Back to Journals » Medical Devices: Evidence and Research » Volume 19
Real-World Performance of the Veriset Hemostatic Patch: A Multicenter Study of Adjunctive Hemostasis
Authors Quyn A, Navarro A, Caldonazo T, Findlay JM, Doenst T, Anderson M, Gong X, Botman JM
Received 13 January 2026
Accepted for publication 20 May 2026
Published 29 May 2026 Volume 2026:19 595863
DOI https://doi.org/10.2147/MDER.S595863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Mohamad Bashir
Aaron Quyn,1 Alex Navarro,2 Tulio Caldonazo,3 John M Findlay,4,5 Torsten Doenst,3 Melissa Anderson,6 Xue Gong,6 Joost MJ Botman7
1John Goligher Colorectal Unit, University of Leeds, St James’s University Hospital, Leeds, UK; 2Hepatico-Pancreatico-Biliary Surgery, Nottingham University Hospitals NHS Trust, Nottingham, UK; 3Department of Cardiothoracic Surgery, Jena University Hospital, Friedrich Schiller University, Jena, Germany; 4Academic Department of Abdominal Wall and Upper GI Surgery, North Devon District Hospital, Royal Devon University Healthcare NHS Foundation Trust, Barnstaple, UK; 5NIHR Exeter Biomedical Research Centre, University of Exeter Medical School, Exeter, UK; 6Medtronic, Minneapolis, MN, USA; 7Department of Vascular Surgery, Ziekenhuisgroep Twente, Almelo, The Netherlands
Correspondence: Aaron Quyn, John Goligher Colorectal Unit, University of Leeds, St James’s University Hospital, Leeds, LS9 7TF, UK, Tel +4401132067219, Email [email protected]
Purpose: Uncontrolled bleeding remains a major surgical challenge, increasing morbidity, operative time, and costs, highlighting the need for effective adjunctive hemostats. Veriset is a synthetic, absorbable patch that promotes clotting and provides mechanical hemostasis. While early studies show efficacy, real-world evidence across diverse settings is needed. This post-market, multicenter study evaluated the safety and effectiveness of Veriset in various surgical procedures.
Methods: This observational, single-arm, prospective study was nested within Medtronic’s product surveillance registry. Sites were selected for procedural diversity (cardiovascular, soft-tissue, solid-organ), high Veriset use, and clinical study experience. Patients treated with Veriset as part of usual care were followed for 30 days post-procedure to monitor adverse events (AEs). The primary safety and effectiveness endpoints were device-related AEs within 30 days and hemostasis within 5 minutes, respectively. Secondary outcomes included time to hemostasis, length of hospital stay, and bleeding-site severity. Results were summarized using descriptive statistics and exact (Clopper–Pearson) confidence intervals.
Results: Veriset was used on-label in 100 patients in cardiovascular (56), soft-tissue (18), solid-organ (18), and other (8) procedures. Most were performed via open surgery (90.0%), with 34% involving anastomoses. Median blood loss was 600 mL (interquartile range 200– 1500), with transfusions in 24 patients. Of the 120 bleeding sites treated, pre-Veriset methods included sutures (55.8%, 67/120) and pressure (29.2%, 35/120). Bleeding was mostly mild/moderate (82.5%, 99/120). Device-related AEs occurred in 1 patient, with no deaths. Hemostasis within 5 minutes was achieved at 91.7% (110/120) of sites and in 96.0% (96/100) of patients. Median time to hemostasis was 2.0 minutes; median hospital stay was 7 days.
Conclusion: This study provides real-world evidence that Veriset is safe and suggests that it may be an efficacious and rapid adjunct for surgical hemostasis, including in high-risk cardiovascular and solid-organ procedures, supporting and extending prior trial data for routine clinical use.
Clinicaltrials.gov Identifier: NCT01524276, Dec 24, 2025.
Plain-language summary: Uncontrolled bleeding during and after surgery can cause complications, make surgeries longer, and increase healthcare costs. Researchers wanted to see if the Veriset hemostatic patch could help stop bleeding quickly in real-world surgeries. The Veriset patch is made from materials that form a gel that initiates the clotting process to stop bleeding. The patch breaks down and disappears in the body after about a month.
To test the patch, researchers collected information from 100 people who had different types of surgery, including cardiovascular, soft-tissue, and solid-organ procedures. They checked how fast the patch stopped bleeding and whether there were any complications associated with the use of the patch.
The study found that Veriset stopped bleeding within five minutes for 96 out of the 100 patients, with most bleeding stopped in about two minutes. The study also checked for any complications related to the use of Veriset. Only one person had a problem that may have been connected to the procedure and the patch, which was successfully managed with medication. There were no complications linked only to the use of Veriset.
These results suggest that the Veriset patch is a safe and effective way to control bleeding during surgery. Its fast action, simple use, and performance in high-risk cases could help people recover better and may reduce the need for blood transfusions.
Keywords: bleeding, surgery, topical hemostat
Introduction
Uncontrolled bleeding remains a major intraoperative and postoperative challenge across a wide range of surgical procedures, contributing to increased morbidity, prolonged operative times, and elevated healthcare costs.1,2 The need for effective adjunctive hemostatic agents has led to the development of a variety of topical hemostatic agents designed to achieve rapid and reliable bleeding control.3–6 The Veriset (Medtronic, Minneapolis, MN, USA) hemostatic patch is a synthetic, absorbable hemostat composed of oxidized cellulose and polyethylene glycol (PEG). The combination of the oxidized, regenerated cellulose and the resultant gel initiates the clotting cascade and acts as a tamponade, physically stemming the flow of a broad spectrum of active bleeding site types. Following activation, the patch absorbs in approximately 28 days.
Preclinical studies and early clinical trials, including randomized controlled trials, have demonstrated that Veriset is effective in achieving hemostasis within minutes in controlled surgical environments.7–10 However, controlled trial settings often fail to capture the complexity and variability of real-world surgical practice when evaluating hemostatic products given the unpredictable nature of their use.8–10 Additionally, while these previous controlled trials have shown median times to hemostasis ranging from 1–1.5 min along with overall adverse event (AE) rates ranging from 75–77% and device-related AE rates from 0–6%, patient inclusion and exclusion criteria and procedural heterogeneity are generally more restricted in controlled clinical trials, so observed hemostatic performance and postoperative complication rates in controlled clinical trials could be expected to differ from rates observed in regular clinical use. Therefore, real-world evidence from observational studies is essential to validate these findings in broader, more heterogeneous patient populations and procedural contexts.
This study aimed to evaluate the real-world safety and efficacy of the Veriset hemostatic patch in a multicenter cohort of patients undergoing a variety of extensive surgical procedures where adjunctive hemostatic control was required. Specifically, we aimed to assess the time to hemostasis, intraoperative blood loss, postoperative bleeding complications, AEs, and overall surgeon satisfaction in routine clinical practice. To clarify how Veriset fits within established intraoperative hemostasis workflows, we outlined a concise, conceptual decision management pathway for this study: (1) Surgeons first identify the bleeding source and attempt standard measures such as pressure, cautery, or suturing, which remain the foundation of bleeding control. (2) When these measures are insufficient—particularly in cases of diffuse oozing, friable tissue, or anatomically constrained fields—adjunctive topical agents are considered. (3) Within this escalation framework, Veriset serves as a mechanical, absorbable patch option that can be selected when a conformable surface hemostat is appropriate. (4) Following application, the surgical field is reassessed, and alternative adjuncts or additional techniques are used only if bleeding persists. By capturing data related to this intraoperative hemostasis workflow for the application of Veriset across diverse surgical specialties and healthcare settings, this study seeks to provide a comprehensive understanding of Veriset’s performance in real-world use, thereby informing clinical decision-making and supporting optimal hemostatic strategies in surgery.
Materials and Methods
Study Design
This prospective, multi-center, observational post-market study on the use of Veriset hemostatic patches utilized data from a product surveillance registry (PSR) maintained by Medtronic. Data collection was reflective of routine clinical practice. The accuracy and completeness of all data was confirmed and approved by the principal investigator or authorized designee at each site, and all data were reviewed by Medtronic, with any apparent discrepancies resolved via discussion with the reporting site. Patients were followed for 30 days post procedure, with follow-up data collected in person, via medical record review, or on remote follow-up in line with standard care. In case of an ongoing AE at day 30, patients were followed until the AE had been resolved or a maximum of 30 additional days. All procedure- and/or device-related events were to be reported upon awareness by the site and in accordance with each site’s ethics board and local and national laws and regulatory requirements.
Site selection criteria included the following: high-volume Veriset users with the infrastructure to conduct a clinical study, participation in Veriset premarket studies, and current participation in the Medtronic PSR. Consideration was also given to the indications that each site used Veriset for to ensure a good representation of the targeted indications categories: cardiovascular surgery, soft-tissue repair procedures, and solid-organ/multi-visceral resection. Decisions to use Veriset were based on the standard of care at each site and discretion of the treating surgeon rather than on involvement in the study. Patient enrollment inclusion criteria were written authorization and/or consent per institution and geographic requirements from the patient or a legally authorized representative provided prior to or up to 30 days after the procedure and patients intended to be treated with Veriset. Regardless of enrollment time, the use of Veriset was at the discretion of the surgeon. Patients who were expected to be inaccessible for follow-up, excluded by local law, or enrolled in or planned to be enrolled in any concurrent drug and/or device study that may confound the PSR results were excluded. The study was reviewed and approved by each site’s ethics committee prior to site activation (Supplemental Table 1). The study was conducted in compliance with the Declaration of Helsinki.
Outcome Measures
The primary safety endpoint was the incidence of device-related AEs within 30 days of procedures where Veriset was utilized for hemostasis, including those occurring intraoperatively and up to discharge. The analyzed cohort was restricted to patients for whom Veriset was applied on-label, ie., use for achieving hemostasis at an active bleeding site. Patients for whom Veriset was applied off-label, ie., prophylactic use at sites where bleeding was anticipated but not actively occurring, were excluded. A 30-day follow-up period was chosen because the mechanism of action, intended use, and regulatory expectations for hemostatic technologies focus on immediate intraoperative performance and early postoperative complications that typically manifest within the first 30 days. The primary effectiveness endpoint was the rate of achieving hemostasis at each bleeding site within 5 minutes of device application as in a previous study of Veriset.8 Hemostasis within 5 minutes is a validated and clinically meaningful endpoint because it captures the critical early phase in which effective bleeding control directly influences blood loss, the need for escalation, operative time, and postoperative complications. This threshold is widely used in hemostatic device trials and is supported by regulatory precedent, as multiple randomized studies of topical agents—including fibrin sealants and flowable hemostats—demonstrate that time to hemostasis within 5 minutes is a sensitive and reproducible measure of efficacy.11 Time to hemostasis and length of hospital stay were also recorded. The characteristics of each bleeding site were evaluated, including the source and anatomic location, and bleeding severity was rated on a scale from 1 (least severe) to 4 (most severe) as follows: 1 = “ooze or intermittent flow”, 2 = “continuous flow”, 3 = “controllable spurting and/or overwhelming flow”, and 4 = “unidentified or inaccessible spurting or gush”.12
Statistical Analysis
Descriptive statistics were used to summarize study outcomes. For continuous variables, mean and standard deviation (SD), median and interquartile range (IQR), and minimum and maximum values were reported. For categorical variables, counts and percentages were used. In addition, statistically appropriate confidence intervals (CIs) were calculated for the primary and secondary endpoints where applicable. The sample size was determined based on the primary safety and effectiveness evaluations, including a review of data from premarket studies on Veriset.8–10 A sample size of 100 patients was determined to provide sufficient power (>80%) to evaluate the primary safety and effectiveness endpoints. The primary safety evaluation was based on a device-related AE threshold of 10% and an expected rate of 3%. The primary effectiveness evaluation was based on a performance goal of 50% and an expected success rate of 75% or higher. The statistical analysis was based on the exact Clopper–Pearson method.
Results
Demographics and Medical History
This study enrolled 112 patients from five sites in Germany (18 patients), the Netherlands (40 patients), and the United Kingdom (54 patients). Participating sites, areas of specialty, and patient enrollment by site are summarized in Supplemental Table 1. Of the 112 patients, 2 were enrolled, but Veriset was not used in the procedure, 4 were exited due to missing documentation, and another 6 were treated off-label. Of the 106 patients treated with Veriset in any manner, 105 completed the 30-day follow-up, and of the 100 treated on-label, 99 completed the 30-day follow-up, with 1 patient lost to follow-up (Figure 1). Demographics for these patients are shown in Table 1. Data on both height and weight were not recorded in all cases, and body mass index (BMI) could only be calculated for 64 patients. The majority of these 100 patients (95%) had a specified comorbidity. Note that the numbers represent the total number of comorbidities present and that an individual patient could have had multiple comorbidities.
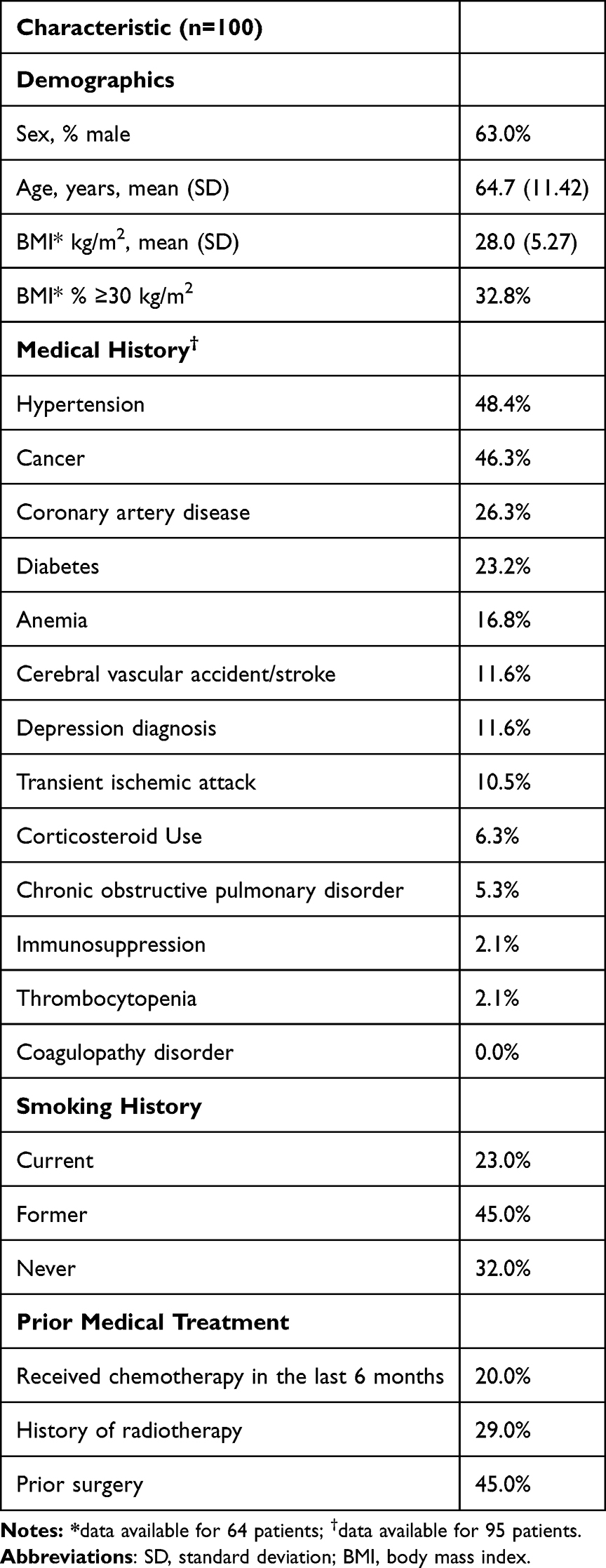 |
Table 1 Patient Demographics |
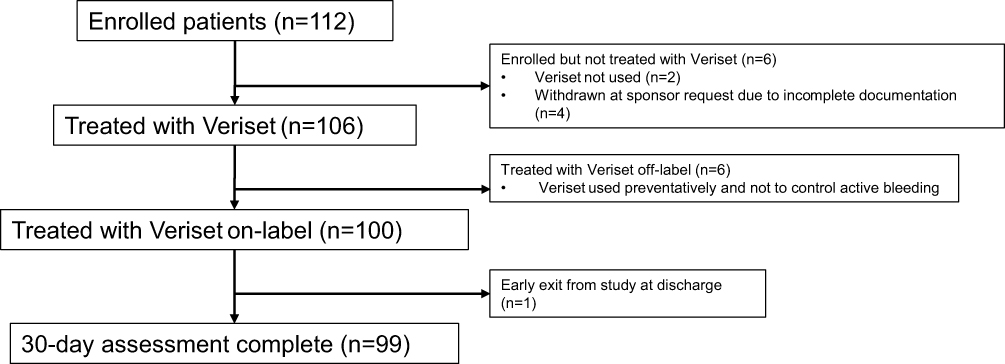 |
Figure 1 Patient enrollment and follow-up. |
Procedural Details
A total of 56/100 patients underwent a cardiovascular procedure, including procedures involving major vascular structures such as advanced pelvic exenteration, 18 underwent a soft-tissue procedure, 18 underwent solid-organ resection, and 8 underwent procedures listed by the site as “other”. The specific primary diagnoses leading to each procedure type and the specific procedures performed are detailed in Supplemental Table 2 and Supplemental Table 3, respectively. The majority (90/100) of procedures were performed using open surgery, 9 were performed laparoscopically, and 1 was performed with robotic-assisted surgery. No procedures were converted from the original surgical approach. Anastomoses were established in 34% of cases, with the majority of cases requiring 1 (52.9%) or 2 (41.2%) anastomoses. Of the 54 anastomoses established, 23 were intestinal, 17 were vascular, 11 were ureteric, and 3 were ureteroileal. Median (IQR) blood loss was 600.0 (200.0–1500.0) mL (note that data on blood loss was available for only 65 cases), and transfusions were necessary in 24 of the procedures. Procedural details by indication type are summarized in Table 2. Overall, 120 active bleeding sites in 100 patients were treated, with 59 bleeding sites treated during cardiovascular procedures, 27 during soft-tissue procedures, 22 during solid-organ procedures, and 12 during other procedure types (Table 3). Most of the 100 patients (84) had 1 bleeding site, while 10 had 2 sites, and 6 had 3 sites (Table 4). The most common conventional methods used to try to obtain hemostasis before the use of Veriset were sutures/ligature (55.8%, 67/120) and pressure on the bleeding site (29.2%, 35/120).
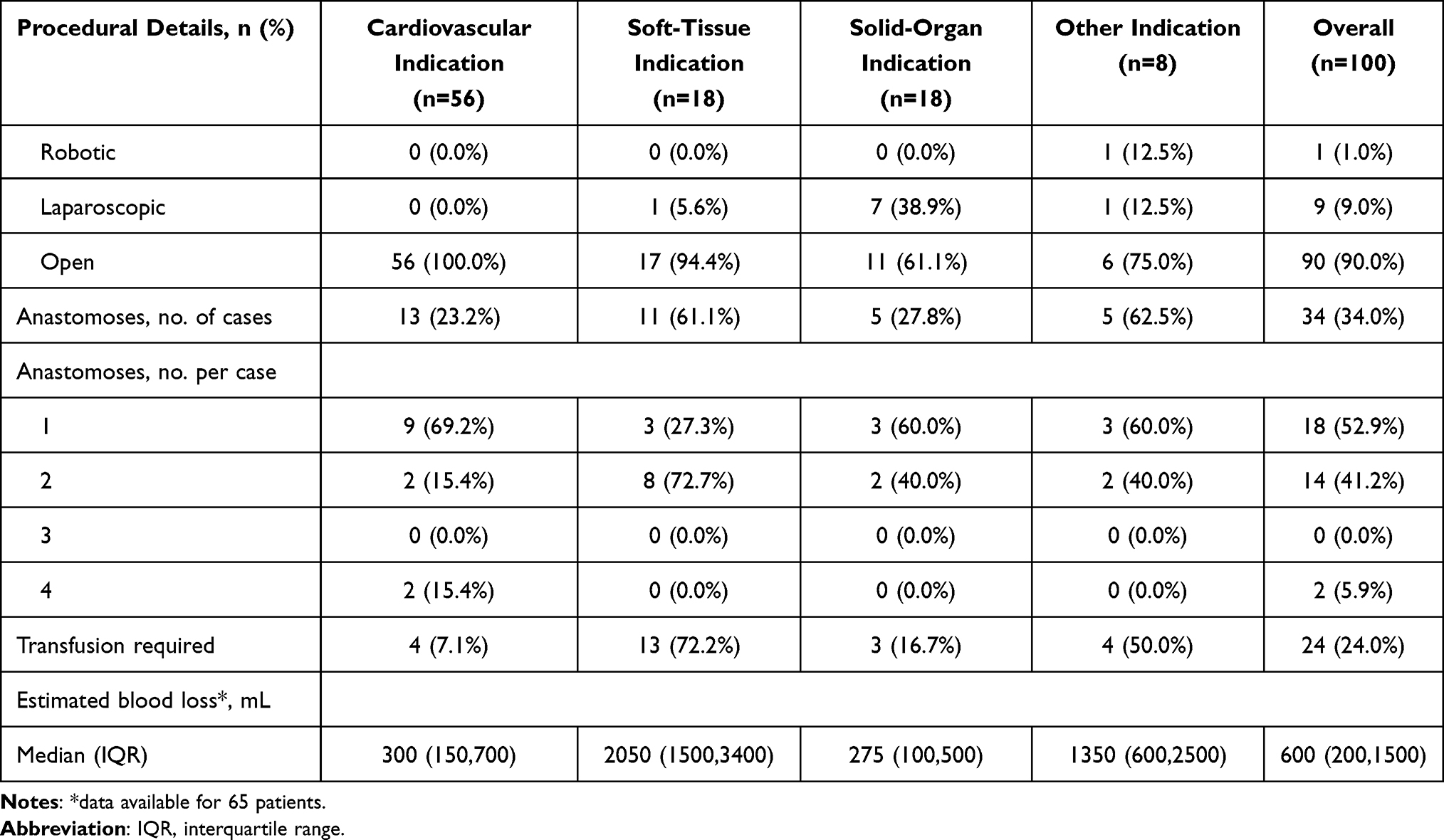 |
Table 2 Procedural Details by Indication |
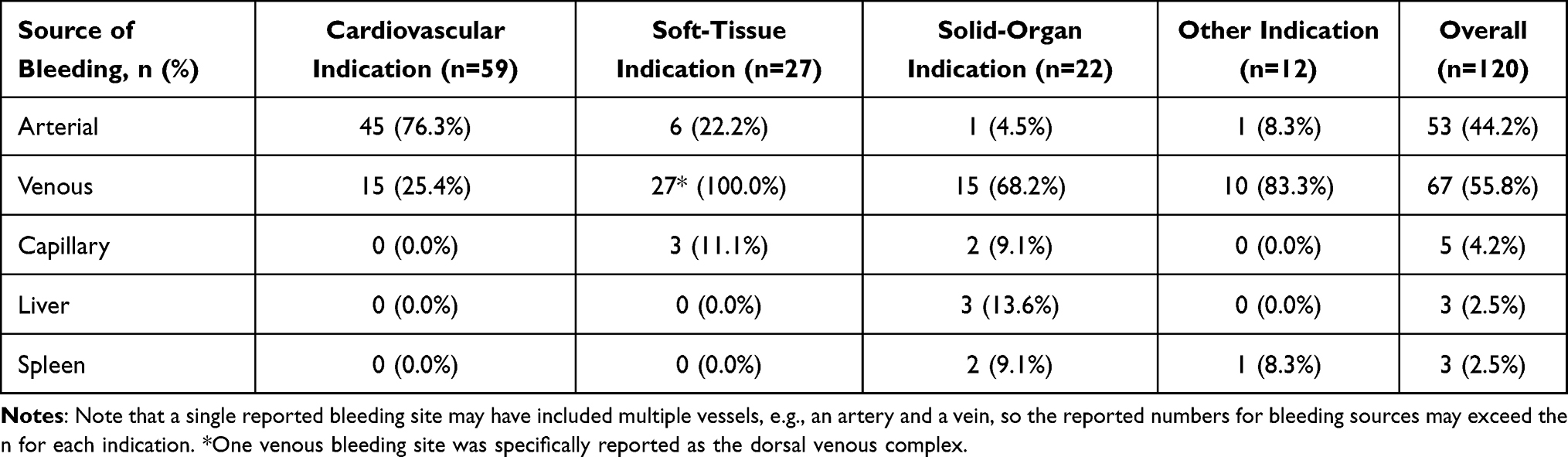 |
Table 3 Summary of Bleeding Sites Sources |
 |
Table 4 Bleeding Site Number per Patient by Indication |
Safety Endpoint Outcomes
The rate of AEs possibly related to the device and procedure within 30 days following the use of Veriset as an adjunct to hemostasis, which was the primary safety endpoint of the study, was 1.0% (1/100, splenic collection), and the 90% CI was 0.1% to 4.7%, which is below the predetermined AE rate threshold of 10% (Table 5). The patient returned to the hospital 3 days post procedure with ongoing left upper quadrant and left-sided abdominal pain, tachycardia, and a fever. Blood tests showed elevated inflammatory markers. A computed tomography scan showed a small amount of fluid collected around a small spleen tear, which was too small for drainage. The patient was given oral antibiotics and an analgesic and recovered without further complications. There were no AEs related only to the use of Veriset. In addition to the 1 AE possibly related to the device and procedure noted previously, there were 60 procedure-related AEs reported in 38/100 patients (see Supplemental Table 4 for a summary of all AEs). Of these, 55 AEs in 36 patients were reported as serious events, with the most common being procedural hemorrhage (26%, 26/100). Note that while all patients had bleeding that was treated with Veriset, not all bleeding events were considered reportable AEs as only events where estimated blood loss exceeded 500 mL were evaluated by the site to determine if it constituted an AE. All reported events were resolved, and there were no deaths reported.
 |
Table 5 Safety and Effectiveness Endpoint Outcomes |
Effectiveness Endpoint Outcomes
For the primary effectiveness endpoint, hemostasis was achieved within 5 minutes of Veriset application for 91.7% (110/120) of the bleeding sites, and the 95% CI was 85.2% to 95.9%, which is above the predetermined threshold of 50% and the expected success rate of 75%. The 10 bleeding sites (4 patients) where hemostasis was not achieved within 5 minutes solely with the use of Veriset required rescue therapy, which consisted of suturing in all 10 cases and additional stapling in 3 of the cases. For 7 of these bleeding sites (3 patients), rescue therapy achieved hemostasis within 5 min, and for the other 3 sites (1 patient), time to hemostasis with rescue therapy exceeded 5 min. All 4 of these patients underwent a general lower abdominal procedure involving exenteration for anorectal cancer (see Supplemental Table 5 for additional details). Across all 120 treated bleeding sites, the median (95% CI) time to hemostasis was 2.0 (1.5, 2.0) min. The median (95% CI) length of hospital stay was 7.0 (4.0, 16.0) days (Table 5). For the 120 treated bleeding sites, 50 (41.7%) had bleeding severity graded as 1, followed by 49 (40.8%) graded as 2, 20 (16.7%) graded as 3, and 1 (0.8%) graded as 4. Rates of hemostasis within 5 min for sites with bleeding severity grades of 1, 2, 3, and 4 were 100.0% (50/50), 91.8% (45/49), 70.0% (14/20), and 100.0% (1/1), respectively. In addition, hemostasis was achieved at all bleeding sites within 5 minutes of Veriset application in 96% (96/100) of the patients.
Discussion
This multicenter, real-world, single-arm study evaluated the safety and effectiveness of the Veriset hemostatic patch in 100 patients treated across a range of surgical specialties. The device appeared to be highly effective, with hemostasis achieved at 91.7% of bleeding sites within five minutes of application and a median time to hemostasis of just 2 minutes. These outcomes compare favorably with published effectiveness rates of other topical hemostatic agents, such as fibrin sealants and oxidized regenerated cellulose products, which typically achieve hemostasis within approximately 5–10 minutes in controlled surgical settings.13,14 Outcomes were also comparable to real-world results from a large registry study of a collagen-based hemostatic patch that showed an overall rate of hemostasis within 2 min of 74.5%.15
This study enrolled a broad and representative surgical population, with 95% of patients presenting with at least one comorbidity and a wide range of procedure types and bleeding severities. Most procedures were performed via open surgery (90%), reflecting real-world practice in more extensive or complex cases.15 Notably, Veriset was successfully used across a range of bleeding severities, including high-flow bleeding (grade 3, 16.7%) and even one grade 4 bleeding event. This highlights its potential as an effective adjunct across the bleeding severity spectrum. Veriset’s rapid action within a median of 2 minutes and its effectiveness across multiple bleeding severities, including high-flow bleeding, highlight a potential performance advantage in time-critical situations. Many of the cases in this study, including those involving the cardiovascular system, liver resection, and pelvic exenteration, are associated with a high bleeding risk and technically demanding hemostatic management.16–18 Despite this complexity, Veriset appeared to achieve rapid and satisfactory hemostatic control across all procedure types, with similar success in soft-tissue, solid-organ, and “other” categories. Furthermore, Veriset was used following conventional hemostatic measures in many cases, particularly sutures or ligatures (55.8%) and direct pressure (29.2%), indicating its potential for use as a secondary adjunct when traditional methods such as suture, cautery, or pressure alone are insufficient.
The need for rescue therapy at 8.3% (10/120) of bleeding sites suggests that while Veriset is highly effective, it may be less reliable in certain high-risk or anatomically complex sites. Further subgroup analyses could help identify predictive factors for success or failure. Similarly, while blood loss and transfusion data were not available for all cases, the median blood loss of 600 mL and transfusion rate of 24% align with expectations for complex surgical cohorts and underscore the clinical need for reliable hemostatic tools in these settings. It is also worth noting that the relatively high median blood loss in patients undergoing soft-tissue procedures was primarily due to the fact that many of these involved pelvic exenteration for rectal cancer, which is often associated with high levels of blood loss.19
Given the 96% patient-level hemostatic success and minimal device-related AEs, Veriset may offer clinical benefits in procedures where bleeding control is challenging, especially when traditional methods are insufficient. Its ease of application and rapid action could potentially contribute to reduced operative times and a decreased need for blood transfusions, although studies making direct comparisons with outcomes from other hemostatic devices are necessary to better evaluate these potential benefits. With 24% of procedures in this study requiring transfusion, improved bleeding control could help mitigate this risk in future surgical care protocols.
While formal surgeon-reported data were not captured in this study, informal feedback from participating investigators noted that Veriset was user-friendly, required minimal preparation, and adhered well to irregular tissue surfaces. Compared to key alternative devices, such as fibrin-based sealants and gelatin-thrombin matrices, Veriset requires no thawing, mixing, or complex handling steps, offering logistical advantages in urgent intraoperative scenarios. Its synthetic and absorbable nature may also reduce immunogenicity.10
Several limitations must be acknowledged. The observational design and absence of a control arm limit the ability to make direct efficacy or safety comparisons with other hemostatic agents, including conservative measures such as a period of direct pressure. Incomplete data, particularly on BMI, blood loss, and transfusions, may have influenced the generalizability of some outcome measures. The sample size, while adequate for an exploratory real-world evaluation, was limited in its power to detect rare safety signals. Another important limitation of this study is the substantial heterogeneity of included surgical procedures, encompassing various specialties and approaches, such as open, laparoscopic, and robotic-assisted techniques, which introduces variability in bleeding profiles, surgical complexity, and hemostatic demands. This diversity, while reflective of real-world practice, can impact the reproducibility of the findings across specific surgical contexts and, given the sample size of this study, limits the ability to perform subgroup analyses. Device use was also limited to a European cohort, with the majority of cardiovascular procedures performed in Germany and the Netherlands and all soft-tissue, solid-organ, and other procedures performed in the UK. Therefore, the findings may not fully translate to different healthcare systems or surgical practices across Europe and globally. Further studies, including comparative analyses of hemostatic performance and cost effectiveness between Veriset and established hemostatic agents in broader patient populations, are warranted. Surgeon-reported usability data and standardized satisfaction metrics should be incorporated to better assess workflow and handling preferences. Additionally, evaluating Veriset in minimally invasive procedures and in populations outside of Europe will be important to confirm broader applicability and optimize clinical decision-making.
Conclusion
This study provides real-world evidence supporting the clinical utility of Veriset as a rapid, effective, and safe adjunct to surgical hemostasis. Its performance in high-risk surgical fields such as cardiovascular and solid-organ procedures suggests that it may be especially valuable in cases where fast, reliable bleeding control is required. These findings align with and extend prior controlled trial data, highlighting the device’s role in routine surgical practice.
Abbreviations
AE, adverse event; BMI, body mass index; CI, confidence interval; IQR, interquartile range; PEG, polyethylene glycol; PSR, product surveillance registry; SD, standard deviation.
Acknowledgments
The authors wish to thank Robert Donovan for medical writing support under the direction of the lead author and in accordance with Good Publication Practice guidelines; Julie Doyle for study conceptualization and administration; Pascal Smeets, Jennifer Bell, and Jennifer Wolvers for study supervision; and Kyle Andrew for data curation. All are employees of Medtronic.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Medtronic provided funding for this study.
Disclosure
AN reports personal fees for teaching and training from Medtronic. JF reports standard commercial research funding paid to his institution from Medtronic. MA and XG – Medtronic employee. The authors report no other conflicts of interest in this work.
References
1. Salenger R, Arora RC, Bracey A, et al. Cardiac surgical bleeding, transfusion, and quality metrics: joint consensus statement by the enhanced recovery after surgery cardiac society and society for the advancement of patient blood management. Ann Thorac Surg. 2025;119(2):280–10. doi:10.1016/j.athoracsur.2024.06.039
2. Corral M, Ferko N, Hollmann S, Broder MS, Chang E. Health and economic outcomes associated with uncontrolled surgical bleeding: a retrospective analysis of the premier perspectives database. Clin Outcomes Res. 2015;7:409–421. doi:10.2147/ceor.s86369
3. von Oppell UO, Zilla P. Tissue adhesives in cardiovascular surgery. J Long Term Eff Méd Implant. 1997;8(2):87–101.
4. Witter K, Tonar Z, Matějka VM, et al. Tissue reaction to three different types of tissue glues in an experimental aorta dissection model: a quantitative approach. Histochem Cell Biol. 2010;133(2):241–259. doi:10.1007/s00418-009-0656-3
5. Cheikh A, Ajaja MR, Rhazali H, et al. Contribution of fibrin glue in the surgery of cyanogenic and non-cyanogenic congenital cardiopathies: retrospective cohort study. BMC Cardiovasc Disord. 2019;19(1):117. doi:10.1186/s12872-019-1102-7
6. Reynolds MW, Clark J, Crean S, Samudrala S. Risk of bleeding in surgical patients treated with topical bovine thrombin sealants: a review of the literature. Patient Saf Surg. 2008;2(1):5. doi:10.1186/1754-9493-2-5
7. Howk K, Fortier J, Poston R. A novel hemostatic patch that stops bleeding in cardiovascular and peripheral vascular procedures. Ann Vasc Surg. 2016;31:186–195. doi:10.1016/j.avsg.2015.09.007
8. Schuhmacher C, Pratschke J, Weiss S, et al. Safety and effectiveness of a synthetic hemostatic patch for intraoperative soft tissue bleeding. Méd Devices. 2015;8:167–174. doi:10.2147/mder.s79556
9. Öllinger R, Mihaljevic AL, Schuhmacher C, et al. A multicentre, randomized clinical trial comparing the Veriset™ haemostatic patch with fibrin sealant for the management of bleeding during hepatic surgery. HPB. 2013;15(7):548–558. doi:10.1111/hpb.12009
10. Glineur D, Hendrikx M, Krievins D, et al. A randomized, controlled trial of VerisetTM hemostatic patch in halting cardiovascular bleeding. Méd Devices. 2018;11:65–75. doi:10.2147/mder.s145651
11. Spotnitz WD, Burks S. Hemostats, sealants, and adhesives: components of the surgical toolbox. Transfusion. 2008;48(7):1502–1516. doi:10.1111/j.1537-2995.2008.01703.x
12. Lewis KM, Li Q, Jones DS, et al. Development and validation of an intraoperative bleeding severity scale for use in clinical studies of hemostatic agents. Surgery. 2017;161(3):771–781. doi:10.1016/j.surg.2016.09.022
13. Schwartz M, Madariaga J, Hirose R, et al. Comparison of a new fibrin sealant with standard topical hemostatic agents. Arch Surg. 2004;139(11):1148–1154. doi:10.1001/archsurg.139.11.1148
14. Brown KGM, Solomon MJ. Topical haemostatic agents in surgery. Br J Surg. 2024;111(1):znad361. doi:10.1093/bjs/znad361
15. Lombardo C, Lopez-Ben S, Boggi U, et al. Hemopatch® is effective and safe to use: real-world data from a prospective European registry study. Updates Surg. 2022;74(5):1521–1531. doi:10.1007/s13304-022-01353-y
16. Garrett C, Brown KGM, Solomon MJ, et al. Conventional versus high-complexity total pelvic exenteration for locally advanced and locally recurrent rectal cancer: an international multicenter study. Dis Colon Rectum. 2026;69(1):34–41. doi:10.1097/dcr.0000000000003986
17. Kim S, Jung YK, Lee KG, et al. A systematic review and meta-analysis of blood transfusion rates during liver resection by country. Ann Surg Treat Res. 2023;105(6):404–416. doi:10.4174/astr.2023.105.6.404
18. Petrou A, Tzimas P, Siminelakis S. Massive bleeding in cardiac surgery. Definitions, predictors and challenges. Hippokratia. 2016;20(3):179–186.
19. Platt E, Dovell G, Smolarek S. Systematic review of outcomes following pelvic exenteration for the treatment of primary and recurrent locally advanced rectal cancer. Techniq Coloproctol. 2018;22(11):835–845. doi:10.1007/s10151-018-1883-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Review of Evidence Supporting the Arista™ Absorbable Powder Hemostat
LyBarger KS
Medical Devices: Evidence and Research 2024, 17:173-188
Published Date: 21 May 2024