Back to Journals » Patient Preference and Adherence » Volume 19
Real-World Acne Treatment Patterns, Preferences, and Adherence in Thailand: A Cross-Sectional Analysis
Authors Paichitrojjana A ![]() , Paichitrojjana A
, Paichitrojjana A ![]()
Received 22 July 2025
Accepted for publication 11 October 2025
Published 16 October 2025 Volume 2025:19 Pages 3197—3210
DOI https://doi.org/10.2147/PPA.S555557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Anon Paichitrojjana,1 Anand Paichitrojjana2
1School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, Bangkok, Thailand; 2Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Anon Paichitrojjana, Email [email protected]
Background: Acne vulgaris is a common, chronic skin condition that affects both physical appearance and psychological well-being. Effective management requires long-term, personalized strategies that prioritize maintenance and adherence. Most research has focused on Western populations, primarily examining topical and oral therapies, while procedural treatments are more prevalent in Thailand. This study aims to explore treatment preferences among individuals with acne, the factors influencing their choices, and adherence patterns.
Materials and Methods: A cross-sectional survey was conducted among 1,237 Thai participants aged 18 to 45 years, utilizing a validated 22-item self-administered questionnaire. The questionnaire assessed demographics, treatment usage, preferences, decision-making factors, satisfaction, and adherence. Statistical analyses included descriptive statistics, chi-square tests, t-tests, and multivariate logistic regression analyses.
Results: Topical treatments were the most used (68.07%), although only 16.25% of patients relied on them alone. Comedone extraction was reported by 51.90% of patients, and 42.28% used over-the-counter products. Oral therapies were less common, with antibiotics used by 16.01% and isotretinoin by 10.67%. Overall, most patients reported using combination therapies. The treatment preferences of the participants closely aligned with their actual usage. Adherence to acne treatment was only observed in 33.71% of participants. Factors significantly associated with higher adherence included a longer treatment duration, the use of multiple treatment modalities, a greater impact of acne on quality of life, and high satisfaction with treatment and communication with healthcare providers. Key barriers to adherence included the cost of treatment, lack of noticeable results, and side effects.
Conclusion: This study reveals real-world patterns of acne treatment in Thailand, where patients commonly favor topical and procedural therapies, while oral treatments are underutilized. Gender differences, cultural norms, and social influences shape choices. These findings underscore the need for culturally sensitive patient education and evidence-based guidance to improve adherence, satisfaction, and treatment outcomes.
Plain Language Summary: Acne is a common skin condition that affects self-confidence and appearance. While many studies on treatment focus on Western countries, there is limited information on how people in Thailand manage their acne and their treatment adherence.
This study surveyed 1,237 individuals in Thailand with acne to understand the treatments they use, their preferences for those treatments, and their adherence to treatment plans. Researchers employed a detailed questionnaire to collect information from participants aged 18 to 45 from various regions of Thailand.
The study revealed that most individuals employed a combination of treatments, particularly topical creams and procedures such as acne injections or extractions. In contrast, fewer individuals opted for oral medications like antibiotics or isotretinoin. Only one in three participants consistently adhered to their treatment plan. People were more likely to adhere to their treatment regimen if they had been managing their acne for an extended period, had utilized multiple treatment types, felt that their acne significantly impacted their daily life, or were satisfied with the treatment and communication they received from their doctor. Cost, side effects, and lack of quick results were the main reasons people stopped using their acne treatments.
The findings suggest that in Thailand, many individuals choose their treatments based on convenience, aesthetics, and cost, rather than solely on medical advice. To improve treatment outcomes, healthcare providers should work closely with patients, clearly explain the available treatment options, and consider what is most important to each individual when planning their care with patient-centered management.
Keywords: acne vulgaris, patient preference, patient adherence, acne treatment, patient-centered care, healthcare accessibility
Introduction
Acne vulgaris is a common, chronic skin condition that primarily affects adolescents, but it can also occur in adults. The global prevalence of acne has increased over the past three decades, rising from 8,563.4 per 100,000 people in 1990 to 9,790.5 per 100,000 in 2021, at an annual rate of approximately 0.43%.1 This condition significantly affects physical health and psychological well-being, highlighting its prevalence and complex causes.2
The goals of acne treatment are to reduce lesions, prevent scarring, improve appearance, and alleviate psychological distress. Effective management typically requires a consistent, multifaceted approach. Acne recurrence is common and influenced by individual factors, making maintenance therapy essential for personalized, long-term management.3–5
Understanding patient preferences is crucial for successful acne treatment, as it necessitates long-term adherence and may involve potential side effects and costs. Aligning treatment plans with patients’ values enhances adherence and outcomes. Incorporating shared decision-making also boosts patient satisfaction and engagement.
Gender differences in acne require attention, as men and women exhibit distinct differences in severity perceptions, healthcare-seeking behaviors, and treatment adherence. Women may pursue cosmetic treatments, while social or occupational factors may influence men’s adherence. Additionally, social media and digital influencers have a significant impact on health behaviors, particularly among young individuals. They shape expectations, drive preferences for products or procedures, and influence treatment behaviors.6 This highlights the need to investigate patient preferences and adherence in real-world contexts.
Research on patient preferences and adherence to acne vulgaris treatment has primarily focused on Western communities. Most existing studies have examined only topical and oral medications.7–9 This differs from the situation in Thailand, where procedural treatments and clinician visits for acne are more accessible and commonly utilized. Addressing this gap is essential for delivering more effective and culturally sensitive treatments.
This study aimed to evaluate real-world patterns of acne treatment, patient preferences, and adherence behaviors among individuals in Thailand. It sought to identify the factors influencing treatment choices and adherence, compare differences between genders, and assess how current practices align with clinical guidelines. The goal was to inform the development of more patient-centered strategies for managing acne.
Materials and Methods
Study Design and Population
This study was designed as a cross-sectional survey conducted among Thai individuals aged 18 to 45 with self-reported acne vulgaris. Eligible participants completed a self-administered questionnaire covering demographics, clinical profiles, treatment preferences, decision-making factors, patient satisfaction, and treatment adherence. Only those who provided written informed consent were included in the study.
The sample size was determined using a standard statistical formula with a 95% confidence level (z = 1.96), an estimated proportion (p) of 0.513, and a margin of error (e) of 0.03. The formula used is n = (Z²) × p(1-p) / E2. To account for potential errors, an additional 10% of questionnaires were collected, resulting in an approximate sample size of 1,187.
Questionnaire Development
The authors developed a comprehensive questionnaire to assess patient preferences and adherence in the management of acne vulgaris. Following validation by three dermatologists and ophthalmologists, a pilot survey was conducted with 30 participants. The questionnaire showed high reliability, with Cronbach’s alpha coefficient exceeding 0.8.
Questionnaire Structure
The study used a 22-item self-administered questionnaire covering six domains: (1) Demographic and Clinical Characteristics (Items 1–8) such as age, gender, acne severity, and quality of life impact; (2) Current Treatment Usage (Items 9–12) for treatment types, duration, and satisfaction; (3) Treatment Preferences (Item 13) rated on a 5-point Likert scale; (4) Factors Influencing Treatment Choices (Items 14–16) addressing motivations and barriers; (5) Adherence to Treatment (Items 17–21), using a 5-point Likert scale; and (6) Barriers to Adherence (Item 22) identifying reasons for skipping treatment.
Data Collection
This survey included participants from urban and semi-urban areas, using paper questionnaires collected at dermatology clinics, academic institutions, and shopping malls. The investigators also shared the survey via Google Forms on social media platforms, including email, Facebook, and Line, to encourage broader participation.
Evaluation and Analysis
Demographic characteristics and clinical data (Section 1) were summarized using descriptive statistics: frequencies, percentages, and means with standard deviations (SDs). Treatment preferences (Section 2) were evaluated through 5-point Likert scales, with mean scores calculated; scores of four or higher indicated a strong preference. Adherence behaviors (Section 3) were measured by summing scores across five questions, with good adherence defined as a score of 20 or higher. Mean total adherence scores and SDs were reported. As the study relied on self-reported acne diagnoses and included both online and offline recruitment, potential recall and selection biases may be present.
Statistical Analysis
Descriptive statistics summarized participant characteristics, current treatment patterns, treatment satisfaction, treatment preferences, and adherence behaviors. Categorical variables were presented as frequencies and percentages, while continuous variables were reported as means with SDs.
Group comparisons (eg, adherent vs non-adherent participants; male vs female participants) were conducted using chi-square tests or Fisher’s exact tests for categorical variables, and independent t-tests or Mann–Whitney U-tests for continuous variables, as appropriate. The normality of continuous variables was assessed using the Shapiro–Wilk test. Univariate logistic regression was used to identify factors associated with poor adherence (score < 20). Variables with a p-value <0.20 in the univariate analysis were subsequently included in multivariate logistic regression models using a backward elimination approach. Crude odds ratios (ORs) and adjusted odds ratios (AORs), along with 95% confidence intervals (CIs), were reported. Statistical significance was set at a two-tailed p-value <0.05.
Model performance was evaluated using the area under the receiver operating characteristic (ROC) curve and the Hosmer–Lemeshow goodness-of-fit test. All statistical analyses were conducted using STATA version 14.0 (StataCorp, College Station, TX, USA).
Results
Participant Characteristics
A total of 1,237 participants were included in the study, with a majority being female (66.3%). The demographic characteristics of the participants are outlined in Table 1. The average age of the participants was 29.56 ± 7.12 years. Males were slightly older than females, with mean ages of 30.09±7.20 years for males and 29.29±7.07 years for females.
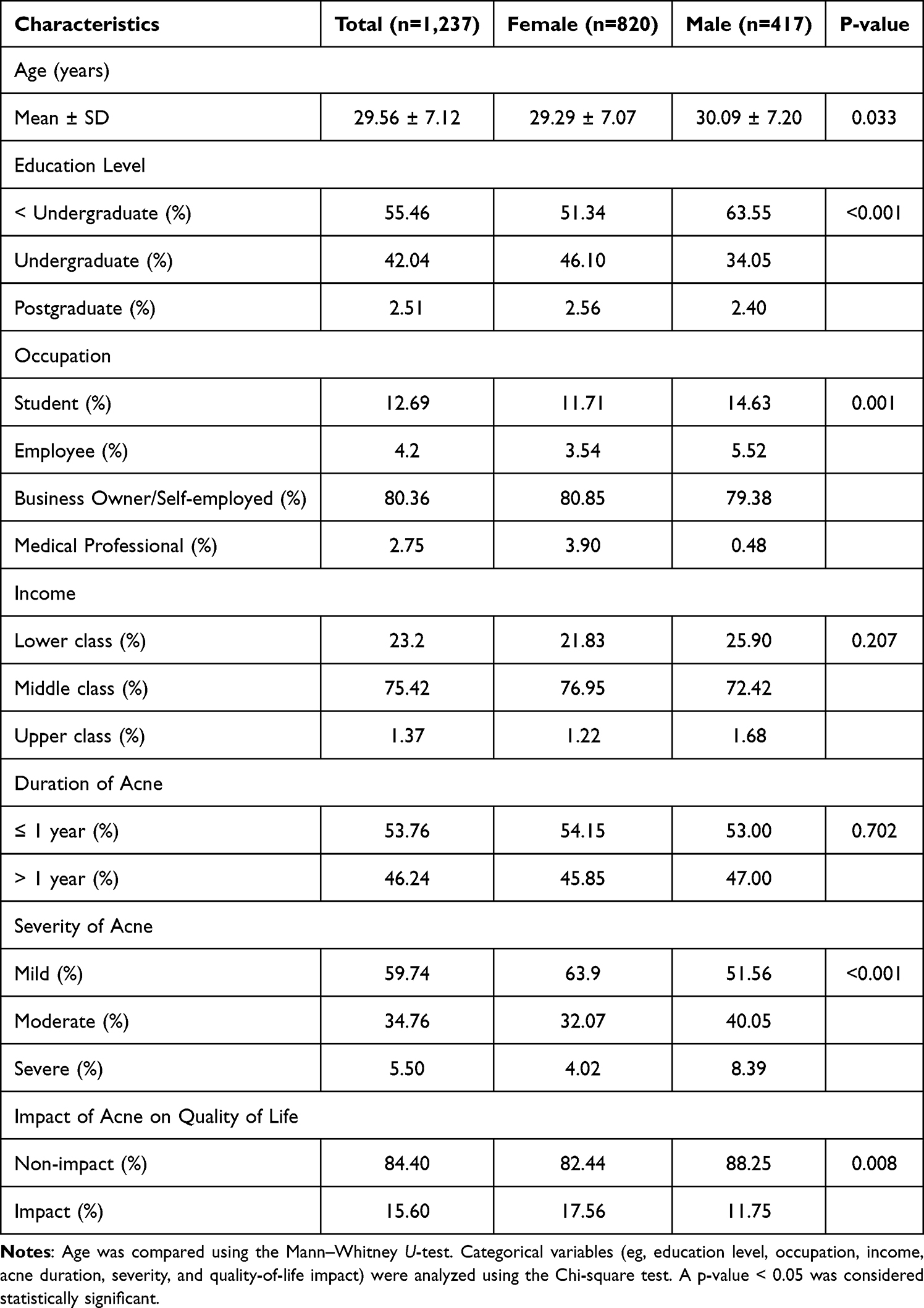 |
Table 1 Demographic Characteristics of the Study Population |
Most participants had not completed a university degree (55.46%), with a higher percentage of males (63.55%) than females (51.34%) lacking an undergraduate education (P < 0.001). Occupational status showed significant gender variation (P = 0.001), with more males identifying as students (14.63% vs 11.71%) and employed (5.52% vs 3.54%). Income distribution was similar across genders (P = 0.207), with the majority classified as middle class (75.42%).
The duration of acne was similar between genders, with 46.24% of participants reporting that it lasted over a year (P = 0.702). However, acne severity differed significantly (P < 0.001), with females more likely to report mild acne (63.9%), while males had higher rates of moderate (40.05%) and severe acne (8.39%). The impact on quality of life also varied (P = 0.008), as more females reported an effect (17.56%) compared to males (11.75%).
Current Acne Treatment Information
All participants reported that topical medications were the most used treatment, with a usage rate of 68.07%. The use of these medications was significantly higher among females compared to males, with rates of 72.20% and 59.95%, respectively (P < 0.001).
Many participants reported undergoing procedural treatments for acne. Comedone extraction was the most common procedure, affecting 51.90% of participants, particularly females (55.73%) more than males (44.36%; P < 0.001). Acne injections were used by 27.32% of participants overall, with a higher prevalence in females (34.63%) compared to males (12.95%; P < 0.001). Laser or light therapy was also more common in females (14.39%) compared to males (7.19%; P < 0.001), with an overall usage rate of 11.96%.
Over-the-counter treatments (OTC) revealed notable gender differences, with cosmeceuticals used more by males (51.08%) than females (37.80%, P = 0.037). The use of supplements did not differ significantly by gender.
In terms of oral treatments, 16.01% of participants reported using oral antibiotics, which were used more frequently by females (17.68%) than by males (12.71%, P = 0.024). Additionally, 10.67% of participants reported using oral isotretinoin, with no significant gender difference observed (P = 0.284).
Most participants (56.43%) had received treatment for over three months, with a significant gender difference noted (P = 0.032). Satisfaction levels revealed that 69.68% of respondents were satisfied with their acne treatment, and 74.86% with healthcare communication. No significant gender differences were found in satisfaction with treatment (P = 0.836) or provider communication (P = 0.502) (Table 2).
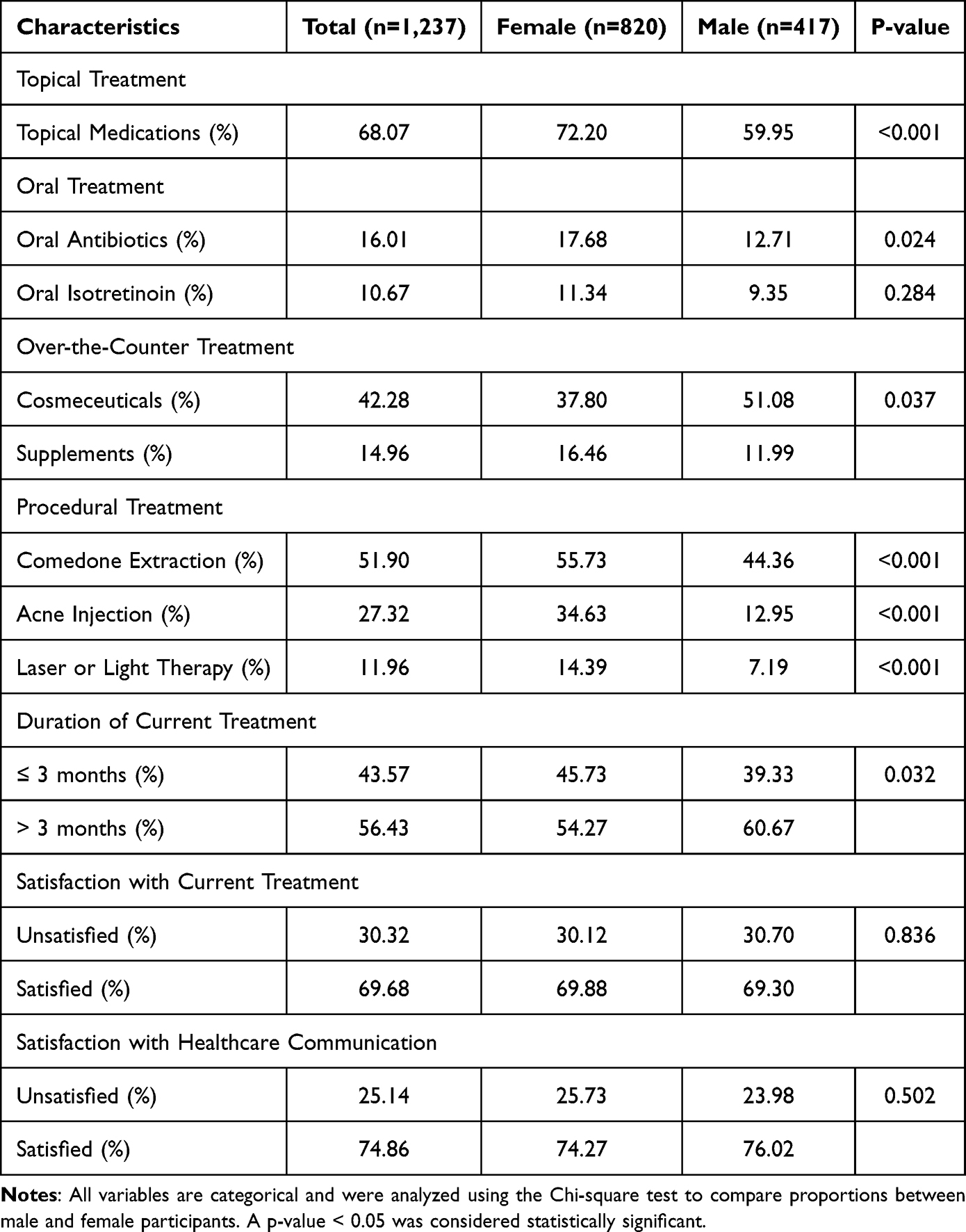 |
Table 2 Current Acne Treatment Information of Study Participants |
Treatment Patterns
Only 16.25% of participants (n = 201) used topical treatment alone. Most chose combination therapies: topical plus procedural treatments accounted for 14.87% (n = 184), while topical, procedural, and OTC treatments made up 10.27% (n = 127). Additionally, 8.97% (n = 111) used a mix of topical, procedural, and oral treatments, and 4.93% (n = 61) utilized all four modalities: topical, oral, OTC, and procedural (Table 3).
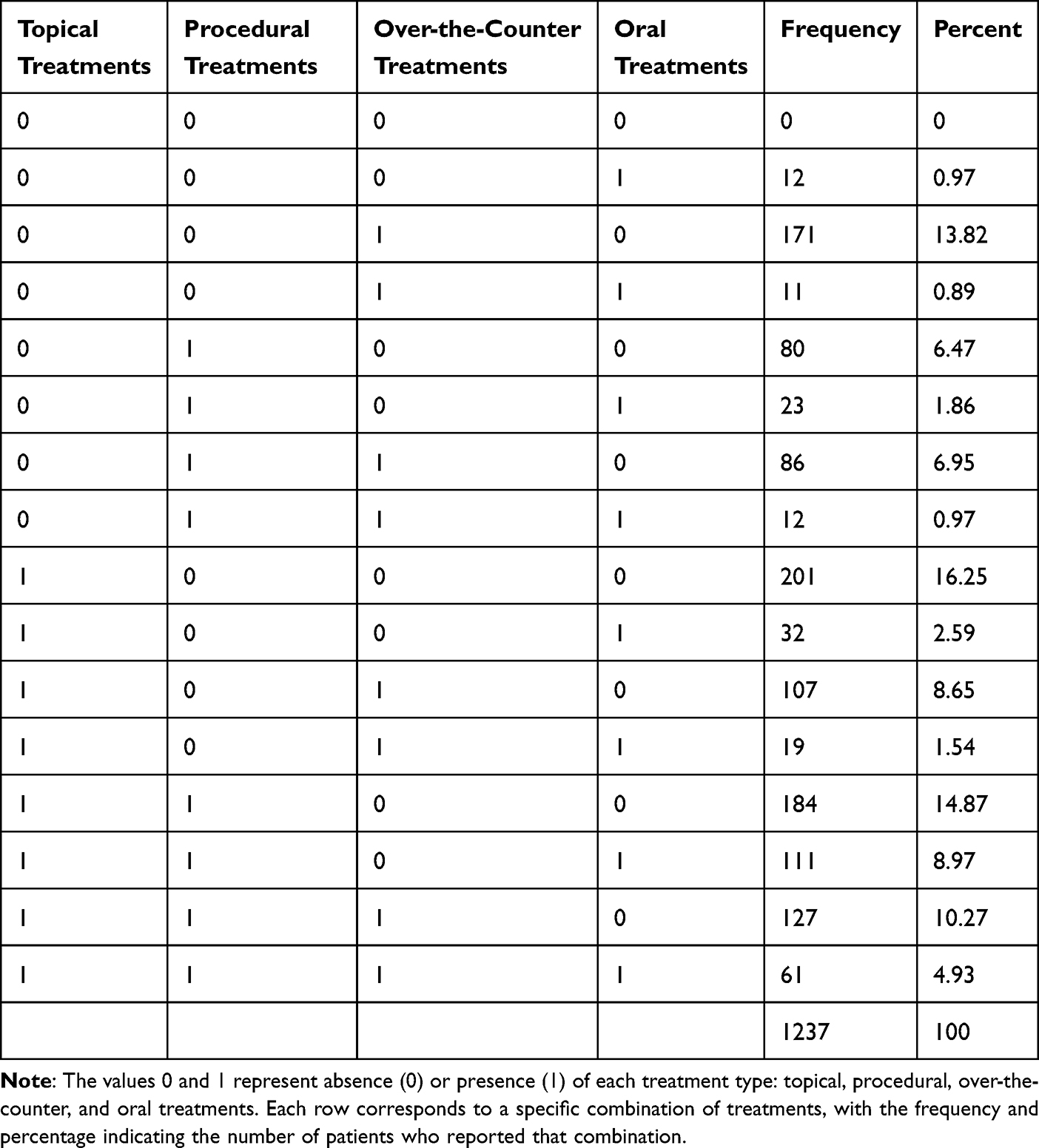 |
Table 3 Treatment Patterns of Study Participants |
Treatment Preferences
Participants indicated their treatment preferences on a 5-point Likert scale. Topical medications scored the highest with a mean of 4.24 ± 0.94, and there was no significant difference between genders (P = 0.244).
Among the oral treatments, this option was the least preferred. Males showed a significantly higher preference for oral antibiotics (mean score, 3.00 ± 1.20) than females (mean score, 2.80 ± 1.25), with a P-value of 0.007. Males also preferred oral isotretinoin more than females (2.93 ± 1.20 vs 2.71 ± 1.27), with a P-value of 0.004.
For OTC, the mean preferences were moderate for cosmeceuticals (3.86 ± 1.11) and supplements (3.44 ± 1.22), with no significant gender differences (P = 0.226 and 0.140).
Males showed a higher preference for comedone extraction (3.68 ± 1.26 vs 3.48 ± 1.32 for females, P = 0.008) and acne injection (3.26 ± 1.35 vs 3.05 ± 1.38, P = 0.012), while preferences for laser or light therapy were similar (P = 0.100) (Table 4).
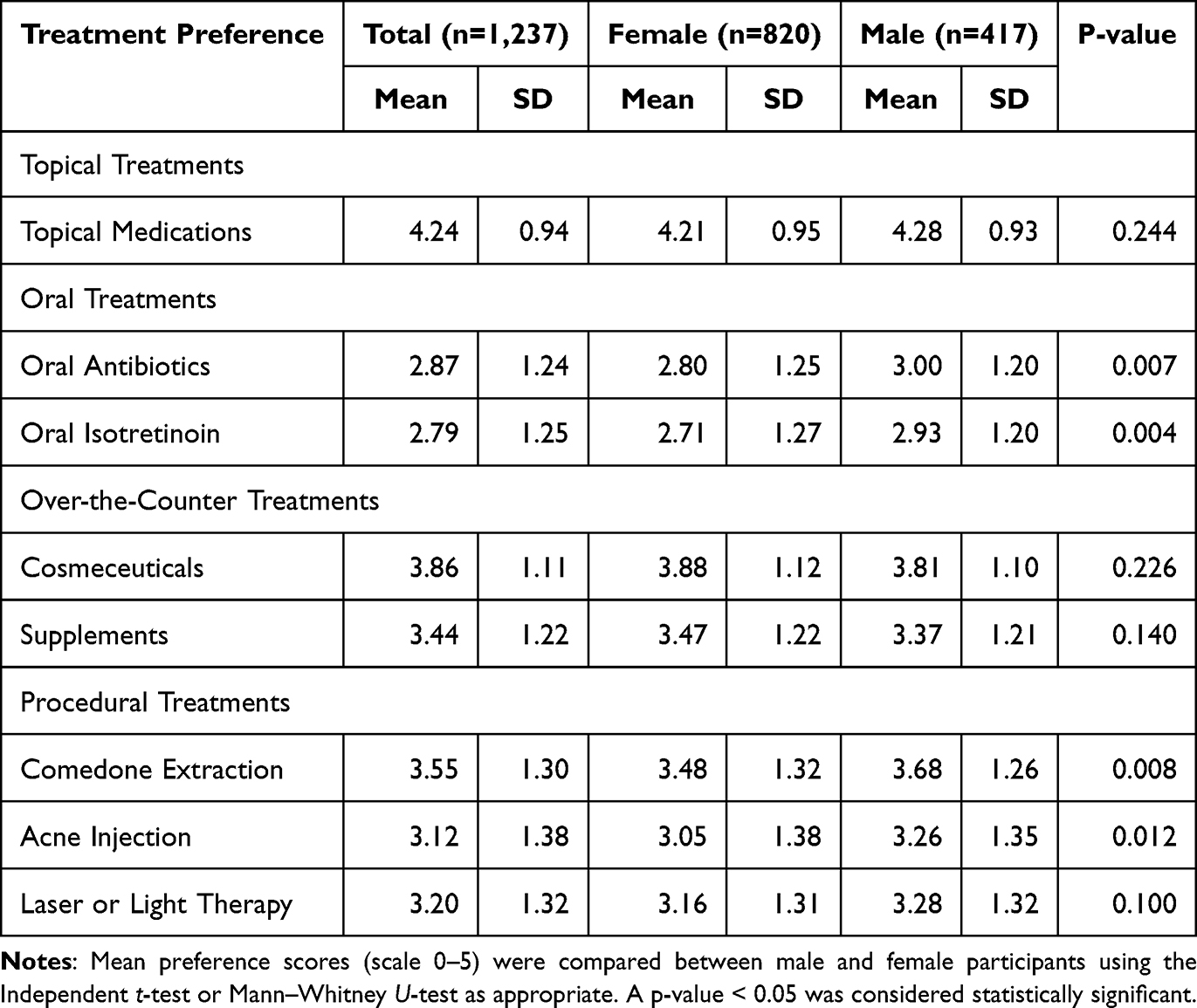 |
Table 4 Treatment Preferences of Study Participants |
Factors in Choosing Acne Treatments
Participants assessed factors influencing their decisions regarding acne treatment using a 5-point Likert scale. The most important factors were proven long-term effectiveness (mean = 4.39 ± 0.83), affordability (mean = 4.31 ± 0.87), quick results (mean = 4.30), and low side effects (mean = 4.27 ± 0.91).
Males rated “works quickly” (mean = 4.38) and “proven long-term effectiveness” (mean = 4.47) higher than females (means of 4.25 and 4.35, respectively; P = 0.018 and P = 0.020). No significant gender differences were found for ease of use, affordability, doctor prescriptions, or social influences (Table 5).
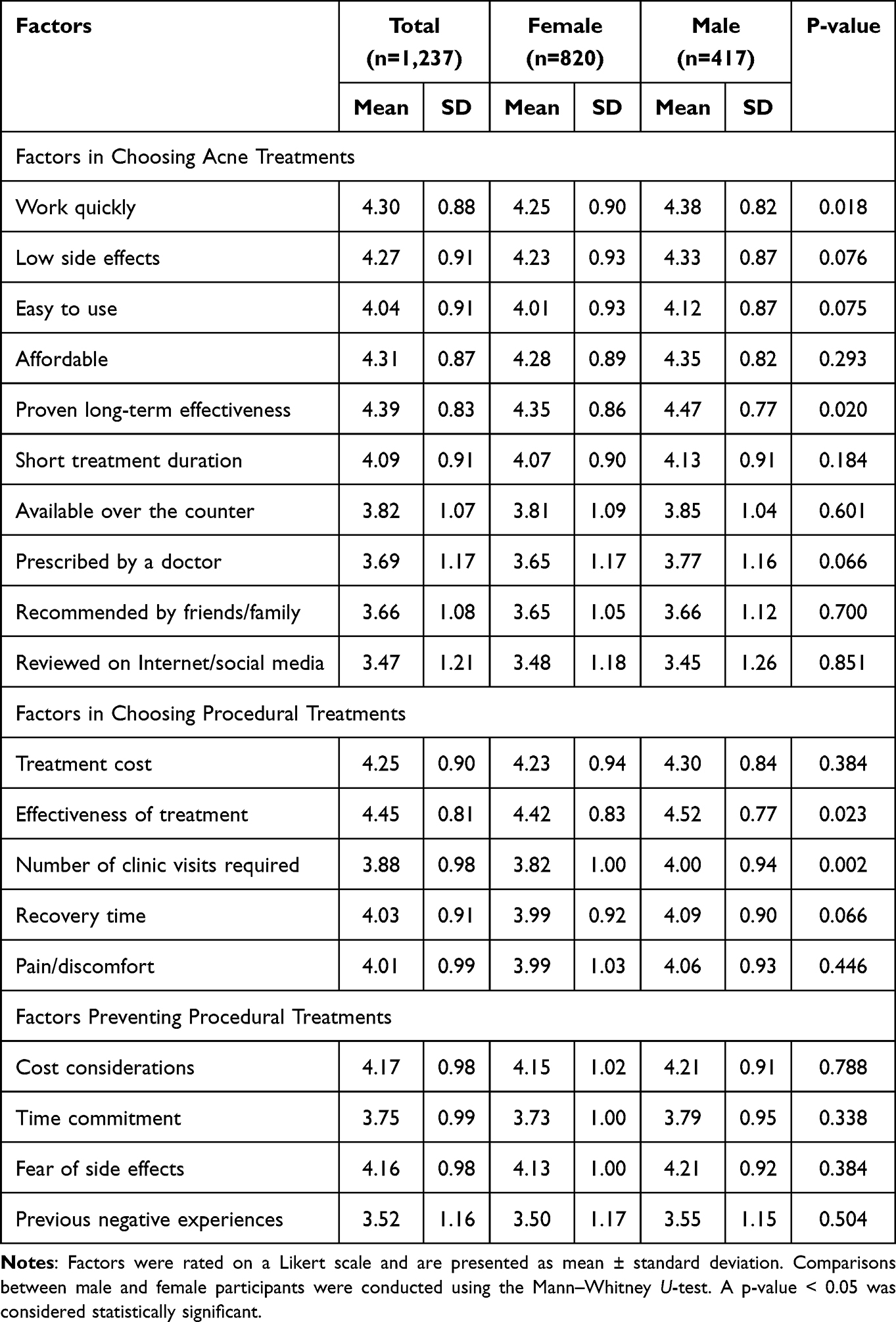 |
Table 5 Factors Influencing Acne Treatment and Procedural Choices |
Factors in Choosing Procedural Treatments
The effectiveness of treatment received the highest rating at 4.45 ± 0.81, followed by the cost at 4.25 ± 0.90 and recovery time at 4.03 ± 0.91. Males rated “treatment effectiveness” (P = 0.023) and “fewer clinic visits” (P = 0.002) as significantly more important compared with females (Table 5).
Factors Preventing Procedural Treatments
Cost considerations (mean = 4.17 ± 0.98) and the fear of side effects (4.16 ± 0.98) were the most common barriers to accessing procedural acne treatments. No significant gender differences were observed across any of the listed barriers (Table 5).
Adherence to Acne Treatment and Associated Factors
Among the total 1,237 participants, 417 (33.71%) were deemed adherent with a cumulative score ≥20. Logistic regression analyses revealed that no demographic factors (age, sex, education, occupation, income) or clinical characteristics (acne duration, severity) significantly predicted adherence. However, participants reporting that acne impacted their quality of life were more likely to adhere to treatment, with an adjusted odds ratio of 1.59 (95% CI: 1.02–2.46, P = 0.04).
Participants using a greater variety of acne treatments showed significantly higher adherence to their prescribed regimen. Specifically, using three types of treatments doubled adherence (AOR = 2.00, 95% CI: 1.37–2.92), and using four types increased it even more (AOR = 5.43, 95% CI: 2.18–13.52, p < 0.001). Longer treatment duration (over three months) was associated with better adherence (AOR = 0.60, 95% CI: 0.46–0.79, p < 0.001). High satisfaction with treatment and provider communication was a strong predictor of adherence, with satisfied individuals showing a higher likelihood of adherence (AORs of 4.73, P < 0.001, and 2.10, P = 0.001, respectively).
The multivariate model showed strong discriminative ability, with an area under the ROC curve (AUC) of 0.7367 and a goodness-of-fit test result of P = 0.096, which indicates an adequate model fit (Table 6).
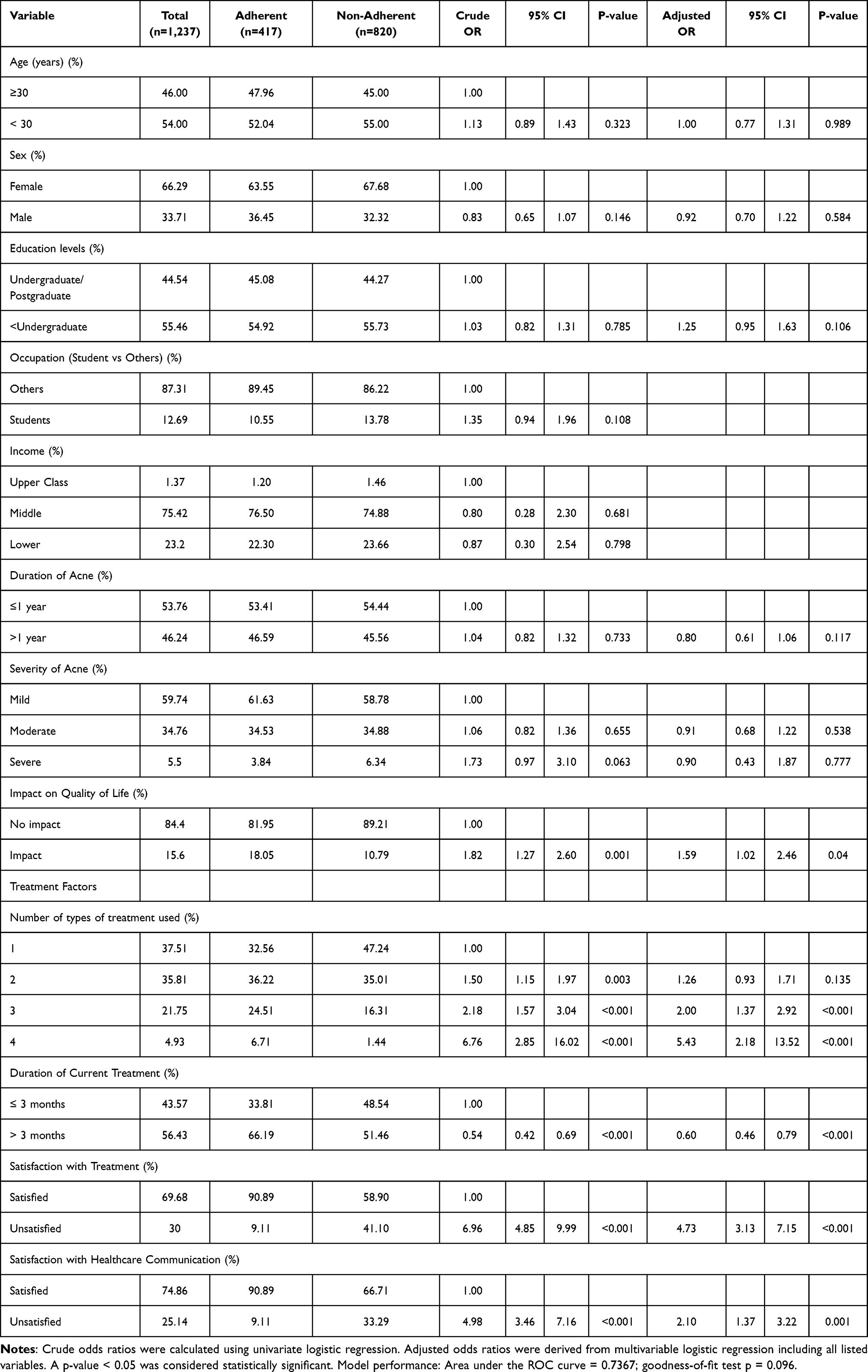 |
Table 6 Patient Adherence to Acne Treatment and Logistic Regression Analysis |
Factors in Skipping Acne Treatments
Participants rated barriers to acne treatment adherence on a 5-point Likert scale. The most common reasons for skipping treatments were cost (mean = 3.76), lack of noticeable results (mean = 3.70), side effects (mean = 3.59), and time commitment (mean = 3.40). Less common barriers included forgetfulness (mean = 3.08) and treatment complexity (mean = 3.09). No significant differences existed between genders regarding these barriers (P > 0.05) (Table 7).
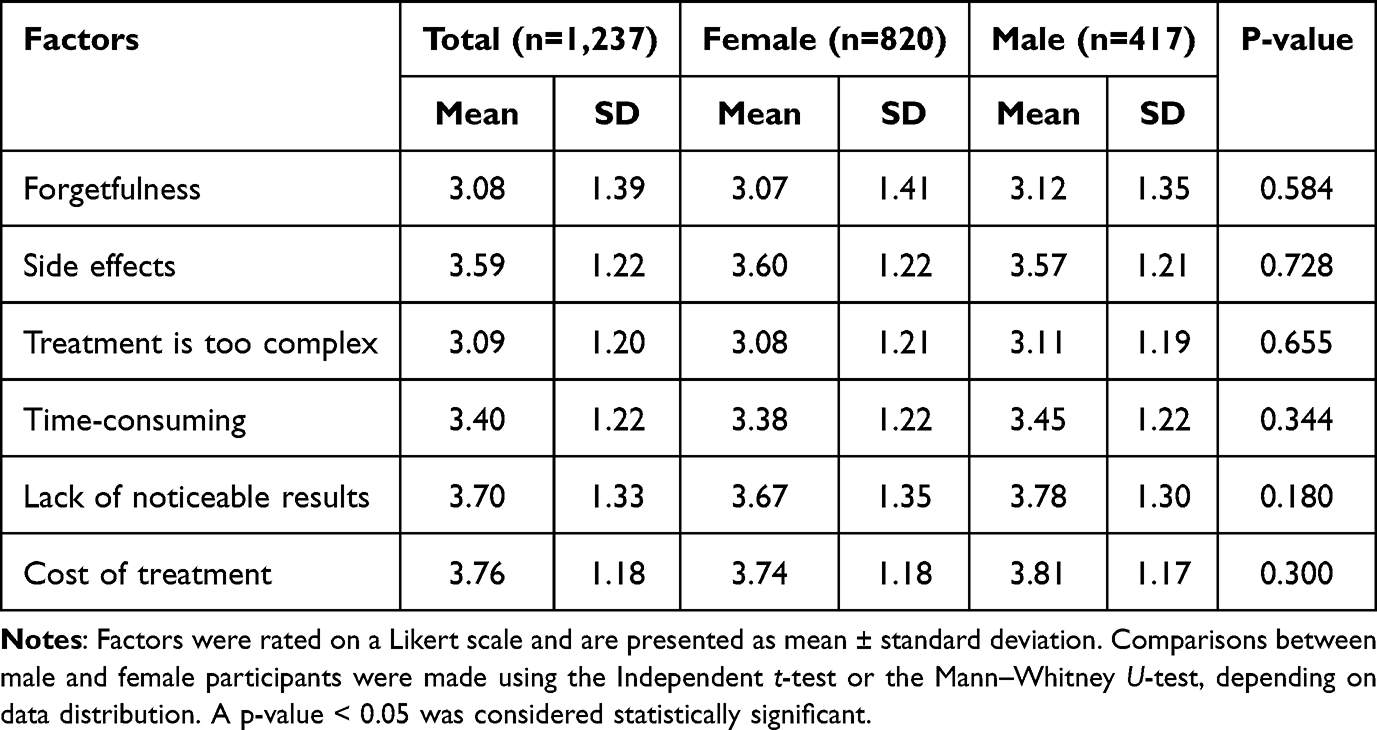 |
Table 7 Factors in Skipping Acne Treatments |
Discussion
This study provides comprehensive insights into patterns, preferences, and adherence behaviors related to acne treatment among Thai participants. It focuses on real-world acne management and identifies actionable areas to enhance patient outcomes. When compared to international literature, several similarities and differences are noted, offering valuable context for both local and global acne care practices.
Current Acne Treatment
The most common treatment among participants was topical therapy, followed by comedone extraction and cosmeceuticals. This finding aligns with a review study that also identified topical therapies as the first-line treatment for mild to moderate acne, supporting global guidelines.3,10 The high use of these treatments is likely due to their convenience, affordability, and accessibility, as many topical medications can be purchased over the counter in Thailand. Comedone extractions are also readily available in both clinics and beauty salons.
The treatment choices in this study can be better understood within the cultural and social context of Thailand. Differences in treatment behaviors between genders likely reflect both variations in perceptions of acne severity and culturally shaped expectations. Procedural treatments were more common among females, specifically comedone extraction, acne injections, and laser therapies. This trend may stem from sociocultural factors, including greater aesthetic concerns and a higher willingness to attend clinic visits, along with targeted marketing of these treatments to women. By contrast, men may be less likely to undergo procedural treatments due to cultural norms, time constraints, and healthcare-seeking behaviors.
An analysis of treatment patterns reveals that while topical treatments are commonly used, many participants prefer combinations with procedural therapies and OTC products, expecting quicker results. This trend highlights a personalized, trial-and-error approach to acne care.
Topical acne treatments include prescription medications applied directly to the skin, such as retinoids (like tretinoin and adapalene), benzoyl peroxide, and topical antibiotics. These require formal approval as they are regulated as drugs. In contrast, cosmeceuticals are over-the-counter products containing active ingredients such as low-strength salicylic acid, AHA, niacinamide, tea tree oil, and zinc. Unlike topical medications, cosmeceuticals are not regulated as drugs and have less stringent evidence requirements. This study also revealed a high use of cosmeceuticals and dietary supplements among Thai patients, indicating that they often self-manage their acne care alongside professional treatment.
The use of oral acne treatments in Thailand is significantly lower than in the USA, with only 16.01% of participants using oral antibiotics compared to 31.3% in the USA, and 10.67% using isotretinoin versus 13.7% in the U.S.11 While the American Academy of Dermatology (AAD) guidelines supports systemic therapies for moderate to severe acne,3 treatment decisions in Thailand often focus on aesthetic goals, accessibility, and patient autonomy instead of strict adherence to clinical guidelines. This may reflect cultural preferences for non-systemic treatments, as well as concerns about costs and side effects.
Treatment Preferences
In this study, participants’ treatment preferences closely matched their actual usage patterns. Topical medications were both the most preferred and the most widely used treatment option. The use of oral acne therapies was the lowest due to concerns about side effects, access to prescriptions, and the predominance of mild acne in the study population. Males showed a significantly higher preference for oral antibiotics and isotretinoin, likely due to a greater incidence of moderate-to-severe acne among them.
In contrast, females tended to favor procedural treatments more, likely due to beauty-related motivations and the availability of aesthetic care options. Cosmeceuticals and dietary supplements demonstrated a moderate preference and high usage, particularly among males, suggesting a tendency towards self-management. The availability of both types of treatments in Thailand, combined with a strong preference for aesthetic outcomes, influences this landscape.
Male participants also showed a higher preference for comedone extraction and acne injections, but underwent these procedures less frequently than females. This suggests potential barriers to access, including lower health-seeking behavior, time constraints, cost concerns, and sociocultural norms that prioritize aesthetic care for women over men.
Factors in Choosing Acne Treatments
Participants prioritized long-term effectiveness, affordability, rapid results, and minimal side effects when choosing acne treatments. Male valued rapid results and long-term effectiveness more than female, highlighting their preference for quick and lasting solutions.
Social media and online reviews have a moderate influence on treatment decisions for both males and females. Females are particularly swayed by social media recommendations, aligning with previous research on its impact on their health behaviors.6
When choosing procedural treatments, both sexes valued effectiveness, cost, and recovery time. However, men prioritized fewer clinic visits and treatment effectiveness, favoring efficient interventions that minimally disrupt their routines.
Common barriers to procedural acne treatments include cost, fear of side effects, and time commitment, affecting all genders similarly. This aligns with previous research on barriers to acne treatment, including the high cost of treatment and potential indirect expenses, difficulty accessing appropriate medical care, and concerns about treatment-related side effects.7 Notably, previous negative experiences did not significantly deter users, suggesting they may still be willing to try procedures if other barriers are resolved.
Adherence to Acne Treatment
Adherence rates for acne treatments vary by study population, type of therapy (oral vs topical), and measurement methods. Most studies depend on subjective self-reports, while only a few utilize objective methods such as pill counts and pharmacy refill data.12 The lack of standardized measurement contributes to variability in reported rates, complicating study comparisons. A systematic review found adherence rates of 76.3% for oral and 75.8% for topical medications, with no significant difference. Key reasons for poor adherence include side effects, young age, and forgetfulness.8 An Iranian study reported that only about 15% of patients had high adherence. Those consistent with topical treatments were likelier to adhere to systemic ones, while food exacerbations and perceived disease severity were also linked to overall adherence.13
The present study shows that only 33.7% of Thai patients consistently adhere to acne treatment. This adherence rate is lower than that reported in previous studies, such as a worldwide observational study by Dréno et al, which found rates of 46–60%,14 and a survey by Pawin et al, which reported a rate of 54% in France.15 Many Thai participants discontinue treatment when symptoms improve or due to side effects like dryness and irritation. They also apply medication irregularly and struggle with follow-up. These findings suggest a need for enhanced patient education, simplified regimens, and improved communication between patients and healthcare providers.
Demographic factors, including age, gender, education, occupation, income, acne duration, and severity, showed no significant impact on treatment adherence in this Thai population, indicating that psychological factors are more influential.
Individuals who felt acne affected their quality of life had higher adherence. Although males had more severe acne, females reported a greater impact on their quality of life, suggesting higher psychosocial sensitivity. This highlights the need for gender-sensitive treatment approaches.
Adherence to treatment improved with the use of multiple therapy types. Patients engaged in multimodal regimens often felt more committed and saw greater benefits. Additionally, treatment lasting over three months correlated with better adherence, likely due to established routines and recognized benefits. High satisfaction with treatment and effective healthcare communication were also key predictors of adherence, emphasizing the importance of communication and trust in the treatment process.
The primary reasons for discontinuing acne treatments are cost, lack of noticeable results, and side effects. Participants often stop due to financial constraints, slow improvements, and discomfort from adverse effects. Interestingly, treatment complexity and forgetfulness were rated low, suggesting that while simplicity matters, the expectation for quick results plays a more influential role among Thai patients. This contrasts with previous studies that identified side effects, young age, and forgetfulness as the top factors affecting adherence.8,16
These findings have important implications for clinical practice and health policy. Acne management in Thailand may be improved by aligning evidence-based recommendations with patient preferences, as patients generally favor topical and procedural treatments over oral therapies. To enhance adherence, clinicians should involve patients in treatment planning, set realistic expectations, and provide structured follow-up. Education on the role and safety of oral therapies remains crucial, particularly for patients with moderate to severe cases. Incorporating procedural options, such as comedone extraction and acne injections, can enhance patient adherence and improve treatment outcomes. Gender-specific preferences should also be considered, with males more inclined toward systemic therapies and females toward procedural approaches. Addressing barriers such as cost and side effects through affordable, well-tolerated regimens and clear communication is crucial. Policymakers and clinicians can build on these insights to design culturally sensitive educational strategies and promote patient-centered care for acne.
As this cross-sectional study cannot establish causality or temporal changes, longitudinal research is needed to better define treatment patterns, adherence, and outcomes across diverse populations.
Limitations of the Study
Several limitations should be acknowledged. The cross-sectional design restricts causal inferences regarding the relationship between treatment type and adherence. Reliance on self-reported diagnoses and behaviors may introduce recall and social desirability biases, while the mix of online and offline recruitment could result in selection bias and limit representativeness. Although the sample size was large, it may not fully reflect all Thai people with acne, particularly those in rural areas. Finally, important clinical and psychosocial factors, such as depression and stigma, which may influence treatment choices and adherence, were not assessed.
Conclusion
This study highlights real-world patterns of acne treatment, preferences, and adherence in Thailand, demonstrating how choices are influenced not only by clinical factors but also by gender differences, cultural norms, and social factors such as media exposure. Procedural therapies were prevalent, reflecting both accessibility of beauty clinics and sociocultural expectations around appearance. These findings underscore the need for culturally sensitive patient education and evidence-based clinical guidance to improve adherence and outcomes.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Ethics Statement
The present study was conducted in accordance with the World Medical Association Declaration of Helsinki. All subjects provided written informed consent, and the study protocol was reviewed and approved by the Ethical Research Committee of Mae Fah Luang University, with approval number COE 232/2024.
Acknowledgments
The authors express their gratitude to Mae Fah Luang University for providing financial support for the publication charges of this work.
Funding
The authors declare that no financial support was received for the research.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Zhu Z, Zhong X, Luo Z, et al. Global, regional and national burdens of acne vulgaris in adolescents and young adults aged 10-24 years from 1990 to 2021: a trend analysis. Br J Dermatol. 2025;192(2):228–237. doi:10.1093/bjd/ljae352
2. Smith H, Layton AM, Thiboutot D, et al. Identifying the impacts of acne and the use of questionnaires to detect these impacts: a systematic literature review. Am J Clin Dermatol. 2021;22(2):159–171. doi:10.1007/s40257-020-00564-6
3. Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):
4. Rocha M, Barnes F, Calderón J, et al. Acne treatment challenges - Recommendations of Latin American expert consensus. An Bras Dermatol. 2024;99(3):414–424. doi:10.1016/j.abd.2023.09.001
5. Ibrahim S, Osman B, Awaad RM, Abdoon I. acne vulgaris relapse in sudanese patients treated with oral isotretinoin: rate and predictive factors. J Multidiscip Healthc. 2023;16:839–849. doi:10.2147/JMDH.S405509
6. Ertekin SS, Salici NS, Manav Bas V, et al. Influence of social media and internet on treatment decisions in adult female acne patients: a cross-sectional survey study. Dermatol Pract Concept. 2024;14(3):e2024156. doi:10.5826/dpc.1403a156
7. Perche P, Singh R, Feldman S. Patient preferences for acne vulgaris treatment and barriers to care: a survey study. J Drugs Dermatol. 2022;21(11):1191–1195. doi:10.36849/JDD.6940
8. Snyder S, Crandell I, Davis SA, Feldman SR. Medical adherence to acne therapy: a systematic review. Am J Clin Dermatol. 2014;15(2):87–94. doi:10.1007/s40257-014-0063-y
9. Lam Hoai XL, De Maertelaer V, Simonart T. Real-world adherence to topical therapies in patients with moderate acne. JAAD Int. 2021;2:109–115. doi:10.1016/j.jdin.2020.12.006
10. Li Y, Hu X, Dong G, Wang X, Liu T. Acne treatment: research progress and new perspectives. Front Med. 2024;11:1425675. doi:10.3389/fmed.2024.1425675
11. Adelman MJ, Sivesind TE, Weber I, et al. Prescribing patterns of oral antibiotics and isotretinoin for acne in a colorado hospital system: retrospective cohort study. JMIR Dermatol. 2023;6:e42883. doi:10.2196/42883
12. Balkrishnan R, Kulkarni AS, Cayce K, Feldman SR. Predictors of healthcare outcomes and costs related to medication use in patients with acne in the United States. Cutis. 2006;77(4):251–255.
13. Salamzadeh J, Torabi Kachousangi S, Hamzelou S, Naderi S, Daneshvar E. Medication adherence and its possible associated factors in patients with acne vulgaris: a cross-sectional study of 200 patients in Iran. Dermatol Ther. 2020;33(6):e14408. doi:10.1111/dth.14408
14. Dréno B, Thiboutot D, Gollnick H, et al. Large-scale worldwide observational study of adherence with acne therapy. Int J Dermatol. 2010;49(4):448–456. doi:10.1111/j.1365-4632.2010.04416.x
15. Pawin H, Beylot C, Chivot M, et al. Creation of a tool to assess adherence to treatments for acne. Dermatology. 2009;218(1):26–32. doi:10.1159/000165628
16. Ling WY, Loo CH, MA NSN, Tan JL, Norazlima MA, Tan WC. The effect of medical education and counselling on treatment adherence and disease severity in patients with acne vulgaris: a non-randomised interventional study. Med J Malaysia. 2023;78(3):263–269.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patients’ Satisfaction with Obstetrics-Gynecology, and Pediatric Healthcare Services in Vietnam: A Multicentre Cross-Sectional Study
Minh Hoang P, Giang LT, Tran MD
Risk Management and Healthcare Policy 2023, 16:1411-1422
Published Date: 4 August 2023
Plasma Treatment – Results of Skin Microbiome Analysis
Watanabe C
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1269-1279
Published Date: 26 May 2025