Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Randomized Controlled Trial Investigating the Impact of High-Flow Nasal Cannula Oxygen Therapy on Patients Undergoing Robotic-Assisted Laparoscopic Rectal Cancer Surgery, with a Post-Extubation Atelectasis as a Complication
Authors Sun L, Wang J, Wei P, Ruan WQ, Guo J, Yin ZY, Li X, Song JG
Received 14 November 2023
Accepted for publication 15 January 2024
Published 26 January 2024 Volume 2024:17 Pages 379—389
DOI https://doi.org/10.2147/JMDH.S449839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Long Sun,* Jing Wang,* Pan Wei, Wen-Qing Ruan, Jun Guo, Zhi-Yu Yin, Xing Li, Jian-Gang Song
Department of Anesthesiology, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian-Gang Song; Xing Li, Department of Anesthesiology, Shuguang Hospital affiliated to Shanghai University of Traditional Chinese Medicine, No. 528 of Zhangheng Road, Pudong District, Shanghai, 201203, People’s Republic of China, Tel +86 13761172886 ; +86 13585562895, Email [email protected]; [email protected]
Background: Utilizing high-flow nasal cannula (HFNC) oxygen therapy may prevent the collapse of alveoli and improve overall alveolar ventilation. In this study, we aimed to investigate the impact of HFNC on postoperative atelectasis in individuals undergoing robotic-assisted laparoscopic surgery.
Methods: Patients undergoing robotic-assisted laparoscopic surgery for rectal cancer were randomly assigned to the control or HFNC groups. After the surgical procedure was complete and the trachea was extubated, both groups underwent an initial lung ultrasound (LUS) scan. In the post-anesthesia care unit (PACU), the control group received conventional nasal cannula oxygen therapy, while the HFNC group received high-flow nasal cannula oxygen therapy. A second LUS scan was conducted before the patient was transferred to the ward. The primary outcome measured was the total LUS score at the time of PACU discharge.
Results: In the HFNC group (n = 39), the LUS score and the incidence of atelectasis at PACU discharge were significantly lower compared to the control group (n = 39) [(5 vs 10, P < 0.001), (48.72% vs 82.05%, P = 0.002)]. None of the patients in the HFNC group experienced hypoxemia in the PACU, whereas six patients in the control group did (P = 0.03). Additionally, the minimum SpO2 value in the PACU was notably higher in the HFNC group compared to the control group [99 vs 97, P < 0.001].
Conclusion: Based on the results, HFNC improves the extent of postoperative atelectasis and decreases the occurrence of atelectasis in individuals undergoing robotic-assisted laparoscopic surgery for rectal cancer.
Keywords: general anesthesia, high-flow nasal cannula oxygen therapy, lung ultrasound, postoperative atelectasis, robotic-assisted laparoscopic surgery
Introduction
Postoperative pulmonary complications (PPCs) present a significant threat to patients on general anesthesia, and can significantly impact their overall well-being, leading to long-term disabilities or even loss of life.1 Postoperative atelectasis is a severe and prevalent postoperative pulmonary complication (PPC) that merits attention. It affects a significant proportion of adult patients, with an estimated incidence rate of approximately 95%.2 This condition results in complications like hypoxemia, requiring prolonged oxygen therapy, and also contributes to extended hospital stays, chances of postoperative pneumonia, and the development of acute lung injury.3,4 Efficiently addressing and effectively managing postoperative atelectasis is paramount in mitigating the negative consequences of this condition and ultimately enhancing patient outcomes following surgery. Proactive measures such as early mobilization, deep breathing exercises, and lung expansion techniques, help to prevent and treat postoperative atelectasis.
Laparoscopic surgery offers numerous advantages, including reduced tissue trauma, shorter surgery duration, improved cosmetic results, and accelerated recovery. Notwithstanding these advantages, the establishment of pneumoperitoneum in laparoscopic procedures can lead to an elevation in intra-abdominal pressure. This heightened pressure exerts additional compression on the diaphragm, causing its upward displacement and subsequent compression of the lower lung regions, which in turn leads to the development of atelectasis.5 Also, the Trendelenburg position, commonly employed during laparoscopic procedures, exacerbates the already heightened abdominal pressure and intensifies the compression exerted on the diaphragm. This enhanced pressure contributes to a more significant collapse of the alveoli within the lungs.6 The combination of pneumoperitoneum and Trendelenburg position poses an increased risk for the development of atelectasis during laparoscopic surgery.
High-flow nasal cannula (HFNC) oxygen therapy represents a cutting-edge and non-invasive approach to providing respiratory support. By delivering a high flow rate of humidified oxygen through nasal cannulas, HFNC therapy can meet the patient’s oxygenation needs while providing several additional benefits. This innovative therapy has gained recognition for its ability to improve oxygenation, ease breathing, and enhance patient comfort, making it a promising option in respiratory care. This technique entails administering heated and humidified air-oxygen blend alongside a low positive end-expiratory pressure (PEEP), using a nasal catheter to deliver the therapy directly to patients. The heated and humidified air-oxygen mixture helps to optimize respiratory conditions by providing the patient with warm and moistened air, which alleviates airway discomfort and improves mucociliary clearance.7 Additionally, applying a low level of PEEP aids in maintaining lung recruitment and enhancing oxygenation efficiency during each respiratory cycle.8 Previous research has demonstrated the effectiveness of this therapy in enhancing functional residual capacity, thereby reducing the incidence of postoperative atelectasis. Positive outcomes have been particularly notable in specific patient populations, including infants, morbidly obese adults, and individuals undergoing thoracic surgery.9–11 These studies have provided evidence of the beneficial effects of HFNC therapy in mitigating the risk of atelectasis and improving respiratory outcomes in these groups, further supporting its utilization in clinical practice.
To address this issue observed in laparoscopic surgery patients placed in the Trendelenburg position, and the potential impact of extended mechanical ventilation on atelectasis development,12 we undertook a randomized controlled trial focusing on individuals undergoing robotic-assisted laparoscopic surgery for rectal cancer. The primary aim was to evaluate the efficacy of HFNC therapy in mitigating the occurrence of postoperative atelectasis. Effects of HFNC therapy in this specific surgical population were observed to provide valuable insights into the potential benefits of this intervention in reducing the risk of atelectasis and improving postoperative outcomes.
Methods
Our study complied with the Declaration of Helsinki. The study was approved by China Ethics Committee of Registering Clinical Trials (ChiECRCT20210263; date of approval: July 20, 2021) and was registered in the Chinese Clinical Trial Registry (ChiCTR2100047235; date of registration: 11/06/2021). The study adhered to the Consolidated Standards of Reporting Trials (CONSORT) Guidelines, ensuring accurate and comprehensive reporting. Additionally, written informed consent was obtained from all participants, ensuring their voluntary participation and awareness of the study’s objectives and procedures.
Participants
Between July 2021 and December 2021, patients scheduled to undergo robotic-assisted laparoscopic rectal cancer surgery were enrolled in the study.
Exclusion criteria as per American Society of Anesthesiologists physical status (ASA) rating higher than III, body mass index exceeding 30 or below 18, respiratory ailments including upper respiratory infection, chronic obstructive pulmonary disease, bronchial asthma, bronchiectasis, interstitial lung disease, and a history of cardiothoracic surgery.
Exit criteria involved the occurrence of significant subcutaneous emphysema during surgery that impeded lung ultrasound (LUS) assessment and the need to convert from laparoscopy to laparotomy.
Randomization and Blinding
To ensure fair participant allocation, a systematic approach was employed before the initiation of the study. Each patient was assigned a distinct identification number using MS Excel software, and corresponding random numbers were generated. These numbers were then arranged in ascending order, and patients were randomized into either the HFNC or control group, maintaining an equal 1:1 ratio.
To maintain the integrity of the allocation process, the assignments were concealed within sealed envelopes, which were only opened by a research nurse upon the patient’s arrival at the post-anesthesia care unit (PACU), ensuring that the group assignments remained undisclosed until the appropriate time. The evaluator conducting lung ultrasonography and the investigators collecting postoperative data were unaware of the group allocation, ensuring blinding. The PACU nurses were aware of the group allocation but were not involved in data collection and administered the designated interventions (HFNC or conventional nasal cannula oxygen therapy) according to patient group assignment.
Anesthesia Protocol
In the operating room, patients were started on low-flow oxygen through nasal prongs, and standard measures such as electrocardiogram, blood pressure, peripheral oxygen saturation (SpO2), and bispectral index (BIS), were consistently monitored. Additionally, central venous and arterial lines were established under local anesthesia.
General anesthesia was induced with dexamethasone 5 mg, propofol 1.5–2.0 mg/kg, rocuronium 0.8 mg/kg, and sufentanil 0.3 μg/kg. Subsequently, endotracheal intubation was performed using a visual laryngoscope, while the body temperature was monitored using a nasopharyngeal temperature probe. Mechanical ventilation was implemented in a volume-controlled mode, delivering a tidal volume of 7 mL/kg (based on ideal body weight), PEEP of 5 cmH2O, inspiration-to-expiration ratio of 1:2, with fractional oxygen concentration of 50%. The respiratory rate was adjusted to maintain an end-tidal partial pressure of CO2 between 35–55 mmHg.
Anesthesia maintenance was achieved through continuous intravenous infusion of propofol, remifentanil, and inhalational sevoflurane. Throughout the procedure, the bispectral index (BIS) value was maintained within the range of 40–60, and the body temperature was maintained above 36 °C using a warm air fan. Postoperative analgesia was attained through 0.375% ropivacaine (10–20 mL) and a patient-controlled intravenous analgesia pump (PCIA).
To reverse residual neuromuscular block, neostigmine and atropine were administered at appropriate dosages. Before tracheal extubation, a recruitment maneuver was conducted, applying positive pressure of 30 cmH2O for 30 seconds. The patients were extubated after they regained consciousness, exhibited adequate muscle strength and maintained satisfactory minute ventilation.
Lung Ultrasound Examination
The initial LUS assessment was conducted in the operating room on removal of the endotracheal tube post-surgery. The Navi Series Ultrasound System (Shenzhen Wisonic Medical Technology Co., Ltd, China) was utilized with a 1 MHz–5 MHz convex probe. As previously described,13 each hemithorax was divided into six segments using three longitudinal lines (parasternal, anterior, and posterior axillary) and two axial lines (one above the diaphragm and another 1 cm above the nipple; see Figure 1).
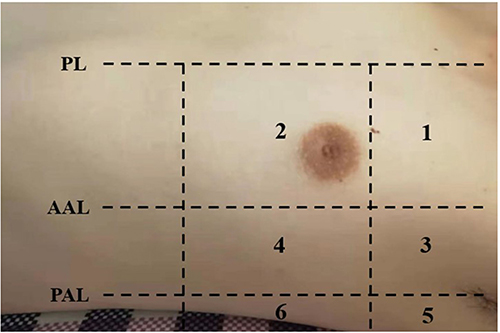 |
Figure 1 Division of the hemithorax into 6 segments for lung ultrasound examination. Abbreviations: PL, parasternal line; AAL, anterior axillary line; PAL, posterior axillary line. |
A total of 12 regions were evaluated and scores assigned based on the modified LUS score system proposed by Monastesse et al.14 The scoring criteria for atelectasis severity in each region were as follows (see Figure 2): 0 indicated 0–2 B lines, 1 represented ≥ 3 B lines or one or multiple small subpleural consolidations separated by a regular pleural line, 2 indicated multiple coalescent B lines or multiple small subpleural consolidations separated by a thickened or irregular pleural line, and 3 signified consolidation or small subpleural consolidation larger than 1×2 cm in diameter. For statistical analysis, the LUS scores of all 12 regions were aggregated to obtain the total LUS score, which reflected the overall severity of atelectasis. Moreover, significant atelectasis was defined as a score of ≥ 2 in any region.
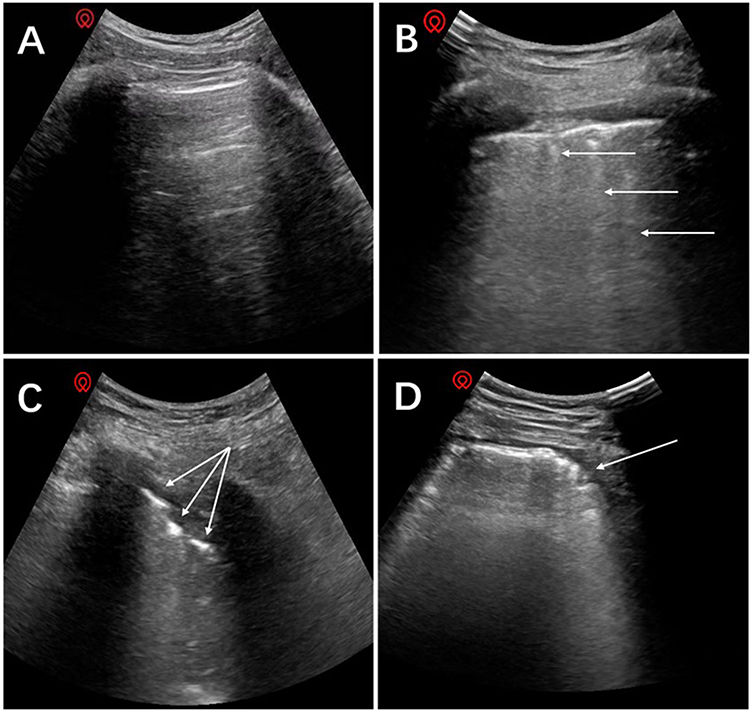 |
Figure 2 Lung ultrasound images with different scores. (A) Normal pattern “bat-sign” with A-lines parallel to the pleural line, score = 0; (B) ≥3 B lines arising from pleural line, score = 1; (C) Multiple subpleural consolidations separated by an irregular pleural line, score = 2; (D) Large-sized consolidation, score = 3. Arrow indicates corresponding pathologic findings of each figure. |
After the patients demonstrated stable vital signs without notable fluctuations, they were transferred to the PACU for further monitoring. Within the PACU setting, the control group received conventional nasal cannula oxygen therapy at a prescribed flow rate of 4 L/min. The HFNC group underwent oxygen administration through an OptiflowTM device from Fisher & Paykel Healthcare Ltd, New Zealand. This device was configured to deliver a high gas flow rate of 30 L/min and an inspiratory oxygen fraction (FiO2) of 50%. To ensure optimal patient comfort, a humidifier was incorporated into the system to maintain the temperature of the inspiratory gas at a constant 37 °C. Before patient transfer to the general ward, a second LUS scan was conducted, and a skilled anesthesiologist meticulously evaluated all the obtained LUS scans to assess the respiratory status of the patient.
Outcome Measurements
The LUS score at the time of discharge from the PACU was the primary outcome measure in this study. Additionally, we included several secondary outcome measures for comprehensive evaluation. These secondary measures encompassed the LUS score after tracheal extubation, the incidence of hypoxemia (defined as SpO2 < 95%) and the minimum SpO2 value observed during PACU stay. Furthermore, we examined the occurrence of postoperative pneumonia, which was defined according to the European Perioperative Clinical Outcome (EPCO) criteria,15 requiring the presence of specific chest X-ray or computed tomography (CT) findings such as infiltrate, consolidation, or cavitation, along with indications of infection such as abnormal body temperature or an elevated white blood cell count. Finally, we also considered the duration of hospitalization as an additional secondary outcome measure in our investigation.
Statistical Analysis
To determine the appropriate sample size for our study, we relied on a previous investigation that explored the effects of HFNC therapy on individuals with blunt chest injuries.16 This reference study reported LUS scores of 13 (with a standard deviation [SD] of 6) in the conventional oxygen therapy group and 9 (with an SD of 6) in the HFNC group. These values served as crucial benchmarks, aiding us in estimating the required sample size to achieve adequate statistical power and detect meaningful differences in LUS scores between our control and HFNC groups. Considering a 10% attrition rate, an alpha of 0.05, and a power of 0.8, the required sample size was calculated as 80 patients (40 in each group) using PASS 15.0 software (NCSS, LLC, Kaysville, UT).
All the data collected in this study were analyzed using SPSS 22.0 software. The normality of distribution for continuous variables was assessed using the Shapiro–Wilk test. Normally distributed measurement data were expressed as mean±standard deviation (SD), while non-normally distributed measurement data were expressed as median (interquartile range), and the comparisons were examined by Student-t test and Mann–Whitney test (non parametric distribution). Paired t-tests were utilized for within-group analyses. The categorical data were expressed as n(%), and the differences between the two groups were examined by chi-square analysis or Fisher’s exact test. P<0.05 was considered statistically significant.
Results
From the initial enrollment of 101 patients, 21 individuals were excluded before the randomization process due to various factors. The final sample size consisted of 80 randomized patients who subsequently received their assigned treatments as per the study protocol. However, two patients had to be excluded from the analysis due to severe subcutaneous emphysema, with a final analysis cohort of 39 patients in each group, as depicted in Figure 3. Detailed demographic information and surgical characteristics of the patients included can be found in Table 1.
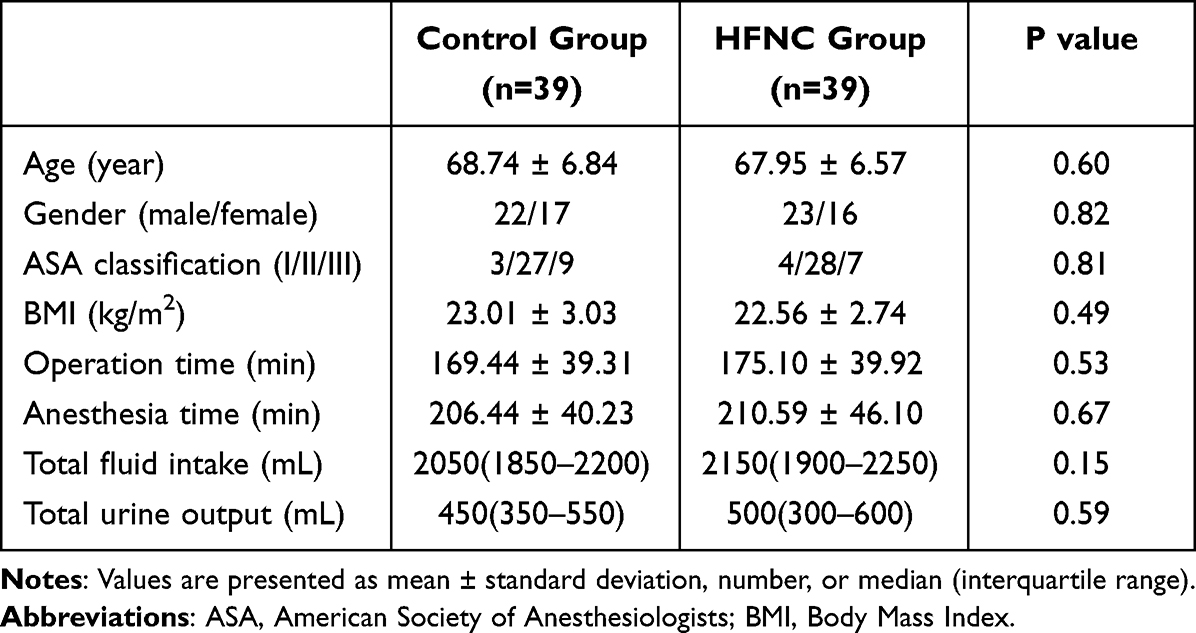 |
Table 1 Demographic Data and Surgical Details |
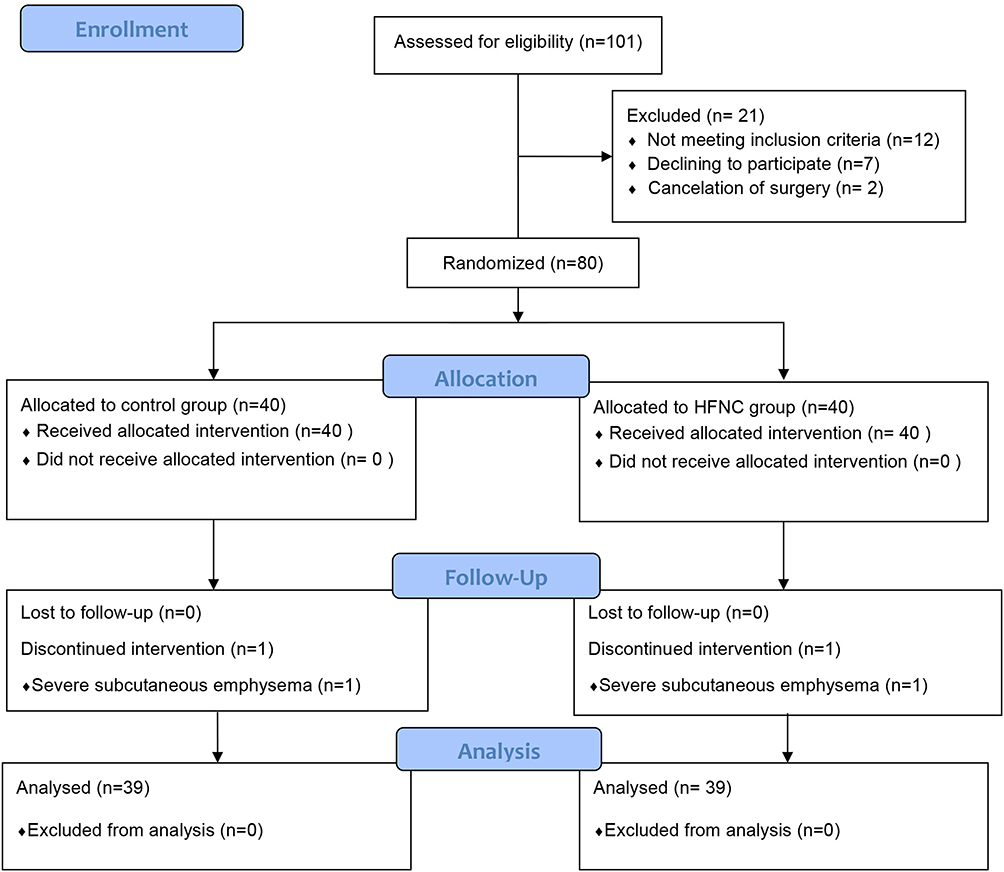 |
Figure 3 Flowchart of participants. |
Analysis of the data presented in Table 2 revealed no significant differences in the total LUS score and the incidence of significant atelectasis between the HFNC group and the control group at the time of tracheal extubation (T1). However, notable disparities emerged at the point of PACU discharge (T2), where the HFNC group exhibited significantly lower total LUS scores and a decreased incidence of atelectasis compared to the control group [(5, interquartile range 3–8) vs 10 (8–12), P < 0.001), (48.72% vs 82.05%, P = 0.002)]. Additionally, within the HFNC group, there was a significant reduction in both the total LUS scores and the incidence of atelectasis at T2 as compared to T1, indicating the effectiveness of the HFNC therapy in mitigating the development of atelectasis over time.
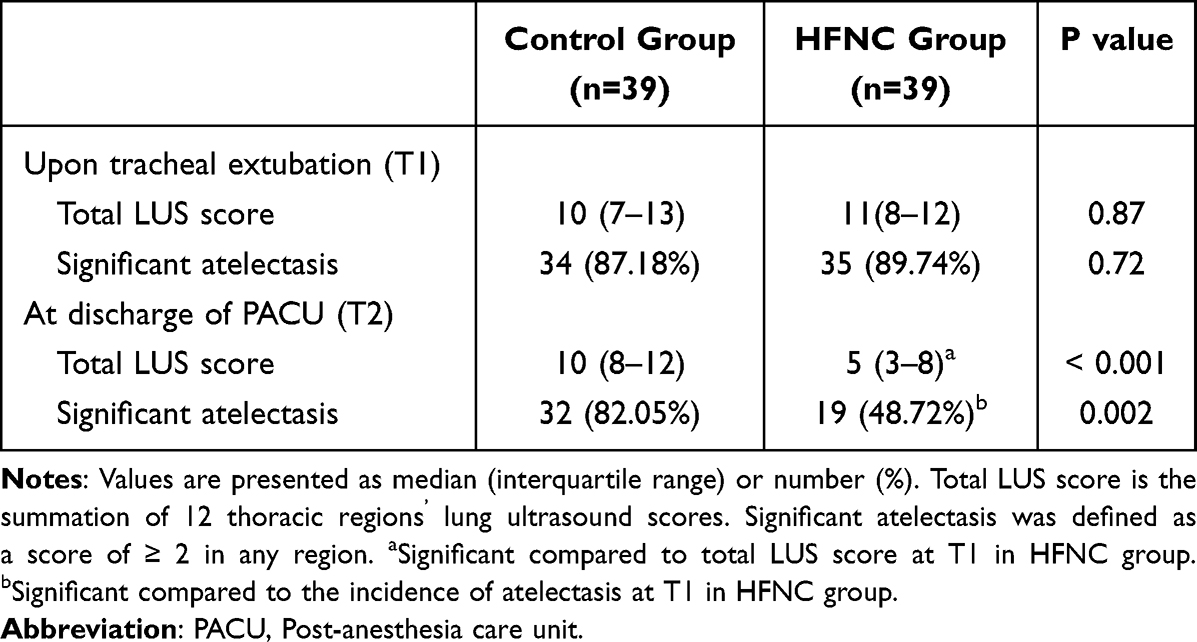 |
Table 2 Lung Ultrasound Measurements at Different Time Points |
Within the HFNC group, none of the patients encountered hypoxemia during their stay in the PACU, whereas 6 patients in the control group experienced hypoxemia (P = 0.03), indicating a significant difference between the two groups. No patients of these 6 patients with SpO2 lower than 90%, so no additional symptomatic treatment was given to avoid interrupting the intervention. After the second lung ultrasound scan completed, we administered mask oxygenation to improve oxygenation, and then returned to the ward. Moreover, the HFNC group demonstrated notably higher minimum oxygen saturation (SpO2) values in the PACU, compared to the control group [99 (interquartile range 98–99) vs 97 (95–98), P < 0.001]. However, no significant differences were observed between the two groups regarding PACU stay duration, incidence of postoperative pneumonia, and length of hospitalization, as indicated in Table 3.
 |
Table 3 Postoperative Variables Between the Control and HFNC Groups |
Discussion
In this prospective randomized study, we collected compelling evidence supporting the efficacy of HFNC therapy in the PACU to reduce total LUS scores and the incidence of significant atelectasis in patients undergoing robotic-assisted laparoscopic rectal cancer surgery, as demonstrated in Table 2. Furthermore, the utilization of HFNC in the PACU yielded improved postoperative oxygenation, as indicated in Table 3. Notably, this is the first study to shed light on the distinctive advantages of HFNC in patients undergoing robotic-assisted laparoscopic rectal cancer surgery, offering valuable insights into optimizing postoperative care and outcomes.
LUS is a critical diagnostic tool for evaluating a range of pulmonary conditions including pneumothorax, pleural effusion, diffuse interstitial syndrome, and atelectasis.17 This imaging modality provides valuable insights into the structural integrity and functionality of the lungs, allowing for comprehensive assessment of these diverse pathological processes. LUS helps healthcare professionals in accurately detecting and monitoring these conditions, enabling timely interventions and tailored treatment strategies to optimize patient care and outcomes. LUS is widely recognized as a rapid, safe, and radiation-free diagnostic method with proven efficacy in accurately detecting adult postoperative atelectasis. Previous studies have reported impressive performance metrics, including a sensitivity of 87.7%, specificity of 92.1%, and an overall diagnostic accuracy of 90.8%.18 These compelling statistics highlight the reliability and precision of LUS as a valuable tool in identifying and assessing atelectasis, allowing for prompt intervention and appropriate management strategies to optimize patient outcomes. During this study, the overall incidence of postoperative atelectasis at T1 was found to be 88.46% (69 out of 78 patients), indicating a significant prevalence following robotic-assisted laparoscopic rectal cancer surgery. This finding aligns with previous research that has utilized CT scans to diagnose and assess postoperative atelectasis,19 further substantiating the high occurrence of this condition in the specified patient population. The observed consistency in the incidence of atelectasis highlights the need for effective preventive measures and interventions to mitigate its impact on patient recovery and overall outcomes.
Our hypothesis suggests that HFNC therapy impacts postoperative atelectasis through two distinct mechanisms. Firstly, despite its noninvasive nature, HFNC can generate PEEP.20 Previous studies have demonstrated that for each 10 L/min increment in HFNC flow rate, pharyngeal PEEP in patients increases by approximately 0.5–1 cmH2O. At higher flow rates, such as 60 L/min, the PEEP within the closed oropharyngeal cavities can reach 4–4.7 cmH2O, providing a potential mechanism for promoting lung function and mitigating atelectasis.21 These findings emphasize the significance of PEEP generation through HFNC as a contributing factor in its efficacy against postoperative atelectasis. Secondly, by delivering warm and humidified gas, HFNC therapy facilitates lung function and alleviates atelectasis. The warm and humid environment created by HFNC minimizes water loss from the nasal mucosa, which helps maintain optimal moisture levels.22 This, in turn, enhances the clearance of cilia and promotes efficient elimination of respiratory secretions.23 HFNC therapy contributes to improved respiratory function and decreased mucus retention, thereby playing a crucial role in mitigating atelectasis and supporting overall pulmonary health. Considering that mucous secretion-induced bronchial obstruction is a crucial contributor to atelectasis,24 we postulate that the warm and humidified gas delivered through HFNC therapy plays a crucial role in alleviating this condition. The combination of warm and humidified gas helps to maintain optimal moisture levels in the airways, promoting adequate mucociliary clearance and minimizing the risk of bronchial obstruction caused by excessive mucus secretion. By addressing this underlying mechanism, HFNC therapy is a valuable intervention in mitigating postoperative atelectasis and improving respiratory outcomes.
The control group in this study exhibited no significant differences in the total LUS score and incidence of significant atelectasis at different time points (T1 and T2), suggesting that postoperative atelectasis does not spontaneously resolve within a short period without intervention. These findings underscore the persistence of atelectasis resulting from general anesthesia for several days following surgery.25 With the absence of specific interventions targeted at atelectasis resolution, the lack of improvement in the control group highlights the importance of proactive measures to address and manage postoperative atelectasis effectively, considering its potential for prolonged impact on patient recovery and respiratory function. Despite the utilization of HFNC therapy, it is noteworthy that 48.72% (19 out of 39) of patients in the HFNC group still exhibited atelectasis at the time of discharge from the PACU (T2). This observation leads us to speculate that atelectasis may be attributed to the residual effects of neuromuscular blockade experienced during the PACU stay. These residual effects can potentially impair respiratory muscle function and contribute to the persistence of atelectasis,26 underscoring the need for further investigations for optimal management of neuromuscular blockade and its impact on postoperative respiratory outcomes.
After tracheal extubation, healthcare providers can access several oxygenation methods to support patients, such as a nasal cannula, oxygen mask, non-invasive ventilator, and HFNC. Extensive research consistently highlights the superiority of HFNC over conventional oxygen therapy, including nasal cannula or mask, when it comes to enhancing oxygenation. Numerous studies have demonstrated that HFNC provides more effective oxygen delivery, ensuring adequate oxygenation levels and improving respiratory outcomes for patients across various clinical settings.27–29 Consistent with previous research findings, the results of our current study reaffirmed the special oxygenation effects of HFNC compared to nasal cannula oxygen therapy (Table 3). Hypoxemia, a decrease in oxygen saturation, is a joint adverse event following tracheal extubation in the PACU. The high fraction of inspired oxygen (FiO2) delivered through the HFNC may significantly prevent hypoxemia episodes. In our study, the FiO2 in the HFNC group was explicitly set at 50% to optimize oxygenation and mitigate the risk of hypoxemia events. The high flow rate of oxygen provided by the HFNC in our study resulted in an inspired oxygen concentration close to 50%.30 In contrast, the control group received oxygen through a regular nasal cannula at a flow rate of 4 L/minute and had an actual FiO2 of no more than 37%. Additionally, the high flow of oxygen delivered by the HFNC offers the advantage of clearing the physiological dead space in the nasopharynx.31 This action enhances alveolar ventilation and improves oxygenation by maximizing the exchange of oxygen and carbon dioxide within the lungs.
Contrary to the results reported in the previous study, our findings did not reveal any notable advantages in terms of postoperative pneumonia incidence and the duration of hospitalization.32 Despite the positive outcomes observed in other aspects of our study, such as reduced atelectasis and improved oxygenation with the use of an HFNC, the lack of significant effects on postoperative pneumonia and length of hospital stay suggests that additional factors or interventions may influence these specific outcomes. Further investigation is warranted to explore the potential reasons behind these discrepancies and to identify other strategies that may reduce postoperative pneumonia and shorten hospitalization duration. The discrepancy in the observed outcomes may be attributed to the deliberate exclusion of patients undergoing thoracic surgery, obese patients, and those with abnormal lung physiology in our study design. By excluding these specific patient groups, who are known to be at a higher risk for postoperative pulmonary complications, our study may have inadvertently selected a population with a lower baseline risk. Consequently, the overall incidence of postoperative complications, including pneumonia, may have been lower than anticipated, limiting our ability to detect significant differences. To better understand the potential benefits of postoperative HFNC in preventing pulmonary complications, future studies should focus on these high-risk groups and assess the impact of HFNC usage on their outcomes. By specifically targeting these patient populations, we can obtain more comprehensive insights into the effectiveness of HFNC in reducing postoperative pulmonary complications and optimizing its clinical application.
This study had several limitations that should be acknowledged to interpret the findings appropriately. Firstly, excluding patients with pre-existing lung diseases may limit the generalizability of our results to a broader patient population. However, our findings still suggest that the proactive use of HFNC may have benefits even in relatively healthy patients undergoing surgery. Secondly, the absence of a LUS immediately after the induction of anesthesia is a limitation. It is known that atelectasis can develop rapidly following preoxygenation and the induction of anesthesia,33 and assessing its presence at that specific time point could have provided valuable insights into the early development of atelectasis. Therefore, the absence of LUS assessments immediately after the induction of anesthesia in our study limited our ability to observe the precise process of atelectasis formation. Future research could consider incorporating early LUS assessments at different time points, including before and after the induction of anesthesia, to capture the dynamics of atelectasis development and gain a more comprehensive understanding of its progression. Such investigations would provide valuable insights into the temporal aspects of atelectasis formation and further inform preventive strategies and interventions.
Conclusion
Our study highlights the significant benefits of implementing HFNC in the PACU for patients undergoing robotic-assisted laparoscopic rectal cancer surgery. The decrease in postoperative atelectasis, as indicated by LUS evaluation, coupled with improvements in oxygenation, substantiates the effectiveness of HFNC therapy in this surgical context. However, future research should include patients with abnormal lung physiology to assess the broader applicability of HFNC and its impact on overall postoperative outcomes, such as postoperative pneumonia, length of hospitalization, and other relevant clinical endpoints. Such investigations will provide valuable insights into optimizing postoperative care and enhancing patient outcomes.
Abbreviations
ASA, American Society of Anesthesiologists; BIS, bispectral index; BMI, body mass index; CONSORT, Consolidated Standards of Reporting Trials; EPCO, European Perioperative Clinical Outcome; FiO2, fraction of inspiratory oxygen; HFNC, high-flow nasal cannula oxygen therapy; LUS, lung ultrasound; PACU, post-anesthesia care unit; PCIA, patient-controlled intravenous analgesia; PEEP, positive end-expiratory pressure; PPCs, postoperative pulmonary complications; SD, standard deviation; SpO2, pulse oxygen saturation.
Data Sharing Statement
The datasets are available from the corresponding author Jian-Gang Song on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by China Ethics Committee of Registering Clinical Trails (ChiECRCT20210263; date of approval: July 20, 2021) and was registered at Chinese Clinical Trial Registry (ChiCTR2100047235; date of registration: 11/06/2021). Written informed consent was obtained from all participants. This study adhered to the CONSORT guidelines, and all methods were carried out in accordance with the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge all the participants in this study.
Funding
This study was supported by National Natural Science Foundation of China (No. 81973652), Shanghai University of Traditional Chinese Medicine budget project (No. 2021LK082) and Shanghai Traditional Chinese Medicine “Three-year Action Plan” [No. ZY (2021-2023)-0211].
Disclosure
The authors declare that they have no competing interests.
References
1. Fernandez-Bustamante A, Frendl G, Sprung J, et al. Postoperative Pulmonary Complications, Early Mortality, and Hospital Stay Following Noncardiothoracic Surgery: a Multicenter Study by the Perioperative Research Network Investigators. JAMA Surgery. 2017;152(2):157–166. doi:10.1001/jamasurg.2016.4065
2. Yang Y, Geng Y, Zhang D, Wan Y, Wang R. Effect of Lung Recruitment Maneuvers on Reduction of Atelectasis Determined by Lung Ultrasound in Patients More Than 60 Years Old Undergoing Laparoscopic Surgery for Colorectal Carcinoma: a Prospective Study at a Single Center. Med Sci Monit. 2021;27:e926748. doi:10.12659/MSM.926748
3. Kendall F, Oliveira J, Peleteiro B, Pinho P, Bastos PT. Inspiratory muscle training is effective to reduce postoperative pulmonary complications and length of hospital stay: a systematic review and meta-analysis. Disabil Rehabil. 2018;40(8):864–882. doi:10.1080/09638288.2016.1277396
4. Duggan M, Kavanagh BP. Atelectasis in the perioperative patient. Curr Opin Anaesthesiol. 2007;20(1):37–42. doi:10.1097/ACO.0b013e328011d7e5
5. Andersson LE, Bååth M, Thörne A, Aspelin P, Odeberg-Wernerman S. Effect of carbon dioxide pneumoperitoneum on development of atelectasis during anesthesia, examined by spiral computed tomography. Anesthesiology. 2005;102(2):293–299. doi:10.1097/00000542-200502000-00009
6. Regli A, Habre W, Saudan S, Mamie C, Erb TO, von Ungern-Sternberg BS; Swiss Paediatric Respiratory Research Group. Impact of Trendelenburg positioning on functional residual capacity and ventilation homogeneity in anaesthetised children. Anaesthesia. 2007;62(5):451–455. doi:10.1111/j.1365-2044.2007.05030.x
7. Frat JP, Thille AW, Mercat A, et al.; FLORALI Study Group; REVA Network. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185–2196. doi:10.1056/NEJMoa1503326
8. Ritchie JE, Williams AB, Gerard C, Hockey H. Evaluation of a humidified nasal high-flow oxygen system, using oxygraphy, capnography and measurement of upper airway pressures. Anaesth Intensive Care. 2011;39(6):1103–1110. doi:10.1177/0310057X1103900620
9. Lee JH, Ji SH, Jang YE, Kim EH, Kim JT, Kim HS. Application of a High-Flow Nasal Cannula for Prevention of Postextubation Atelectasis in Children Undergoing Surgery: a Randomized Controlled Trial. Anesth Analg. 2021;133(2):474–482. doi:10.1213/ANE.0000000000005285
10. Ferrando C, Puig J, Serralta F, et al. High-flow nasal cannula oxygenation reduces postoperative hypoxemia in morbidly obese patients: a randomized controlled trial. Minerva Anestesiol. 2019;85(10):1062–1070. doi:10.23736/S0375-9393.19.13364-0
11. Xia M, Li W, Yao J, et al. A postoperative comparison of high-flow nasal cannula therapy and conventional oxygen therapy for esophageal cancer patients. Ann Palliat Med. 2021;10(3):2530–2539. doi:10.21037/apm-20-1539
12. Tinguely P, Badenoch A, Krzanicki D, et al.; ERAS4OLT.org Working Group. The role of early extubation on short-term outcomes after liver transplantation - A systematic review, meta-analysis and expert recommendations. Clin Transplant. 2022;36(10):e14642. doi:10.1111/ctr.14642
13. Acosta CM, Maidana GA, Jacovitti D, et al. Accuracy of transthoracic lung ultrasound for diagnosing anesthesia-induced atelectasis in children. Anesthesiology. 2014;120(6):1370–1379. doi:10.1097/ALN.0000000000000231
14. Monastesse A, Girard F, Massicotte N, Chartrand-Lefebvre C, Girard M. Lung Ultrasonography for the Assessment of Perioperative Atelectasis: a Pilot Feasibility Study. Anesth Analg. 2017;124(2):494–504. doi:10.1213/ANE.0000000000001603
15. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
16. Lu X, Wu C, Gao Y, Zhang M. Bedside Ultrasound Assessment of Lung Reaeration in Patients With Blunt Thoracic Injury Receiving High-Flow Nasal Cannula Oxygen Therapy: a Retrospective Study. J Intensive Care Med. 2020;35(10):1095–1103. doi:10.1177/0885066618815649
17. Xirouchaki N, Kondili E, Prinianakis G, Malliotakis P, Georgopoulos D. Impact of lung ultrasound on clinical decision making in critically ill patients. Intensive Care Med. 2014;40(1):57–65. doi:10.1007/s00134-013-3133-3
18. Yu X, Zhai Z, Zhao Y, et al. Performance of Lung Ultrasound in Detecting Peri-Operative Atelectasis after General Anesthesia. Ultrasound Med Biol. 2016;42(12):2775–2784. doi:10.1016/j.ultrasmedbio.2016.06.010
19. Gunnarsson L, Tokics L, Gustavsson H, Hedenstierna G. Influence of age on atelectasis formation and gas exchange impairment during general anaesthesia. Br J Anaesth. 1991;66(4):423–432. doi:10.1093/bja/66.4.423
20. Parke R, McGuinness S, Eccleston M. Nasal high-flow therapy delivers low level positive airway pressure. Br J Anaesth. 2009;103(6):886–890. doi:10.1093/bja/aep280
21. Zochios V, Klein AA, Jones N, Kriz T. Effect of High-Flow Nasal Oxygen on Pulmonary Complications and Outcomes After Adult Cardiothoracic Surgery: a Qualitative Review. J Cardiothorac Vasc Anesth. 2016;30(5):1379–1385. doi:10.1053/j.jvca.2015.12.023
22. Shen J, An Y. 拔除气管导管后患者的经鼻高流量吸氧治疗 [High flow nasal cannula in patients after trachea extubation]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017;29(1):85–89. doi:10.3760/cma.j.issn.2095-4352.2017.01.019 Chinese.
23. MacIntyre NR. Humidified High-Flow Nasal Cannula Oxygen-More Than Just Supplemental Oxygen. Crit Care Med. 2017;45(12):2103–2104. doi:10.1097/CCM.0000000000002725
24. Schindler MB. Treatment of atelectasis: where is the evidence? Crit Care. 2005;9(4):341–342. doi:10.1186/cc3766
25. Hedenstierna G, Rothen HU. Respiratory function during anesthesia: effects on gas exchange. Compr Physiol. 2012;2(1):69–96. doi:10.1002/cphy.c080111
26. Kumar GV, Nair AP, Murthy HS, Jalaja KR, Ramachandra K, Parameshwara G. Residual neuromuscular blockade affects postoperative pulmonary function. Anesthesiology. 2012;117(6):1234–1244. doi:10.1097/ALN.0b013e3182715b80
27. Wang R, Li HC, Li XY, et al. Modified high-flow nasal cannula oxygen therapy versus conventional oxygen therapy in patients undergoing bronchoscopy: a randomized clinical trial. BMC Pulm Med. 2021;21(1):367. doi:10.1186/s12890-021-01744-8
28. Wang Y, Zhu J, Wang X, et al. Comparison of High-flow Nasal Cannula (HFNC) and Conventional Oxygen Therapy in Obese Patients Undergoing Cardiac Surgery: a Systematic Review and Meta-analysis. Vivo. 2021;35(5):2521–2529. doi:10.21873/invivo.12533
29. Yu Y, Qian X, Liu C, Zhu C. Effect of High-Flow Nasal Cannula versus Conventional Oxygen Therapy for Patients with Thoracoscopic Lobectomy after Extubation. Can Respir J. 2017;2017:7894631. doi:10.1155/2017/7894631
30. Chikata Y, Onodera M, Oto J, Nishimura M. FIO2 in an Adult Model Simulating High-Flow Nasal Cannula Therapy. Respir Care. 2017;62(2):193–198. doi:10.4187/respcare.04963
31. Masclans JR, Pérez-Terán P, Roca O. The role of high flow oxygen therapy in acute respiratory failure. Med Intensiva. 2015;39(8):505–515. doi:10.1016/j.medin.2015.05.009
32. Lu Z, Chang W, Meng S, et al. The Effect of High-Flow Nasal Oxygen Therapy on Postoperative Pulmonary Complications and Hospital Length of Stay in Postoperative Patients: a Systematic Review and Meta-Analysis. J Intensive Care Med. 2020;35(10):1129–1140. doi:10.1177/0885066618817718
33. Nimmagadda U, Salem MR, Crystal GJ. Preoxygenation: physiologic Basis, Benefits, and Potential Risks. Anesth Analg. 2017;124(2):507–517. doi:10.1213/ANE.0000000000001589
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.