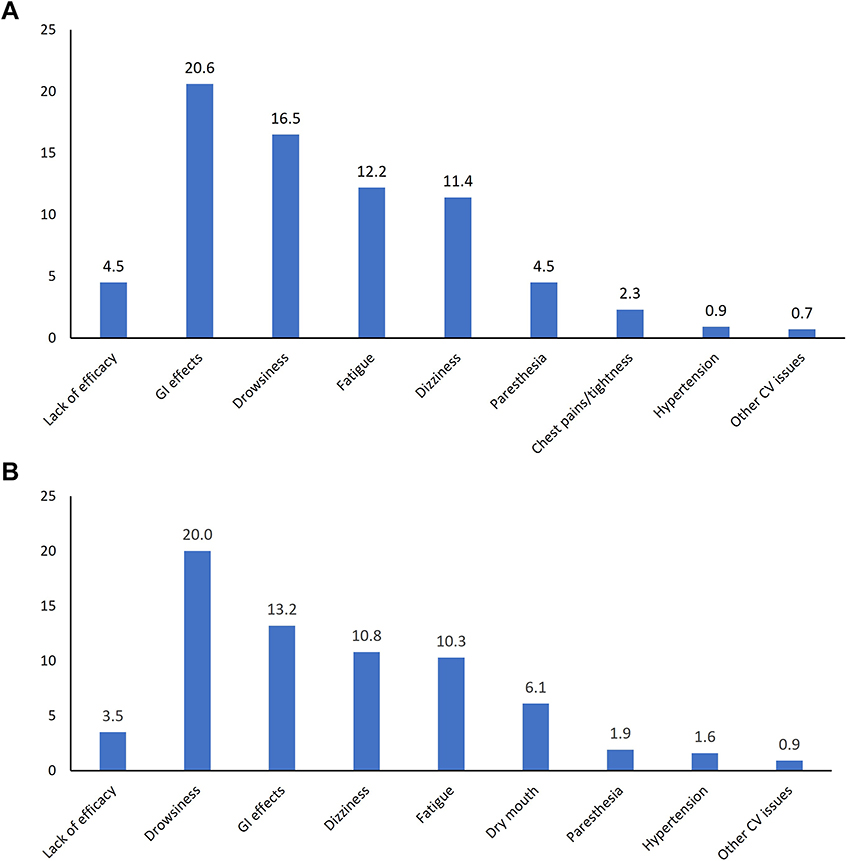 |
Figure 1 Issues/unmet medical need (%) with the current acute (N = 958) (A) and preventive treatment (N = 426) (B). Abbreviations: CV, cardiovascular; GI, gastrointestinal. |
Response to Acute Medication Treatment
The data for response to acute treatment, as reported by patients (n=803) in the patient-self-completion questionnaire, revealed 42.5% of patients had insufficient response (migraine pain fully resolved within 2 hours in ≤3/5 attacks), with 33.6% of patients having pain fully resolved within 2 hours in 3/5 attacks, 7.6% in 2/5 attacks, 0.4% in 1/5 attacks, and 0.9% not having their pain resolved. Accordingly, sufficient response to acute treatment was reported in 57.5% of patients, with migraine pain fully resolved within 2 hours in all 5 attacks in 17.1% of patients and in 4/5 attacks in 40.5% of patients (Figure 2).
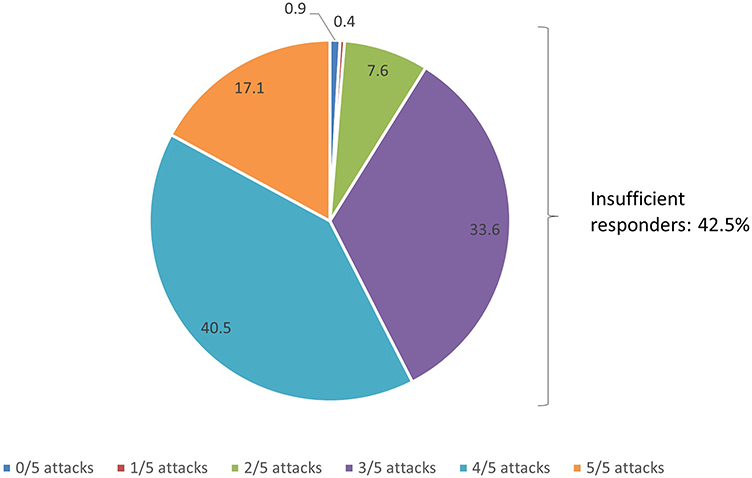 |
Figure 2 Response to current acute treatment (%) (N = 803). |
Migraine-related symptoms (including nausea, photophobia, or phonophobia) were fully controlled in less than 50% of patients on acute medication. Photophobia was fully controlled in 31.0% of patients receiving NSAIDs alone and in 34.6% of patients receiving triptans alone; likewise, nausea was fully controlled in 38.4% of those receiving NSAIDs alone and 32.4% receiving triptans alone. Phonophobia was fully controlled in 43.5% and 21.7% of patients receiving triptans alone and NSAIDs alone, respectively. For patients receiving ergotamine and derivatives, nausea, photophobia and phonophobia were fully controlled in approximately 50% of patients (Figure 3).
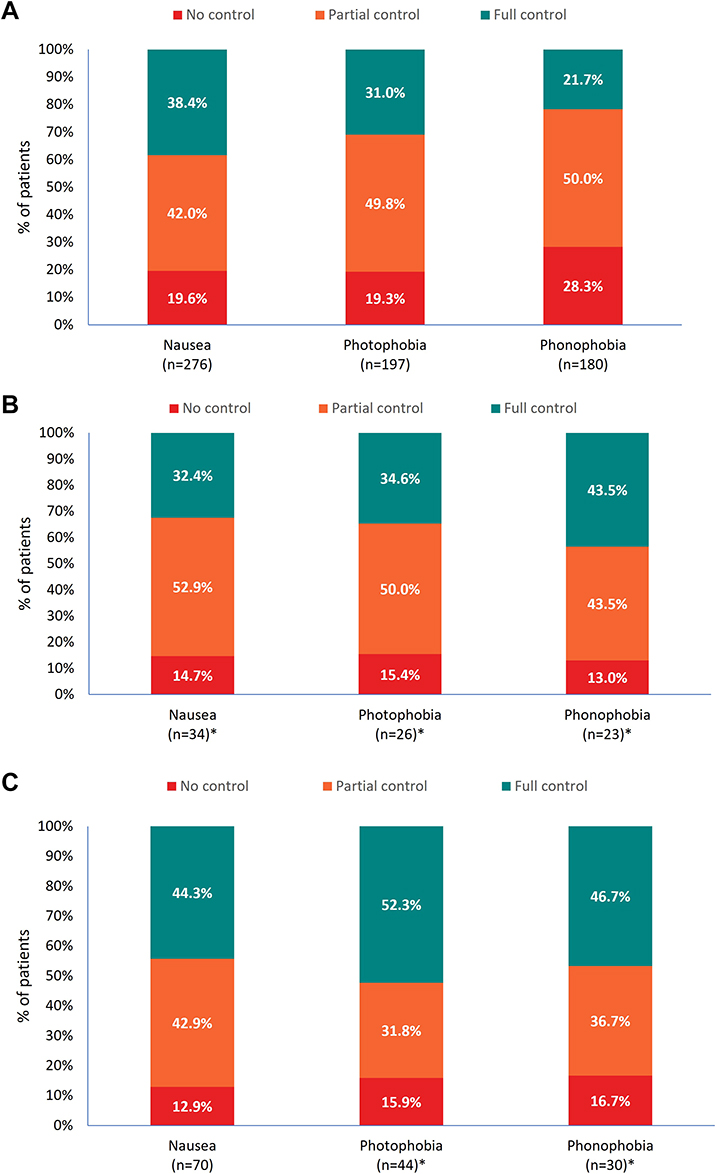 |
Figure 3 Physician-reported level of symptom control with NSAIDs alone (A), triptans alone (B), and Ergotamine and derivatives (C)a. aPatients may or may not have also been receiving preventive treatment. *Low base. Abbreviations: n, number of patients in each category; NSAID, non-steroidal anti-inflammatory drug. |
Migraine Burden
As reported by patients in the patient self-completion questionnaires (n=944), the mean MIDAS score for any kind of migraine-related disability (mean MIDAS total score) was 5.8. The mean MIDAS total score was lowest in the HDM 0–3 cohort (3.7), and it increased with HDM (HDM 4–7: 8.2, 8–14: 10.2). Severe and very severe disability were reported by 4.1% of patients (HDM 0–3: 2.3%, 4–7: 6.2%, 8–14: 9.1%), while moderate disability was reported by 13.2% of patients (HDM 0–3: 8.0%, 4–7: 19.6%, 8–14: 21.2%). Over 60% of patients reported little or no disability and approximately 20% reported mild disability.
The analysis showed the mean impairment in work productivity (WPAI) was 58.0% (HDM 0–3: 55.8%, 4–7: 60.3%, 8–14: 65.4%); mean activity impairment (WPAI) was similar across cohorts, although it was highest in HDM 8–14 (54.9%), followed by HDM 0–3 (53.8%), and lowest in HDM 4–7 (51.1%) (Table 3).
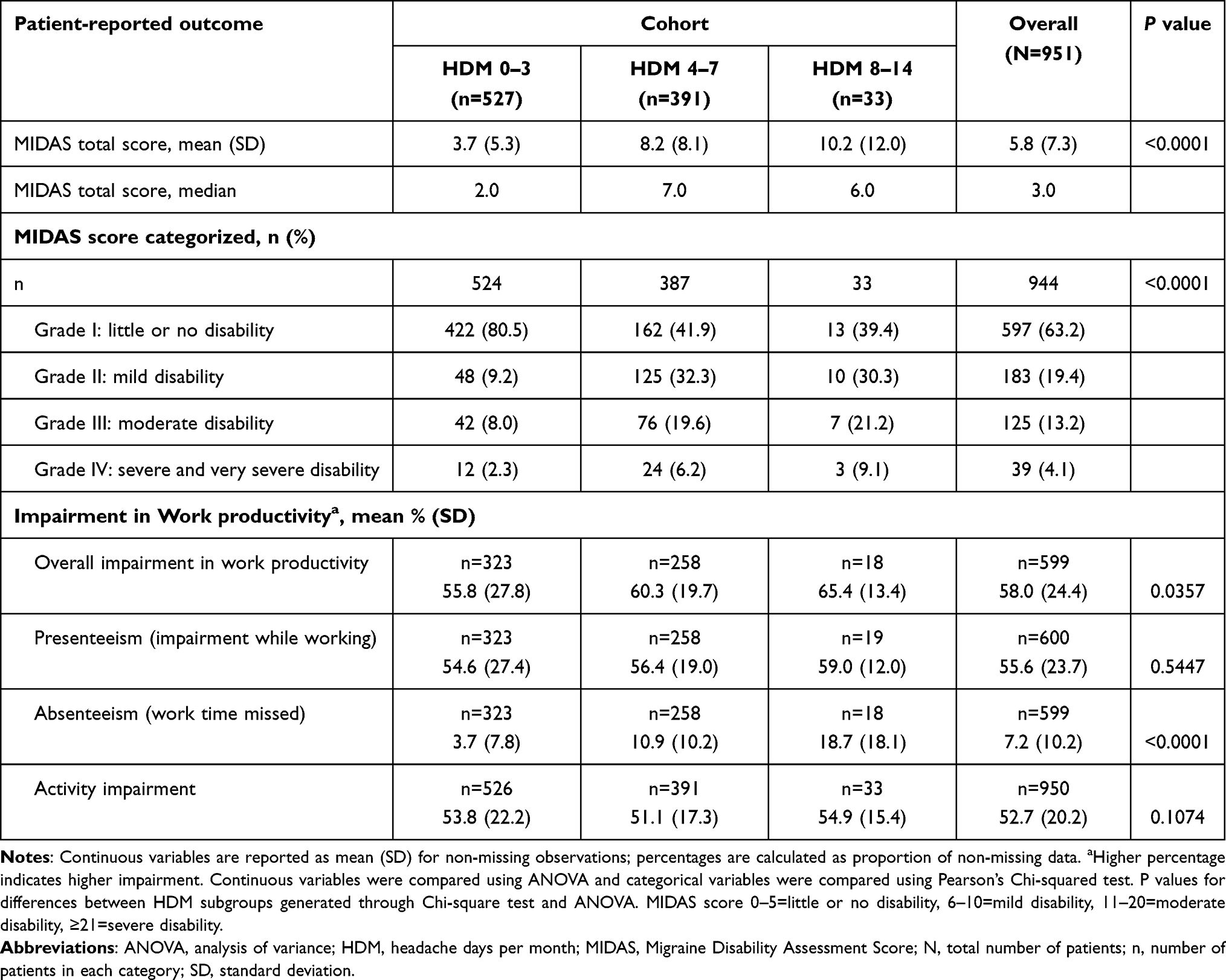 |
Table 3 Burden of Illness in Patients with Episodic Migraine (Patient Self-Completion Form Data) |
Discussion
Overall Observations from the Study
The Adelphi Migraine DSP was the first survey of its kind to be conducted among the Chinese population with migraine. The DSP has a unique design for analyses of real-world data compared to other previously reported population-based studies. This analysis revealed that the majority of patients with EM in China were receiving acute treatment, while only two-fifths were prescribed preventive treatment. It also revealed that half of patients on both acute and preventive treatment experienced at least 1 issue with their current medication; migraine-related symptoms were only partially or not at all controlled by the current acute treatment in half of patients, while two-fifths reported an insufficient response to their acute treatment. Patient-reported data also suggested considerable impairment in work productivity and activity.
These results provide insights into the real-world assessment of EM, as well as valuable information on clinical characteristics, disease burden, and treatment patterns of patients with EM being treated in clinical practice in China.
Demographic Profile of Patients with EM in China Compared to Previous Studies
In the current study, the demographic profile of patients with EM in China was similar when compared to previous population-based studies2,21 and Adelphi Migraine DSP surveys conducted in the US16 and Japan,17 which all reported a high number of female patients (>70%) with EM.
Consistent with the US and Japanese Adelphi Migraine DSP surveys, the mean number of migraine HDM in EM patients in China (3.2) was similar to that reported in the US (3.2)16 and Japan (3.0);17 this similarity between EM patients was also seen for the percentage of patients with tension-type headache, which ranged between 21% and 34% and was higher when compared to medication overuse headache in all surveys.
The most common comorbid condition reported in this survey was hypertension (15.2%). This value is consistent with that reported in the US, where more than 1 in 5 patients had hypertension,16 and in Japan, where 27.5% reported hypertension.17 The occurrence of other comorbidities (≥5%) reported in Chinese patients with EM appeared to be lower than both the US and Japan. In the US, anxiety, depression, and hyperlipidemia were reported in over 10% of patients with EM, and sleep disorder in approximately 10% of patients.16 Similarly, in Japan, hyperlipidemia, anxiety, and sleep disorders were reported in over 10% of patients with EM.17 In addition to these, the Japanese survey reported gastrointestinal disorders and depression in over 10% of patients,17 contrasting with results of the present study which reported lower proportions for these comorbidities in patients with EM.
Prescription Patterns Observed in China in the Adelphi DSP Study versus Other Studies
A previous study from China (China Health Insurance Research Association, CHIRA) reported that acute therapy was prescribed in 26.4% of patients with migraine which was lower than in the current study (86.1%).22 This difference may reflect the different study design: in the DSP study, the physician-reported questionnaire was completed for actively consulting patients, possibly leading to a higher prescription rate than those reported in previous population based studies.22 In line with our results, another study reported that only about 35% of patients were prescribed preventive therapy for migraine.23 The observations from this study regarding patients not on current preventive treatment or never having received a preventive treatment are similar to those reported in Japan and the US (nearly 60% of patients with EM in Japan17 and approximately 50% in the US had never received a prescription for preventive therapy).16 Despite substantial migraine burden and issues with current acute treatment, findings concerning lower prescription rates of preventive therapy highlight the existing unmet medical need for better management through pharmacological migraine-preventive therapy.
In this study, under current acute treatment, a high number of prescriptions of NSAIDs (63%) was in line with Chinese guidelines that recommend their use in these cases. NSAIDs are also widely used in China due to their low price and high accessibility. According to Chinese guidelines, triptans are recommended as level A treatment; however, as observed here, they are not commonly used in China owing to limited patient accessibility, limited choice of drugs (only 3 drugs are available in China vs 7 in the US), and limited formulation choice (eg non-availability of subcutaneous formulations). Ergotamines and derivatives are only recommended as second-line treatment by Chinese guidelines.12 When compared to other studies, the prescription pattern of triptans for acute medication was found to be much higher in the US16 and Japan17 than China. The acute medication prescription pattern in this study was consistent with the CHIRA study of migraine treatment in China.22
This difference in prescription pattern between China and the US was also observed for preventive therapy. In the US DSP, patients with EM were prescribed (>5%) with topiramate (18%), propranolol (8.5%), and amitriptyline (5%).16,17 The preventive prescription pattern observed in this study, however, was consistent with the results of the CHIRA study,22 and generally in line with the Adelphi Japanese Migraine DSP, with the majority of patients prescribed a calcium channel antagonist (flunarizine).17 In China, the preference to use flunarizine as a preventive medication for treatment of EM may be due to the fact flunarizine is the only drug in this class with migraine prevention indication in its label.24
Issues with Current Medication in Chinese Patients Compared to That Reported in Other Patient Population
According to the physician-reported data, more than 50% of patients had at least 1 issue with their current acute or preventive treatment, with the majority reporting gastrointestinal side effects as an issue with their current acute treatment, while drowsiness/sedation was most frequently reported with preventive medication. This contrasts with the Japan study which reported lack of efficacy as the most frequent problem with acute and preventive treatment.17 In the current study, as per the physician-reported questionnaire, approximately 4% of patients were noted to have lack of efficacy with both acute and/or preventive treatment. The possible reasons for the low number of lack of efficacy (4%) as reported by physicians compared with that reported by patients (46%) could be that there was no definition for physician-reported efficacy in the questionnaire, hence the gap may have been due to the lack of communication between physician and patient owing to the heavy work load of physicians in China. Additionally, physicians might consider safety concerns as a more serious issue than lack of efficacy, indicating that physicians need more education in the treatment goal for migraine (for example, they might regard “feeling better” is the indication of good efficacy instead of freedom from pain). Overall, issues with current acute treatment were similar to those reported in Japan (>50%), although for preventive treatment this number was lower in Japan (>20%).17 The US population-based American Migraine Prevalence and Prevention (AMPP) longitudinal study reported that over 40% of patients with EM had at least 1 unmet medical need with their current acute treatment, including lack of efficacy, tolerance, or overall satisfaction.25 Issues due to lack of efficacy or tolerability, which are reported with both acute and preventive therapy, may result in poor adherence to treatment and should be taken into consideration by physicians for more effective management of migraine.
We further assessed data for sufficient/insufficient response to acute treatment from patient self-completion questionnaires. The current study showed 42% of patients with EM were insufficient responders to their current acute medication (defined as those whose migraine pain was not fully resolved within 2 hours in ≤3/5 attacks). These results echoed the findings of the Japanese survey which reported approximately 42% of patients were insufficient responders to current acute treatment,26 and the US DSP which reported 34% insufficient responders.27 In the AMPP study, 56% of patients were insufficient responders (the definition of adequate 2-hour pain freedom was different in the AMPP study ie, adequate 2-hour pain freedom was pain resolved in half the time or more) to acute treatment.28 Overall, these findings report an unmet medical need owing to insufficient response to current acute treatment in patients with EM. Patients with EM who are insufficient responders to acute treatment run the risk of progressing to chronic migraine.29
Furthermore, as per US Food and Drug Administration guidance, the co-primary endpoints to be evaluated in the acute treatment of migraine are: a) having no headache at 2 hours after dose, and b) a demonstrated effect on the most bothersome migraine-associated symptom at 2 hours after dose.30 Hence, to assess the efficacy of acute treatment, in addition to pain-related symptoms, we also assessed the level of symptom control with acute medications which indicated migraine-related symptoms were not fully controlled in half the patients taking acute medications: this is cause for concern and should be further evaluated and taken into consideration for improved management of migraine-related symptoms.
Disease Burden Due to Migraine as Reported in China Compared to Previous Data from Other Countries
It is well established that people with migraine have a considerable disease burden and experience effects on HRQoL.31,32 Our analysis on migraine burden revealed almost 32% of patients had mild or moderate disability, which trended upwards with an increased number of HDM (HDM 8–14 > 4–7 > 0–3). Furthermore, the current study revealed that among employed patients a notable percentage (58%) had their work time impaired due to headaches. This impairment included work time missed and impairment while working. There was an increasing trend for impairment while working and work time missed with an increased number of HDM (HDM 8–14 > 4–7 > 0–3). WPAI scores reported in the Japan DSP were lower for impairment while working (29–37%), work time missed (2–4%), and activity impairment (32–46%), with a lack of trend with increasing number of HDM.17 The WPAI scores as reported by the US patient population were also lower for impairment while working (16–42%), work time missed (2–6%), and activity impairment (19–45%) when compared to EM patients in China.16 In accordance with our study, a cross-sectional study that reported the burden of migraine in Europe observed that a higher number of HDM was associated with an incremental burden of migraine characterized by poorer HRQoL.33 Another previous study also reported that increasing HDM increased impairment in HRQoL.34 One of the major reasons for this burden of migraine could be that physical activities at work or working on cell phones or computers worsen migraine symptoms, especially headaches. Additionally, patients may encounter difficulties performing general and social activities due to phonophobia and photophobia.35 There also appears to be a general stigma surrounding a person with migraine with only about 22% of employers considering migraine a serious enough reason for an employee to be absent from work.35 These findings emphasize the need for an effective acute treatment as a solution to achieve pain relief or pain freedom, which, in turn, may improve patients’ HRQoL and help with EM management.
Strengths and Limitations
Among the strengths of the current study, this analysis included real-world data collected through the validated DSP methodology and reflecting current clinical practice. The large sample size provided valuable inputs on EM patient characteristics, treatment patterns, and HRQoL in China, as well as valuable information to understand and counter unmet medical need in this patient population.
Some limitations of this analysis should be considered. The DSP is not based on a true random sample of physicians or patients. While minimal inclusion criteria governed the selection of participating physicians, participation was influenced by willingness to complete the survey. Physicians recruited consecutive consulting patients avoid selection bias, but no formal patient selection verification procedures were in place. What’s more, there were potential recall bias. However, physicians had access to individual patient clinical records and data were collected at the time of consultation to mitigate against recall bias. The sample is representative of consulting patients with migraine, but the results may not be generalizable to the wider migraine population (eg those living in rural areas and who are undiagnosed or have less severe illness); all data collected relied on accurate reporting by physicians and patients. The sample size in the HDM 8–14 cohort was low. The point-in-time design of the study prevents any conclusions about causal relationships. Also, the data was collected in 2014, however, results could be still considered relevant as the treatment paradigm has not changed much since there is no new medication approved in China over the past 2 decades, and moreover, the treatment guidelines remain similar. Despite such limitations, real-world studies play an important part in highlighting areas of concern that are not addressed in clinical trials.
Conclusions
This real-world study of the Chinese Adelphi Migraine DSP provides information on the clinical characteristics, disease burden, and treatment patterns of people with EM treated in clinical practice in China, which can serve as a guide to healthcare professionals. The analysis suggested that, despite existing treatment options for managing this illness, disease burden and unmet medical need remain substantial in Chinese patients with EM. This study might therefore serve as a basis to explore current treatment patterns depending on patient characteristics and to standardize treatment guidelines in China for better management of patients with EM.
Abbreviations
AM, acute medication; AMPP, American Migraine Prevalence and Prevention; CHIRA, China Health Insurance Research Association; DSP, Disease Specific Programme™; EM, episodic migraine; HDM, headache days per month; HRQoL, health-related quality of life; MIDAS, Migraine Disability Assessment; NSAID, non-steroidal anti-inflammatory drug; PM, preventive medication; US, United States; WPAI, Work Productivity and Activity Impairment.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from Sarah Cotton ([email protected]) on reasonable request.
Ethics Approval and Informed Consent
The DSP was conducted in accordance with the European Pharmaceutical Market Research Association code of conduct and, as such, did not require ethical review. As this was a retrospective analysis that used deidentified, previously collected, data, patient participants were not required to provide formal Consent to Release Information forms for the current analyses; the original consent from those who provided data in the DSP covered the planned analyses in this study.
Acknowledgments
The authors would like to thank Deepika Kajarekar, from Syneos Health, for medical writing support.
Author Contributions
All authors made significant contribution to the conception, study design, execution, acquisition of data, analysis and interpretation of the work reported; critically reviewed and revised the manuscript drafts and provided approval on the final draft for submission to the journal.
Funding
Data collection was undertaken by Adelphi Real World as part of an independent survey, entitled the Adelphi Migraine Disease Specific Programme, sponsored by multiple pharmaceutical companies, one of which was Eli Lilly and Company. The study described here using data from the Adelphi Migraine Disease Specific Programme was funded by Eli Lilly and Company. All data that support the findings of this study are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to Sarah Cotton at [email protected].
Disclosure
Sarah Cotton is an employee of Adelphi Real World. Wenyu Ye is an employee and received stocks from Eli Lilly and Company. Lei Zhang, Janet Ford, Shiying Zhong, Jinnan Li and Antje Tockhorn-Heidenreich are employees of Eli Lilly and Company. Hongru Zhao, Zheman Xiao and Chunfu Chen declare no conflict of interest.
References
1. ICHD-3, Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38:1–211. doi:10.1177/0333102417738202
2. Katsarava Z, Buse DC, Manack AN, Lipton RB. Defining the differences between episodic migraine and chronic migraine. Curr Pain Headache Rep. 2012;16:86–92. doi:10.1007/s11916-011-0233-z
3. Leonardi M, Raggi A. A narrative review on the burden of migraine: when the burden is the impact on people’s life. J Headache Pain. 2019;20:41. doi:10.1186/s10194-019-0993-0
4. Steiner TJ, Stovner LJ, Jensen R, et al. Migraine remains second among the world’s causes of disability, and first among young women: findings from GBD2019. J Headache Pain. 2020;21:137. doi:10.1186/s10194-020-01208-0
5. Steiner TJ, Stovner LJ, Birbeck GL. Migraine: the seventh disabler. J Headache Pain. 2013;14:1. doi:10.1186/1129-2377-14-1
6. Safiri S, Pourfathi H, Eagan A, et al. Global, regional, and national burden of migraine in 204 countries and territories, 1990 to 2019. Pain. 2021;26. doi:10.1097/j.pain.0000000000002275
7. Woldeamanuel YW, Cowan RP. Migraine affects 1 in 10 people worldwide featuring recent rise: a systematic review and meta-analysis of community-based studies involving 6 million participants. J Neurol Sci. 2017;372:307–315. doi:10.1016/j.jns.2016.11.071
8. Yu S, Liu R, Zhao G, et al. The prevalence and burden of primary headaches in China: a population-based door-to-door survey. Headache. 2012;52(4):582–591. doi:10.1111/j.1526-4610.2011.02061.x
9. Takeshima T, Wan Q, Zhang Y, et al. Prevalence, burden, and clinical management of migraine in China, Japan, and South Korea: a comprehensive review of the literature. J Headache Pain. 2019;20:111. doi:10.1186/s10194-019-1062-4
10. Burch RC, Ailani J, Robbins MS. The American headache society consensus statement: update on integrating new migraine treatments into clinical practice. Headache. 2022;62:111–112. doi:10.1111/head.14245
11. Antonaci F, Dumitrache C, De Cillis I, Allena M. A review of current European treatment guidelines for migraine. J Headache Pain. 2010;11:13–19. doi:10.1007/s10194-009-0179-2
12. Chinese Medical Association Group. Guide to the prevention and treatment of migraine in China [Chinese]. Chin J Pain Med. 2016;22:721–727.
13. Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: disease-specific programmes - a means to understand. Curr Med Res Opin. 2008;24:3063–3072. doi:10.1185/03007990802457040
14. Babineaux SM, Curtis B, Holbrook T, Milligan G, Piercy J. Evidence for validity of a national physician and patient-reported, cross-sectional survey in China and UK: the disease specific programme. BMJ Open. 2016;6:e010352. doi:10.1136/bmjopen-2015-010352
15. Higgins V, Piercy J, Roughley A, et al. Trends in medication use in patients with type 2 diabetes mellitus: a long-term view of real-world treatment between 2000 and 2015. Diabetes Metab Syndr Obes. 2016;9:371–380. doi:10.2147/DMSO.S120101
16. Ford JH, Jackson J, Milligan G, Cotton S, Ahl J, Aurora SK. A real-world analysis of migraine: a cross-sectional study of disease burden and treatment patterns. Headache. 2017;57:1532–1544. doi:10.1111/head.13202
17. Ueda K, Ye W, Lombard L, et al. Real-world treatment patterns and patient-reported outcomes in episodic and chronic migraine in Japan: analysis of data from the Adelphi migraine disease specific programme. J Headache Pain. 2019;20:68. doi:10.1186/s10194-019-1012-1
18. Stewart WF, Lipton RB, Dowson AJ, Sawyer J. Development and testing of the migraine disability assessment (MIDAS) questionnaire to assess headache-related disability. Neurology. 2001;56:S20–S28. doi:10.1212/WNL.56.suppl_1.S20
19. Stewart WF, Lipton RB, Kolodner K, Liberman J, Sawyer J. Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia. 1999;19:107–114. doi:10.1046/j.1468-2982.1999.019002107.x
20. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4:353–365. doi:10.2165/00019053-199304050-00006
21. Buse DC, Manack A, Serrano D, Turkel C, Lipton RB. Sociodemographic and comorbidity profiles of chronic migraine and episodic migraine sufferers. J Neurol Neurosurg Psychiatry. 2010;81:428–432. doi:10.1136/jnnp.2009.192492
22. Yu S, Zhang Y, Yao Y, Cao H. Migraine treatment and healthcare costs: retrospective analysis of the China Health Insurance Research Association (CHIRA) database. J Headache Pain. 2020;21:53. doi:10.1186/s10194-020-01117-2
23. Blumenfeld AM, Bloudek LM, Becker WJ, et al. Patterns of use and reasons for discontinuation of prophylactic medications for episodic migraine and chronic migraine: results from the second international burden of migraine study (IBMS-II). Headache. 2013;53:644–655. doi:10.1111/head.12055
24. Karsan N, Palethorpe D, Rattanawong W, Marin JC, Bhola R, Goadsby PJ. Flunarizine in migraine-related headache prevention: results from 200 patients treated in the UK. Eur J Neurol. 2018;25:811–817. doi:10.1111/ene.13621
25. Lipton RB, Buse DC, Serrano D, Holland S, Reed ML. Examination of unmet treatment needs among persons with episodic migraine: results of the American Migraine Prevalence and Prevention (AMPP) study. Headache. 2013;53:1300–1311. doi:10.1111/head.12154
26. Hirata K, Ueda K, Ye W, et al. Factors associated with insufficient response to acute treatment of migraine in Japan: analysis of real-world data from the Adelphi Migraine Disease Specific Programme. BMC Neurol. 2020;20:274. doi:10.1186/s12883-020-01848-4
27. Lombard L, Ye W, Nichols R, Jackson J, Cotton S, Joshi S. A real-world analysis of patient characteristics, treatment patterns, and level of impairment in patients with migraine who are insufficient responders vs responders to acute treatment. Headache. 2020;60:1325–1339. doi:10.1111/head.13835
28. Lipton RB, Munjal S, Buse DC, Fanning KM, Bennett A, Reed ML. Predicting inadequate response to acute migraine medication: results from the American Migraine Prevalence and Prevention (AMPP) study. Headache. 2016;56:1635–1648. doi:10.1111/head.12941
29. Lipton RB, Fanning KM, Serrano D, Reed ML, Cady R, Buse DC. Ineffective acute treatment of episodic migraine is associated with new-onset chronic migraine. Neurology. 2015;84:688–695. doi:10.1212/WNL.0000000000001256
30. Migraine: developing drugs for acute treatment guidance for industry; 2018. Available from: https://www.fda.gov/media/89829/download.
31. Lipton RB, Hamelsky SW, Kolodner KB, Steiner TF, Stewart WF. Migraine, quality of life, and depression: a population-based case-control study. Neurology. 2001;55:629–635. doi:10.1212/WNL.55.5.629
32. Blumenfeld AM, Varon SF, Wilcox TK, et al. Disability, HRQoL and resource use among chronic and episodic migraineurs: results from the International Burden of Migraine Study (IBMS). Cephalalgia. 2010;31:301–315. doi:10.1177/0333102410381145
33. Doane MJ, Gupta S, Fang J, Laflamme AK, Vo P. The humanistic and economic burden of migraine in Europe: a cross-sectional survey in five countries. Neurol Ther. 2020;9:535–549. doi:10.1007/s40120-020-00196-2
34. Torres-Ferrús M, Quintana M, Fernandez-Morales J, Alvarez-Sabin J, Pozo-Rosich P. When does chronic migraine strike? A clinical comparison of migraine according to the headache days suffered per month. Cephalalgia. 2017;37:104–113. doi:10.1177/0333102416636055
35. Shimizu T, Sakai F, Miyake H, et al. Disability, quality of life, productivity impairment and employer costs of migraine in the workplace. J Headache Pain. 2021;22:29. doi:10.1186/s10194-021-01243-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient-Reported Outcomes in Ovarian Cancer: Facilitating and Enhancing the Reporting of Symptoms, Adverse Events, and Subjective Benefit of Treatment in Clinical Trials and Clinical Practice
Campbell R, King MT, Stockler MR, Lee YC, Roncolato FT, Friedlander ML
Patient Related Outcome Measures 2023, 14:111-126
Published Date: 8 May 2023
TRITRIAL: The Impact of Fixed Triple Therapy with Beclometasone/Formoterol/Glycopyrronium on Health Status and Adherence in Chronic Obstructive Pulmonary Disease in an Italian Context of Real Life
Richeldi L, Schino P, Bargagli E, Ricci A, Rocca A, Marchesani F, Pennisi A, Camiciottoli G, D'Amato M, Macagno F, Scaffidi Argentina U, Ingrassia E, Piraino A
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:475-487
Published Date: 23 February 2024