Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Randomized Clinical Trial Examining the Impact of Lactobacillus rhamnosus GG Probiotic Supplementation on Cognitive Functioning in Middle-aged and Older Adults
Authors Sanborn V, Azcarate-Peril MA ![]() , Updegraff J, Manderino L, Gunstad J
, Updegraff J, Manderino L, Gunstad J
Received 1 July 2020
Accepted for publication 2 September 2020
Published 13 November 2020 Volume 2020:16 Pages 2765—2777
DOI https://doi.org/10.2147/NDT.S270035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Victoria Sanborn,1 M Andrea Azcarate-Peril,2 John Updegraff,1 Lisa Manderino,1 John Gunstad1,3
1Department of Psychological Sciences, Kent State University, Kent, OH, USA; 2Department of Cell Biology and Physiology and Microbiome Core Facility, UNC School of Medicine, Chapel Hill, North Carolina, USA; 3Brain Health Research Institute, Kent State University, Kent, OH, USA
Correspondence: Victoria Sanborn
Kent State University, Kent, OH, USA
Tel +1 508-344-3215
Fax +1 330-672-3786
Email [email protected]
Purpose: The gut microbiome has been linked to cognitive function and appears to worsen with aging. Probiotic supplementation has been found to improve the health of the gut microbiome. As such, it is possible that probiotic supplementation may protect the aging brain. The current study examined the cognitive benefits of probiotic supplementation (Lactobacillus rhamnosus GG) in healthy middle-aged and older adults.
Materials and Methods: The study was a double-blind, placebo-controlled, randomized clinical trial. Two hundred community-dwelling adults aged 52– 75 were enrolled (mean age=64.3, SD=5.52). A three-month intervention involved daily consumption of probiotic or placebo. Independent sample t-tests, chi-squared tests, and repeated measure ANOVAs compared groups and examined changes over time. Primary outcome was change in NIH Toolbox Total Cognition Score from baseline to follow-up.
Results: A total of 145 participants were examined in primary analyses (probiotic=77, placebo=68) and excluded persons due to discontinuation, low adherence, missing data, or outlier values. Established criteria (ie ≥ 1 subtest t-scores ≤ 35; n=19, n=23) were used to operationally define cognitive impairment. Repeated measures ANOVAs revealed that persons with cognitive impairment who consumed probiotics exhibited a greater total cognition score improvement than persons with cognitive impairment in the placebo group and cognitively intact persons in probiotic or placebo groups.
Conclusion: Lactobacillus rhamnosus GG probiotic supplementation was associated with improved cognitive performance in middle-aged and older adults with cognitive impairment. Probiotic supplementation may be a novel method for protecting cognitive health in aging.
Keywords: cognitive aging, dementia, microbiota, gastrointestinal microbiome, probiotics
Introduction
Cognitive Aging
Decline in mental abilities is normal with advancing age and coincides with changes in brain structure and function, including reductions in global and regional brain volume.1–4 These changes are known to be mitigated by education5 and physical activity,6 though cognitive aging cannot be avoided.
Gut Microbiota as Risk Factor for Cognitive Decline
There is increasing reason to believe that gut microbiota may be an important contributor to cognitive aging.7,8 The term gut microbiota refers to the 10–100 trillion symbiotic microbial cells living in the human gut and the term gut microbiome refers to the catalog of their nucleic acids (DNA and RNA molecules).9 Four major phyla of gut bacteria are present in mammals, namely: Bacteroidetes, Proteobacteria, Actinobacteria, and Firmicutes, identified through microbial DNA sequencing.10 The primary microbial phyla in humans are Firmicutes and Bacteroidetes and comprise up to 90% of our gut microbiome.11 Dysbiosis refers to a state of the gut microbiota in which the proportions of bacteria are atypical, resulting in a disease-promoting state.12 Gut dysbiosis can be readily detected in both human and animal models, including the comparison of stool samples of lean with obese individuals or individuals who eat a healthy diet with those who eat a high fat/Western diet.13,14 More importantly, gut dysbiosis has been associated with a number of medical conditions including inflammatory bowel disease (IBD),15,16 cardiovascular disease,17 metabolic disorders,18,19 and autoimmune disorders,20,21 each of which has been associated with poorer cognitive function.22–25 Further, the aging process is associated with progressive decline in gut microbiota diversity and proportions of core microbiota.26
Gut-brain-microbiome Axis
The gut, the gut microbiota, and the brain form an interconnected system of processes and communication referred to as the gut-brain-microbiome axis. This complex system involves bidirectional signaling through several pathways, including immune responses,27 the vagus nerve,28 enteroendocrine cells,29 and metabolites that influence the production of neurotransmitters.30 These pathways provide signaling information among microbiota, the gut, and the brain regarding a wide range of processes, including inflammation and satiety, as well as complex behaviors like social isolation or repetitive movement.31 The gut microbiota appears to influence the brain by altering axis signaling through bile acids,7,32 inflammatory markers,31,33 and metabolites.31,34 These altered signals lead to changes in key neurochemical processes. Certain bile acids have been associated with brain volume, amyloid beta deposition,7 and later development of Alzheimer’s disease.35 Short-chain fatty acid (SCFA) metabolites modulate neurotransmission impacting synthesis of noradrenaline and dopamine,30 and also induce neuronal nerve activation.34
Can Probiotics Improve Cognitive Function?
Given the influence of the gut microbiome on the brain, modification of the gut microbiome through probiotic supplementation may protect against cognitive impairment. Probiotics are living microorganisms which, when administered, provide health benefit to the host.36 Fermented foods can contain beneficial bacteria, which could be considered probiotics. Those include sauerkraut, pickles, yogurt, and miso,37 though the ease and convenience of taking probiotic supplements containing larger proportions of bacteria appears to be more appealing for some individuals.10
A particularly promising strain of probiotic is Lactobacillus rhamnosus GG. This bacterium is known for its rapid growth, adhesive properties, and bile resistance38 allowing it to remain in the gut longer and exert a greater influence than other strains, including protecting the gut lining.39 Along the gut-brain-microbiome axis, strains of Lactobacillus probiotics have been associated with reduced inflammatory cytokines,40 enhanced levels of cAMP response element binding protein (CREB) and brain derived neurotrophic factor (BDNF) in the hippocampus of rats,41 and reduced kynurenine metabolites.42 Lactobacillus rhamnosus GG itself has been found to protect intestinal epithelial cells43 and reduce inflammatory markers such as interleukin-8 (IL-8).44 It has also been found to improve metabolic factors including glucose tolerance, insulin-sensitivity, adiposity,45 and inflammation.46,47 Through these direct and indirect mechanisms, Lactobacillus rhamnosus GG may impact brain health and cognitive function. In fact, Lactobacillus rhamnosus GG supplementation has been associated with reduced anxiety-like,48 obsessive compulsive disorder-like,49 and depressive behaviors50 in mouse models and has been associated with reduced risk of developing neuropsychiatric disorders in children.51
Although previous research has examined the role of Lactobacillus rhamnosus GG on physical and psychological outcomes, little is known about its potential impact on cognitive function. One RCT examined the possible cognitive benefits of eight weeks of Lactobacillus rhamnosus GG supplementation on cognitive function in young adult males. No significant changes for inflammatory markers, stress-related anxiety behaviors, or performance on cognitive function were shown in that sample.52 However, cognitive improvement in a healthy young sample may be unlikely due to range restriction and further investigation on the effects of Lactobacillus rhamnosus GG in samples of persons at risk for cognitive impairment is needed.
Current Study
The current study investigated whether Lactobacillus rhamnosus GG probiotic supplementation could be associated with improved cognitive function in community-dwelling middle-aged and older adults. Two hundred individuals were recruited into a double-blind RCT. Cognitive function was assessed at baseline and following three months of supplementation of either probiotic or placebo. It was hypothesized that Lactobacillus rhamnosus GG supplementation would be associated with improvements in cognitive performance both in persons with and without evidence of cognitive impairment.
Materials and Methods
All data was obtained in compliance with the regulations set forth by the Kent State University Institutional Review Board (approval no. #16-321) and was conducted in accordance with the Declaration of Helsinki. All participants were informed of the purpose of the study. Recruitment and data collection were partly financially supported by i-Health, Inc., a division of Royal DSM. All participants provided written consent acknowledging that any published work would not include identifying information. Participant data has been fully anonymized. All safety precautions (ie university physician oversight, adverse event reporting, eligibility screening for individuals at risk for physical discomfort/symptom exacerbation by probiotic use, participant written agreement to discuss with treating physician before participation) were determined prior to study onset, approved by the Kent State University Institutional Review Board, and adhered to throughout the project. Study methods have been described in detail previously.53 Briefly, we conducted a parallel, double-blind, placebo controlled, RCT with a 1:1 allocation ratio. See Supplementary Table 1. The study was listed in advance of participant recruitment through clinicaltrials.gov (study no. NCT03080818). Two hundred healthy, middle-aged and older adults (aged 52–75) were recruited from the local community through fliers and advertisements. Sample size was predetermined through power analyses using G*Power 3.0.10 software.
Persons were excluded if they reported history of developmental, neurological, or severe psychiatric disorder, recent consumption of antibiotics, acid-blocking medication, prebiotic, or probiotic supplements, past alcohol or illicit drug dependence, history of severe heart, liver, or kidney problems, immunosuppression, or severe gastrointestinal conditions. Participants were randomized to a study group using a computerized number generator by the principal investigator (JG). The principal investigator was the only staff member aware of participant group assignment and prepared capsules for distribution in advance using unmarked containers. Other research staff, responsible for recruitment and study testing, and participants were blind to group assignment by using unmarked containers and restricted access to randomization documentation. To increase similarity between control and intervention procedures, all participants completed the same study protocol and placebo and probiotic capsules were identical in appearance and packaging.
Lactobacillus rhamnosus GG was selected for two reasons. Although previous research has encouraged the use of multi-strain probiotic supplementation,54 it is unclear whether Lactobacillus rhamnosus GG as a single-strain or multi-strain confers greater benefit for physical and psychological outcomes.55 Examining Lactobacillus rhamnosus GG in isolation also allowed examination of its independent effects on cognitive function, which would be difficult to accomplish in the presence of other probiotic strains. Intervention included Culturelle Vegetarian Capsules containing a 10 billion CFU blend of Lactobacillus rhamnosus GG (manufactured by iHealth, Inc., Cromwell, CT, USA) for the experimental group and Culturelle Placebo Veggie capsules containing microcrystalline cellulose for the control group. Participants were instructed to take two capsules daily.
For the study, participants completed telephone eligibility screening, baseline testing, two adherence visits, and follow-up testing. Study visits were conducted at a local retirement community in Northeastern Ohio to promote convenience . Participants were enrolled for approximately 90 days including baseline visit, adherence visits once a month for the following two months and follow-up visit. Baseline and follow-up visits involved brief medical interview, physical measures, computerized neuropsychological assessment using the NIH Toolbox Assessment of Neurological and Behavioral Function—Cognition battery, provision of capsules, and compensation. The NIH Toolbox Total Cognition Score (ie composite index score based on age, sex, education, race, and mother’s education reflecting performance on all cognitive subtests) was used as the primary outcome. NIH Toolbox was selected for its strong psychometric properties,56,57 close association with traditional pencil-and-paper neuropsychological tests,58 and ability to assess healthy samples like those found in the current study.
Adherence visits involved brief medical interview, count of nonconsumed capsules, provision of new capsules, and compensation. Study adherence was calculated by dividing self-reported number of capsules consumed by total number of capsules provided and multiplying that value by 100 to obtain a percentage. The primary outcome was the possible change in cognitive function at follow-up across persons randomized to probiotic vs placebo.
Data Analysis
Preliminary Analyses
All participants with missing data, low adherence (ie <80%), and/or incomplete study visits were excluded from analyses. Normality was assumed for variables with skewness <2.0 and kurtosis <6.0. Potential outliers were identified by examining boxplot graphs and clarified using the approach proposed by Iglewicz and Hoalgin59 for each variable (ie creating zmodified transformation scores and removing any values >3.5). Per protocol (PP) and intention-to-treat (ITT) analyses were conducted to determine any significant difference in dropout rates between probiotic and placebo groups.60,61 To identify possible between-group differences between those who were retained or excluded, independent samples t-tests and chi-squared tests compared groups on age, education, sex, BMI, ethnicity, medical history (ie diabetes, hypertension, sleep apnea, anxiety/depression) and baseline NIH Toolbox scores. Finally, Petersen/Winblad criteria (ie one or more NIH Toolbox t scores at or below 35) was used to operationally define cognitive impairment using baseline test results including subtest scores and total composite score.
Hypothesis Testing
A 2 (probiotic vs placebo)⨰2 (cognitive impairment vs intact)⨰2 (baseline to follow-up) repeated measures ANOVA was used to identify possible changes in total cognition score over time by the cognitive group. This analysis was then repeated for each individual NIH Toolbox subtest score to clarify any significant omnibus test.
The effect of time, intervention group, and cognitive status were examined independently, as well as multiple interactions (ie time⨰group, time⨰cognitive status, time⨰group⨰cognitive status).
To minimize potential impact of practice effects, reliable change indices (RCI; ie standardized z-scores) were calculated for individual subtest scores and total cognition score for each of the four final subgroups (ie probiotic vs placebo and intact vs impaired).62 Steps for these calculations included: (1) calculation of standard error values for each cognition score using the square root of 1 minus the published reliability of each test,61 (2) calculation of standard error of the difference values for each cognition score using the square root of two times the squared value of the standard error, and (3) calculation of the absolute value of change in each score divided by the standard error of the difference. RCIs (ie, z-scores reflecting standardized amount of change) calculated for subtest and total cognition scores with an absolute value greater than 1.96, reflecting less than 5% chance that scores were due to standard error,62 were considered to reflect significant change.
Results
Data Cleaning
Recruitment began in May 2017 and ended in September 2019. From the original sample of 200 participants, data from 52 individuals were excluded from primary analyses due to discontinuation (n=15), missing cognitive data (n=28), missing medical history data (n=2), or low compliance (ie <80%; n=7). Reasons for study discontinuation included reported gastrointestinal symptoms (n=6), extenuating personal circumstances (n=1), starting antibiotics (n=1), abnormal liver enzyme panel (n=1), or lost to follow-up (n=6). See Figure 1. At the entire group level (n=148), no outliers for cognitive scores were identified (all zmodified <3.5). When examining intervention groups separately (nprobiotic=78, nplacebo=70), one outlier was identified and removed from the probiotic group. When examining those with evidence of cognitive impairment (n=44), two outliers were identified and removed. See Table 1 for demographic and medical characteristics of retained study participants (n=145; nprobiotic=77, nplacebo=68).
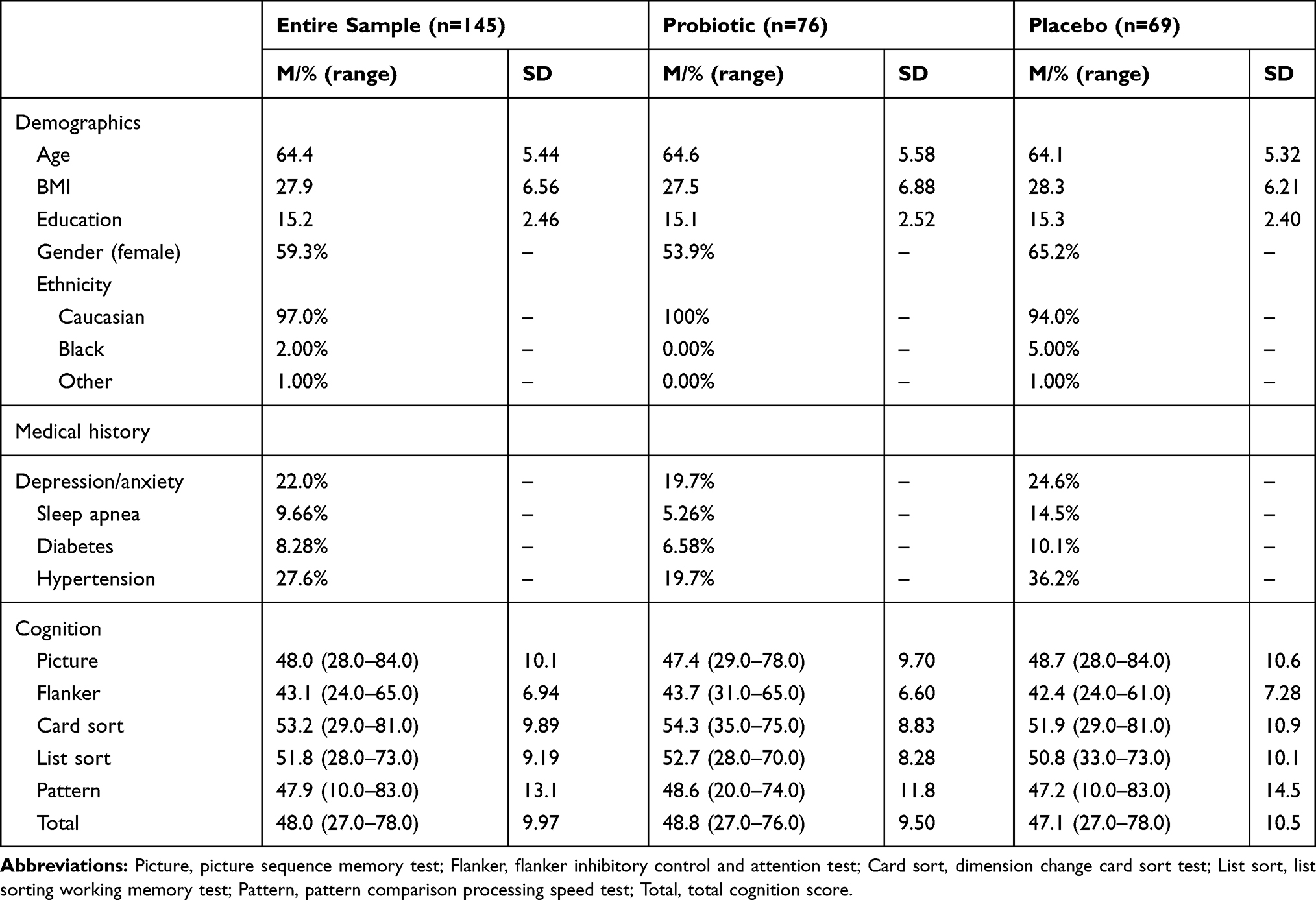 |
Table 1 Demographic, Medical, and Cognitive Characteristics by Study Group (n=145) |
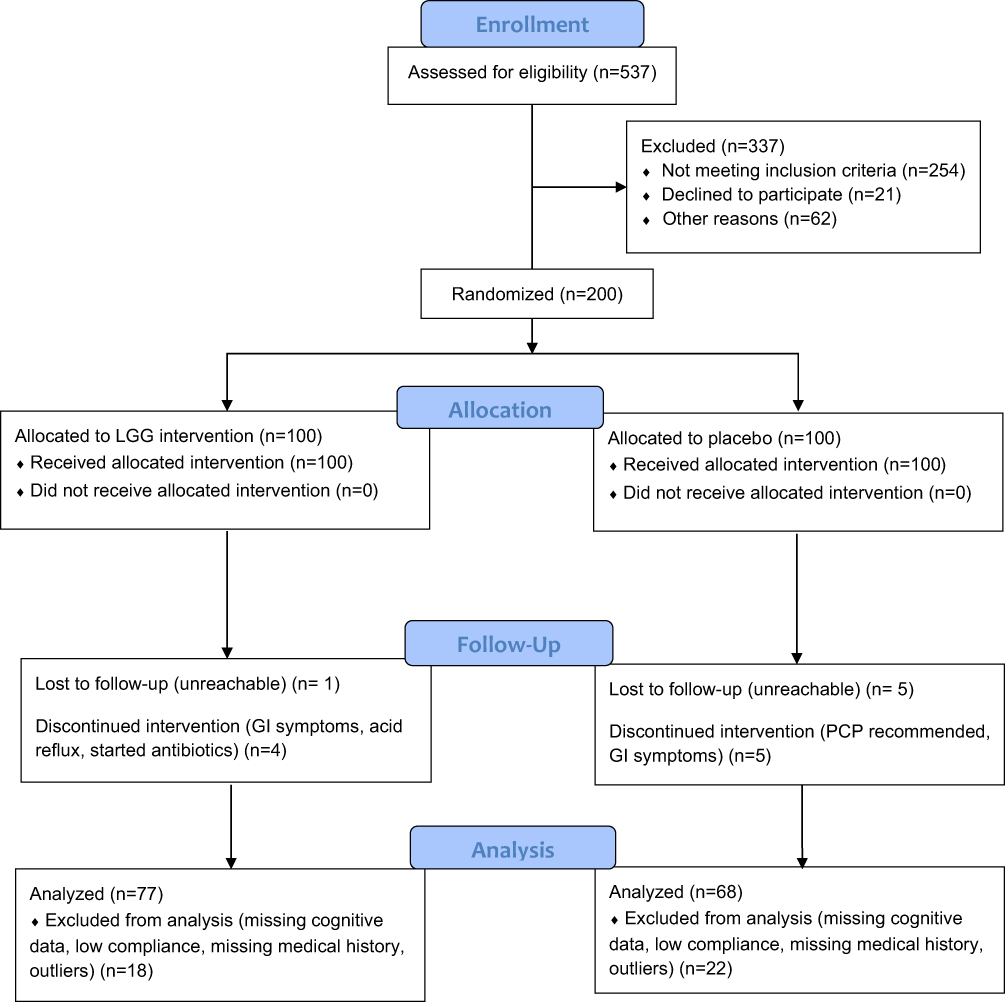 |
Figure 1 CONSORT (Consolidated Standards of Reporting Trials) flowchart. 2010 CONSORT Flow Diagram, Adapted from Schulz, KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Obstet Gynecol. 2010;115(5):1063–70.63 |
Of the 55 participants excluded from primary analyses, all had complete data for age, education, ethnicity and gender while only 45 had complete data for BMI, 34 had complete data for cognitive subtests, and 32 had complete data for total cognition score. Incomplete cognitive data was due to a malfunction with a tablet used to administer testing. Excluded participants were not significantly different from included participants in demographic, medical, or cognitive function characteristics (all p>0.05; See Table 2).
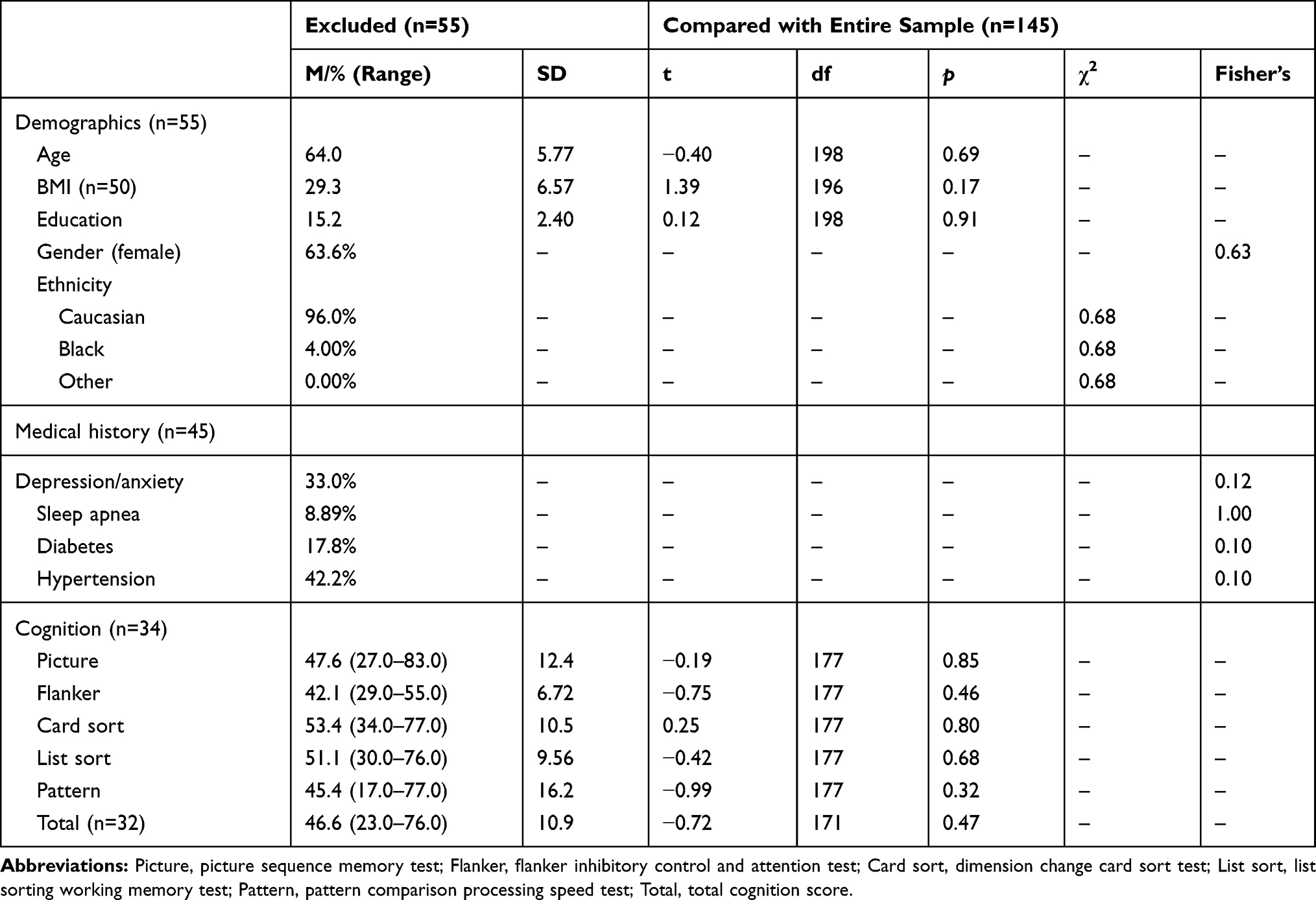 |
Table 2 Comparing Participants Who Were Excluded or Included in the Study |
Sample Characteristics
PP analysis showed that no differences in dropout rates emerged between probiotic (6%) and placebo groups (13%). This was confirmed through ITT analysis, which showed comparable dropout rates between probiotic (5%) and placebo groups (10%). These results suggest Lactobacillus rhamnosus GG was well-tolerated (p>0.05).
Within the probiotic supplementation group, participants that dropped out (M=13.0, SD=0.71) reported fewer years of education than those who completed the study (M=15.1, SD=2.59; t=4.95, df=13.2, p<0.01). No other differences emerged in demographic, medical, or cognitive variables (all p>0.05). Similarly, no differences emerged within the placebo group between those that dropped or remained (all p>0.05).
In the entire sample (n=145), there was a higher proportion of participants in the placebo group (36%) reporting hypertension than participants in the probiotic group (19%; p=0.02, Fisher’s exact test). No differences emerged between probiotic and placebo groups for other variables of interest (all p>0.05; See Table 1). A significantly greater portion of participants with objective evidence of cognitive impairment (n=42) reported history of sleep apnea compared with cognitively intact participants (n=103). No other differences emerged between cognitively impaired and intact participants on medical or demographic characteristics (all p>0.05; See Table 3).
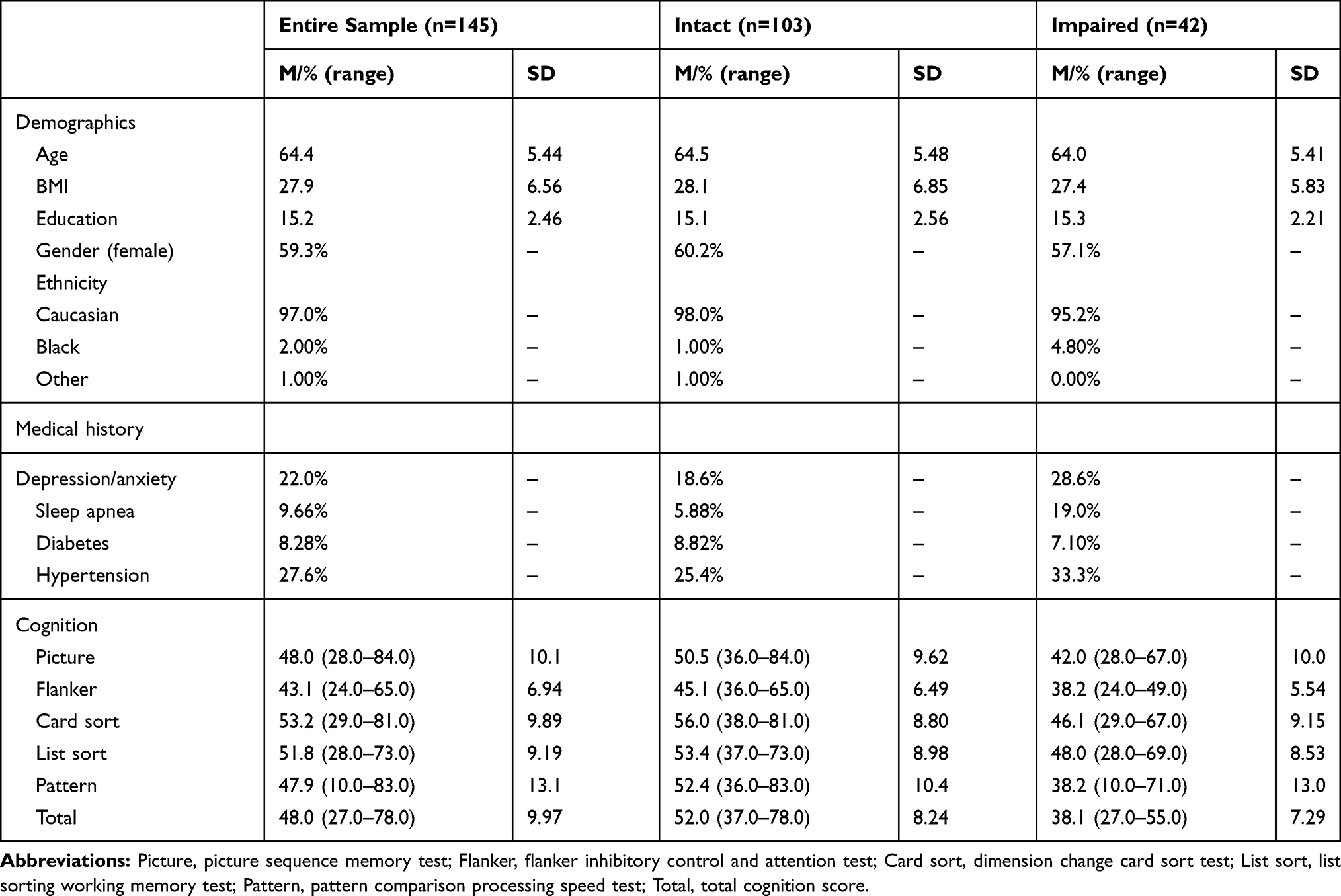 |
Table 3 Demographic, Medical, and Cognitive Characteristics by Cognitive Status (n=145) |
ITT analyses largely replicated PP analyses regarding baseline comparisons between intervention groups. For those with complete data, a significantly greater portion of participants in the placebo group had hypertension (40%) and sleep apnea (14%) than those in the probiotic group (23% and 6%). No significant differences in other demographic or medical characteristics emerged (all p> 0.05).
It was noted that though no participants reported taking medications that met exclusion criteria for the current trial (eg antibiotics, prebiotics), number of self-reported medications and supplements ranged from 0 to 13 in the total sample; for participants with cognitive impairment, 13 participants in the probiotic group and 16 in the probiotic group reported taking medications beyond vitamins/supplements. The most common medications included statins, beta-blockers, metformin, antidepressants, anxiolytics, nonsteroidal anti-inflammatories, and pain medications. Groups did not differ on the prevalence of medications and it was not utilized in primary analyses.
Lactobacillus rhamnosus GG Improves Cognition in Persons with Cognitive Impairment
PP analyses using repeated measures ANOVA found a significant group by cognitive status by time interaction for total cognition score (F[1,141]=4.60, p=0.03, ηp2=0.03); see Table 4. Though all groups improved from baseline to follow-up, participants with cognitive impairment in the probiotic group (Mbaseline=38.7, Mfollow-up=47.6) showed significantly greater improvement in total cognition score than participants with cognitive impairment in the placebo group (Mbaseline=37.7, Mfollow-up=42.4) and participants without cognitive impairment in the probiotic (Mbaseline=52.1, Mfollow-up=54.5) and placebo (Mbaseline=51.8, Mfollow-up=54.6) groups. When comparing change in total cognition score from baseline to follow-up to RCI estimates, it was discovered that change in total cognition score was reliable for participants with cognitive impairment in the probiotic group (RCI=2.07) but not for any other group (cognitive impairment-placebo, RCI=1.34; intact-probiotic RCI=0.54; intact-placebo, RCI=0.63). See Tables 5 and 6.
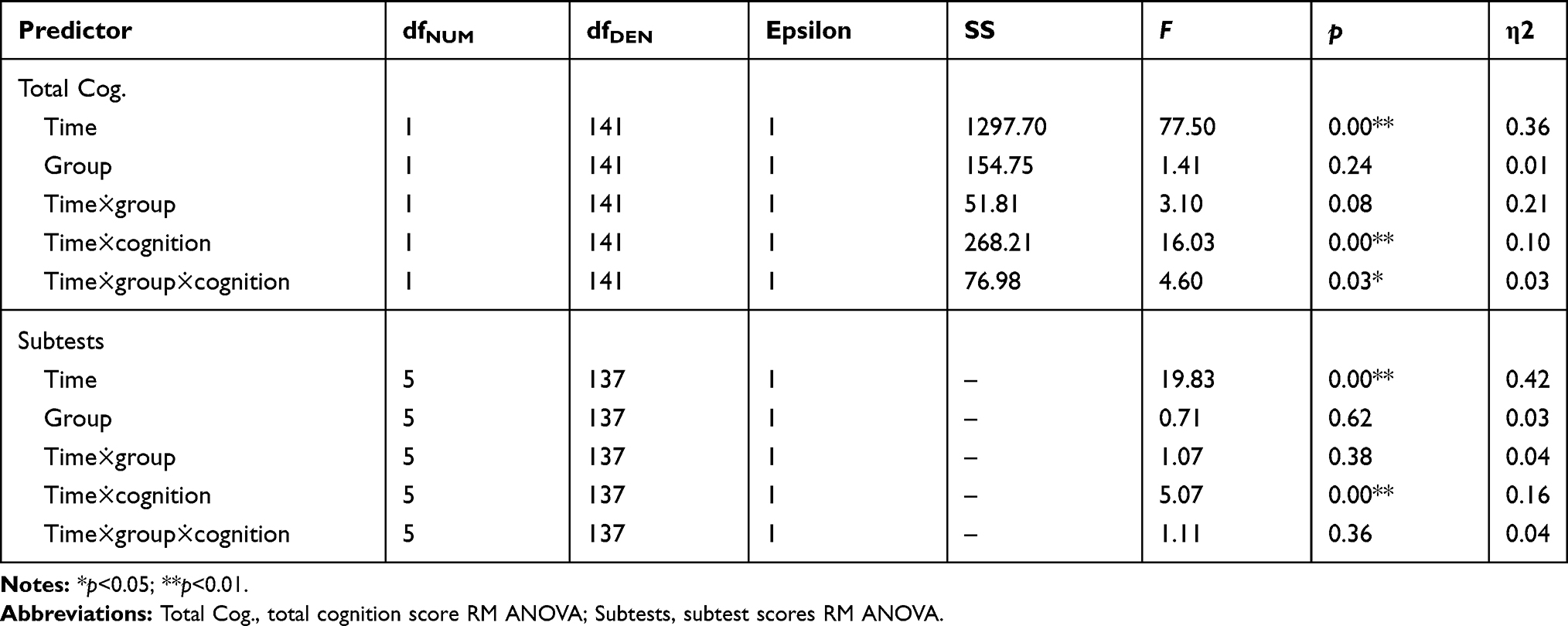 |
Table 4 RM ANOVAs Examining Effect of Study Group and Cognitive Status on Total Cognition Score and Subtest Scores |
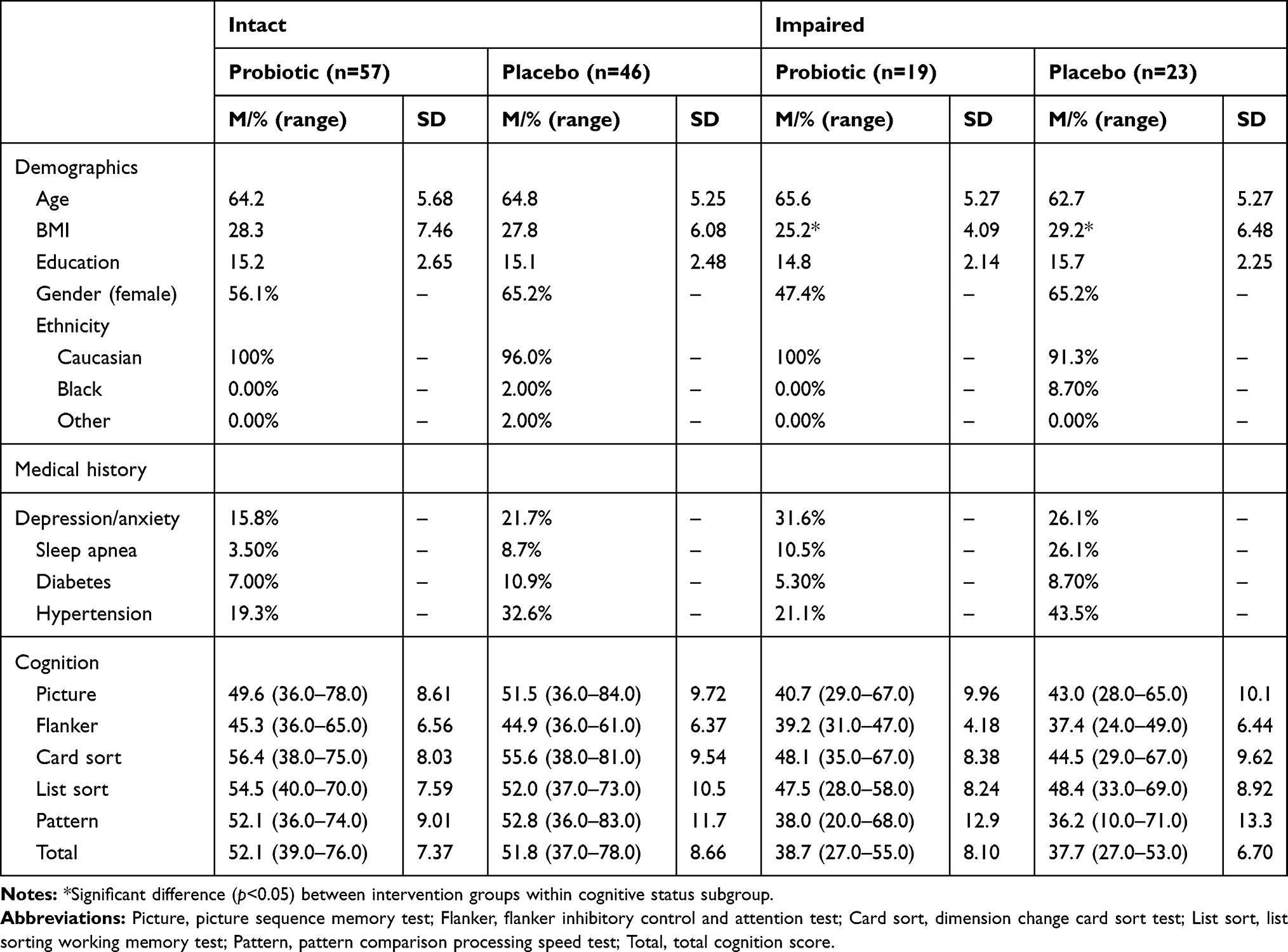 |
Table 5 Demographic, Medical, and Cognitive Characteristics of Intervention by Cognitive Status Groups |
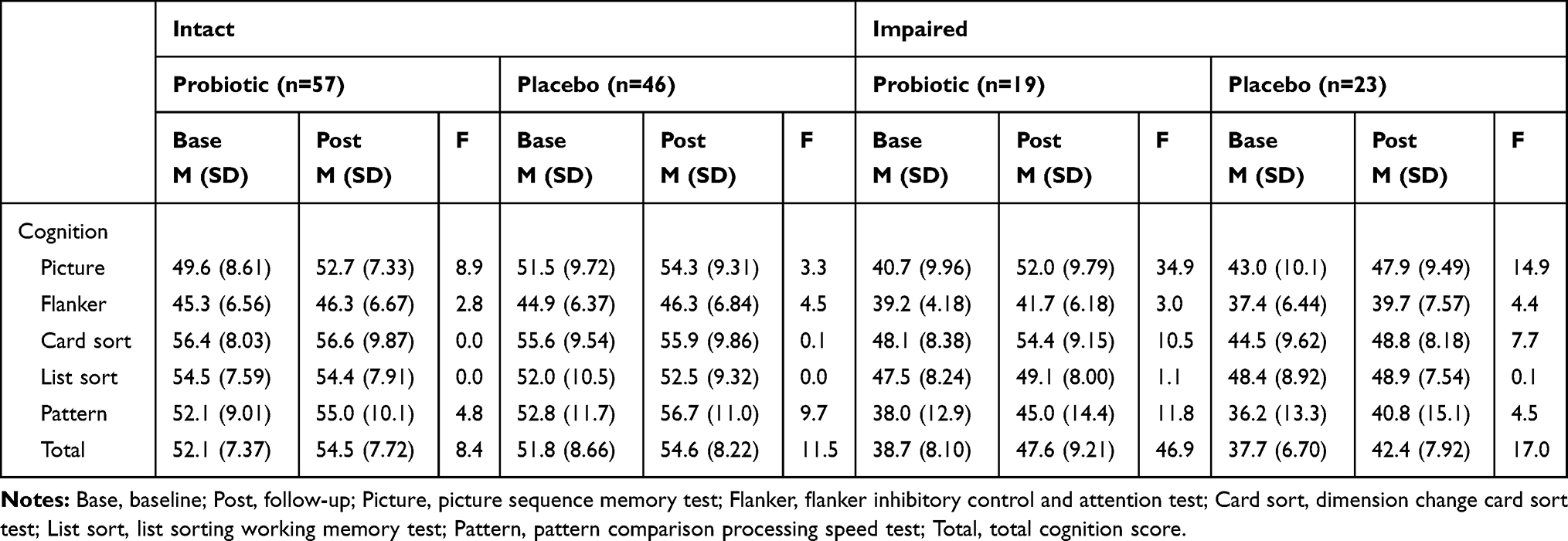 |
Table 6 Baseline and Follow-up Cognitive Test Scores of Intervention by Cognitive Status Groups |
To clarify this improvement on the total cognition score, repeated measures ANOVA were performed for specific subtests from the NIH Toolbox. No group by cognitive status by time interaction emerged (p>0.05).
ITT analyses using the carry-forward method (ie, inserting baseline values for missing outcome values63) largely corroborated these findings. Repeated measures ANOVA (n=173) showed a borderline significant group by time by cognitive status interaction (F[1,169]=3.90, p=0.05, ηp2=0.02), such that impaired persons in the probiotic group (Mbaseline=39, Mfollow-up=46) showed greater improvement in cognitive performance than impaired persons in the placebo group (Mbaseline=37, Mfollow-up=42), intact persons in the probiotic group (Mbaseline=53, Mfollow-up=54), and intact persons in the placebo group (Mbaseline=51, Mfollow-up=54). No group by cognitive status by time interaction was identified (>0.05).
Discussion
Summary of Findings
The current study examined the possible cognitive benefits of Lactobacillus rhamnosus GG in a sample of healthy middle-aged and older adults. Results showed that Lactobacillus rhamnosus GG supplementation was associated with improvement in total cognition score in persons with objective evidence of cognitive impairment, though no such effect emerged in persons with intact cognitive function or those randomized to placebo. Several aspects of these findings warrant brief discussion.
Test Improvement in Persons with Cognitive Dysfunction
The exact reason for finding cognitive benefits of Lactobacillus rhamnosus GG in persons with cognitive impairment, but not those with normal cognitive function, is unclear. One possible explanation involves a limited capacity for improvement. At baseline, the total cognition score for the normal cognition subsample fell in the average range (M=48.0, SD=9.97). As noted above, past studies show that probiotic supplementation is associated with improved cognitive function in persons with baseline cognitive impairment64,65 but, thus far, it has been found to have limited impact in persons with intact abilities.66 Such findings suggest that probiotics may help to alleviate deficits in cognitive function (ie return to premorbid range) but may not be sufficient to improve test performance beyond that expected by an individual’s preexisting genetic and biological capacity. Further examination of this possibility—especially clarification of benefits across the adult lifespan—is much needed.
Mechanisms for Cognitive Improvement from Lactobacillus rhamnosus GG
There are also several mechanistic pathways through which Lactobacillus rhamnosus GG probiotic supplementation may improve cognitive function in at-risk individuals. Along the gut-brain-microbiome axis, the gut microbiota and the brain engage in bidirectional signaling through bile acids,7,32 metabolites,34 and immune responses.31 These means of signaling have been associated with a wide range of neurodegenerative disorders,7,35 neuronal protein expression,33 neurotransmission,29 synaptic pruning,67,68 and behavioral change.69,70 As described previously, Lactobacillus strains in particular have been found to reduce inflammatory cytokines40 and metabolites in humans,42 and enhance levels of CREB and BDNF in rats.41 As probiotics can modulate the composition and functionality of the gut microbiota, Lactobacillus rhamnosus GG could have improved these signaling markers as well—ultimately leading to better cognitive function.
It is also possible that Lactobacillus rhamnosus GG may improve cognitive function through indirect pathways. Lactobacillus rhamnosus GG specifically has been shown to improve glucose tolerance and insulin sensitivity45 and reduce inflammatory responses.46,71 As metabolic dysfunction24,72,73 and inflammatory diseases74–76 are associated with poor cognitive functioning, Lactobacillus rhamnosus GG may have indirectly improved cognitive health by reducing pathological responses associated with these conditions. Additional work is much needed to begin to clarify possible neuroprotective effects of Lactobacillus rhamnosus GG and other probiotics in aging adults.
Limitations
The current study is limited in several ways. Though concerted efforts were made, the exact number of days of supplementation differed slightly due to participant scheduling conflicts (Mdays=92, SD=5.17). As previous research has shown that the gut microbiome can change quickly,77 this variability may have subtle impact on study findings. Similarly, no gold standard for duration of probiotic supplementation has been established. Though the current study followed participants for a sufficient time to identify cognitive changes,78 it is possible that supplementation could have differential cognitive effects at other timepoints, as past work has examined effects of supplementation from as little as three weeks to as long as six months.64,79,80 As suggested above, much longer trials (eg 12–24 months) are also needed to clarify the possible protective effects of probiotic supplementation on cognitive decline in at-risk individuals. Relatedly, the absence of a no-treatment follow-up period in enrolled study participants limits the opportunity to clarify specific, acute benefits of Lactobacillus rhamnosus GG.
Another limitation is found in the use of self-report to identify psychiatric and neurodegenerative disorders. It is possible that participants denied such disorders to ensure eligibility for participation or may have been unaware that they met criteria for such diagnoses.
The observed practice effects also introduce a possible concern for the current study. Though previous research suggests that NIH Toolbox has limited practice effects,56 probiotic and placebo groups both showed improvement on testing. Though the current study methodology (including use of RCI) helps to mitigate possible confound, the possibility of test-related issues or familiarity with testing itself,81 cannot be fully ruled out. Similarly, minor differences were found between analyses that included all persons that fully adhered to study protocol vs those that did not or dropped out. This finding requires clarification in future studies, as explanations may include dose–response relationships for the cognitive benefits of probiotic supplementation or artifact due to the difficulties in adhering to study protocol in persons with cognitive dysfunction.82
A final limitation of the current study is the lack of data regarding changes in the gut microbiome during the study period. Past research concerning the effects of probiotics on cognitive and/or health outcomes have directly examined the microbiome using DNA sequencing.10,83,84 As increases/decreases of certain microbial groups have been associated with changes in a variety of health and psychological outcomes (eg increased Bacteroidetes associated with increased inflammatory responses, increased Lactobacillus associated with reduced glucoregulatory markers);69,85,86 DNA sequencing may help clarify the underlying mechanisms responsible for the observed cognitive gains. Stool samples have been collected in a subsample of participants, though are not available for analysis at the present time.
Conclusion
Persons with cognitive impairment who received Lactobacillus rhamnosus GG probiotic supplementation showed improvement on neuropsychological testing over a three-month period. These benefits emerged despite no difference in dropout rates between study arms, suggesting that Lactobacillus rhamnosus GG was well-tolerated and had no deleterious impact on health, consistent with past work.87–89 Should these findings be replicated in larger and clinical samples including persons with diagnosed neurodegenerative and neuropsychiatric conditions, probiotic supplementation may ultimately prove to be a low-risk and cost-effective approach to promote cognitive health in older adults.
Data Sharing Statement
Data from the current research study is not available for public dissemination. If others are interested in working in collaboration regarding the referenced data, requests can be made directly to the PI (Dr John Gunstad) via email ([email protected]). All data available for sharing will be de-identified.
Acknowledgment
This work was supported by i-Health, Inc., a division of Royal DSM.
Disclosure
Dr John Gunstad reports grants from DSM Royal, during the conduct of the study. The authors report no other potential conflicts of interest in this work.
References
1. Adamson MM, Samarina V, Xiangyan X, et al. The impact of brain size on pilot performance varies with aviation training and years of education. J Int Neuropsychol Soc. 2010;16:412–423. doi:10.1017/S1355617710000111
2. Chee MWL, Chen KHM, Zheng H, et al. Cognitive function and brain structure correlations in healthy elderly East Asians. NeuroImage. 2009;46:257–269. doi:10.1016/j.neuroimage.2009.01.036
3. Chee MWL, Zheng H, Goh JOS, Park D. Brain structure in young and old East Asians and Westerners: comparisons of structural volume and cortical thickness. J Cogn Neurosci. 2011;23:1065–1079. doi:10.1162/jocn.2010.21513
4. Carlesimo GA, Cherubini A, Caltagirone C, Spalletta G. Hippocampal mean diffusivity and memory in healthy elderly individuals: a cross-sectional study. Neurology. 2010;74:194–200.
5. Gupta VK, Winter M, Cabral H, et al. Disparities in age-associated cognitive decline between African-American and Caucasian populations: the roles of health literacy and education. J Am Geriatr Soc. 2016;64(8):1716–1723. doi:10.1111/jgs.14257
6. Sofi F, Valecchi D, Bacci D, et al. Physical activity and risk of cognitive decline: a meta-analysis of prospective studies. Intern Med J. 2011;269(1):107–117. doi:10.1111/j.1365-2796.2010.02281.x
7. Wilkins JM, Trushina E. Application of metabolomics in Alzheimer’s disease. Front Neurol. 2017;8:719. doi:10.3389/fneur.2017.00719
8. Manderino L, Carroll I, Azcarate-Peril MA, et al. Preliminary evidence for an association between the composition of the gut microbiome and cognitive function in neurologically healthy older adults. J Int Neuropsychol Soc. 2017;23(8):700–705. doi:10.1017/S1355617717000492
9. Ursell LK, Metcalf JL, Parfrey LW, Knight R. Defining the human microbiome. Nutr Rev. 2012;70(Suppl 1):S38–S44. doi:10.1111/j.1753-4887.2012.00493.x
10. Gulati G, Mulryan D. The psychobiotic revolution: mood, food and the new science of the gut-brain connection edited by Scott C. Anderson, John F. Cryan and Ted Dinan. ISBN 9781426218460. National geographic, Washington, DC, 2017. Ir J Psychol Med. 2017;1.
11. Dethlefsen L, McFall-Ngai M, Relman DA. An ecological and evolutionary perspective on human–microbe mutualism and disease. Nature. 2007;449(7164):811–818. doi:10.1038/nature06245
12. Tilg H, Kaser A. Gut microbiome, obesity, and metabolic dysfunction. J Clin Invest. 2011;121(6):2126–2132. doi:10.1172/JCI58109
13. Ley RE, Bäckhed F, Turnbaugh P, Lozupone CA, Knight RD, Gordon JI. Obesity alters gut microbial ecology. P Natl Acad Sci USA. 2005;102(31):11070–11075.
14. Ley RE, Turnbaugh PJ, Klein S, Gordon JI. Microbial ecology: human gut microbes associated with obesity. Nature. 2006;444(7122):1022. doi:10.1038/4441022a
15. Frank DN, Amand ALS, Feldman RA, Boedeker EC, Harpaz N, Pace NR. Molecular-phylogenetic characterization of microbial community imbalances in human inflammatory bowel diseases. Proc Natl Acad Sci. 2007;104(34):13780–13785. doi:10.1073/pnas.0706625104
16. Tong M, Li X, Parfrey LW, et al. A modular organization of the human intestinal mucosal microbiota and its association with inflammatory bowel disease. PLoS One. 2013;8(11):e80702. doi:10.1371/journal.pone.0080702
17. Tang WW, Kitai T, Hazen SL. Gut microbiota in cardiovascular health and disease. Circ Res. 2017;120(7):1183–1196. doi:10.1161/CIRCRESAHA.117.309715
18. Gérard P. Gut microbiota and obesity. Cell Mol Life Sci. 2016;73(1):147–162.
19. Lippert K, Kedenko L, Antonielli L, et al. Gut microbiota dysbiosis associated with glucose metabolism disorders and the metabolic syndrome in older adults. Benef Microbes. 2017;8(4):545–556. doi:10.3920/BM2016.0184
20. Knip M, Siljander H. The role of the intestinal microbiota in type 1 diabetes mellitus. Nat Rev Endocrinol. 2016;12:154–167. doi:10.1038/nrendo.2015.218
21. Maeda Y, Kurakawa T, Umemoto E, et al. Dysbiosis contributes to arthritis development via activation of autoreactive T cells in the intestine. Arthritis Rheum. 2016;68(11):2646–2661. doi:10.1002/art.39783
22. Kennedy PJ, Clarke G, O’Neill A, et al. Cognitive performance in irritable bowel syndrome: evidence of a stress-related impairment in visuospatial memory. Psychol Med. 2014;44(7):1553–1566. doi:10.1017/S0033291713002171
23. Harrison SL, Ding J, Tang EY, et al. Cardiovascular disease risk models and longitudinal changes in cognition: a systematic review. PLoS One. 2014;9(12):e114431. doi:10.1371/journal.pone.0114431
24. Ravona-Springer R, Heymann A, Schmeidler J, et al. Trajectories in glycemic control over time are associated with cognitive performance in elderly subjects with type 2 diabetes. PLoS One. 2014;9(6):e97384. doi:10.1371/journal.pone.0097384
25. Flanagan EP, Drubach DA, Boeve BF. Autoimmune dementia and encephalopathy. In: Handbook of Clinical Neurology. Vol. 133. Elsevier; 2016:247–267.
26. O’Toole PW, Jeffery IB. Gut microbiota and aging. Science. 2015;350(6265):1214–1215. doi:10.1126/science.aac8469
27. El Aidy S, Dinan TG, Cryan JF. Immune modulation of the brain-gut-microbe axis. Front Microbiol. 2014;5:146. doi:10.3389/fmicb.2014.00146
28. Dinan TG, Cryan JF. The impact of gut microbiota on brain and behaviour: implications for psychiatry. Curr Opin Clin Nutr Metab Care. 2015;18(6):552–558. doi:10.1097/MCO.0000000000000221
29. Latorre R, Sternini C, De Giorgio R, Greenwood-van Meerveld B. Enteroendocrine cells: a review of their role in brain-gut communication. Neurogastroenterol Motil. 2016;28(5):620–630.
30. Nankova BB, Agarwal R, MacFabe DF, La Gamma EF. Enteric bacterial metabolites propionic and butyric acid modulate gene expression, including CREB-dependent catecholaminergic neurotransmission, in PC12 cells - possible relevance to autism spectrum disorders. PLoS One. 2014;9(8):e103740. doi:10.1371/journal.pone.0103740
31. Sherwin E, Sandhu KV, Dinan TG, Cryan JF. May the force be with you: the light and dark sides of the microbiota–gut–brain axis in neuropsychiatry. CNS Drugs. 2016;30(11):1019–1041. doi:10.1007/s40263-016-0370-3
32. Schroeder BO, Bäckhed F. Signals from the gut microbiota to distant organs in physiology and disease. Nat Med. 2016;22(10):1079–1089.
33. Goehler LE, Gaykema RP, Opitz N, Reddaway R, Badr N, Lyte M. Activation in vagal afferents and central autonomic pathways: early responses to intestinal infection with Campylobacter jejuni. Brain Behav Immun. 2005;19(4):334–344. doi:10.1016/j.bbi.2004.09.002
34. De Vadder F, Kovatcheva-Datchary P, Goncalves D, et al. Microbiota-generated metabolites promote metabolic benefits via gut-brain neural circuits. Cell. 2014;156(1):84–96. doi:10.1016/j.cell.2013.12.016
35. Mapstone M, Cheema AK, Fiandaca MS, et al. Plasma phospholipids identify antecedent memory impairment in older adults. Nat Med. 2014;20(4):415–418.
36. Food and Agricultural Organization of the United Nations and World Health Organization. Health and nutritional properties of probiotics in food including powder milk with live lactic acid bacteria. World Health Organization; 2001 [Online].
37. Hutkins R. Fermented foods: live microbes and fermented foods. International scientific association for probiotics and prebiotics. 2016 Online. Available from: https://isappscience.org/fermented-foods/.
38. Doron S, Snydman DR, Gorbach SL. Lactobacillus GG: bacteriology and clinical applications. Gastroenterol Clin. 2005;34(3):483–498. doi:10.1016/j.gtc.2005.05.011
39. Segers ME, Lebeer S. Towards a better understanding of Lactobacillus rhamnosus GG–host interactions. Microb Cell Factories. 2014;13(Suppl 1):S1–S7. doi:10.1186/1475-2859-13-S1-S7
40. Lew LC, Hor YY, Yusoff NAA, et al. Probiotic Lactobacillus plantarum P8 alleviated stress and anxiety while enhancing memory and cognition in stressed adults: a randomised, double-blind, placebo-controlled study. Clin Nutr. 2019;38(5):2053–2064.
41. Lee HJ, Hwang YH, Kim DH. Lactobacillus plantarum C29-fermented soybean (DW2009) alleviates memory impairment in 5XFAD transgenic mice by regulating microglia activation and gut microbiota composition. Mol Nutr Food Res. 2018;62(20):1800359. doi:10.1002/mnfr.201800359
42. Rudzki L, Ostrowska L, Pawlak D, et al. Probiotic Lactobacillus Plantarum 299v decreases kynurenine concentration and improves cognitive functions in patients with major depression: a double-blind, randomised, placebo controlled study. Psychoneuroendocrinology. 2019;100:213–222. doi:10.1016/j.psyneuen.2018.10.010
43. Yan F, Polk DB. Probiotic bacterium prevents cytokine-induced apoptosis in intestinal epithelial cells. J Biol Chem. 2002;277(52):50959–50965. doi:10.1074/jbc.M207050200
44. Lebeer S, Claes I, Tytgat HL, et al. Functional analysis of Lactobacillus rhamnosus GG pili in relation to adhesion and immunomodulatory interactions with intestinal epithelial cells. Appl Environ Microbiol. 2012;78(1):185–193.
45. Park KY, Kim B, Hyun CK. Lactobacillus rhamnosus GG improves glucose tolerance through alleviating ER stress and suppressing macrophage activation in db/db mice. J Clin Biochem Nutr. 2015;56(3):240–246. doi:10.3164/jcbn.14-116
46. Ganguli K, Collado MC, Rautava J, et al. Lactobacillus rhamnosus GG and its SpaC pilus adhesin modulate inflammatory responsiveness and TLR-related gene expression in the fetal human gut. Pediatr Res. 2015;77(4):528–535.
47. Bermudez-Brito M, Munoz-Quezada S, Gomez-Llorente C, Romero F, Gil A. Lactobacillus rhamnosus and its cell-free culture supernatant differentially modulate inflammatory biomarkers in Escherichia coli-challenged human dendritic cells. Br J Nutr. 2014;111(10):1727–1737. doi:10.1017/S0007114513004303
48. McVey Neufeld KA, O’Mahony SM, Hoban AE, et al. Neurobehavioural effects of Lactobacillus rhamnosus GG alone and in combination with prebiotics polydextrose and galactooligosaccharide in male rats exposed to early-life stress. Nutr Neurosci. 2019;22(6):425–434. doi:10.1080/1028415X.2017.1397875
49. Kantak PA, Bobrow DN, Nyby JG. Obsessive–compulsive-like behaviors in house mice are attenuated by a probiotic (Lactobacillus rhamnosus GG). Behav Pharmacol. 2014;25(1):71–79. doi:10.1097/FBP.0000000000000013
50. Bravo JA, Forsythe P, Chew MV, et al. Ingestion of Lactobacillus strain regulates emotional behavior and central GABA receptor expression in a mouse via the vagus nerve. Proc Natl Acad Sci. 2011;108(38):16050–16055. doi:10.1073/pnas.1102999108
51. Pärtty A, Kalliomäki M, Wacklin P, Salminen S, Isolauri E. A possible link between early probiotic intervention and the risk of neuropsychiatric disorders later in childhood: a randomized trial. Ped Res. 2015;77(6):823–828. doi:10.1038/pr.2015.51
52. Kelly JR, Allen AP, Temko A, et al. Lost in translation? The potential psychobiotic Lactobacillus rhamnosus (JB-1) fails to modulate stress or cognitive performance in healthy male subjects. Brain Behav Immun. 2017;61:50–59. doi:10.1016/j.bbi.2016.11.018
53. Sanborn V, Azcarate-Peril MA, Updegraff J, Manderino LM, Gunstad J. A randomised clinical trial examining the impact of LGG probiotic supplementation on psychological status in middle-aged and older adults. Contemp Clin Trials Commun. 2018;12:192–197. doi:10.1016/j.conctc.2018.11.006
54. Chapman CMC, Gibson GR, Rowland I. Health benefits of probiotics: are mixtures more effective than single strains? Eur J Nutr. 2011;50(1):1–17. doi:10.1007/s00394-010-0166-z
55. Ouwehand AC, Invernici MM, Furlaneto FA, Messora MR. Effectiveness of multistrain versus single-strain probiotics: current status and recommendations for the future. J Clin Gastroenterol. 2018;52:S35–S40. doi:10.1097/MCG.0000000000001052
56. Heaton RK, Akshoomoff N, Tulsky D, et al. Reliability and validity of composite scores from the NIH toolbox cognition battery in adults. J Int Neuropsychol Soc. 2015;20(6):588–598.
57. Weintraub S, Dikmen SS, Heaton RK, et al. Cognition assessment using the NIH toolbox. Neurology. 2013;80(11 Suppl 3):S54–S64. doi:10.1212/WNL.0b013e3182872ded
58. Buckley RF, Sparks KP, Papp KV, et al. Computerised cognitive testing for use in clinical trials: a comparison of the NIH toolbox and cogstate C3 batteries. J Prev Alzheimers Dis. 2017;4(1):3–11.
59. Iglewicz B, Hoaglin DC. How to Detect and Handle Outliers. Vol. 16. Asq Press; 1993.
60. Gupta SK. Intention-to-treat concept: a review. Perspect Clin Res. 2011;2(3):109–112. doi:10.4103/2229-3485.83221
61. McCoy CE. Understanding the intention-to-treat principle in randomised controlled trials. West J Emerg Med. 2017;18(6):1075–1078. doi:10.5811/westjem.2017.8.35985
62. Blampied N. Reliable change & the reliable change index in the context of evidence-based practice: a tutorial review. 2016 [PowerPoint]. Available from: https://ir.canterbury.ac.nz/bitstream/handle/10092/13399/12664317_Reliable%20Change%5ETutorial%5ENZPsS%5E2016.pdf?sequence=1.
63. Schulz, KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Obstet Gynecol. 2010;115(5):1063–1063.
64. Ceccarelli G, Fratino M, Selvaggi C, et al. A pilot study on the effects of probiotic supplementation on neuropsychological performance and microRNA-29a-c levels in antiretroviral-treated HIV-1-infected patients. Brain Behav. 2017;7(8):e00756. doi:10.1002/brb3.756
65. Kobayashi Y, Kinoshita T, Matsumoto A, Yoshino K, Saito I, Xiao JZ. Bifidobacterium Breve A1 supplementation improved cognitive decline in older adults with mild cognitive impairment: an open-label, single-arm study. J Prev Alzheimers Dis. 2019;6(1):70–75.
66. Allen AP, Hutch W, Borre YE, et al. Bifidobacterium longum 1714 as a translational psychobiotic: modulation of stress, electrophysiology and neurocognition in healthy volunteers. Transl Psychiatry. 2016;6(11):e939. doi:10.1038/tp.2016.191
67. Eltokhi A, Janmaat IE, Genedi M, Haarman BC, Sommer IE. Dysregulation of synaptic pruning as a possible link between intestinal microbiota dysbiosis and neuropsychiatric disorders. J Neurosci Res. 2020;98(7):1335–1369. doi:10.1002/jnr.24616
68. Erny D, Hrabě de Angelis AL, Jaitin D, et al. Host microbiota constantly control maturation and function of microglia in the CNS. Nat Neurosci. 2015;18(7):965–977. doi:10.1038/nn.4030
69. MacFabe DF, Cain DP, Rodriguez-Capote K, et al. Neurobiological effects of intraventricular propionic acid in rats: possible role of short chain fatty acids on the pathogenesis and characteristics of autism spectrum disorders. Behav Brain Res. 2007;76(1):149–169. doi:10.1016/j.bbr.2006.07.025
70. Schroeder FA, Lin CL, Crusio WE, Akbarian S. Antidepressant-like effects of the histone deacetylase inhibitor, sodium butyrate, in the mouse. Biol Psychiatry. 2007;62(1):55–64. doi:10.1016/j.biopsych.2006.06.036
71. Khailova L, Petrie B, Baird CH, Dominguez Rieg JA, Wischmeyer PE. Lactobacillus rhamnosus GG and Bifidobacterium longum attenuate lung injury and inflammatory response in experimental sepsis. PLoS One. 2014;9(5):e97861. doi:10.1371/journal.pone.0097861
72. Luchsinger JA, Ma Y, Christophi CA, et al. Metformin, lifestyle intervention, and cognition in the diabetes prevention program outcomes study. Diabetes Care. 2017;40(7):958–965. doi:10.2337/dc16-2376
73. Samaras K, Lutgers HL, Kochan NA, et al. The impact of glucose disorders on cognition and brain volumes in the elderly: the Sydney memory and ageing study. Age. 2014;36(2):977–993.
74. Marsland AL, Gianaros PJ, Kuan DC-H, Sheu LK, Krajina K, Manuck SB. Brain morphology links systemic inflammation to cognitive function in midlife adults. Brain Behav Immun. 2015;48:195–204. doi:10.1016/j.bbi.2015.03.015
75. Bettcher BM, Kramer JH. Longitudinal inflammation, cognitive decline, and Alzheimer’s disease: a mini-review. Clin Pharmacol Ther. 2014;96(4):464–469. doi:10.1038/clpt.2014.147
76. Perry VH, Holmes C. Microglial priming in neurodegenerative disease. Nat Rev Neurol. 2014;10(4):217–224. doi:10.1038/nrneurol.2014.38
77. Turnbaugh PJ, Ridaura VK, Faith JJ, Rey FE, Knight R, Gordon JI. The effect of diet on the human gut microbiome: a metagenomic analysis in humanised gnotobiotic mice. Sci Transl Med. 2009;1(6):6ra14. doi:10.1126/scitranslmed.3000322
78. David LA, Maurice CF, Carmody RN, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. 2013;505(7484):559–563. doi:10.1038/nature12820
79. Roman P, Estévez AF, Miras A, et al. A pilot randomised controlled trial to explore cognitive and emotional effects of probiotics in fibromyalgia. Sci Rep. 2018;8(1):10965. doi:10.1038/s41598-018-29388-5
80. Akbari E, Asemi Z, Daneshvar Kakhaki R, et al. Effect of probiotic supplementation on cognitive function and metabolic status in Alzheimer’s disease: a randomised, double-blind and controlled trial. Front Aging Neurosci. 2016;8:256. doi:10.3389/fnagi.2016.00256
81. Reeve CL, Heggestad ED, Lievens F. Modeling the impact of test anxiety and test familiarity on the criterion-related validity of cognitive ability tests. Intelligence. 2009;37(1):34–41. doi:10.1016/j.intell.2008.05.003
82. Sanborn V, Azcarate-Peril MA, Gunstad J. The effects of medication adherence on study outcomes in randomized clinical trials: a role for cognitive dysfunction? Appl Neuropsychol Adult. 2019;1–6.
83. Volokh O, Tyakht A, Berezhnaya Y, Nesterova P, St. Peter JV. Human gut microbiome response induced by fermented dairy product intake. FASEB J. 2017;31(1):965.
84. Cheng R, Guo J, Pu F, et al. Loading ceftriaxone, vancomycin, and Bifidobacteria bifidum TMC3115 to neonatal mice could differently and consequently affect intestinal microbiota and immunity in adulthood. Sci Rep. 2019;9(1):3254. doi:10.1038/s41598-018-35737-1
85. Giacomin P, Croese J, Krause L, Loukas A, Cantacessi C. Suppression of inflammation by helminths: a role for the gut microbiota? Philos Trans R Soc Lond B Biol Sci. 2015;370:1675. doi:10.1098/rstb.2014.0296
86. Mariat D, Firmesse O, Levenez F, et al. The Firmicutes/Bacteroidetes ratio of the human microbiota changes with age. BMC Microbiol. 2009;9(1):123. doi:10.1186/1471-2180-9-123
87. Scalabrin D, Harris C, Johnston WH, Berseth CL. Long-term safety assessment in children who received hydrolyzed protein formulas with Lactobacillus rhamnosus GG: a 5-year follow-up. Eur J Pediatr. 2016;176(2):217–224. doi:10.1007/s00431-016-2825-4
88. Szajewska H, Horvath A. Lactobacillus rhamnosus GG in the primary prevention of eczema in children: a systematic review and meta-analysis. Nutrients. 2018;10(9):1319. doi:10.3390/nu10091319
89. Hibberd PL, Kleimola L, Fiorino AM, et al. No evidence of harms of probiotic Lactobacillus rhamnosus GG ATCC 53103 in healthy elderly—a phase I open label study to assess safety, tolerability and cytokine responses. PLoS One. 2014;9(12):e113456. doi:10.1371/journal.pone.0113456
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.