Back to Journals » Clinical Ophthalmology » Volume 17
Evaluating the Performance of Verofilcon A Daily Disposable Contact Lenses in a Group of Heavy Digital Device Users
Authors Schulze MM ![]() , Fadel D
, Fadel D ![]() , Luensmann D, Ng A
, Luensmann D, Ng A ![]() , Guthrie S
, Guthrie S ![]() , Woods J
, Woods J ![]() , Jones L
, Jones L ![]()
Received 20 July 2023
Accepted for publication 16 October 2023
Published 24 October 2023 Volume 2023:17 Pages 3165—3175
DOI https://doi.org/10.2147/OPTH.S429250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marc-Matthias Schulze, Daddi Fadel, Doerte Luensmann, Alison Ng, Sarah Guthrie, Jill Woods, Lyndon Jones
Centre for Ocular Research & Education (CORE), University of Waterloo, Waterloo, ON, Canada
Correspondence: Marc-Matthias Schulze, Centre for Ocular Research & Education (CORE), University of Waterloo, Waterloo, ON, Canada, Tel +1 519-888-4742, Fax +1-519-888-4303, Email [email protected]
Purpose: The purpose of this study was to evaluate the performance of verofilcon A daily disposable contact lenses (CL) in CL wearers who identified themselves as heavy digital device users.
Patients and Methods: This prospective, non-masked, open-label study enrolled CL wearers who reported ≥ 6 hours digital device use per day. Participants were dispensed with the verofilcon A study lenses for 14± 2 days, to be worn for at least 5 days a week and 10 hours per day, while continuing their normal routine of digital device use. Participants rated the lens performance at the Day 14 visit using a 0– 100 (with 100 being best) scale. Ratings were completed at lens insertion, after 6 hours of digital device use, just before CL removal and for overall experience. Participants also completed a 4-point (strongly agree/disagree, slightly agree/disagree) Likert scale-based questionnaire.
Results: Thirty-two participants were eligible and completed the study (27 females; age 25.8 ± 6.0 years, ranging from 19 to 40). Overall lens performance ratings at the Day 14 visit (mean ± standard deviation) for comfort, dryness, and clarity of vision were 91 ± 11, 88 ± 11, and 92 ± 9, respectively. Subjective ratings were stable throughout the day with no significant differences after insertion, after 6 hours of digital device use and before CL removal (all p> 0.05). The majority of participants agreed that the study lenses performed well, provided good all-day comfort (28/32; p< 0.01) and good all-day vision (29/32; p< 0.01). Participants also agreed that after ≥ 6 hours of digital device use they were satisfied with CL comfort (27/32; p< 0.01), vision (29/32; p< 0.01) and that the lenses provided good performance (26/32; p< 0.01).
Conclusion: Verofilcon A lenses were found to perform well, with high ratings for comfort, dryness and vision that remained high throughout the day, during extensive digital device use.
Keywords: digital device, vision, comfort, verofilcon A, lens wettability, contact lenses
Introduction
The number of contact lens (CL) wearers globally exceeds 140 million, with roughly one-third of wearers being based in the United States.1,2 Despite these numbers, anywhere between 12 and 51% of CL wearers have been reported to cease CL wear within the first year, with discomfort, poor distance and/or near vision as well as handling being the main reasons for discontinuation.2–5
With today’s ever-expanding access to digital devices, the number of potential CL wear dropouts may further be affected by digital device use. Sheppard and Wolffsohn reported that there was a higher prevalence of symptoms of eye strain, eye fatigue, or blurred vision in CL wearers compared to non-CL wearers (65% vs 50%) when using digital devices.6 The symptoms associated with digital device use in CL wear may be affected by multiple factors, including an insufficient blink rate, which is reduced during digital device activity7–14 or for a poorly wetting CL.15–17 Several studies have explored the impact of digital device use on eye health, revealing that it can lead to symptoms such as eye strain, dryness, and discomfort.7–14 Blink rate and amplitude may decrease during extended periods of visual attention on digital devices, contributing to ocular dryness and discomfort.7–14 Overall, these studies suggest that there is a relationship between prolonged visual attention, blink rate, and tear film integrity, and various strategies can be employed to reduce the negative effects of digital device use on eye health. According to the recently published TFOS Lifestyle report on the impact of the digital environment on the ocular surface,14 these strategies include the use of oral Omega-3 fatty acid supplements, taking regular breaks from viewing the device, reminders to blink more frequently, a more ergonomic office setup, adjustments to screen and/or font size and improved environmental conditions (ie increased humidity). Truong et al recommended a personalized approach to CL fitting and management, taking into account individual factors such as CL material, wear time, environment, age, and gender, to address discomfort associated with CL use.15
Contact lens manufacturers continue to develop novel materials to improve CL wear experience and reduce wearer symptoms. One such material, verofilcon A, has recently been introduced as a new silicone hydrogel daily disposable (DD) lens option (PRECISION1®, Alcon Laboratories Inc, Fort Worth TX, USA). Incorporating silicone into the material renders it inherently more hydrophobic than hydrogel materials, necessitating some form of advanced technology to enhance lens surface wettability, allowing the lens to be wetted effectively by the tear film while on the eye.18 Verofilcon A DD CLs have 51% core water content, an oxygen permeability (Dk) of 90 and a central Dk/t of 100 barrers/cm at −3.00D.19 While the silicone hydrogel core of the verofilcon A material provides high levels of oxygen permeability and easy handling, the SMARTSURFACE® Technology helps to support lens surface wettability, comfort, and to maintain an optically precise tear film for sustained, high-quality vision.20 SMARTSURFACE® Technology is a micro-thin moisture layer (approximately 2–3 microns) enveloping the lens core, with >80% water content. The significance of this SMARTSURFACE® layer lies in its ability to help maintain a consistent pre-lens tear film during wear.19 During the manufacturing process, the lenses undergo a series of treatments during which the lenses are immersed in specialized baths containing hydrogel polymers, notably polyacrylic acid (PAA), an exceptionally hydrophilic polymer. These polymers integrate with the core material, draw water to the surface of the lens and create the lens surface, establishing a water-friendly layer spanning a few microns. This process conceals the silicone within the contact lens, ensuring the lens surface remains wettable.19 While a number of studies have reported on the clinical performance21–24 of verofilcon A lenses in symptomatic and asymptomatic wearers and on the material’s in vitro surface wettability,25 its performance for CL wearers who spend the majority of their lens wear time in front of digital devices is yet to be evaluated and reported.
The purpose of this study was to evaluate the subjective and clinical performance of verofilcon A DD CLs in a group of CL wearers who used digital devices for at least 6 hours while wearing their habitual CLs.
Materials and Methods
Study Design
This was a prospective, non-masked, open-label dispensing study (clinicaltrials.gov registration NCT04201639). Users of digital devices for at least six hours on a typical day while wearing CLs were enrolled. This clinical study was conducted in compliance with the ethical principles in the Declaration of Helsinki, the ICH guidelines for Good Clinical Practice (GCP), the University of Waterloo’s Guidelines for Research with Human Participants, and the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, 2nd Edition. Ethics clearance was obtained through the Office of Research Ethics at the University of Waterloo before the commencement of the study. In addition, all participants had signed written informed consent prior to any study measurements being performed.
The study included a total of three study visits, with Visit 1 (V1; Screening and Study CL fitting) and Visit 2 (V2; Baseline and Lens Dispense) being conducted consecutively on the same day. At the end of V2, participants were dispensed with the verofilcon A CLs and asked to wear the study lenses for at least ten hours per day for five days per week, while maintaining their habitual digital device routine of at least six hours per day for the duration of the study. Participants were asked to self-monitor their lens wear experience during the 14 days of wear for three time-points:
- directly after lens insertion,
- after they estimated that they had approximately six hours of digital device use
- just before removal.
The study lenses were worn bilaterally and on a daily disposable basis; no lens care solution was required or dispensed. Participants were discouraged from using rewetting drops; however, those who habitually used them were allowed to continue using their normal drops. Participants returned for the Day 14 visit (Visit 3 (V3); 14 ± 2 days after V2) after at least six hours of study lens wear and exited the study at the end of this visit.
Eligibility Criteria
To be eligible for this study, potential participants had to be habitual wearers of daily, spherical, soft CLs for at least five days a week and at least ten hours per day during the month before enrolment, and routinely use digital devices for at least six hours on a typical day while also wearing CLs. The minimum of six hours of digital device use was chosen to ensure that a large portion of the time during which a participant wore their habitual CLs (minimum 10 hours/day) was spent using digital devices; participants had no limitation regarding the maximum hours of digital device use and lens wear times. Any combination of digital device use, such as PC, laptop, smartphone, or tablet, was permitted. The age range was limited to 18 to 40 years of age (inclusive) to reduce a potential impact of presbyopia on visual performance during digital device use. Participants were required to have a vertex-corrected spherical equivalent distance refraction between −0.50D and −6.00D in each eye and a vertex-corrected refractive cylinder of no more than −1.00DC. Participants were excluded if they were current wearers of the study lenses (verofilcon A), bifocal or multifocal CLs, wore their CLs on an extended wear basis, or as a monovision correction. Participants were also excluded if they had undergone refractive error surgery or were pregnant, lactating or planning a pregnancy at the time of enrolment. Additional exclusion criteria were the presence of any known active ocular disease and/or infection or a systemic condition, a known sensitivity to sodium fluorescein, aphakia, and the use of any systemic or topical medications.
Study Procedures
At the Day 14 visit (V3), participants were asked to report on their self-monitored experience with the lenses overall and for the three different time-points: at lens insertion, after six hours of digital device use, and just before CL removal. To do so, participants rated the performance of the lenses by assigning a numerical rating on a 0 (ie worst) to 100 (ie best) scale corresponding to the levels of comfort, dryness and clarity of vision they experienced with the study lenses on a typical day during the two weeks of lens wear. The rating scales included descriptors at the 0 and 100 endpoints for comfort (0 = “painful” to 100 = “can’t feel the lenses”), dryness (0 = “extremely dry” to 100 = “no dryness”) and clarity of vision (0 = “very blurred” to 100 = “very clear”). Participants were also asked to rate their satisfaction (4-point Likert scale: strongly disagree, slightly disagree, slightly agree, strongly agree) with the study CLs for eight statements evaluating the overall lens performance and while using digital devices:
- The study lenses provide good comfort all day long.
- The study lenses provide good vision all day long.
- I am satisfied with the comfort the study lenses provide when I use digital devices for ≥6 hours.
- I am satisfied with the vision the study lenses provide when I use digital devices for ≥6 hours.
- I do not experience eye strain when I wear the study lenses and use digital devices for ≥6 hours.
- I do not experience eye fatigue (tired eyes) when I wear the study lenses and use digital devices for ≥6 hours.
- I do not experience episodes of blurred vision when I wear the study lenses and use digital devices for ≥6 hours.
- Overall, these lenses provide good performance when using digital devices for ≥6 hours.
A reduced blink rate is often associated with digital device use8,9,11,26 and may result in blurry or degraded vision in contact lens wearers when the pre- and post-lens tear film is not sufficiently replenished by blinking.9,11,26 A novel metric to quantify the impact of prolonged eye opening on the visual quality when looking at a computer screen has recently been developed at the Centre for Ocular Research & Education (CORE). The metric, time-to-haze (TTH), is used to measure the maximum time an individual can keep their eyes open without their vision becoming hazy. In this study, TTH was measured at V2 after insertion and V3 after 6 hours of CL wear using a custom VA system which allowed adjustments to contrast levels on a logarithmic scale. Participants were seated in a dark exam room at a distance of 1m in front of a computer screen on which a single five-letter line corresponding to a letter size of +0.5 logMAR was presented. They were asked to read the five letters, and if read correctly, a new line of five new letters of the same size but at the next (lower) contrast level was presented; as an example for this system, a change from level 7 to level 8 corresponded to a decrease in contrast by 24%. The participant continued to read the letters at gradually decreasing contrast levels until they indicated that they were no longer able to read them; at this point, the contrast was re-adjusted to one level above their contrast threshold and legibility of all five letters was confirmed. The participant was instructed to blink three times and to hold their eyes open while continuously looking at the row of letters, and to immediately indicate the moment when at least one or more letters had become illegible, at which point they would be asked to blink until all letters were clear again. TTH (in seconds) was measured using a stopwatch which was started after the last of three blinks; once the participant indicated that at least one letter had become illegible, the time was stopped and the number of blinks it took until the participant could see all five letters clearly again was counted.
Lens fit was assessed at the slit-lamp biomicroscope by observing lens centration, movement and tightness. Lens centration was assessed using a scale from 0 (optimal) to 3 (excessive and occasionally encroaching limbus). Lens movement on primary gaze was assessed using a scale ranging from +2 (unacceptably loose fit) to −2 (unacceptably tight fit), with 0 being optimal. Lens tightness on push-up was assessed using a scale from 0 (falls from cornea without lid support) to 100 (no movement), with 50 being optimal.
Other variables included lens surface and tear film characteristics (wettability, deposits, and pre-lens tear film break-up time (TBUT)), conjunctival redness, and visual acuity (VA). Lens surface wettability was assessed at the slit-lamp biomicroscope by observing the appearance of the specular reflection of the Purkinje image in the pre-lens tear film under high magnification using a 0–4 scale in 0.25 steps, where 0 corresponds to a smooth surface and 4 to a lens surface that shows incomplete rewetting and immediate drying.16,27 Visible deposits were assessed at the slit-lamp biomicroscope using a 0–4 scale in 0.25 steps (0 being excellent). Pre-lens TBUT was measured using a stopwatch (in seconds) at a placido disc instrument (Atlas 991 corneal topographer; Zeiss Humphrey Systems, Dublin, California, USA); three measurements for each eye were taken and averaged, using the averaged TBUT for analysis. A full biomicroscopic evaluation was conducted at V1 to obtain baseline levels of ocular surface health (no CL wear for at least 12 hours prior to visit) and after study lens removal at the Day 14 visit (V3; after at least six hours of verofilcon A lens wear). Conjunctival redness was assessed for the bulbar and limbal conjunctiva using the Efron grading scale28 (0 to 4, with 0 = normal; 0.1 increments) to identify any hypoxia-induced changes after at least 6 hours of verofilcon A wear at V3 compared to baseline levels. Safety assessments at V1 and V3 included evaluation of corneal integrity (presence/absence of external adnexa and corneal abnormalities, including opacities and infiltrates), grading of corneal and conjunctival staining by zone after application of sodium fluorescein using blue light and a Wratten 12 filter as well as grading of palpebral redness and roughness. High illumination high contrast (HIHC) logMAR VA with the study lenses was measured after lens insertion at the lens dispense visit and after at least six hours of lens wear at the Day 14 visit.
Statistical Analysis
The sample size required for a 2-tailed matched paired t-test to detect a change of 5 points on a 0–100 subjective rating scale, with α=0.05, power of 0.90, and an effect size of 0.60 resulted in a minimum sample size of 32 participants to complete the study. Data analysis was conducted using Statistica 13.5 (Tibco, Palo Alto, CA, USA) and IBM SPSS Statistics 27.0 (IBM, Armonk, NY, USA).
Statistical analysis showed that data for the majority of variables were not normally distributed (Kolmogorov–Smirnov test; p<0.05); therefore, for consistency, all data were analyzed using non-parametric statistics. Wilcoxon matched pairs testing was performed to identify differences between eyes or for different time points, with the significance level set to α=0.05. For assessments conducted for each eye separately, the right eye was used for analysis if there was no difference between eyes.
Binomial testing was conducted to analyze Likert-type questionnaires (strongly agree, slightly agree, slightly disagree, strongly disagree) to determine whether participants had a positive or negative experience with the study lens. For this analysis, “strongly agree” and “agree” were combined into a single “agreement” category; similarly, “strongly disagree” and “disagree” were combined into a single “disagreement” category. Study data are presented as mean, median and count as described in this section, individual participant data will not be shared.
Results
Participants
Thirty-five participants were enrolled in the study, with 32 participants being eligible (27 females, 5 males; mean age 25.8 ± 6.0 years, ranging from 19 to 40). All 32 eligible participants completed the study, comprising 20 habitual wearers of reusable lens types (63%) and 12 DD CL wearers (37%). Three participants were ineligible due to active ocular findings detected at the screening visit, prior to exposure to the study lenses.
There was no statistically significant difference in digital device usage on a typical day while wearing habitual lenses and while wearing the study lenses during the two-week study wear period (p=0.37; Table 1). The mean comfortable wear time with the verofilcon A lenses increased by about one hour compared to the participant’s habitual CLs (10.5 vs 11.4 hours, respectively), however, this difference was not statistically significant (p=0.23; Table 1).
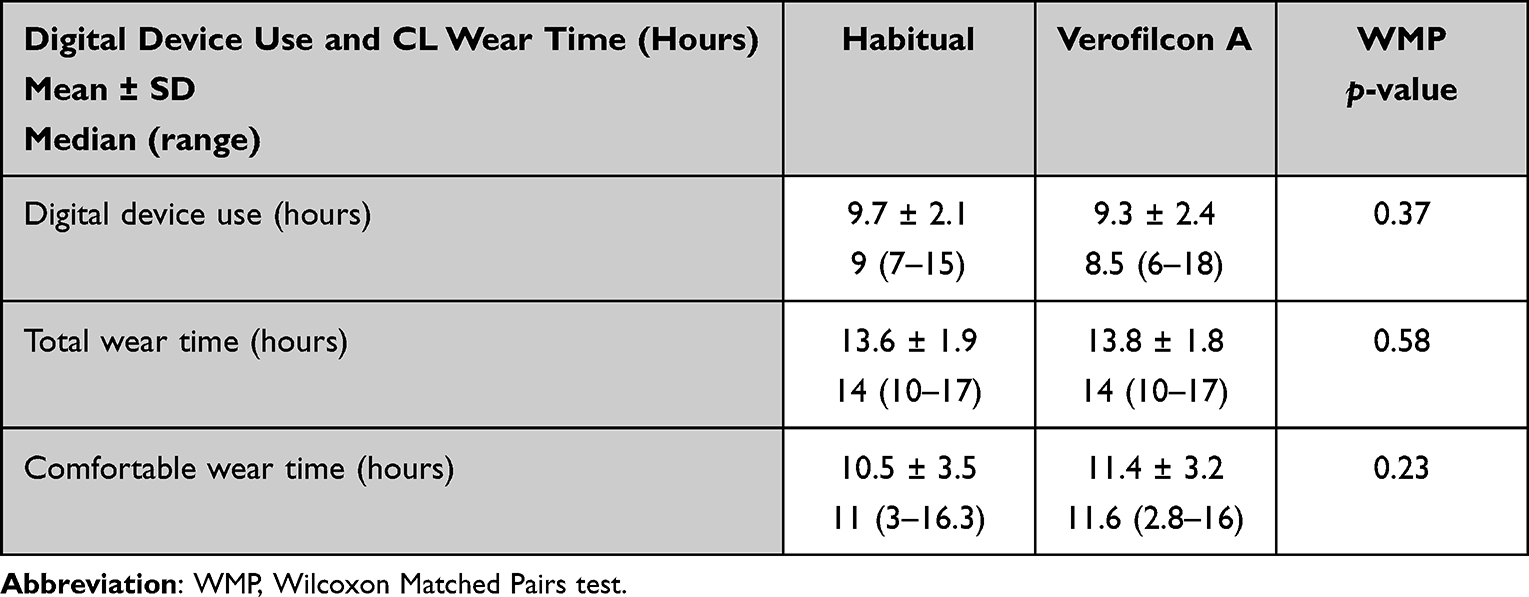 |
Table 1 Digital Device Use and CL Wear Times for a Typical Day with Habitual and Study CLs |
Subjective Ratings
Table 2 shows the subjective ratings collected at the dispensing visit, immediately after lens insertion, and at the Day 14 visit, reflecting a typical lens wear day. Initial ratings of comfort, dryness and clarity of vision were high at the dispensing visit and similarly, were rated highly on a typical day of lens wear during the study period at V3. There were no statistically significant differences in any ratings between time points within a typical day for comfort, dryness, or clarity of vision during the study period (p>0.05, Figure 1).
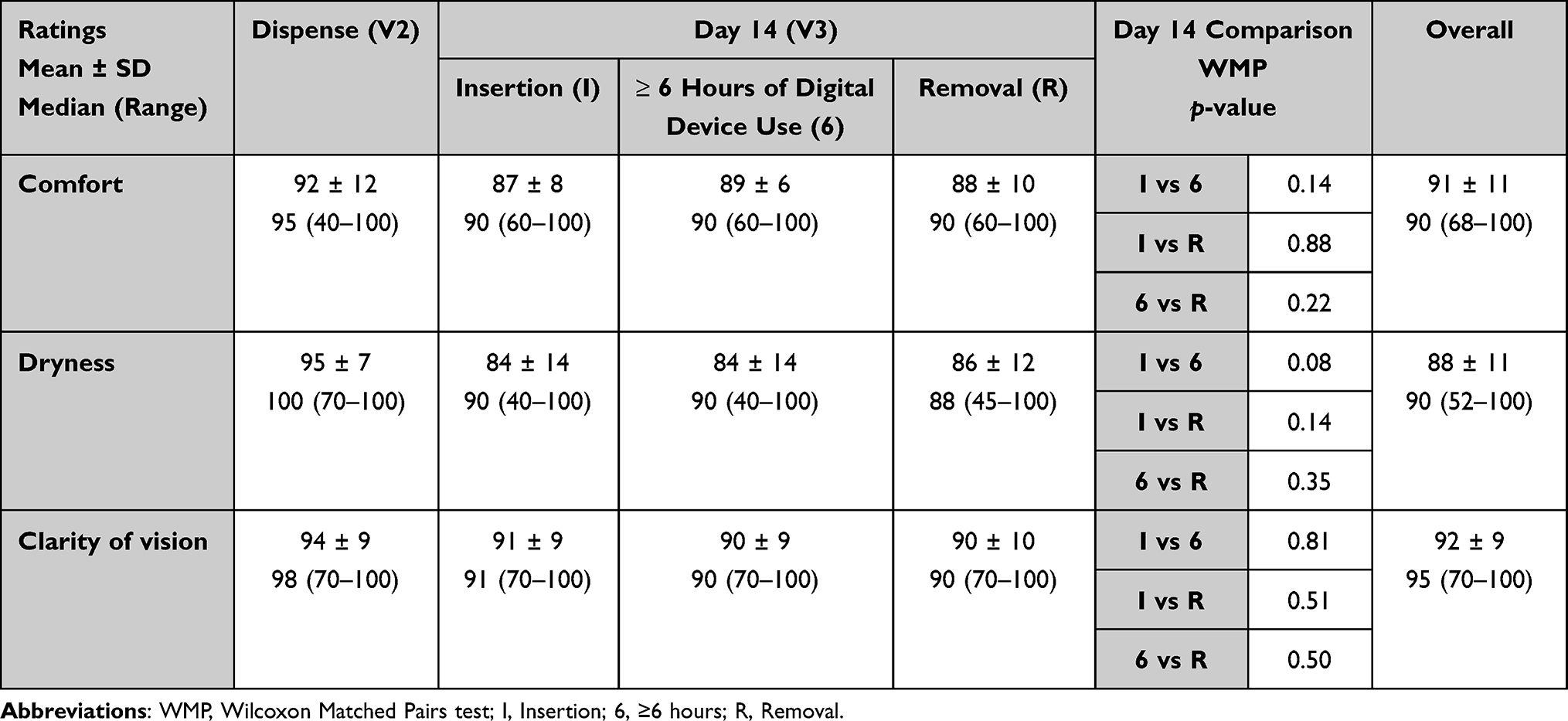 |
Table 2 Ratings for Comfort, Dryness and Clarity of Vision at the Dispensing Visit (Immediately After Insertion) and the Day 14 Visit (for a Typical Lens Wear Day), 0–100 Scale with 100 Being Best: Mean ± SD, Median (Range) |
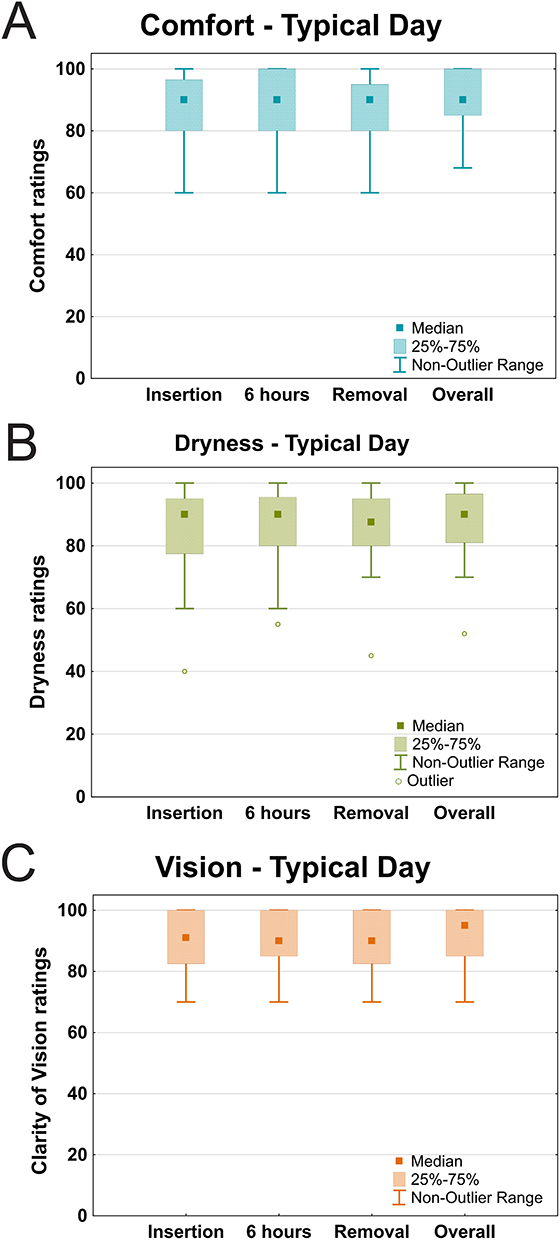 |
Figure 1 Day 14 ratings (0–100, with 100 being best) on a typical lens wear day for comfort (A), dryness (B) and clarity of vision (C); ratings are shown for three time-points across the day (after insertion, after at least 6 hours of digital device use and prior to lens removal) and with regard to overall performance. |
Satisfaction Ratings (Likert Scale)
At the Day 14 visit, participants reported a positive experience when responding to statements related to their satisfaction with the study lenses. Figure 2 shows the distribution of responses for each statement and the associated significance level from binomial testing. After two weeks of wear, the majority of participants agreed that the study lenses provided good all-day comfort (28/32, 88%; p<0.01) and good all-day vision (29/32, 91%; p<0.01). Similarly, the majority of participants were satisfied with the comfort (27/32, 84%; p<0.01), vision (29/32, 91%; p<0.01), and overall performance (26/32, 81%; p<0.01) they experienced with the study lenses while using digital devices for at least six hours. Additionally, most agreed they did not experience eye strain while using the study lenses (24/32, 75%; p<0.01). The number of respondents in agreement with the statement “I don’t experience eye fatigue (tired eyes) when I wear the study lenses and use digital devices for at least 6 hours” narrowly failed to meet the criteria for significance (22/32, 69%; p=0.0501). There was no significant difference between the number of responses in agreement (18/32, 56%) and disagreement (14/32, 44%) with the statement “I don’t experience episodes of blurred vision when I wear the study lenses and use digital devices for ≥6 hours” (p=0.60).
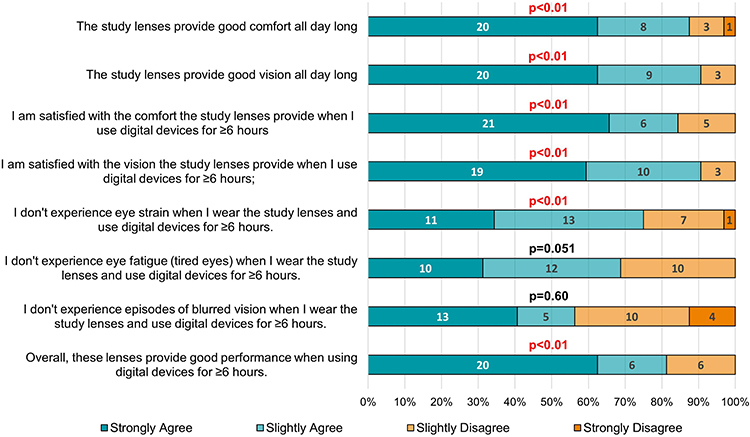 |
Figure 2 Participant answers to lens performance statements, based on selection of one of four Likert scale-based options (strongly agree, slightly agree, slightly disagree, strongly disagree). |
Clinical Performance
Lens fit assessments were conducted after lens insertion at the dispensing visit (V2) and after at least six hours of lens wear at the Day 14 visit (V3). There were no significant differences in lens centration after lens insertion at V2, with a mean centration grade of 0.6 ± 0.5 compared to a grade of 0.5 ± 0.5 after at least six hours of wear at V3 (p=0.42). At V3, lens centration was assessed as optimal (17/32, 53%) or slightly decentered (15/32, 47%), with all lenses fully covering the limbus for all participants. Lens movement on primary gaze and tightness on push-up were close to optimal, with a tendency for slightly loose fits, at V2 after lens insertion and similarly at V3 after at least six hours of wear (movement on primary gaze: V2: 0.3 ± 0.6mm, V3: 0.3 ± 0.5mm, p=0.83; lens tightness V2: 47 ± 7%, V3: 47 ± 5%, p=0.78).
Table 3 summarizes the lens surface and tear film related assessments. The study lenses showed close to excellent wettability with very minimal deposits, shortly after lens insertion (V2) and after six hours of wear (V3; Table 3). There was a statistically significant difference in pre-lens TBUT between eyes at V2, directly after insertion; however, this difference was not present at V3 when TBUT was assessed after six hours of wear. TTH values were similar after lens insertion and after at least six hours of lens wear at the Day 14 visit (median TTH 7.5 seconds for both V2 and V3, p=0.33; Table 3). On average, participants needed one blink to clear their vision at both visits (p=0.65; Table 3).
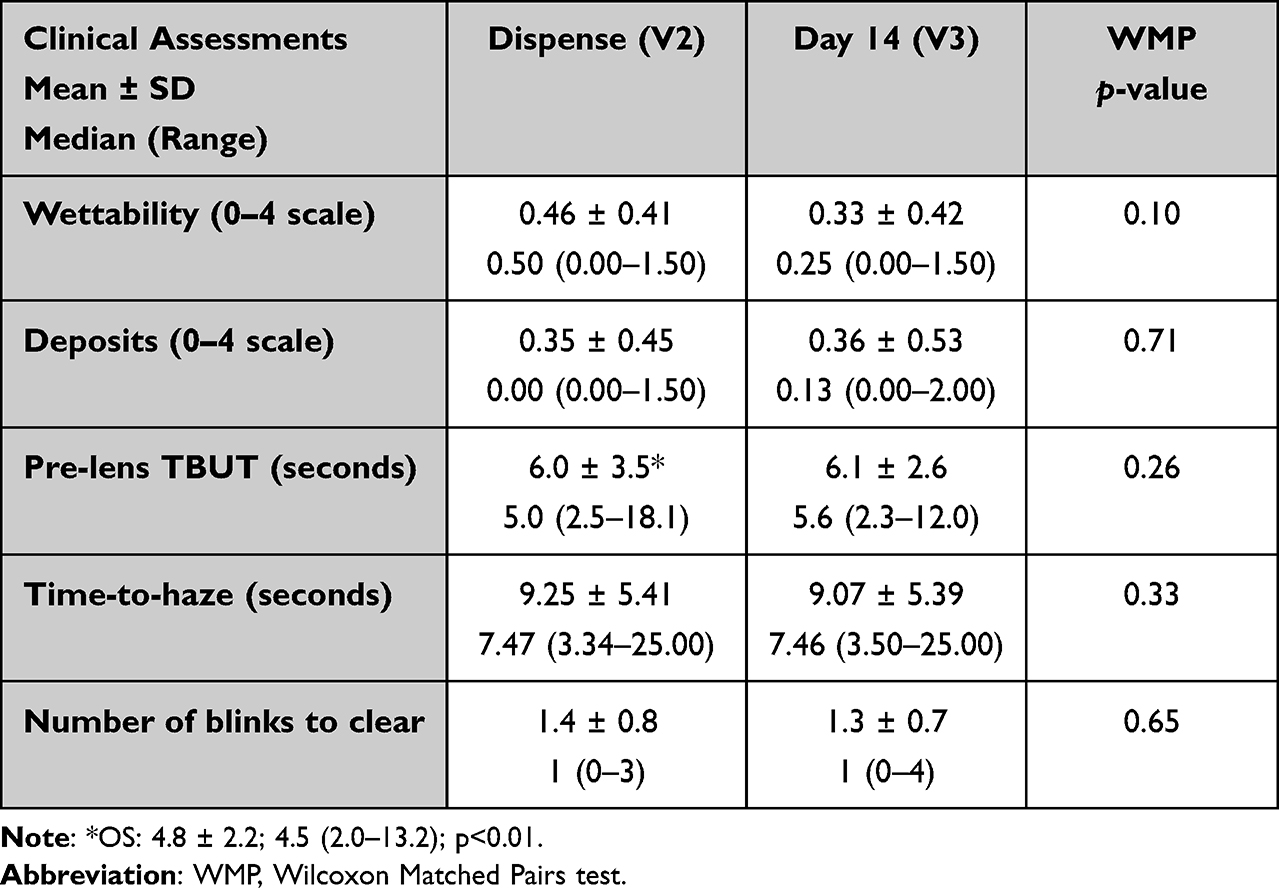 |
Table 3 Lens Surface and Tear Film Related Assessments at Dispense and Day 14 Follow-Up Visit |
Both bulbar and limbal redness levels were low, with mean grades of no more than 1.1 on the 0 to 4 scale at V2 and V3. There was no difference in mean bulbar (p=0.72) or limbal redness levels (p=0.42) between the screening visit, when no lenses had been worn for at least 12 hours prior (bulbar 1.0 ± 0.3; limbal 0.8 ± 0.3), and redness at the Day 14 visit after at least six hours of CL wear (bulbar 1.0 ± 0.3; limbal 0.9 ± 0.3). Similarly, no changes in ocular physiology were observed at V3 for any of the assessed safety variables (all p>0.05); none of the participants presented with any conjunctival indentation after at least 6 hours of verofilcon A wear.
HIHC distance logMAR VA with study lenses was high, with median logMAR VA being similar after insertion (−0.10, ranging from −0.22 to 0.00) to after six hours of wear (−0.08, ranging from −0.20 to +0.06; p=0.11).
Discussion
This study evaluated the performance of a new SiHy DD CL manufactured from verofilcon A material in a group of existing soft CL wearers who were heavy (ie ≥6 hours during CL wear) users of digital devices.
Overall, the study lenses performed very well clinically. The study lenses were successfully fitted to all 32 eligible study participants and were found to have a highly wettable surface, with very few visible deposits both shortly after insertion and after at least six hours of wear. Assessments of lens fit, including centration, movement, and tightness, were close to optimal, with a small trend towards slightly loose fits. Lens fit and centration were also similar to initial fitting after at least six hours of wear on Day 14. Visual acuity with the study lenses was high, with no visual deterioration after at least six hours of lens wear and subjectively, 91% agreed that the study lenses provided good vision all day long and were satisfied with the vision when they used digital devices for ≥6 hours. The study lenses were also found to not impact ocular physiology after two weeks of wear, with none of the participants presenting with changes to baseline for any of the safety variables evaluated. Bulbar and limbal redness levels after 6 hours of verofilcon A wear at V3 were very low, with Efron grades around 1 or less, and these were similar compared to baseline levels (baseline levels were obtained after a participant had not worn their habitual lenses for at least 12 hours).
The main purpose of this study was to evaluate the performance of this lens in pre-existing CL wearers who identified themselves as heavy digital devices users (defined in this study as at least six hours of device use per day). In today’s world, digital devices are used everywhere, with the majority of time being spent using them indoors – which often means being in an environment where eyes are exposed to dry heat or air conditioning, compounding symptoms of ocular discomfort and dryness that might arise from reduced blinking during screen use.14 This becomes even more relevant for CL wearers, with dryness and discomfort being among the main reasons for cessation of lens wear in adapted wearers.2,29 Hence, CL wearers who spend many hours in front of digital devices benefit from lenses that are comfortable while providing continuously clear vision at all times under challenging conditions.
Stable CL performance throughout the day is crucial for maintaining both comfort and optimal visual performance. Notably, dropout rates are high within the first year of lens wear, with 41% of individuals experiencing vision problems and 36% reporting discomfort.5 This is particularly relevant for those people who wear CL and spend over six hours a day on the computer, as they face a higher risk of developing Computer Vision Syndrome compared to non-lens wearers with similar computer usage.30 Ocular comfort naturally decreases throughout the day, regardless of lens wear, but studies have shown that comfort tends to decline more when wearing CLs.31,32 However, evaluating end-of-day comfort can be challenging, since patients have varying definitions of their “end of day”.24 In addition to discomfort, temporary blurry vision while wearing soft CL has been identified as a common cause of CL dissatisfaction.2,9,33–35 Thus, maintaining a consistent optical surface is critical for reducing light scattering and preventing optical aberrations during CL wear.36
Based on their clinical and subjective performance in this study, verofilcon A lenses may be a viable option for lens wearers who spend extensive hours in front of digital screens. In this study, median digital device use time for a typical CL wearer was 8.5 hours per day, ranging from 6 to 18 hours. Subjective ratings for overall lens performance on a typical day within the two-week study wear period were very high for comfort, dryness and vision. More importantly, wearers reported consistently high levels of comfort, dryness and clarity of vision across the course of a full day of study lens wear, from immediately after lens insertion, after six hours of digital device use through to just before lens removal. This long-lasting performance is especially notable considering that at least one participant wore their study lenses for up to 17 hours while using digital devices. Participants were allowed to use their habitual rewetting drops during the study, which may be considered a limitation. A comparison of rewetting drop use with habitual and study CLs showed that while six out of seven habitual users of rewetting drops continued to use their drops while wearing the study lenses, all but one participant reduced the frequency of their rewetting drop use when wearing verofilcon A lenses.
Participants were also in agreement that the lenses provided good comfort and vision all day long – with or without digital device use – and agreed that they were satisfied with the lens performance even after more than six hours of wear while using digital devices (Figure 2). Blurred vision is a well-documented “side-effect” for many digital device users, even for those not requiring any kind of vision correction.6,7,37,38 Episodes of blurry vision have been associated with insufficient blink rates or the presence of incomplete blinks,6,7,10,38–40 with symptoms of blur being exacerbated by digital device use.41 CL wear further impacts a patient’s blinking behaviour7,9,11 and results in the occurrence of transient blurry vision during CL wear that can be cleared up by blinking.2,9,33–35 In a study evaluating four different digital device tasks both with spectacles and three different CL types, the number of blinks while wearing CLs increased by a factor of 1.7 to 2.5 compared to spectacle wear, with a greater proportional change for more demanding visual tasks.11 The finding that there was no statistically significant difference in the number of participants reporting episodes of blurred vision (18/32) to those who did not experience those episodes (14/32; p=0.60) in this current study was therefore not surprising, as people use digital devices for a range of tasks, from scrolling social media for leisure to reading extensive texts, which differ in visual and cognitive demand and did not appear to impact the participant satisfaction with the overall performance of the study CLs when using digital devices (Table 2 and Figure 2).
The pre-lens TBUT and TTH metrics that were measured at both V2 and V3 provided some useful insight into CL wearer behaviour while using digital devices. Knowing that prolonged eye-opening results in a deteriorating tear film (which may temporarily impact vision) that can be replenished by blinking,2,9,33–35 the average pre-lens TBUT of roughly 5 to 6 seconds (Table 3) suggests that a study participant would have needed to blink about 10 to 12 times per minute to maintain a stable tear film and clear vision. It is well known that the introduction of a CL contributes to an interruption of the tear film integrity, and the TBUTs found in this study align closely with those reported in previous studies.42,43 However, the first appearance of a deteriorating tear film does not necessarily mean that vision becomes blurry immediately. The median TTH measures in this study were approximately 7.5 seconds both at the dispense visit (V2; after lenses had settled for up to 10 minutes) and after six hours of lens wear at the Day 14 visit (V3) (Table 3). Using the same rationale as above, this suggests that a blink rate of at least 8 blinks per minute (60s/7.5s = 8 blinks) should have theoretically allowed most participants to maintain clear vision when wearing the lenses during digital device use. The finding that some participants still reported episodes of blurred vision with digital device use suggests that the time between blinks while using digital devices may have exceeded these 7.5 seconds. This is particularly relevant when considering that the TTH data were collected by displaying letters just above contrast threshold and not at typical contrast levels for text and graphics on digital device displays. Another explanation for this finding may be the level of visual demand that was needed to be met at the time when the blur occurred, with more demanding tasks such as playing a fast-paced game resulting in longer periods of eye opening compared to simpler tasks like streaming a show.7,11
While this study was relatively short in nature and only evaluated the performance of a single lens type, the clinical and subjective performance in this study makes the verofilcon A lens a promising option for digital device users who are prone to experiencing discomfort or degrading vision during prolonged periods of digital device use. The verofilcon A study lenses performed very well in a group of CL wearers who routinely used digital devices for six to 18 hours per day. The lenses could be successfully fit to all participants, with participant-rated lens performance attributes remaining stable throughout a typical day.
Abbreviations
CL, contact lens; DD, daily disposable; SiHy, silicone hydrogel; TTH, time-to-haze; VA, visual acuity; TBUT, Tear Break up time; HIHC, High illumination high contrast.
Funding
This investigator-initiated study was funded by Alcon Vision, LLC.
Disclosure
All authors are affiliated with CORE. Over the past three years, CORE has received research funding and/or honoraria from Alcon Inc, Azura Ophthalmics, Bausch + Lomb Corp, CooperVision, Essilor, Hoya, i-Med Pharma, Johnson & Johnson Vision, Menicon, Novartis, Ophtecs, Oté Pharma, Santen, SightGlass, SightSage, Topcon, Visioneering Tech Inc. Over the past 3 years, Daddi Fadel has received financial support or lectureship honoraria from the following companies: Augmented Vision Labs, Baush & Lomb, Boston Materials, Bostonsight, British Contact Lens Association, Chio by Cliara, Contamac, DMV, Eaglet Eye, EasyLac, Hakim Group, Medlac, Medmont, Menicon, Multilens, Occhio x Occhio, Oculus, OptiforuM, Scleral Lens Society, Scope, SynergEyes, Swisslens, Topcon healthcare, Wave Software. The authors report no other conflicts of interest in this work.
References
1. Cope JR, Collier SA, Nethercut H, Jones JM, Yates K, Yoder JS. Risk behaviors for contact lens-related eye infections among adults and adolescents - United States, 2016. MMWR Morb Mortal Wkly Rep. 2017;66(32):841–845. doi:10.15585/mmwr.mm6632a2
2. Pucker AD, Tichenor AA. A review of contact lens dropout. Clin Optomet. 2020;12:85–94. doi:10.2147/OPTO.S198637
3. Dumbleton K, Woods CA, Jones LW, Fonn D. The impact of contemporary contact lenses on contact lens discontinuation. Eye Contact Lens. 2013;39(1):93–99. doi:10.1097/ICL.0b013e318271caf4
4. Nichols JJ, Willcox MD, Bron AJ, et al. The TFOS International Workshop on Contact Lens Discomfort: executive summary. Invest Ophthalmol Vis Sci. 2013;54(11):TFOS7–TFOS13. doi:10.1167/iovs.13-13212
5. Sulley A, Young G, Hunt C, McCready S, Targett MT, Craven R. Retention rates in new contact lens wearers. Eye Contact Lens. 2018;44(Suppl 1):S273–s282. doi:10.1097/ICL.0000000000000402
6. Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3(1):e000146. doi:10.1136/bmjophth-2018-000146
7. Cardona G, García C, Serés C, Vilaseca M, Gispets J. Blink rate, blink amplitude, and tear film integrity during dynamic visual display terminal tasks. Curr Eye Res. 2011;36(3):190–197. doi:10.3109/02713683.2010.544442
8. Himebaugh NL, Begley CG, Bradley A, Wilkinson JA. Blinking and tear break-up during four visual tasks. Optom Vis Sci. 2009;86(2):106–114. doi:10.1097/OPX.0b013e318194e962
9. Jansen ME, Begley CG, Himebaugh NH, Port NL. Effect of contact lens wear and a near task on tear film break-up. Optom Vis Sci. 2010;87(5):350–357. doi:10.1097/OPX.0b013e3181d951df
10. Portello JK, Rosenfield M, Chu CA. Blink rate, incomplete blinks and computer vision syndrome. Optom Vis Sci. 2013;90(5):482–487. doi:10.1097/OPX.0b013e31828f09a7
11. Schulze MM, Wong A, Haider S, et al. Blink rate in silicone hydrogel contact lens wearers during digital device use.
12. Coles-Brennan C, Sulley A, Young G. Management of digital eye strain. Clin Exp Optom. 2019;102(1):18–29. doi:10.1111/cxo.12798
13. Talens-Estarelles C, García-Marqués JV, Cerviño A, García-Lázaro S. Determining the best management strategy for preventing short-term effects of digital display use on dry eyes. Eye Contact Lens. 2022;48(10):416–423. doi:10.1097/ICL.0000000000000921
14. Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: impact of the digital environment on the ocular surface. Ocul Surf. 2023;28:213–252. doi:10.1016/j.jtos.2023.04.004
15. Truong TN, Graham AD, Lin MC. Factors in contact lens symptoms: evidence from a multistudy database. Optom Vis Sci. 2014;91(2):133–141. doi:10.1097/OPX.0000000000000138
16. Keir N, Jones L. Wettability and silicone hydrogel lenses: a review. Eye Contact Lens. 2013;39(1):100–108. doi:10.1097/ICL.0b013e31827d546e
17. Yu Z, Croner D, Huth S, Panganiban O. Wettability of contact lenses: are wetting angles clinically significant? Rev Cornea Contact Lenses. 2006;42:47.
18. Willcox M, Keir N, Maseedupally V, et al. BCLA CLEAR - Contact lens wettability, cleaning, disinfection and interactions with tears. Contact Lens Anterior Eye. 2021;44(2):157–191. doi:10.1016/j.clae.2021.02.004
19. Mathew JH. White paper: PRECISION1® Contact Lenses With SMARTSURFACE® Technology: Material Properties, Surface Wettability and Clinical Performance; 2019. Available from: https://us.alconscience.com/sites/g/files/rbvwei1736/files/pdf/1906A195-US-DP1-19-E-1306_DP1-White-Paper_iPad.pdf.
20. Shi C, Cantu-Crouch D, Sharma V, Wu J. Characterization of a novel surface modified silicone hydrogel contact lens in fully hydrated environments. Invest Ophthalmol Vis Sci. 2019;60(9):6349.
21. Subbaraman L, Spear KG, Brobst A, Cummings S. Clinical lens fit characteristics of a new silicone hydrogel daily disposable and two commercially available daily disposable contact lenses. Contact Lens Anterior Eye. 2021;44(Supplement 1):5.
22. Schulze MM, Ng A, Luensmann D, Guthrie S, Woods J, Jones L. The subjective response to verofilcon A daily disposable contact lenses during extensive digital device use.
23. Miller J, Giedd B, Subbaraman LN. Clinical comparison of a silicone hydrogel and a conventional hydrogel daily disposable contact lens. Clin Ophthalmol. 2021;15:4339–4345. doi:10.2147/OPTH.S332651
24. Fogt JS, Patton K. Long day wear experience with water surface daily disposable contact lenses. Clin Optom. 2022;14:93–99. doi:10.2147/OPTO.S367891
25. Subbaraman L, Tucker B, Leveillee E, Bauman E Characterizing the surface properties of daily disposable contact lens materials.
26. Efron N. Blinking abnormalities. In: Contact Lens Complications. Elsevier Ltd; 2012:39–46. chap 4.
27. Luensmann D, Keir N, Richter D, Despres M, Woods C, Fonn D. In vivo wettability changes over 3 days using daily disposable contact lenses. Optomet Vis Sci. 2011;88:E–abstract 115384.
28. Efron N. Grading scales for contact lens complications. Ophthalmic Physiol Optics. 1998;18(2):182–186. doi:10.1046/j.1475-1313.2001.00575.x
29. Dumbleton K, Caffery B, Dogru M, et al. The TFOS international workshop on contact lens discomfort: report of the subcommittee on epidemiology. Invest Ophthalmol Vis Sci. 2013;54(11):TFOS20–TFOS36. doi:10.1167/iovs.13-13125
30. Tauste A, Ronda E, Molina M-J, Seguí M. Effect of contact lens use on computer vision syndrome. Ophthalmic Physiol Optics. 2016;36(2):112–119. doi:10.1111/opo.12275
31. Willcox MD, Zhao Z, Naduvilath T, Lazon de la Jara P. Cytokine changes in tears and relationship to contact lens discomfort. Mol Vis. 2015;21:293–305.
32. McMonnies CW. An amplifying cascade of contact lens-related end-of-day hyperaemia and dryness symptoms. Curr Eye Res. 2018;43(7):839–847. doi:10.1080/02713683.2018.1457163
33. Richdale K, Sinnott LT, Skadahl E, Nichols JJ. Frequency of and factors associated with contact lens dissatisfaction and discontinuation. Cornea. 2007;26(2):168–174. doi:10.1097/01.ico.0000248382.32143.86
34. Begley CG, Caffery B, Nichols KK, Chalmers R. Responses of contact lens wearers to a dry eye survey. Optom Vis Sci. 2000;77(1):40–46. doi:10.1097/00006324-200001000-00012
35. Chalmers R, Long B, Dillehay S, Begley C. Improving contact-lens related dryness symptoms with silicone hydrogel lenses. Optom Vis Sci. 2008;85(8):778–784. doi:10.1097/OPX.0b013e318181a90d
36. Schafer J, Steffen R, Reindel W, Chinn J. Evaluation of surface water characteristics of novel daily disposable contact lens materials, using refractive index shifts after wear. Clin Ophthalmol. 2015:1973–1979. doi:10.2147/OPTH.S90376
37. Abusharha AA. Changes in blink rate and ocular symptoms during different reading tasks. Clin Optom. 2017;9:133–138. doi:10.2147/OPTO.S142718
38. Al-Mohtaseb Z, Schachter S, Shen Lee B, Garlich J, Trattler W. The relationship between dry eye disease and digital screen use. Clin Ophthalmol. 2021;15:3811–3820. doi:10.2147/OPTH.S321591
39. Chu CA, Rosenfield M, Portello JK. Blink patterns: reading from a computer screen versus hard copy. Optom Vis Sci. 2014;91(3):297–302. doi:10.1097/OPX.0000000000000157
40. Koh S, Maeda N, Hori Y, et al. Effects of suppression of blinking on quality of vision in borderline cases of evaporative dry eye. Cornea. 2008;27(3):275–278. doi:10.1097/ICO.0b013e31815be9c8
41. Cardona G, Gómez M, Quevedo L, Gispets J. Effects of transient blur and VDT screen luminance changes on eyeblink rate. Contact Lens Anterior Eye. 2014;37(5):363–367. doi:10.1016/j.clae.2014.05.005
42. Guillon M, Dumbleton KA, Theodoratos P, et al. Association between contact lens discomfort and pre-lens tear film kinetics. Optom Vis Sci. 2016;93(8):881–891. doi:10.1097/OPX.0000000000000866
43. Thai LC, Tomlinson A, Doane MG. Effect of contact lens materials on tear physiology. Optom Vis Sci. 2004;81(3):194–204. doi:10.1097/00006324-200403000-00012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Wear Experience with Soft Daily Disposable Lenses for Astigmatism over 16 Hours of Wear
Fogt JS, Patton K
Clinical Optometry 2022, 14:207-214
Published Date: 28 October 2022
Real-Time Ocular Comfort Reporting in Monthly Replacement Contact Lens Wearers
Call T, Pucker AD, McGwin Jr G, Franklin QX, Logan A
Clinical Optometry 2023, 15:97-103
Published Date: 5 May 2023
Performance of Delefilcon A Daily Disposable Contact Lenses in a Group of Digital Device Users
Wong S, Woods J, Schulze MM, Fadel D, Stahl U, Jones L
Clinical Ophthalmology 2025, 19:2439-2452
Published Date: 25 July 2025
Subjective Grading and Objective Assessment After Switching to a Daily Disposable Silicone Hydrogel Contact Lens
Chen YY, Yang RY, Sun HY
Clinical Ophthalmology 2025, 19:3273-3281
Published Date: 6 September 2025