Back to Journals » Clinical Optometry » Volume 15
Real-Time Ocular Comfort Reporting in Monthly Replacement Contact Lens Wearers
Authors Call T ![]() , Pucker AD, McGwin Jr G, Franklin QX, Logan A
, Pucker AD, McGwin Jr G, Franklin QX, Logan A
Received 18 January 2023
Accepted for publication 29 April 2023
Published 5 May 2023 Volume 2023:15 Pages 97—103
DOI https://doi.org/10.2147/OPTO.S403319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Mr Simon Berry
Terri Call,1,* Andrew D Pucker,1,* Gerald McGwin Jr,2 Quentin X Franklin,1 Amy Logan1
1Department of Optometry and Vision Science, University of Alabama at Birmingham, Birmingham, AL, USA; 2Department of Epidemiology, University of Alabama at Birmingham, Birmingham, AL, USA
*These authors contributed equally to this work
Correspondence: Andrew D Pucker, University of Alabama at Birmingham, School of Optometry, 1716 University Blvd, Birmingham, AL, 35233, USA, Tel +1 920 579-2900, Email [email protected]
Purpose: To map contact lens (CL) comfort over the full wear day and across 1 month’s wear in established, asymptomatic to minimally symptomatic, reusable, soft CL wearers.
Methods: Adult, 18- to 45-year-old, participants were recruited and required to have 20/20 best-corrected visual acuity or better and must have been asymptomatic to minimally symptomatic CL wearers. Participants were required to be able to wear TOTAL30® sphere CLs and have minimal astigmatism. Participants were fit in the study CLs and asked to wear these CLs daily for the next month for 16 hours per day each day. Participants were asked to complete a visual analog scale (VAS) survey via text message at time of CL application and after 8, 10, 12, 14, and 16 hours of wear and at CL removal on days 1, 2, 3, 4, and 5 and at 2 weeks and 1 month. The utilized VAS had a ± 50 scale with positive scores being comfortable, negative scores being uncomfortable, and scores of 0 being neutral comfort.
Results: Forty-eight participants were recruited who had a mean ± SD age of 26.2 ± 5.2 years (71% female). Mean initial VAS CL comfort scores at initial CL dispense were 45.56 ± 9.20 units. Mean CL wear times for any of the days evaluated were at least 14.80 ± 2.41 hours per day and did not differ across the study (p = 0.77). Mean comfort VAS scores significantly decreased over the wear day (all days p ≤ 0.02), yet there were no significant differences in VAS comfort scores across the same time of day for the duration of the study (all times p ≥ 0.06).
Conclusion: This study determined that while CL wearers were slightly less comfortable at the end of the day compared to application, this comfort change was minimal given that the average participants had overwhelmingly good comfort at all time-points evaluated. Comfort scores were likewise consistent across 1 month of wear.
Keywords: comfort, contact lenses, monthly, reusable, text message, visual analog scale
Introduction
Contact lens (CL) discomfort affects millions of patients with discomfort consistently being the top reason why established CL wearers cease wearing CLs.1,2 In fact, studies have consistently found that the frequency of CL dropout is around 20% with this dropout frequency staying relatively stable since the advent of frequent replacement CLs.1,3–5 This static frequency of CL dropout is surprising given that there have been several dramatic soft CL innovations, which include widely available daily disposable CLs, silicone hydrogel CL materials with high oxygen transmissibility, advanced CL surface technologies, and expanded CL parameters.1
The literature specifically indicates that CL discomfort symptoms frequently increase towards the end of the CL wear day.6–8 Indeed, Woods et al found that in symptomatic CL wearers, CL comfort declines significantly over 8 hours of wear regardless of the CL material.7 This decreased end-of-day comfort could be caused by factors such as CL dehydration, tear film deposition, decreased CL wettability, and tear osmolarity changes throughout the CL wear day.6 The literature also suggests that wearers who are about to drop out of CLs are significantly more likely to wear their CLs for fewer days per week than comfortable CL wearers, again likely because of poor comfort, with Pucker et al determining that recent CL dropouts were only wearing their CLs 6 or more days per week 24% of the time.9
While comfortable CL wear times vary from patient to patient, Terry et al has suggested that patients should be able to comfortably wear their CLs for at least 12 hours per day for at least 6 days per week.10 Nevertheless, the literature currently lacks sufficient data to comment fully on the full day wear experience, which for many patients may be 16 or more hours per day, especially if they have demanding careers. The literature likewise lacks guidance on how CL comfort changes across the first month of wearing a reusable CL. One CL that has the potential to allow for all-day comfort is the TOTAL30® sphere CL (Alcon, Fort Worth, TX, USA), which is a new water gradient, monthly replacement CL aimed at delivering all-day comfort and visual performance. The purpose of this study was therefore to map CL comfort over the full wear day in established, asymptomatic, soft CL wearers who were refit into the study CLs. These data are not only important for providing some of the first insights into the full day CL wearing experience over 1 month with the study lens during the initial adaption period to the CLs, but they will likewise help the community understand how the study CLs perform in near real-time during the initial adaptation period.
Materials and Methods
Participants
This 1-month, 3-visit study was conducted at the University of Alabama at Birmingham (Birmingham, AL, USA). This work was registered with ClinicalTrials.gov (NCT05183022), and it was approved by the University of Alabama at Birmingham’s Institutional Review Board for Human Use (IRB-300008004). This study followed the Declaration of Helsinki. Participants were recruited via clinic records, email, and fliers, and were screened prior to the study visit with an Institutional Review Board approved phone screening survey. Inclusion criteria were designed to recruit the typical non-presbyopic CL wearer. Adult, 18- to 45-year-old, male or female CL wearers who had 20/20 visual acuity or better in their habitual spectacle correction and who were asymptomatic to minimally symptomatic CL wearers were recruited. CL comfort was confirmed by having participants be required to have Contact Lens Dry Eye Questionnaire (CLDEQ)-8 scores ≤10 units.9,11 While participants were aware that the CLDEQ-8 was being used as a study entry criterion, they were masked to the magnitude and direction of the score needed to be able to participate in the study. Furthermore, the current study used a more conservative cutoff score than the published value for the CLDEQ-8 (scores ≥12 suggest a needed change) to help ensure that the included participants were truly minimally symptomatic CL wearers. Participants were required to be able to wear the study CLs, and they were required to have a smartphone with text messaging capabilities to be able to answer electronic survey questions. Participants were required to have astigmatism better than or equal to −0.50 D in each eye and be a current CL wearer who had consistently worn biweekly or monthly CLs within the past 6 months. Participants were required to provide a glasses prescription that was less than 3 years old. Participants were required to be willing to start wearing their CLs between 6:00 AM and 8:00 AM each day. This requirement was set to help standardize text message deployment. Participants were excluded if they were current or past hard CL wearers, had known systemic health conditions that are thought to alter tear film physiology, had a history of viral eye disease, had a history of ocular surgery, had a history of severe ocular trauma, had active ocular infection or inflammation, were currently using isotretinoin-derivatives or ocular medications, were currently using rewetting drops or artificial tears, or if they were pregnant or breastfeeding.12
Surveys and Clinical Tests
Participants were asked to bring their spectacles to the first study visit and to adhere to the inclusion and exclusion factors described above. The first visit commenced with reviewing the Institutional Review Board approved screening survey to ensure that they still qualified for the study. The participants then completed the CLDEQ-8 questionnaire while considering their habitual CL wear over the past 2 weeks even though they wore their spectacles to the baseline visit. Scores were then tallied in office to confirm that the participant was a minimally symptomatic CL wearer. Spectacle prescriptions were reviewed to verify that they were eligible for the spherical study CLs. Non-eligible participants were dismissed at this time. Participants who met all study criteria were enrolled following the informed consent process.
Participant demographics were collected (age, sex, race, ethnicity). Visual acuity was obtained while participants wore their habitual spectacles and recorded in logarithm of the minimum angle of resolution (logMAR). Manifest refraction was measured with a phoropter, including a binocular balance with dissociation. Best-corrected visual acuity was determined through the phoropter with a Snellen chart and recorded in logMAR equivalent. Slit-lamp biomicroscopy was performed to rule out any pathology that might prohibit CL wear.
Participants were fit in the study CLs with prescriptions directly determined from the spherical equivalent power found during manifest refraction. CLs were evaluated for centration, movement, and coverage. CL power adjustments were determined with loose lenses and were made if Snellen visual acuity improved by one or more lines. Participants were educated to wear their CLs every day while on study. Participants were given a 1-month supply of CLEAR CARE® CL solution (Alcon, Fort Worth, TX, USA) and were educated on its use along with how to use the study CLs. A test text message was sent after CL application to confirm digital receipt. All text messages were sent via Qualtrics (Qualtrics; Provo, UT). This first text message was completed during the CL settling period and before CL evaluation. This first text message was a visual analog scale (VAS) survey aimed at determining initial CL comfort directly after CL application. The investigators used this opportunity to educate the participants about the text message system and the frequency of text messages to be sent during the study. The participants were specifically educated that the VAS had a ±50 scale with +50 being maximum comfort, −50 being worst comfort, and 0 being neutral comfort. Participants were asked to complete VAS surveys via text message at CL application and after 8, 10, 12, 14, and 16 hours (comfort directly before CL removal) of wear and directly after CL removal on days 1 through 5 and at 2 weeks and 1 month of CL wear. Qualtrics was pre-programmed to deploy individual text messages to participants at each given time-point analyzed. Text messages were named by day and time. Participants were educated to answer each message in real-time on schedule, and they were monetarily incentivized to complete at least 90% of the text messages. Data were evaluated based upon the deployment time, and participants were educated to report their ratings based upon the deployment schedule. Since some variability in CL application and removal times were expected among the participants, they were required to self-report their CL application and removal times; these data were used to calculate CL wear times. Qualtrics was monitored to help ensure proper text message deployment, and reeducation was performed if text messages were missed. Uncompleted text messages were treated as missing data in the statistical analysis. Participants were notified at the end of 5 days that there would be a break in text messages. Participants were sent email reminders before the 2-week and 1-month messages to help improve compliance with these specific visits because the participants were only required to provide text message data daily during the first 5 days of wear. Qualtrics data were saved in Qualtrics, exported as an Excel file, and analyzed as described below.
When participants returned for their 1-week visit, they completed visual acuity, slit-lamp biomicroscopy, and the CLs were evaluated as described above for visual acuity and fit and adjusted in power if it enhanced visual acuity. CL power changes were only made if they improved visual acuity by one or more lines. When participants returned for their 1-month visit, the same testing as the 1-week visit was completed. The participants were then released from the study.
Sample Size and Statistical Analysis
This study aimed to understand CL comfort throughout the day in monthly soft CL wearers. It was estimated that 40 participants were needed to gain a general understanding of ocular comfort across the entire day based upon past research.13–15 An additional 8 participants were recruited to account for missing text message data. All data were analyzed with SAS Version 9.4 (SAS; Cary, NC, USA). Clinical data were collected via Research Electronic Data Capture (REDCap; Vanderbilt University Medical Center, Nashville, TN, USA).16,17 Participants survey data were collected via Qualtrics. Means and standard deviations (SD) were presented to understand trends. Repeated measures ANOVA was used to compare comfort within and across the CL wear day.
Results
A total of 48 participants were recruited with all of them completing the study. The participants had a mean ± SD age of 26.2 ± 5.2 years (71% female). The sample was 65% White, 10% Black or African American, 23% Asian, and 2% more than one race. A total of 4% of these participants identified as Hispanic. Manifest refraction sphere and cylinder at the initial visit was −3.42 ± 2.43 D and 0.00 ± 0.40 D for the right eye and −3.44 ± 2.55 D and −0.04 ± 0.29 for the left eye, respectively. The mean CL power for the right eye was −3.32 ± 2.26 D, while the mean CL power for the left eye was −3.28 ± 2.37 D. Two participants lost or damaged their CLs before the 1-week visit. These participants underwent a short washout period, and they restarted the full-text message schedule with a new pair of CLs. One participant had a CL power change at the 1-week visit; this participant proceeded on schedule. Snellen visual acuity converted to a logMAR scale with the study CLs after power adjustments at the initial fitting was −0.01 ± 0.06 for the right eye and −0.01 ± 0.05 for the left. At the 1-week visit, Snellen visual acuity converted to logMAR while wearing CLs was −0.03 ± 0.10 for the right eye and −0.02 ± 0.07 for the left eye. At the 1-month visit, Snellen visual acuity converted to logMAR while wearing CLs was −0.03 ± 0.06 for the right eye and −0.03 ± 0.06 for the left eye. No adverse events were detected by slit-lamp biomicroscopy in any participant, and no adverse events were reported by the participants during the study.
A primary goal of this study was to understand CL comfort across the CL wear day and across the first month of CL wear. A total of 70.8% of the participants completed 80% or more of the text message questions probed in Table 1. Mean CL wear times at 1 day, 2 days, 3 days, 4 days, 5 days, 2 weeks, and 1 month were 15.72 ± 1.31, 15.46 ± 0.98, 15.31 ± 1.27, 14.80 ± 2.41, 15.47 ± 1.32, 15.55 ± 1.44, and 15.33 ± 2.18 hours per day (p = 0.77), respectively. The mean initial VAS CL comfort at first application of the study CLs was 45.56 ± 9.20 units.
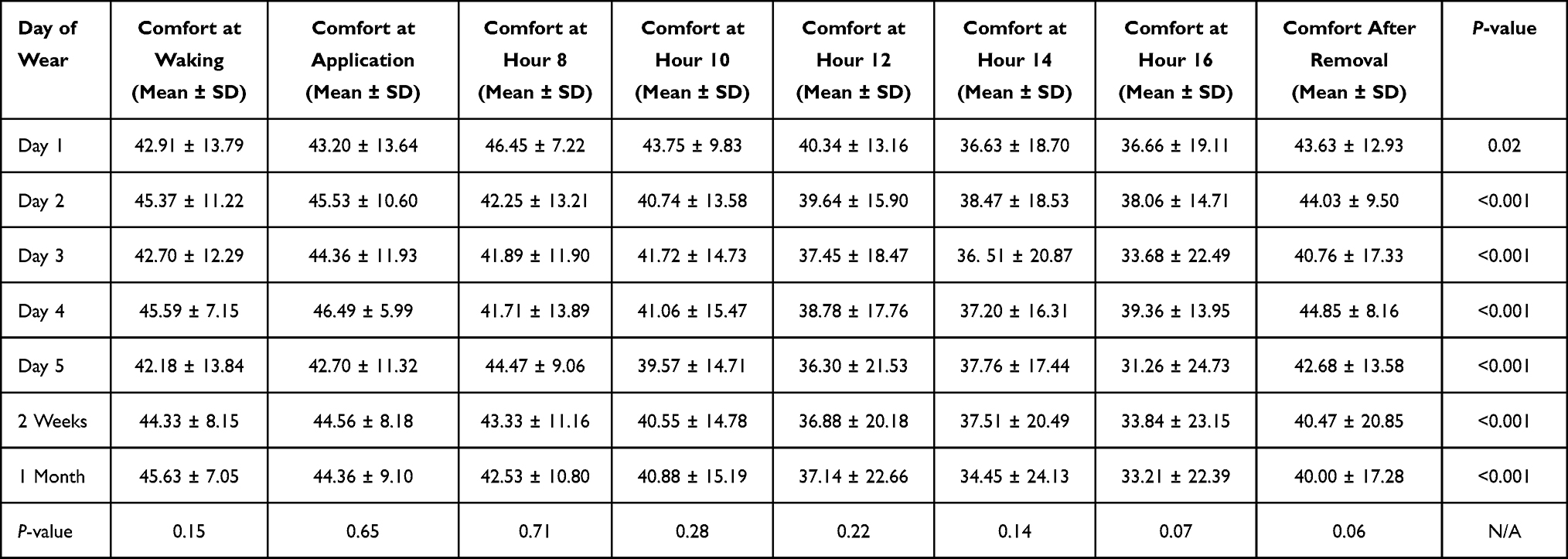 |
Table 1 Eye Comfort Visual Analog Scale (VAS) Scores of Study Participants |
This study found that the participants reported excellent subjective comfort across this 1-month study (Table 1). When evaluating CL comfort across the same time of day (application, 8-hours, 10-hours, 12-hours, 14-hours, 16-hours, or CL removal) across the wear month, there were no significant changes in comfort at any time-point (all p >0.06); however, when evaluating CL comfort across the same day, CL comfort was significantly worse at the end of the day starting at wear day 2 through the end of the study (all p < 0.001). Nevertheless, the mean end-of-day comfort scores were overwhelmingly comfortable (positive VAS scores), and only 8 out of 48 participants reported discomfort (negative VAS scores) at the 16-hour time point and only 6 out of 48 participants reported discomfort at CL removal at night during the study. Only one participant reported negative VAS scores at every time point measured at the 16-hour and CL removal time points (same participant). The other participants with negative VAS scores presented with no discernable pattern in CL comfort at these time points.
Discussion
The primary goals of this investigation were to understand how the comfort of a monthly CL changed during the CL wear day and across the life of the CL. These goals were accomplished by subjectively evaluating CL comfort in real-time with text message questions that utilized a VAS that clearly delineated between comfortable (positive VAS scores) and uncomfortable (negative VAS scores) CLs. This study determined that while there was slightly worse CL comfort after about 16 hours of CL wear prior to CL removal starting at day 2 through the rest of the life of the CL, this change in comfort was unlikely to be clinically meaningful given that the average participants had overwhelmingly positive comfort scores at all time-points evaluated in the study. This comfort was likewise consistent at each individual time-point across the life of the CL, suggesting that the study CL provides consistently favorable subjective comfort over 1 month.
It is well established that ocular comfort decreases at the end of the day compared to at the beginning of the day in both CL and non-CL wearers, though diurnal variation in comfort tends to be more pronounced in CL wearers than non-CL wearers and participants with symptomatic eyes than non-symptomatic eyes.7,8 Furthermore, this decrease in CL comfort is true irrespective of CL material (silicone hydrogel vs hydrogel; soft CL vs hard CL).7 However, few studies have examined the comfort of CL wear over time periods longer than 1 day or for an average of several days. As monthly CL comprise about 60% of all soft CLs prescribed in the United States,18 data examining comfort over a month’s wear time are valuable and may provide insight into CL comfort at the end-of-life for a monthly CL as opposed to solely end-of-day. In addition, as the primary reason for discontinuation of CL wear in established CL wearers is discomfort, improvements in comfort not only throughout the day but throughout the life of reusable CLs should improve CL wear adherence and allow patients to continue CL wear as desired.
The act of sending text messages to participants to understand patient-reported CL comfort is not a novel methodological approach, yet it is a relatively uncommon method within the field. The sparse use of sending data collection text messages to participants may be because planned deployment of text messages to a diverse group of participants is logistically challenging. In 2010, Santodomingo-Rubido et al was one of the first group of investigators to use text messages to obtain information in the CL comfort arena, with the group aiming to understand ocular comfort differences between CL and non-CL wearers. The authors evaluated ocular comfort with a 0–100 scale in the morning, afternoon, and night, and they determined that silicone hydrogel, hydrogel, hard, and non-CL wearers experienced similar comfort at each time point, but all 4 groups had decreased ocular comfort across the day. More recently, Fogt and Patton have produced a pair of studies that have used text messages to evaluate real-time comfort in daily disposable spherical CL wearers (n = 35) and daily disposable toric CL wearers (n = 30).19,20 Each study evaluated participants after they adapted to the CL. The investigators sent text messages to the participants for 5 weekdays first thing in the morning and then after 10, 12, 14, and 16 hours of CL wear (0–10 scale with integer responses). Both studies found that median CL comfort scores were high across these 5 days during hours 10 through 16 of wear (median score between time periods ranged from 7.4 to 10.0 units); however, CL comfort did decrease between hours 10 and 16 of wear by a small amount. The current study came to a similar conclusion, though the current study reached this conclusion by analyzing seven different timepoints over the life of the monthly replacement CL. The likely difference in analysis approaches between the current study and Fogt and Patton’s studies is that Fogt and Patton evaluated daily disposable CLs while the current study evaluated monthly replacement CLs.
After 1 month of wear, participants in the current study reported a minimal loss in mean VAS comfort at any given time point with participants reporting no significant differences for a specific time of day across the life of the CL (eg, comfort at application on 1 day was not significantly worse at 1 month). Decreases in mean VAS CL comfort scores occurred at all time points measured starting at day 2 through the life of the CL, though this change in comfort is unlikely to be clinically meaningful except for maybe the 14- and 16-hour time points. This limited clinically meaningful difference is highlighted by the scores in Table 1 only decreasing at the 14- and 16-hour time points by 4.42 to 12.42 units for any given time-point. Papas et al’s data suggest that a 6.8 unit change in a 0 to 100 scale is needed for a clinically meaningful difference.21 The limited clinically meaningful difference found in this study is likewise bolstered by mean comfort scores being overwhelmingly within the positive range, which suggests good CL comfort on this study’s novel ±50 VAS. This ±50 VAS, thus, has a clear advantage over the traditional 0–100 VAS because the ±50 VAS clearly differentiates between comfortable and not while the traditional 0–100 VAS is only able to evaluate relative subjective comfort changes.
It is also commonly known that CL wear time is an integral factor in patient CL success with the Tear Film and Ocular Surface Society (TFOS) citing that decreased wear times is a preceding factor for CL dropout.22 Terry et al has suggested that patients should be able to comfortably wear their CLs for a minimum 12 hours per day for 6 days per week to be considered successful CL wearers,10 yet many active patients wish to wear their CLs for 16 or more hours per day. The need for long wear times is highlighted by the two-thirds of US adults who spend 5 or more hours per day on a digital device.23 The current study specifically requested that participants wear their CL for 16 or more hours per day, and on average the included participants roughly met this goal at every time point polled while still having good CL comfort at the end of the day. These data provide evidence that innovative CLs such as the study CL, and likely future iterations, have the potential to help CL adherence and curb CL dropout rates.
While this study had several strengths, which included measuring CL comfort in real-time via text messages, monitoring CL comfort across the whole wear day and across the life of a monthly CL, and using an innovative VAS which can clearly delineate between comfortable and uncomfortable CL wear, this study is not without limitations. A primary study limitation is that only one CL brand and one CL care system were evaluated. This approach was taken to allow for the initial evaluation of real-time comfort of monthly CLs; nevertheless, future investigations that evaluate multiple reusable CLs in parallel are needed. These data could furthermore be supplemented by evaluating how different care systems affect CL comfort within a given CL material. An additional related limitation is that this study was only conducted in participants who were asymptomatic to minimally symptomatic CL wearers who were initially adapting to the study lenses; thus, this study needs to be repeated in symptomatic CL wearers and for a greater duration of time to see how the results may vary. Nonetheless, this report is still important because it shows proof of concept for end-of-day and month-long comfort in the same brand of CLs without presenting the data in aggregate. This study also suffered from having a somewhat low text message response rate among its first 8 participants because of a glitch in the text messaging system that blocked message deployments. Nevertheless, this issue was quickly corrected, and the initial sample size was originally inflated to account for any issues related to poor response compliance. This concern is further mitigated by this study deploying about 2400 texts messages across the life of the study. Comfort difference, or the lack thereof, were furthermore put into context by qualifying if the reported comforts were clinically meaningful or not; thus, even if a significant difference was missed it would be highly unlikely to be clinically meaningful given that most differences in comfort across time were small. Lastly, while participants were requested to wear their CLs for 16 or more hours per day, the mean CL wear times on each study day were slightly less than 16 hours per day. Participants likely wore their CLs for fewer than 16 hours per day because of natural human sleep patterns; nevertheless, the reported mean CL wear times are likely representative a full day’s worth of CL wear.
Conclusions
Historical evidence suggests that CL comfort generally decreases towards the end of the day, yet this study determined that the study CLs provide consistently good comfort throughout the day and across the life of the CL. Nevertheless, there was potentially a clinically meaningful decrease in CL comfort across the wear day during the first month of CL wear when one compares comfort before CL application to comfort at about 14 or 16 hours of wear directly before CL removal. Thus, this study suggests that while there is a slight decrease in CL comfort across the wear day with the study lens, patients can maintain long wear schedules suitable for active lifestyles for the full life of the study CLs. With overall decreased CL discomfort, general CL wear discontinuation should also be decreased, which should allow patients to maintain the convenience of wearing CLs. This discussion will allow for broadened CL choices for patients and prescribers who prefer the monthly CLs. While the results of this study should help propel the field, more work is needed to compare the study CLs to other reusable CLs and more work is needed to map in real-time the comfort of other reusable CLs. These data should help practitioners make better patient recommendations for reducing CL dropout.
Data Sharing Statement
No additional data beyond this reported will be publicly shared.
Acknowledgments
Alcon Research, LLC supported this study. REDCap data collection was supported by the University of Alabama at Birmingham’s CTSA Grant (UL1TR001417).
Funding
Alcon Research, LLC supported this research.
Disclosure
The authors have received support from Alcon Research, LLC (All), Art Optical (ADP), Contamac (ADP), CooperVision (ADP), Euclid Systems (ADP), EyeGate Pharmaceuticals, Inc (ADP), EpiTech (ADP), Kala (ADP), Nevakar, Inc (ADP), Optikal Care Inc (ADP). Dr Pucker is currently an employee of Lexitas Pharma Services; however, he still holds a part-time position at the University of Alabama at Birmingham.
References
1. Pucker AD, Tichenor AA. A review of contact lens dropout. Clin Optom. 2020;12:85–94. doi:10.2147/OPTO.S198637
2. Begley CG, Chalmers RL, Mitchell GL, et al. Characterization of ocular surface symptoms from optometric practices in North America. Cornea. 2001;20:610–618. doi:10.1097/00003226-200108000-00011
3. Pritchard N, Fonn D, Brazeau D. Discontinuation of contact lens wear: a survey. Int Contact Lens Clin. 1999;26:157–162. doi:10.1016/S0892-8967(01)00040-2
4. Richdale K, Sinnott LT, Skadahl E, Nichols JJ. Frequency of and factors associated with contact lens dissatisfaction and discontinuation. Cornea. 2007;26:168–174. doi:10.1097/01.ico.0000248382.32143.86
5. Dumbleton K, Woods CA, Jones LW, Fonn D. The impact of contemporary contact lenses on contact lens discontinuation. Eye Contact Lens. 2013;39:93–99. doi:10.1097/ICL.0b013e318271caf4
6. Santodomingo-Rubido J, Barrado-Navascues E, Rubido-Crespo MJ. Ocular surface comfort during the day assessed by instant reporting in different types of contact and non-contact lens wearers. Eye Contact Lens. 2010;36:96–100. doi:10.1097/ICL.0b013e3181d1d5a5
7. Woods CA, Bentley SA, Fonn D. Temporal changes in contact lens comfort over a day of wear. Ophthalmic Physiol Opt. 2016;36:643–648. doi:10.1111/opo.12318
8. Dumbleton KA, Guillon M, Theodoratos P, Patel T. Diurnal variation in comfort in contact lens and non-contact lens wearers. Optom Vis Sci. 2016;93:820–827. doi:10.1097/OPX.0000000000000920
9. Pucker AD, Jones-Jordan LA, Marx S, et al. Clinical factors associated with contact lens dropout. Cont Lens Anterior Eye. 2019;42:318–324. doi:10.1016/j.clae.2018.12.002
10. Terry RL, Schnider CM, Holden BA, et al. CCLRU standards for success of daily and extended wear contact lenses. Optom Vis Sci. 1993;70:234–243. doi:10.1097/00006324-199303000-00011
11. Chalmers RL, Keay L, Hickson-Curran SB, Gleason WJ. Cutoff score and responsiveness of the 8-item Contact Lens Dry Eye Questionnaire (CLDEQ-8) in a large daily disposable contact lens registry. Cont Lens Anterior Eye. 2016;39:342–352. doi:10.1016/j.clae.2016.04.005
12. Sullivan BD, Crews LA, Sonmez B, et al. Clinical utility of objective tests for dry eye disease: variability over time and implications for clinical trials and disease management. Cornea. 2012;31:1000–1008. doi:10.1097/ICO.0b013e318242fd60
13. Duong K, Pucker AD, McGwin G, Franklin QX, Cox J. An established soft contact lens wearers’ awareness of and initial experience with orthokeratology. Ophthalmic Physiol Opt. 2021;41:673–682. doi:10.1111/opo.12828
14. Maldonado-Codina C, Navascues Cornago M, Read ML, et al. The association of comfort and vision in soft toric contact lens wear. Cont Lens Anterior Eye. 2021;44:101387. doi:10.1016/j.clae.2020.11.007
15. Diec J, Tilia D, Thomas V. Comparison of silicone hydrogel and hydrogel daily disposable contact lenses. Eye Contact Lens. 2018;44:S167–S172. doi:10.1097/ICL.0000000000000363
16. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research Electronic Data Capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381. doi:10.1016/j.jbi.2008.08.010
17. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
18. Morgan PB, Efron N. Global contact lens prescribing 2000–2020. Clin Exp Optom. 2022;105:298–312. doi:10.1080/08164622.2022.2033604
19. Fogt JS, Patton K. Evaluation of wear experience with soft daily disposable lenses for astigmatism over 16 hours of wear. Clin Optom. 2022;14:207–214. doi:10.2147/OPTO.S387740
20. Fogt JS, Patton K. Long day wear experience with water surface daily disposable contact lenses. Clin Optom. 2022;14:93–99. doi:10.2147/OPTO.S367891
21. Papas EB, Keay L, Golebiowski B. Estimating a just-noticeable difference for ocular comfort in contact lens wearers. Investig Ophthalmol Vis Sci. 2011;52:4390–4394. doi:10.1167/iovs.10-7051
22. Nichols JJ, Willcox MD, Bron AJ, et al. The TFOS international workshop on contact lens discomfort: executive summary. Investig Ophthalmol Vis Sci. 2013;54:TFOS7–TFOS13. doi:10.1167/iovs.13-13212
23. Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3:e000146. doi:10.1136/bmjophth-2018-000146
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluating the Performance of Verofilcon A Daily Disposable Contact Lenses in a Group of Heavy Digital Device Users
Schulze MM, Fadel D, Luensmann D, Ng A, Guthrie S, Woods J, Jones L
Clinical Ophthalmology 2023, 17:3165-3175
Published Date: 24 October 2023
Real-Time Changes in the Comfort of a Toric, Monthly, Soft Contact Lens Over a Long Day of Wear
Lievens C, Perkins A, Rayborn E, Wang Y, Franklin Q, May K, Kannarr S, Bromley M, Pucker AD
Clinical Optometry 2024, 16:317-325
Published Date: 17 December 2024