Back to Journals » Therapeutics and Clinical Risk Management » Volume 19
Real-World Evaluation of a Pharmacoinvasive Strategy for STEMI in Latin America: A Cost-Effective Approach with Short-Term Benefits
Authors Arias-Mendoza A, Ortega-Hernández JA ![]() , Araiza-Garaygordobil D, González-Pacheco H, Martínez-García M, Hernández-Lemus E
, Araiza-Garaygordobil D, González-Pacheco H, Martínez-García M, Hernández-Lemus E ![]() , Gopar-Nieto R, Sandoval-Aguilar TT, Sierra-Lara Martinez D, Mendoza-García S, Altamirano-Castillo A, Briseño-de-la-Cruz JL, Ortega-Hernández MA, Soliz-Uriona LA, Gaspar-Hernández J
, Gopar-Nieto R, Sandoval-Aguilar TT, Sierra-Lara Martinez D, Mendoza-García S, Altamirano-Castillo A, Briseño-de-la-Cruz JL, Ortega-Hernández MA, Soliz-Uriona LA, Gaspar-Hernández J
Received 23 August 2023
Accepted for publication 30 October 2023
Published 10 November 2023 Volume 2023:19 Pages 903—911
DOI https://doi.org/10.2147/TCRM.S432683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Alexandra Arias-Mendoza,1 Jorge A Ortega-Hernández,1 Diego Araiza-Garaygordobil,1 Héctor González-Pacheco,1 Mireya Martínez-García,2 Enrique Hernández-Lemus,3 Rodrigo Gopar-Nieto,1 Tomás Tadeo Sandoval-Aguilar,1 Daniel Sierra-Lara Martinez,1 Salvador Mendoza-García,1 Alfredo Altamirano-Castillo,1 José Luis Briseño-de-la-Cruz,1 Midori Alondra Ortega-Hernández,4 Luis Alejandro Soliz-Uriona,1 Jorge Gaspar-Hernández5
1Coronary Care Unit, Instituto Nacional de Cardiología Ignacio Chávez, Mexico City, Mexico; 2Immunology, Instituto Nacional de Cardiología Ignacio Chávez, Mexico City, Mexico; 3Computational Genomics, Instituto Nacional de Medicina Genómica, Mexico City, Mexico; 4Facultad de Ciencias, Universidad Nacional Autónoma de México, Mexico City, Mexico; 5Instituto Nacional de Cardiología Ignacio Chávez, Mexico City, Mexico
Correspondence: Alexandra Arias-Mendoza, Coronary Care Unit, Instituto Nacional de Cardiología Ignacio Chávez, Juan Badiano, Sección XVI, 14080, Tlalpan, Mexico City, Mexico, Tel +52-55- 54852219, Fax +52-55-54852219, Email [email protected]
Purpose: While pharmacoinvasive strategy (PI) is a safe and effective approach whenever access to primary percutaneous intervention (pPCI) is limited, data on each strategy’s economic cost and impact on in-hospital stay are scarce. The objective is to compare the cost-effectiveness of a PI with that of pPCI for the treatment of ST-elevation myocardial infarction (STEMI) in a Latin-American country.
Patients and Methods: A total of 1747 patients were included, of whom 470 (26.9%) received PI, 433 (24.7%) pPCI, and 844 (48.3%) NR. The study’s primary outcome was the incremental cost-effectiveness ratio (ICER) for PI compared with those for pPCI and non-reperfused (NR), calculated for 30-day major cardiovascular events (MACE), 30-day mortality, and length of stay.
Results: For PI, the ICER estimates for MACE showed a decrease of $– 35.81/per 1% (95 confidence interval, – 114.73 to 64.81) compared with pPCI and a decrease of $– 271.60/per 1% (95% CI, – 1086.10 to – 144.93) compared with NR. Also, in mortality, PI had an ICER decrease of $– 129.50 (95% CI, – 810.57, 455.06) compared to pPCI and $– 165.27 (– 224.06, – 123.52) with NR. Finally, length of stay had an ICER reduction of − 765.99 (− 4020.68, 3141.65) and − 283.40 (− 304.95, − 252.76) compared to pPCI and NR, respectively.
Conclusion: The findings of this study suggest that PI may be a more efficient treatment approach for STEMI in regions where access to pPCI is limited or where patient and system delays are expected.
Keywords: pharmacoinvasive, cost-effectiveness, STEMI, Latin-America
Introduction
Timely reperfusion is paramount in patients with ST-elevation myocardial infarction (STEMI). Although primary percutaneous intervention (pPCI) is recommended as the preferred strategy, access to pPCI may be limited in various regions for many reasons, particularly in middle-income countries. In contrast, a pharmacoinvasive strategy (PI) is based on the widespread availability of fibrinolysis and its relative simplicity in restoring myocardial blood flow. Coupled with cardiac catheterization and appropriate coronary intervention, PI can be delivered urgently to patients who fail to reperfuse or scheduled in those with successful lysis. Randomized clinical trials and observational studies have demonstrated similar efficacy and safety of PI. However, data on each strategy’s economic costs and impact on in-hospital stay remain scarce.1–3
The present study assessed economic costs, hospital length of stay, and clinical outcomes of patients with STEMI undergoing either PI or pPCI in a prospective cohort from Mexico City.
Materials and Methods
We conducted a prospective, observational single-center study that included consecutive patients aged >18 years diagnosed with STEMI who were primarily treated in any non-PCI hospital within the Mexico City STEMI Network and transferred to the study center for either pPCI or cardiac catheterization within the scope of PI. The design of the PHASE-MX study (ClinicalTrials.gov identifier NCT03974581) is discussed elsewhere, and this work represents a continuation of the original research up to January 2021.4 Patients with STEMI receiving late reperfusion (>12h since symptom onset) or no reperfusion within the same timeframe were included as negative controls (NR) (Figure 1).
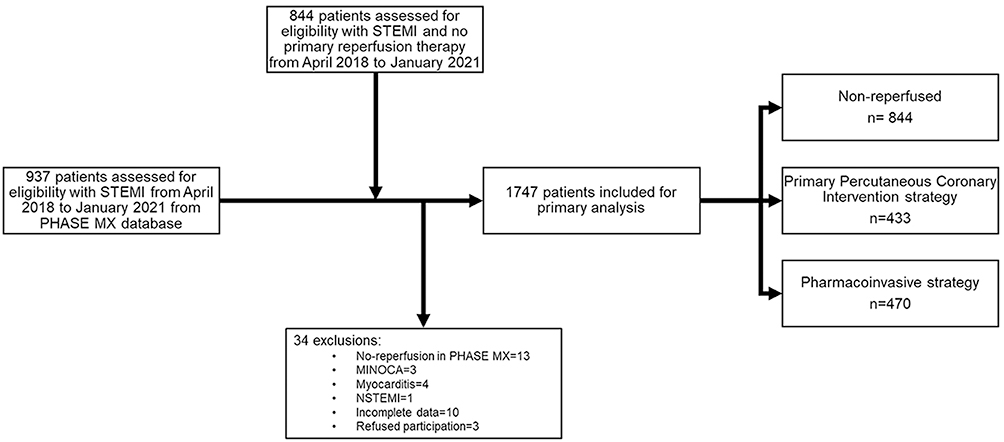 |
Figure 1 Flow chart of the study. Abbreviations: STEMI, ST-elevation myocardial infarction. NSTEMI, non-ST elevation myocardial infarction. MINOCA, Acute Myocardial Infarction with Non-Obstructive Coronary Arteries. |
The study research team prospectively assessed baseline clinical characteristics, hospital stay, and outcomes. Major cardiovascular events (MACE) were defined as the 30-day incidence of death, heart failure, cardiogenic shock development, major bleeding (Bleeding Academic Research Consortium [BARC] ≥3 criteria), or stroke.
The protocol complied with the Declaration of Helsinki and received approval from the “Institutional Research or Ethics Committees” of the Instituto Nacional de Cardiología Ignacio Chávez. Patients were treated under local and international guidelines; informed consent was waived by “Institutional Research or Ethics Committees” of the Instituto Nacional de Cardiología Ignacio Chávez because the observational retrospective nature of the study and no randomized intervention was performed also data was anonymized for the current analysis.
Outcomes and Cost Analysis
The study’s primary outcome was the incremental cost-effectiveness ratio (ICER) for PI compared with those for pPCI and NR, calculated for 30-day MACE. ICERs were also calculated for hospital stay and mortality. Cost analysis was made in US dollars (USD) after converting from Mexican pesos (MXN) using the conversion factor of 20.36 MXN = 1 USD. Costs were obtained as assigned at the actual in-hospital cost determined by the hospital board in 2021, obtained from the total in-hospital length of stay (In case of death censored to 30 days), thrombolytic therapy, and percutaneous intervention for primary intervention in PI and pPCI groups.
Statistical and Cost-Effectiveness Analysis
The data on clinical and imaging parameters are expressed as the median and interquartile range (IQR). The chi-squared test was used to compare nominal characteristics. Kruskal–Wallis tests for group comparisons were performed with Bonferroni correction for pairwise comparison. Kaplan–Meier curves were plotted to display the unadjusted relationship between the reperfusion strategy and the primary endpoint compared with the Log rank test groups. Kaplan–Meier estimated rates, hazard ratios (HRs), and 95% confidence intervals (CIs) within 1 year are also reported. Cox regression models were adjusted for confounders for variables with P ≤ 0.1.
ICERs were calculated to reduce outcomes (MACE, mortality, and length of stay) and the adjusted cost estimate. ICER was calculated by dividing the difference in mean cost (intervention minus control) by the difference in outcome measures. In this study, the active comparator was the PI strategy. The ICER formula represents the additional cost to prevent an incidence of the endpoints. (5, 6) Bootstrapping methods (using 1000 replications) examined the joint probability distribution of costs and outcomes. Bootstrapped costs and outcome pairs are graphically displayed as a scatter plot on an incremental cost-effectiveness plane.
To understand the impact of data uncertainty on our findings, we conducted a univariate analysis with the change of cost in the PI group from 90% to 200% cost in these groups. 2-way sensitivity analysis was assessed by the previous shift in cost in the PI groups vs an effect difference of ±20%.
The willingness-to-pay threshold was defined by the monthly per capita GDP in Mexico (Mx-GDP; $695 USD in 2020)5 and stratified into cost-saving groups: ICER <0 = very cost-effective; ICER 0–1× Mx-GDP = cost-effective; ICER 1–3× Mx-GDP = poorly cost-effective; and ICER >3× Mx-GDP = not cost-effective.
All statistical tests were two-sided, and a P-value < 0.05 was considered significant. The analysis was performed using IBM SPSS Statistics for Windows, Version 22.0 (Armonk, NY: IBM Corp. IBM Corp.) and MedCalc for Windows (v19.4; MedCalc Software, Ostend, Belgium); SAS 9.3 (SAS Institute, Cary NC) and R (R Foundation for Statistical Computing, Vienna, Austria) for the ICER analysis.
Results
Baseline characteristics are described in Table 1 according to the treatment strategy and show that patients in the PI group were younger (P < 0.001). A greater prevalence of diabetes was seen in the NR group (47.5% vs 33% for the pPCI and 39.6% for the PI groups, respectively). Active smoking was less prevalent in the NR group (P < 0.001). History of heart failure was more prevalent in NR. In addition, the NR group had higher Killip–Kimball scores ≥2 of 71% vs 40% in the pPCI and 46% in the PI groups; TIMI risk scores were overall higher in the NR group. Furthermore, the PI group had thrombolysis in 115 (24.5%) with alteplase and 355 (75.5%) with Tenecteplase.
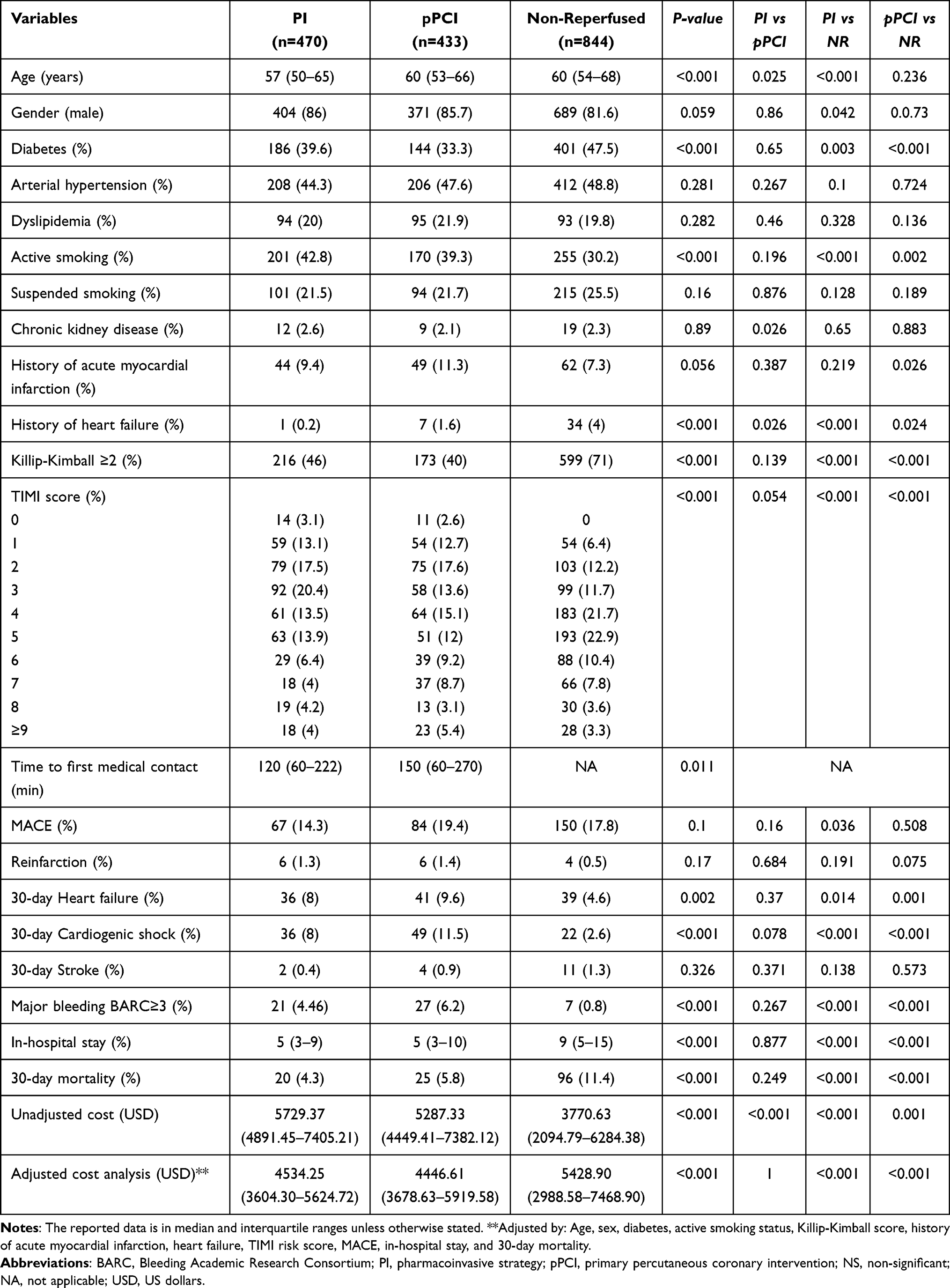 |
Table 1 Baseline Characteristics, Outcomes, and Costs in Patients with STEMI |
Comparison of Length of Stay and Mortality
Thirty-day length of stay showed a significant difference between groups. In the pairwise comparison of the PI and pPCI groups, 5 (3–10) in the pPCI group and 5 (3–9) in the PI group (P = 1.0) did not show significant differences; however, they differed compared with the NR group with 9 (5–15) (P < 0.001 for both comparisons). A Kaplan–Meier curve was constructed as the probability of being in hospital over the length of stay in the three groups. A Log rank test was significant (P < 0.001), and the HR was 0.97 (0.83–1.13; P = 0.53) when the PI strategy was compared with pPCI, and the HR was 0.6 (0.53–0.67; P < 0.001) in the case of PI patients compared with NR patients (Figure S1). The Cox model for the pPCI strategy had a non-significant ratio of 1.09 (0.95–1.25; P = 0.23), and NR had a significant difference with an HR of 0.63 (0.55–0.71; P < 0.001) when the PI strategy was compared with NR (Figure S2).
Thirty-day mortality was similar in the two invasive strategy groups, with 5.8% in the pPCI group and 4.3% in the PI group (P > 0.05), but it was significantly different compared with the NR group (11.4%; P < 0.001). In contrast, significant differences in the log-rank curve were found with P = 0.006, there were no differences when the PI strategy was compared with pPCI with an HR of 0.71 (0.43–1.17; P = 0.22). When the PI strategy was compared with NR, there was a significant difference with an HR of 0.49 (0.33–0.73; P = 0.002). The Cox model adjusted by the PI strategy had a non-significant ratio of 0.85 (0.45–1.59; P = 0.61), and when compared with the NR group, a statistically significant ratio of 0.55 (0.33–0.93; P = 0.026) (Figure S2).
Cost Comparison
Unadjusted cost analysis showed that PI was more expensive than pPCI and NR ($5729.37 vs $5287.33 and $3770.63, respectively, with a median difference of $442.04 and $1958.74; P < 0.001 and a pairwise comparison of P < 0.001).
When adjusted by age, sex, diabetes, active smoking status, history of acute myocardial infarction, heart failure, TIMI score, MACE, in-hospital stay, and 30-day mortality, the adjusted cost analysis showed an overall significant difference when analyzed by pairwise comparison. A similar cost was found in the PI and pPCI groups ($4534.25 vs $4446.61 with a median difference of $87.64, P = 1.0). Higher costs were seen when NR patients were compared with PI ($4534.25 vs $5428.90, a median difference of $894.65; P < 0.001), and when NR patients were compared with pPCI ($4446.61 vs $5428.90, a median difference of $982.29; P < 0.001) (Figure 2A).
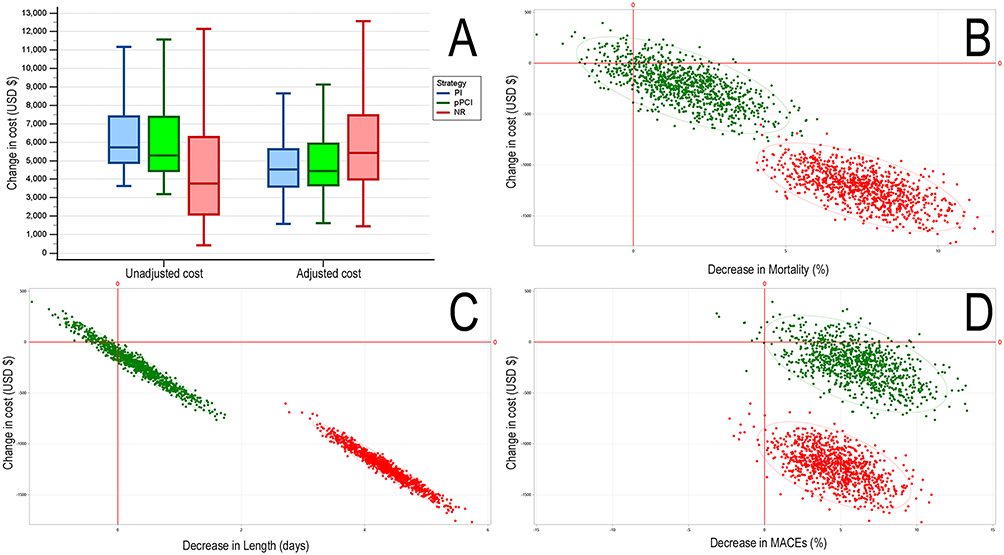 |
Figure 2 (A) Box and whiskers graph of unadjusted vs adjusted cost in US dollars (USD) of the three strategies in STEMI. (B–D) indicate the ICER bootstrap values for mortality, length of stay, and MACE, comparing the cost-effectiveness against pPCI (green) and NR (red). Abbreviations: PI, pharmacoinvasive strategy; pPCI, primary percutaneous coronary intervention; NR, non-reperfused. |
Secondary Outcomes
MACE had a lower 30-day incidence in the PI group than the pPCI group (14.3 vs 19.4%), but no significant difference was found when analyzed against the whole cohort. In addition, higher bleeding events were seen in patients with an invasive strategy than in NR patients, but pairwise comparison did not show significant differences between PI and pPCI.
Incremental Cost-Effectiveness Ratio (Table S1 and Figure 2B–D)
The mean cost difference between PI and pPCI was $ –215.58 (–601.41 to 171.10), and when compared to NR, the mean exceeding cost was $1221.69 (896.22 to 1567.181).
The ICER estimates for the length of stay were –$283.40 (–304.95 to –252.76) per day of stay, and an effect decrease in length of stay estimate of 4.31 days (3.44–5.21) when compared with the NR group. Comparison with pPCI revealed an ICER of –$765.99 (–4020.68 to 3141.65) and an effect size of 0.28 days less (CI, –0.71 to 1.31). The bootstrapping simulation showed that the PI strategy was cost-effective for this outcome in 100% of cases when compared to NR, whereas PI vs pPCI was cost-effective in only 70% of cases, 13.6% less effective-less costly, and 15.7% less effective-more costly.
The mortality ICER analysis revealed an effective decrease of the PI strategy vs the NR group by 7.39 (4.91–10.26) percentage points with an ICER decrease of –$165.27 (–224.06 to –123.52). In contrast to the comparison of pPCI, the effect size was 1.64 percentage points of mortality (–1.05 to 4.43) and an ICER decrease of –$129.50 (–810.57 to 455.06). When simulations were analyzed, PI was dominant in 100% and 79.4% of cases against NR and pPCI, respectively. A close look at the comparison of PI vs pPCI shows a 6% less effective- more costly, 7% of less cost-effective, and finally, 7.6% of more costly-effective.
In cost–MACE analysis, the estimate was a decrease of $–35.81 (–114.73 to 64.81) in the likelihood of presenting MACE when compared with pPCI and a decrease of $–271.60 (–1086.10 to –144.93) compared with NR. The effect size difference was 6.02 (0.61–8.63) compared with pPCI and 4.5 (1.23–10.74) with NR. The bootstrap cost-effectiveness graph shows a dominant prevalence in 98% and 86.2% of cases for NR and pPCI, respectively, when compared with the PI strategy. In 1.2% and 0.2% of cases (NR and pPCI, respectively), low cost and low cost-effectiveness were seen. Finally, against the pPCI group, 12.8% was more effective-more costly, and 0.8% a more costly-less effective therapy.
Multivariate Sensitivity Analysis
A one-way tornado plot (Figure S3) against the possible scenarios was plotted. Only if the cost variance achieved up to 200% in the PI intervention group was not a cost-effective strategy. All other scenarios had at least a cost-effective analysis of a cost-saving intervention, especially against the NR group.
In the case of pPCI, the length of stay had more area of not cost-effectiveness decaying if the values were 110% more even though the effects were higher; and in mortality costs above 160% to 180% spectrum had a non-cost-effectiveness strategy. Nevertheless, in the MACE analysis, the intervention of PI was cost-effective across this sensitivity analysis (Figure 3).
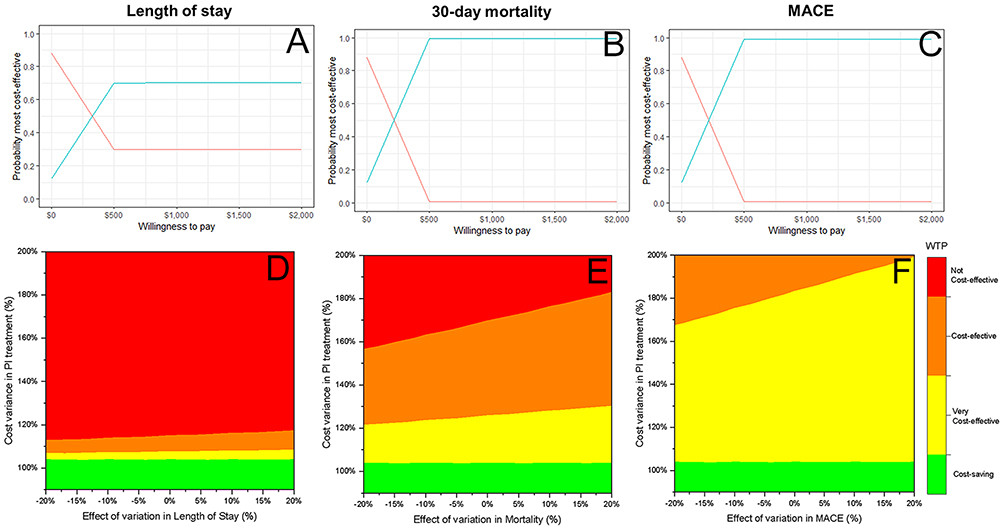 |
Figure 3 PI vs pPCI estimates. Cost-effectiveness acceptability curve from probabilistic sensitivity analysis against one-way sensitive analysis (blue = PI vs red = pPCI) against the analyzed outcomes length of stay (A), mortality (B), and MACE (C). A two-way sensitivity analysis was performed to determine the effects of length of stay (D), mortality (E), and MACE (F). (D–F) are color-coded to identify different willingness-to-pay (WTP) thresholds. Green indicates a cost-saving ICER<0. Yellow indicates a very cost-effective 0–1× Mx-GDP. Orange indicates a WTP threshold 1–3× Mx-GDP. Red indicates variable inputs that exceed a WTP threshold 3× Mx-GDP. Abbreviation: Mx-GDP, Mexico’s monthly gross domestic product per capita. |
Two-way sensitivity analysis with varying costs, previously described against the effect variations studied in the groups with a difference of ±20%, showed that all study points—length of stay, 30-day mortality, and MACE—were cost-effective against NR (Figure 4).
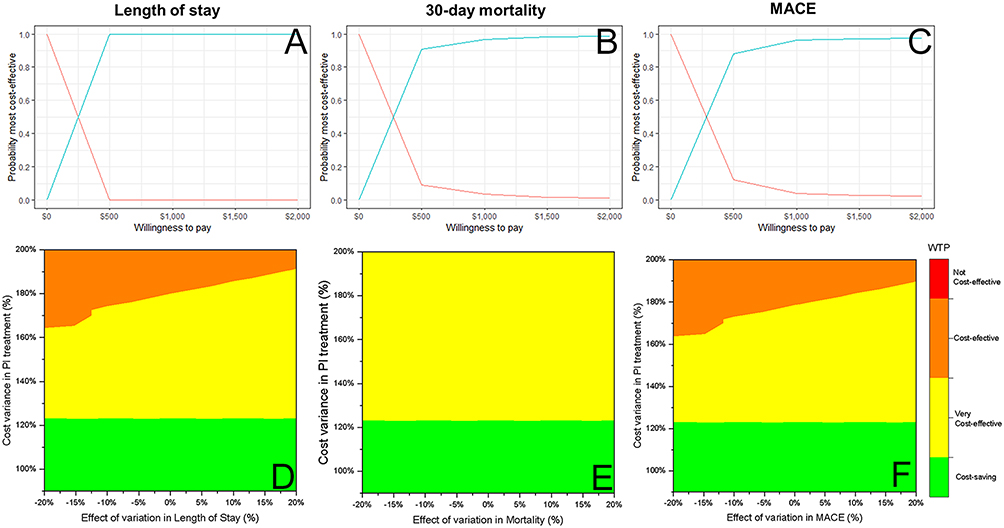 |
Figure 4 PI vs NR estimates. Cost-effectiveness acceptability curve from probabilistic sensitivity analysis against one-way sensitive analysis (blue = PI vs red = NR) of the length of stay (A), mortality (B), and MACE (C). A two-way sensitivity analysis was performed to determine the effects of length of stay (D), mortality (E), and MACE (F). (D–F) are color-coded to identify different willingness-to-pay (WTP) thresholds. Green indicates a cost-saving ICER <0. Yellow indicates a very cost-effective 0–1× Mx-GDP. Orange indicates a WTP threshold 1–3× Mx-GDP. Red indicates variable inputs that exceed a WTP threshold 3× Mx-GDP. Abbreviation: Mx-GDP, Mexico’s monthly gross domestic product per capita. |
Discussion
This study highlights that no difference was seen in the economic cost of PI compared with pPCI in a real-world setting within a developing country’s STEMI governmental healthcare system. We demonstrate that the PI strategy is similar in economic cost, mortality, and length of stay, with a lower incidence in MACE compared with pPCI. Furthermore, in a limited constraint environment where the pPCI strategy cannot be delivered in a timely manner, PI is an economically feasible strategy comparable in economic cost with pPCI; moreover, PI also reduces the burden of the length of stay and mortality compared with NR. To our knowledge, this is one of only a few studies,6,7 and the first in Latin America, to examine the economic impact of these two strategies.
Despite the cost difference between PI and pPCI, no differences were revealed when confounders were adjusted. Our analysis demonstrates that NR increases the economic burden and strain in our system with the mean exceeding a cost of $1221.69 (896.22–1567.18) per patient in PI and $1006.11 (635.18–1352.73) in pPCI vs patients who were not reperfused in a timely manner (NR). This gives PI an edge in our area, where a pPCI center strategy can take longer than the international guidelines recommend.
Our findings support that the PI strategy for treating STEMI patients in government healthcare systems with limited access to pPCI can help lower the burden of STEMI sequelae with no increase in costs compared with pPCI and with reduced costs against NR. In other studies,7,8 NR patients were associated with increased costs due to higher mortality, and we found similar findings in the present study. ICER graphs confirmed that the PI strategy was dominant compared with NR and pPCI. Moreover, in most instances, PI had more chances of being cost-effective in our area than pPCI.
In our cohort, we found a similar length of stay between the two invasive strategies, and when adjusted for covariables, there was no difference in the time to discharge. Previous studies have shown different perspectives on the length of stay. The GWTG‐CAD registry had a longer median length of stay for patients receiving PI than pPCI (4 vs 3 days).8 Similarly, Rashid et al9 and Bainey et al10 obtained comparable results between pPCI and PI, with a median length of stay of 4 and 5 days, respectively, with both studies revealing no significant differences. Importantly, we found no differences in mortality between the reperfusion strategies and the safety endpoint of bleeding. The mortality rate (4.3% vs 5.8%) of the PI strategy group against pPCI was comparable with data published in STREAM (4.6% vs 4.4%).2
Interestingly, our study showed a lower incidence of MACE at 30 days in the PI group, although it did not reach statistical significance in the cohort as previous trials suggested.2 Regarding major bleeding events, no differences were found between groups in terms of BARC ≥3 criteria, which in our cohort were lower than in the STREAM study (21.8% vs 20.2%); as expected, a higher incidence of this endpoint was seen in comparison with an NR strategy.2
Although primary coronary intervention is the preferred reperfusion strategy in STEMI within the first hours of symptom onset, its superiority has been demonstrated in high-volume centers in developed countries. In contrast, the reality differs in developing countries like Mexico, where pPCI is not always an immediate option, and the transfer period can be >3 h. By initiating prompt intravenous thrombolysis with PI, we allow more time for transportation to a pPCI center with equivalent length of stay and safety outcomes. Furthermore, pPCI can potentially translate to lower mortality, MACE, disability, and cost-saving compared with an NR patient.
Our study has limitations regarding the long-term data (>30 days) in outcomes. In addition, the appropriateness and cost of maximal medical therapy were not assessed. The observational and non-blinded nature of the registry could lead to potentially biased selections and retrospective analysis of registry data, where confounding variables could have impacted the results. However, we controlled for known confounding variables in this study’s statistical Cox regressions. We did not assess patient-level expenditures such as laboratory tests, imaging, or pharmacological therapy such as devices (mechanical ventilation, IABP, and other support), so the overall cost presented here is lower than previously reported. However, adjusting the costs of a healthcare intervention can help provide a more accurate estimate of the total cost of the intervention, as it accounts for the additional costs associated with treating these outcomes. And perspective gained by the 1 and 2-way sensitivity analysis is important due to the uncertainty surrounding real-world costs, as well as the potential variability in patient outcomes and healthcare resource utilization. Despite these shortcomings, we can confirm that the NR strategy, known to have more MACE and higher resource consumption, came at a higher burden to the financial healthcare system.
Since STEMI continues to be one of the most significant public health burdens in our healthcare system, the present findings should encourage policymakers and health services to identify the PI strategy as an appropriate strategy in the context of STEMI in our area. Where pPCI centers are scarce, using a PI strategy can lead to a practical approach equal to that of pPCI in reducing the net financial burden of STEMI on the healthcare system. Moreover, it may reduce the strain imposed on the physician and the patient dealing with STEMI-related complications and the net financial burden by giving time to refer to a PCI center.
Conclusions
In an upper-middle-income country, where patient and system delays are expected, the PI was associated with a similar length of stay and mortality and no increased costs. Furthermore, with lower MACE compared with pPCI, PI is a cost-effective and cost-saving strategy compared with NR.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Acknowledgment
The authors thank the secretarial staff of the Coronary Care Unit, Leticia Casiano and Laura Armas, for their valuable cooperation in the preparation of this manuscript.
Disclosure
Dr Alexandra Arias-Mendoza reports personal fees from Boehringer, personal fees from Novartis, personal fees from Novonordisk, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevationThe Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/EURHEARTJ/EHX393
2. Armstrong PW, Gershlick AH, Goldstein P, et al. Fibrinolysis or primary PCI in ST-segment elevation myocardial infarction. N Engl J Med. 2013;368(15):1379–1387. doi:10.1056/NEJMoa1301092
3. Fernandez-Avilés F, Alonso JJ, Castro-Beiras A, et al. Routine invasive strategy within 24 hours of thrombolysis versus ischaemia-guided conservative approach for acute myocardial infarction with ST-segment elevation (GRACIA-1): a randomised controlled trial. Lancet. 2004;364(9439):1045–1053. doi:10.1016/S0140-6736(04)17059-1
4. Baeza-Herrera LA, Araiza-Garaygordobil D, Gopar-Nieto R, et al. Evaluation of pharmacoinvasive strategy versus percutaneous coronary intervention in patients with acute myocardial infarction with ST segment elevation at the National Institute of Cardiology (PHASE-MX). Arch Cardiol Mex. 2020;90(2):158–162. doi:10.24875/ACM.19000185
5. PIB per cápita. Cuéntame de México. Available from: https://cuentame.inegi.org.mx/economia/pibpc.aspx?tema=e.
6. Zubaid M, Khraishah H, Alahmad B, et al. Efficacy and safety of pharmacoinvasive strategy compared to primary percutaneous coronary intervention in the management of ST-segment elevation myocardial infarction: a Prospective Country-Wide Registry. Ann Glob Health. 2020;86(1). doi:10.5334/AOGH.2632
7. Mohan VN, Alexander T, Muraleedharan VR, et al. Economic and societal impact of a systems-of-care approach for STEMI management in low and middle-income countries: insights from the TN STEMI program. Ann Glob Health. 2019;85(1):122–123. doi:10.5334/AOGH.2508/METRICS/
8. Hira RS, Bhatt DL, Fonarow GC, et al. Temporal trends in care and outcomes of patients receiving fibrinolytic therapy compared to primary percutaneous coronary intervention: insights from the Get With the Guidelines Coronary Artery Disease (GWTG-CAD) registry. J Am Heart Assoc. 2016;5(10). doi:10.1161/JAHA.116.004113
9. Rashid MK, Guron N, Bernick J, et al. Safety and efficacy of a pharmacoinvasive strategy in ST-segment elevation myocardial infarction. JACC Cardiovasc Interv. 2016;9(19):2014–2020. doi:10.1016/j.jcin.2016.07.004
10. Bainey KR, Armstrong PW, Zheng Y, et al. Pharmacoinvasive strategy versus primary percutaneous coronary intervention in ST-elevation myocardial infarction in clinical practice: insights from the Vital Heart Response Registry. Circ Cardiovasc Interv. 2019;12(10). doi:10.1161/CIRCINTERVENTIONS.119.008059
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.