")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Patients’ Satisfaction with Obstetrics-Gynecology, and Pediatric Healthcare Services in Vietnam: A Multicentre Cross-Sectional Study
Authors Minh Hoang P, Giang LT, Tran MD
Received 5 April 2023
Accepted for publication 28 July 2023
Published 4 August 2023 Volume 2023:16 Pages 1411—1422
DOI https://doi.org/10.2147/RMHP.S415967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jongwha Chang
Phuong Minh Hoang,1,2 Long Thanh Giang,2 Minh Dien Tran3
1Department of Finance and Accounting, National Children’s Hospital, Hanoi, Vietnam; 2Faculty of Economics, National Economics University, Hanoi, Vietnam; 3National Children’s Hospital, Hanoi, Vietnam
Correspondence: Phuong Minh Hoang, Department of Finance and Accounting, National Children’s Hospital, 18/879 La Thanh, Lang Thuong Ward, Dong Da District, Hanoi, 100000, Vietnam, Tel +84982425452, Email [email protected]
Purpose: Despite improvements in maternal and child health in Vietnam, sustained efforts are required to improve healthcare quality and resolve persistent disparities, highlighting the universal significance of customer satisfaction in healthcare. This study aims to assess patient satisfaction with healthcare services and associated factors at obstetrics-gynecology and pediatric hospitals across different geographical areas in Vietnam.
Patients and Methods: A cross-sectional study was conducted in 2019 among 647 patients or caregivers of hospitalized children at three major obstetrics-gynecology and pediatric hospitals, representing different geographical areas in Northern Vietnam. A Ministry of Health-approved satisfaction instrument was utilized to assess patient satisfaction. The instrument included 31 items measuring five dimensions of perceived satisfaction. Exploratory factor analysis examined the construct validity of the satisfaction measurement, and multivariate linear regression determined the factors associated with patient satisfaction.
Results: Among the 643 participants, 520 were female (89.87%), and nearly half were aged 18– 29 years old (43.7%). Factor analysis revealed three dimensions: “Competency and Outcomes”, “Accessibility and Procedures”, and “Facilities and Equipment”, with mean domain scores of 4.6 ± 0.43, 4.28 ± 0.67, and 4.53 ± 0.51, respectively. The proportion of participants completely satisfied with overall service quality was 48.52%, and expectation met was 34.53%. Multivariate linear regression indicated that patients from hospitals in the Red River Delta region had higher satisfaction scores than those in the Middle region across all domains (p< 0.05). Higher health insurance coverage was associated with increased satisfaction, while education level, economic status, and ethnicity also influenced satisfaction.
Conclusion: The study revealed moderate to high levels of satisfaction among patients at three major obstetrics-gynecology and pediatric hospitals in northern Vietnam. The findings may provide useful evidence for implementing hospital quality control in Vietnam, focusing on patient-centered goals.
Keywords: patient preference, quality of care, developing countries
Introduction
The main goal of all businesses, including medical services, is to achieve customer satisfaction.1–3 Understanding and examining patients’ perspectives serves as a fundamental yet indispensable methodology for assessing and refining the efficacy of a healthcare system, thereby promoting its success.4–6 In developing nations, the burgeoning focus on patient satisfaction can be attributed to empirical evidence that substantiates its role as a crucial determinant in health outcomes.7,8 Patients exhibiting a higher degree of satisfaction with the healthcare they receive and possessing a robust sense of confidence in their primary care physicians are more inclined to adhere to prescribed therapeutic regimens, ultimately resulting in superior treatment outcomes.9–11 Various factors contribute to shaping patient satisfaction, including the patients’ perceived needs, their expectations, and their actual experiences during the course of treatment. A comprehensive analysis of the existing literature on patient satisfaction reveals nine provider-related determinants of health services.12 These encompass technical care, interpersonal care, the physical environment, access (encompassing accessibility, availability, and financial considerations), organizational characteristics, continuity of care, and the outcome of care.12 Each of these components holds the potential to influence patient satisfaction. Of particular note, four determinants emerge as playing a vital role in enhancing patient satisfaction levels and exerting the most considerable impact on variations in satisfaction. These include the provision of technical treatment, the delivery of interpersonal care, the assurance of continuity of care, and the ultimate outcome of care.13 By addressing these crucial factors, healthcare providers can optimize patient satisfaction and contribute to the overall success of the healthcare system.
In Vietnam, the issue of dissatisfaction with the services provided by healthcare providers has not been afforded the priority consideration it necessitates. The concept of “considering patients as the focal point of healthcare and treatment operations” has only recently emerged as a viable approach in the country’s healthcare landscape.14 The previous healthcare system in Vietnam was disease-centric and reactive, with healthcare providers making the majority of decisions.15 The economic growth has fundamentally altered healthcare services, necessitating a transition toward a more patient-centered approach.16,17 It was not until 2016 that the Ministry of Health issued the first comprehensive standards for evaluating the quality of healthcare institutions, which included the systematic measurement of both patient and healthcare worker satisfaction.18 In addition to clinical outcomes, patient satisfaction and experience are now considered in quality evaluations.
Prior to this development, reporting of satisfaction in public medical facilities was primarily limited to individual hospital assessments and was mainly conducted for academic research purposes. The rapid economic growth and human development that Vietnam has experienced over the past two decades have contributed significantly to the improvement of maternal health and children’s well-being. Access to adequate medical care has expanded for the vast majority of children in the country, a fact underscored by the declining neonatal and under-five mortality rates, as well as the reduction in maternal deaths.19 However, despite these commendable advancements, disparities in disease burden among Vietnamese children persist, with both infectious and non-communicable diseases continuing to pose significant challenges.20 In this situation, it is imperative that efforts to improve healthcare quality are sustained and intensified, as this constitutes a critical component for achieving the Sustainable Development Goal (SDG) indicators in maternal and children’s health. There were very few studies has been conducted in Vietnam to study patients’ satisfaction with inpatients services for obstetrics-gynecology and pediatric services, mostly using self-developed non-standardized instrument to measure satisfaction obstetrics-gynecology and pediatric services. This study aims to assess patient satisfaction with healthcare services and examine the factors associated with varying satisfaction levels at different tiers of obstetrics-gynecology and pediatric hospitals using an instrument that recommended by the Ministry of Health in Vietnam. This investigation is particularly pertinent in the current context, as the Ministry of Health has recently begun implementing routine hospital quality assessments at the national level, signaling a more concerted effort to systematically monitor and improve healthcare quality and, by extension, patient satisfaction.
Materials and Methods
Study Design and Settings
We conducted a cross-sectional study in 2019 among patients or caregivers of children hospitalized at three major obstetrics-gynecology and pediatric hospitals in Vietnam. We purposely selected hospitals that represent three geographical regions, including one hospital in Red River Delta Region, one hospital in Northern Midland and Mountainous Region and one hospital from North Central Coast Region. All hospitals are specialized in woman and children health with general details were described in Table 1. The inclusion criteria for selecting hospitals to represent the study were as follows: 1) The hospital must be a provincial institution, ensuring that it serves a diverse population within the region; 2) The hospital must hold a Class 1 designation in Vietnam, which indicates that it meets the highest standards of healthcare service provision in the country; 3) The hospital must have a capacity of at least 500 beds, demonstrating its ability to accommodate a significant number of patients; and 4) The hospital administration must express willingness to participate in the study, ensuring cooperation and support throughout the research process. By adhering to these criteria, we aimed to select hospitals that not only provide high-quality care but also adequately represent the diverse range of healthcare settings and patient experiences within Vietnam’s obstetrics-gynecology and pediatric care system.
 |
Table 1 General Characteristics of Participated Hospitals |
Participants and Sampling
Eligible participants for this study were patients or caregivers of children admitted to the participating hospitals, aged 18 years or older, and willing to partake in the research. The sampling methodology adhered to the survey technique proposed by Hair et al,21 which recommends a minimum of five samples per observed variable to facilitate the performance of exploratory factor analysis. Given that our investigation consisted of 31 items to measure patient satisfaction, we calculated a minimum sample size of 450.
To recruit participants, we employed a convenience sampling approach. Our recruitment process was conducted without quotas or competition between institutions; instead, an invitation to participate in the study was extended to all subjects who met the eligibility requirements. The duration of the data collection was one week. A sampling frame was provided by the research hospital based on the list of hospitalized patients before data collection was carried out. A total of 647 eligible patients were enrolled in the study. These patients were approached by well-trained staff during their hospitalization and invited to participate in the research. To ensure privacy and minimize potential bias, interviews were conducted in private settings, and the interviewers were not staff members of the participating hospitals. Those who agreed to participate were asked to provide informed consent and complete a questionnaire that had previously been piloted to refine language adaptability and ensure the instrument’s appropriateness for the target population.
Study Variables and Instruments
Demographic Characteristics
Data pertaining to the demographic characteristics of the participating caregivers were collected in the study. These characteristics included gender, age, education level, ethnicity, employment status, and monthly income. Age was classified into distinct categories, such as young, middle-aged, and elderly individuals. Monthly income was categorized according to the base salary structure issued by Vietnam Government in 2009 (~60 USD).22
Hospitalization Information
Information concerning the duration of hospital stays, health insurance status, and the number of hospitalizations at the respective facilities for each participant was extracted from their medical records.
Satisfaction with Healthcare Services Measurement
We utilized a patient satisfaction instrument, developed and approved by the Ministry of Health in 2016,23 to assess the various aspects of patient satisfaction in the study. The instrument comprises 31 items that evaluate five key dimensions of perceived satisfaction among hospitalized patients: (i) Accessibility, (ii) Transparency of information and procedures for medical examination and treatment, (iii) Availability and quality of facilities and equipment, (iv) Attitude and professional competence of medical staff, and (v) Service delivery outcomes. A 5-point Likert scale was employed for response options, with 1 representing complete dissatisfaction and 5 denoting complete satisfaction. Domain scores were calculated by averaging the scores of all items within each domain. Higher satisfaction scores indicated greater levels of patient satisfaction with healthcare and treatment services. In addition to the domain-specific assessments, we incorporated two global rating questions to evaluate overall satisfaction with health services (5-point Likert scale) and the extent to which patients’ expectations were met (Visual Analog scale 0–100 points).
Data Analysis
Data were analyzed by STATA version 17.0 (Stata Corp. LP, College Station, USA). We employed Exploratory Factor Analysis (EFA) to examine the construct validity of the satisfaction measurement instrument. Principal Component Analysis (PCA) was utilized to extract components with eigenvalues of 1.4 or higher, which served as the threshold determined by the scree test, marking the point where the eigenvalue curve flattened out. To enhance the interpretability of these factors, the items of the instrument were reclassified using orthogonal Varimax rotation with Kaiser normalization. A threshold of 0.50 was set for factor loadings to be considered significant.
Cronbach’s alpha was employed to assess the internal consistency reliability of the instrument’s domains. To identify the components associated with overall satisfaction, we conducted a multivariable linear regression analysis. A stepwise forward model construction approach was applied, wherein variables were selected based on a log-likelihood ratio test with a p-value of 0.1 or lower, and variables were removed if their p-value exceeded 0.2.24 A p-value of less than 0.05 was deemed statistically significant for the analysis.
Ethical Consideration
This study received approval from the Institutional Review Board and the Principal of the National Economics University (Number No.59/QD-DHKTQD). All patients or caregivers participating in the study provided informed consent, acknowledging their voluntary involvement. This is an observation study, thus did not interfere with the standard care and treatment provided by the participating hospitals, and there were no potential harm posed to the patients, caregivers, or healthcare staff involved. Upon completion of the study, we communicated our findings and recommendations to the leadership of the participating hospitals and their respective provincial health departments for their consideration and possible implementation.
Results
Of the 643 patients and caregivers included in the final analysis, 520 were female (80.87%). Almost half of the participants were aged between 18–29 years old (43.7%), followed by those aged 30–39 years old (33.13%). A majority of participants had completed high school (69.67%), and among them, 22.08% held a college diploma, bachelor’s degree, or higher. Over 90% of the study sample identified as Kinh people. Most participants were employed, with only 2.18% reporting unemployment. Approximately 78.07% of patients were discharged within seven days of hospitalization. Most patients had health insurance, with a coverage rate of over 80% for nearly half of the sample (45.72%). Patients with a monthly income between $165 and $300 accounted for the highest proportion (45.1%), followed by those earning between $300 and $600 (16.95%), and $100 and $165 (12.44%) (Table 2).
 |
Table 2 Demographic Characteristics of Participated Patients |
Table 3 presents satisfaction scores (Mean ± SD) and the percentage of completely satisfaction (5-points scored) for each satisfaction items of the scale. The highest-rated categories included flat, easy-to-walk corridors (4.66 ± 0.49, 66.66%), blocks, stairs, and rooms easy to find (4.63 ± 0.54, 65.79%), Quality drug dispensing and instructions (4.62 ± 0.56, 64.7%), and Access to medical staff when needed (4.62 ± 0.56, 65.32%). And the lowest-rated categories include quality canteen services (4.03 ± 1.07, 40.59%), privacy during hospital stay (4.15 ± 0.95, 43.55%), and hot and cold drinking water (4.16 ± 1.02, 46.66%). The percentage of participants completely satisfied with overall service quality and expectation met was 48.52% and 34.53%, respectively.
 |
Table 3 Profile of Patient’s Satisfaction Items |
Table 4 displays the construct validity and reliability of the satisfaction measurement. Factor analysis revealed three dimensions accounting for 61.73% of the variance: “Competency and Outcomes”, “Accessibility and Procedures”, and “Facilities and Equipment”. The first factor accounted for 51.17% of the variance. Cronbach’s alpha across domains ranged from good to excellent (0.92–0.96). The average domain score varied across the three domains, with the highest score in “Competency and Outcomes” (4.6 ± 0.43) and the lowest in “Accessibility and Procedures” (4.28 ± 0.67). Convergent validity of satisfaction dimensions correlated well with “general satisfaction with health services” and fairly with “general % expectation met” (Figure 1).
 |
Table 4 Exploratory Factor Analysis of Patient’s Satisfaction Scores |
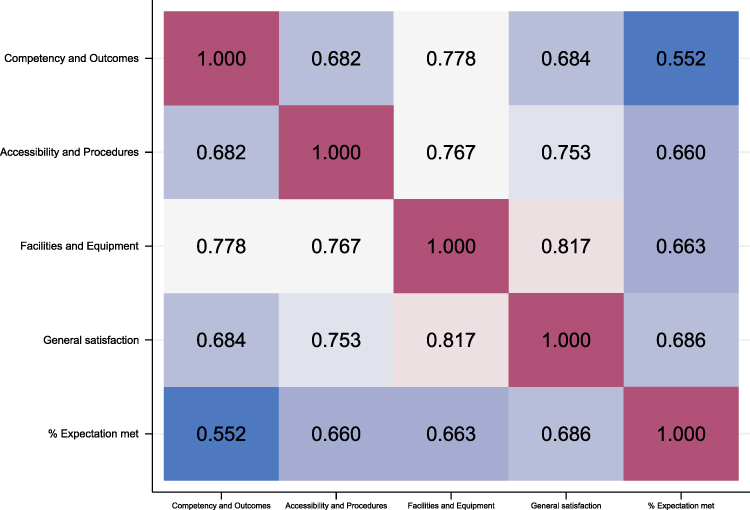 |
Figure 1 Correlation of satisfaction domains and general satisfaction scale. |
Table 5 presents the associations between patient characteristics and satisfaction across different dimensions. In linear regression, the geographic location of hospitals was significantly associated with all satisfaction domains, as well as general satisfaction and expectation met (p<0.05). Patients from hospitals in the Northern Midland and Mountainous and Red River Delta regions were more likely to have higher satisfaction scores compared to patients from the North Central Coast Region. At the individual level, patients with a greater percentage of health insurance coverage were also more satisfied. Certain individual characteristics were associated with lower satisfaction, including higher education levels, higher economic status, and minority ethnic backgrounds.
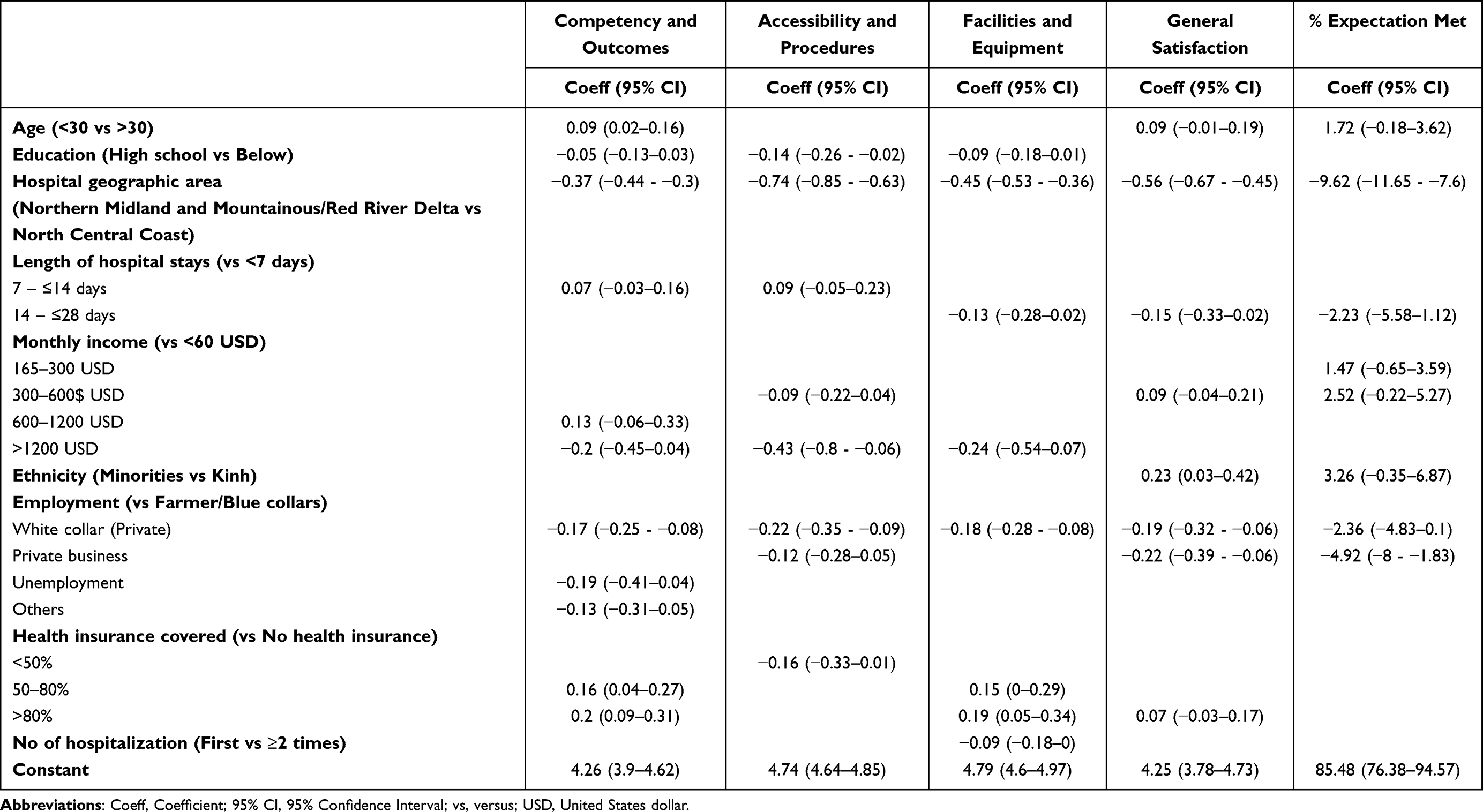 |
Table 5 Factors Associated with Satisfaction Among Participated Patients |
Discussion
In this study, we documented a moderate to high degree of patient satisfaction with inpatient healthcare services at three prominent obstetrics-gynecology and pediatric hospitals in northern Vietnam. Utilizing a standardized scale approved by the Ministry of Health, we observed that complete satisfaction across the 31 measured items ranged from 40.59% to 66.56% (employing a 5-level Likert scale). The overall satisfaction score was 4.44 ± 0.62, with a general satisfaction prevalence of 48.52%. This figure is slightly higher than those reported in recent analogous studies conducted in the country, which focused on inpatient care,25–27 but considerably lower than those concerning outpatient settings.28 The disparities in results between these studies may be attributed to the utilization of different measurement scales, the examination of distinct hospital departments, or variations in the levels of sampled hospitals. Studies conducted in several developing countries have reported that patient satisfaction levels in obstetrics-gynecology and pediatric departments are marginally higher than in other departments.29,30 Some hypotheses suggest that the intimate nature of obstetrics and gynecology treatment, as well as the pivotal role healthcare workers play during the most memorable periods of women’s and children’s lives, such as pregnancy, childbirth, and child care, contribute to deeper and more personal relationships between patients, caregivers, and medical professionals.29,31 However, these assertions have not been substantiated by experimental research, and larger-scale studies or qualitative assessments may provide additional insight. Comparing outpatient and inpatient services, evidence from middle-income countries in Asia indicates that patient satisfaction is generally higher in outpatient settings relative to inpatient services.32,33 Further research is necessary to elucidate the underlying reasons for these differences and to identify areas for improvement in both outpatient and inpatient healthcare services.
In Vietnam, the Ministry of Health has mandated the routine monitoring of both patient and healthcare worker satisfaction as a means of quality control improvement since 2016. Numerous studies have developed and validated their own scales for measuring patient satisfaction in various settings within Vietnam, encompassing primary healthcare,25,28 HIV/AIDS,34 and ophthalmology.27 However, for the purpose of informing policymaking at the national level, it is crucial to have a universal instrument that facilitates comparison between diverse facilities and patient groups. In our study, the instrument provided by the Ministry of Health demonstrated robust convergent validity and reliability in measuring patient satisfaction within the realms of obstetrics-gynecology and pediatric care and treatment (Cronbach’s alpha ranged from 0.93 to 0.96 across the three domains). This finding suggests that the instrument may be effectively employed on a larger scale, although additional research is required to assess the validity of this tool among patients in other disease groups or geographic regions. Furthermore, it is essential to ensure that the instrument is subject to regular updates based on empirical evidence and analysis derived from national surveillance results originating from participating hospitals. Such a dynamic approach will help maintain the instrument’s relevance and applicability, ultimately contributing to the development of evidence-based policies that facilitate improvements in healthcare quality and patient satisfaction.
In our study, the mean scores of the three domains reconstructed from the EFA were highest for “Competency and Outcomes”, followed by “Facilities and Equipment”, and lowest for “Accessibility and Procedures”. These findings are consistent with other similar studies that identified the lack of convenience in administrative procedures as the primary source of dissatisfaction among both in- and out-patients.25,35 The majority of hospitals in Vietnam continue to rely on paper-based systems for most activities, including registration, medical and laboratory records, as well as financial and payment processes. Recent reports indicate a dearth of research evidence and effective solutions for the widespread implementation of digital health in the country,36 despite acknowledgment from policymakers. While the transition to health information systems is occurring rapidly, significant disparities exist between different hospital levels and local provinces, which can considerably impact patient satisfaction. Although Vietnam is progressively transitioning to a model of financial autonomy for public hospitals, where each facility is responsible for its own operations, strong leadership and governance are still required to ensure equity in healthcare. The linear regression analysis revealed that the level of health insurance covering healthcare costs was associated with patient satisfaction. This finding suggests that reducing patients’ financial concerns regarding their treatments and enhancing their overall impressions of medical personnel are key factors in improving satisfaction. This conclusion aligns with other reports in Vietnam that found a positive impact of insurance coverage on patient satisfaction.26,37
The findings suggest that there are associations between patient characteristics and their satisfaction levels with hospital services across different domains. One significant finding is that the geographical location of hospitals affects patient satisfaction. Patients from hospitals in the Northern Midland, Mountainous, and Red River Delta regions are more likely to be satisfied compared to those from the North Central Coast Region. This may be due to differences in healthcare quality, accessibility, or inequity in health across regions.38 Addition to that, we found certain individual characteristics such as higher education levels, higher economic status, and minority ethnic backgrounds were associated with lower satisfaction, that in-line with several studies has been conducted in the country.26,28,37
Since 1992, Vietnam’s social health insurance scheme has undergone significant evolution to expand its coverage and scope. Initially targeting low-income individuals and employees in the formal sector, the program has gradually extended its reach to include a wider range of demographics. As of May 2019, the social health insurance covered an impressive 89% of Vietnam’s population, equivalent to 84 million people.37 Despite the high proportion of insured patients, our study’s findings suggest that the extent of treatment cost coverage may not be entirely satisfactory for patients. This highlights the need for a more comprehensive and detailed healthcare payment system to address these concerns. Vietnam’s ongoing transition to a mixed market economy and the adoption of fee-for-service medicine in public hospitals present both opportunities and challenges for the nation’s healthcare system. In this context, it is essential to consider the potential consequences of these changes on patient satisfaction, particularly in relation to the financial burden of healthcare.
In this study, our strength is to have multicentre sites of major obstetrics-gynecology and pediatric hospitals that represents for different geographic area of Northern and North Middle of Vietnam. However, several limitations that should be acknowledge. Firstly, the cross-sectional design employed in this research may hinder the ability to establish causal relationships. Furthermore, the random selection of patients at hospitals implies that the sample may not be representative of the broader population of obstetrics-gynecology and pediatric patients, thereby constraining the capacity to generalize the study’s findings.
Conclusion
Our study revealed that patients admitted to three major obstetrics-gynecology and pediatric hospitals in the northern region of Vietnam experienced moderate to high levels of satisfaction with healthcare services. Although general satisfaction and fulfillment of outcome expectations were satisfactory, several service aspects warrant improvement at both the policymaking and individual hospital levels. These aspects include the convenience of administrative procedures, the health insurance payment system, and the availability of services provided. These findings may offer valuable evidence to support the widespread implementation of hospital quality control measures in Vietnam, with an emphasis on patient-centered objectives. By addressing these areas of concern, healthcare stakeholders can work towards enhancing the overall patient experience and fostering a more efficient and responsive healthcare system.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to restrictions, for example, their containing information that could compromise the privacy of research participants.
Ethics Approval and Informed Consent
We comply with the Declaration of Helsinki. The study was approved by the Institutional Review Board and the Principal of the National Economics University (Number No.59/QD-DHKTQD), and all participants were provided informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors did not receive any financial support for the survey work or for publication of the article.
Disclosure
The authors reports no conflicts of interest in this work.
References
1. Aiken LH, Sermeus W, Van den Heede K, et al. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344:e1717. doi:10.1136/bmj.e1717
2. Lin BY, Lin CC, Lin YK. Patient satisfaction evaluations in different clinic care models: care stratification under a national demonstration project. Health Place. 2010;16(1):85–92. doi:10.1016/j.healthplace.2009.08.008
3. Prakash B. Patient satisfaction. J Cutan Aesthet Surg. 2010;3(3):151–155. doi:10.4103/0974-2077.74491
4. Jenkinson C, Coulter A, Bruster S, Richards N, Chandola T. Patients’ experiences and satisfaction with health care: results of a questionnaire study of specific aspects of care. Qual Saf Health Care. 2002;11(4):335–339. doi:10.1136/qhc.11.4.335
5. Al-Abri R, Al-Balushi A. Patient satisfaction survey as a tool towards quality improvement. Oman Med J. 2014;29(1):3–7. doi:10.5001/omj.2014.02
6. Karaca A, Durna Z. Patient satisfaction with the quality of nursing care. Nurs Open. 2019;6(2):535–545. doi:10.1002/nop2.237
7. Das J. The quality of medical care in low-income countries: from providers to markets. PLoS Med. 2011;8(4):e1000432. doi:10.1371/journal.pmed.1000432
8. Kim JH, Bell GA, Ratcliffe HL, et al. Predictors of patient-reported quality of care in low- and middle-income countries: a four-country survey of person-centered care. Int J Qual Health Care. 2021;33(3). doi:10.1093/intqhc/mzab110
9. Shirley ED, Sanders JO. Patient satisfaction: implications and predictors of success. J Bone Joint Surg Am. 2013;95(10):e69. doi:10.2106/jbjs.L.01048
10. Wartman SA, Morlock LL, Malitz FE, Palm EA. Patient understanding and satisfaction as predictors of compliance. Med Care. 1983;21(9):886–891. doi:10.1097/00005650-198309000-00005
11. Marquis MS, Davies AR, Ware JE Jr. Patient satisfaction and change in medical care provider: a longitudinal study. Med Care. 1983;21(8):821–829. doi:10.1097/00005650-198308000-00006
12. Batbaatar E, Dorjdagva J, Luvsannyam A, Savino MM, Amenta P. Determinants of patient satisfaction: a systematic review. Perspect Public Health. 2017;137(2):89–101. doi:10.1177/1757913916634136
13. Saultz JW, Albedaiwi W. Interpersonal continuity of care and patient satisfaction: a critical review. Ann Fam Med. 2004;2(5):445–451. doi:10.1370/afm.91
14. The National Assembly. Law on Medical Examination and Treatment. No 15/2023/QH15. Hanoi, Vietnam: The National Assembly; 2023.
15. Montegut AJ, Cartwright CA, Schirmer JM, Cummings S. An international consultation: the development of family medicine in Vietnam. Fam Med. 2004;36(5):352–356.
16. Dang TH, Nguyen TA, Hoang Van M, Santin O, Tran OMT, Schofield P. Patient-centered care: transforming the health care system in Vietnam with support of digital health technology. J Med Internet Res. 2021;23(6):e24601. doi:10.2196/24601
17. Takashima K, Wada K, Tra TT, Smith DR. A review of Vietnam’s healthcare reform through the direction of healthcare activities (Doha). Environ Health Prev Med. 2017;22(1):74. doi:10.1186/s12199-017-0682-z
18. Ministry of Health. Circular No 6858/QĐ-BYT on Approval of the National Hospital Quality Standards; 2016.
19. UNICEF. Viet Nam Sustainable Development Goal Indicators on Children and Women (SDGCW) Survey 2020-2021. UNICEF; 2022.
20. Nguyen TT, Trevisan M. Vietnam a country in transition: health challenges. BMJ Nutrition. 2020;69. doi:10.1136/bmjnph-2020-000069
21. Hair JFA. Multivariate Data Analysis with Readings. Macmillan Publishing Company; 1995.
22. The National Assembly. Resolution No. 86/2019/QH14 on State budget estimates in 2020; 2020.
23. Ministry of Health. Decision 4939/QD-BYT 2016 on Measuring patient’s satisfaction with public health services; 2016.
24. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. John Wiley & Sons; 2013.
25. Thach Phuong N, Vu Hoang P, Mac Dang T, Nguyen Thi Huyen T, Ngo Thi T. Improving hospital’s quality of service in Vietnam: the patient satisfaction evaluation in multiple health facilities. Hosp Top. 2021;1–11. doi:10.1080/00185868.2021.1969871
26. Nguyen T, Nguyen H, Dang A. Determinants of patient satisfaction: lessons from large-scale inpatient interviews in Vietnam. PLoS One. 2020;15(9):e0239306. doi:10.1371/journal.pone.0239306
27. Van Huy N, Dung NN, Thang CD, Hanh LT. Patient satisfaction with health care services at a national institute of ophthalmology. Int J Health Plann Manage. 2018;33(1):e251–e262. doi:10.1002/hpm.2449
28. Quyen BTT, Ha NT, Van Minh H. Outpatient satisfaction with primary health care services in Vietnam: multilevel analysis results from the Vietnam health facilities assessment 2015. Health Psychol Open. 2021;8(1):20551029211015117. doi:10.1177/20551029211015117
29. Patel I, Chang J, Srivastava J, Feldman S, Levender M, Balkrishnan R. Patient satisfaction with obstetricians and gynecologists compared with other specialties: analysis of US self-reported survey data. Patient Relat Outcome Meas. 2011;2:21–26. doi:10.2147/prom.S15747
30. Aga TB, Ferede YM, Mekonen EG. Satisfaction and associated factors towards inpatient health care services among adult patients at Pawie General Hospital, West Ethiopia. PLoS One. 2021;16(4):e0249168. doi:10.1371/journal.pone.0249168
31. Uhas AA, Camacho FT, Feldman SR, Balkrishnan R. The relationship between physician friendliness and caring, and patient satisfaction: findings from an internet-based survey. Patient. 2008;1(2):91–96. doi:10.2165/01312067-200801020-00004
32. Lv Y, Xue C, Ge Y, et al. Analysis of factors influencing inpatient and outpatient satisfaction with the Chinese Military Health Service. PLoS One. 2016;11(3):e0151234. doi:10.1371/journal.pone.0151234
33. Kaur M, Bashar A, Singh T, Kumar R. Cross-sectional study of clients’ satisfaction with outpatient and inpatient services of public health facilities of a North Indian State. Health Serv Insights. 2020;13:1178632920929969. doi:10.1177/1178632920929969
34. Tran BX, Nguyen NPT. Patient Satisfaction with HIV/AIDS Care and Treatment in the decentralization of services delivery in Vietnam. PLoS One. 2012;7(10):e46680. doi:10.1371/journal.pone.0046680
35. Tran BX, Dang AK, Vu GT, et al. Patient satisfaction with HIV services in Vietnam: status, service models and association with treatment outcome. PLoS One. 2019;14(11):e0223723. doi:10.1371/journal.pone.0223723
36. Tran DM, Thwaites CL, Van Nuil JI, McKnight J, Luu AP, Paton C. Digital health policy and programs for hospital care in Vietnam: scoping review. J Med Internet Res. 2022;24(2):e32392. doi:10.2196/32392
37. Vuong Q-H. Sociodemographic factors influencing Vietnamese patient satisfaction with healthcare services and some meaningful empirical thresholds. Iran J Public Health. 2018;47(1):119–126.
38. Målqvist M, Hoa DT, Liem NT, Thorson A, Thomsen S. Ethnic minority health in Vietnam: a review exposing horizontal inequity. Glob Health Action. 2013;6:1–19. doi:10.3402/gha.v6i0.19803
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.