")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Real-World Effectiveness of Fluticasone Furoate/Umeclidinium/Vilanterol Once-Daily Single-Inhaler Triple Therapy for Symptomatic COPD: The ELLITHE Non-Interventional Trial
Authors Beeh KM , Scheithe K, Schmutzler H, Krüger S
Received 26 September 2023
Accepted for publication 8 December 2023
Published 17 January 2024 Volume 2024:19 Pages 205—216
DOI https://doi.org/10.2147/COPD.S427770
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Kai-Michael Beeh,1 Karl Scheithe,2 Heike Schmutzler,3 Saskia Krüger3
1Insaf Respiratory Research Institute, Wiesbaden, Germany; 2Department of Biostatistics, GKM Gesellschaft Für Therapieforschung mbH, Munich, Germany; 3Medical Department, BERLIN-CHEMIE AG, Berlin, Germany
Correspondence: Kai-Michael Beeh, Insaf Respiratory Research Institute, Biebricher Allee 34, Wiesbaden, 65187, Germany, Tel +49 (0) 611 9854410, Email [email protected]
Purpose: Real-life effectiveness data on once-daily single-inhaler triple therapy (odSITT) with the inhaled corticosteroid fluticasone furoate (FF), the long-acting muscarinic antagonist umeclidinium (UMEC), and the long-acting β2-agonist vilanterol (VI) in patients with chronic obstructive pulmonary disease (COPD) are important to complement evidence from well-controlled randomized clinical trials. Effectiveness of odSITT was quantified by assessing health status and symptoms in usual care.
Patients and Methods: ELLITHE was a single-country (Germany), multicenter, open-label, non-interventional effectiveness study between 2020 and 2022, evaluating the effect of treatment initiation with FF/UMEC/VI 100/62.5/25 μg once-daily via the ELLIPTA inhaler on improvements in clinical outcomes versus baseline in COPD patients. The primary endpoint was the change in the total COPD Assessment Test (CAT) score between baseline and month 12. Key secondary endpoints included change in CAT score over time, occurrence of exacerbations until month 12, changes in forced expiratory volume in one second (FEV1), inhaler adherence, and safety.
Results: Nine hundred and six patients were included (age 66.6 years, 55.6% male, mean FEV1 52.6% of predicted, mean CAT 21.5 units, 1.4 exacerbations/year pre-study). About 63.9% of patients were escalated from dual therapies, and 18% were switched from multiple-inhaler triple therapies. Reductions in CAT score at month 12 were statistically significant and above the threshold of clinical importance (− 2.6 units; p < 0.0001). CAT score also improved at interim visits. CAT improvements were more pronounced in patients with high baseline scores and better inhaler adherence. Exacerbations during follow-up were rare (0.2 events/year) compared to pre-study (1.4 events/year). FEV1 was improved by 93 mL (p < 0.0001). No new safety effects were observed.
Conclusion: In usual care, treatment with odSITT resulted in significant and clinically relevant improvements of CAT score and FEV1 in COPD patients, regardless of the occurrence of exacerbations. These findings challenge the current guideline recommendations for SITT only in patients experiencing exacerbations.
Keywords: CAT score, real-world evidence, lung function, exacerbation, treatment adherence
Introduction
Triple therapy with inhaled corticosteroid (ICS), long-acting β2-agonist (LABA) and long-acting muscarinic antagonist (LAMA) is currently approved as treatment option for moderate-to-severe chronic obstructive pulmonary disease (COPD) patients uncontrolled on dual-combination therapies.1–3 As of today, three single-inhaler triple therapies (SITT) have been licensed for COPD treatment, avoiding the necessity to use multiple inhalers and more frequent dosing schemes, thus offering the potential to improve treatment adherence, which could in turn lead to improved clinical outcomes.4,5
Current national6 and international7 guidelines and strategies recommend triple therapy for patients experiencing frequent moderate or severe exacerbations as an escalation step from long-acting bronchodilator therapy. The use of blood eosinophil count is also strongly promoted to identify patients with high likelihood of benefitting from an ICS-containing therapy.8 In contrast, triple therapy is not mentioned as a part of follow-up therapy in non-exacerbating patients with persistent symptoms, namely dyspnea, beyond dual LAMA/LABA bronchodilation. This recommendation is somehow more restrictive than the current approval status of SITTs, which includes COPD patients uncontrolled on either dual therapies, regardless of whether this is defined by persistent symptoms and/or exacerbations.
In several large-scale, randomized controlled trials (RCTs), once-daily SITT (odSITT) with fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) has demonstrated a wide range of clinical benefits, including reduction of moderate-to-severe exacerbations and symptoms while improving health status and lung function versus dual therapies FF/VI, UMEC/VI9 and budesonide/formoterol.10 Importantly, a relative reduction in the mortality rate was observed versus dual LAMA/LABA therapy11 similar to findings in the ETHOS trial.12 A recent network meta-analysis suggested, that odSITT may provide superior improvements in lung function than other available SITTs.13 Finally, the real-world open-label randomized INTREPID study demonstrated that odSITT resulted in a larger likelihood of health status improvement over 6 months versus usual care with multiple-inhaler triple therapies (MITT).14
However, while RCTs remain the gold standard to generate top-level evidence with high internal consistency, they mostly include highly selected or enriched patient populations and may therefore lack external validity and generalization to usual clinical practice.15,16 Therefore, real-world observational studies in routine care can provide important evidence of effectiveness that is complementary to RCTs.17–19
The ELLITHE (A prospective non-interventional study to assess quality of life and COPD symptoms in patients with COPD on FF/UMEC/VI triple therapy) study was designed to evaluate the effectiveness of odSITT on improving health status over 12 months in previously uncontrolled COPD patients treated in multiple sites in Germany. We also sought to describe baseline characteristics of COPD patients in Germany initiated on odSITT under real-life practice conditions.
Materials and Methods
Trial Design and Oversight
ELLITHE was a multicenter, non-interventional, open-label, effectiveness study evaluating once-daily single-inhaler FF/UMEC/VI delivered by the ELLIPTA inhaler in uncontrolled COPD patients in a usual clinical practice setting. The primary objective was to evaluate the effectiveness of odSITT on health status in patients with COPD after 12 months of treatment versus baseline.
The inclusion and exclusion criteria were minimal to align with use according to EU label; details are provided in the Supplementary Table 1. All patients had a confirmed COPD diagnosis by spirometry in the medical records of their treating physician.
This trial was conducted at 119 centers in Germany from June 2020 to July 2022 in pulmonology specialist (N = 111) and internal/general medicine (N = 8) practices. The study was carried out in accordance with Good Clinical Practice guidelines under the provisions of the Declaration of Helsinki and received approval from independent ethics committees. The study was registered at the German Clinical Trials Register (DRKS00031897). All patients provided signed informed consent.
To minimize deviations from usual care and impact on normal patient behavior, patients were managed by their clinician in accordance with usual care practice, and only five study visits were planned: one at baseline/enrollment (Visit 1, V1) and one after 3, 6, 9 and 12 months on treatment (Visit 2–5, V2-V5). At each visit, patients completed a COPD Assessment Test (CAT) within their routine clinical COPD workup. The CAT is a simple instrument to assess health and functional status in patients with COPD.20 The CAT consists of 8 items, each formatted as a semantic six-point differential scale. These 8 items cover cough, phlegm, chest tightness, breathlessness when going up hills/stairs, activity limitations at home, confidence leaving home, sleep and energy. Each item is scored from 0 to 5 giving a total score ranging from 0 to 40. The questionnaire was to be filled out by the patient, and the total score was to be entered into the electronic case report form (eCRF). Patients should fill out the CAT at the initial study visit and after approximately 3, 6, 9 and 12 months.
In addition, patients were evaluated for occurrence of exacerbations and filled out the Test of Adherence to Inhalers (TAI) questionnaire. The TAI is a validated questionnaire designed to identify aspects of the daily use of inhalers.21 The questionnaire consists of 10 questions, eg, how often patients have forgotten or deliberately avoided inhalation and if they have any problems with handling the inhaler. The scoring range for each question is from 1 (worst compliance) to 5 (best compliance). The minimum and maximum possible total scores are 10 and 50. A total score of 50 points reflects good adherence, 46 to 49 points intermediate adherence and ≤45 points poor adherence. The questionnaire was to be filled out by the patient, and the total score was to be entered into the eCRF. Patients should fill out the TAI at baseline and after approximately 3, 6, 9 and 12 months. Patients also rated the ability to handle their ELLIPTA inhaler using a Likert scale ranging from 1 (very good) to 6 (very bad) at the end of the study period (months 12 or at discontinuation).
At each visit, pulmonary function tests were performed if they were part of routine care and forced expiratory volume in one second (FEV1) was recorded.
Safety information was collected at all scheduled or usual care visits and recorded in the eCRF.
Where available, peripheral blood eosinophil counts were collected at baseline or using the historical value closest to the patient’s consenting visit.
Effectiveness Outcomes
The prespecified primary endpoint was the change from baseline in mean CAT score at 12 months. A clinically meaningful response is defined as a decrease in CAT score of ≥2 units from baseline.22 Prespecified secondary endpoints included change from baseline in CAT score at months 3, 6, and 9, the percentage of patients experiencing mild (increased short-acting bronchodilator use only), moderate (prescription of antibiotics and/or oral corticosteroids) or severe (additional inpatient treatment) exacerbations, the time to first exacerbation, absolute (L) changes in FEV1 versus baseline, treatment adherence assessed by the TAI questionnaire at months 3, 6, 9, and 12, and safety.
Safety Assessments
Adverse event (AE) recording included treatment-related AEs, serious AEs (SAEs) and AEs leading to study treatment discontinuation or study withdrawal. Serious AEs of special interest (AESI), ie, SAEs that have specified areas of interest for FF, UMEC or VI or the overall COPD population, were also collected.
Statistical Considerations
The full analysis set (FAS) consisted of all patients who gave written informed consent, for whom all inclusion criteria and all exclusion criteria were confirmed and who received at least one dose of FF/UMEC/VI via the ELLIPTA inhaler. Additionally, a subpopulation of the FAS including patients on LAMA/LABA, LABA/ICS or LAMA/LABA/ICS therapy before switch to odSITT was analyzed. In general, data were analyzed descriptively. Arithmetic data were presented as mean values with 95% confidence intervals (CI) or standard deviation (SD). Median values were reported with min-max. In this study, the primary endpoint was the change in the total CAT score between baseline and month 12. In cases where patients discontinued from study treatment or follow-up prior to the final visit at month 12, the last-observation-carried-forward (LOCF) approach was used. Statistical tests and confidence intervals were calculated to assess statistically significant changes. Specific tests for outcome parameters are listed in the respective figure and table legends. All statistical analyses were carried out by means of the SAS® package (version 9.4).
As for non-interventional studies, typically a power analysis is not performed, a sample size justification based on the statistical precision for the estimation of the primary endpoint was used. A previous study22 investigated the change in the total CAT score in COPD patients over 12 months and found a standard deviation for change from baseline of 9 points.
Assuming a standard deviation of 9 points, a two-sided 95% confidence interval leads to a precision of ± 0.46 points when 1500 patients are enrolled in this study.
Results
Trial Population
Between June 2020 and July 2021, a total of 931 patients were enrolled. The enrollment was lower than originally planned due to restrictions during the COVID-19 pandemic. However, the precision estimate of the primary endpoint was minimally affected by the lower recruitment rate and was thus deemed to be acceptable
Nine hundred and twenty-seven patients were treated with the study medication, of whom all inclusion/exclusion criteria were confirmed for 906 patients and were thus included in the FAS. Four hundred and seventy patients completed the study, while 461 patients discontinued the study prior to the final visit (V5) after 12 months (Supplementary Figure 1). Reasons for study discontinuation were amongst others “Patient’s wish” (6.2%), “Lost to follow-up” (3.5%) and “Withdrawal of informed consent” (2.2%). The median duration of follow-up and treatment exposure was 337 days (range 1–508 days). Baseline characteristics of the FAS patients are summarized in Table 1 and Supplementary Table 2. In general, patients were predominantly males aged >60 years, former smokers, and had a history of typical symptoms and/or COPD diagnosis of >5 years. A small proportion of patients (<10%) had a history of atopy and/or asthma diagnosis before the age of 40, while 46.5% had symptoms or a history of chronic bronchitis. Eosinophils were only available in a small subset of patients (N = 158/906). All patients had a history of at least one exacerbation in the year prior to enrolment, with a mean rate of 1.4 events (mild: 0.4/year; moderate: 0.8/year; severe: 0.1/year). Patients were highly symptomatic (mean CAT score 21.5 ± 6.7; mMRC grade II–IV in 70.4% of patients) despite pretreatment with dual LAMA/LABA (49.6%), LABA/ICS (14.3%) or free or fixed triple LAMA/LABA/ICS (22.8%) combination. The main reasons for initiation of odSITT were lack of symptom control (54.2%), simplification of therapy (42.3%), COPD deterioration (35.5%), and increased exacerbation frequency (35.1%; multiple entries possible) (Supplementary Table 3). Baseline data were similar for the patient population with prior LAMA/LABA, LABA/ICS or LAMA/LABA/ICS COPD maintenance treatment (Supplementary Tables 4 and 5).
 |
Table 1 Baseline Patient Demographics and Characteristics |
Primary and Secondary Effectiveness Analyses
CAT Score
Between V1 and V5, enrolled patients on odSITT experienced a significant and clinically meaningful (≥2 units) reduction in the CAT score from 21.5 to 18.6 units, corresponding to a mean change from baseline of −2.6 units (95% CI −3.14;-2.05; p < 0.0001). Improvements in CAT score were observed consistently at all follow-up visits, with a mean change of −2.7 units occurring already after 3 months at V2 (Figure 1A).
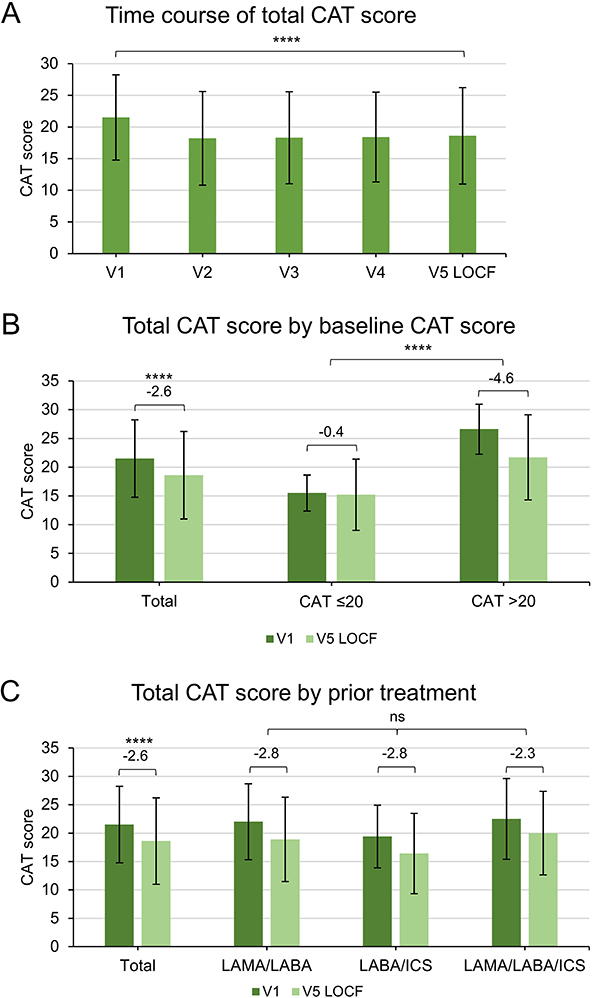 |
Figure 1 Change in CAT score after initiation of odSITT over the study period. (A) CAT score was determined at every visit. It was significantly reduced by −2.6 units between baseline and final visit. **** P-value (t-test) <0.0001. (B) Patients were categorized into two groups depending on their baseline symptom load: CAT >20 (severely symptomatic), CAT ≤20 (less severely symptomatic). At the final visit, CAT scores were assessed and change in CAT score by baseline score determined. Severely symptomatic patients at baseline benefitted more from odSITT regarding the reduction in CAT score (−4.6 units) than less severely symptomatic patients (−0.4 units). Group comparison of mean change in CAT score between groups **** p-value (t-test) <0.0001. In comparison, reduction in CAT score in the total study population after odSITT initiation was −2.6 units. Mean change in CAT score between V1 and V5 LOCF **** p-value (t-test) <0.0001. (C) CAT scores in patients were determined at baseline and final visit by treatment prior to switch to odSITT. Independent of their prior treatment (LAMA/LABA, LABA/ICS or LAMA/LABA/ICS), CAT score was significantly reduced. Group comparison of mean change in CAT score between groups not significant (ns) p-value (ANOVA) >0.05. Reduction in CAT score by prior medication was similar to the total study population. Mean change in CAT score between V1 and V5 LOCF **** p-value (t-test) <0.0001. Abbreviations: CAT, COPD assessment test; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; LOCF, last-observation-carried-forward; odSITT, once-daily single-inhaler triple therapy; V1, visit 1 (baseline). |
The change in CAT score was most pronounced in severely symptomatic patients with a high baseline CAT score as depicted in Figure 1B. In the group of COPD patients with CAT >20 units at V1, there was a large reduction of CAT after initiation of odSITT (mean change −4.6 units; 95% CI −5.40; −3.82), whereas the reduction of −0.4 units in patients with CAT ≤20 at V1 was not significant (95% CI −1.10; 0.24).
Overall, significant reductions in CAT score were observed when patients were analyzed according to their COPD maintenance treatment prior to switch to odSITT (Figure 1C). The largest improvements were seen in patients escalated from dual therapies LAMA/LABA (−2.8 units; 95% CI −3.52; −2.04) or LABA/ICS (−2.8 units; 95% CI −4.03; −1.49), while the change from baseline in patients switched from other triple therapy regimes (MITT or SITT) was significant with −2.3 units (95% CI −3.48; −1.17).
COPD Exacerbations
At the time of odSITT initiation, the mean number of all exacerbations in the 12 months prior to V1 was 1.4/year, corresponding to a rate of 0.4/year mild, 0.8/year moderate, and 0.1/year severe exacerbations. During the one-year observation period, only 8.1% (N = 73) of included patients experienced any exacerbation. At the end of the study, the mean annual exacerbation rates for total, mild, moderate, and severe exacerbations were 0.2/year, 0/year, 0.2/year and 0/year, respectively. There were 113 events in total (9 mild, 86 moderate, 15 severe, 3 not classified). In those patients experiencing any exacerbation, the median time to first exacerbation was 307 days (range 0–507 days).
Lung Function
At baseline, the majority of patients (N = 894) underwent spirometric assessments (Figure 2, Supplementary Figures 2 and 3). The mean FEV1 was 1.46 ± 0.53 L, corresponding to 52.6 ± 13.7% of the predicted value. After initiation of odSITT, FEV1 improved on average by 93 ± 390 mL until the end of the study at V5 (p < 0.0001). Meaningful improvements in FEV1 were observed already at V2, and mean changes from baseline remained stable over time. Furthermore, forced vital capacity (FVC) significantly improved on average by 64 ± 525 mL from baseline to study end (p < 0.001).
 |
Figure 2 Change in lung function by FEV1 after initiation of odSITT over the study period. FEV1 was measured at every visit possible. At baseline, mean FEV1 was 1.46 ± 0.53 L. Already at the second visit after 3 months the FEV1 significantly increased by 96 mL to 1.54 ± 0.59 L. **** P-value (t-test) <0.0001. This increase remained stable over the course of the study with an overall increase of 93 mL at the final visit (mean FEV1 1.55 ± 0.65 L). **** P-value (t-test) <0.0001. Abbreviations: FEV1, forced expiratory volume in one second; LOCF, last-observation-carried-forward; odSITT, once-daily single-inhaler triple therapy; V1, visit 1 (baseline). |
TAI and Inhaler Handling
The mean TAI score at baseline for all patients was 47.0 points, indicating intermediate adherence for the overall group. Of these, 17% showed poor (TAI score ≤45 points), 20.5% intermediate (46–49 points), and 62.5% good (50 points) adherence. The mean TAI scores improved by 1.6 ± 7.3 points at V5 (p < 0.0001). Likewise, the percentage of patients with good adherence increased to 77.1% at study end (p < 0.0001) (Figure 3A, Supplementary Figure 4).
 |
Figure 3 Change in adherence by TAI after initiation of odSITT by the end of the study. (A) Adherence was measured by TAI questionnaire. The level of adherence is distributed in three categories depending on the total score: good adherence (50 points), intermediate adherence (46–49 points) and poor adherence (≤45 points). The percentage of patients with good adherence significantly improved from baseline to final visit (**** p-value (McNemar’s test) <0.0001) while less patients were distributed to intermediate and poor adherence after initiation of odSITT. (B) Patients were distributed in the three TAI categories. Changes in CAT score were assessed for each adherence level from baseline to final visit. Patients with good or intermediate adherence had greater improvements in CAT score at the final visit compared to those with poor adherence (−2.5 and −2.3 versus +0.4 units, respectively). Group comparison of mean change in CAT score between groups * p-value (ANOVA) <0.05. Abbreviations: CAT, COPD assessment test; LOCF, last-observation-carried-forward; odSITT, once-daily single-inhaler triple therapy; TAI, test of adherence to inhalers; V1, visit 1 (baseline). |
Patients with good or intermediate adherence had on average greater improvements in CAT score at the final visit compared to those with poor adherence (−2.5 and −2.3 versus +0.4 units, respectively), shown in Figure 3B.
The distribution of patients over adherence categories was comparable in the patients with exacerbations (N = 73) to those without and to the general study population. After the 12 month treatment period, patients with an exacerbation had 75% good, 20.3% intermediate, and 4.7% poor adherence (TAI scores available N = 64/73) (Supplementary Figure 5).
About 95.5% of subjects already received training on the ELLIPTA device before study participation. When asked about inhaler handling at the end of the observation period, ELLIPTA was rated as “very good” or “good” by 35.4% and 32.8% of patients, respectively (Supplementary Table 6).
When we excluded 120 patients not on prior LAMA/LABA, LABA/ICS or LAMA/LABA/ICS COPD maintenance treatment before switch to odSITT, still all outcomes were significantly improved. Details are provided in the supplement (Supplementary Figures 6–9, Supplementary Tables 6 and 7).
Safety Results
In total, 234 AEs occurred in 148 patients (16.3% of the patients) displayed in Table 2. Fifty-eight serious AEs (SAEs) were documented for 4.6% of the patients and 68 adverse drug reactions (ADRs) for 5.0% of the patients. “Respiratory, thoracic and mediastinal disorders” was the most frequently reported system organ class among all AEs (8.9% of the patients), SAEs (1.5% of the patients), and ADRs (2.1% of the patients). A causality between the AE and the intake of odSITT was assumed for 7.7% of the AEs. For 2.1% of the AEs a causality was considered as almost certain, for 3.0% as probable and for 16.2% as possible. There were 5 cases of pneumonia during the study period, with 3 of them classified as serious. Six deaths occurred during the 12 month period, none of these was judged to be causally related to the intake of odSITT. Safety results were similar in patients with prior LAMA/LABA, LABA/ICS or LAMA/LABA/ICS COPD maintenance treatment (Supplementary Table 8).
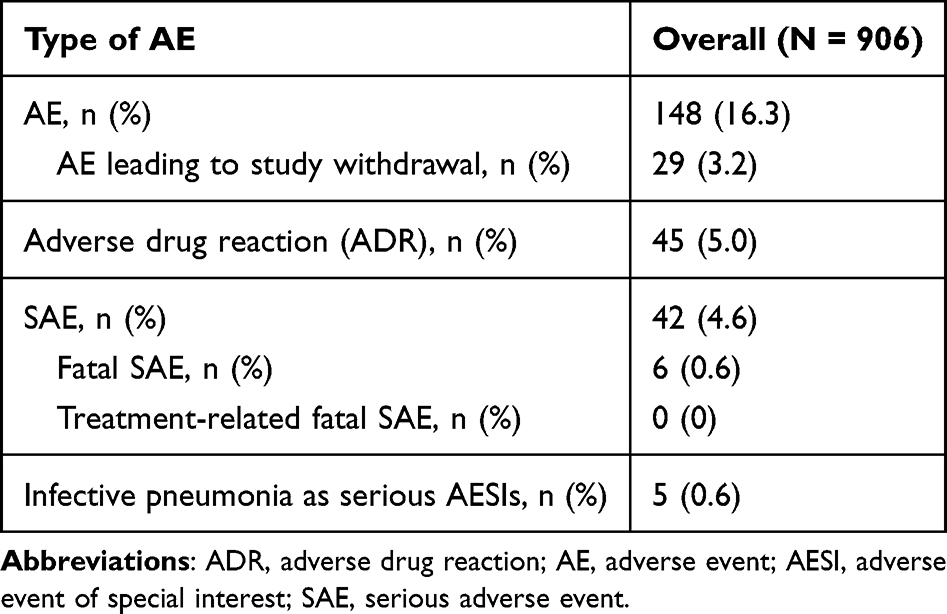 |
Table 2 Incidence of On-Treatment AEs |
Discussion
In the ELLITHE non-interventional study, we provide real-world evidence of rapid, sustained, and clinically meaningful improvements in health status in a large group of COPD patients who were initiated on odSITT in German specialist and general practices. These results support the findings from well-controlled clinical studies with odSITT.9,10 We used CAT score as primary outcome measure, a validated instrument with published minimal clinically important differences (MCIDs) that is frequently used in research settings and, importantly, also in routine clinical care. The overall benefits with odSITT generally exceeded the MCID of ≥2 units, were demonstrable already at the first follow-up visit (V2), and were sustained throughout the study period of 12 months, despite established prior dual (LAMA/LABA, LABA/ICS) or LAMA/LABA/ICS maintenance therapies. Importantly, the benefits of odSITT were most pronounced in patients with high baseline CAT scores (>20 units), and good or intermediate treatment adherence. The improvements in CAT in ELLITHE, in contrast to other large-scale trials,9,12,23,24 are unlikely to be driven by (frequent) exacerbations impacting health status, as the overall frequency of exacerbations in the prospective ELLITHE study period was very low (less than 10% of patients experiencing any exacerbation). Hence, the results of ELLITHE clearly underscore the potential of odSITT to improve symptomatic COPD even in the absence of exacerbations. These findings also challenge current national or international management strategies6,7 reserving the use of ICS-containing triple therapies only for patients experiencing exacerbations (GOLD group “E”). In the EU, available triple therapies are approved for the maintenance treatment of patients with moderate-to-severe COPD insufficiently controlled on dual or “open” triple inhaler therapies, which may or may not be defined by the occurrence of exacerbations.1–3 Thus, it is worthwhile to reconsider the role of LAMA/LABA/ICS therapies also in selected group “B” patients. In the KRONOS trial,25 benefits of SITT on multiple outcomes were observed in group B COPD patients without a history of exacerbations. A growing body of evidence has unanimously underscored the negative impact of moderate-to-severe exacerbations on disease progression in COPD.26 Even a single or first exacerbation accelerates lung function decline27 and is associated with increased long-term mortality.28 Escalation of inhaled therapy according to the current “treat-to-fail” strategy may therefore fall short in comprehensively addressing individual risk as part of a preventative approach. Risk-based management is an established, evidence-based strategy in numerous therapeutic areas including, eg, cardiovascular medicine,29 diabetes,30 or osteoporosis31 treatment. Identifying at-risk COPD patients prior to the occurrence of exacerbations is therefore pivotal to implement preventative interventions earlier in the course of the disease. While exacerbations are a main driver of mortality, morbidity and progression, other clinical characteristics are also independently associated with mortality and future exacerbations, such as low lung function, high symptom burden, frequent rescue inhaler use, elevated blood eosinophils or plasma fibrinogen, and presence of cardiovascular risk factors.32–36 The results from ELLITHE underscore the importance of prospective trials with triple therapies in group B patients stratified according to these established risk factors.
Despite a history of COPD exacerbations in the past, the prospective exacerbation rate during 12 months treatment with odSITT was extremely low. Although differences of historic and prospective annual exacerbation rates have been noted in other large-scale COPD and asthma trials,37,38 the observed rate difference exceeds published data by far. Besides optimized pharmacotherapeutic prevention of exacerbations by effective odSITT, the timing of the study during phases of restrictions and lockdowns due to the COVID-19 pandemic has likely significantly contributed to this finding. COPD exacerbations have dramatically declined during the pandemic in many regions globally due to restrictions or shielding measures, underscoring the importance of viral infections as main triggers of these events.39,40 It is also possible that some events were not reported due to limited access to health care during the pandemic, although this explanation seems unlikely for ELLITHE, where most patients attended regular follow-up visits. Nevertheless, the ELLITHE data impressively show that a significant and distinct reduction of moderate-to-severe exacerbations is possible in COPD patients by a combination of effective pharmacotherapy and non-pharmacological measures.
In addition to CAT score and exacerbations, spirometric benefits were also demonstrable at study end and approached 100 mL with odSITT versus baseline, an effect size estimated to be clinically important even when measured against placebo.41,42 These results are in line with data from well-controlled clinical studies, reporting improvements of similar magnitude compared to dual-combination therapies.9,10
Taken together, the add-on effects of therapy escalation with odSITT compared to prior dual therapies are likely the main driver for improvements. However, meaningful benefits were also observed in prior “triple” (SITT or MITT) users, similar to findings in the INTREPID study.14 In these patients, advantages of the individual pharmacological components of odSITT improved adherence or device handling/performance issues may have contributed to clinical effectiveness. Evidence from few direct non-inferiority studies has demonstrated better outcomes with, eg, UMEC/VI over other available LAMA/LABA combinations,43,44 and a recent network meta-analysis also showed greater improvements in lung function and exacerbations with odSITT versus other available SITTs.13 Importantly, ELLITHE study results on CAT score are in line with recent findings in a non-interventional study with a different, twice-daily SITT (beclomethasone/formoterol/glycopyrronium via pressurized metered dose inhaler).45 In this study, improvements in CAT score of 2.7 units were observed, with similar overall baseline CAT scores (21.5 units), although the observation period of 6 months was considerably shorter than in ELLITHE.
The main indication that drove physicians in ELLITHE to initiate odSITT was exacerbations. Notably, in a large number of patients “persistent symptoms” were also named as reason, besides adherence or inhaler issues. Perhaps surprisingly, a blood eosinophil count was not used to support initiation of triple therapy in the vast majority of patients. In fact, eosinophils were measured routinely only in a very small group of patients. In this subgroup, at least some physicians listed the eosinophil count as one parameter that supported the treatment decision. The reasons for this reluctance toward using eosinophils as biomarker in COPD are not clear. Contrary to guidelines, however, physicians appear to rely almost exclusively on clinical features when prescribing odSITT. Given the general availability, low cost and reasonable predictive value of eosinophils in COPD, more education may be needed to reinforce routine implementation of this biomarker in clinical practice.
Due to the character of the study design, there are also some important limitations, mainly the lack of a control group that would substantiate an estimate of, eg, potential Hawthorne or regression to the mean effects on main study outcomes.19,41,46,47 It is therefore important to note that benefits of odSITT on CAT - an established, yet subjective, patient-reported outcome measure - were backed by clinically meaningful improvements of FEV1, a robust, objective physiological marker reflecting airflow limitation. As with most real-world effectiveness studies, the identification of concise reasons behind the observed clinical benefits with odSITT is also somewhat limited. However, our data support possible contributions of ease of inhaler use, adherence, and dosing regime as well as pharmacological properties of active drugs. Importantly, with the non-interventional study design, patients were only observed within routine care. That is why study discontinuations and missing visits are more common. As in comparable observational-studies,45,48 the number of patients who discontinued the study or missed visits was relatively high. Again, this could have also resulted from patients’ cautiousness during the COVID-19 pandemic to reduce doctor’s appointments. Finally, the study is representative for the German health-care system, and results may not necessarily be applicable to other countries.
Conclusion
In summary, ELLITHE demonstrates rapid, sustained, and clinically meaningful improvements in CAT score and other important outcomes with odSITT in a large group of COPD patients treated in Germany under usual care conditions. The observed benefits over 12 months indicate that triple therapy should be considered in severely symptomatic COPD patients regardless of the occurrence of exacerbations, which is in contrast to current guideline recommendations.
Abbreviations
ADR, adverse drug reaction; AE, adverse event; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; FF, fluticasone furoate; FEV1, forced expiratory volume in one second; GOLD, The Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; MITT, multiple-inhaler triple therapy; mMRC, modified medical research council dyspnea scale; odSITT, once-daily single-inhaler triple therapy; SAE, serious adverse event; SD, standard deviation; TAI, test of the adherence to inhalers; UMEC, umeclidinium; VI, vilanterol.
Data Sharing Statement
Study synopsis and protocol are available at the BfArM-study registry DRKS. The data analyzed in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was carried out in accordance with Good Clinical Practice guidelines under the provisions of the latest version of the Declaration of Helsinki (2013) and received approval from the State Chamber of Physicians of Hesse as the ethics committee of the national chief investigator. The study was registered at the German Clinical Trials Register (DRKS00031897).
Acknowledgments
The authors would like to thank Dr. Robert Brinkmann (Medical Department, BERLIN-CHEMIE AG, Berlin, Germany) for support in conducting the study and preparation of manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. All authors engaged in drafting, revising or critically reviewing the article. They gave final approval of the version to be published and all versions before submission. All authors have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Funding
The ELLITHE study was funded by BERLIN-CHEMIE AG, Berlin, Germany.
Disclosure
Kai-Michael Beeh has received personal and/or institutional compensation for clinical research, consulting, lecturing fees from AstraZeneca, Boehringer Ingelheim, Bosch AG, GSK, Novartis, Menarini/Berlin Chemie and Chiesi; consulting and lecturing fees from Sanofi and Elpen; and consulting fees from Sterna. The authors report no other conflicts of interest in this work.
References
1. European Medicines Agency: EMA/697484/2018 – Elebrato Ellipta. Available from: https://www.ema.europa.eu/en/documents/overview/elebrato-ellipta-epar-medicine-overview_en.pdf.
2. European Medicines Agency: EMA/229136/2019 – Trimbow. Available from: https://www.ema.europa.eu/en/documents/overview/trimbow-epar-medicine-overview_en.pdf.
3. European Medicines Agency: EMA/561272/2020 – Trixeo Aerosphere. Available from: https://www.ema.europa.eu/en/documents/overview/trixeo-aerosphere-epar-medicine-overview_en.pdf.
4. Zhang S, King D, Rosen VM, Ismaila AS. Impact of Single Combination Inhaler versus Multiple Inhalers to Deliver the Same Medications for Patients with Asthma or COPD: a Systematic Literature Review. Int J Chron Obstruct Pulmon Dis. 2020;15:417–438. doi:10.2147/COPD.S234823
5. Mäkelä MJ, Backer V, Hedegaard M, Larsson K. Adherence to inhaled therapies, health outcomes and costs in patients with asthma and COPD. Respir Med. 2013;107(10):1481–1490.
6. Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie COPD – Leitlinienreport, 2. Auflage. Version 1; 2021. Available from: www.leitlinien.de/copd.
7. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2023 update. Available from: https://goldcopd.org/2023-gold-report-2/.
8. Singh D, Agusti A, Anzueto A, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
9. Lipson DA, Barnhart F, Brealey N, et al. Once-Daily Single-Inhaler Triple versus Dual Therapy in Patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
10. Lipson DA, Barnacle H, Birk R, et al. FULFIL Trial: once-Daily Triple Therapy for Patients with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2017;196(4):438–446. doi:10.1164/rccm.201703-0449OC
11. Lipson DA, Crim C, Criner GJ, et al. Reduction in All-Cause Mortality with Fluticasone Furoate/Umeclidinium/Vilanterol in Patients with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2020;201(12):1508–1516. doi:10.1164/rccm.201911-2207OC
12. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple Inhaled Therapy at Two Glucocorticoid Doses in Moderate-to-Very-Severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
13. Ismaila AS, Haeussler K, Czira A, et al. Fluticasone Furoate/Umeclidinium/Vilanterol (FF/UMEC/VI) Triple Therapy Compared with Other Therapies for the Treatment of COPD: a Network Meta-Analysis. Adv Ther. 2022;39(9):3957–3978. doi:10.1007/s12325-022-02231-0
14. Halpin DMG, Worsley S, Ismaila AS, et al. INTREPID: single- versus multiple-inhaler triple therapy for COPD in usual clinical practice. ERJ Open Research. 2021;7(2). doi:10.1183/23120541.00950-2020
15. Halpin DM, Kerkhof M, Soriano JB, Mikkelsen H, Price DB. Eligibility of real-life patients with COPD for inclusion in trials of inhaled long-acting bronchodilator therapy. Respir Res. 2016;17(1):120. doi:10.1186/s12931-016-0433-5
16. Treweek S, Zwarenstein M. Making trials matter: pragmatic and explanatory trials and the problem of applicability. Trials. 2009;10():37. doi:10.1186/1745-6215-10-37
17. Vestbo J, Leather D, Diar Bakerly N, et al. Effectiveness of Fluticasone Furoate-Vilanterol for COPD in Clinical Practice. N Engl J Med. 2016;375(13):1253–1260. doi:10.1056/NEJMoa1608033
18. Heddini A, Sundh J, Ekström M, Janson C. Effectiveness trials: critical data to help understand how respiratory medicines really work? Eur Clinical Respir J. 2019;6(1):1565804. doi:10.1080/20018525.2019.1565804
19. Pate A, Barrowman M, Webb D, et al. Study investigating the generalisability of a COPD trial based in primary care (Salford Lung Study) and the presence of a Hawthorne effect. BMJ Open Respir Res. 2018;5(1):e000339. doi:10.1136/bmjresp-2018-000339
20. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
21. Plaza V, Fernández-Rodríguez C, Melero C, et al. Validation of the ‘Test of the Adherence to Inhalers’ (TAI) for Asthma and COPD Patients. J Aerosol Med Pulm Drug Deliv. 2016;29(2):142–152. doi:10.1089/jamp.2015.1212
22. Kon SS, Canavan JL, Jones SE, et al. Minimum clinically important difference for the COPD Assessment Test: a prospective analysis. Lancet Respir Med. 2014;2(3):195–203. doi:10.1016/S2213-2600(14)70001-3
23. Calverley PMA, Anzueto AR, Carter K, et al. Tiotropium and olodaterol in the prevention of chronic obstructive pulmonary disease exacerbations (DYNAGITO): a double-blind, randomised, parallel-group, active-controlled trial. Lancet Respir Med. 2018;6(5):337–344. doi:10.1016/S2213-2600(18)30102-4
24. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
25. Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, Phase 3 randomised controlled trial. Lancet Respir Med. 2018;6(10):747–758. doi:10.1016/S2213-2600(18)30327-8
26. Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
27. Dransfield MT, Kunisaki KM, Strand MJ, et al. Acute Exacerbations and Lung Function Loss in Smokers with and without Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2017;195(3):324–330. doi:10.1164/rccm.201605-1014OC
28. Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural History of Chronic Obstructive Pulmonary Disease Exacerbations in a General Practice-based Population with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
29. Del Pinto R, Giua C, Keber E, Grippa E, Tilotta M, Ferri C. Impact of 2021 ESC Guidelines for Cardiovascular Disease Prevention on Hypertensive Patients Risk: secondary Analysis of Save Your Heart Study. High Blood Press Cardiovasc Prev. 2023;30(2):167–173. doi:10.1007/s40292-023-00568-3
30. Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2022;65(12):1925–1966. doi:10.1007/s00125-022-05787-2
31. Kanis JA, Cooper C, Rizzoli R, Reginster JY. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2019;30(1):3–44. doi:10.1007/s00198-018-4704-5
32. Singh D, Hurst JR, Martinez FJ, et al. Predictive modeling of COPD exacerbation rates using baseline risk factors. Ther Adv Respir Dis. 2022;16:17534666221107314. doi:10.1177/17534666221107314
33. Singh D, Criner GJ, Dransfield MT, et al. InforMing the PAthway of COPD Treatment (IMPACT) trial: fibrinogen levels predict risk of moderate or severe exacerbations. Respir Res. 2021;22(1):130. doi:10.1186/s12931-021-01706-y
34. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to Exacerbation in Chronic Obstructive Pulmonary Disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
35. Celli BR, Locantore N, Yates J, et al. Inflammatory Biomarkers Improve Clinical Prediction of Mortality in Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2012;185(10):1065–1072. doi:10.1164/rccm.201110-1792OC
36. Vestbo J, Anderson JA, Brook RD, et al. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): a double-blind randomised controlled trial. Lancet. 2016;387(10030):1817–1826. doi:10.1016/S0140-6736(16)30069-1
37. Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol–Glycopyrronium versus Salmeterol–Fluticasone for COPD. N Engl J Med. 2016;374(23):2222–2234. doi:10.1056/NEJMoa1516385
38. Ortega HG, Liu MC, Pavord ID, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014;371(13):1198–1207. doi:10.1056/NEJMoa1403290
39. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Reduction in hospitalised COPD exacerbations during COVID-19: a systematic review and meta-analysis. PLoS One. 2021;16(8):e0255659. doi:10.1371/journal.pone.0255659
40. Dezman ZDW, Stryckman B, Zachrison KS, et al. Masking for COVID-19 Is Associated with Decreased Emergency Department Utilization for Non-COVID Viral Illnesses and Respiratory Conditions in Maryland. Am J Med. 2021;134(10):1247–1251. doi:10.1016/j.amjmed.2021.06.008
41. Jones PW, Beeh KM, Chapman KR, Decramer M, Mahler DA, Wedzicha JA. Minimal Clinically Important Differences in Pharmacological Trials. Am J Respir Crit Care Med. 2014;189(3):250–255. doi:10.1164/rccm.201310-1863PP
42. Cazzola M, MacNee W, Martinez FJ, et al. Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J. 2008;31(2):416–469. doi:10.1183/09031936.00099306
43. Maltais F, Ferguson GT, Feldman GJ, et al. A Randomized, Double-Blind, Double-Dummy Study of Glycopyrrolate/Formoterol Fumarate Metered Dose Inhaler Relative to Umeclidinium/Vilanterol Dry Powder Inhaler in COPD. Adv Ther. 2019;36(9):2434–2449. doi:10.1007/s12325-019-01015-3
44. Feldman GJ, Sousa AR, Lipson DA, et al. Comparative Efficacy of Once-Daily Umeclidinium/Vilanterol and Tiotropium/Olodaterol Therapy in Symptomatic Chronic Obstructive Pulmonary Disease: a Randomized Study. Adv Ther. 2017;34(11):2518–2533. doi:10.1007/s12325-017-0626-4
45. Gessner C, Trinkmann F, Bahari Javan S, et al. Effectiveness of Extrafine Single Inhaler Triple Therapy in Chronic Obstructive Pulmonary Disease (COPD) in Germany - The TriOptimize Study. Int J Chron Obstruct Pulmon Dis. 2022;17:3019–3031. doi:10.2147/COPD.S382405
46. Sciurba F, Rennard SI. Rationale for a redundant formulary. The Hawthorne effect and the art of medicine. Am J Respir Crit Care Med. 2015;191(11):1224–1225. doi:10.1164/rccm.201503-0496ED
47. Bland JM, Altman DG. Regression towards the mean. BMJ. 1994;308(6942):1499. doi:10.1136/bmj.308.6942.1499
48. Plate T, Friedrich FW, Beier J. Effectiveness and Tolerability of LABA/LAMA Fixed-Dose Combinations Aclidinium/Formoterol, Glycopyrronium/Indacaterol and Umeclidinium/Vilanterol in the Treatment of COPD in Daily Practice - Results of the Non-Interventional DETECT Study. Int J Chron Obstruct Pulmon Dis. 2020;15:1335–1347. doi:10.2147/COPD.S252354
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.