Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Real-Life Effectiveness of Aclidinium/Formoterol on COPD Control: The REDACT Observational Study
Authors Kostikas K ![]() , Loukides S
, Loukides S ![]() , Tzanakis N, Porpodis K, Tryfon S, Katsoulis K, Hillas G, Gioldasi I, Delicha E, Gogali A
, Tzanakis N, Porpodis K, Tryfon S, Katsoulis K, Hillas G, Gioldasi I, Delicha E, Gogali A ![]() , Miravitlles M
, Miravitlles M ![]()
Received 24 March 2026
Accepted for publication 14 June 2026
Published 26 June 2026 Volume 2026:21 611733
DOI https://doi.org/10.2147/COPD.S611733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Konstantinos Kostikas,1 Stylianos Loukides,2 Nikolaos Tzanakis,3 Konstantinos Porpodis,4 Stavros Tryfon,5 Konstantinos Katsoulis,6 Georgios Hillas,2 Ioanna Gioldasi,7 Evie Delicha,8 Athena Gogali,1 Marc Miravitlles9
1Respiratory Medicine Department, University of Ioannina, Ioannina, Greece; 2Second Respiratory Medicine Department, General University Hospital ‘Attikon’, Medical School, National and Kapodistrian University of Athens, Athens, Greece; 3Department of Respiratory Medicine, University Hospital of Heraklion, Medical School, University of Crete, Heraklion, Greece; 4Pulmonary Department, Aristotle University of Thessaloniki, G. Papanikolaou Hospital, Thessaloniki, Greece; 5Pulmonary Department (NHS), George Papanikolaou General Hospital of Thessaloniki, Thessaloniki, Greece; 6Pulmonary Department, 424 Army General Hospital, Thessaloniki, Greece; 7Pharmabide LTD, Athens, Greece; 8ASTAT, Athens, Greece; 9Pneumology Department Hospital Universitari Vall d’Hebron, Vall d’Hebron Institut de Recerca, Vall d’Hebron Hospital Campus, Barcelona, Spain
Correspondence: Konstantinos Kostikas, Respiratory Medicine Department, University of Ioannina, Ioannina, Greece, Email [email protected]
Background: COPD control evaluates changes in patients’ status based on clinical impact and stability. There are limited data on the effectiveness of dual bronchodilation on COPD control.
Methods: REDACT was a multicenter, prospective, single-arm, longitudinal real-life observational study that evaluated COPD control in uncontrolled COPD patients after 12 weeks of treatment with aclidinium/formoterol (Duaklir Genuair®). Eligible patients were previously receiving any inhaled medication except triple therapy (fixed or open combinations). The primary objective was to assess the proportion of patients who achieved COPD control after 12 weeks. Secondary aims included changes in COPD assessment test (CAT) and forced expiratory volume in 1 second (FEV1).
Results: A total of 1038 patients with uncontrolled COPD, mean age 68.9 years, 69.6% male, were recruited and 1014 (97.7%) completed follow-up. The proportion of patients who achieved COPD control at 12 weeks was 83.7% (95% CI 81.3 to 86.0%). Low baseline FEV1 (% pred), history of moderate/severe exacerbation in the past year and history of cardiovascular disease were predictors of lack of control. Change from baseline in FEV1 was 124.8 mL (95% CI 108.7 to 141.0 mL, p< 0.001) and in CAT score − 7.6 points (95% CI − 7.9 to 7.3 points, p< 0.001). Proportions of patients that achieved the minimally clinically important difference of +100 mL in FEV1 and − 2 points in the CAT score were 50.4% and 90.5%, respectively.
Conclusion: After 12 weeks of treatment with aclidinium/formoterol, a significant proportion of uncontrolled COPD patients achieved COPD control, with significant improvements in lung function and health status.
Keywords: COPD control, RADAR score, aclidinium, formoterol, LABA/LAMA combinations
Introduction
COPD is one of the leading causes of morbidity and mortality worldwide,1 and will continue affecting millions of people in the following decades.2 The prevalence of COPD in Greece is 8.4% in adults over 35 years, higher in men (11.6%) than women (4.8%).3 Many COPD patients have daily symptoms that are associated with airflow limitation severity, worse patient-reported outcomes and limited physical activity.4 In a recent study in Greece, 80% of COPD patients were symptomatic, with 59% classified as non-exacerbators and 21% as exacerbators, according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017.5 The recognition of clinical phenotypes has substantially shaped current approaches to COPD management, by allowing tailored treatment selection according to the dominant clinical features of the disease.6
Dual bronchodilator therapy with long-acting muscarinic antagonists (LAMA) and long-acting β2-agonists (LABA) is proposed in GOLD recommendations as initial first-line treatment in non-exacerbating symptomatic patients (GOLD B), and in those with any history of moderate/severe exacerbations (GOLD E), as well as step-up treatment from mono-bronchodilators in patients with persistent dyspnea.1 Other guidelines7,8 recommend the use of LAMA/LABA combinations as first line treatment in symptomatic low-risk patients and in high-risk non-exacerbators and non-eosinophilic exacerbators, with “high risk” assessment based on the presence of severe airflow limitation, clinically significant dyspnea and exacerbation history.8 Aclidinium/formoterol is a LAMA/LABA with a robust clinical body of evidence, both from randomized controlled trials9–12 and real-life studies13,14 in patients with COPD.
The 2026 GOLD update extensively highlights disease activity,1 suggesting to report disease stability15 and clinical control.16 COPD control is a composite measure of disease activity,16 since it has been shown to be a sensitive tool to evaluate changes in patients’ status within 3-month intervals in an international study of the Respiratory Effectiveness Group (REG).17 Patients with poor control were at higher risk of future exacerbations at 12 months in an analysis of the 64-week SPARK study.18 Moreover, as shown in a study from the CHAIN cohort, COPD control may provide prognostic information on survival.19 Recently, a new score derived from COPD control, the RADAR score (Rescue medication, Acute exacerbations, Dyspnea, physical Activity, and Risk) was able to predict clinical risk and health status, offering a practical tool to monitor COPD control and identify patients at risk.20 However, there is no data on the effectiveness of dual bronchodilation on COPD control in real-life.
The aim of this real-life observational study was to evaluate the change in COPD control status after 12 weeks of treatment with aclidinium/formoterol, as prescribed according to the decision of treating physicians in patients with uncontrolled moderate to very severe COPD in real-life settings. Secondary aims included the evaluation of changes in lung function and COPD health status.
Methods
The Real-life Effectiveness of Dual bronchodilation with Aclidinium/formoterol in COPD conTrol (REDACT) study was a 12-week, multicenter, observational study of two visits (baseline and at 12 weeks) that aimed to evaluate the impact of dual bronchodilation with aclidinium/formoterol (Duaklir Genuair®) on COPD control in a large cohort of Greek COPD patients. Additionally, we aimed to investigate the impact of dual bronchodilation on health status and spirometric values, as well as to evaluate the potential role of patient characteristics and comorbidities on COPD control.
The study was performed in accordance with the recommendations of the Declaration of Helsinki, the International Conference of Harmonisation–Good Clinical Practice (ICH-GCP) Guidelines, the EU-Directive 2001/20 and all national requirements, and was approved by the Institutional Review Board (IRB) of the University Hospital of Ioannina and all other major study centers. Written informed consent was obtained from all participants prior to inclusion in the study.
The decision for administration of aclidinium/formoterol was based on treating physicians’ judgment, before including patients in the study. The medication was delivered at the approved dose of 1 inhalation twice daily.
The study consisted of 2 visits: (1) Baseline Visit (Day 1) where informed consent was obtained and patients’ eligibility (including COPD control) and characteristics were recorded, followed by spirometry, assessment of health status and training on the appropriate use of the inhalation device and (2) Follow-up Visit at 12 weeks (Day 84 ± 7) where the above measurements except baseline characteristics were repeated, with additional evaluation of adherence to treatment and potential adverse effects of the study treatment.
Patient Population
We recruited patients diagnosed with COPD, considered as eligible for treatment with aclidinium/formoterol by their treating physician. Eligible patients were of at least 40 years of age, current or ex-smokers with a smoking history of ≥10 pack-years, with established diagnosis of COPD at least for 1 year, without COPD control at baseline,21 receiving previously any inhaled medication except triple therapy [LAMA + LABA + inhaled corticosteroid (ICS), fixed or open combinations], with a recent initiation with aclidinium/formoterol for no more than one week. Exclusion criteria included a diagnosis of asthma or asthma-COPD overlap, bronchiectasis, or other chronic respiratory disease different from COPD, history of COPD exacerbation or lower respiratory tract infection in the previous 6 weeks, treatment with triple therapy (LAMA+LABA+ICS, fixed or open combinations), any acute or chronic condition that could limit patients’ ability to complete questionnaires or participate in this study, participation in another study and inability to give informed consent.
Endpoints
The primary endpoint of the study was to determine the proportion of patients who achieved COPD Control after 12 weeks of treatment with aclidinium/formoterol compared to baseline.
Secondary endpoints included the change in forced expiratory volume in 1 second (FEV1, in L/mL) at 12 weeks compared to baseline, the change in the chronic airways assessment test (CAAT – previously CAT) score at 12 weeks compared to baseline, the proportion of patients achieving the minimally clinically important difference (MCID) of 100 mL in FEV1 and 2 points in the CAAT score at 12 weeks compared to baseline, and analysis of the baseline characteristics (including previous treatments) that may predict the achievement of COPD Control at 12 weeks, assessment of the adherence to treatment with aclidinium/formoterol and its safety during follow-up.
Assessments
COPD Control
The concept of COPD control is based on the evaluation of clinical stability and the impact of the disease to patients.21,22 Stability is based on history of exacerbations in the previous 3 months, whereas impact is based on dyspnea, mucus production, use of rescue medication and physical activity. A detailed evaluation of COPD control is presented in Table 1 (from reference23). Due to the recent publication of the development and validation of the RADAR score derived from COPD control, presented in Table 2 (from reference20), we have performed an additional post-hoc analysis to evaluate this score at baseline and at 12 weeks on dual bronchodilation. Briefly, patients with score 0–1 presented good control, 2–3 partial control, and ≥4 poor control.20
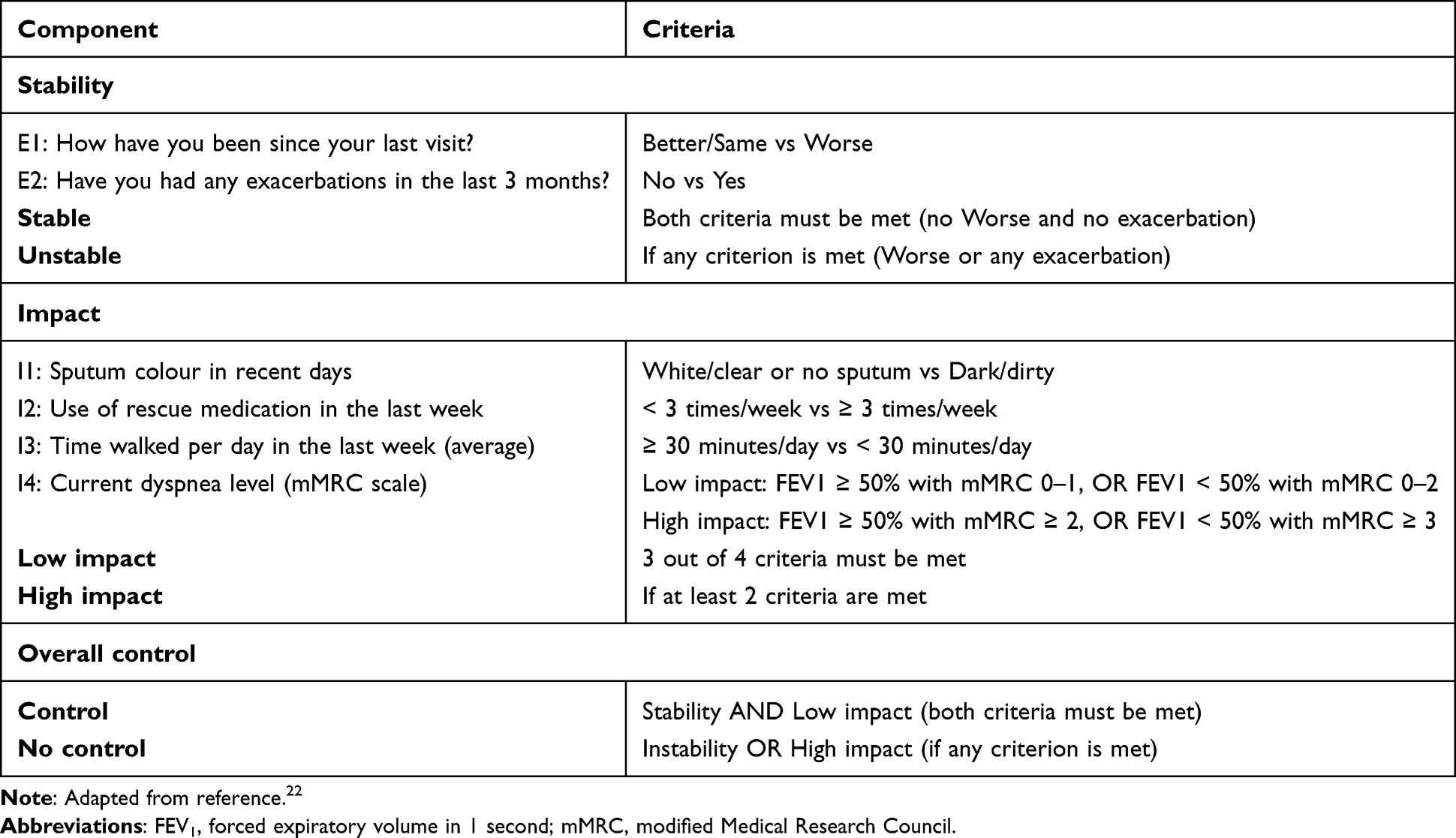 |
Table 1 COPD Clinical Control Questionnaire |
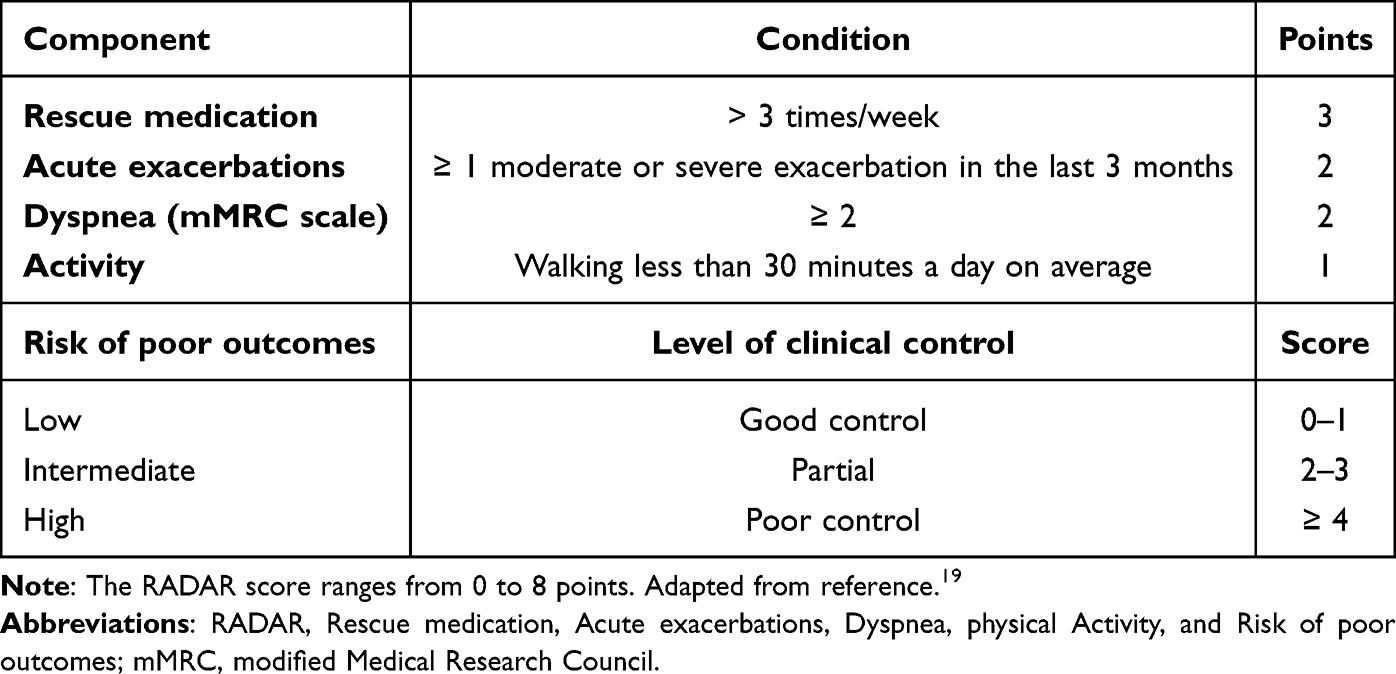 |
Table 2 The RADAR Score for Quantitative Assessment of Clinical Control |
Chronic Airways Assessment Test (CAAT) - Previously COPD Assessment Test (CAT)
This is a patient-completed questionnaire assessing the impact of COPD on patients’ health status. The total score ranges from 0 to 40, and higher scores denote a more severe impact.24 The MCID of CAAT is 2 points.25
Lung Function Testing
Spirometry was performed as per usual clinical practice at each center, and the values of FEV1 (% pred. and in L), forced vital capacity (FVC, % pred. and in L) and their FEV1/FVC ratio will be recorded. The MCID for FEV1 is 100 mL.26
Assessment of Comorbidities
Comorbidities were recorded as reported by the patient. The comorbidities specifically recorded were: hypertension, cardiovascular disease (ischemic heart disease, arrhythmias, heart failure, peripheral vascular disease, and stroke), diabetes mellitus, hyperlipidemia/dyslipidemia, osteoporosis, gastroesophageal reflux disease (GERD) and anxiety and/or depression.
Statistical Analysis
Continuous variables are summarized using descriptive statistical measures (mean, median, standard deviation), while categorical variables are reported as n (%). The primary endpoint [proportion of patients who achieve COPD Control after 12 weeks of treatment with aclidinium/formoterol is followed by the corresponding 95% confidence intervals (CI). Changes in FEV1 (in mL) and CAAT score at 12 weeks compared to baseline are summarized using descriptive statistics. Linear regression models were fitted with dependent variables, the changes from baseline in FEV1 or CAAT and independent factors demographic, baseline characteristics, previous treatments and comorbidities. The number and the proportion of patients achieving the MCID of 100 mL in FEV1 and 2 points in the CAAT score at 12 weeks compared to baseline were provided followed by the corresponding 95% CI. To evaluate predictors of COPD control at 12 weeks, a binomial logistic regression model was fitted with dependent variable the COPD control at 12 weeks and as independent variables the baseline and other clinical characteristics, previous treatments and presence of comorbidities. All tests were 2-sided using alpha = 0.05 level of significance. All analyses have been performed in R version 4.5.0 (R Foundation for Statistical Computing, Vienna, Austria).
The target sample size was calculated for the primary endpoint, defined as the proportion of patients achieving COPD control after 12 weeks of treatment with aclidinium/formoterol. The null reference proportion was set at 20%, based on the proportion of patients classified as controlled at weeks 1–12 in the SPARK study population, where the prospective value of the COPD control concept was validated.18 An expected proportion of 25% achieving COPD control at 12 weeks was hypothesised in the present cohort of previously uncontrolled patients receiving dual bronchodilation with aclidinium/formoterol. Using a one-sample test of proportions with a two-sided significance level of 0.05 and a statistical power of 90%, approximately 800 evaluable patients were required to detect this 5 percentage-point difference. Accounting for an anticipated drop-out rate of 20%, a target enrolment of approximately 1000 patients was set.
Results
The study was conducted in respiratory medicine departments of 16 hospitals with the contribution of 60 office-based pulmonologists. A total of 1038 patients were recruited, of whom 1014 (97.7%) completed the study. The flow chart of study participants is presented in Figure 1. Demographics and baseline characteristics of the study participants are presented in Table 3.
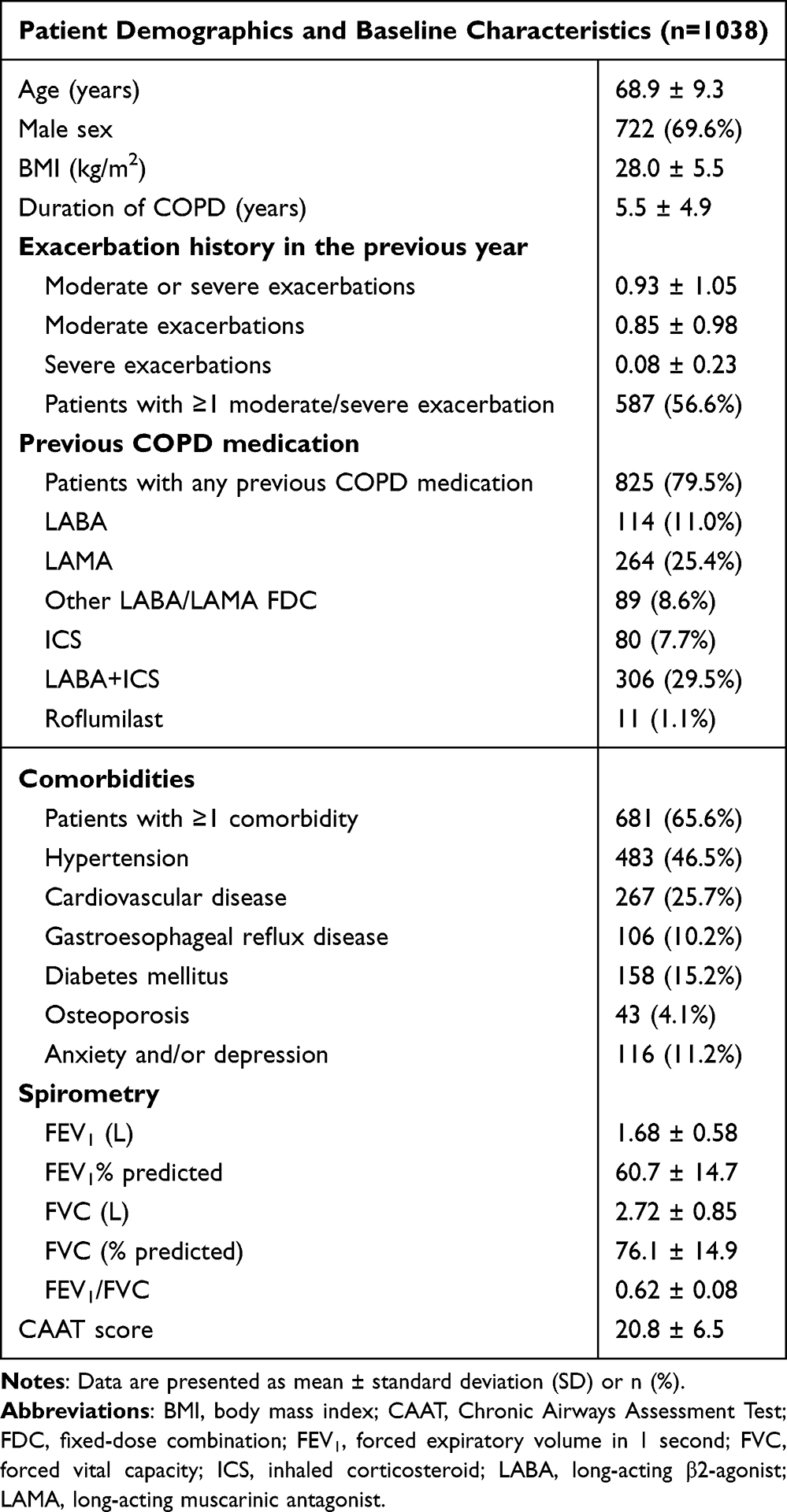 |
Table 3 Demographics and Baseline Characteristics of Study Participants |
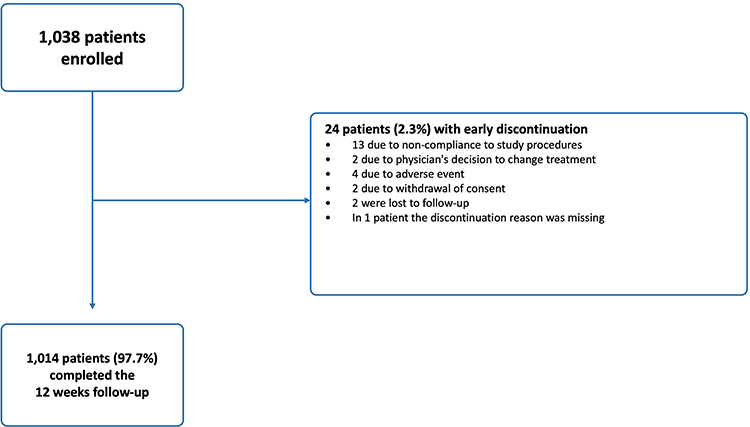 |
Figure 1 Flow chart of study participants. |
COPD Control at Week 12 (Primary Endpoint)
At baseline, all patients enrolled (n=1038) were uncontrolled, as per the inclusion criteria. At the follow-up visit (week 12), 849 of 1014 patients who completed the follow-up achieved COPD control (83.7%) (Figure 2A). Of the uncontrolled patients at 12 weeks, 40 (3.9%) were unstable (33 or 3.3% due to exacerbations), and 156 (15.4%) presented high impact of their disease.
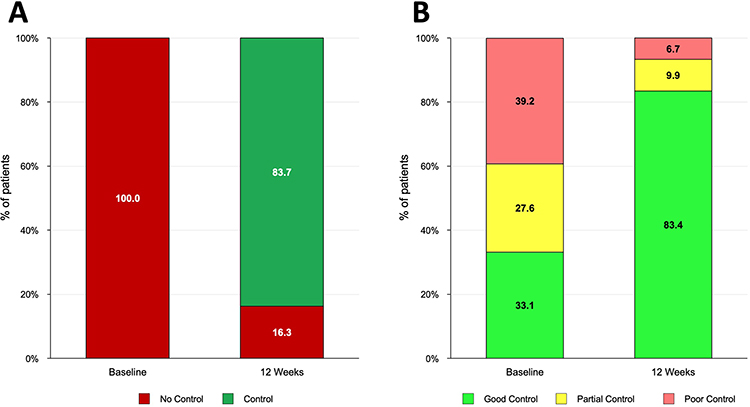 |
Figure 2 Patient status at baseline and after 12 weeks of treatment with Aclidinium/formoterol. (A) Patient status according to COPD control. (B) Patient status according to the RADAR score (Rescue medication, Acute exacerbations, Dyspnea, physical Activity, and Risk of poor outcomes). Numbers represent % of total patients (n=1038 at baseline and n=1014 at 12 weeks). |
A multivariate logistic regression analysis was performed to baseline identify statistically significant independent predictors of achieving COPD control. Baseline characteristics that were independent predictors of lack of COPD control at week 12 were low baseline FEV1 (% pred), the presence of any moderate/severe exacerbation in the past year and a history of cardiovascular disease (Table 4). Specifically, patients who had any moderate/severe exacerbation in the past year were 55% less likely to achieve COPD control, and the presence of cardiovascular disease was associated with 43% lower odds of achieving COPD control. In addition, for each 1% increase in FEV1, the odds of achieving COPD control increased by 4%.
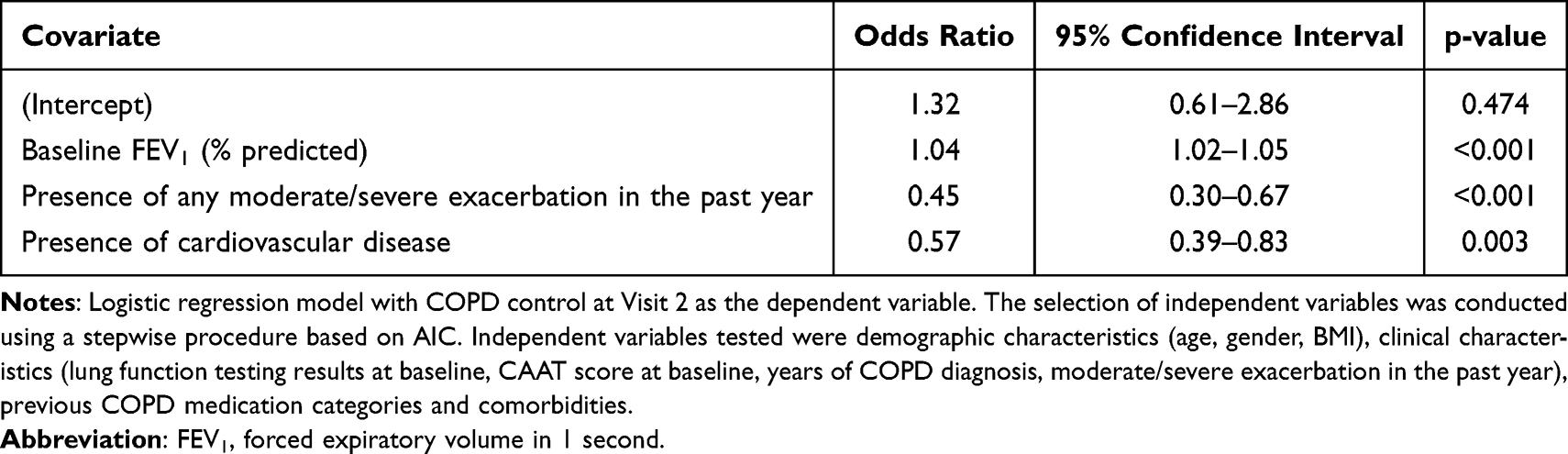 |
Table 4 Multivariate Logistic Regression Analysis of Independent Predictors of COPD Control |
In a post-hoc analysis, using the recently published RADAR score, at baseline 344 patients (33.1%) had good control, 287 (27.6%) had partial control, and 407 (39.2%) patients had poor control. At the follow-up visit (week 12), 846 patients (83.4%) had had good control, 100 (9.9%) had partial control, and only 68 (6.7%) patients had poor control (Figure 2B).
Secondary Outcomes
In patients with available spirometries at both visits (n=926), we observed a statistically significant and clinically relevant improvement in FEV1 at week 12 of 124.8 mL (95% CI 108.7 to 141.0) (p<0.001), that corresponded to a mean improvement in FEV1% predicted of 4.7%. A total of 467 (50.4%, 85% CI 47.2 to 53.7%) achieved the MCID of 100 mL. We also observed a mean increase in FVC of 110.1 mL (p<0.001).
In patients with data at the follow-up visit (n=1014), we observed a statistically significant and clinically relevant adjusted mean change in CAAT score at 12 weeks from baseline of −7.6 points (95% CI: −7.9 to −7.3, p<0.001). The proportion of patients achieving the minimally clinically important difference of −2 points in CAAT score was 90.5% (918/1014, 95% CI: 88.6% to 92.3%).
Adherence to treatment with aclidinium/formoterol (as evaluated by the electronic prescription system and the counters of the inhalers) was 95.8%.
Safety Outcomes
Four patients (4/1038, 0.4%) experienced treatment emergent adverse events (TEAEs), 3 of whom (3/1038, 0.3%) experienced serious TEAEs (palpitations, tachycardia and dyspnoea). Four patients (4/1038, 0.4%) discontinued due to adverse events.
Discussion
In this 12-week observational study including more than 1000 patients with uncontrolled COPD who received dual bronchodilation with aclidinium/formoterol, we observed achievement of COPD control in 83.7% of the patients, accompanied by clinically relevant improvements in lung function and health status. Patients with better lung function had a higher probability to achieve control, whereas those with a history of exacerbations in the previous year or a history of cardiovascular disease were less likely to reach control status. In a post-hoc analysis using the recently published RADAR score, we showed a significant shift towards good control. The REDACT study is, to the best of our knowledge the first large study to evaluate change in COPD control as a primary outcome in patients receiving dual bronchodilation therapy.
The high proportion (83.7%) of patients achieving COPD control after 12 weeks of dual bronchodilation is particularly noteworthy when compared with previous observational studies evaluating clinical control.16,21 A significant difference of the REDACT study was that it included intervention with a dual bronchodilator, while previous COPD control trials involved only observation of patients on standard treatment. An earlier analysis from the REG cohort study reported more modest transitions toward controlled status over time; however, uncontrolled patients at baseline presented higher risk of exacerbations at follow-up.17 In contrast, REDACT specifically enrolled uncontrolled patients and demonstrated a rapid shift toward stability and low impact within 3 months of treatment with dual bronchodilation. Interestingly, most uncontrolled patients were due to high symptomatic impact of their disease and only few (3.3%) presented with an exacerbation, possibly due to the 12-week study duration. This magnitude of improvement likely reflects both the high symptomatic burden of uncontrolled patients and the effectiveness of dual bronchodilation in symptomatic patients.
The post-hoc analysis on the recent RADAR score further strengthens our findings. According to the recent validation study by Soler-Cataluña et al,20 the RADAR score effectively stratifies patients according to clinical risk and future adverse outcomes. In that cohort, a considerable proportion of patients were categorized as partial or poor control, particularly among those with frequent exacerbations. In REDACT, the shift from 66.8% of patients with poor or partial control at baseline to only 16.6% of poor or partial control at 12 weeks represents a clinically meaningful redistribution of a large number of patients towards lower risk status. Our results extend RADAR validation, by demonstrating longitudinal responsiveness to dual bronchodilation, suggesting that the score may not only have a prognostic role, but may also be suitable for the evaluation of treatment effectiveness in real-life.
The improvement in FEV1 of 124 mL is consistent with, and in some cases exceeds, improvements reported in randomized control trials and in other real-world LABA/LAMA studies. In the DETECT study that evaluated various dual bronchodilators, FEV1 improvements ranged between 60–120 mL depending on baseline lung function and prior treatment exposure.14 The improvement in FEV1% predicted in REDACT (4.7%) was slightly larger than that reported with dual bronchodilation in the Greek DANICO study (3.2%), possibly reflecting the effectiveness of LABA/LAMA in this population of uncontrolled patients.13 Moreover, randomized controlled trials, such as the AMPLIFY trial, demonstrated improvements with aclidinium/formoterol of approximately 84 mL versus each of its monocomponents.12 Notably, more than half of our patients achieved the MCID of 100 mL, demonstrating the clinical relevance of the management with aclidinium/formoterol.
The mean reduction of −7.6 points in CAAT score is substantially above the MCID of −2 points. This improvement is numerically greater than those reported in several real-world LABA/LAMA studies, where reductions typically range between 3 and 7 points.13,14 The high proportion of responders (90.5% achieving MCID) may reflect the high baseline symptom burden (mean CAAT 20.7) of our uncontrolled patients, supporting the concept that symptomatic patients may benefit more from optimized bronchodilation. Moreover, our findings confirm that dual bronchodilation produces clinically meaningful improvements in health status, and together with achieving clinical control may address multiple components of the disease, besides the improvement in lung function.27
A subgroup of 89 patients (8.6%) was already receiving a LABA/LAMA combination at baseline and was switched to aclidinium/formoterol. The improvement observed in this subgroup is most plausibly explained by a change in the inhaler device and/or the specific LABA/LAMA molecule, rather than by a step-up of pharmacological class. This is consistent with previous evidence demonstrating that switching the inhalation device or the molecule in symptomatic patients can result in clinically meaningful improvements in disease control without a change in therapeutic class.28 In our cohort, treating physicians may have preferred a switch within the LABA/LAMA class over an escalation to triple therapy in patients without frequent exacerbations or elevated eosinophils, in line with current recommendations for ICS-sparing strategies in non-eosinophilic disease.29 The observed improvement in this subgroup may therefore reflect a combination of better device handling and adherence with the device and the specific pharmacological properties of aclidinium/formoterol.
From a phenotypic perspective, the heterogeneity of bronchodilator response in COPD has long been recognised, with reversible and non-reversible airflow obstruction phenotypes carrying different therapeutic implications.30 The magnitude of the FEV1 improvement observed in REDACT (mean 124.8 mL; 50.4% of patients achieving the 100 mL MCID) is consistent with a substantial proportion of patients carrying a reversible/bronchodilator-responsive phenotype. At the same time, the parallel improvement in CAAT score and COPD control achieved across the cohort, including in patients without a large FEV1 increase, indicates that the benefit of dual bronchodilation extends beyond the bronchodilator-responsive phenotype.
Our study presents some limitations. First, the single-arm observational design cannot control for potential biases in patient reported outcomes. Moreover, we included only uncontrolled patients, thus regression to the mean cannot be fully excluded. However, the large study population involving over 1000 patients with high treatment adherence, where we showed contemporaneous improvement in lung function, partially validates the reported improvement in COPD control and health status. Second, spirometry was performed according to routine practice, which may have introduced some variability; nevertheless, all centers involved had previous experience in the conduct of spirometry studies. Third, the analysis on the RADAR score was not predefined, and therefore does not allow us to draw firm conclusions on this endpoint. Fourth, the mean duration of COPD in the included patients was a little over 5 years, and this may represent a bias due to the inclusion of earlier stage patients. However, it should be interpreted in the context of the real-life study design and Greek real-world practice, as the inclusion of patients was purely the treating physicians’ decision, and we did not impose any upper limit on disease duration. In the same context, patients with severe, longstanding, triple-therapy-treated COPD were under-represented and that our findings are most directly applicable to symptomatic, uncontrolled patients eligible for dual bronchodilation. Finally, the relatively short follow-up of 12 weeks does not allow for conclusions regarding long-term sustainability of control and exacerbation prevention. The very small number of patients with an exacerbation event during these 12 weeks (33 or 3.3%) compared to 587 (56.6%) in the previous year further supports exacerbation prevention by dual bronchodilation in symptomatic patients.31 Although a parallel comparator group was not included, indirect comparison with previously published cohorts of uncontrolled COPD patients, in which spontaneous transitions to controlled status were substantially smaller over comparable time periods, supports an intervention effect over and above natural variation or regression to the mean.17,18 Future studies could consider analytical approaches such as propensity-matched historical controls or pragmatic randomized trials of LABA/LAMA combinations versus continued previous therapy in uncontrolled COPD patients to further strengthen causal inference. Additionally, longitudinal studies should evaluate whether improvements in COPD control and RADAR score translate into sustained reductions in exacerbations and long-term clinical outcomes.
In conclusion, REDACT is the first study to demonstrate that effective dual bronchodilation with aclidinium/formoterol is associated with rapid and clinically meaningful improvement in COPD control, in a large real-life cohort of previously uncontrolled patients. This improvement was consistently observed with improvements in the novel recently published RADAR score. Improvements in lung function and health status were observed in parallel with the improvement of clinical control and were consistent those observed in randomized trials and other real-life studies. These findings support the integration of COPD control, and potentially the novel RADAR score, into routine clinical practice while reinforcing the central role of dual bronchodilation for the management of appropriate uncontrolled patients.
Acknowledgment
The REDACT study has been presented at the European Respiratory Society (ERS) congress and the abstract of the paper is available at: https://doi.org/10.1183/13993003.congress-2025.PA5690. The authors would like to acknowledge the important contribution of the following respiratory physicians to the study: Nikolaos Aggelis, Anastasios Anagnostopoulos, Georgios Androutsopoulos, Athina Antonopoulou, Kyriaki Asimomyti, Petros Bakakos, Christos Bampalis, Konstantinos Bartziokas, Vanesa Bellou, Afroditi Boutou, Nikolaos Chainis, Eleni Chamerzokova-Iliadi, Panagiotis Chinelis, Konstantinos Charitopoulos, Konstantinos Christou, Christos Chronis, Damianos Damianakos, Georgios Efraimidis, Christoforos Efthymiou, Angeliki Florou, Konstantinos Fragkos, Eleni Gaki, Ioannis Giannarakis, Evangelos Giannoulis, Eirini Gerogianni, Konstantinos Gourgoulianis, Gavriil Isaakidis, Paschalis Kakavelas, Maria Kallieri, Panagiota Karydi, Charalambos Kerasiotis, Michalis Kovaios, Georgia Kotantoula, Andreas Koulelidis, Georgios Krommydas, Christos Kyriakopoulos, Zacharoula Kyriakaki, Dimitrios Latsios, Christina Leontaridi, Emmanouil Manos, Nikos Maniakos, Miltiadis Markatos, Nikolaos Mousiadis, Andreas Ntanasis, Christos Ntochas, Andriana Papaioannou, Dimosthenis Papapetrou, Georgios Patentelakis, Asimina Paspala, Konstantinos Porpodis, Ioannis Roussis, Despoina Saatzoglou, Anastasia Samakovli, Konstantinos Samitas, Sofia Schiza, Marianna Siganaki, Alexandra Sistou, Anna Maria Sosi, Paschalis Steiropoulos, Violeta Talou, Elpida Theodorakopoulou, Chrysoula Trampari, Christos Tzolidis, Maria-Ypatia Tsopela, Drosos Tsavlis, Argyris Tzouvelekis, Kamelia Vasileskou, Georgios Violatos, Michalis Volonakis, Stelios Vittorakis, Stavros Vogiatzis, Grigorios Voudrislis, Garyfallia Vlachou, Areti Xyfteri, Eleftherios Zervas, Nikolaos Zias, Panagiotis Zois.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The study was funded by Specialty Therapeutics.
Disclosure
Konstantinos Kostikas has received honoraria for presentations and/or consultancy fees from AstraZeneca, Berlin-Chemie, Boehringer Ingelheim, Chiesi, ELPEN, GSK, Guidotti, Menarini, Pfizer, Sanofi, and Specialty Therapeutics; his department has received funding and/or grants for my Department from AstraZeneca, Boehringer Ingelheim, Berlin-Chemie, Chiesi, ELPEN, GSK, Guidotti, and Menarini; he worked as Global Medical Head Respiratory Biologics AstraZeneca (02.09.2024 to 29.11.2024). Stylianos Loukides has received speaker and advisory fees from Chiesi, Menarini, Guidotti, GSK, Elpen, Astra Zeneca and Sanofi. Nikolaos Tzanakis has received honoraria for presentations and/or consultancy fees from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, Guidotti, Menarini, Pfizer, Sanofi, Gilead, MSD and Specialty Therapeutics; his department has received funding and/or grants from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, and Menarini. He is the vice president of Hellenic Respiratory Society. Konstantinos Porpodis has received grants from GSK; consulting fees from AstraZeneca, Boehringer, Chiesi, ELPEN, GSK, Guidotti, Menarini, Novartis, Sanofi; honoraria from AstraZeneca, Chiesi, CSL Behring, ELPEN, GSK, Guidotti, Menarini, Novartis, Pfizer, Sanofi; support for attending meetings from AstraZeneca, Chiesi, ELPEN, Innovis, GSK, Guidotti, Menarini, Sanofi. Stavros Tryfon has received honoraria for presentations from AstraZeneca, Chiesi, GSK, ELPEN, Menarini, Specialty Therapeutics and support for attending meetings from AstraZeneca, Chiesi, GSK, ELPEN, Menarini. Konstantinos Katsoulis has received honoraria for presentations and/or consultancy fees from Astra Zeneca, Chiesi, Menarini, GSK, Guidotti, Specialty Therapeutics and Boehringer Ingelheim. Georgios Hillas has received consulting fees from AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, ELPEN, GSK, Guidotti, Menarini, Novartis, Pharmathen, Sanofi and Specialty Therapeutics; honoraria from AstraZeneca, Alector Pharmaceuticals, Boehringer Ingelheim, Chiesi, CSL Behring, ELPEN, Innovis, GILEAD, GSK, Menarini, Novartis, Pharmathen, Sanofi, Specialty Therapeutics, and UCB; support for attending meetings from AstraZeneca, Boehringer Ingelheim, Chiesi, Elpen, Innovis, GSK, Menarini and Novartis. Evie Delicha has received consultancy fees from Specialty Therapeutics. Athena Gogali has received honoraria for presentations and/or consultancy fees from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, Guidotti, Menarini, Pfizer, Guidotti, Vicore Pharma. Marc Miravitlles has received speaker fees from AstraZeneca, Boehringer Ingelheim, Bial, Chiesi, Cipla, GlaxoSmithKline, Menarini, Kamada, Takeda, Zambon, Tabuk Pharmaceuticals, CSL Behring, Specialty Therapeutics, Sanofi/Regeneron and Grifols; consulting fees from AstraZeneca, AIRNA, Atriva Therapeutics, BEAM Therapeutics, GondolaBio, Chiesi, GlaxoSmithKline, CSL Behring, Korrobio, Menarini, Mereo Biopharma, Specialty Therapeutics, Takeda, Novo Nordisk, Roche, Sanofi/Regeneron, Zambon, Zentiva and Grifols; and research grants from Grifols. The authors report no other conflicts of interest in this work.
References
1. 2026 GOLD Report and Pocket Guide. Global Initiative for Chronic Obstructive Lung Disease-GOLD. 2025. Available from: https://goldcopd.org/2026-gold-report-and-pocket-guide/.
2. Boers E, Barrett M, Su JG, et al. Global Burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
3. Tzanakis N, Anagnostopoulou U, Filaditaki V, Christaki P, Siafakas N; COPD group of the Hellenic Thoracic Society. Prevalence of COPD in Greece. Chest. 2004;125(3):892–11. doi:10.1378/chest.125.3.892
4. Miravitlles M, Worth H, Soler Cataluña JJ, et al. Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: results from the ASSESS study. Respir Res. 2014;15(1):122. doi:10.1186/s12931-014-0122-1
5. Tzanakis N, Koulouris N, Dimakou K, et al. Classification of COPD patients and compliance to recommended treatment in Greece according to GOLD 2017 report: the RELICO study. BMC Pulm Med. 2021;21(1):216. doi:10.1186/s12890-021-01576-6
6. Turner AM, Tamasi L, Schleich F, et al. Clinically relevant subgroups in COPD and asthma. Eur Respir Rev. 2015;24(136):283–298. doi:10.1183/16000617.00009014
7. Tzanakis N, Kosmas E, Papaioannou AI, et al. Greek guidelines for the management of COPD, a proposal of a holistic approach based on the needs of the Greek community. J Pers Med. 2022;12(12):1997. doi:10.3390/jpm12121997
8. Miravitlles M, Calle M, Molina J, et al. Update 2025 of the Spanish COPD Guidelines (GesEPOC): pharmacological treatment of stable COPD. Arch Bronconeumol. 2025;61(12):766–782. doi:10.1016/j.arbres.2025.10.008
9. Vogelmeier C, Paggiaro PL, Dorca J, et al. Efficacy and safety of Aclidinium/formoterol versus salmeterol/fluticasone: a Phase 3 COPD study. Eur Respir J. 2016;48(4):1030–1039. doi:10.1183/13993003.00216-2016
10. Bateman ED, Chapman KR, Singh D, et al. Aclidinium bromide and formoterol fumarate as a fixed-dose combination in COPD: pooled analysis of symptoms and exacerbations from two six-month, multicentre, randomised studies (ACLIFORM and AUGMENT). Respir Res. 2015;16(1):92. doi:10.1186/s12931-015-0250-2
11. Donohue JF, Soong W, Wu X, Shrestha P, Lei A. Long-term safety of Aclidinium bromide/formoterol fumarate fixed-dose combination: results of a randomized 1-year trial in patients with COPD. Respir Med. 2016;116:41–48. doi:10.1016/j.rmed.2016.05.007
12. Sethi S, Kerwin E, Watz H, et al. AMPLIFY: a randomized, Phase III study evaluating the efficacy and safety of Aclidinium/formoterol vs monocomponents and tiotropium in patients with moderate-to-very severe symptomatic COPD. Int J Chron Obstruct Pulmon Dis. 2019;14:667–682. doi:10.2147/COPD.S189138
13. Kostikas K, Dimakou K, Gourgoulianis K, et al. A real-world study on the day and night-time symptoms among Greek COPD patients who recently initiated treatment with dual Bronchodilation: the DANICO Study. COPD. 2022;17:2027–2041. doi:10.2147/COPD.S367553
14. Plate T, Friedrich FW, Beier J. Effectiveness and tolerability of LABA/LAMA fixed-dose combinations Aclidinium/formoterol, glycopyrronium/indacaterol and umeclidinium/vilanterol in the treatment of COPD in daily practice - results of the non-interventional DETECT study. Int J Chron Obstruct Pulmon Dis. 2020;15:1335–1347. doi:10.2147/COPD.S252354
15. Singh D, Han MK, Bhatt SP, et al. Is disease stability an attainable chronic obstructive pulmonary disease treatment goal? Am J Respir Crit Care Med. 2025;211(3):452–463. doi:10.1164/rccm.202406-1254CI
16. Soler-Cataluña JJ, Marzo M, Catalán P, Miralles C, Alcazar B, Miravitlles M. Validation of clinical control in COPD as a new tool for optimizing treatment. Int J Chron Obstruct Pulmon Dis. 2018;13:3719–3731. doi:10.2147/COPD.S178149
17. Miravitlles M, Sliwinski P, Rhee CK, et al. Changes in control status of COPD over time and their consequences: a prospective international study. Arch Bronconeumol. 2021;57(2):122–129. doi:10.1016/j.arbres.2020.06.003
18. Barrecheguren M, Kostikas K, Mezzi K, et al. COPD clinical control as a predictor of future exacerbations: concept validation in the SPARK study population. Thorax. 2020;75(4):351–353. doi:10.1136/thoraxjnl-2018-212752
19. Rubio C, Hermosa R, De Torres JL. COPD clinical control: predictors and long-term follow-up of the CHAIN cohort. Respir Res. 2021;22(1).
20. Soler-Cataluña JJ, Villagrasa M, Catalán P, Alcázar-Navarrete B, Calle Rubio M, Miravitlles M. Risk validation of a new quantitative score for clinical control of chronic obstructive pulmonary disease: the RADAR score. Arch Bronconeumol. 2026;62(1):28–34. doi:10.1016/j.arbres.2025.06.003
21. Soler-Cataluña J, Alcázar-Navarrete J, Miravitlles B. The concept of control in COPD: a new proposal for optimising therapy. Eur Respir J. 2014;44(4):1072–1075. doi:10.1183/09031936.00064414
22. Soler-Cataluña JJ, Alcázar-Navarrete B, Miravitlles M. The concept of control of COPD in clinical practice. Int J Chron Obstruct Pulmon Dis. 2014;9:1397–1405. doi:10.2147/COPD.S71370
23. Miravitlles M, Calle M, Molina J, et al. [Translated article] Spanish COPD guidelines (GesEPOC) 2021: updated pharmacological treatment of stable COPD. Arch Bronconeumol. 2022;58(1):T69–T81. doi:10.1016/j.arbres.2021.03.026
24. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
25. Kon SSC, Canavan JL, Jones SE, et al. Minimum clinically important difference for the COPD Assessment Test: a prospective analysis. Lancet Respir Med. 2014;2(3):195–203. doi:10.1016/S2213-2600(14)70001-3
26. Donohue JF. Minimal clinically important differences in COPD lung function. COPD. 2005;2(1):111–124. doi:10.1081/COPD-200053377
27. Kostikas K, Greulich T, Mackay AJ, et al. Treatment response in COPD: does FEV1 say it all? A post hoc analysis of the CRYSTAL study. ERJ Open Res. 2019;5(1):00243–02018. doi:10.1183/23120541.00243-2018
28. Tamási L, Bartha A, Ferencz A, et al. Effectiveness and treatment compliance of salmeterol-fluticasone Easyhaler® among patients with asthma, COPD, or asthma-COPD overlap syndrome: real-world study findings. Pulm Ther. 2022;8(4):369–384. doi:10.1007/s41030-022-00201-z
29. Hillas G, Gogali A, Loukides S, Kostikas K. GOLD 2026 report: what is new and what is noteworthy for the practicing clinician. COPD. 2026;23(1):2622744. doi:10.1080/15412555.2026.2622744
30. Hizawa N. Clinical approaches to discovering asthma-related and chronic obstructive pulmonary disease-related phenotypes. Int J Chron Obstruct Pulmon Dis. 2016;11:543–550. doi:10.2147/COPD.S100850
31. Beeh KM, Burgel PR, Franssen FME, et al. How do dual long-acting bronchodilators prevent exacerbations of chronic obstructive pulmonary disease? Am J Respir Crit Care Med. 2017;196(2):139–149. doi:10.1164/rccm.201609-1794CI
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.