Back to Journals » Lung Cancer: Targets and Therapy » Volume 15
Real-World Outcomes with Lurbinectedin in Second Line and Beyond for Extensive Stage Small Cell Lung Cancer in Korea
Authors Shim JS ![]() , Kim Y, Yuh T, Lee JB
, Kim Y, Yuh T, Lee JB ![]() , Kim HR, Hong MH, Cho BC, Lim SM
, Kim HR, Hong MH, Cho BC, Lim SM
Received 21 August 2024
Accepted for publication 18 October 2024
Published 30 October 2024 Volume 2024:15 Pages 149—159
DOI https://doi.org/10.2147/LCTT.S485320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sai-Hong Ou
Joo Sung Shim,1 Youhyun Kim,1 Taeho Yuh,1 Jii Bum Lee,2 Hye Ryun Kim,2 Min Hee Hong,2 Byoung Chul Cho,2 Sun Min Lim2
1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Republic of Korea; 2Division of Medical Oncology, Department of Internal Medicine, Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Republic of Korea
Correspondence: Sun Min Lim, Division of Medical Oncology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, 03722, Republic of Korea, Tel +82-2-2228-1946 ; +82-10-2520-3969, Email [email protected]
Purpose: Small-cell lung cancer (SCLC) accounts for approximately 10– 15% of all lung cancers and is characterized by a high recurrence rate, early metastasis, and poor prognosis. Before the FDA approved lurbinectedin for SCLC that progressed on or after platinum-based chemotherapy in 2020, topotecan was the sole second-line option associated with hematological toxicities and modest efficacy. Lurbinectedin received conditional approval in Korea in September 2022 for metastatic SCLC progression, with the same indications. Real-world data on its efficacy remains scarce owing to its recent implementation.
Patients and Methods: Patients with metastatic SCLC who progressed on or after first-line therapy (n = 51) at Yonsei Cancer Center, Seoul, received lurbinectedin at 3.2 mg/m². Efficacy data, including tumor response, progression, survival, and demographics, were recorded.
Results: A total of fifty-one patients received lurbinectedin between April 2023 and March 2024, with thirty-four patients being eligible for the assessment. At diagnosis, approximately one-third of the patients were female, 3% had a poor performance status with an Eastern Cooperative Oncology Group Performance Score (ECOG PS ≥ 2), and the median age was 68. Most patients (80%) had extensive disease. Overall objective response rate (ORR) and disease control rate (DCR) were 20% and 47%, respectively. The median progression-free survival (PFS) was 2.8 months, and the median overall survival (OS) was 3.3 months. Never smokers showed prolonged OS compared with current/former smokers (Smokers; 3.0 vs 7.3 months). Common adverse effects were nausea (53%), loss of appetite (24%), general weakness (18%), anemia (29%), neutropenia (12%), dizziness (6%), alopecia (6%), thrombocytopenia (3%), and pneumonia (3%). Overall, 24% of the patients experienced grade ≥ 3 adverse events (AEs), with the most common being anemia (9%) and neutropenia (9%).
Conclusion: Real-world data suggest that lurbinectedin is a viable option for patients with SCLC who have progressed on or after platinum-based chemotherapy.
Keywords: SCLC, lurbinectedin, real-world evidence, second line
Introduction
Small-cell lung cancer (SCLC), which accounts for approximately 10–15% of all lung cancers, is characterized by a high recurrence rate, a strong tendency for early metastasis, and poor prognosis.1 Most patients are diagnosed with extensive disease, with only one-third presenting with early stage disease amenable to potentially curative multimodality therapy.2 Because SCLC is clinically and biologically distinct from other types of lung cancer, progress in its therapeutic advancement stands in stark contrast to that observed in non-small cell lung cancer (NSCLC).3,4
Current evidence suggests platinum-based chemotherapy combined with etoposide and anti-PD-L1 antibody as first-line therapy, although the median OS remains at approximately 1 year even with the addition of atezolizumab.5,6 This is partly due to the high recurrence rate of the disease, and almost all patients with SCLC relapse after achieving a dramatic response to 1st line therapy.7,8 Before lurbinectedin, a marine-derived selective inhibitor of oncogenic transcription, was approved for metastatic SCLC after first-line therapy in 2020, only a few treatment options were available for SCLC that has progressed after the initial therapy. Among these, topotecan is the most widely used second-line treatment for metastatic SCLC. However, its efficacy was limited, with a median progression-free survival (PFS) of 2.7 months, and topotecan was associated with a significant degree of hematological toxicities9–12
Lurbinectedin was approved in Korea in September 2022 for the treatment of adult patients with metastatic SCLC with disease progression on or after platinum-based chemotherapy. However, real-world data on its efficacy is scarce because of its recent implementation.13–16 In this study, we investigated real-world data of patients with metastatic SCLC treated with lurbinectedin in Korea.
Materials and Methods
Patients and Data Collection
This study enrolled a total of 51 patients treated with lurbinectedin from April 2023 to March 2024. Seventeen patients were unable to be evaluated for response evaluation, and total 34 patients were evaluated. For patients who are classified as “Unable to obtain 1st RECIST”, four patients received lurbinectedin but passed away before tumor response evaluation could be completed. One patient discontinued lurbinectedin due to grade 4 general weakness and poor oral intake. Lastly, three patients stopped lurbinectedin based on their personal preferences/beliefs. Patients who are classified as “Follow up loss” were those who did not return to the clinic after receiving lurbinectedin. Lastly, one patient was referred to a hospice care unit before tumor response evaluation (Figure 1). This study was conducted as a retrospective chart review of patients with pathologically confirmed small cell lung cancer (SCLC) who received lurbinectedin beyond first-line therapy at Severance Hospital, Republic of Korea, between April 2023 and March 2024. We excluded patients who received lurbinectedin for indications other than SCLC, such as extrapulmonary small cell cancers.
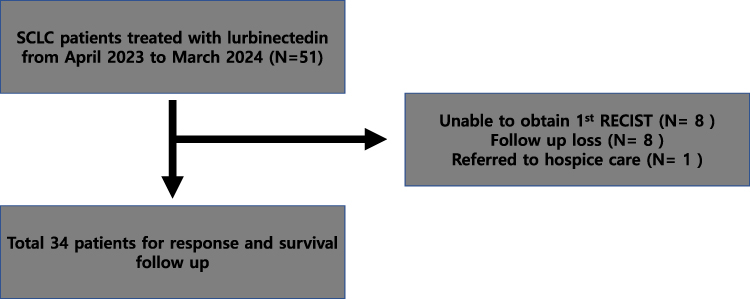 |
Figure 1 Flow chart of the patients enrolled. Fifty-one patients were initially screened for the study. Seventeen patients did not meet the study criteria and failed to enroll the study. A total of 34 patients were investigated for response and survival outcomes. |
Efficacy Assessment
Tumor assessments were conducted prior to treatment initiation, and follow-up evaluations were performed via computed tomography within the first three months. Tumor size was measured by investigators in accordance with RECIST 1.1 criteria.17 Overall response was defined as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). Additional efficacy parameters included the disease control rate, duration of response, PFS, and OS. PFS was defined as the duration from the initiation of lurbinectedin treatment to disease progression or mortality from any cause. OS was defined as the period from lurbinectedin treatment initiation to all-cause mortality.
Efficacy Comparison with Other 2nd Line Chemotherapies
The comparison of PFS between lurbinectedin and other second-line chemotherapy regimens (topotecan, irinotecan + platinum (IP), and belotecan) was conducted using retrospective data from patients who were treated with chemotherapeutic agents other than lurbinectedin in 2nd lines of therapy but later received lurbinectedin in lines beyond the second, between April 2023 and March 2024. The patient characteristics of each group are described in Tables 1 and 2.
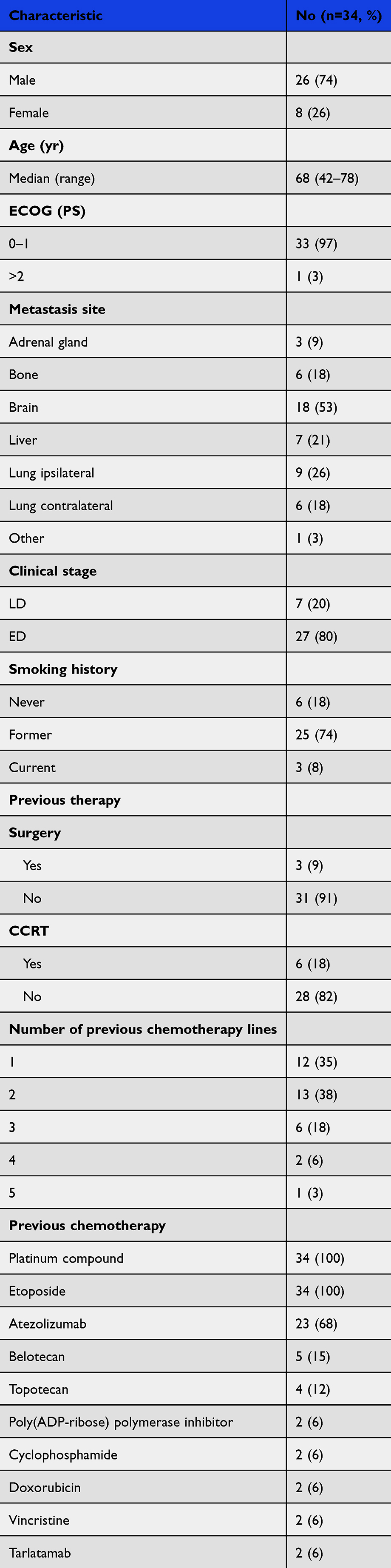 |
Table 1 Baseline Characteristics of the Patients |
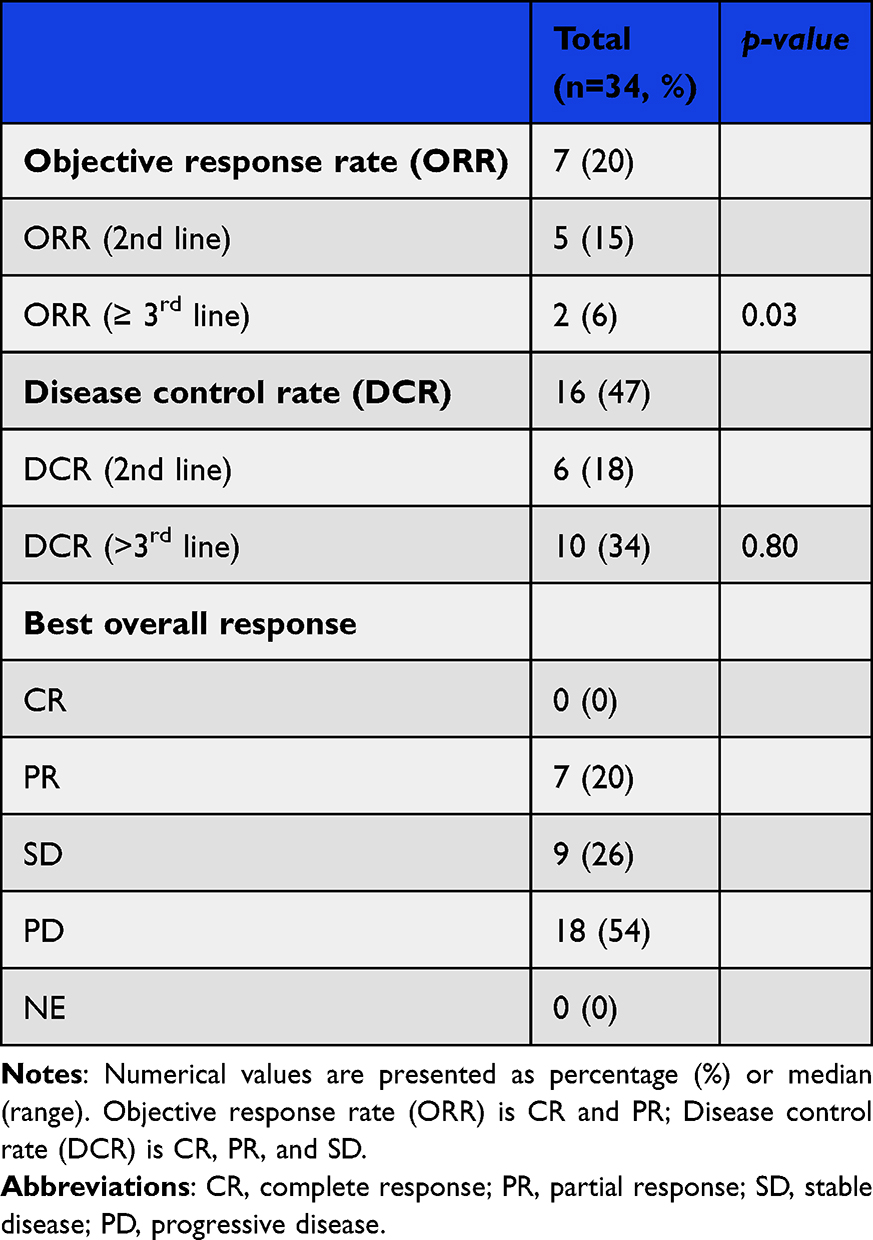 |
Table 2 Overall Objective Response |
Safety Assessment
Safety was assessed at each patient's visit by routine physical examination and laboratory tests as needed by the physician. Toxicity was classified according to the Common Terminology Criteria for Adverse Events ver. 5 (CTCAE v 5.0). Specifically, we abstracted toxicities, including anemia, neutropenia, thrombocytopenia, fatigue, nausea, anorexia, febrile neutropenia, and an increase in laboratory tests, including creatinine, alanine transaminase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (ALP). Toxicity data, including symptoms such as nausea, fatigue, anorexia, and diarrhea, were extracted from the Electronic Medical Record (EMR).
Statistical Analysis
Data were summarized using descriptive statistics or contingency tables for the demographic and baseline characteristics, response measurements, and safety measurements. The Kaplan–Meier method was used to graphically demonstrate progression free and OS. Statistical analyses were conducted using R studio (Ver 2024.04.1) and GraphPad Prism software (ver 8.0.1).
Ethical Statement
Although the study was retrospective in nature, an informed consent form (ICF) was obtained from all patients before initial treatment. The study protocol adhered to the principles of Good Clinical Practice and was approved by the Institutional Review Board of Severance Hospital (IRB No. 4–2023-0841). The study complied with the Declaration of Helsinki.
Result
Baseline Characteristics
We screened 51 patients with SCLC treated with lurbinectedin between April 2023 and March 2024. A total of 34 patients were eligible for per-protocol analysis (Figure 1). The median follow-up time was 15.8 months (95% confidence interval [CI] 14.6 to 25.76). The median age of all patients was 68 years (range, 42–80 years) and 26 patients (74%) were male. The majority of patients (97%) had an ECOG PS of 0–1, while 1 patient (3%) had an ECOG PS of 2. At the time of initial diagnosis, only 7 patients (20%) had a limited stage, and 27 patients (80%) were in the extended stage. The most common site of metastasis was the brain (53%), followed by the lungs (44%), liver (21%), and bone (18%). Regarding smoking history, 6 patients (18%) were never smokers, 25 patients (74%) were former smokers, and 3 patients (8%) reported themselves as current smokers. In terms of previous therapy history, 18% of the patients received concurrent chemoradiotherapy (CCRT), and only 9% of the patients underwent surgery. Furthermore, 65% of the patients received two or more lines of chemotherapy, ranging from 2 to 4th lines (Table 1).
Efficacy
Within the study population, the median number of lurbinectedin cycles was four (range: 1–16). Specifically, the median number of cycles was 4.5 for second-line patients and 3 for third-line and beyond patients. No patient with CR was recorded for the best objective response rate (ORR) of the study cohort. Partial remission (PR) was observed in 7 patients (20%), stable disease (SD) in 9 (26%), and progressive disease (PD) in 18 (53%). The ORR and disease control rate (DCR) were 20 and 47%, respectively. We analyzed the ORR and DCR in patients who received lurbinectedin as second- or third-line treatment. The ORR was significantly higher in the second-line group compared to the beyond 2nd line group (15% vs 6%, 95% CI 1.2–39.4, p = 0.03), whereas no statistically significant difference in DCR was found (18% vs 34%, 95% CI 0.07–2.90, p = 0.80) (Table 2).
The Kaplan–Meier curves for PFS and OS are shown in Figure 2A and B. The median PFS was 2.8 months, and the median OS was 3.4 months. The median duration of response (DOR) was significantly longer in patients with a chemotherapy-free interval (CTFI) > 90 days compared to those with a CTFI shorter than 90 days (6.70 months vs 2.00 months; 95% CI 0.75–15.1, p = 0.01).
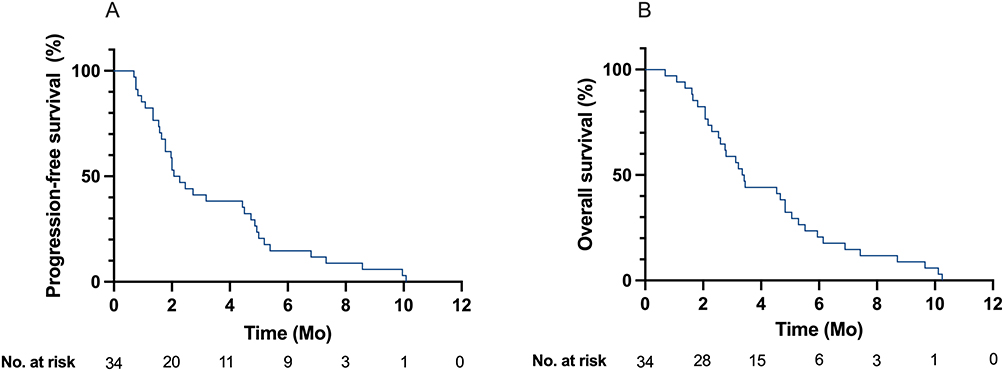 |
Figure 2 Progression-free survival (A) and overall survival (B). Abbreviation: Mo, months. |
Next, we compared PFS and OS according to the lurbinectedin line (Figure 3A and B). The median PFS and OS for 2nd line lurbinectedin was higher compared to the 3rd line lurbinectedin (3.4 vs 2.2 months, 95% CI 0.30–1.15; 4.8 vs 3.3 months, 95% CI 0.29–1.20) although it was not statistically significant. Finally, the PFS of different 2nd line regimens for SCLC from our center was analyzed using retrospective data from patient records. Lurbinectedin was superior to topotecan in terms of median PFS (3.4 vs 1.4 months, 95% CI 0.02–0.81). For irinotecan + platinum (IP) and belotecan, the difference in median PFS was not statistically significant (Figure 4).
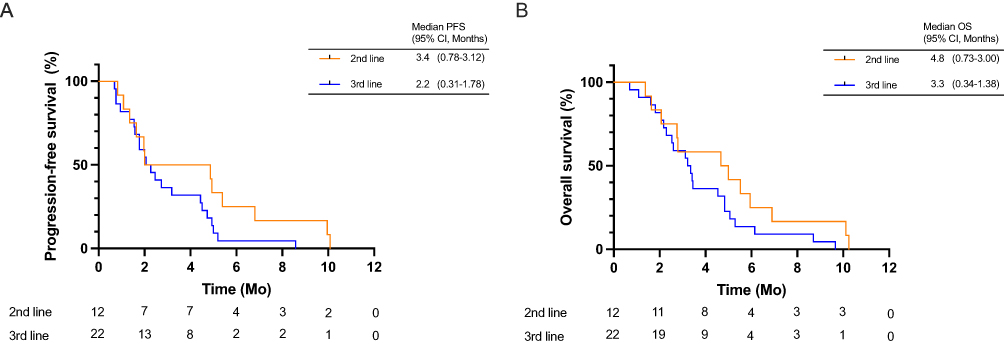 |
Figure 3 Progression-free survival (A) and overall survival (B) according to the line of treatment. Abbreviations: Mo, months; PFS, Progression-free survival; OS, Overall survival. |
 |
Figure 4 Progression-free survival comparison in different 2nd line treatments. IP, Irinotecan plus platinum-containing lines. Abbreviations: PFS, progression-free survival; Mo, months; CI, confidence interval. |
Efficacy in Specific Subgroups
We analyzed the ORR and DCR of lurbinectedin according to the smoking history and CTFI (Table S1). There were no statistically significant differences in the ORR and DCR between never-smokers and smokers. However, patients with a CTFI >90 days showed a significantly better ORR than those with a CTFI <90 days (46% vs 14%, p = 0.027).
Next, we analyzed the PFS and OS in patients treated with lurbinectedin who had a history of smoking and CTFI. PFS and OS were analyzed according to smoking history (Figure S1A and B), and we found that although there was no statistically significant difference in PFS (2.0 vs 3.6, 95% CI 0.23–1.34), OS was significantly better in never smokers than in smokers (3.0 vs 7.3 months, 95% CI 0.17–0.99, HR 0.44, p = 0.03). We then analyzed whether CTFI affected PFS and OS of patients treated with lurbinectedin in a real-world setting. Patients with longer CTFI had better PFS (2.4 vs 1.9 months, 95% CI 0.37–1.65) and OS (4.1 vs 3.3 months, 95% CI 0.59–2.45) compared to patients with shorter CTFI, although it was not statistically significant (Figure S2A and B).
Cox Proportional Hazard Regression Analysis
Next, we performed Cox proportional hazard regression analysis to assess the role of each clinical parameter on OS and PFS. Cox regression analysis identified older age, male sex, extended disease, brain metastasis, liver metastasis, and a CTFI shorter than 90 days as negative factors for OS (Table 3). Cox hazard regression analysis of PFS showed a trend similar to that of OS, while brain metastasis was not statistically significant (Table S2).
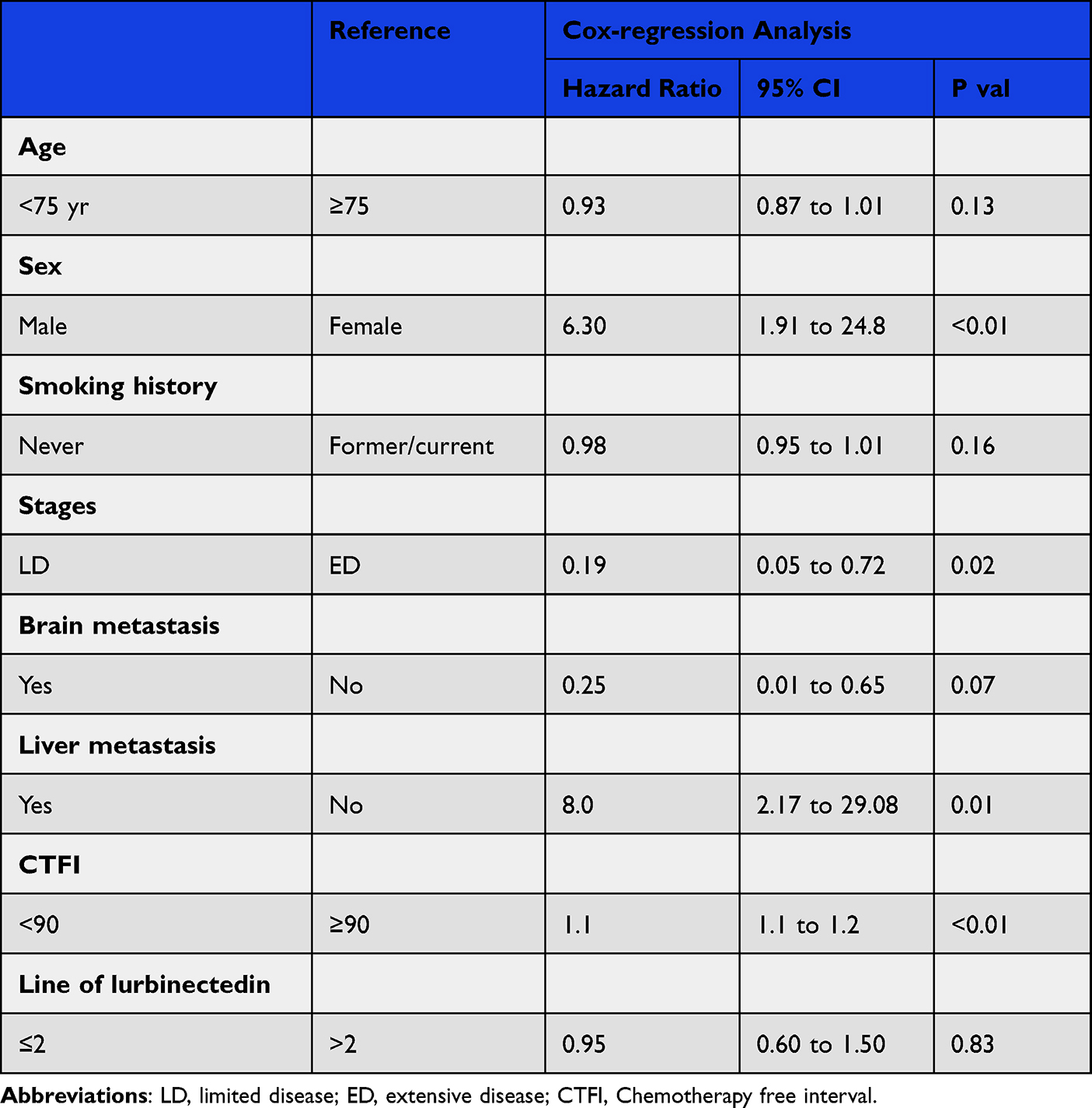 |
Table 3 Cox Proportional Hazard Regression for OS |
Safety
Treatment-related AE of any grade and grade 3–4 events were identified in 58% and 24% of patients, respectively. The most common treatment-related AEs were nausea (53%), anemia (29%), and loss of appetite (24%). General weakness was reported in 18% of patients. The most common grade 3–4 AEs were anemia (9%) and neutropenia (9%). Fifteen percent of patients discontinued lurbinectedin, and 3% discontinued permanently due to treatment-related AEs (Table 4). Other notable grade 3–4 treatment-related AEs included pneumonia (3%) and thrombocytopenia, which required hospitalization (3%).
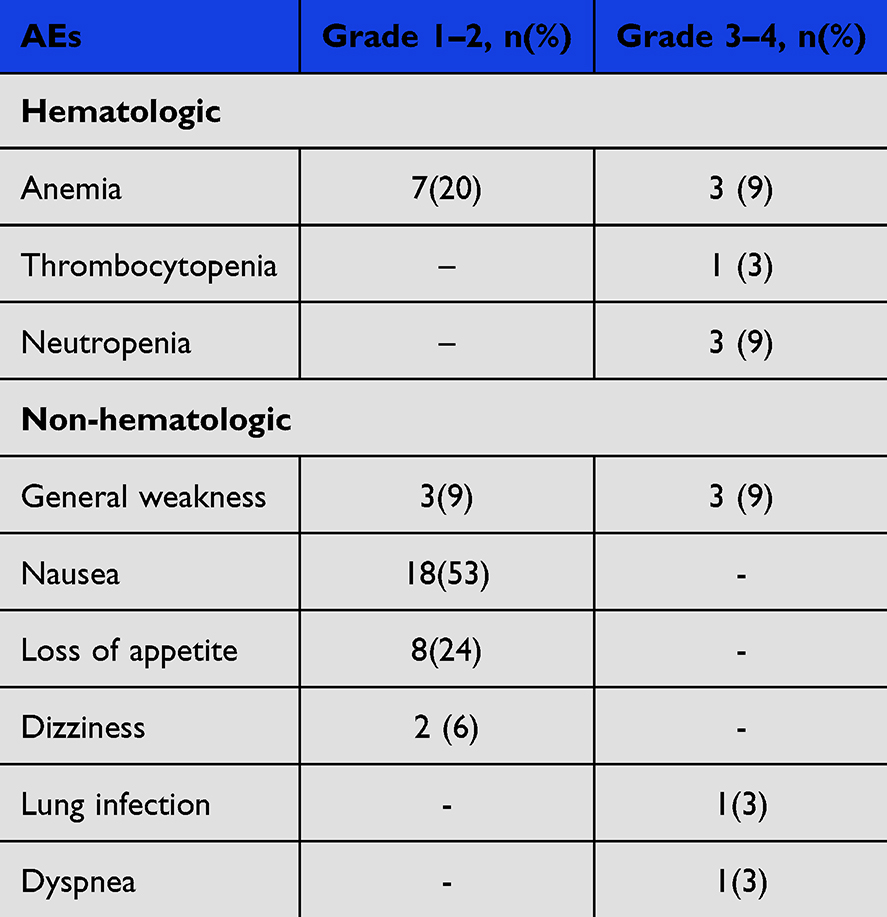 |
Table 4 Most Common Grade ≥ 3 Treatment-Related AEs |
Lastly, we compared G3/G4 AEs with other 2nd line treatments, namely topotecan and belotecan, using previously published data.10 Although cross-trial comparison should be dealt with caution, compared to topotecan and belotecan, lurbinectedin showed lower incidence of anemia, neutropenia, and thrombocytopenia (Figure 5).
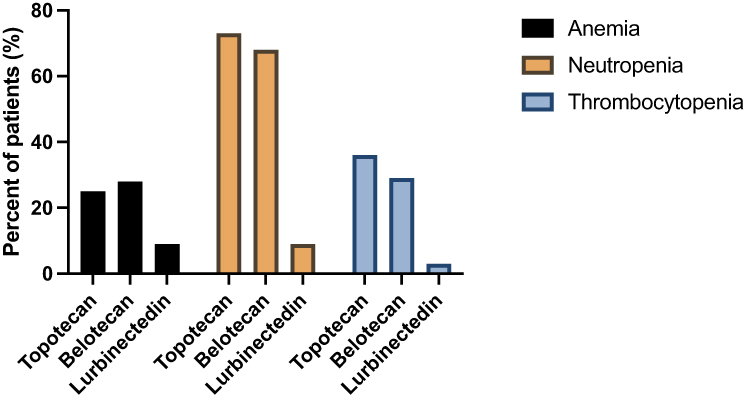 |
Figure 5 G3/4 hematological toxicities of lurbinectedin, topotecan and belotecan. |
Discussion
In this real-world analysis of the efficacy and safety of lurbinectedin in patients with SCLC beyond 2nd line of therapy, the PFS was 2.8 months and OS was 3.4 months, which are comparable to previously reported real-world data.14,15,18 For instance, real-world outcomes have been demonstrated in a large cohort of patients (n = 396) treated with lurbinectedin, with a median PFS of 2.5 months.19 Another real-world study of lurbinectedin found that the median PFS is 1.9 months and OS is 2.1 months.13 Furthermore, the efficacy of lurbinectedin has been reported to be greater in patients with CTFI exceeding 90 days, which aligns with our findings.20 These safety profiles were comparable to those reported in previous studies.
Unlike the single-arm Phase II basket trial that investigated lurbinectedin as a second-line therapy for SCLC, our data demonstrated shorter PFS and OS.21 In the phase II trial, the median PFS and OS were 3.5 and 9.3 months, respectively, with the median number of prior therapy lines being 1 and CNS metastasis present only 4% of the patients. In contrast, our patient cohort had median PFS and OS of 2.8 and 3.4 months, a much higher rate of brain metastasis (53%) and was predominantly on 3rd line therapy. This discrepancy may explain the differences of PFS and OS between phase II trial and the real-world data from our center.
Our study demonstrated that Cox regression analysis revealed that a CTFI shorter than 90 days is a negative prognostic factor for OS. PFS and OS were not statistically different according to the CTFI, which is consistent with previous findings.18 Platinum-sensitive SCLC patients (CTFI > 90) with relapsed disease, platinum re-challenge has been considered a valuable option; however, its usage has been approached with caution due to concerns about cumulative toxicity.22–24 Additionally, the DOR was significantly longer in patients with a CTFI greater than 90 days than in those with a CTFI of <90 days, highlighting its importance in predicting treatment outcomes with lurbinectedin.
Subgroup analysis showed that patients who received lurbinectedin in 2nd line of therapy had a higher median PFS and OS than those who received lurbinectedin beyond 2nd line of therapy, although this was not statistically significant. We compared the efficacy of lurbinectedin in 2nd line therapy with other drugs, namely topotecan, belotecan, and IP chemotherapy. As previously reported, the median PFS was significantly higher with lurbinectedin than with topotecan, as previously reported.25 Furthermore, lurbinectedin showed a lower incidence of G3/4 hematological AEs compared to topotecan and belotecan. Before the recent accelerated approval of lurbinectedin by the FDA, the only available treatment options for patients with relapsed SCLC were topotecan and platinum re-challenge. Our results suggest that lurbinectedin has a survival benefit and favorable hematological safety profile compared to topotecan and belotecan, which is in agreement with a recent study.26
Our study was limited by its retrospective, single-center design, which included a small number of patients and may introduce selection bias. Data for the safety profile were collected based on self-reported documentation of the symptoms. Therefore, our results may not be generalizable to SCLC patients at other institutions. Other limitations of this study include overlapping confidence intervals and cross-trial comparisons. However, to our knowledge, this study is the first to analyze the efficacy and safety profile of lurbinectedin in patients with SCLC in Asia.
In summary, the efficacy and safety profiles of lurbinectedin are comparable to those of other real-world data. Our data suggest that lurbinectedin is a viable treatment option for patients with relapsed SCLC.
Acknowledgments
We express our gratitude to PharmaMar and Boryung for their review and insightful comments. The current study was not sponsored by PhamaMar or Boryung. The abstract of this paper was presented at the ASCO Breakthrough 2024 Conference name ‘Real-world outcomes with lurbinectedin in second-line and beyond for small cell lung cancer in Korea’ as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Journal of Clinical Oncology ‘Real-world outcomes with lurbinectedin in second-line and beyond for small cell lung cancer in Korea’: https://doi.org/10.1200/JCO.2024.42.23_suppl.211
Disclosure
Prof. Dr. Byoung Chul Cho reports personal fees/grants from Champions Oncology, Crown Bioscience, Imagen, PearlRiver Bio GmbH, MOGAM Institute, LG Chem, Oscotec, Interpark Bio Convergence Corp, GIInnovation, GI-Cell, Abion, AbbVie, AstraZeneca, Bayer, Blueprint Medicines, Boehringer Ingelheim, Champions Oncology, CJ bioscience, CJ Blossom Park, Cyrus, Dizal Pharma, Genexine, Janssen, Lilly, MSD, Novartis, Nuvalent, Oncternal, Ono, Regeneron, Dong-A ST, Bridgebio therapeutics, Yuhan, ImmuneOncia, Illumina, Kanaph therapeutics, Therapex, JINTSbio, Hanmi, CHA Bundang Medical Center, Vertical Bio AG, Abion, BeiGene, Novartis, AstraZeneca, Boehringer-Ingelheim, Roche, BMS, CJ, CureLogen, Cyrus therapeutics, Ono, Onegene Biotechnology, Yuhan, Pfizer, Eli Lilly, GI-Cell, Guardant, HK Inno-N, Imnewrun Biosciences Inc., Janssen, Takeda, MSD, Janssen, Medpacto, Blueprint medicines, RandBio, Hanmi, Yonsei University Health System, KANAPH Therapeutic Inc, Bridgebio therapeutics, Cyrus therapeutics, Guardant Health, Oscotec Inc, J INTS Bio, Therapex Co., Ltd, Gliead, Amgen, TheraCanVac Inc, Gencurix Inc, Bridgebio therapeutics, KANAPH Therapeutic Inc, Cyrus therapeutics, Interpark Bio Convergence Corp., J INTS BIO, J INTS BIO; Founder of DAAN Biotherapeutics, outside the submitted work. Dr. Sun Min Lim reports receiving research funding from Yuhan, Johnson & Johnson, and MSD, and serves in a consulting role for AstraZeneca, Boehringer Ingelheim, Lilly, Takeda, J Ints Bio, BMS, MSD, Oscotec, and Therapex. Additionally, Dr. Lim receives research support from AstraZeneca, Boehringer Ingelheim, GSK, Roche, Hengrui, BridgeBio Therapeutics, Oscotec, Daiichi-Sankyo, and Therapex. The authors report no other conflicts of interest in this work.
References
1. Rudin CM, Brambilla E, Faivre-Finn C, Sage J. Small-cell lung cancer. Nat Rev Dis Primers. 2021;7(1):3. doi:10.1038/s41572-020-00235-0
2. Dingemans AC, Fruh M, Ardizzoni A, et al. Small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up(☆). Ann Oncol. 2021;32(7):839–853. doi:10.1016/j.annonc.2021.03.207
3. Jordan EJ, Kim HR, Arcila ME, et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies. Cancer Discov. 2017;7(6):596–609. doi:10.1158/2159-8290.CD-16-1337
4. Nguyen HS, Ho DKN, Nguyen NN, Tran HM, Tam KW, Le NQK. Predicting EGFR mutation status in non-small cell lung cancer using artificial intelligence: a systematic review and meta-analysis. Acad Radiol. 2024;31(2):660–683. doi:10.1016/j.acra.2023.03.040
5. Horn L, Mansfield AS, Szczesna A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. doi:10.1056/NEJMoa1809064
6. Liu SV, Reck M, Mansfield AS, et al. Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133). J Clin Oncol. 2021;39(6):619–630. doi:10.1200/JCO.20.01055
7. Meriggi F. Second-line treatment options for small-cell lung cancer: a light at the end of the tunnel. Cancers. 2024;16(2):255. doi:10.3390/cancers16020255
8. Ellis PM, Swaminath A, Pond GR. Patterns of relapse in small cell lung cancer: competing risks of thoracic versus CNS relapse. Curr Oncol. 2021;28(4):2778–2788. doi:10.3390/curroncol28040243
9. Baize N, Monnet I, Greillier L, et al. Carboplatin plus etoposide versus topotecan as second-line treatment for patients with sensitive relapsed small-cell lung cancer: an open-label, multicentre, randomised, Phase 3 trial. Lancet Oncol. 2020;21(9):1224–1233. doi:10.1016/S1470-2045(20)30461-7
10. Kim C, Sohn JH, Kim JH, et al. Phase II study of topotecan and etoposide as second-line treatment in chemotherapy-refractory small-cell lung cancer. Cancer Res Treat. 2002;34(5):334–338. doi:10.4143/crt.2002.34.5.334
11. Petrelli F, Ghidini A, Luciani A. Topotecan or other agents as second-line therapy for relapsed small-cell lung cancer: a meta-analysis of randomized studies. Mol Clin Oncol. 2021;15(4):218. doi:10.3892/mco.2021.2383
12. Zhao L, Zhao Z, Yan X, Hu X, Feng J, Yu S. Comparison of efficacy and safety of second-line treatment options for advanced small-cell lung cancer: a retrospective analysis. Technol Cancer Res Treat. 2024;23:15330338241227055. doi:10.1177/15330338241227055
13. Toublanc AC, Guecamburu M, Veillon R, Rosellini P, Girodet PO, Zysman M. Second-line lurbinectedin as a new treatment option for small-cell lung cancer: preliminary results in real-clinical practice. Thorac Cancer. 2022;13(15):2248–2252. doi:10.1111/1759-7714.14464
14. Dumoulin DW, Cantini L, Cornelissen R, et al. Lurbinectedin shows clinical activity and immune-modulatory functions in patients with pre-treated small cell lung cancer and malignant pleural mesothelioma. Eur J Cancer. 2022;172:357–366. doi:10.1016/j.ejca.2022.06.020
15. Wasifuddin M, Ilerhunmwuwa NP, Becerra H, et al. Review of real-world experience with lurbinectedin in relapsed/refractory small cell lung cancer. J Chemother. 2024:1–6. doi:10.1080/1120009X.2024.2302736
16. Alexander M, Rogers J, Parakh S, et al. Lurbinectedin in small cell lung cancer: real-world experience of a multicentre national early access programme. Intern Med J. 2024;54(7):1087–1096. doi:10.1111/imj.16348
17. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
18. Desai A, Smith CJ, Ashara Y, et al. Real-world outcomes with lurbinectedin in second-line setting and beyond for extensive stage small cell lung cancer. Clin Lung Cancer. 2023;24(8):689–695e1. doi:10.1016/j.cllc.2023.09.001
19. Estrin A, Wang X, Boccuti A, et al. Real-world (RW) outcomes of second-line (2L) small cell lung cancer (SCLC) patients treated with lurbinectedin.
20. Subbiah V, Paz-Ares L, Besse B, et al. Antitumor activity of lurbinectedin in second-line small cell lung cancer patients who are candidates for re-challenge with the first-line treatment. Lung Cancer. 2020;150:90–96. doi:10.1016/j.lungcan.2020.10.003
21. Trigo J, Subbiah V, Besse B, et al. Lurbinectedin as second-line treatment for patients with small-cell lung cancer: a single-arm, open-label, Phase 2 basket trial. Lancet Oncol. 2020;21(5):645–654. doi:10.1016/S1470-2045(20)30068-1
22. Naito Y, Yamada K, Imamura Y, et al. Rechallenge treatment with a platinum-based regimen in patients with sensitive relapsed small-cell lung cancer. Med Oncol. 2018;35(5):61. doi:10.1007/s12032-018-1123-6
23. Shiozawa T, Sekine I, Aida Y, et al. Rechallenge with first-line platinum chemotherapy for sensitive-relapsed small-cell lung cancer. Case Rep Oncol. 2018;11(3):622–632. doi:10.1159/000492780
24. Rossi A. Relapsed small-cell lung cancer: platinum re-challenge or not. J Thorac Dis. 2016;8(9):2360–2364. doi:10.21037/jtd.2016.09.28
25. Hanvesakul R, Rengarajan B, Naveh N, et al. Indirect treatment comparison of lurbinectedin versus other second-line treatments for small-cell lung cancer. J Comp Eff Res. 2023;12(5):e220098. doi:10.57264/cer-2022-0098
26. Peters S, Trigo J, Besse B, et al. Lurbinectedin in patients with small cell lung cancer with chemotherapy-free interval >/=30 days and without central nervous metastases. Lung Cancer. 2024;188:107448. doi:10.1016/j.lungcan.2023.107448
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.