Back to Journals » OncoTargets and Therapy » Volume 18
Real-World Experience of Niraparib as Maintenance Therapy in Patients with Newly Diagnosed Advanced Ovarian Cancer: A Single-Center Retrospective Study
Authors Liu W, Zhang L, Wu H, Chen Y, Ma Y, Bao L, Fu X, Wang K
Received 20 May 2025
Accepted for publication 15 September 2025
Published 29 October 2025 Volume 2025:18 Pages 1201—1208
DOI https://doi.org/10.2147/OTT.S528382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Wenxin Liu,1,2 Li Zhang,1,2 Huijuan Wu,1,2 Ying Chen,1,2 Yaomei Ma,1,2 Lewen Bao,1,2 Xin Fu,1,2 Ke Wang1,2
1Department of Gynecological Oncology, Tianjin Medical University Cancer Institute & Hospital, Tianjin, People’s Republic of China; 2National Clinical Research Center for Cancer, State Key Laboratory of Cancer Prevention and Therapy of Tianjin, Tianjin’s Clinical Research Center for Cancer, Tianjin, People’s Republic of China
Correspondence: Ke Wang, Department of Gynecological Oncology, Tianjin Medical University Cancer Institute & Hospital, Tianjin, 300060, People’s Republic of China, Email [email protected]
Objective: This study aimed to evaluate the efficacy and safety of niraparib as a maintenance treatment for newly diagnosed advanced ovarian cancer in a real-world setting.
Methods: This retrospective observational study included patients with histologically confirmed epithelial ovarian cancer, primary peritoneal or fallopian tube cancer who received niraparib as first-line maintenance therapy at Tianjin Cancer Hospital between January 2021 and January 2023. Clinicopathological characteristics and treatment outcomes were extracted from medical records. The efficacy of niraparib was evaluated by progression-free survival (PFS), and safety was assessed using the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Results: A total of 102 patients were enrolled in this study. After a median follow-up of 21.4 months (IQR 20.4– 22.5 months), the median PFS was 25.7 months in the overall population, not reached in the BRCA mutation group, and 23.0 months in the wild-type group. A total of fifty patients with a known status of homologous recombination deficiency (HRD) were observed. The median PFS was not reached and 23.0 months in the homologous recombination deficiency and proficient groups, respectively. In the BRCA wild-type group, patients who received more than six cycles of platinum-based chemotherapy had a better prognosis. Furthermore, 20.6% of patients experienced grade 3 or higher treatment-emergent adverse events, while 39.2% experienced treatment interruption, 37.3% underwent dose reduction, and 6.9% discontinued treatment. No new safety signals were observed.
Conclusion: In the real-world setting, the use of niraparib as a maintenance treatment for newly diagnosed advanced ovarian cancer has been shown to be effective and well tolerated, which is consistent with the results of previous randomized Phase III trials.
Keywords: ovarian cancer, niraparib, real-word, maintenance
Introduction
Epithelial ovarian cancer, which includes ovarian cancer, fallopian tube cancer, and primary peritoneal cancer, is one of the most common tumors of the female reproductive organs, with the incidence rate that ranks first and the mortality rate that ranks second.1 Owing to the occult onset of the disease and the difficulty in early detection, approximately 3/4 of the patients were already in an advanced stage at the time of diagnosis. Once advanced, treatment outcomes are consistently unsatisfactory.2
The advent of maintenance therapy, represented by poly (adenosine diphosphate-ribose) polymerase inhibitors (PARPi), has revolutionized the treatment paradigm of ovarian cancer, transforming it into a novel model where adjuvant chemotherapy follows surgery, succeeded by maintenance therapy. Based on the SOLO1 trial, the FDA approved olaparib in 2018 for the maintenance treatment of advanced ovarian cancer patients who have achieved a complete or partial response to first-line platinum-based chemotherapy. However, this approval was limited to patients with germline or somatic BRCA mutations.3 Subsequently, the PRIMA and PRIME trials demonstrated a significant progression-free survival (PFS) benefit of niraparib as a first-line maintenance treatment, regardless of biomarker status. Consequently, niraparib was approved by both the FDA and NMPA for all comers.4,5 Notably, unlike PRIMA, PRIME only enrolled Chinese patients and included a broader and more representative patient population, including patients with stage III disease who achieved R0 resection during primary debulking surgery.5
However, randomized controlled clinical trials have strict inclusion and exclusion criteria whereas the status and treatment of patients in the real world are complex and diverse.6 Several retrospective real-world studies have been published and are only dominated by southern populations.7–10 Thus, the objective of this study was to evaluate the efficacy and safety of niraparib as a maintenance treatment for newly diagnosed advanced ovarian cancer in a real-world setting, particularly in northern populations, which could also be an important supplement to randomized controlled studies.
Materials and Methods
Study Design and Participants
This was a single-center retrospective observational study. Patients diagnosed with histologically confirmed epithelial ovarian cancer, fallopian tube cancer, and primary peritoneal cancer who received niraparib as a first-line maintenance treatment at Tianjin Cancer Hospital between January 2021 and January 2023 were eligible for study enrollment. Patients with missing clinical data due to loss or refusal to follow-up were excluded. Clinical data were obtained from the Information System of Tianjin Cancer Hospital (including the HIS and PACS systems), and the following information was collected: a) demographic data: age, BRCA and homologous recombination deficiency (HRD) status; b) surgery-related data: postoperative status of cytoreductive surgery (R0/R1/R2), postoperative pathological diagnosis, and International Federation of Gynecology and Obstetrics (FIGO) stage; c) postoperative treatment data, including chemotherapy regimen and cycle, CA-125 elimination rate constant K (KELIM) score, and the best response to platinum-based chemotherapy. Maintenance treatment data including CT/MRI/B-ultrasound results before maintenance, initiation time of maintence, initial and stable dose of niraparib, adverse events during treatment, reasons for treatment interruption and reduction, as well as the time of disease progression. Missing information was supplemented by telephone follow-ups with patients and their families.
Outcome Evaluation
Effectiveness was evaluated using PFS, which is defined as the time from the initial maintenance therapy to the date of disease progression, death from any cause, or study cutoff. The safety was evaluated using Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Clinical and objective radiology assessments were performed according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1.
Statistical Analysis
SPSS software (version 25.0) was used for statistical analysis. Categorical variables are expressed as percentages, and continuous variables are expressed as median values and ranges. Survival analysis was performed using the Kaplan-Meier method and the Log rank test. The safety data were summarized using descriptive statistics (numbers and percentages). Univariate analysis was performed using the Cox proportional hazards regression model to identify the possible risk factors for the BRCA wild-type population. Hazard ratios (HR) and 95% confidence intervals (CI) were reported, with a 2-tailed P value < 0.05 considered to indicate significant differences.
Results
Demographic and Clinical Characteristics
In total, 109 eligible patients were screened and seven were excluded due to missing baseline data. Ultimately, 102 patients were included in this study (Supplementary Figure S1). The cutoff date was March 1, 2024. Patient demographics and baseline characteristics are summarized in Table 1.
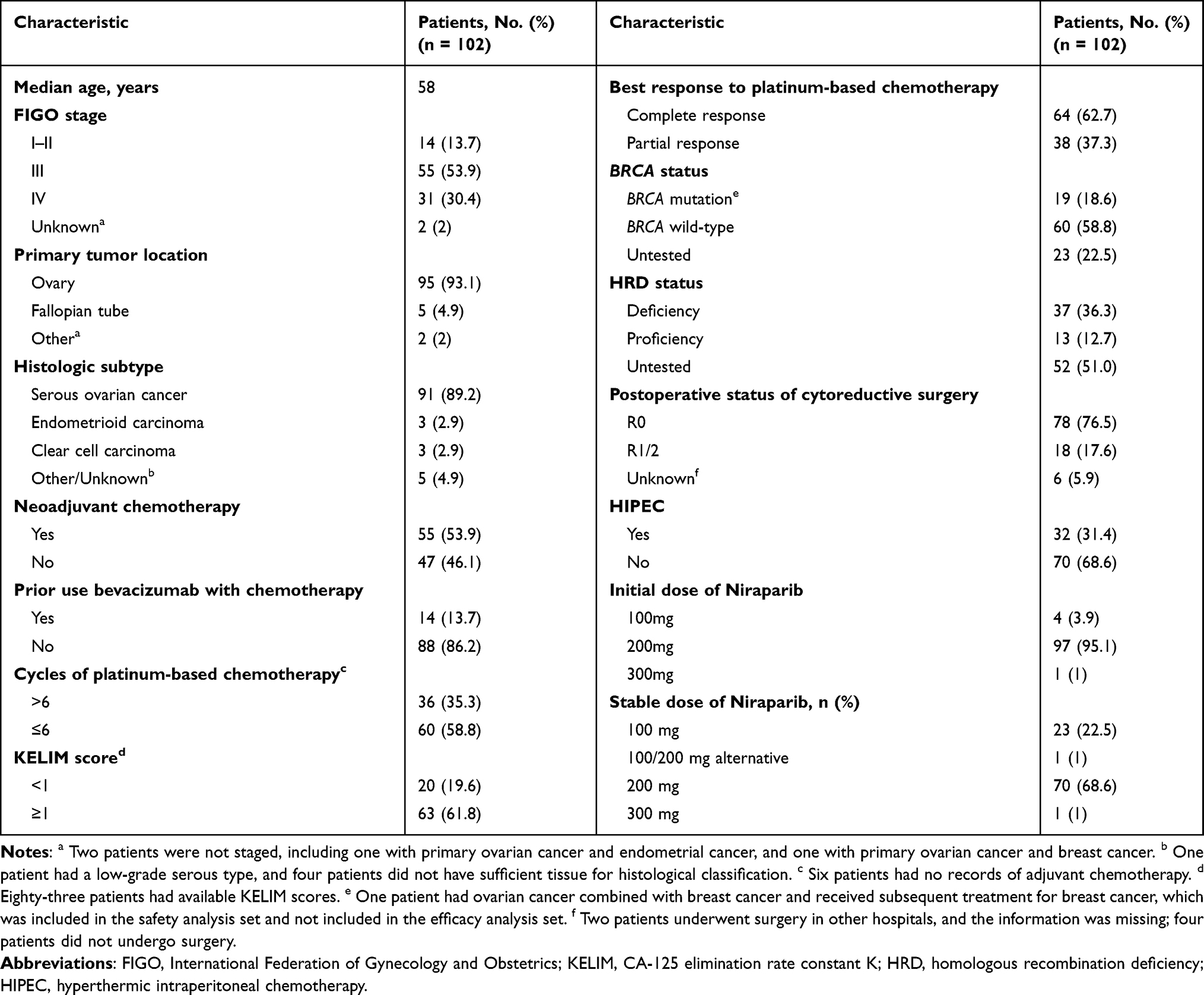 |
Table 1 Baseline Demographics and Clinical Characteristics |
The median age of the patients was 58 years. Among them, 86 patients (84.3%) had FIGO stage III/IV, 55 patients (53.9%) received neoadjuvant chemotherapy, 18 patients (17.6%) achieved R1/R2 status after cytoreductive surgery, and 38 patients (37.3%) had a partial response to platinum-based chemotherapy. Among the entire population, 19 patients (18.6%) had a BRCA mutation and 60 patients (58.8%) had BRCA wild-type, whereas the remaining 23 patients (22.5%) were not tested for BRCA status. Similarly, 37 patients (36.3%) were HRD-positive and 13 patients (12.7%) were HRD-negative, whereas the remaining 52 patients (51%) were not tested for HRD status. Of these, 13.7% received chemotherapy with bevacizumab (either neoadjuvant or adjuvant). Hyperthermic intraperitoneal chemotherapy (HIPEC) was administered to 31.4% of the patients. The number of platinum-based chemotherapy cycles these patients had received ranged from 4 to 12, with a median of 6.
Efficacy
As of the data cutoff, the median follow-up time for PFS was 21.4 months (IQR 20.4–22.5 months), and the data maturity was 39.2%. In the overall population, the median PFS was 25.7 months, and the probability of PFS at 24 months was 51.87% (Figure 1A). The median PFS was not reached (95% CI, not estimable (NE)-NE), 23 months (95% CI, 15.16–30.84), and 15.5 months (95% CI, 4.9–26.10) in the BRCA mutation, BRCA wild-type, and BRCA untested groups, respectively, while the probabilities of PFS at 24 months were 85.6%, 46.2%, and 40.7%, respectively (Figure 1B). The median PFS were not reached (95% CI, NE-NE) and 23 months (95% CI, 2.62–43.38) in the homologous recombination deficiency and proficient groups, respectively (Figure 1C). Further details are provided in Table 2.
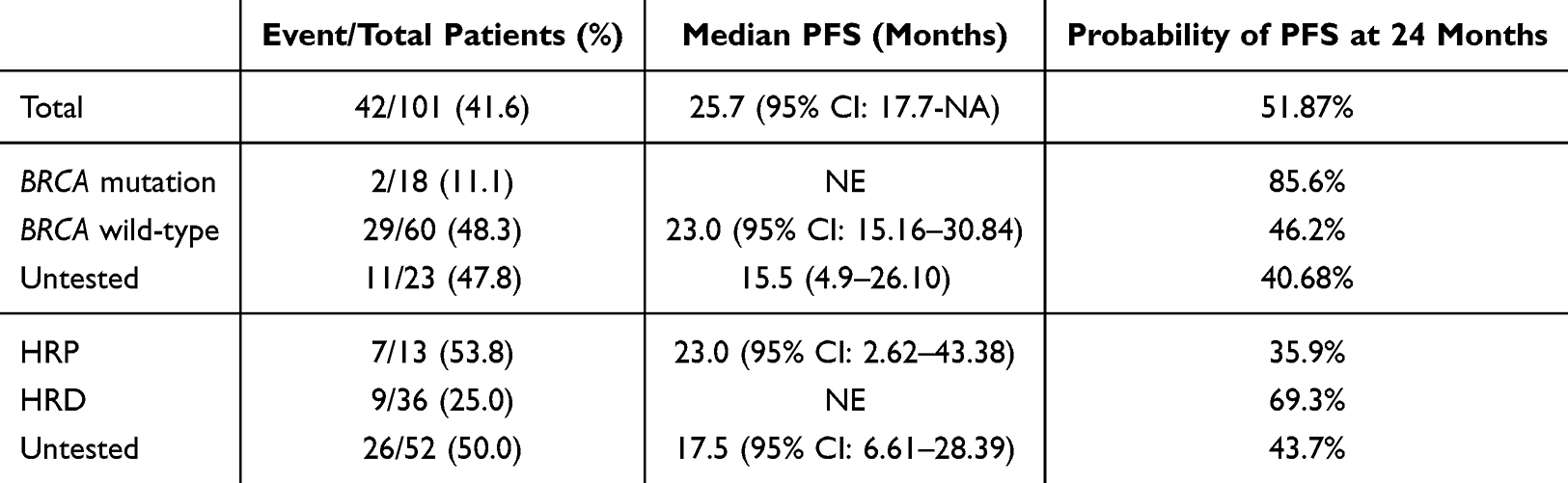 |
Table 2 PFS by the Intention-to-Treat Population, BRCA Statuses and HRD Statuses |
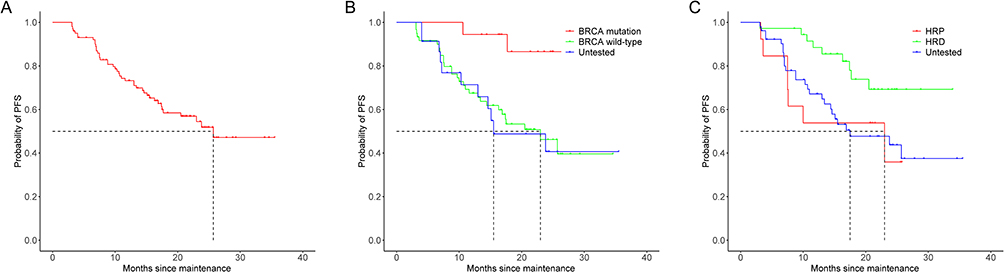 |
Figure 1 Kaplan-Meier PFS curves. (A) The intention-to-treat population; (B) The population with different BRCA statuses; (C) The population with different HRD statuses. |
Univariate Analysis of BRCA Wild-Type Population
Patients with BRCA wild-type usually have a poorer prognosis.11 To evaluate the clinical factors affecting their prognosis, six clinical factors, including FIGO staging, KELIM score, postoperative status of cytoreductive surgery, number of platinum-based chemotherapy cycles, best response to platinum-based chemotherapy, and HIPEC were included in the univariate Cox regression analysis. The results showed that the number of platinum-based chemotherapy cycles may be an independent prognostic factor in BRCA wild-type population (P = 0.0128). Further details are provided in Table 3.
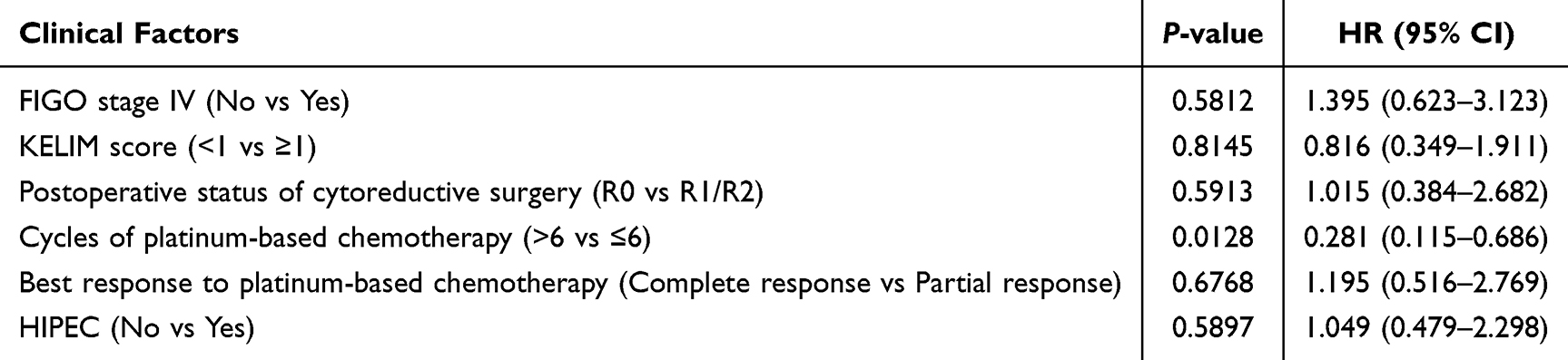 |
Table 3 Univariate Analysis of BRCA Wild-Type Population |
Safety
During treatment with niraparib, 80 patients (78.4%) experienced treatment-emergent adverse events (TEAEs) of any grade and 21 patients (20.6%) experienced at least one grade 3 or higher TEAE. Forty patients (39.2%) experienced treatment interruption, of which 27 were caused by hematological TEAEs. Thirty-eight patients (37.3%) experienced dose reduction, of which 25 were caused by hematological TEAEs. Specifically, fourteen patients successfully escalated to the initial dose after demonstrating tolerance for at least one cycle following a dose reduction without experiencing any treatment interruptions or dose reductions. Seven patients (6.9%) discontinued the treatment because of TEAEs. The most common hematological TEAEs during treatment were anemia and decreased platelet count, decreased neutrophil count, and decreased white blood cell count. The most common non-hematological TEAEs were nausea, decreased appetite, and fatigue. No new safety signals were observed. Refer to Figure 2, Table 4, and Supplementary Table S1 for details.
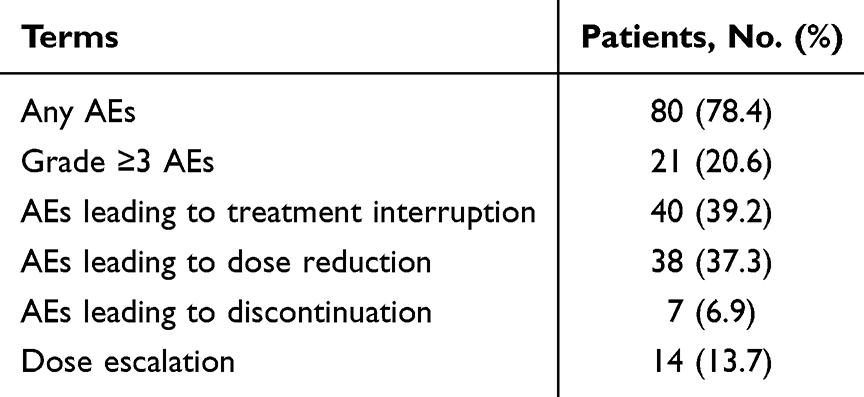 |
Table 4 Safety |
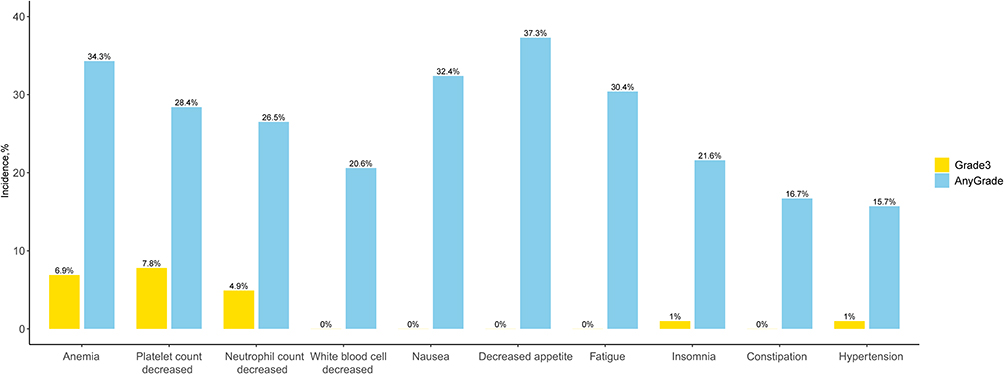 |
Figure 2 Incidence rates of any grade and grade ≥3 treatment-emergent adverse events. |
Correlations of TEAEs and PFS in Patients Treated with Different Doses and Initiation Time
Among patients with an initial dose of 200 mg, the median PFS was 16.9 months in the group with dose reduction due to TEAE and not reached in the group without dose reduction, respectively, with no statistical difference between the two groups (P=0.0539). Furthermore, for the initiation time of maintenance therapy, which is defined as the interval from the end of chemotherapy to the start of niraparib maintenance treatment, the median PFS was 23.8 months in the <12 weeks group and NE in the ≥12 weeks group, with no statistical significance (P=0.4059). Further details are provided in Supplementary Table S2.
Discussion
This was a single-center real-world study, particularly in northern populations, demonstrating the effectiveness and tolerability of niraparib as a first-line maintenance therapy for ovarian cancer. For patients with BRCA wild-type, the number of platinum-based chemotherapy cycles was an independent factor associated with longer PFS; however, this finding still needs to be further confirmed with long-term follow-up and a large sample size.
Previous studies have confirmed the effectiveness of PARPi in patients with BRCA mutations, who are the most sensitive to PARPi. This is despite variations in study design and populations, including olaparib in SOLO-1, niraparib in PRIMA and PRIME, rucaparib in ATHENA-MONO, and senaparib in FLEAMS.3–5,12,13 Although the data were retrospective and limited in number, this study demonstrated improved outcomes in the BRCA mutation population compared to the BRCA wild-type population, with a median follow-up of 21.4 months and a median PFS that has not yet been reached. This finding is consistent with the results of previous studies.3–5,12,13
For patients with BRCA wild-type, who constitutes approximately 75% of ovarian cancer, the median PFS of PARPi as first-line maintenance treatment was 19.3 months in the PRIME study and remained not reached after a median follow-up of 22.3 months in the FLEAMS study.5,13 In this study, 60 patients with BRCA wild-type, with a median PFS of 23.0 months, also demonstrated a favorable effect of niraparib maintenance therapy. As patients with BRCA wild-type usually have a poor prognosis,11 a univariate analysis was conducted to explore the prognostic factors for this group. Our study identified the number of platinum-based chemotherapy cycles (>6 vs ≤6) as an independent prognostic factor (P = 0.0128), indicating that in clinical practice, completing full-course chemotherapy should be given greater emphasis in patients with BRCA wild-type.
Currently, there are no approved commercial HRD assays in China, and those used in clinical practice are diverse and mostly laboratory-developed. The BGI HRD assay was used in the PRIME study, and the results demonstrated that first-line maintenance with niraparib significantly extended PFS in both the homologous recombination-positive and proficient groups.5 The TruSight Oncology 500 HRD assay was used in the FLEAMS study, and exploratory analysis also indicated that maintenance with senaparib showed a PFS benefit trend regardless of HRD status, although the data were retrospective.13 In this study, fifty patients underwent various HRD assays to determine HRD status, and the median PFS were not reached and 23.0 months in the homologous recombination-positive and proficient groups, respectively. This retrospective real-world study also confirmed that patients in the HRD group had better clinical outcomes. At the same time, although the sample size was limited, the median PFS in the HRP group was 23 months, while, without maintenance, the median PFS ranged from 5.4 months to 19.5 months in previous randomized phase III trials.4,5,12,13 Therefore, maintenance therapy is crucial for this population.
Overall survival (OS) is a key goal of all anticancer treatments. In the phase III PRIMA trial, it was observed that for newly diagnosed advanced ovarian cancer, niraparib maintenance therapy showed no difference in OS compared with placebo.14 However, it is important to note that all patients enrolled in PRIMA were at high risk of disease progression or death, including those with stage III disease (with residual disease after primary debulking surgery), those with stage IV disease, and those who received neoadjuvant chemotherapy. Second, OS was a secondary endpoint of PRIMA, and the results were susceptible to being affected by subsequent confounding factors, such as subsequent PARPi therapy, subsequent new drug treatment and re-cytoreductive surgery.14 PFS, as the primary endpoint, holds significant importance. In PRIMA, patients who received niraparib as first-line maintenance therapy had significantly longer PFS than those who received placebo both in patients with HRD (24.5 months vs 11.2 months; hazard ratio, 0.51) and those with HRP (8.4 months vs 5.4 months; hazard ratio, 0.67), indicating a 49% and 33% reduction in the risk of disease progression or recurrence, respectively.14 This confirms the clinical value of niraparib as first-line maintenance therapy. Consistent with PRIMA, this study demonstrates that niraparib shows favorable efficacy in both patients with HRD and those with HRP, and notably, the efficacy is more pronounced in the HRD group. Regarding OS, due to insufficient OS data maturity, long-term follow-up is still required to analyze the factors influencing the clinical benefit of PARPi. In real-world settings, although OS is also susceptible to the impact of subsequent treatments, we will continue follow-up to evaluate the significance of niraparib as first-line maintenance on the overall survival of patients with newly diagnosed advanced ovarian cancer.
The safety results showed that the individualized starting dose regimen, which is based on body weight and platelet count, had better tolerance in Chinese patients, with a treatment interruption rate of 39.2%, dose reduction rate of 37.3%, and treatment discontinuation rate of 6.9%. The reasons for treatment interruption and reduction were hematological TEAEs (mostly grade ≥3) and non-hematological TEAEs (mainly grade 1 or 2). We noted that, after experiencing dose reduction during PARPi treatment, fourteen patients demonstrated good tolerance in subsequent treatment cycles, successfully re-escalating to the initial dose and maintaining stability. This provides a new approach for patients with stable symptoms after a dose reduction.
To our knowledge, this is the first study to evaluate the efficacy and safety of niraparib as first-line maintenance therapy for ovarian cancer, particularly in northern populations. This study had some limitations. First, the clinical data were retrospectively collected through systematic records and telephone follow-up. Therefore, the incompleteness of data collection may have led to bias, especially the completeness of TEAEs. Second, this is single-center data, which also needs to be confirmed with multicenter data from northern China. Finally, the data maturity was still not sufficiently high, and a longer follow-up time is needed. The overall survival data should be collected in future studies.
Maintenance therapy with niraparib for newly diagnosed advanced ovarian cancer is effective and well-tolerated, without any safety concerns. For the BRCA wild-type population, the completion of full-course chemotherapy should be given greater emphasis, and a few more cycles of chemotherapy should be feasible.
Conclusion
This real-world study confirmed the effectiveness and tolerability of niraparib as a maintenance treatment for newly diagnosed advanced ovarian cancer, particularly in patients in northern China.
Ethical Approval
The study was conducted strictly following the guiding principles of the Declaration of Helsinki. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because informed consent was waived by competent authorities due to the anonymized nature of patient data and the retrospective design of the study. This study was approved by the Ethics Committee of Tianjin Cancer Hospital (approval number: bc20241252).
Acknowledgments
We would like to thank all the patients included in this retrospective study. The abstract of this paper was presented at the ESMO Asia Congress 2023 (Singapore; December 1–3, 2023) as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Annals of Oncology: [https://doi.org/10.1016/j.annonc.2023.10.436].
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could influence the work reported in this study.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Lheureux S, Gourley C, Vergote I, Oza AM. Epithelial ovarian cancer. Lancet. 2019;393(10177):1240–1253. doi:10.1016/S0140-6736(18)32552-2
3. Moore K, Colombo N, Scambia G, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2018;379:2495–2505. doi:10.1056/NEJMoa1810858
4. González-Martín A, Pothuri B, Vergote I, et al. Niraparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2019;381:2391–2402. doi:10.1056/NEJMoa1910962
5. Li N, Zhu J, Yin R, et al. Treatment with niraparib maintenance therapy in patients with newly diagnosed advanced ovarian cancer: a phase 3 randomized clinical trial. JAMA Oncol. 2023;9:1230–1237. doi:10.1001/jamaoncol.2023.2283
6. Blonde L, Khunti K, Harris SB, Meizinger C, Skolnik NS. Interpretation and impact of real-world clinical data for the practicing clinician. Adv Ther. 2018;35(11):1763–1774. doi:10.1007/s12325-018-0805-y
7. Li J, Yang J, Shou H, et al. Real-world outcomes of niraparib treatment in patients with ovarian cancer: a multicenter non-interventional study in China. Cancer Commun. 2023;43:1–4. doi:10.1002/cac2.12418
8. Zhao M, Qiu S, Wu X, et al. Efficacy and safety of niraparib as first-line maintenance treatment for patients with advanced ovarian cancer: real-world data from a multicenter study in China. Target Oncol. 2023;18:869–883. doi:10.1007/s11523-023-00999-x
9. Chen J, Zhang M, Kemin L, et al. PARP inhibitor maintenance treatment for newly diagnosed ovarian cancer patients: a real-world study from China. Front Oncol. 2024;14:1336616. doi:10.3389/fonc.2024.1336616
10. Wang D, Shi X, Pei J, et al. Olaparib and niraparib as maintenance therapy in patients with newly diagnosed and platinum-sensitive recurrent ovarian cancer: a single-center study in China. Chin Med J. 2024;52:1–8. doi:10.1142/S0192415X24500010
11. Paik ES, Heo EJ, Choi CH, et al. Prevalence and clinical characterization of BRCA1 and BRCA2 mutations in Korean patients with epithelial ovarian cancer. Cancer Sci. 2021;112:5055–5067. doi:10.1111/cas.15166
12. Monk BJ, Parkinson C, Lim MC, et al. A randomized, phase III trial to evaluate rucaparib monotherapy as maintenance treatment in patients with newly diagnosed ovarian cancer (ATHENA-MONO/GOG-3020/ENGOT-ov45). J Clin Oncol. 2022;40:3952–3964. doi:10.1200/JCO.22.01003
13. Xiaohua W, Liu J, Wang J, et al. Senaparib as first-line maintenance therapy in advanced ovarian cancer: a randomized phase 3 trial. Nat Med. 2024;30(6):1612–1621. doi:10.1038/s41591-024-03003-9
14. Monk BJ, Barretina-Ginesta MP, Pothuri B, et al. Niraparib first-line maintenance therapy in patients with newly diagnosed advanced ovarian cancer: final overall survival results from the PRIMA/ENGOT-OV26/GOG-3012 trial. Ann Oncol. 2024;35:981–992. doi:10.1016/j.annonc.2024.08.2241
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.