Back to Journals » Advances in Medical Education and Practice » Volume 14
Readiness for Interprofessional Learning Among Students of Four Undergraduate Health Professions Education Programs
Authors Atwa H ![]() , Abouzeid E, Hassan N, Abdel Nasser A
, Abouzeid E, Hassan N, Abdel Nasser A ![]()
Received 12 January 2023
Accepted for publication 3 March 2023
Published 11 March 2023 Volume 2023:14 Pages 215—223
DOI https://doi.org/10.2147/AMEP.S402730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Hani Atwa,1,2 Enjy Abouzeid,2,3 Nahla Hassan,2 Asmaa Abdel Nasser2,4
1Medical Education Department, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Kingdom of Bahrain; 2Medical Education Department, Faculty of Medicine, Suez Canal University, Ismailia, Egypt; 3Faculty of Medicine, Ulster University, Londonderry, UK; 4Health Professions Education Center, Ibn Sina National College for Medical Studies, Jeddah, Saudi Arabia
Correspondence: Hani Atwa, Medical Education Department, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Kingdom of Bahrain, Tel +97335635809, Email [email protected]; [email protected]
Background: In interprofessional learning, students from different professions learn about, from, and with each other so that they can collaborate effectively, deliver high-quality healthcare, and achieve positive health outcomes. This study aimed to explore the readiness of students from four health professions education programs for interprofessional learning.
Methods: A cross-sectional descriptive study was carried out on 339 students. The Readiness for Interprofessional Learning Scale (RIPLS) was used to collect data. Descriptive statistics were used. Paired-samples t-test and ANOVA test were used to compare the responses of participants. Correlations between dependent and independent variables were explored by Pearson’s correlation test. The statistical significance level was set at p < 0.05.
Results: The reliability study of the collected data showed excellent internal consistency (Cronbach’s ɑ = 0.819). Results revealed a statistically significant difference between the responses of students from the four programs regarding the “Roles and Responsibilities” subscale (p = 0.000). A statistically significant difference between male and female students regarding two statements within the “Teamwork and Collaboration” subscale and one statement within the “Negative Professional Identity” subscale (p < 0.05) was also detected. The correlation study showed a weak but statistically significant correlation between RIPLS mean scores and the students’ study program (p < 0.015).
Conclusion: In conclusion, the students showed readiness for IPL as evidenced by their positive perception of the interprofessional learning concepts.
Keywords: RIPLS, interprofessional learning, health professions students, readiness for interprofessional learning
Introduction
In interprofessional learning (IPL), students from different professions learn about, from, and with each other so that they can collaborate effectively, deliver high-quality healthcare, and achieve positive health outcomes.1,2 Learning together improves collaborative working in the future, which is the rationale behind IPL. The rationale for IPL is that learning together enhances future collaborative working together.3 IPL is driven by evolving models of healthcare delivery within an aging population context and the rising prevalence of chronic health problems, as well as patient safety issues.4 The delivery of complex healthcare requires a team-based and collaborative approach.4,5 Improvements in patient outcomes, patient safety, and quality of healthcare have been linked to interprofessional education and practice.6
Emphasizing IPL was proposed as an effective way of preparing medical students for future work contexts where interprofessional collaboration may improve patient care and outcomes.7,8 In their study on promoting IPL between biomedical science and medicine, Leadbeater et al9 reported that their students reported that they gained a good understanding of the importance of working collaboratively and how each professional plays a crucial role in treating the patient. Understanding the way IPL influences healthcare providers’ ability to effectively work together has incredible significance, as collaboration and teamwork are crucial for a high quality of care. On the contrary, uncoordinated teamwork and collaboration failures are expected to cause serious errors in managing healthcare.10
Traditionally, educational programs for learners of health professions have occurred in uni-professional teaching and learning settings in their own schools or colleges by same profession’ members.11 However, in real life, healthcare is typically delivered by a team of diverse healthcare providers who can hardly work separately from other professionals. One healthcare professional alone cannot meet a patient’s needs in the current care model. A useful therapeutic partnership between the providers of healthcare and patients now consists of providers from diverse specialties, in addition to those who are seeking medical care as well as their families and caregivers. As part of the process of providing adequate preparation for future healthcare team members, IPL is the groundwork upon which learners become competent and safe healthcare team members.12
Several learning theories combine to explain IPL including cognitivism, constructivism, and humanism. For IPL to take place, all healthcare professionals must be willing to adjust their way of educating and practicing. This adjustment needs a shift in mindsets to engender a paradigm shift in patient care.13
The most current evidence has proven that IPL has been practiced mostly in developed countries.14,15 On the contrary, inadequate evidence exists from developing countries.2 This deficiency of evidence necessitates that developing countries consider the assumptions and tools derived from the experiences of developed countries, as well as the barriers and challenges they encountered when they introduce IPL in their educational programs.15
To plan and implement IPL courses or activities, it is necessary to measure the readiness of the students to learn in an interprofessional setting to achieve positive outcomes that address important IPL dimensions, including relationships among various professional groups, teamwork and collaboration, roles and responsibilities of each professional group, and the benefits to patients, health systems, and individual practitioners.16
The rationale behind this study was to explore the readiness of health professions students in four programs: Medicine, Dentistry, PharmD, and Nursing at Ibn Sina National College for Medical Studies (ISNC) in the Kingdom of Saudi Arabia for IPL before introducing IPL courses and activities in such programs.
Methods
Study Design
This is a descriptive cross-sectional study that explored the readiness of health professions students for interprofessional learning.
Study Context
The study was conducted at the ISNC, which is a fully accredited health professions education institution that has four health professions programs (Medicine, Dentistry, PharmD, and Nursing), which provides an opportunity for students to practice interprofessional learning, especially since the college has also two affiliated hospitals that provide an added opportunity for training and work in an interprofessional manner.
Sample Size and Type
The study employed a comprehensive sampling technique, where all first-year students from the four programs were targeted. The study included all health professions education students who joined the four programs of the college during the academic year 2021–2022. The number of male and female students who fully responded to the survey was 339.
Data Collection
Instrument
Data were collected through the modified, validated version of the Readiness for Interprofessional Learning Scale (RIPLS)7,8 that was originally developed by Parsell and Bligh.16
RIPLS is a 19-item instrument scored on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). The items are classified under four subscales: “Teamwork and Collaboration” (items from 1 to 9), “Negative Professional Identity” (items from 10 to 12), “Positive Professional Identity” (items from 13 to 16), and “Roles and Responsibilities” (items from 17 to 19). The items under “Negative Professional Identity” subscale were reverse scored during the analysis of data (5 = strongly disagree to 1 = strongly agree).
Timing
Data was collected from students towards the end of their first year at ISNC, since at that time the students in each program would have formed a general idea about the nature of the study of students in the other programs.
Data Analysis
Data was analyzed by SPSS v.25. Descriptive statistics were used, and data were presented in the form of means and standard deviations. Demographic data were presented as frequencies and percentages. Responses were compared by paired-samples t-test and analysis of variance (ANOVA) was used for comparing more than two groups. Pearson’s correlation test was used to explore correlations between dependent and independent variables. The significance level was set at p<0.05.
Ethical Approval
Ethical approval was obtained from the ISNC Research and Ethics Committee (REF No: H-26-13022019). Participants were given the right to decline to participate in the study for any reason without prejudice to them. Data were kept confidential, and the survey form was anonymous.
Results
The study employed the well-known, validated modified version of the RIPLS tool to collect data on the perception of students from different health professions programs regarding interprofessional learning. Reliability study of the collected data revealed high internal consistency (Cronbach’s alpha = 0.819), which supports the findings of this study.
The study sample included 339 students from four programs (Medicine, Nursing, PharmD, and Dentistry). Females were around two-thirds of the study sample (63.7%). Students from the Medicine program composed most of the study sample (57.8%). The great majority of the students in the sample came from either governmental schools (48.4%) or private schools (45.7%), with only a small percentage that came from international program schools (5.9%). The great majority of the students (91.4%) had a score of more than 90% in high school. Regarding the GAT score, the great majority of students (87%) had a score between 70% and 90%. Likewise, in the SAAT Science score, the majority of students (79.4%) had a score between 70% and 90% (Table 1).
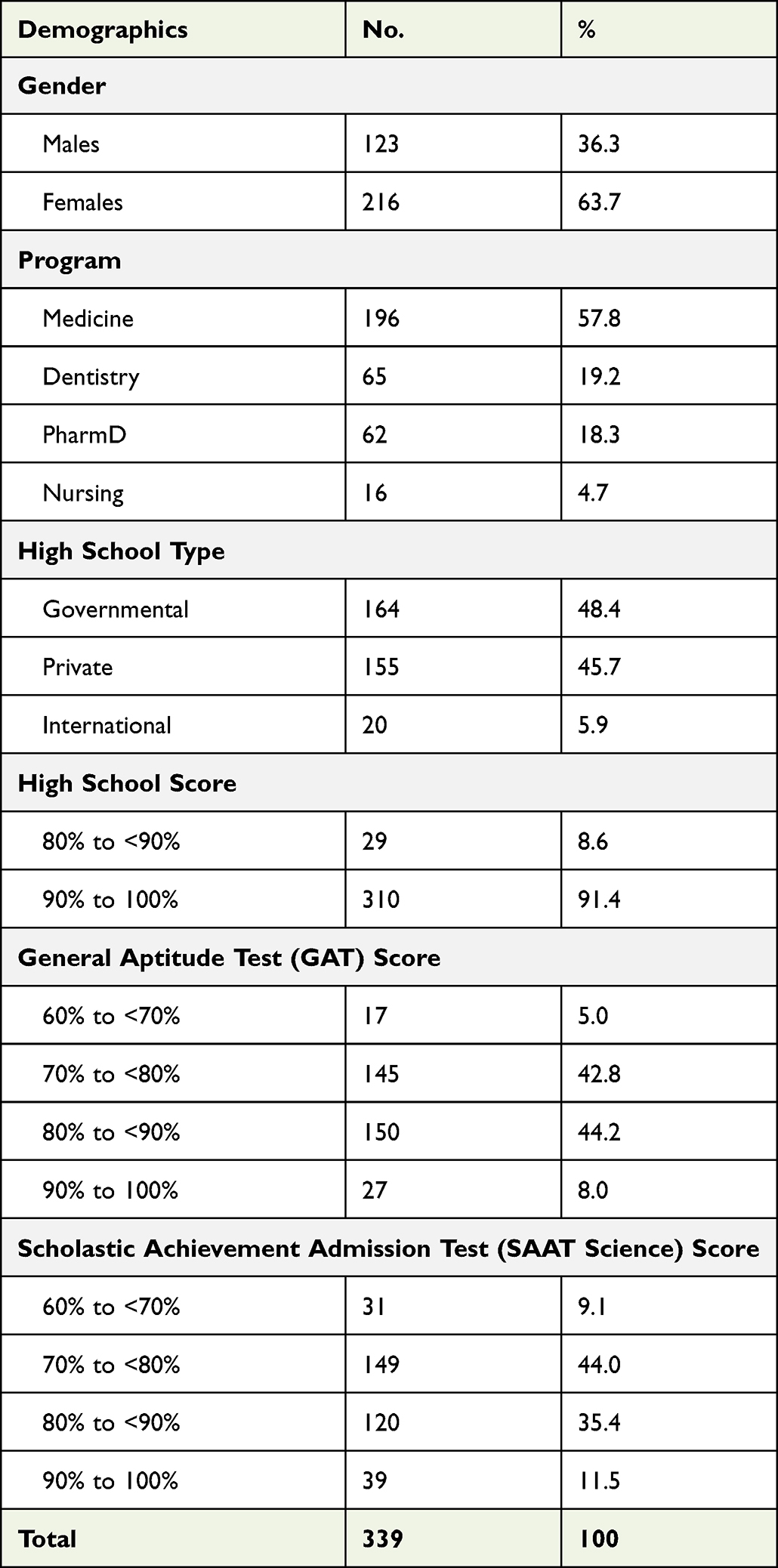 |
Table 1 Demographic Characteristics of the Study Population |
Table 2 shows the mean scores of individual statements and overall mean score for each subscale. The statements “Learning with other students will help me to become a more effective member of a healthcare team” and “Patients would ultimately benefit if healthcare students worked together to solve patient problems” showed the highest mean scores. On the other hand, the statements “Clinical problem-solving can only be learnt effectively with students from my own department/school”, “I’m not sure what my professional role will be”, and “I do not want to waste my time learning with other healthcare students” showed the lowest mean scores. Overall, the average mean score for the “Teamwork and Collaboration” subscale was the highest (4.33±0.56), while the “Negative Professional Identity” subscale had the lowest average mean score (3.59±1.03) and all the individual statements within this subscale showed low mean scores.
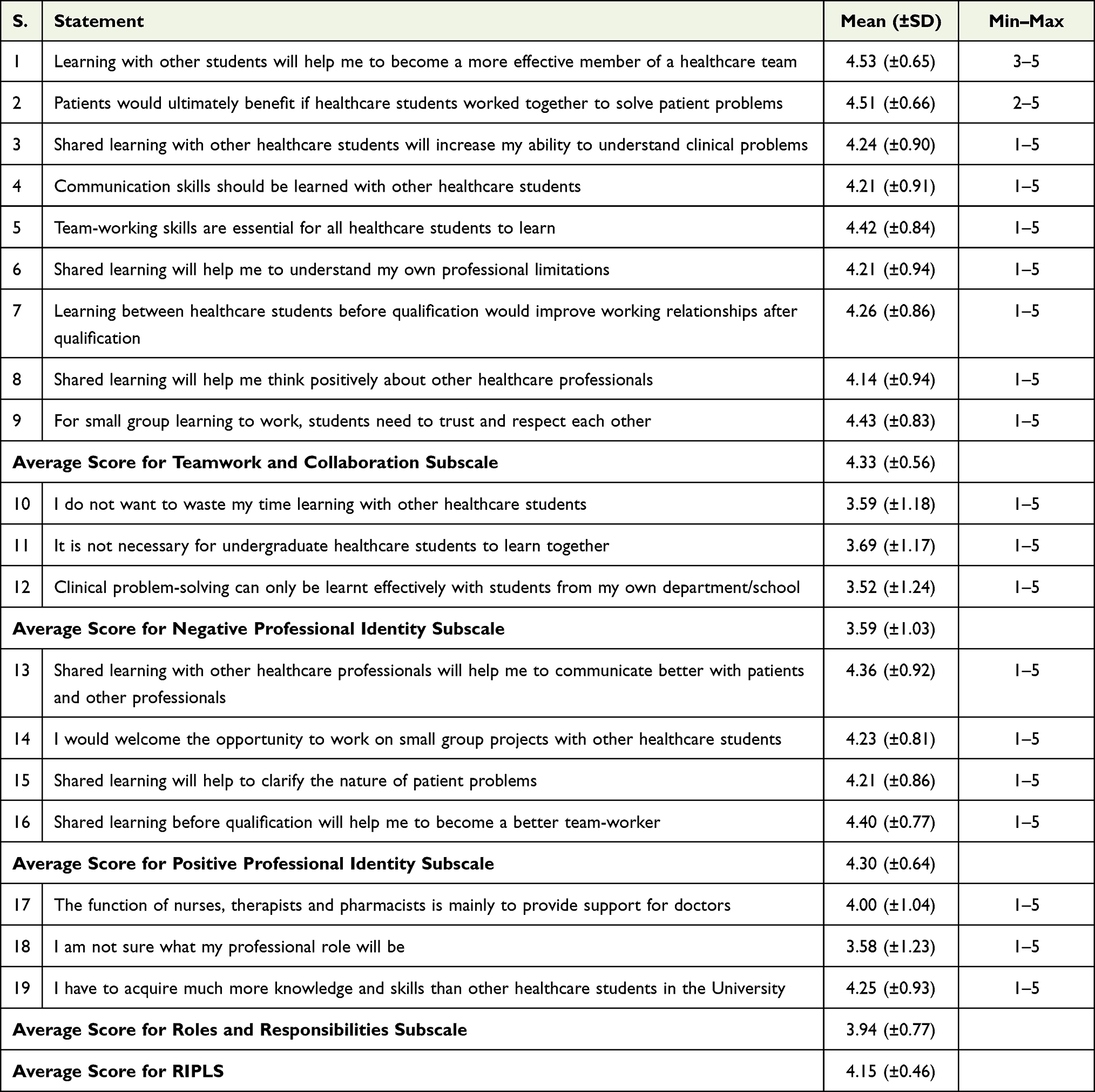 |
Table 2 Descriptive Statistics of the HPE Students’ Responses to the RIPLS (n=339) |
Correlation study showed a weak but statistically significant correlation between the average RIPLS mean scores and the study program (p < 0.015), as shown in Table 3. On the other hand, the correlation between the average RIPLS mean scores and the other variables (gender, high school score, high school type, GAT score, and SAAT score) was very weak and statistically insignificant.
 |
Table 3 Correlation Between the Average Score of the RIPLS Score and Other Independent Variables |
ANOVA revealed a statistically significant difference between the four programs regarding the “Roles and Responsibilities” subscale (p = 0.000), as shown in Table 4.
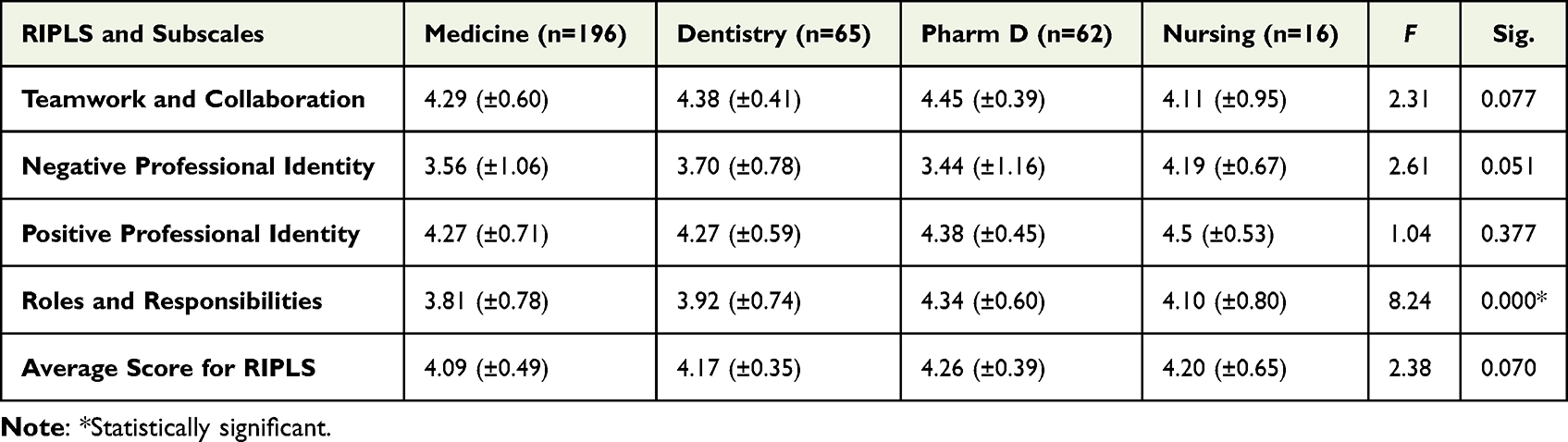 |
Table 4 Analysis of Variance (ANOVA) Among the Participants’ Responses of Different Programs |
Responses of male and female students were compared through the paired samples t-test (Table 5). Results revealed a statistically significant difference between male and female students regarding two statements within the “Teamwork and Collaboration” subscale (“Communication skills should be learned with other healthcare students” and “Team-working skills are essential for all healthcare students to learn”) and one statement within the “Negative Professional Identity” subscale (“Clinical problem-solving can only be learnt effectively with students from my own department/school”) (p < 0.05). The mean scores of male and female students in regard to the other statements are very comparable, and no statistically significant differences were detected (p > 0.05).
 |
Table 5 Descriptive Statistics of Male versus Female Students’ Responses to the RIPLS |
Discussion
There is a growth in the use of IPL in training healthcare professionals due to the referencing of IPL in different accreditation standards.17 Thus, the current study is coping with the raised regional and international interest in studying IPL in health professions education to add evidence about the readiness of undergraduate health professions students for IPL. IPL initiatives and evaluations are expected to expand given that IPL has been recognized on a global scale as a necessary element in enhancing collaborative practice and patient care.
The highest mean score was for the “Teamwork and Collaboration” subscale. This is in agreement with the results of a study conducted at a college of applied medical sciences in Saudi Arabia,18 where students’ scores indicated that they are knowledgeable about the roles of diverse health professionals and the role of collaboration in providing patients with high-quality patient care, and indicated, as well, that they appreciate the shared learning and teamwork to provide patients with high-quality care.
The statements “Clinical problem-solving can only be learnt effectively with students from my own department/school” and “I do not want to waste my time learning with other healthcare students” showed the lowest mean scores. Additionally, the least mean scores were for “Negative Professional Identity” subscale. These results may indicate a change in the mindset of the medical students favoring the collaborative model to work. This result can be a promising indicator for the medical school that ensures graduating better healthcare providers who meet higher professional and ethical standards. On the contrary, Alzamil and Meo19 showed that most of the participants in their study believed that physicians need to have more knowledge than other healthcare professionals, as well as AlAhmari,20 who stated that some roles are higher than others and doctors are considered as leaders of the patient management team.
The statements “Learning with other students will help me to become a more effective member of a healthcare team” and “Patients would ultimately benefit if healthcare students worked together to solve patient problems” showed the highest mean scores. These responses indicate readiness for working collaboratively with other healthcare team members and it would reflect improvement in the postgraduate practice as healthcare organizations run with many conflicting demands and deal with challenging everyday tasks, which, consequently, indicates the need to focus on coordination, role distribution, and accountability of staff as indicated by Edmondson and Harvey.21
There was a statistically significant difference between the RIPLS scores and the students’ study programs. This finding seems to confirm past research work which suggested that the attitudes of students towards IPL vary based on their professional background.22 Further analysis showed that the statistically significant difference between the four programs was in relation to the “Roles and Responsibilities” subscale. This contradicted the results of a study by Aziz et al23 who reported a statistically significant difference between four health professions education programs in the other three subscales. This difference can be explained by the probably unclear role boundaries which may contribute as a source of interpersonal problems among healthcare professionals. This role confusion is further proven in the current study as the statement “I’m not sure what my professional role will be” showed high mean scores. On the other hand, the confusion may be conditionally attributed to respondents’ lack of professional experience.24 Thus, the clinical professionals’ roles and responsibilities may not be completely clear to the inexperienced young clinical undergraduate which indicates a need for awareness and orientation during their undergraduate study to prepare them for practical life and minimize conflicts in the workplace.
Results of the current study showed a statistically significant difference between male and female students within the “Teamwork and Collaboration” and “Negative Professional Identity” subscales. This can be referred to the fact that around two-thirds of the study sample were females, or as female students showed a more positive attitude towards IPL than male students as stated by Talwalkar et al.25 Similarly, Coster et al26 highlighted some gender-related differences in learning styles that might have caused females to be more interested in IPL. Specifically, females have more tendency to listening, understanding, and trusting others’ views while learning. Other studies, however, reported that there is no consistent gender-specific association with differences in RIPLS scores.18,27 This discrepancy highlights an important view that needs to be considered when planning recruitment policies in hospitals. Furthermore, it indicates a need for further research to investigate the gender difference in IPL readiness.
Limitations
This study has a couple of limitations. There were additional health-related professions that were not accessible, despite the study’s inclusion of medical, dental, pharmacy, and nursing students. Further studies are needed to include other groups. Moreover, the self-reported attitude of students about interprofessional education at a single institution placed a constraint on this study, so further larger studies as well as more qualitative studies are needed to capture a deep and full picture of interprofessional education from the students’ point of view.
Conclusion
Undergraduate health professions students in our study showed readiness for the concepts of IPL, which was supported by the high perception mean scores in all RIPLS subscales. For IPL to be successful in our context, we recommend that educational planners should deal with the confounding roles and role boundaries through shared activities, clarify the roles and responsibilities of each healthcare professions, and enforce role models from different health professions who would contribute to creating and implementing successful IPL programs and improving interprofessional collaboration in the healthcare system. Furthermore, a longitudinal study would be useful for further exploring the potential long-term impact of IPL on health professions education graduates, especially in regard to their input in improving collaborative practice and, ultimately, quality of care.
Acknowledgment
We would like to express our deep gratitude and appreciation to the students who participated in the study and to the administration of the college for their endless support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; have took part in drafting or writing, or substantially revised or critically reviewed the article; have agreed on the journal to which the article will be submitted; have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage; and have agreed to take responsibility and be accountable for the contents of the article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yan J, Gilbert JH, Hoffman SJ. World Health Organization study group on interprofessional education and collaborative practice. J Interprof Care. 2007;21(6):588–589. doi:10.1080/13561820701775830
2. World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice (No. WHO/HRH/HPN/10.3). World Health Organization; 2010.
3. Barr H, Koppel I, Reeves S, Hammick M, Freeth DS. Effective Interprofessional Education: Argument, Assumption and Evidence (Promoting Partnership for Health). John Wiley & Sons; 2008.
4. Reeves S, Zwarenstein M, Espin S, Lewin S. Interprofessional Teamwork for Health and Social Care. John Wiley & Sons; 2011.
5. Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2013;3. doi:10.1002/14651858.cd002213.pub3
6. El Bakry AA, Farghaly A, Hany M, Shehata AM, Hosny S. Evaluation of an interprofessional course on leadership and management for medical and nursing pre-registration house officers. Educ Med J. 2018;10(1):41–52. doi:10.21315/eimj2018.10.1.6
7. McFadyen AK, Webster V, Strachan K, Figgins E, Brown H, McKechnie J. The readiness for interprofessional learning scale: a possible more stable sub-scale model for the original version of RIPLS. J Interprof Care. 2005;19(6):595–603. doi:10.1080/13561820500430157
8. McFadyen AK, Webster VS, Maclaren WM. The test-retest reliability of a revised version of the Readiness for Interprofessional Learning Scale (RIPLS). J Interprof Care. 2006;20(6):633–639. doi:10.1080/13561820600991181
9. Leadbeater W, Pallett R, Dunn E, Bashir A, Virtual A. Approach to Promote Inter-Professional Learning (IPL) between biomedical science and medicine in higher education for the benefit of patient care. Front Public Health. 2021;9:747751. doi:10.3389/fpubh.2021.74775
10. Lateef F. Inter-professional education, inter-professional practice and team science: learning together; working together. Educ Med J. 2018;10(4). doi:10.21315/eimj2018.10.4.8
11. Buring SM, Bhushan A, Broeseker A, et al. Interprofessional education: definitions, student competencies, and guidelines for implementation. Am J Pharm Educ. 2009;73(4). doi:10.5688/aj730459
12. Thompson S, Metcalfe K, Boncey K, et al. Interprofessional education in geriatric medicine: towards best practice. A controlled before–after study of medical and nursing students. BMJ Open. 2020;10(1):e018041. doi:10.1136/bmjopen-2017-018041
13. Olenick M, Allen LR, Smego RA Jr. Interprofessional education: a concept analysis. Adv Med Educ Pract. 2010;1:75. doi:10.2147/AMEP.S13207
14. Hammick M, Freeth D, Koppel I, Reeves S, Barr H. A best evidence systematic review of interprofessional education: BEME Guide no. 9. Med Teach. 2007;29(8):735–751. doi:10.1080/01421590701682576
15. Sunguya BF, Hinthong W, Jimba M, Yasuoka J. Interprofessional education for whom?—challenges and lessons learned from its implementation in developed countries and their application to developing countries: a systematic review. PLoS One. 2014;9(5):e96724. doi:10.1371/journal.pone.0096724
16. Parsell G, Bligh J. The development of a questionnaire to assess the readiness of healthcare students for interprofessional learning (RIPLS). Med Educ. 1999;33(2):95–100. doi:10.1046/j.1365-2923.1999.00298.x
17. Grymonpre RE, Bainbridge L, Nasmith L, Baker C. Development of accreditation standards for interprofessional education: a Canadian case study. Hum Resour Health. 2021;19(1):1–10. doi:10.1186/s12960-020-00551-2
18. Alruwaili A, Mumenah N, Alharthy N, Othman F. Students’ readiness for and perception of interprofessional learning: a cross-sectional study. BMC Med Educ. 2020;20(1):1–7. doi:10.1186/s12909-020-02325-9
19. Alzamil H, Meo SA. Medical students’ readiness and perceptions about interprofessional education: a cross sectional study. Pak J Med Sci. 2020;36(4):693. doi:10.12669/pjms.36.4.2214
20. AlAhmari MD. Interprofessional education: Saudi health students’ attitudes toward shared learning. Adv Med Educ Pract. 2019;10:1061. doi:10.2147/AMEP.S226477
21. Edmondson AC, Harvey JF. Cross-boundary teaming for innovation: integrating research on teams and knowledge in organizations. Hum Resour Manage Rev. 2018;28(4):347–360. doi:10.1016/j.hrmr.2017.03.002
22. Curran VR, Sharpe D, Flynn K, Button P. A longitudinal study of the effect of an interprofessional education curriculum on student satisfaction and attitudes towards interprofessional teamwork and education. J Interprof Care. 2010;24(1):41–52. doi:10.3109/13561820903011927
23. Aziz Z, Teck LC, Yen PY. The attitudes of medical, nursing and pharmacy students to inter-professional learning. Procedia Soc Behav Sci. 2011;29:639–645. doi:10.1016/j.sbspro.2011.11.287
24. Lestari E, Stalmeijer RE, Widyandana D, Scherpbier A. Understanding students’ readiness for interprofessional learning in an Asian context: a mixed-methods study. BMC Med Educ. 2016;16(1):1–11. doi:10.1186/s12909-016-0704-3
25. Talwalkar JS, Fahs DB, Kayingo G, Wong R, Jeon S, Honan L. Readiness for interprofessional learning among healthcare professional students. Int J Med Educ. 2016;7:144–148. doi:10.5116/ijme.570d.7bd8
26. Coster S, Norman I, Murrells T, et al. Interprofessional attitudes amongst undergraduate students in the health professions: a longitudinal questionnaire survey. Int J Nurs Stud. 2008;45(11):1667–1681. doi:10.1016/j.ijnurstu.2008.02.008
27. Ahmad MI, Chan SW, Wong LL, Tan ML, Liaw SY. Are first-year healthcare undergraduates at an Asian university ready for interprofessional education? J Interprof Care. 2013;27(4):341–343. doi:10.3109/13561820.2013.769094
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.