Back to Journals » Infection and Drug Resistance » Volume 19
Rapid Diagnosis of Mucor and Aspergillus Co-Infection by Direct Microscopic Examination: A Case Report and Literature Review
Received 26 October 2025
Accepted for publication 24 February 2026
Published 8 April 2026 Volume 2026:19 576917
DOI https://doi.org/10.2147/IDR.S576917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Qian Ning,* Jueqi Lv,* Yanbin Wu
Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Guangxi Medical University, Nanning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanbin Wu, Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Guangxi Medical University, No. 6 Shuangyong Road, Qingxiu District, Nanning, Guangxi, 530000, People’s Republic of China, Email [email protected]
Background: Mixed infections of Mucor and Aspergillus are very rare clinically and have a poor prognosis, primarily occurring in immunocompromised patients. Direct microscopic examination for early rapid diagnosis is of great significance in improving patient prognosis.
Case Presentation: This report describes a 61-year-old male patient with a history of chronic obstructive pulmonary disease and rheumatoid arthritis who had been receiving long-term treatment with prednisone. The patient was admitted to the hospital due to aggravated fever, cough and shortness of breath. The initial diagnosis was pulmonary aspergillosis, and antifungal treatments such as voriconazole, caspofungin and posaconazole were administered successively. However, the patient’s symptoms continued to worsen, with persistently high inflammatory markers. Chest X-ray indicated progression of pulmonary lesions, and ulceration of the nasal mucosa developed. The clinical diagnosis of a mixed infection of Mucor and Aspergillus was ultimately confirmed through direct microscopic examination of nasal ulceration mucosal secretions and bronchoalveolar lavage fluid smears. Despite timely treatment with amphotericin B, the patient died due to the severity of the condition and multiple organ failure.
Conclusion: For patients with pulmonary aspergillosis undergoing immunosuppressive therapy who fail to respond to standard anti-aspergillosis treatment, the possibility of concurrent mucor infection should be highly suspected. Emphasize the advantages of direct microscopic examination in rapidly identifying pathogen infections, optimizing treatment strategies, and improving prognosis.
Keywords: mucormycosis, aspergillosis, direct microscopy, immunosuppression, mixed infection
Introduction
Mucormycosis is a potentially fatal infection caused by fungi of the order Mucorales, commonly affecting the lungs, sinuses, brain, skin, and gastrointestinal tract, and its clinical manifestations are complex and varied, lacking specificity.1–3 It is invasive and vascularly invasive, leading to high morbidity and mortality rates.3,4 It is noteworthy that mixed infections of Mucor and Aspergillus are extremely rare, as both share similar risk factors and clinical characteristics, making their diagnosis challenging.4,5 Mixed infection of Mucor and Aspergillus indicates severe immunosuppression and high mortality rates, making early identification and intervention critical. Microbial culture and histopathology are generally regarded as the “gold standard” for diagnosing fungal infections. However, the urgency of Mucor infection, the long culture time and the low detection rate pose challenges for clinical diagnosis. Direct microscopic examination can bypass the time lag of fungal culture and provide immediate morphological clues, which is of great significance for promptly initiating appropriate antibacterial treatment.
This case describes a patient with chronic obstructive pulmonary disease (COPD) and rheumatoid arthritis(RA) who had been treated with prednisone for a long time. The patient was clinically diagnosed with a mixed infection of Mucor and Aspergillus based on direct microscopic examination of nasal ulceration secretions and bronchoalveolar lavage fluid smears. Based on literature review, this study aims to enhance clinical attention to this mixed infection and emphasize the crucial role of rapid etiological diagnostic techniques in optimizing treatment plans and improving patient prognosis.
Case Presentation
A 61-year-old man, presented with fever, cough, and shortness of breath for two weeks, with symptoms worsening over the past week. He was admitted to our Respiratory Intensive Care Unit (RICU) on December 20, 2024. The patient has smoked for nearly 50 years and has a history of COPD, interstitial pneumonia, and RA. Long-term medications include tripterygium glycosides 20mg twice daily and prednisone tablets 10mg once daily. The patient has no history of diabetes in the past. Two weeks ago, the patient developed fever and cough with wheezing after exposure to cold, with symptoms progressively worsening. Laboratory tests at another hospital indicated positive G and GM tests, and Aspergillus had been cultured in sputum. Chest CT shows emphysema and infection in both lungs. At another hospital, the patient was diagnosed with pulmonary aspergillosis and received antifungal therapy with fluconazole (December 14 to 16) and amphotericin B (December 16 to 20), along with adjunctive treatment including nasal high-flow oxygen therapy and bronchodilators. The patient continued to exhibit cough, sputum production, and wheezing, with persistently elevated inflammatory markers and no clinical improvement in the pulmonary infection. Consequently, the patient was transferred to our hospital’s RICU on December 20.
On presentation, the patient’s temperature was 37.7°C, pulse rate 84 beats per minute, respiratory rate 21 breaths per minute, and blood pressure 109/75 mmHg. The patient was conscious. The patient had clear breath sounds bilaterally, with bilateral basal Velcro rales that were more pronounced on the right. Arterial blood gas analysis indicated Type I respiratory failure. Random blood glucose was 7.29 mmol/L. A chest CT scan performed on December 20, 2024 (Figure 1) revealed imaging features of COPD and interstitial pneumonia in both lungs.
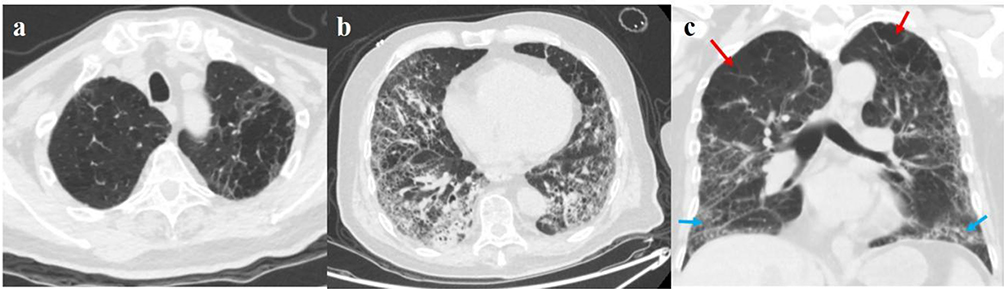 |
Figure 1 Chest CT on December 20, 2024. (a) Multiple round, thin-walled, translucent lesions in the upper lobes of both lungs; (b) Multiple patchy, cord-like, nodular and grid-like increased density shadows occur in the lower lobes of both lungs. (c) Multiple round, thin-walled, translucent lesions in the upper lobes of both lungs (red arrow), Multiple patchy, cord-like, nodular and grid-like increased density shadows occur in the lower lobes of both lungs (blue arrow). |
After admission, the patient was intubated and placed on mechanical ventilation for poor oxygenation. Treatment was started with voriconazole 0.2 g every 12 hours, along with methylprednisolone for RA. On the second day of admission, next-generation sequencing technology (NGS) of the patient’s blood indicated Aspergillus. A chest X-ray on the third day revealed patchy areas of increased density in both lung fields, with blurred margins, suggestive of pneumonia (Figure 2a). Bronchoscopy revealed copious grayish-white viscous sputum. Bronchoalveolar lavage fluid (BALF) was collected for NGS. On the fourth day of admission, BALF NGS detected Aspergillus. Based on voriconazole blood concentration results, the dosage of voriconazole was adjusted to 0.1g orally every 12 hours. On the fifth day of admission, the patient’s inflammatory markers decreased compared with before, but the G test and GM test of the BALF were high (Table 1). Considering worsening fungal infection, caspofungin 70mg everyday was added for antifungal therapy. On the 11th day of admission, bronchoscopy revealed moderate amounts of grayish-white viscous sputum in both lower lungs. Chest X-ray revealed patchy areas of increased density in both lung fields, which have slightly decreased compared to previous findings, suggesting a slight improvement in the inflammation of both upper lungs (Figure 2b). The voriconazole dosage was adjusted to 0.2 g every 12 hours. On the 14th day of admission, the patient’s CRP levels increased. Bronchoscopy revealed moderate amounts of grayish-white, stringy, viscous sputum in both lower lungs. The antifungal therapy was adjusted to posaconazole 0.3 g once daily. On the 15th day of admission, bedside chest X-ray indicated patchy, fluffy and cord-like dense shadows in both lung fields, with blurred edges, suggesting that the bilateral pneumonia has progressed compared to before (Figure 2c). On the 16th day of admission, the patient’s breathing was unstable, the oxygenation index was extremely poor, the pulse oximetry level was still low in pure oxygen conditions, and the pulmonary infection was severe. On the 17th day of admission, the patient’s pulse oximetry and oxygenation index gradually declined. It is considered that the patient is in the terminal stage, with severe pulmonary infection and inability to maintain ventilation function. The patient’s nasal mucosa was ulcerated and bleeding, with some scabs formed but poor healing (Figure 3). Other fungal infections were considered. Nasal secretion fungal culture, fungal smear and other examinations were completed, and amphotericin B 5mg bid for nebulization was added. At 17:00 on the 17th day of admission, the nasal secretions and BALF of the patient showed right-angled branched, few septate, broad, and ribbon-like mucor filaments (Figure 4). That night, the patient’s oxygen saturation and blood pressure could not be maintained, and he subsequently died. The cause of death was considered respiratory failure. The entire treatment process of the patient is shown in Figure 5.
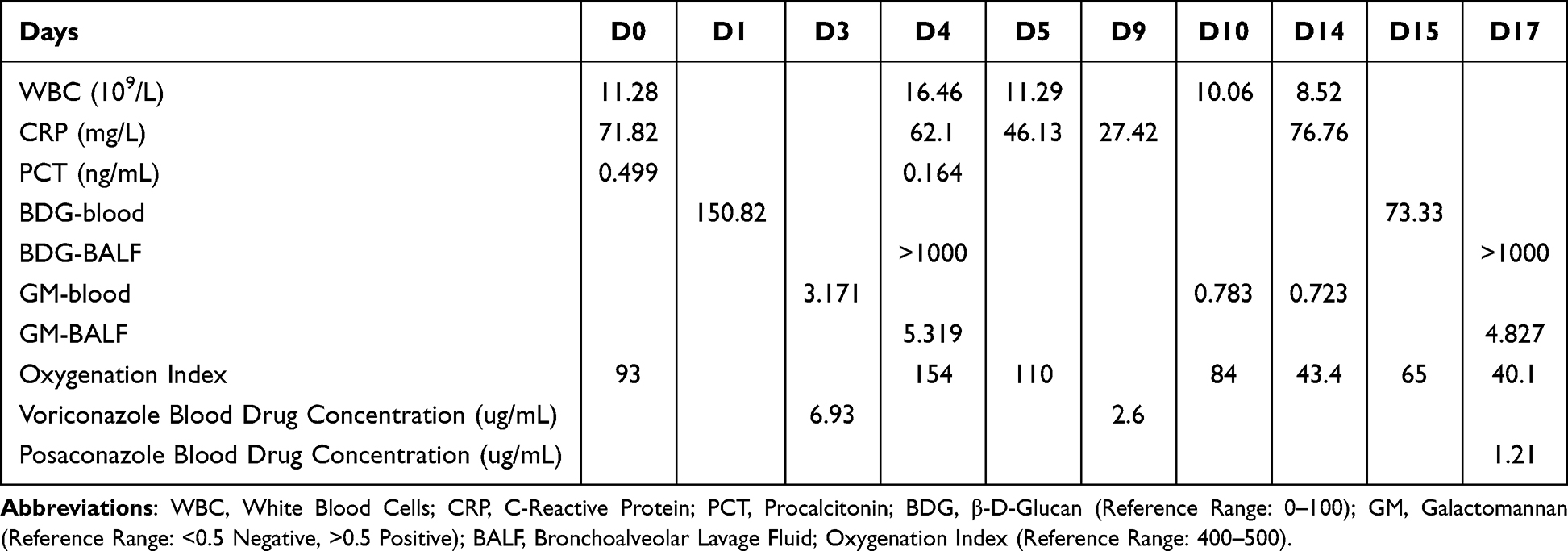 |
Table 1 Laboratory Test Results of the Patient During Hospitalization |
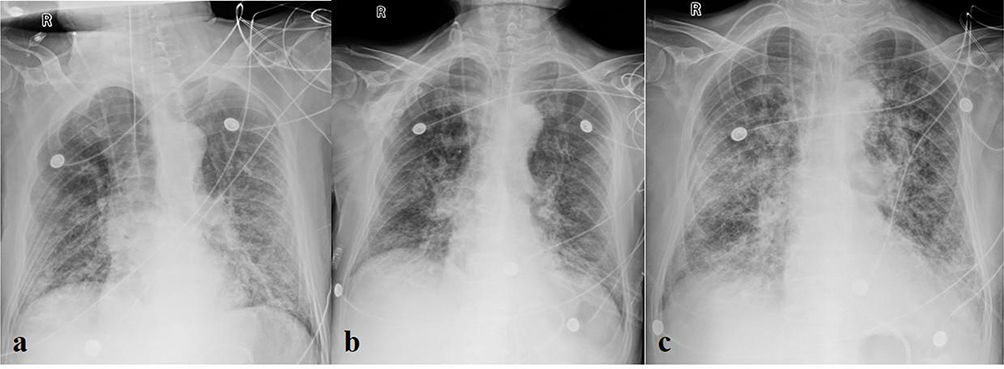 |
Figure 2 Chest X-ray (a) December 23, 2024: Both lung fields show patchy areas of increased density with blurred margins, suggestive of pneumonia. (b) December 31, 2024: Both lung fields show patchy areas of increased density, which have slightly decreased compared to previous findings, suggesting a slight improvement in the inflammation of both upper lungs. (c) January 4, 2025: Both lung fields show patchy, fluffy, and linear dense shadows with blurred margins, suggesting progression of bilateral pulmonary inflammation. |
 |
Figure 3 The patient’s nasal mucosa is ulcerated and bleeding, with some areas scabbing over. |
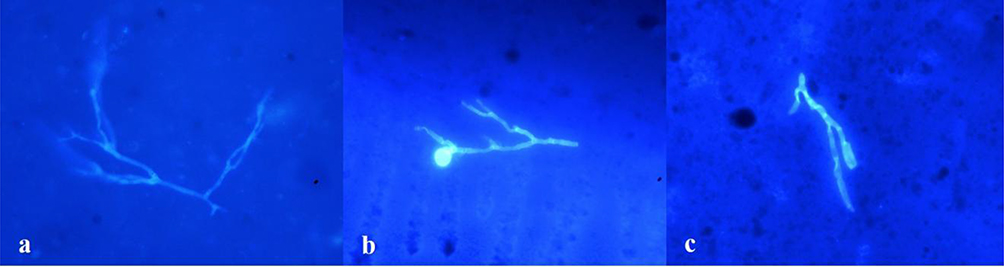 |
Figure 4 The smears of nasal secretions (a) and bronchoalveolar lavage fluid (b and c) show right-angled branches, few septate, wide, and band-like mucor filaments (fungus fluorescent staining, 400×magnification). |
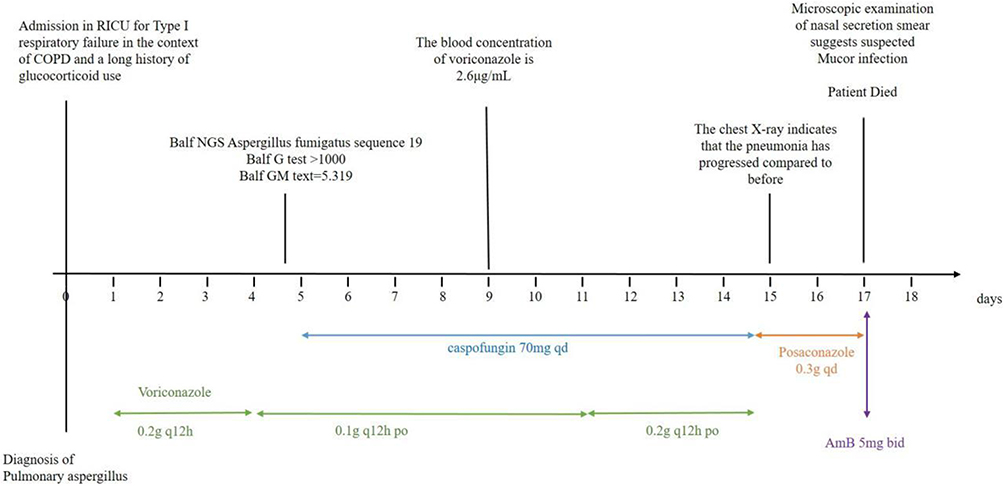 |
Figure 5 The treatment schedule of the patient. |
Systematic Review
This study searched the PubMed database for relevant literature from January 2015 to January 2025 using the search terms “Aspergillosis”, “zygomycosis”, “mucormycosis”, “Rhizopus” and “Cunninghamella”. Articles that did not provide detailed explanations for each case were excluded. A total of 72 patients’ data were extracted, including this case. Clinical data including age, gender, underlying conditions, detection method for Mucor, antifungal treatment, and disease outcomes were systematically categorized and analyzed (Table 2). A detailed summary of the relevant cases can be found in Table S1.6–59 Among these patients, the majority were male (44/70, 62.9%), with ages ranging from 17 months to 79 years and a median age of 53.5 years. The most frequently reported risk factors were diabetes (38/72, 52.8%), corticosteroid use (38/72, 52.8%), COVID-19 (30/72, 41.7%), use of immunosuppressant or chemotherapy (18/72, 25%), and hematologic malignancies (11/72, 15.3%). Other risk factors included organ transplantation (5/72, 6.9%), connective tissue disease (3/72, 4.2%), COPD (3/72, 4.2%), malignancies of other systems (3/72, 4.2%), and trauma (2/72, 2.8%). The primary detection methods for Mucor species in 72 cases were direct microscopy, culture, and histopathology, with respective utilization rates of 33.3% (24/72), 45.8% (33/72), and 69.4% (50/72). Nineteen patients received only drug therapy, with 7 (36.8%) surviving, 10 (52.6%) dying, and 2 cases not mentioned. Forty-six patients underwent combined drug therapy and surgery, with 32 (69.6%) surviving, 12 (26.0%) dying, and 2 cases not mentioned. Apart from our patient, we have not found any reports that take positive direct microscopic examination as the sole biological evidence for mucormycosis.
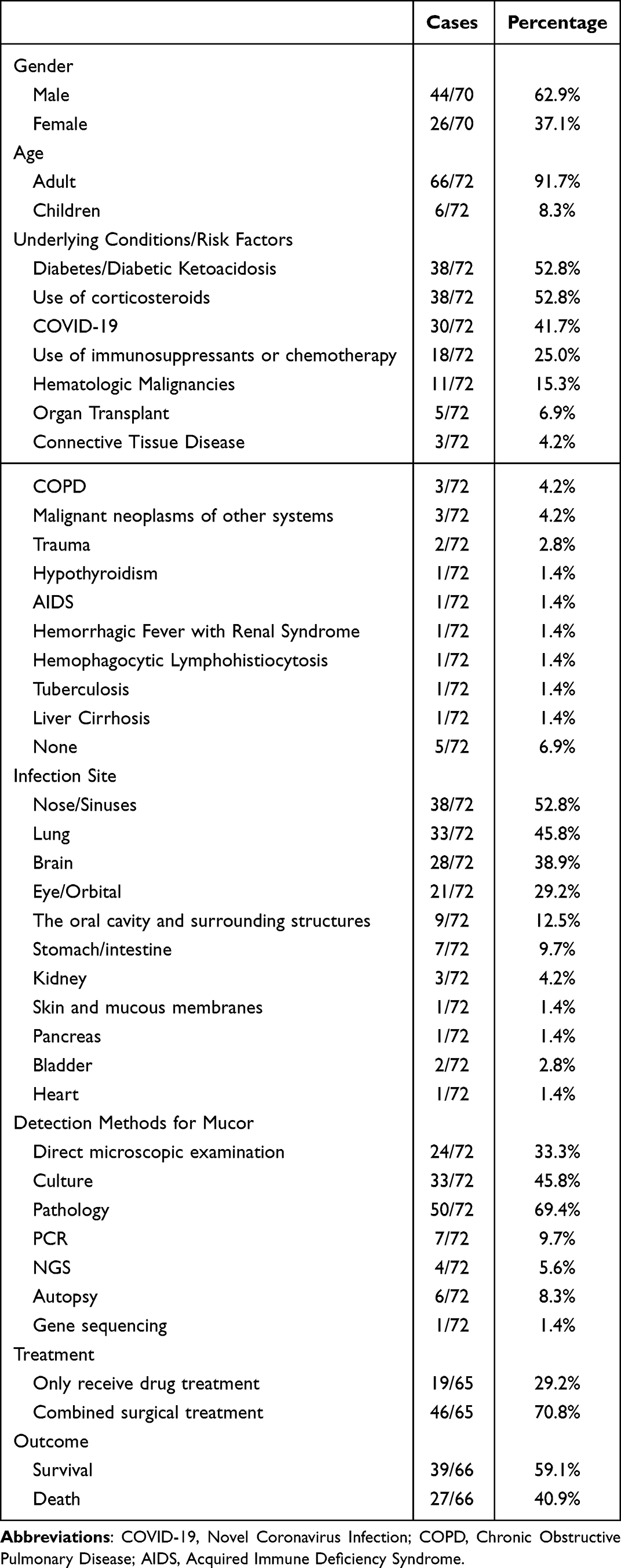 |
Table 2 Summary of 72 Cases of Mixed Infection of Aspergillosis and Mucormycosis |
Discussion
Invasive pulmonary aspergillosis and mucormycosis share partially overlapping risk factors, including prolonged or high-dose corticosteroid use, underlying immunosuppression (such as hematologic malignancies, solid organ or hematopoietic stem cell transplantation, immunosuppressive therapy, or chemotherapy), and neutropenia.1,34,35,60 It is particularly important to note that diabetes (especially when blood glucose control is poor or concurrent ketoacidosis) is the most common risk factor for mucormycosis.1,34 In the context of the global COVID-19 pandemic, the incidence of invasive fungal infections has increased, including rare cases of mixed infections caused by Aspergillus and Mucor.61 COVID-19 infection makes patients prone to secondary or opportunistic fungal infections. However, this patient had no history of diabetes and was not infected with COVID-19. The primary risk factor for him is long-term use of glucocorticoids. Long-term use of glucocorticoids is not only a therapeutic need for COPD, but also due to the fact that the control of rheumatoid arthritis requires continuous immunosuppression. This leads to the patient’s immune defense being extremely fragile, making him an ideal host for Aspergillus and Mucor infections.
It is known that Mucor infection is associated with a high mortality rate. Early diagnosis and treatment are crucial for preventing adverse outcomes. In the early stage of infection of this patient, the diagnosis of pulmonary aspergillosis was very clear. Voriconazole and caspofungin were used successively. These two drugs are first-line drugs for treating Aspergillus, but their activity against Mucor is limited.62,63 Therefore, it is important to distinguish between invasive mucormycosis and aspergillosis, and the standard treatment regimen for mucormycosis is liposomal amphotericin B or isavuconazole.64,65 Although posaconazole exhibits some activity against Mucor and is commonly used for preventive and salvage treatment, it was ineffective in this case. This may be related to the infection having progressed to an advanced stage or the fungal strain itself having certain drug resistance.66,67 In addition, the application of voriconazole in the early stage of the aspergillosis treatment cycle has the potential to enhance the virulence of Mucor.66 This patient’s body temperature fluctuated greatly and the infection was not controlled after treatment with voriconazole and caspofungin. In the later stage, the patient’s nasal mucosa ulcerates, and the healing and scabbing process is slow. At this point, we highly suspect that the patient has a combined mucor infection. Previous literature has indicated that the increase in the number of mucor infection cases in clinical practice may be related to the clinical application of anti-aspergillus drugs.68,69
Mucormycosis and Aspergillosis share similar clinical features, and it is difficult to distinguish them from each other through clinical and imaging signs.70,71 Moreover, the chest CT of this patient did not show typical signs of Aspergillosis or Mucormycosis. We need to rely on some detection methods for a definite diagnosis. In recent years, next-generation sequencing technology (NGS) has been increasingly widely applied in the clinical field and has demonstrated irreplaceable potential value in the identification and diagnosis of fungal infections.72 Compared with traditional culture methods, NGS not only has higher sensitivity and specificity, but also can significantly shorten the diagnostic cycle and achieve earlier diagnosis.71,73 In this case, our patient received two NGS tests, both of which indicated Aspergillus infection, but Mucor infection was not found. It is considered that this might be related to the characteristics of the cell wall of Mucor itself and the load of Mucor pathogen. On the one hand, the cell wall of Mucor is relatively tough, which may affect the efficiency of nucleic acid extraction.74 If the nucleic acid extraction is insufficient, it will lead to a weak signal during sequencing, and thus Mucor will not be detected. On the other hand, it might be that in the early stage of Mucor infection, the pathogen load is relatively low. If the pathogen load is lower than the detection value, then NGS will not detect Mucor. As the disease progresses and the pathogen load increases, the detection rate may rise. Furthermore, aspergillus bloodstream infection is very rare,75,76 but in this case, Aspergillus was detected by blood NGS. The literature indicates that blood NGS has unique advantages in the early diagnosis of invasive fungal diseases.77,78 Therefore, it is crucial to determine whether the detected nucleic acid signals are the transient bacterial shedding from lung lesions or a true bloodstream infection. In patients with pulmonary aspergillosis, fungal hyphae can invade the pulmonary blood vessels, causing the release of fungal DNA, galactomannan and β-D-glucan into the bloodstream. These substances can be detected through NGS, GM test and G test, but they do not necessarily indicate a true blood infection.75 In this case, after 10 days of effective antifungal treatment, the blood GM value and G test results significantly decreased. At the time of admission, there was no imaging evidence of extrapulmonary dissemination. Therefore, we tend to believe that the initial positive result of blood NGS is more likely to be caused by shedding from fungal infection of the lungs.75
Traditional detection methods mainly rely on direct microscopic examination, microbial culture and histopathology when diagnosing Aspergillus and Mucor infections. Microbial culture and histopathology are generally regarded as the “gold standard” for diagnosing fungal infections.79 Through cultivation, fungi can be precisely identified to the genus or even species level, which is of great significance for subsequent in vitro drug sensitivity tests and guiding targeted treatment. However, its obvious drawback is that the culture period is relatively long, lasting for several weeks or even a month, which leads to poor diagnostic timeliness. Moreover, when detecting Mucor, the detective rate is relatively low, and its culture sensitivity is only 20% to 50%.22,74 In this case, we performed cultures on multiple biological specimens including blood, sputum, and BALF. None of the reported results indicated fungal infections of Mucor and Aspergillus. Direct microscopy examination is a valuable diagnostic tool due to its low cost and ability to provide rapid early diagnosis. Aspergillus and Mucor exhibit morphological differences: Aspergillus hyphae are slender, septate, and branch at approximately 45°. Mucor hyphae are wider, non-septate or sparsely septate, and branch at nearly 90°.3,80 In this case, when the patient presented with poor healing of nasal mucosal ulcers and inadequate control of infection despite anti-Aspergillus therapy, we strongly suspected Mucor infection. We collected secretions from the nasal ulcer and BALF for fungal smear microscopy. The same-day results revealed Mucor hyphae with right-angled branching, few septa, wide cross-sections, and ribbon-like appearance, aiding in the diagnosis of mucormycosis. Although microbial culture is regarded as the gold standard for diagnosing mucormycosis, in our case, the patient had risk factors for Mucor infection and corresponding clinical symptoms. Direct microscopic examination of nasal and pulmonary specimens yielding positive results provides strong evidence for Mucor infection.79,81 Direct microscopic examination yields positive results, aiding physicians in making rapid diagnoses and initiating prompt treatment.82 Therefore, any positive test result for Mucor should be considered clinically relevant, particularly in the presence of predisposing factors. While focusing on microbial culture and NGS, we should not overlook the direct smear microscopy—a convenient and rapid diagnostic method that may help confirm or rule out infection.
The rapid differentiation between mucor and aspergillus is not merely a technical detail in diagnosis, it is of great significance for optimizing treatment and improving prognosis. This highlights the advantage of direct microscopic examination in assisting diagnosis and treatment. In situation of co-infection, the presence of Aspergillus in the culture often leads clinicians to use voriconazole based on their experience, but this is ineffective against concurrent Mucor infection. Delay in identifying Mucor infection may lead to the rapid progression of vascular invasion and tissue necrosis. Direct microscopic examination bypasses the time lag of fungal culture and provides immediate morphological clues. This enables clinicians to recognize the presence of mixed infections and prompts them to immediately commence combined antifungal treatment targeting both pathogens. Therefore, in this situation, direct microscopic examination has become a crucial decision-making tool, directly influencing the treatment outcome of the patients.
This case demonstrates that direct microscopic examination can serve as a powerful tool for rapid diagnosis of mixed infections caused by mucor and aspergillus. However, the sensitivity and specificity of this method need to be further investigated in a larger group of similar patients to confirm their validity.
Conclusion
We report a case of a patient with underlying chronic obstructive pulmonary disease and rheumatoid arthritis. The patient was initially diagnosed with pulmonary aspergillosis and received standard anti-aspergillosis treatment, but the therapeutic effect was not satisfactory. Eventually, Mucor infection was detected through direct microscopic examination, but the patient died due to the severity of the condition and multiple organ failure. In this case, we emphasize the advantages of direct smear microscopy in identifying pathogen infections, optimizing treatment strategies, and improving prognosis.
Ethics Approval and Consent to Participate
Ethical approval to report this case was not required as the data had been analyzed in a retrospective manner.
Consent for Publication
Written informed consent was obtained from the patient’s family for publication of this case report and all accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; approved final version of the manuscript; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Health Commission of Guangxi Zhuang Autonomous Region Western medicine category self-funded project [Approval No. Z-A20240531] and Guangxi Appropriate Medical Health Technology Promotion Project [Approval No. S2024023].
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Liang M, Xu J, Luo Y, Qu J. Epidemiology, pathogenesis, clinical characteristics, and treatment of mucormycosis: a review. Ann Med. 2024;56(1):2396570. doi:10.1080/07853890.2024.2396570
2. Gupta I, Baranwal P, Singh G, Gupta V. Mucormycosis, past and present: a comprehensive review. Future Microbiol. 2023;18:217–11. doi:10.2217/fmb-2022-0141
3. Steinbrink JM, Miceli MH. Mucormycosis. Infect Dis Clin North Am. 2021;35(2):435–452. doi:10.1016/j.idc.2021.03.009
4. Spellberg B, Edwards J, Ibrahim A. Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clin Microbiol Rev. 2005;18(3):556–569. doi:10.1128/CMR.18.3.556-569.2005
5. Dagenais TRT, Keller NP. Pathogenesis of Aspergillus fumigatus in Invasive Aspergillosis. Clin Microbiol Rev. 2009;22(3):447–465. doi:10.1128/CMR.00055-08
6. Sakalihasan S, Lifrange F, Czajkowski M, et al. Severe dual fungal infection after bispecific antibody therapy: a case of invasive aspergillosis and mucormycosis in immunocompromised patient. Idcases. 2025;39:e02140. doi:10.1016/j.idcr.2024.e02140
7. Wang S, Yang S, Ma J, et al. The first child with mixed invasive pulmonary mucor and aspergillus infection: a case report and literature review. Front Med. 2024;11:1387278. doi:10.3389/fmed.2024.1387278
8. Wang Q, Huang Y, Ma H, Fan GK. A case report: comorbidity of rhinocerebral mucormycosis and pulmonary aspergillosis with challenging diagnosis. Front Med. 2024;11:1398714. doi:10.3389/fmed.2024.1398714
9. Bredehoeft CT, Sarwar S, Marschalk N. Simultaneous invasive aspergillosis and mucormycosis after orthotopic liver transplant. Transpl Infect Dis off J Transplant Soc. 2024;26(6):e14381. doi:10.1111/tid.14381
10. Ling FX, Qu DM, Lu YQ, Li R, Zhao L. Successful treatment of mixed pulmonary aspergillus and mucor infection using intrabronchial amphotericin B infusion: a case report and literature review. BMC Pulm Med. 2024;24:436. doi:10.1186/s12890-024-03234-z
11. Gotecha S, Chugh A, Punia P, Lachake A. Endoscopic transnasal navigation guided treatment of clivus abscess in adult with mucormycosis: a rare report. Indian J Otolaryngol Head Neck Surg. 2024;76(1):1066–1070. doi:10.1007/s12070-023-04117-1
12. Sasani E, Pakdel F, Khodavaisy S, et al. Mixed aspergillosis and mucormycosis infections in patients with COVID-19: case series and literature review. Mycopathologia. 2024;189(1):10. doi:10.1007/s11046-023-00808-z
13. Menia R, Raychaudhuri S, Agarwal C, Taneja J. COVID-19-associated mucormycosis - “the black fungus” with associated invasive aspergillosis and actinomycosis infection: series of 5 cases in the indian scenario. Indian J Pathol Microbiol. 2023;66(4):823–828. doi:10.4103/ijpm.ijpm_507_22
14. Zhang Y, Yang M. Leukemia followed by mixed infection with mucormycosis and aspergillosis: a case report and literature review. J Cent South Univ Med Sci. 2023;48(7):1105–1112. doi:10.11817/j.issn.1672-7347.2023.230039
15. Sun G, Weiss A, Zhao J, Silver M, DeMaio M, Dehbashi S. Isolated cerebral mucormycosis and aspergillosis coinfection in an immunocompromised adult. BMJ Case Rep. 2023;16(8):e255909. doi:10.1136/bcr-2023-255909
16. Nair AS, Jadav D, Shekhawat RS, Rathore M, Khera S, Sharma R. Autopsy diagnosis of invasive pulmonary aspergillosis and fungal encephalitis due to disseminated pulmonary mucormycosis in a pediatric patient. Am J Forensic Med Pathol. 2023;44(4):e117–e119. doi:10.1097/PAF.0000000000000847
17. Pérez MA, Martínez L, Bravo J, Rodríguez B, Quintero P, Moncada P. Infección por aspergillus flavus y rhizopus oryzae complex en paciente con diabetes mellitus. Biomédica. 2023;43(1):27–36. doi:10.7705/biomedica.6358
18. Murray J, Lu ZA, Miller K, Meadows A, Totten M, Zhang SX. Dual disseminated aspergillosis and mucormycosis diagnosed at autopsy: a report of two cases of coinfection and a review of the literature. J Fungi. 2023;9(3):357. doi:10.3390/jof9030357
19. Sardeshmukh AA, Kshirsagar RA, Prasannakumar P, Nair VS, Jha GK, Warade P. Mucormycosis and aspergillosis infection following maxillofacial trauma: case report. Indian J Otolaryngol Head Neck Surg. 2023;75(2):1245–1249. doi:10.1007/s12070-023-03492-z
20. Mohanty B, Ansari Z, Prasad A, Gupta M, Kumar A. Mucormycosis and aspergillosis: the deadly duo in COVID-19—a case report. J Fam Med Prim Care. 2022;11(10):6529–6532. doi:10.4103/jfmpc.jfmpc_359_22
21. Guo L, Zhang J, Lei J, Wang G. Hemorrhagic fever with renal syndrome complicated with rhino mucormycosis: a case report. Infect Drug Resist. 2022;15:7139–7145. doi:10.2147/IDR.S391035
22. Loubet D, Sarton B, Lelièvre L, et al. Fatal mucormycosis and aspergillosis coinfection associated with haemophagocytic lymphohistiocytosis: a case report and literature review. J Med Mycol. 2023;33(1):101325. doi:10.1016/j.mycmed.2022.101325
23. Ramani P, Krishnan RP, Pandiar D, Benitha JG, Ramalingam K, Gheena S. Chronic invasive aspergillosis with fulminant mucormycosis sparing palate in a post-COVID-19 patient - a case report. Ann Maxillofac Surg. 2022;12(1):102–105. doi:10.4103/ams.ams_296_21
24. Kumar M, Kaundal P, Sharma S, Rana K. Mucormycosis in the urinary bladder—the devil is in the details. Indian J Surg. 1–3. doi:10.1007/s12262-022-03556-4
25. Paul M, Sasidharan J, Taneja J, et al. Invasive mucormycosis and aspergillosis coinfection associated with post-COVID-19 pneumonia in a tertiary care hospital. Med Mycol J. 2022;63(3):59–64. doi:10.3314/mmj.21-00019
26. Kim JH, Kim M, Lim S, et al. A fatal case report of invasive pulmonary aspergillosis and mucormycosis coinfection in an immunocompetent patient with coronavirus disease 2019 in korea. Acute Crit Care. 2023;38(3):382–388. doi:10.4266/acc.2021.01340
27. Serris A, Ouedrani A, Uhel F, et al. Case report: immune checkpoint blockade plus interferon-Γ add-on antifungal therapy in the treatment of refractory covid-associated pulmonary aspergillosis and cerebral mucormycosis. Front Immunol. 2022;13:900522. doi:10.3389/fimmu.2022.900522
28. Rathna R, D’Souza C, D’Silva C, Joseph JM, Varghese AK. Two uncommon presentations of COVID-19-associated mucormycosis. Cureus. 2022;14(1):e21229. doi:10.7759/cureus.21229
29. Melchers M, Festen B, den Dekker BM, et al. A 67-year-old male patient with COVID-19 with worsening respiratory function and acute kidney failure. Chest. 2022;161(1):e5–e11. doi:10.1016/j.chest.2021.08.045
30. Olivo Freites C, Sy H, Miguez P, Salonia J. Uncommon pathogens in an immunocompetent host: respiratory isolation of cunninghamella bertholletiae, aspergillus Niger, staphylococcus pseudintermedius and adenovirus in a patient with necrotising pneumonia. BMJ Case Rep. 2022;15(1):e240484. doi:10.1136/bcr-2020-240484
31. Ramírez-Hinojosa JP, Medrano-Ahumada S, Arenas R, et al. Fungal invasive Co-infection due to aspergillus fumigatus and rhizopus arrhizus: a rhino-orbital presentation. J Fungi. 2021;7(12):1096. doi:10.3390/jof7121096
32. Benhadid-Brahmi Y, Hamane S, Soyer B, et al. COVID-19-associated mixed mold infection: a case report of aspergillosis and mucormycosis and a literature review. J Mycol Medicale. 2022;32(1):101231. doi:10.1016/j.mycmed.2021.101231
33. Teng P, Han X, Zhang S, et al. Mixed invasive pulmonary mucor and aspergillus infection: a case report and literature review. Chin Med J (Engl). 2022;135(7):854–856. doi:10.1097/CM9.0000000000001839
34. Lai CC, Wu CJ, Lee YC, Liu WL. COVID-19 associated with concomitant mucormycosis and aspergillosis. J Microbiol Immunol Infect. 2022;55(2):353–354. doi:10.1016/j.jmii.2021.09.001
35. Ravindra CM, Rajaram M, Madhusmita M, ChToi P, Sneha L. Pulmonary aspergillus and mucor Co-infection. Sultan Qaboos Univ Med J. 2021;21(3):495–498. doi:10.18295/squmj.8.2021.126
36. Sahu ES, Sahu A, Ghodgaonkar P, Lahoti K, Bhargava A. COVID-19-associated rhino-orbital- cerebral mixed mycoses with intracranial fungal granuloma – an aggressively managed rare entity. Indian J Ophthalmol. 2021;69(9):2537–2539. doi:10.4103/ijo.IJO_1598_21
37. min HZ, lan WL, Zou L, et al. Coinfection pulmonary mucormycosis and aspergillosis with disseminated mucormycosis involving gastrointestinalin in an acute B-lymphoblastic leukemia patient. Braz J Microbiol. 2021;52(4):2063–2068. doi:10.1007/s42770-021-00554-8
38. Johnson AK, Ghazarian Z, Cendrowski KD, Persichino JG. Pulmonary aspergillosis and mucormycosis in a patient with COVID-19. Med Mycol Case Rep. 2021;32:64–67. doi:10.1016/j.mmcr.2021.03.006
39. Bellanger AP, Navellou JC, Lepiller Q, et al. Mixed mold infection with aspergillus fumigatus and rhizopus microsporus in a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) patient. Infect Dis Now. 2021;51(7):633–635. doi:10.1016/j.idnow.2021.01.010
40. Jawanda MK, Narula R, Gupta S, Sharma V, Gupta P, Kaur M. Dual fungal infections (aspergillosis and mucormycosis) in a diabetic mellitus patient leading to maxillary sinusitis as a post-COVID manifestation: first case report. Acta Medica. 2021;64(4):227–231. doi:10.14712/18059694.2022.7
41. Zayet S, Zaghdoudi A, Ammari L, Kilani B, Tiouiri Benaissa H. Cerebro-rhino-orbital mucormycosis and aspergillosis coinfection in a patient with diabetes mellitus: a case report. Idcases. 2020;23e01022. doi:10.1016/j.idcr.2020.e01022
42. Malhothra S, Mandal S, Meena R, Patel P, Bhatia NK, Duggal N. A treated case of rhinocerebral zygomycosis with aspergillosis: a case report from India. Access Microbiol. 2020;2(8):acmi000139. doi:10.1099/acmi.0.000139
43. Tsikala-Vafea M, Cao W, Olszewski AJ, Donahue JE, Farmakiotis D. Fatal mucormycosis and aspergillosis in an atypical host: what do we know about mixed invasive mold infections? Case Rep Infect Dis. 2020;2020:8812528. doi:10.1155/2020/8812528
44. Aqsa A, Droubi S, Glaser A. Aspergillus and rhizopus fungal coinfection in a patient with multiple myeloma. Cureus. 2020;12(5):e8050. doi:10.7759/cureus.8050
45. Mantero V, Basilico P, Pozzetti U, et al. Concomitant cerebral aspergillosis and mucormycosis in an immunocompetent woman treated with corticosteroids. J Neurovirol. 2020;26(2):277–280. doi:10.1007/s13365-019-00804-4
46. Lin L, Xue D, Lin TY, Wu YX, Jiang YT, Chen LM. Pulmonary aspergillosis, mucormycosis, and actinomycosis co-infection presenting as a cavitary lesion in a patient with diabetes. Chin Med J (Engl). 2019;132(20):2512–2513. doi:10.1097/CM9.0000000000000468
47. Urs AB, Augustine J, Singh S. Histopathological evaluation of a rare fulminant case of contemporaneous mucormycosis, aspergillosis and actinomycosis. J Oral Maxillofac Pathol JOMFP. 2019;23(1):144–146. doi:10.4103/jomfp.JOMFP_64_19
48. Zhang Q, Liu H, Qiu S, et al. A rare case of pulmonary coinfection by lichtheimia ramosa and aspergillus fumigatus in a patient with delayed graft function after renal transplantation. Transplant Proc. 2019;51(2):551–555. doi:10.1016/j.transproceed.2018.12.006
49. Pouvaret A, Guery R, Montillet M, et al. Concurrent cerebral aspergillosis and abdominal mucormycosis during ibrutinib therapy for chronic lymphocytic leukaemia. Clin Microbiol Infect. 2019;25(6):771–773. doi:10.1016/j.cmi.2019.01.016
50. Trachuk P, Szymczak WA, Muscarella P, Sarwar UN. A case of invasive gastrointestinal mycotypha infection in a patient with neutropenia. Case Rep Infect Dis. 2018;2018:5864175. doi:10.1155/2018/5864175
51. Persichino JG, Can AD, Van TT, Matthews MN, Filler SG. Invasive pulmonary mucormycosis and aspergillosis in a patient with decompensated hepatic cirrhosis. Med Mycol Case Rep. 2018;21:12–15. doi:10.1016/j.mmcr.2018.03.004
52. Kaneko Y, Oinuma KI, Terachi T, et al. Successful treatment of intestinal mycosis caused by a simultaneous infection with lichtheimia ramosa and aspergillus calidoustus. Intern Med. 2018;57(16):2421–2424. doi:10.2169/internalmedicine.0254-17
53. Point S, Gabriel F, Bégueret H, et al. Tumor shape pulmonary mucormycosis associated with sinonasal aspergillosis in a diabetic patient. Med Mycol Case Rep. 2017;19:13–17. doi:10.1016/j.mmcr.2017.08.001
54. Habroosh FA, Eatamadi H, Mohamed RM. Concomitant orbital aspergillosis and mucormycosis in a 17 months old immunocompetent child. Saudi J Ophthalmol. 2017;31(3):193–195. doi:10.1016/j.sjopt.2017.05.006
55. Bhagat M, Rapose A. Rapidly progressing dual infection with aspergillus and rhizopus: when soil inhabitants become deadly invaders. BMJ Case Rep. 2016;2016:bcr2016217535. doi:10.1136/bcr-2016-217535
56. Chermetz M, Gobbo M, Rupel K, et al. Combined orofacial aspergillosis and mucormycosis: fatal complication of a recurrent paediatric glioma-case report and review of literature. Mycopathologia. 2016;181(9–10):723–733. doi:10.1007/s11046-016-0021-8
57. Mahomed S, Basanth S, Mlisana K. The successful use of amphotericin B followed by oral posaconazole in a rare case of invasive fungal sinusitis caused by co-infection with mucormycosis and aspergillus. Idcases. 2015;2(4):116–117. doi:10.1016/j.idcr.2015.10.001
58. Torres-Damas W, Yumpo-Cárdenas D, Mota-Anaya E. coinfection of rhinocerebral mucormycosis and sinus aspergillosis. Rev Peru Med Exp Salud Publica. 2015;32(4):813–817. doi:10.17843/rpmesp.2015.324.1777
59. Jc PL, PM A, Jc RA, et al. mixed invasive fungal infection due to rhizomucor pusillus and aspergillus Niger in an immunocompetent patient. Rev Iberoam Micol. 2015;32(1). doi:10.1016/j.riam.2013.03.002
60. Cadena J, Thompson GR, Patterson TF. Aspergillosis: epidemiology, Diagnosis, and Treatment. Infect Dis Clin North Am. 2021;35(2):415–434. doi:10.1016/j.idc.2021.03.008
61. Jeican II, Horhat DI, Dumitru M, et al. COVID-19-associated rhino-orbital mucormycosis: histological and electron microscopy characteristics. Diagnostics. 2024;14(4):429. doi:10.3390/diagnostics14040429
62. Alastruey-Izquierdo A, Castelli MV, Cuesta I, Monzon A, Cuenca-Estrella M, Rodriguez-Tudela JL. Activity of posaconazole and other antifungal agents against mucorales strains identified by sequencing of internal transcribed spacers. Antimicrob Agents Chemother. 2009;53(4):1686–1689. doi:10.1128/AAC.01467-08
63. Yang N, Zhang L, Feng S. Clinical features and treatment progress of invasive mucormycosis in patients with hematological malignancies. J Fungi. 2023;9(5):592. doi:10.3390/jof9050592
64. Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the european confederation of medical mycology in cooperation with the mycoses study group education and research consortium. Lancet Infect Dis. 2019;19(12):e405–e421. doi:10.1016/S1473-3099(19)30312-3
65. Medical Mycology Society of Chinese Medicine and Education Association; Chinese Mucormycosis Expert Consensus Group. [Expert consensus on diagnosis and management of mucormycosis in China]. Zhonghua nei ke za zhi. 2023;62(6):597–605. doi:10.3760/cma.j.cn112138-20220729-00557
66. Lanternier F, Sun HY, Ribaud P, Singh N, Kontoyiannis DP, Lortholary O. Mucormycosis in organ and stem cell transplant recipients. Clin Infect Dis off Publ Infect Dis Soc Am. 2012;54(11):1–8. doi:10.1093/cid/cis195
67. Sağıroğlu P, Nedret Koç A, Atalay MA, Altinkanat Gelmez G, Canöz Ö, Mutlu Sarıgüzel F. Mucormycosis experience through the eyes of the laboratory. Infect Dis. 2019;51(10):730–737. doi:10.1080/23744235.2019.1645962
68. Siwek GT, Dodgson KJ, De magalhaes-silverman M, et al. Invasive zygomycosis in hematopoietic stem cell transplant recipients receiving voriconazole prophylaxis. Clin Infect Dis off Publ Infect Dis Soc Am. 2004;39(4):584–587. doi:10.1086/422723
69. Kontoyiannis DP, Lionakis MS, Lewis RE, et al. Zygomycosis in a tertiary-care cancer center in the era of aspergillus-active antifungal therapy: a case-control observational study of 27 recent cases. J Infect Dis. 2005;191(8):1350–1360. doi:10.1086/428780
70. Jung J, Kim MY, Lee HJ, et al. Comparison of computed tomographic findings in pulmonary mucormycosis and invasive pulmonary aspergillosis. Clin Microbiol Infect. 2015;21(7):684.e11–684.e18. doi:10.1016/j.cmi.2015.03.019
71. Zhang M, Lu W, Xie D, et al. Metagenomic next-generation sequencing for diagnostically challenging mucormycosis in patients with hematological malignancies. Infect Drug Resist. 2022;15:7509–7517. doi:10.2147/IDR.S393201
72. Wang W, Yao Y, Li X, et al. Clinical impact of metagenomic next-generation sequencing of peripheral blood for the diagnosis of invasive mucormycosis: a single-center retrospective study. Microbiol Spectr. 2024;12(1):e0355323. doi:10.1128/spectrum.03553-23
73. Shi Y, Peng JM, Hu XY, Yang QW, Wang Y. Metagenomic next-generation sequencing for detecting Aspergillosis pneumonia in immunocompromised patients: a retrospective study. Front Cell Infect Microbiol. 2023;13:1209724. doi:10.3389/fcimb.2023.1209724
74. 王维, 周华, 陈琳. PCR和mNGS诊断侵袭性曲霉病和毛霉病的研究进展. 中华医院感染学杂志. Available from: https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CAPJ&dbname=CAPJLAST&filename=ZHYY20250703002.
75. Kaur I, De St Maurice A. Catheter-related aspergillus fungemia: case report and literature review. Pediatr Infect Dis J. 2023;42(8):e308–e311. doi:10.1097/INF.0000000000003942
76. Molina M, Javed N, Penikilapate S, Alao O. Aspergillus fumigatus bloodstream infection in the absence of classic risk factors: expanding the spectrum of invasive aspergillosis. Cureus. 2025;17(3):e80576. doi:10.7759/cureus.80576
77. Liu Q, Liu X, Hu B, et al. Diagnostic performance and clinical impact of blood metagenomic next-generation sequencing in ICU patients suspected monomicrobial and polymicrobial bloodstream infections. Front Cell Infect Microbiol. 2023;13:1192931. doi:10.3389/fcimb.2023.1192931
78. 中华医学会检验医学分会临床微生物学组, 中华医学会微生物学与免疫学分会临床微生物学组, 中国医疗保健国际交流促进会临床微生物与感染分会. [Chinese expert consensus on metagenomics next-generation sequencing application on pathogen detection of infectious diseases]. 宏基因组高通量测序技术应用于感染性疾病病原检测中国专家共识. 中华检验医学杂志. 2021;442:107–120. doi:10.3760/cma.j.cn114452-20201026-00794
79. Walsh TJ, Gamaletsou MN, McGinnis MR, Hayden RT, Kontoyiannis DP. Early clinical and laboratory diagnosis of invasive pulmonary, extrapulmonary, and disseminated mucormycosis (zygomycosis). Clin Infect Dis off Publ Infect Dis Soc Am. 2012;54(1):S55–60. doi:10.1093/cid/cir868
80. Ribes JA, Vanover-Sams CL, Baker DJ. Zygomycetes in Human Disease. Clin Microbiol Rev. 2000;13(2):236–301. doi:10.1128/cmr.13.2.236-301.2000
81. Yong JY, Chong KL, Gan WF, Zaidan NZ. Mucormycosis: a Case Series. Cureus. 2023;15(7):e41375. doi:10.7759/cureus.41375
82. Mohanty A, Gupta P, Arathi K, et al. Evaluation of direct examination, culture, and histopathology in the diagnosis of mucormycosis: reiterating the role of koh mount for early diagnosis. Cureus. 2021;13(11):e19455. doi:10.7759/cureus.19455
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Salvage Treatment for Invasive Aspergillosis and Mucormycosis: Challenges, Recommendations and Future Considerations
Egger M, Bellmann R, Krause R, Boyer J, Jakšić D, Hoenigl M
Infection and Drug Resistance 2023, 16:2167-2178
Published Date: 12 April 2023