Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Real-World Clinical and Economic Outcomes Associated with Surgiflo® vs Floseal in Cardiovascular Surgeries in the US
Authors Danker III W ![]() , Aggarwal J
, Aggarwal J ![]() , Kelkar SS
, Kelkar SS ![]() , Marston XL, Gao X, Johnston SS
, Marston XL, Gao X, Johnston SS
Received 14 October 2021
Accepted for publication 27 January 2022
Published 10 March 2022 Volume 2022:14 Pages 129—138
DOI https://doi.org/10.2147/CEOR.S338672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Walter Danker III,1 Jyoti Aggarwal,2 Sneha S Kelkar,2 Xiaocong L Marston,2 Xin Gao,2 Stephen S Johnston3
1Ethicon Inc., Somerville, NJ, USA; 2OPEN Health, Bethesda, MD, USA; 3Johnson & Johnson Co., New Brunswick, NJ, USA
Correspondence: Jyoti Aggarwal, OPEN Health, 4350 East West Hwy #1100, Bethesda, MD, 20814, USA, Tel +1-240-821-1265, Email [email protected]
Background: Topical hemostatic agents are an option for controlling bleeding during cardiovascular surgery. Previous studies comparing topical hemostatic agents in cardiovascular surgery predate the 2012 reformulation of Surgiflo®, which had been re-engineered to increase paste viscosity and thus be more adherent to the bleeding surface.
Objective: To compare clinical and economic outcomes in patients receiving the current formulation of Surgiflo vs Floseal during cardiovascular surgeries.
Methodology: A retrospective analysis was conducted using the Premier Healthcare Database. Eligible patients had an inpatient cardiovascular surgery between 1/1/2013 and 6/1/2018, were ≥ 18 years old and received the current formulation of Surgiflo or Floseal during surgery. Propensity score matching was performed, with exact matching on the surgery year and surgery type (aortic, coronary artery bypass grafting, valve, or other). Descriptive analysis and generalized estimating equations models compared outcomes between the Surgiflo and Floseal groups.
Results: The matched sample included 5768 patients in each group (mean age: 66.5 years; 66.3% male). In the matched sample, rates of any documented bleeding event were similar in Surgiflo and Floseal groups (6.9% vs 7.2%; P = 0.576). Differences in transfusion rates between patients receiving Surgiflo vs Floseal varied by operational definition and timing of measurement but did not differ by > 2 percentage points. Compared to Floseal, patients who received Surgiflo experienced longer surgery duration (306.0 vs 299.4 minutes), lower hospitalization cost ($44,146 vs $46,812), and lower odds of readmission at 30, 60, and 90 days post-discharge (all P < 0.05). Inpatient mortality and LOS were comparable between Surgiflo and Floseal (all P > 0.05).
Conclusion: In this large study of real-world clinical and economic outcomes after cardiovascular surgery involving the current formulation of Surgiflo vs Floseal, Surgiflo was associated with mostly similar clinical outcomes as compared with Floseal. Differences in selected economic/resource use outcomes were also observed, for which root-cause analysis in future research would be informative.
Keywords: Surgiflo®, Floseal, cardiovascular surgery, economic outcomes, bleeding, transfusion
Introduction
Cardiovascular (CV) disease is highly prevalent and responsible for approximately one-third of mortality in people over the age of 35 years.1,2 Depending on the severity and anatomy of CV disease, it may be treated by surgical intervention such as coronary artery bypass grafting (CABG), aortic procedures, or valvular procedures.3,4 Intra‐ or postoperative bleeding is a recognized complication of cardiac surgery, particularly among patients undergoing complex procedures that require long operating times and in patients receiving anticoagulant therapies preoperatively and intraoperatively.5–9 Severe bleeding occurs in approximately 3.4% of the people undergoing CABG, 23% of the people undergoing aortic valve replacement, and over 30% of the people undergoing aortic root replacement.10–13 Bleeding and reoperation for bleeding are associated with increased mortality, risk of complications, and risk of transfusions.12 Bleeding complications also substantially increase healthcare resource utilization; increasing hospital length of stay and time spent in critical care units.14 Effective approaches to maintain hemostasis and avoid complications associated with significant blood loss during CV surgery are essential to providing successful care to patients.
Topical hemostats are an option to control bleeding during surgery when conventional methods (such as suturing, cautery, or manual compression) are inadequate or impractical.15 Two commonly used gelatin-thrombin-based flowable topical hemostats are Floseal Hemostatic Matrix (Baxter Healthcare Corporation, Deerfield, IL) and Surgiflo® Hemostatic Matrix (Ethicon Incorporated, Somerville, NJ).16 Surgiflo and Floseal have dual blood clotting mechanisms: 1) contact activation and 2) biologic agents (thrombin). Both products’ ability to conform to tissue to fill deep lesions are advantageous in CV surgery.17,18 Surgiflo and Floseal have been shown to reduce surgery duration, reduce transfusion need, better manage an anticoagulated patient, improve recovery time, and reduced wound exposure.19
Few studies have performed head-to-head comparison between Surgiflo and Floseal in the context of CV surgery. A retrospective claims database analysis by Tackett et al of cardiac surgical cases from 2006 to 2012 concluded that Floseal was associated with fewer negative clinical consequences than Surgiflo.16 Building on that research, Makhija et al used the clinical outcomes from Tackett et al to construct a cost-consequence model to evaluate the economic impact Surgiflo vs Floseal.20 However, a newer formulation of Surgiflo has been available since 2012. This newer formulation of Surgiflo possesses a re-engineered gelatin matrix that increases the degree of cross-linking of gelatin particles and increases solid content in the gelatin matrix, which leads to increased paste viscosity, less runniness, and better adherence to the bleeding surface relative to the prior formulation. This limits the present-day applicability of both Tackett et al and Makhija et al’s findings, as both papers used data on Surgiflo’s previous formulation. Thus, the objective of this study was to compare clinical and economic outcomes in patients treated with the current formulation of Surgiflo vs Floseal during CV surgeries.
Materials and Methods
Data Source
The data for this retrospective study was obtained from the Premier Healthcare Database (PHD) for years 2013–2018. PHD is a large US-hospital-based all-payer database which covers over 700 hospitals representing over 8 million inpatient encounters per year. The PHD is geographically diverse and captures 20% of inpatient hospital discharges in the US.21 PHD data were deidentified in compliance with the US Health Insurance Portability and Accountability Act (HIPAA). As such, there was no requirement for institutional review board approval.
Cohort Selection
Patients included in this study underwent an inpatient CV surgery (index surgery and admission) between January 1, 2013, and June 1, 2018. CV surgeries were defined as CABG, aortic procedures, or valvular procedures classified by primary International Classification of Diseases, 9th and 10th Revision (ICD-9-CM/ICD-10-PCS) procedure codes. Details on each code used to identify surgery clinical features are available in Appendix A. Patients were at least 18 years of age at the admission date of the surgery-related hospitalization and received the current formulation of hemostatic agent Surgiflo or Floseal during the surgery. For patients having multiple eligible CV surgeries on record, only the first hospitalization was used for the study.
Exclusion criteria included the following: both Surgiflo and Floseal were administered during the index surgery, surgery duration was missing, duration of surgery was less than 1 hour or more than 12 hours, admission or discharge date was missing, patient had secondary procedure codes for other surgeries such as spine surgery during the same hospitalization, and surgeries using Surgiflo and Floseal with unclear product description (eg, no description of formulation or dosage). Clinical information such as diagnoses, procedures, hemostatic matrix use and formulation, and comorbidity information were defined using a combination of ICD-9-CM codes, ICD-10-CM codes, procedure codes, and text searches in hospital chargemaster data as applicable. Use of Surgiflo and Floseal product and units of product used were verified using product description and quantity of the product reported (Surgiflo 8mL and Floseal 5mL or 10 mL). More information on variable definitions including the ICD-9-CM/ICD-10-CM coding schema is available in Appendices B and C.
Patient and Hospital Characteristics
The following patient and hospital characteristics were assessed: patient demographics (age, sex, race, and payor), clinical characteristics (admission type, Charlson Comorbidity Index score, and surgical details), and hospital characteristics (hospital region, location, teaching-status, and bed size).
Outcomes
Clinical outcomes included bleeding diagnoses and transfusions recorded during the index admission. Bleeding diagnoses were documented by ICD-9-CM/ICD-10-CM diagnosis codes designated as not present on admission or any ICD-9-CM/ICD-10-PCS bleeding event procedure codes during the hospitalization (Appendix B). Transfusions were documented by ICD-9-CM/ICD-10-PCS codes and hospital charge master records (Appendix C). Blood transfusion and packed red blood cell (PRBC) transfusion during the hospitalization were defined as: “Any transfusion,” which indicated any transfusion event recorded during the hospital stay, or “Any transfusion from day of surgery through day 4,” which indicated any transfusion event on the day of surgery or within 4 days post-surgery. As topical hemostats are used to control bleeding, the documentation of a bleeding diagnoses despite topical hemostat use was presumed to be a marker of bleeding severity. Inpatient mortality was assessed using hospital discharge status.
Healthcare resource utilization outcomes included the following: length of stay (LOS) measured in days; intensive care unit (ICU) admission; duration of surgery in hours; and 30-, 60-, and 90-day readmission to the same hospital in which the index CV surgery was performed. Hospital costs, which were contributed to the PHD directly from hospitals based on their internal cost accounting systems, were adjusted to 2018 US dollars using the Medical Care component of the US Bureau of Labor Statistics Consumer Price Index.
Statistical Analysis
A descriptive analysis was conducted to understand the differences between Surgiflo and Floseal groups. For continuous variables, means, standard deviation, and ranges were calculated. Student’s t-tests were conducted with a normal distribution and Wilcoxon rank sum tests for variables with skewed distribution, such as costs. For categorical variables, frequencies, proportions, and Pearson chi-square tests were conducted.
Patients in the Surgiflo group were propensity score matched (PSM) to those in the Floseal group using 1:3 variable-ratio matching without replacement. The propensity score was derived from a multivariable logistic regression in which the dependent variable was membership in the Surgiflo vs Floseal group and the independent variables were all patient demographics, patient and surgery clinical characteristics, and hospital characteristics described above. In addition, patients were exactly matched on index year and type of CV procedure (CABG, aortic, valvular, or other). After PSM, a sampling weight (probability weight for Floseal patients that was inversely proportional to the total number of Floseal patients that were matched to the same Surgiflo patient) was applied to account for the variable-ratio nature of the match, effectively rendering the weighted post-matching sample to be 1:1. The standardized differences of the matching covariates were calculated to verify appropriate balance, indicated by an absolute value of 10%.
Outcomes were compared between the matched Surgiflo and Floseal groups using Generalized Estimating Equations (GEE) with an exchangeable working correlation structure.22 For binary outcomes (eg, inpatient mortality), a binomial distribution and logit link was used; for LOS and number of ICU days, a negative binomial distribution and log link was used; for costs, a gamma distribution and log link was used.23 All post-matching multivariable regression models were adjusted for unbalanced characteristics after PSM.
As prolonged surgery time can be reflective of either an outcome of topical hemostat use or instead a potential proxy measure of the inherent complexity of a surgical case, a sensitivity analysis was performed to evaluate outcomes when adjusting for surgery time.
All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC), and a two-sided p-value of <0.05 was considered statistically significant.
Results
Study Sample
Prior to matching, 5768 patients who received Surgiflo and 24,420 patients who received Floseal met the patient selection criteria. After PSM and reweighting, 5768 patients who received Surgiflo were matched to 5768 patients who received Floseal. Figure 1 illustrates the cohort selection process. Please refer to Appendix D for PSM results.
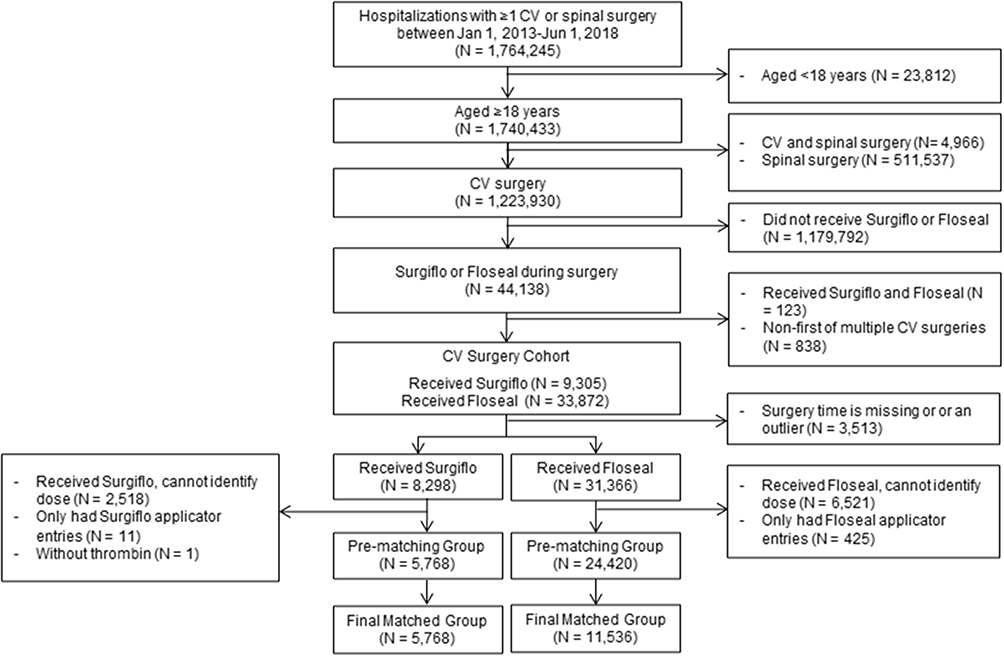 |
Figure 1 Cohort selection flowchart. Abbreviation: CV, cardiovascular. |
Patient and Hospital Characteristics
Table 1 provides descriptive statistics of patient and hospital characteristics before and after PSM. Prior to matching, average patient age was approximately 67 years and approximately two-thirds of the sample was male. Prior to matching, patients who received Surgiflo® and patients who received Floseal differed in race, admission type (greater frequency of emergent admission in the Surgiflo® group), surgery type (greater proportion of valvular procedures in the Floseal group), and hospital characteristics. After PSM, the patients who received Surgiflo and patients who received Floseal groups were similar on matching variables except for urban vs rural hospital type (SMD >10%). Therefore, urban vs rural hospital type was adjusted for in the post-matching multivariable GEE models.
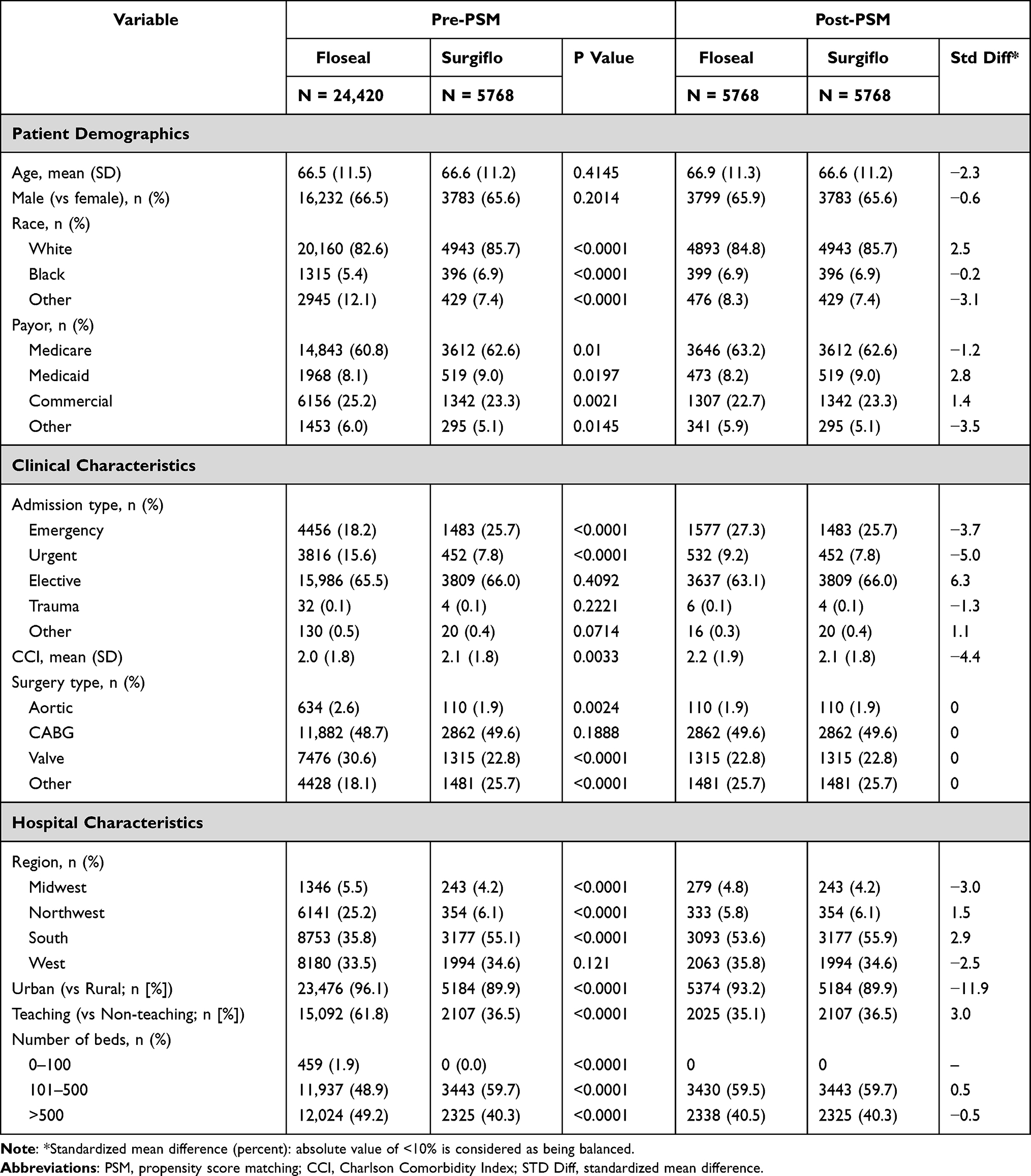 |
Table 1 Comparison of Patient Demographics, Clinical Characteristics, and Hospital/Provider Characteristics Between Surgiflo and Floseal Groups, Before and After PSM |
In the post-matching sample, CABG procedures accounted for 49.6% of index surgeries followed by 22.8% for valvular procedures, 1.9% for aortic surgeries, and 25.7% for other types of CV surgeries. The majority of surgeries in both groups were elective (Surgiflo®: 65.5%; Floseal: 64.0%). The majority of surgeries occurred in urban hospitals (Surgiflo®: 89.9%; Floseal: 93.2%).
Comparative Outcomes
Table 2 shows the results of the post-matching multivariable analysis. The incidence of any documented bleeding event was similar between the Surgiflo and Floseal groups (6.9% vs 7.2%; odds ratio (OR): 0.96; 95% CI: 0.84–1.10; P=0.576) and the incidence of any postoperative bleeding event was lower in the Surgiflo vs Floseal group (0.8% vs 1.2%; OR: 0 68; 95% CI: 0.48–0.97; P=0.032). The incidence of any transfusion was greater in the Surgiflo vs Floseal group (42.1% vs 40.8%; OR: 1.08; 95% CI: 1.01–1.15; P=0.018). However, the incidence of any transfusion on or within 4 days of surgery were comparable between the groups (38.6% vs 37.7%; OR: 1.07; 95% CI: 1.00–1.14; P=0.057), while the incidence of any PRBC transfusion on or within 4 days of surgery was lower in the Surgiflo vs Floseal group (17.1% vs 19.1%; OR: 0.88; 95% CI: 0.81–0.96; P=0.005). Inpatient mortality was similar between the Surgiflo and Floseal groups (3.0% vs 3.1%; OR: 0.98; 95% CI: 0.81–1.19; P=0.8716).
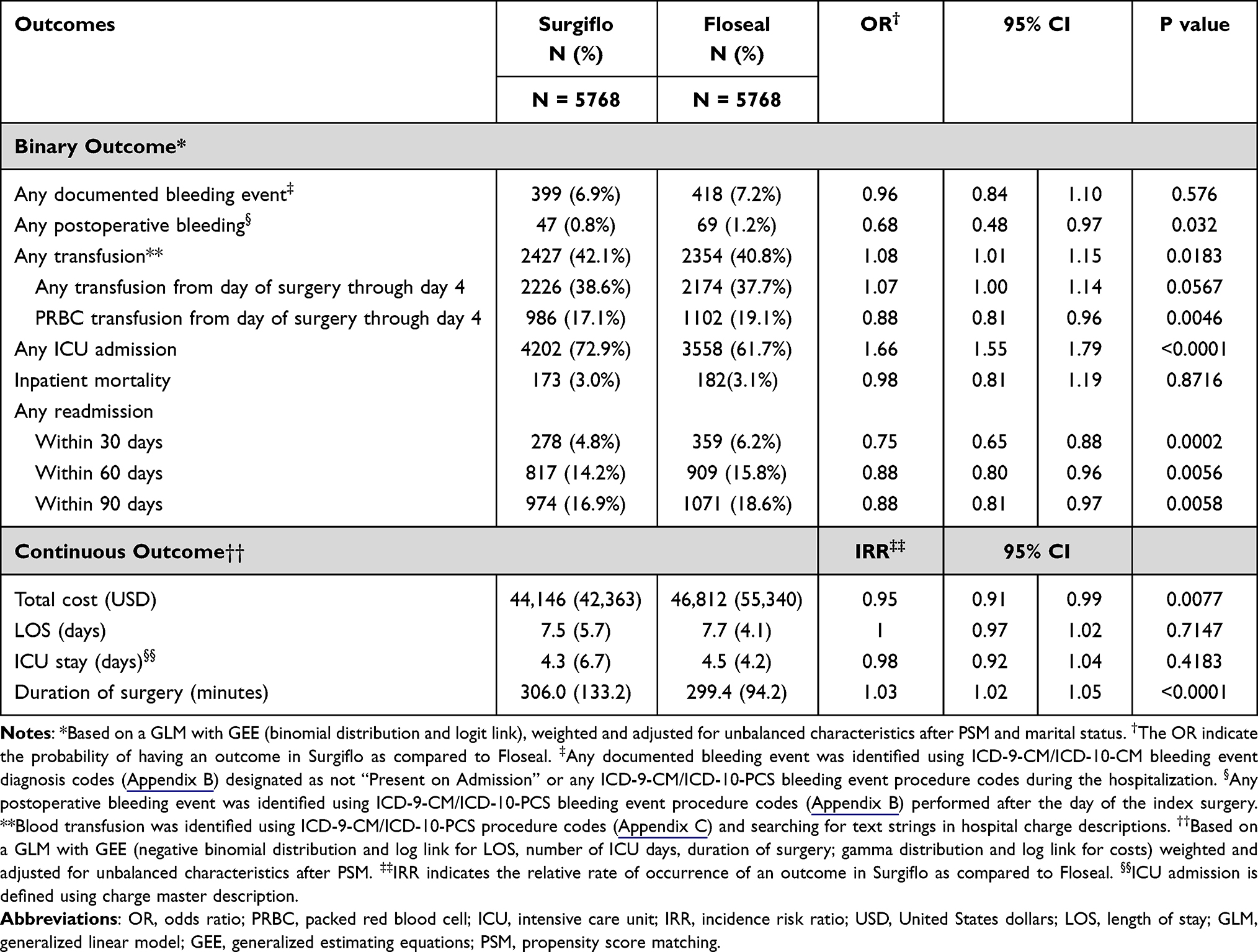 |
Table 2 Post-Matching Multivariable Analysis |
The rate of ICU admission was higher in the Surgiflo vs Floseal group (72.9% vs 61.7%; OR: 1.66; 95% CI: 1.55–1.79; P<0.0001). Despite the difference in ICU admission, mean total length of stay was similar between the Surgiflo and Floseal group (7.5 days vs 7.7 days; incidence risk ratio (IRR): 1.00; 95% CI: 0.97–1.02; P=0.7147) and duration of ICU stay was similar between the Surgiflo and Floseal group (4.3 days vs 4.5 days; IRR: 0.98; 95% CI: 0.92–1.04; P=0.4183). The mean duration of surgery was longer in the Surgiflo vs Floseal group (306.0 minutes vs 299.4 minutes; IRR: 1.03; 95% CI: 1.02–1.05; P<0.0001). Patients receiving Surgiflo were 25% less likely to be readmitted at 30 days (4.8% vs 6.2%; OR: 0.75; 95% CI: 0.65–0.88; P=0.0002) compared to patients that received Floseal. This difference was consistent at 60- and 90-day time points. Patients receiving Surgiflo were 12% less likely to be readmitted at 60-days (14.2% vs 15.8%; OR: 0.88; 95% CI: 0.80–0.96; P=00.56) and 12% at 90-days (16.9% vs 18.6%; OR: 0.88; 95% CI: 0.81–0.97; P=0.0058) compared to patients who received Floseal.
The mean total cost of the index admission was lower in the Surgiflo vs Floseal group ($44,146 vs $46,812; IRR: 0.95; 95% CI: 0.91–0.99; P=0.0077).
Sensitivity and Exploratory Analyses
A sensitivity analysis was conducted to assess the consistency of study findings when examining the two most common cardiovascular surgery types, namely CABG (N=2862 matched patients) and valve surgeries (N=1315 matched patients). The results for both these types of surgeries were consistent with the overall population (Appendix E). The odds of any transfusion was insignificantly higher in the Surgiflo vs Floseal group undergoing CABG surgeries (OR: 1.07; 95% CI: 0.96–1.19; P=0.231), and insignificantly lower in the Surgiflo vs Floseal group undergoing valve surgeries (OR: 0.93; 95% CI: 0.78–1.10; P=0.395). Incidence of bleeding, readmission, and inpatient mortality was insignificantly lower in the Surgiflo vs Floseal group undergoing CABG surgeries. Length of stay was insignificantly lower in the Surgiflo vs Floseal group undergoing CABG (IRR: 0.98; 95% CI: 0.96–1.01; P=0.150) and insignificantly higher in the Surgiflo vs Floseal group undergoing valve surgery (IRR: 1.02; 95% CI: 0.98–1.06; P<0.340). Length of ICU stay was significantly lower in the Surgiflo vs Floseal group undergoing CABG (IRR: 0.95; 95% CI: 0.91–1.00; P=0.0424) and in the Surgiflo vs Floseal group undergoing valve surgery (IRR: 0.88; 95% CI: 0.94–0.92; P=0.0002). Duration of surgery was significantly longer in the Surgiflo vs Floseal group undergoing CABG (IRR: 1.05; 95% CI: 1.04–1.07; P<0.0001) and there was no significant difference in duration of surgery in Surgiflo vs Floseal group undergoing valve surgeries. Cost was lower in the Surgiflo vs Floseal group in both CABG and valve surgeries (cost difference of $2604 for CABG, P<0.001, and $4570 for valve surgery, P=0.121).
As prolonged surgery time can be reflective of either an outcome of topical hemostat use or the inherent complexity of a surgical case, a sensitivity analysis was performed to evaluate outcomes when adjusting for surgery duration. After adjusting for surgery duration, risk of any transfusion was no longer significantly different between Surgiflo and Floseal groups (OR: 1.01; 95% CI: 0.94–1.09; P=0.779; results not presented), and the Surgiflo group had significantly lower length of stay (IRR: 0.95; 95% CI: 0.93–0.98; P<0.001) and significantly reduced number of days in ICU (IRR: 0.94; 95% CI: 0.89–1.00; P=0.013) vs Floseal group.
Discussion
To our knowledge, this study represents the largest comparative retrospective analysis to compare real-world outcomes of the latest formulation of Surgiflo vs Floseal in cardiovascular surgery.
The current study updates previous findings from Tackett et al, which examined a previous formulation of Surgiflo and reported that Floseal was associated with lower risks of negative outcomes after cardiovascular surgery than Surgiflo.16 Strikingly, they reported that the odds of any blood product transfusion were nearly 5 times higher in the Surgiflo group as compared with the Floseal group (OR = 4.90, p < 0.001); however, this difference was unexplained and the authors acknowledged that inter-hospital variation in transfusion practice patterns may have contributed to that finding. The same is the case in the present study, wherein absolute and between-group differences in transfusion rates varied by operational definition, timing of measurement, and whether or not surgery duration was adjusted for, but did not differ by more than 2 percentage points between the comparison groups, in contrast with the previous study. There are several potential reasons for the between-study differences in findings. First, the former study was based upon an older formulation of Surgiflo, though such large variations in transfusion risk are unlikely to be explained by formulation differences alone. Second, the study by Tackett et al included only 324 cardiovascular surgeries which utilized Surgiflo during 2006–2012 making the (relatively small) Surgiflo group particularly susceptible to the influence of inter-hospital variation in transfusion-related practice patterns. Third, the way in which transfusions are recorded in the PHD is not standard. Indeed, among 261 hospitals included in the present study, 43 had no records of transfusion. Among those that did have records of transfusion, 32.2% were documented only in the charge master records. For these reasons, results related to transfusion must be interpreted considering these limitations. Given that the present analysis is based on a far greater sample size (5768 vs 324), is based on the most current formulation of Surgiflo, and yielded results with more plausible clinical face validity, the previous findings by Tackett et al should be considered inapplicable to present day clinical practice.
Furthermore, rates of documented bleeding diagnoses, a presumed marker of bleeding severity, were similar between the two groups. We are unaware of studies examining whether variation in diagnosis coding practices would result in less measurement error than variation in charge master documentation; however, it is well known that charge master data are more suitable for active comparisons of positively identified product use than for the definition of endpoints.
Aside from the bleeding and transfusion outcomes, the present study found that Surgiflo was associated $2666 lower average total hospitalization cost and somewhat lower risks of 30, 60, and 90-day readmission as compared with Floseal. Although Surgiflo was associated with higher risk of ICU admission, it was nevertheless associated with similar but numerically lower average days spent in the ICU and overall length of stay. Indeed, the finding that not everyone was admitted to the ICU could be suggestive of measurement error in the charge master data given postoperative transfer to the cardiac or surgical ICU is highly routine course of action for patients recovering from cardiac surgery.
As noted above, while surgery time could be influenced by topical hemostat use, it could also be a potential proxy measure of the inherent complexity of a surgical case. In the sensitivity analysis adjusting for surgery time, which was 7 minutes longer on average in the Surgiflo group, Surgiflo was further associated with significantly lower length of stay and duration of ICU stay. Thus, the study findings suggest that, at a minimum, Surgiflo is not associated with unfavorable length of stay and ICU outcomes.
Limitations
The current study has limitations inherent with retrospective database analyses. The study sample was not randomly assigned to either the Surgiflo or Floseal group, introducing potential treatment selection bias. Although PSM was used to balance the two comparison groups and to ensure that the groups were comparable, PSM is only able to balance confounding variables available in the database. Thus, the findings of the current study may still be subject to residual confounding. The study also has limitations inherent in the PHD. The PHD is a hospital-based database that collects data from hospitals across the US. Coding practices and criteria may not be consistent across different hospitals. Additionally, total hospital costs may be driven by several factors beyond those which can be attributed to topical hemostats. A formal cost-effectiveness analysis in which costs that are directly attributable to the supplies, medications, and interventions that can be explained specifically by differences in the clinical efficacy of topical hemostats would provide a clearer picture of the specific drivers of relevant cost differences between products. The PHD does not capture data elements such as longitudinal use of medication or rehospitalizations to hospitals other than the one in which the index surgery was performed, resulting in the potential for suboptimal sensitivity for identification of readmissions. We are also limited in our ability to pinpoint the specific reasons for which significant differences were found between the study groups in the rate of readmission, and therefore this finding warrants further investigation. Therefore, outcomes such as readmission rates in the current study may be underestimated.
Conclusion
Active flowable hemostatic matrices are a useful tool to control intraoperative bleeding during cardiovascular surgery. Active flowable hemostatic matrices are reported to be more effective compared with passive non-flowable hemostatic agents.15,17,25,26 Additionally, compared to other passive topical hemostats, active flowable hemostatic matrices have been associated with lower rates of surgical revisions, blood transfusions, and post-surgical complications and shorter operation times.25,26 The current study represents the largest evaluation of economic and clinical outcomes of the most common active flowable hemostatic matrices and is the only analysis analyzing the latest formulation of Surgiflo. Our findings suggest that Surgiflo is associated with mostly similar clinical outcomes as compared with Floseal. Differences in selected economic/resource use outcomes were also observed, for which root-cause analysis in future research would be informative.
Prior Peer-Reviewed Presentation at a Professional/Scientific Conference
Real-World Economic and Clinical Outcomes Associated with Current Hemostatic Matrix Use in Cardiovascular Surgery. Poster Presentation. Virtual ISPOR 2020 Conference, May 18–20, 2020.
Ethical Disclosure
Data were deidentified in compliance with the US Health Insurance Portability and Accountability Act (HIPAA). As such, there was no requirement for internal institutional review board approval.
Acknowledgments
Medical writing/editorial support was provided by Gregory Poorman, MPH, from OPEN Health, Bethesda, MD, USA.
Funding
Research funding was provided by Ethicon Inc.
Disclosure
WD III is an employee of Ethicon, Inc., the study sponsor. SSJ is an employee of Johnson & Johnson. JA, SSK, XLM and XG are employees of OPEN Health, which received consultancy fees from Ethicon. The authors report no other conflicts of interest in this work.
References
1. Abubakar I, Tilmann T, Banerjee A. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–171.
2. Ali M, Beusenberg M, Bloessner M. World health statistics; 2009. Available from: https://www.who.int/gho/publications/world_health_statistics/EN_WHS09_Full.pdf.
3. Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541–2619. doi:10.1093/eurheartj/ehu278
4. Chang M, Ahn JM, Lee CW, et al. Long-term mortality after coronary revascularization in nondiabetic patients with multivessel disease. J Am Coll Cardiol. 2016;68(1):29–36. doi:10.1016/j.jacc.2016.04.034
5. Verma K, Errico TJ, Vaz KM, Lonner BS. A prospective, randomized, double-blinded single-site control study comparing blood loss prevention of tranexamic acid (TXA) to epsilon aminocaproic acid (EACA) for corrective spinal surgery. BMC Surg. 2010;10:13. doi:10.1186/1471-2482-10-13
6. Hassan N, Halanski M, Wincek J, et al. Blood management in pediatric spinal deformity surgery: review of a 2-year experience. Transfusion. 2011;51(10):2133–2141. doi:10.1111/j.1537-2995.2011.03175.x
7. Neilipovitz DT, Murto K, Hall L, Barrowman NJ, Splinter WM. A randomized trial of tranexamic acid to reduce blood transfusion for scoliosis surgery. Anesth Analg. 2001;93(1):82–87. doi:10.1097/00000539-200107000-00018
8. Boldt J, Schindler E, Osmer CH, Wittstock M, Stertmann WA, Hempelmann G. Influence of different anticoagulation regimens on platelet function during cardiac surgery. Br J Anaesth. 1994;73(5):639–644. doi:10.1093/bja/73.5.639
9. Gravlee GP, Scott Haddon W, Rothberger HK, et al. Heparin dosing and monitoring for cardiopulmonary bypass: a comparison of techniques with measurement of subclinical plasma coagulation. J Thorac Cardiovasc Surg. 1990;99(3):518–527. doi:10.1016/S0022-5223(19)36983-1
10. Williams JB, Phillips-Bute B, Bhattacharya SD, et al. Predictors of massive transfusion with thoracic aortic procedures involving deep hypothermic circulatory arrest. J Thorac Cardiovasc Surg. 2011;141(5):1283–1288. doi:10.1016/j.jtcvs.2010.07.098
11. Kinnunen EM, De Feo M, Reichart D, et al. Incidence and prognostic impact of bleeding and transfusion after coronary surgery in low‐risk patients. Transfusion. 2017;57(1):178–186. doi:10.1111/trf.13885
12. Généreux P, Cohen DJ, Williams MR, et al. Bleeding complications after surgical aortic valve replacement compared with transcatheter aortic valve replacement: insights from the PARTNER I trial (Placement of Aortic Transcatheter Valve). J Am Coll Cardiol. 2014;63(11):1100–1109. doi:10.1016/j.jacc.2013.10.058
13. Beverly A, Ong G, Wilkinson KL, Doree C, Welton NJ, Estcourt LJ. Drugs to reduce bleeding and transfusion in adults undergoing cardiac surgery: a systematic review and network meta‐analysis. Cochrane Database Syst Rev. 2019;2019(9). doi:10.1002/14651858.CD013427
14. Al-Attar N, Johnston S, Jamous N, et al. Impact of bleeding complications on length of stay and critical care utilization in cardiac surgery patients in England. J Cardiothorac Surg. 2019;14(1):64. doi:10.1186/s13019-019-0881-3
15. Nasso G, Piancone F, Bonifazi R, et al. Prospective, randomized clinical trial of the FloSeal matrix sealant in cardiac surgery. Ann Thorac Surg. 2009;88(5):1520–1526. doi:10.1016/j.athoracsur.2009.07.014
16. Tackett SM, Calcaterra D, Magee G, Lattouf OM. Real-world outcomes of hemostatic matrices in cardiac surgery. J Cardiothorac Vasc Anesth. 2014;28(6):1558–1565. doi:10.1053/j.jvca.2014.05.010
17. Oz MC, Cosgrove DM, Badduke BR, et al. Controlled clinical trial of a novel hemostatic agent in cardiac surgery. Ann Thorac Surg. 2000;69(5):1376–1382. doi:10.1016/S0003-4975(00)01194-2
18. Woodworth BA, Chandra RK, LeBenger JD, Ilie B, Schlosser RJ. A gelatin-thrombin matrix for hemostasis after endoscopic sinus surgery. Am J Otolaryngol. 2009;30(1):49–53. doi:10.1016/j.amjoto.2007.11.008
19. Vyas KS, Saha SP. Comparison of hemostatic agents used in vascular surgery. Expert Opin Biol Ther. 2013;13(12):1663–1672. doi:10.1517/14712598.2013.848193
20. Makhija D, Rock M, Ikeme S, et al. Cost-consequence analysis of two different active flowable hemostatic matrices in spine surgery patients. J Med Econ. 2017;20(6):606–613. doi:10.1080/13696998.2017.1292916
21. Premier Applied Sciences® PI. Premier healthcare database white paper: data that informs and perform; 2019. Available from: https://learn.premierinc.com/white-papers/premier-healthcaredatabase-whitepaper.
22. Ballinger GA. Using generalized estimating equations for longitudinal data analysis. Organ Res Methods. 2004;7(2):127–150. doi:10.1177/1094428104263672
23. Manning WG, Mullahy J. Estimating log models: to transform or not to transform? J Health Econ. 2001;20(4):461–494. doi:10.1016/S0167-6296(01)00086-8
24. Renkens KL, Payner TD, Leipzig TJ, et al. A multicenter, prospective, randomized trial evaluating a new hemostatic agent for spinal surgery. Spine (Phila Pa 1976). 2001;26(15):1645–1650. doi:10.1097/00007632-200108010-00002
25. Weaver FA, Hood DB, Zatina M, Messina L, Badduke B. Gelatin-thrombin-based hemostatic sealant for intraoperative bleeding in vascular surgery. Ann Vasc Surg. 2002;16(3):286–293. doi:10.1007/s10016-001-0073-0
26. Gill IS, Ramani AP, Spaliviero M, et al. Improved hemostasis during laparoscopic partial nephrectomy using gelatin matrix thrombin sealant. Urology. 2005;65(3):463–466. doi:10.1016/j.urology.2004.10.030
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.