Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Real-World Eculizumab Dosing Patterns Among Patients with Paroxysmal Nocturnal Hemoglobinuria in a US Population
Authors Cheng WY, Sarda SP, Mody-Patel N, Krishnan S, Yenikomshian M, Kunzweiler C, Vu JD, Cheung HC ![]() , Duh MS
, Duh MS ![]()
Received 6 November 2021
Accepted for publication 12 April 2022
Published 3 May 2022 Volume 2022:14 Pages 357—369
DOI https://doi.org/10.2147/CEOR.S346816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Wendy Y Cheng,1 Sujata P Sarda,2 Nikita Mody-Patel,2 Sangeeta Krishnan,2 Mihran Yenikomshian,1 Colin Kunzweiler,1 Jensen Duy Vu,1 Hoi Ching Cheung,1 Mei Sheng Duh1
1Analysis Group, Inc., Boston, MA, USA; 2Apellis Pharmaceuticals, Inc., Waltham, MA, USA
Correspondence: Wendy Y Cheng, Analysis Group, Inc., 111 Huntington Ave, 14th Floor, Boston, MA, 02199, USA, Tel +1 617 425 8219, Fax +1 617 425 8000, Email [email protected]
Purpose: Current pharmacologic management of paroxysmal nocturnal hemoglobinuria (PNH) consists of C5 inhibitors, eculizumab and ravulizumab; however, because patients experience incomplete symptom control, off-label doses may be utilized. We conducted a retrospective, longitudinal cohort study of provider-based claims data to assess the real-world eculizumab dosing patterns in PNH patients.
Patients and Methods: Patients were ≥ 12 years, received ≥ 2 eculizumab infusions between January 1, 2015 and September 30, 2019, and had ≥ 3 months of continuous clinical activity prior to index. The index date was the first claim for eculizumab. Patients with ≥ 1 diagnosis of another indication for eculizumab were excluded. Treatment patterns including the proportion with high, label-recommended, and low dosages during induction (first 28 days) and maintenance (beginning day 29) phases were described. The proportion and time-to-first dose escalation, defined as an increase in dose or frequency of infusion, were assessed among a subset of patients (ie, escalation analysis cohort).
Results: A total of 707 patients were examined. Mean (standard deviation [SD]) starting dose was 862mg (412mg) and was higher than label-recommended 600mg for 64% of the patients. Mean (SD) dose per infusion was 859mg (391mg) during the induction phase; average dose was higher than label-recommended 600mg for 68%. Mean (SD) dose per infusion during the maintenance phase was 1005mg (335mg); average dose was higher than label-recommended 900mg for 43%. Dose escalation occurred in 40/121 escalation analysis cohort patients. Median time-to-first dose escalation was ∼ 12 months.
Conclusion: Results suggest that deviations from label-recommended dosing patterns were common. Future budget impact assessments of eculizumab should account for real-world dosing patterns to comprehensively assess costs and benefits.
Keywords: complement inhibitors, dose escalation, dosing patterns, eculizumab, paroxysmal nocturnal hemoglobinuria
Introduction
Paroxysmal nocturnal hemoglobinuria (PNH) is an acquired, chronic, rare, and potentially life-threatening disorder that results from the destruction of blood cells by the complement system due to the absence of complement inhibiting proteins on the cell’s surface.1 In the United States (US), the prevalence of PNH has been estimated to be 12–13 cases per 1,000,000 individuals.2 Although PNH is an acquired disease that can affect any age group, patients are commonly diagnosed in their early 30s.3 Clinical manifestations of PNH include hemolytic anemia, thrombosis, bone marrow failure, abdominal pain, and hemoglobinuria.4
Currently, the C5 inhibitors eculizumab and ravulizumab, both humanized monoclonal antibodies that interfere with C5 thus blocking complement-activated hemolysis, have received approval by the US Food and Drug Administration (FDA) to treat PNH.4,5 Due to the limited real-world data currently available for ravulizumab (approval was in December 2018), our analysis sought to evaluate eculizumab, the first-to-market treatment for PNH, given its broader long term use among patients with PNH. Available as an intravenous infusion, eculizumab is administered in two phases: an induction phase (standard dosage: 600 mg/week for the first 4 weeks) and a maintenance phase (900 mg for the fifth dose 1 week later, and 900 mg every 2 weeks thereafter).5 The standard two-phase dosing regimen is aimed to maintain eculizumab serum concentration >35 μg/mL, which has been shown in clinical trials to be sufficient to ensure complete and consistent blockade of complement-mediated intravascular hemolysis in most patients with PNH.6 Yet despite significant reductions in complement-mediated hemolysis and associated symptoms observed in clinical trials,7–12 many patients do not experience sustained symptom control with the label-recommended eculizumab dosage.7,13–15
To address PNH symptoms related to breakthrough hemolysis (BTH) and reestablish complete complement blockade, clinicians may modify the dosing schedule of eculizumab via an increase in dosage, frequency of infusions, or both (referred to as “dose escalation” in the present study).16–20 For example, in an analysis of 195 clinical trial patients receiving eculizumab, 21 (10.8%) patients had a median of 22 reductions (range: 3–124) in dose interval (ie, reducing time between infusions to <14 days) following inadequate symptom control.11 Additionally, in response to BTH among a small number of clinical trial patients, clinicians examined alternative eculizumab dosing schedules, including modifications to frequency (ie, reducing the number of days between infusions) and dosage (ie, increasing dosage per infusion to 1200 mg) during the induction and maintenance phases.14 Other events that may prompt clinicians to escalate the dose of eculizumab include variations in patient’s body weight,21 transfusion dependence,12 breakthrough thrombosis,22 and recurrence of PNH symptoms prior to the administration of the new dose.20 However, there is limited evidence regarding eculizumab dosing patterns, particularly dose escalation, in the real-world settings. A retrospective, single-center study of 30 patients with PNH who were treated with eculizumab found that 2 (6.7%) of 30 patients required repeated dose escalations in order to adequately manage symptoms related to intravascular hemolysis.13 Despite dose escalation to 1200 mg every 12 days, followed by 1500 mg every 12–14 days, both patients reported a return of BTH symptoms by day 10 or 11 of the dosing schedule.13 As these studies demonstrate that dose escalation occurs for patients with PNH, additional doses may result in increased costs, which can be better understood by examining real-world dosing patterns.
Given the lack of information on the treatment for PNH with eculizumab in the real world, a comprehensive assessment of the dosing patterns of eculizumab in a large, nationally representative real-world patient population is needed to understand the clinical unmet needs among patients with PNH. The present study evaluated dosing patterns among patients with PNH who were treated with eculizumab using a health insurance claims database in the US.
Materials and Methods
Data Source
This study used data from Symphony Health IDV® (Integrated Dataverse; October 1, 2014 to September 30, 2019). Symphony Health IDV is a large nationally representative claims database covering approximately 280 million US beneficiaries each year and represents over 73% of specialty prescriptions, 58% of medical claims, and 30% of hospital claims volume in the US. Symphony Health IDV aggregates data from physician practices, outpatient (OP) and specialty pharmacies, and hospitals to provide a longitudinal view of patient treatment patterns across all payer types. Thus, the Symphony database provides relevant information about IV medications ordered which were of particular interest to this study. All data contained in the database are de-identified and compliant with the patient confidentiality requirements of the Health Insurance Portability and Accountability Act. Institutional review board approval was not required for this study.
Study Design
This retrospective, longitudinal, cohort study was conducted using data from medical and pharmacy claims. The date of the first eculizumab infusion occurring on or after January 1, 2015, was used to define the index date. Patients had ≥3 months of continuous clinical activity prior to the index date, which was used to define the baseline period. The observation period for each patient spanned from the index date to the end of continuous clinical activity or end of data availability, whichever occurred first.
Eculizumab dosing patterns were examined during each patient’s treatment period, which was defined as the period from the index date to the date of the last infusion of eculizumab prior to treatment discontinuation, end of continuous clinical activity, or end of data availability, whichever was earlier. The induction phase was the first 28 days following the index date, which corresponds with weekly infusions for the first 4 weeks per the approved labeling. The maintenance phase started on day 29 after the index date. Similar to a previous real-world study of insurance claims data, treatment discontinuation was defined as a gap of >42 days between eculizumab infusions (which reflects a 14-day exposure period plus 28-day grace period between infusions, and is equivalent to missing two infusions based on the biweekly schedule of eculizumab), or between the last infusion and the end of the observation period.2
Sample Selection
To be included in this study, patients were required to meet the following criteria: have ≥2 or more medical claims for infusion of eculizumab (identified using Healthcare Common Procedure Coding System [HCPCS] code J1300) between January 1, 2015 and September 30, 2019; have data available for a minimum of 3 months of continuous clinical activity prior to the index date (ie, baseline period); and be ≥12 years of age on the index date. Patients were excluded if they had (a) ≥1 medical claim for infusion of eculizumab prior to January 1, 2015 or (b) ≥1 diagnosis of another indication for eculizumab during the baseline period or on the index date as identified based on diagnosis codes from the International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification (ICD-9/10-CM) that included atypical hemolytic uremic syndrome (ICD-9-CM: 283.11; ICD-10-CM: D59.3), generalized myasthenia gravis (ICD-9-CM: 358.0; ICD-10-CM: G70.0x), and/or neuromyelitis optica spectrum disorder (ICD-9-CM: 341.0; ICD-10-CM: G36.0). This constituted the overall cohort. Because the ICD-9 diagnosis code for PNH is an imprecise, broad code that encompasses other related diagnoses, this inclusion by exclusion principle as shown in exclusion criterion (b), in which patients were excluded if they had ≥1 diagnosis of another indication of eculizumab, rather than a conventional approach of including patients with ≥1 diagnosis of PNH, helps to improve specificity of the treated population and ensure that eculizumab was given for the indication of PNH. Patients who received ravulizumab were not assessed in this study given that the current data were available through September 2019 and the HCPCS J-code was not effective until October 2019.
Per FDA prescribing information, patients with PNH initiating treatment with eculizumab, a C5 inhibitor, receive four weekly infusions during the induction phase. Dose escalation was assessed during the maintenance phase and was restricted to a subset of patients from the overall cohort (referred to as the “escalation analysis cohort”) with a label-recommended induction phase (ie, received exactly four infusions of 600 mg eculizumab, each 7 days ± 2 days apart) and ≥1 infusion of eculizumab during the maintenance phase.
Baseline Characteristics
Patient demographics assessed at index date included age, sex, year of first eculizumab infusion, geographic region of residence, and insurance plan type. Clinical characteristics assessed during the 3-month baseline period prior to the index date included the Quan-Charlson Comorbidity Index (Quan-CCI),23 Elixhauser comorbidities (Supplemental Table 1),23 PNH-related comorbidities (ie, aplastic anemia and myelodysplastic syndrome), PNH-related symptoms (ie, anemia other than aplastic anemia, viral and bacterial infections, chronic kidney disease, fatigue, abdominal pain, dyspnea, thrombosis, pulmonary hypertension, dysphagia, and erectile dysfunction), use of PNH-related treatments (ie, corticosteroid therapy, blood transfusions, anticoagulants, immunosuppressants, iron therapy, iron-chelation therapy, and androgen therapy), as well as all-cause and PNH-related healthcare resource utilization (HRU). Specific diagnosis codes, drug codes, and procedure codes used to identify these characteristics are provided in the online electronic Supplemental Tables 2–10.
Study Outcomes
Dosing Patterns
All eculizumab infusions received during the first 4 days beginning on the index date were summed and considered the starting dose. The number and proportion of patients with a high (>600 mg), label-recommended (600 mg), or low (<600 mg) starting dose were assessed. The number of infusions received, average number of days between infusions by patient, average dose per infusion by patient, and the number and proportion of patients with a high (>600 mg during the induction phase, >900 mg during the maintenance phase), label-recommended (600 mg during the induction phase, 900 mg during the maintenance phase), or low (<600 mg during the induction phase, <900 mg during the maintenance phase) average dose per infusion were assessed during the induction phase and maintenance phase.
Dose Escalation
For patients in the escalation analysis cohort, additional outcomes that were assessed included the proportions of patients with ≥1 and ≥2 episodes of dose escalation, time-to-first dose escalation, and probability of dose escalation by the end of 3, 6, 9, and 12 months following the index date. Dose escalation during the maintenance phase was defined as either an increase in dose (ie, receiving >900 mg on a single infusion day) or an increase in frequency of infusion (ie, receiving >900 mg of eculizumab within 12 days); consecutive escalated doses were considered part of the same dose escalation episode. Given that the FDA prescribing information allows for the administration of eculizumab within 2 days of the recommended dosage regimen time points,5 infusions administered 12–16 days apart during the maintenance phase were considered to be consistent with the label recommendation.
Statistical Analyses
Descriptive summary statistics (eg, mean, median, standard deviation [SD], interquartile range [IQR]) were generated for baseline characteristics, eculizumab dosing patterns, and dose escalation outcomes, as applicable. For patients in the escalation analysis cohort, the time-to-first dose escalation was evaluated using Kaplan–Meier methodology, which censored patients at the end of continuous eculizumab treatment, continuous clinical activity, or end of data availability. All analyses were conducted using SAS Enterprise Guide v7.1 (Cary, NC).
Results
Of the 3057 patients with ≥2 medical claims for infusion of eculizumab between January 1, 2015 and September 30, 2019, a total of 707 patients were included in the overall study sample (Figure 1). Patients were included in the overall cohort after excluding those who did not have ≥3 months of continuous eligibility before the index date (n=318), were not ≥12 years of age on the index date (n=168), had ≥1 medical claim for infusion of eculizumab any time prior to the index date (n=520), or had ≥1 diagnosis of another indication (ie, not PNH) for eculizumab during the baseline period or on the index date (n=1344). Furthermore, among the overall study sample, 121 patients were included in the escalation analysis cohort (ie, these patients received four weekly 600 mg infusions of eculizumab during the induction phase and received ≥1 infusions of eculizumab during the maintenance phase).
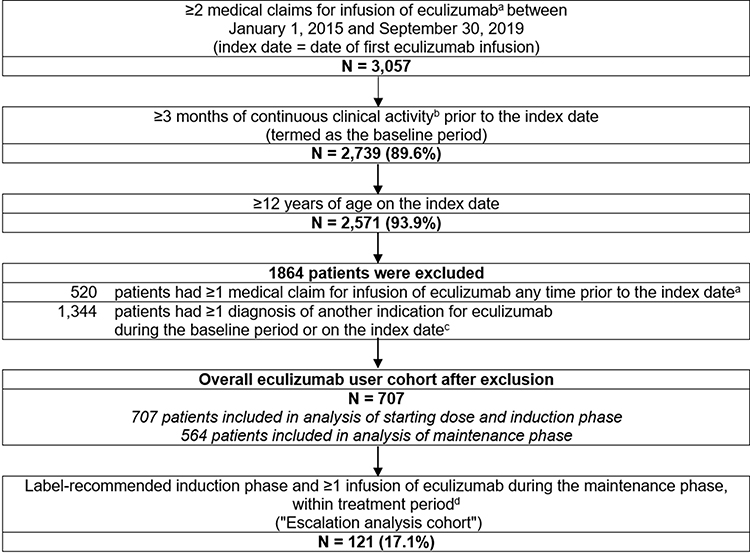 |
Figure 1 Patient disposition. Abbreviations: HCPCS, Healthcare Common Procedure Coding System; ICD-9-CM, International Classification of Diseases, 9th Revision, Clinical Modification; ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification; PNH, paroxysmal nocturnal hemoglobinuria. Notes: aEculizumab was identified using the HCPCS procedure code J1300. bClinical activity was measured in increments of calendar year quarters and was used as a proxy for health plan enrollment given the lack of eligibility files in Symphony Health IDV database; a patient was considered to be active for the quarter if there was ≥1 claim of any type (ie, medical or prescription) during the quarter. cOther indications of eculizumab include atypical hemolytic uremic syndrome (ICD-9-CM: 283.11; ICD-10-CM: D59.3), generalized myasthenia gravis (ICD-9-CM: 358.0; ICD-10-CM: G70.0x), and neuromyelitis optica spectrum disorder (ICD-9-CM: 341.0; ICD-10-CM: G36.0). dThe escalation analysis cohort is a subset of patients from the overall eculizumab cohort who had a label-recommended induction phase (ie, received 4 doses of 600 mg eculizumab infusion, each 7 days ±2 days apart) and received ≥1 dose of eculizumab infusion during treatment in the maintenance phase. The treatment period was defined as the period from the index date (ie, date of first eculizumab infusion) to the date of the last infusion of eculizumab prior to treatment discontinuation, end of continuous clinical activity, or end of data availability, whichever was the earliest. Discontinuation was defined as a gap of >42 days between eculizumab infusions, or between the last infusion and the end of observation period. |
Baseline Characteristics
Among all patients, mean age was 45.4 years, and 55.7% were female (Table 1). Additionally, the majority of patients (77.1%) were insured through a commercial insurance plan. More than a quarter (29.3%) of the overall sample had a claim with aplastic anemia diagnosis during the 3-month baseline period. Several PNH-related symptoms were also common during the baseline period including anemia other than aplastic anemia (43.1%), viral and bacterial infections (22.5%), and chronic kidney disease (16.7%). The prevalence of Elixhauser comorbidities during the baseline period are presented in Supplementary Table 1; the most frequent comorbidities included hypertension (25.5%), coagulopathy (24.3%), and renal failure (18.0%). Among all patients, 83.2% and 46.7% of the patients had ≥1 all-cause and PNH-related OP visits during baseline, respectively; 26.2% and 6.6% of the patients had ≥1 all-cause and PNH-related hospitalization during baseline, respectively. Mean number of all-cause and PNH-related hospitalizations was 0.6 and 0.1, respectively, while the mean number of all-cause and PNH-related OP visits was 7.3 visits and 1.4 visits, respectively.
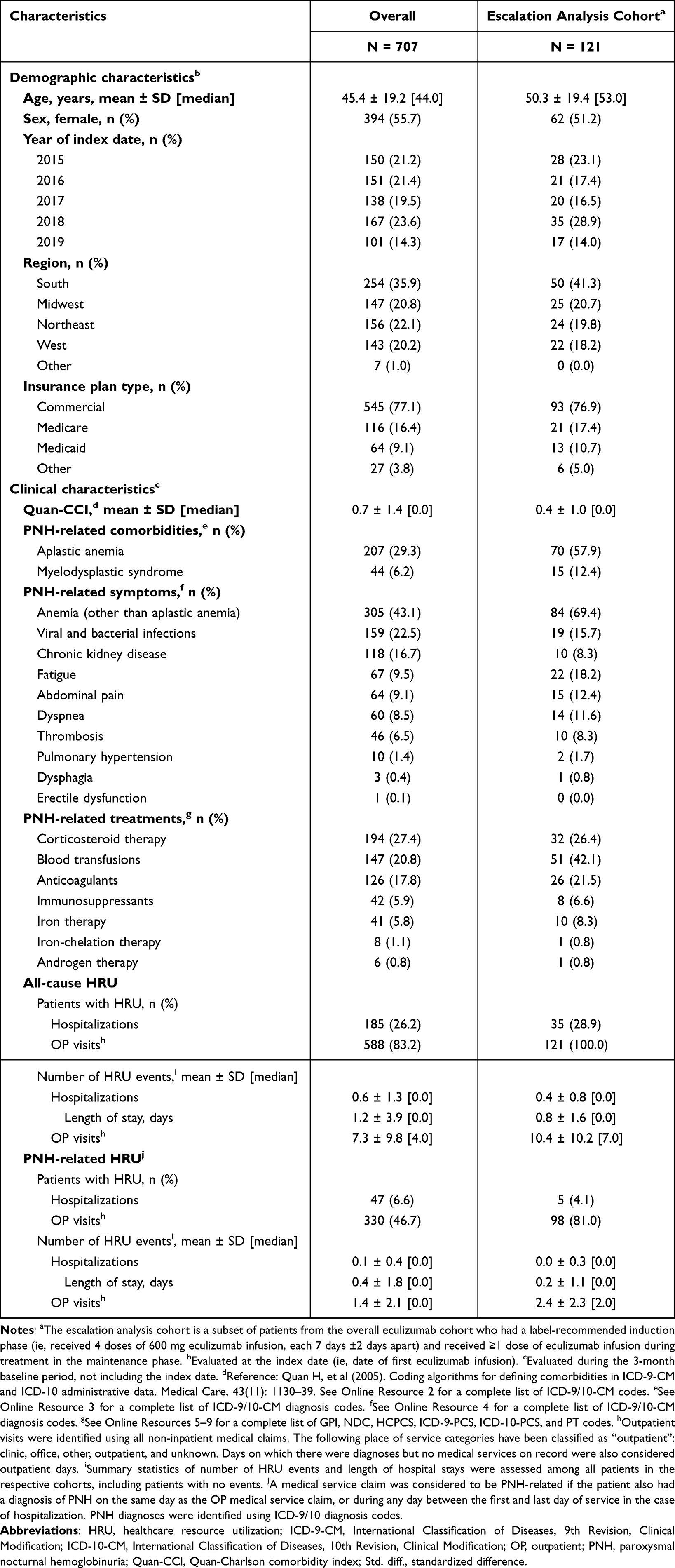 |
Table 1 Baseline Demographic and Clinical Characteristics, Overall and Among the Escalation Analysis Cohort |
Patients included in the escalation analysis cohort had a mean age of 50.3 years, and 51.2% were female. Among the 121 patients included in the escalation analysis cohort, the prevalence of aplastic anemia and myelodysplastic syndrome during the baseline period was 57.9% and 12.4%, respectively. Additionally, 69.4% of the patients reported anemia other than aplastic anemia. As shown in Online Resource 1, the most frequent Elixhauser comorbidities in the escalation analysis cohort were coagulopathy (39.7%), hypertension (24.8%), and deficiency anemias (19.0%).
Dosing Patterns
Among all patients, median length of the treatment period, defined as the period between the index date and the date of the last infusion of eculizumab prior to treatment discontinuation, end of continuous clinical activity, or end of data availability, was 4.5 months (Table 2). The mean (SD) starting dose was 861.7 mg (411.8 mg), with median 900 mg (IQR [Q1, Q3]: 600 mg, 900 mg). The majority of patients (64.1%) had a starting dose that was higher than the label-recommended 600 mg, while less than one-third (30.6%) received the label-recommended starting dose of 600 mg. About 75% of the patients in the overall cohort discontinued treatment, with a median time from index date to discontinuation of 6.0 months (data not shown).
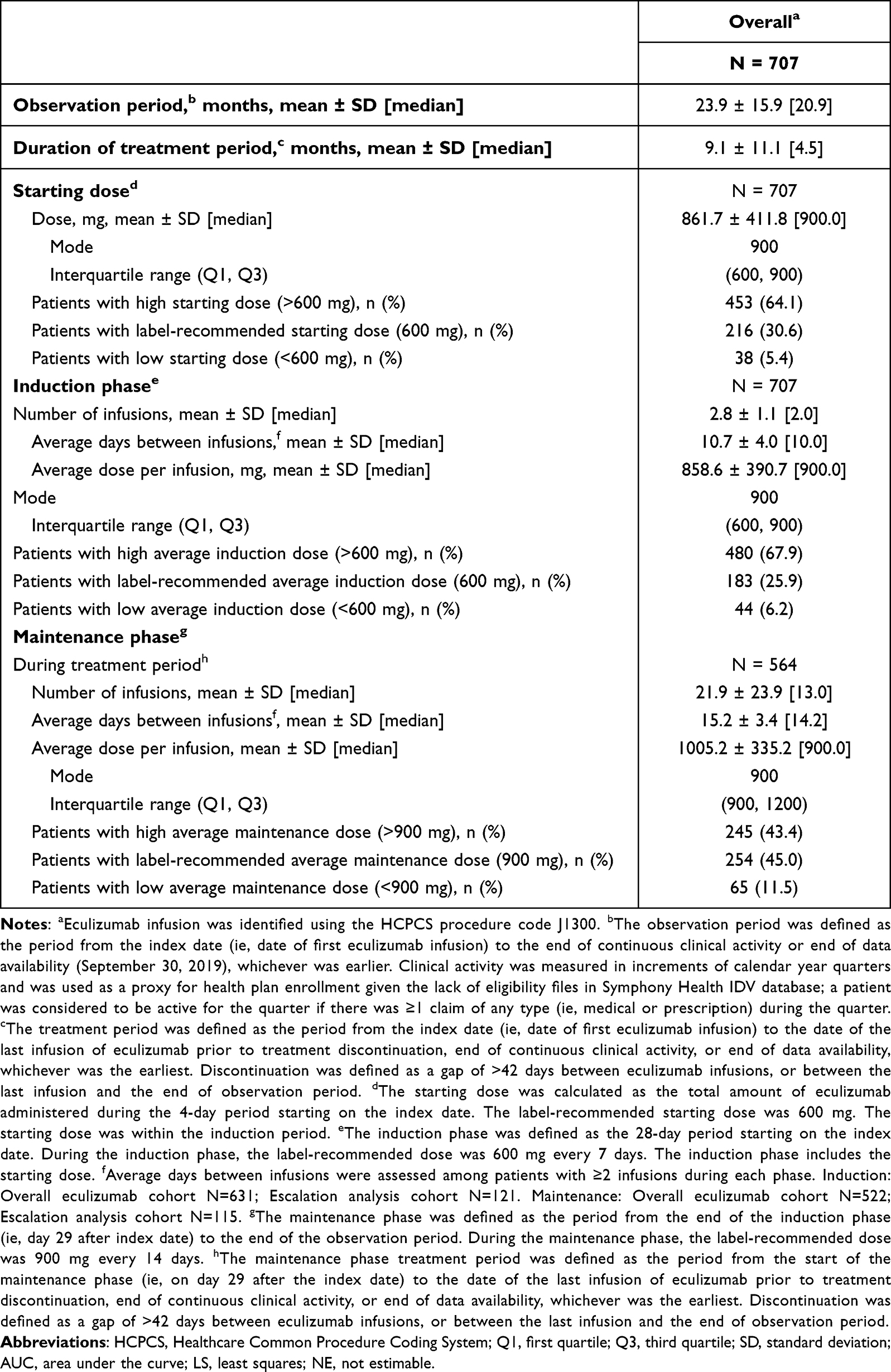 |
Table 2 Eculizumab Dosing Patterns (N=707) |
During the induction phase, all patients received a mean (SD) of 2.8 (1.1) infusions (the eculizumab prescribing information recommends four weekly infusions during this period), and the mean (SD) number of days between infusions was 10.7 days (4.0 days) (Table 2). The average (SD) dose per infusion during the induction phase was 858.6 mg (390.7 mg), with median dose of 900 mg (IQR [Q1, Q3]: 600 mg, 900 mg). The proportion of patients whose average dose per infusion during the induction phase was high (>600 mg), label-recommended (600 mg), and low (<600 mg) was 67.9%, 25.9%, and 6.2%, respectively.
Of the 707 patients included in this analysis, 564 (79.8%) patients had ≥1 doses of eculizumab during the maintenance phase (Table 2). Patients had a mean (SD) of 21.9 (23.9) infusions, and a median of 13.0 infusions during the maintenance phase. Mean (SD) number of days between infusions during the treatment period was 15.2 (3.4) days. The average (SD) dose per infusion during the maintenance phase was 1005.2 mg (335.2 mg); median was 900 mg (IQR [Q1, Q3]: 900 mg, 1200 mg). The proportion of patients whose average dose per infusion during the treatment period was high (>900 mg), label-recommended (900 mg), and low (<900 mg) was 43.4%, 45.0%, and 11.5%, respectively.
Dose Escalation
Among patients in the escalation analysis cohort (N=121), mean (SD) number of infusions during the maintenance phase was 22.2 (24.5); patients had a median of 12.0 infusions (data not shown). Time between infusions was approximately 2 weeks apart (mean ± SD [median]: 14.4 days ± 1.8 days [14.0 days]). Average (SD) dose per infusion was 933.5 mg ± 100.4 mg (median: 900 mg; IQR [Q1, Q3]: 900, 900 mg), and the average maintenance dose during the treatment period was the label-recommended 900 mg for most patients (72.7%).
Within the escalation analysis cohort, 40 patients (33.1%) had ≥1 and 15 patients (12.4%) had ≥2 episodes of dose escalation (Table 3). Among 40 patients with ≥1 dose escalation episodes, median time-to-first dose escalation was 4.2 months (mean: 7.3 months; SD: 9.0 months). Using Kaplan–Meier methodology, the median time-to-first dose escalation was 12.3 months among the escalation analysis cohort (Figure 2). The probability of experiencing a dose escalation was 13.6%, 26.9%, 36.3%, and 47.4% by the end of 3, 6, 9, and 12 months after eculizumab initiation, respectively (Table 3).
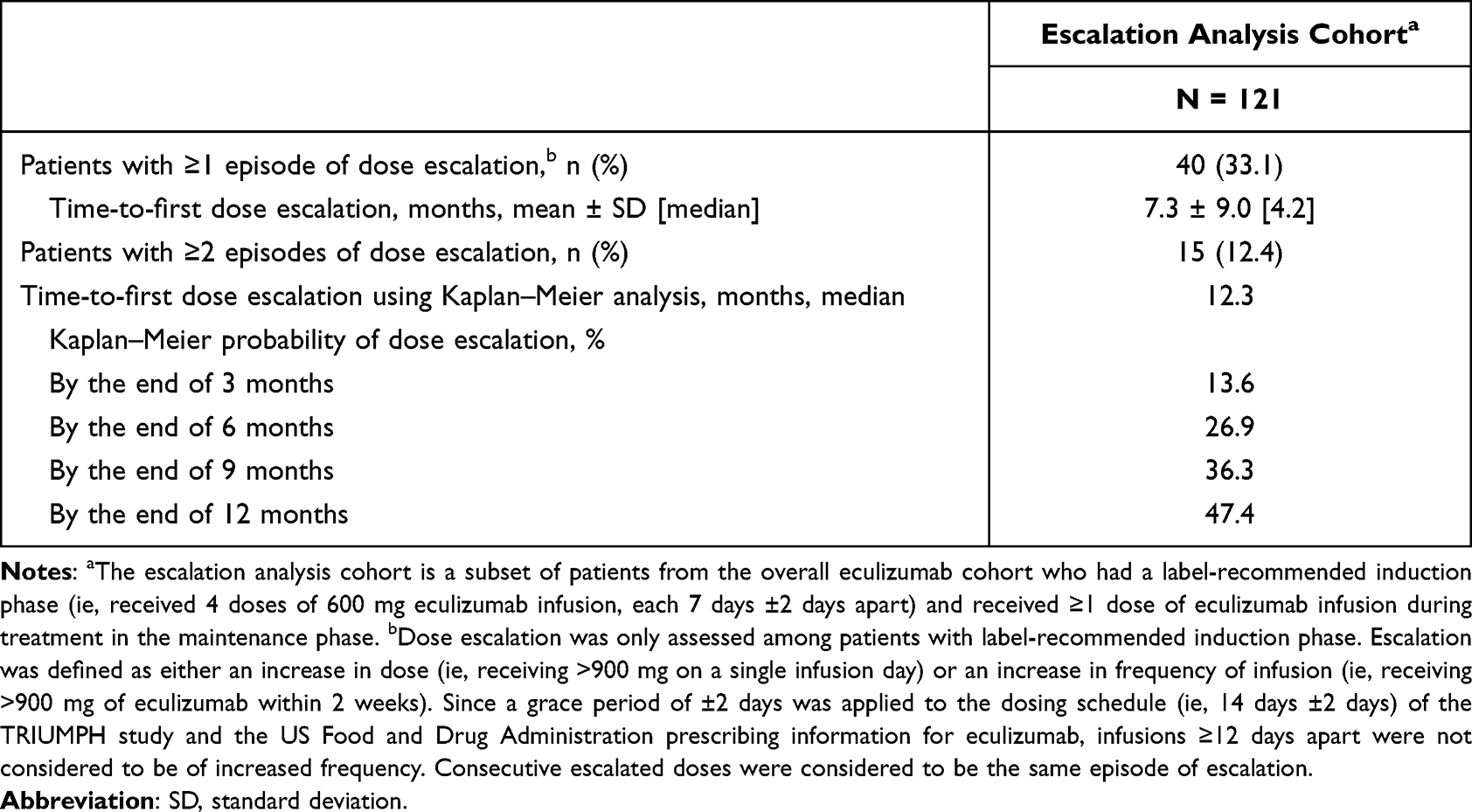 |
Table 3 Dose Escalation Among the Escalation Analysis Cohort (N=121) |
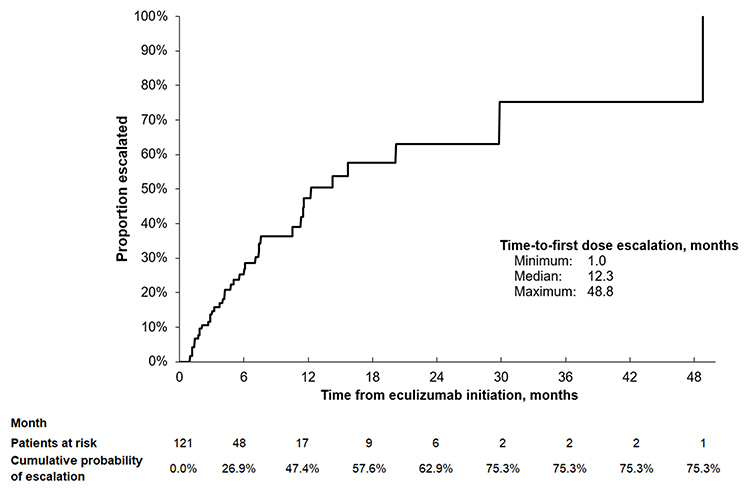 |
Figure 2 Time-to-first dose escalation among the escalation analysis cohort (n=121).a Notes: aDose escalation was only assessed among patients with label-recommended induction phase. Escalation was defined as either an increase in dose (ie, receiving >900 mg on a single infusion day) or an increase in frequency of infusion (ie, receiving >900 mg of eculizumab within 2 weeks). Since a grace period of ±2 days was applied to the dosing schedule (ie, 14 days ±2 days) of the TRIUMPH study and the US Food and Drug Administration prescribing information for eculizumab, infusions ≥12 days apart were not considered to be of increased frequency. |
Discussion
C5 complement inhibitors such as eculizumab and ravulizumab are the only FDA-approved drugs for treatment of PNH. While the efficacy and safety of eculizumab have been evaluated in multinational clinical trials, there is a paucity of evidence that critically examines its use in real-world settings. This study examined the real-world dosing patterns and dose escalation among a sample of 707 patients with PNH receiving eculizumab through a large provider-based claims database. The results of this study suggest that deviations from the label-recommended dose schedule are common. Moreover, dose escalations occur shortly after initiation of treatment.
The majority of patients examined in this study received a higher starting dose (64.1%, n=453/707) and had a higher average dose during the induction phase (67.9%, n=480/707) than what is recommended in the label. In addition, nearly half of patients (43.4%, n=245/564) had an average dose during the maintenance phase that was higher than the label-recommended dose of 900 mg. Only a small portion of patients (17.1%) in this cohort completed a label-recommended induction phase of four weekly infusions of 600 mg, and among the 121 patients with a label-recommended induction phase, 1 in 3 experienced ≥1 dose escalation episodes. Thus, the results of this study demonstrate that the standard eculizumab dosing schedule is insufficient in real-world practice. Because C5 inhibitors address intravascular, but not extravascular hemolysis, the inability to completely control complement-mediated hemolysis may be due to the mechanism of action of eculizumab.
We were unable to assess reasons for dose escalation in this study; based on the data source analyzed, clinical measures that may have been indicators of treatment adjustments were unavailable. Although we cannot confirm the reasons underlying the dosing modifications observed with eculizumab, this study may still serve as a benchmark for future studies aimed at clarifying the reasons for treatment modifications observed. In clinical practice, patients typically receive higher than label-recommended dosing in response to episodes of BTH, ongoing blood transfusions, or disease progression.13 Evidence from clinical trials and real-world studies suggests that the proportion of patients treated with eculizumab who experience BTH ranges from 5% to 37%.11,13,15,24,25 Future research should examine the range of clinical contributors beyond BTH and blood transfusion requirements in real-world settings to explain deviations from the standard dose schedule of eculizumab.
The patient characteristics described in this study are generally consistent with evidence from previous real-world studies, including the International PNH Registry (NCT01374360), a large, global, prospective, non-interventional, observational study of patients with PNH. Similar to the results reported here, the proportion of patients with a history of aplastic anemia enrolled in the registry was high (53%).26 Additionally, anticoagulant use, which may be used as supportive care in response to disease activity, was consistent among patients in the escalation analysis cohort and in the registry (22% vs 20%, respectively).26 Fewer patients in the escalation analysis cohort received blood transfusions during baseline than in the registry (42% vs 61%, respectively).26 However, this may be due to differences in study design (eg, the baseline period is 6 months for the registry, but 3 months here) and data collection (eg, patients and physicians report information in the registry, while this study relied on administrative claims data).26 Evidence from a retrospective analysis of the MarketScan insurance claims database and the present study also suggests that a substantial portion of patients with PNH receiving eculizumab may discontinue treatment. In the previous real-world study, ~33% of the patients receiving eculizumab discontinued within the first year of treatment, and in the present study, ~75% of the patients discontinued, with a median time to discontinuation of 6 months.2 The reasons for this discrepancy in the proportion of patients who discontinued therapy in the present study relative to previously published literature remains unclear. However, it is possible that many of the patients in the present study switched to a different therapeutic regimen, particularly if encouraged to enroll in a clinical trial. Further, switching to ravulizumab in routine clinical practice may have been more common due to the relatively recent study period, which included dosing patterns following the FDA approval of ravulizumab (ie, from December 2018 onward).
As seen in this study, the probability of dose escalation was approximately 50% by the end of 12 months of treatment. Given that treatment with eculizumab is lifelong, it is clear that additional drug costs may be realized quickly following initiation of eculizumab, and incurred indefinitely, especially among patients with incomplete control of PNH. In order to comprehensively assess the financial costs associated with eculizumab treatment in real-world settings, future analyses should take into consideration substantial, ongoing deviations from the label-recommended dosing regimen. Such an analysis would be particularly relevant given that eculizumab is among the most expensive drugs in the world, and treatment costs approximately US$500,000 per patient per year based on the label recommended dose.27 Based on the wholesale acquisition cost of $6523 per vial, the higher than label-recommended average dose received during the maintenance phase (>1000 mg per infusion) observed in this study translates to approximately $60,000 per patient per year in additional drug costs for payers. Further evidence regarding the HRU (eg, hospitalizations, outpatient visits) and direct medical costs among eculizumab-treated PNH patients is also warranted.28 In particular, there is a need for comparative assessments of the economic and clinical outcomes among eculizumab-treated patients who received a regularly scheduled dose relative to those with deviations from label-recommended dosing, including those who required dose escalation.
While eculizumab, as a first-to-market therapy for PNH, has been used to treat patients with PNH, the observed dose escalations and discontinuation in this study and elsewhere2 suggest that for a subset of patients there is unmet clinical need. The expansion of the PNH treatment landscape to include the 2018 FDA approval of the C5 inhibitor, ravulizumab, has provided options to address this need.29 Research has indicated that ravulizumab is associated with an immediate and sustained therapeutic response when administered according to the recommended 8-week dosing schedule.30,31 In the clinical trial setting, fewer complement-naïve patients treated with ravulizumab experienced BTH relative to eculizumab (4.0% vs 10.7%), and similar results were observed among patients that were stabilized on eculizumab during the baseline period of the trial (0% vs 5.1%).30 Ravulizumab has also been linked to substantial cost reductions relative to eculizumab (-$1,673,465, based on a 2020 cost utility analysis) in the US. In 2021, the treatment landscape for patients with PNH that may not experience symptom resolution with C5 inhibitors further expanded with approval by the FDA of the C3 inhibitor, pegcetacoplan.32 The availability of multiple therapies indicated for PNH is expected to assist healthcare stakeholders with treatment optimization.
The results of this study are subject to certain limitations. While this study examined administrative claims with some electronic health records data, the Symphony Health IDV database lacked important clinical and behavioral predictors of continued use, dose escalations, or reason for discontinuations, all of which are critical to stratify patients and perform inferential analyses. Specifically, the data used in this study did not include potentially relevant clinical measures (eg, PNH clone size, clone changes over time, incidence of BTH, serum measurements of eculizumab) and data on the signs and symptoms that may prompt modifications of eculizumab therapy. We further note that the reasons for deviations from label-recommended dosing (ie, higher or lower than FDA-approved doses), dose escalation, and treatment discontinuation are not available in administrative claims data. The ICD-9/10-CM diagnosis codes are not limited to PNH diagnosis and may not be applied systematically in clinical practice. Thus, to minimize imprecision in patient selection using these codes, the study cohort was selected using an “inclusion-by-exclusion” principle where patients were excluded if they had ≥1 diagnosis of another indication for eculizumab (ie, atypical hemolytic uremic syndrome, generalized myasthenia gravis, and neuromyelitis optica spectrum disorder). As a result, the number of patients with PNH may be underestimated as patients with concomitant diagnoses for any of these three conditions and PNH were excluded. Similar to all analyses that examine administrative claims data, potential misspecification of diagnosis, procedure, or drug codes may have resulted in the underestimation or overestimation of dosing patterns. Because Symphony Health IDV does not include eligibility files, quarterly claims activity was used as a proxy for health plan enrollment. The limitation of this method is that patients or events may have been missed if there was a change in the patient’s point of care. Similarly, because Symphony Health IDV is a provider-based database, as opposed to an insurance-based database, patients may be counted as multiple patients if they were treated by different doctors or at different offices. However, Symphony Health IDV minimizes this discrepancy with a linking algorithm. Finally, while it was not possible to analyze the dosing patterns of ravulizumab in this study, similar trends would be expected given both drugs share the same mechanism of action.
Conclusion
PNH is a rare, acquired hematological disease characterized by complement-mediated hemolysis. Numerous clinical trials and related extension studies have examined the therapeutic management of PNH with the C5 complement inhibitor eculizumab. However, there are limited published data describing treatment and dosing strategies in real-world settings. The results of this study address this gap and suggest that patients commonly receive higher than label-recommended doses of eculizumab. Patients examined in this study exhibit a high level of morbidity and it is possible that a significant portion of patients with PNH have unmet clinical needs while receiving the standard eculizumab dose. Future studies assessing the budget impact of eculizumab treatment should account for the real-world dosing patterns reported here.
Acknowledgments
Apellis Pharmaceuticals, Inc. and Swedish Orphan Biovitrum AB reviewed and provided feedback on the manuscript. Medical writing assistance was provided by Gloria DeWalt, an employee of Analysis Group, Inc., and funded by Apellis Pharmaceuticals, Inc. An abstract of this paper was presented at the 62nd Annual American Society of Hematology Meeting and Exposition as a poster presentation and conference talk with interim findings. The poster’s abstract was published in Blood: https://doi.org/10.1182/blood-2020-141636.
Disclosure
Sujata P Sarda, Nikita Mody-Patel, and Sangeeta Krishnan are employees of Apellis Pharmaceuticals, Inc. and own stock/stock options. Wendy Y Cheng, Mihran Yenikomshian, Jensen Duy Vu, and Mei Sheng Duh are employees of Analysis Group, Inc., which has received research funding from Apellis Pharmaceuticals, Inc. to conduct the current study. Colin Kunzweiler and Hoi Ching Cheung were employees of Analysis Group, Inc. during the conduct of this study. The authors report no other conflicts of interest in this work.
References
1. Brodsky RA. Paroxysmal nocturnal hemoglobinuria. Blood. 2014;124(18):2804–2811. doi:10.1182/blood-2014-02-522128
2. Jalbert JJ, Chaudhari U, Zhang H, Weyne J, Shammo JM. Epidemiology of PNH and real-world treatment patterns following an incident PNH diagnosis in the US. Blood. 2019;134(Supplement_1):3407. doi:10.1182/blood-2019-125867
3. Canadian Association of PNH Patients. The guide to living well with PNH. 2018. Available from: https://pnhca.org/the-guide-to-living-well-with-pnh. Accessed October 26, 2020.
4. Hill A, DeZern AE, Kinoshita T, Brodsky RA. Paroxysmal nocturnal haemoglobinuria. Nat Rev Dis Primers. 2017;3:17028. doi:10.1038/nrdp.2017.28
5. U.S. Food and Drug Administration. Highlights of prescribing information: SOLIRIS® (eculizumab); 2019:1–9. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/125166s172lbl.pdf.
6. European Medicines Agency. Soliris - summary of product characteristics. 2009. Available from: https://www.ema.europa.eu/en/documents/product-information/soliris-epar-product-information_en.pdf. Accessed October 26, 2020.
7. Brodsky RA, Young NS, Antonioli E, et al. Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood. 2008;111(4):1840–1847. doi:10.1182/blood-2007-06-094136
8. Hill A, Hillmen P, Richards SJ, et al. Sustained response and long-term safety of eculizumab in paroxysmal nocturnal hemoglobinuria. Blood. 2005;106(7):2559–2565. doi:10.1182/blood-2005-02-0564
9. Hillmen P, Elebute M, Kelly R, et al. Long-term effect of the complement inhibitor eculizumab on kidney function in patients with paroxysmal nocturnal hemoglobinuria. Am J Hematol. 2010;85(8):553–559. doi:10.1002/ajh.21757
10. Hillmen P, Muus P, Duhrsen U, et al. Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria. Blood. 2007;110(12):4123–4128. doi:10.1182/blood-2007-06-095646
11. Hillmen P, Muus P, Röth A, et al. Long-term safety and efficacy of sustained eculizumab treatment in patients with paroxysmal nocturnal haemoglobinuria. Br J Haematol. 2013;162(1):62–73. doi:10.1111/bjh.12347
12. Hillmen P, Young NS, Schubert J, et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2006;355(12):1233–1243. doi:10.1056/NEJMoa061648
13. DeZern AE, Dorr D, Brodsky RA. Predictors of hemoglobin response to eculizumab therapy in paroxysmal nocturnal hemoglobinuria. Eur J Haematol. 2013;90(1):16–24. doi:10.1111/ejh.12021
14. Kelly R, Arnold L, Richards S, et al. Modification of the eculizumab dose to successfully manage intravascular breakthrough hemolysis in patients with paroxysmal nocturnal hemoglobinuria. Blood. 2008;112(11):3441. doi:10.1182/blood.V112.11.3441.3441
15. Kulasekararaj AG, Hill A, Rottinghaus ST, et al. Ravulizumab (ALXN1210) vs eculizumab in C5-inhibitor-experienced adult patients with PNH: the 302 study. Blood. 2019;133(6):540–549. doi:10.1182/blood-2018-09-876805
16. Röth A, Dührsen U. Treatment of paroxysmal nocturnal hemoglobinuria in the era of eculizumab. Eur J Haematol. 2011;87(6):473–479. doi:10.1111/j.1600-0609.2011.01701.x
17. Röth A, Rottinghaus ST, Hill A, et al. Ravulizumab (ALXN1210) in patients with paroxysmal nocturnal hemoglobinuria: results of 2 phase 1b/2 studies. Blood Adv. 2018;2(17):2176–2185. doi:10.1182/bloodadvances.2018020644
18. Füreder W, Valent P. Switching from high-dose eculizumab to ravulizumab in paroxysmal nocturnal hemoglobinuria: a case report. HemaSphere. 2020;4(4):e455. doi:10.1097/HS9.0000000000000455
19. Risitano AM, Marotta S, Ricci P, et al. Anti-complement treatment for paroxysmal nocturnal hemoglobinuria: time for proximal complement inhibition? A position paper from the SAAWP of the EBMT. Front Immunol. 2019;10:1157. doi:10.3389/fimmu.2019.01157
20. Al-Ani F, Chin-Yee I, Lazo-Langner A. Eculizumab in the management of paroxysmal nocturnal hemoglobinuria: patient selection and special considerations. Ther Clin Risk Manag. 2016;12:1161–1170. doi:10.2147/TCRM.S96720
21. Wijnsma KL, Ter Heine R, Moes D, et al. Pharmacology, pharmacokinetics and pharmacodynamics of eculizumab, and possibilities for an individualized approach to eculizumab. Clin Pharmacokinet. 2019;58(7):859–874. doi:10.1007/s40262-019-00742-8
22. Griffin M, Munir T. Management of thrombosis in paroxysmal nocturnal hemoglobinuria: a clinician’s guide. Ther Adv Hematol. 2017;8(3):119–126. doi:10.1177/2040620716681748
23. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
24. Lee JW, Sicre de Fontbrune F, Wong Lee Lee L. Sicre de Fontbrune F, Wong Lee Lee Let al. Ravulizumab (ALXN1210) vs eculizumab in adult patients with PNH naive to complement inhibitors: the 301 study. Blood. 2019;133(6):530–539. doi:10.1182/blood-2018-09-876136
25. Nakayama H, Usuki K, Echizen H, Ogawa R, Orii T. Eculizumab dosing intervals longer than 17 days may be associated with greater risk of breakthrough hemolysis in patients with paroxysmal nocturnal hemoglobinuria. Biol Pharm Bull. 2016;39(2):285–288. doi:10.1248/bpb.b15-00703
26. Schrezenmeier H, Röth A, Araten DJ, et al. Baseline clinical characteristics and disease burden in patients with paroxysmal nocturnal hemoglobinuria (PNH): updated analysis from the international PNH registry. Ann Hematol. 2020;99(7):1505–1514. doi:10.1007/s00277-020-04052-z
27. Ricklin D, Mastellos DC, Reis ES, Lambris JD. The renaissance of complement therapeutics. Nat Rev Nephrol. 2018;14(1):26–47. doi:10.1038/nrneph.2017.156
28. Cheng WY, Sarda SP, Mody-Patel N, et al. Real-World Healthcare Resource Utilization (HRU) and costs of patients with Paroxysmal Nocturnal Hemoglobinuria (PNH) receiving eculizumab in a US population. Adv Ther. 2021;38(8):4461–4479. doi:10.1007/s12325-021-01825-4
29. U.S. Food and Drug Administration. Highlights of prescribing information: ULTOMIRIS ™ (ravulizumab-cwvz); 2018. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761108s000lbl.pdf.
30. Brodsky RA, Peffault de Latour R, Rottinghaus ST, et al. Characterization of breakthrough hemolysis events observed in the phase 3 randomized studies of ravulizumab versus eculizumab in adults with paroxysmal nocturnal hemoglobinuria. Haematologica. 2021;106(1):230–237. doi:10.3324/haematol.2019.236877
31. Schrezenmeier H, Kulasekararaj A, Mitchell L, et al. One-year efficacy and safety of ravulizumab in adults with paroxysmal nocturnal hemoglobinuria naive to complement inhibitor therapy: open-label extension of a randomized study. Ther Adv Hematol. 2020;11:2040620720966137. doi:10.1177/2040620720966137
32. US Food and Drug Administration. Highlights of prescribing information: EMPAVELI™ (pegcetacoplan). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/215014s000lbl.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.